Embed Size (px)
Citation preview

[CANCER RESEARCH 49, 5385-5391, October 1, 1989]
Pharmacokinetics of Buthionine Sulfoximine (NSC 326231) and Its Effect onMelphalan-induced Toxicity in Mice1
Adaline C. Smith,2 James T. F. Liao, John G. Page, M. Guillaume Wientjes, and Charles K. Grieshaber
Toxicology Branch, Developmental Therapeutics Program, Division of Cancer Treatment, National Cancer Institute, Bethesda, Maryland 20892 [A. C. S., C. K. G.J;Springborn Life Sciences, Inc., Spencerville, Ohio 45887 [J. T. F. L.]; and Battelle Columbus Division, Columbus, Ohio 43201 [J. G. P., M. G. W.]
ABSTRACT
Intravenous doses of buthionine sulfoximine (BSO, NSC 326231), aninhibitor of glutathione synthesis, were eliminated rapidly from mouseplasma in a biexponential manner. The initial phase of the plasmaconcentration versus time curve had a half-life of 4.9 min and accountedfor 94% of the total area under the curve. The half-life of the terminalphase of the curve was 36.7 min and the area accounted for only 6% ofthe total area under the curve. Plasma clearance of BSO was 28.1 ml/min/kg and the steady state volume of distribution was 280 ml/kg. Theoral bioavailability of BSO, based on plasma BSO levels, was extremelylow. However, comparable glutathione depletion was apparent after i.v.and p.o. doses of BSO, suggesting a rapid tissue uptake and/or metabolism of BSO. Therefore, due to the rapid elimination of BSO from mouseplasma, plasma drug levels do not directly correlate with BSO-inducedtissue glutathione depletion. Administration of multiple i.v. doses of BSOto male and female mice resulted in a marked 88% depletion of liverglutathione at doses of 400-1600 mg/kg/dose. Toxicity of i.v. administered BSO was limited to a transient depression of peripheral WBClevels in female mice given six doses of 1600 mg/kg. Multiple i.v. dosesof BSO of up to 800 mg/kg/dose (every 4 h for a total of six doses) didnot alter the toxicity of i.v. administered melphalan. However, multipledoses of 1600 mg/kg/dose of BSO did potentiate histopathological evidence of melphalan-induced bone marrow toxicity in 30% of the miceand, additionally, the combination of BSO and melphalan produced renaltubular necrosis in 80% of the male mice. The potentiation of melphalan-induced toxicity did not appear to be related to GSH depletion, since aquantitatively similar amount of GSH depletion occurred at lower dosesof BSO without any increase in melphalan toxicity.
INTRODUCTION
Treatment of certain types of neoplasms with chemothera-peutic agents is frequently hindered by the development ofresistance of tumor cells to the antineoplastic agents. There area number of specific biochemical alterations, such as decreaseddrug uptake, increased drug efflux, and increased drug metabolism, which occur in resistant tumor cells and explain thedevelopment of cellular resistance to some types of cytotoxicchemotherapeutic agents (1, 2). Recently, evidence has beencollected which suggests that in some tumors clinical resistancemay be correlated to the ability of tumor cells to detoxify thecytotoxic moiety of the antineoplastic agent (3).
Intracellular GSH3 provides one of the primary mechanisms
by which cells detoxify activated molecules, including variouschemotherapeutic agents. GSH, a ubiquitously distributed in-tracellular sulfhydryl tripeptide, normally protects cells fromdamage produced by toxic agents either by binding directly tothe activated molecule or by providing reducing equivalents (4,
Received 2/22/89; revised 6/2/89; accepted 6/23/89.The costs of publication of this article were defrayed in part by the payment
of page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
1This work was supported by Contracts NOl-CM-17365andNOl-CM-87256
from the National Cancer Institute.2To whom requests for reprints should be addressed, at Toxicology Branch,
DTP, DCT, National Cancer Institute, Executive Plaza North, Room 843,Bethesda, M D 20892.
1The abbreviations used are: GSH, glutathione; BSO, i.-buthionine sulfoxi
mine; VCTL, vehicle; AUC, area under the plasma concentration versus timecurve.
5). Ozols et al. (6-8) have developed a human ovarian tumormodel system which consists of cell lines derived from tumorsthat are clinically resistant to alkylating agents and from chemotherapy-sensitive tumors. Intracellular GSH is highest in thecell lines derived from clinically resistant tumors, while GSHlevels are comparatively much lower in cell lines derived fromtumors that are clinically sensitive to cytotoxic chemotherapeutic agents (9, 10). The same GSH pattern was also described inmurine L1210 leukemia cell lines (11-13) and in human me-dulloblastoma cell lines (14); cell lines that are resistant toalkylating agents have much higher levels of intracellular GSHthan cell lines which were sensitive to cytotoxic chemotherapeutic agents.
The correlation of tumor cell glutathione to the relativesensitivity of cells to cytotoxic chemotherapeutic agents can beexploited therapeutically (4, 15, 16). In theory, depletion ofintracellular glutathione in tumor cells should allow subsequently administered chemotherapy to be more efficacious.BSO is a selective inhibitor of glutathione biosynthesis (15, 17)which produces a dose-dependent depletion of intracellularglutathione in vitro and in vivo in both tumor tissue and normaltissue (18). In tumor-bearing mice, BSO pretreatment increasedthe efficacy of several chemotherapeutic agents, such as mito-mycin C (19), melphalan (13, 20-22), cisplatin (23), bleomycin(23), and cyclophosphamide (19, 24, 25). In most animal tumormodels, BSO administered as a single agent at doses whichproduced GSH depletion did not alter tumor growth in vitro(21, 26-28) or in tumor-bearing mice (22, 24, 31) and, additionally, BSO alone did not alter tumor-associated lethality (13,20, 30). However, exposure of tumor cells to high concentrations of BSO for extended periods inhibits protein and DNAsynthesis (29) and tumor cell survival in clonogenic assays (30).
The ability of BSO pretreatment to potentiate the efficacy ofcancer chemotherapeutic agents is dependent on the cytotoxicagent and the tumor model system. BSO given prior to theadministration of melphalan or cyclophosphamide markedlyenhanced the efficacy of the cytotoxic agent, as measured byclonogenic assays (13, 19, 23, 31), and there is an increase inlife span of mice treated with BSO and melphalan, comparedwith mice treated with melphalan alone, in animal models forhuman ovarian (20) and medulloblastoma (22) tumors. BSOpretreatment, however, does not potentiate the efficacy of allchemotherapeutic agents in all types of tumor models. In sometumor-bearing murine models, BSO pretreatment does not alter
the efficacy of various chemotherapeutic agents (32) or, eventhough the cytotoxicity of the chemotherapeutic agent is increased by BSO pretreatment, there is no increase in animalsurvival (13). These apparent discrepancies may be due todifferences in the kinetics of tumor cell growth, BSO pretreatment schedule, and/or the inherent sensitivity of the tumorcells to the particular chemotherapeutic agent.
Because BSO pretreatment has been shown preclinically topotentiate the efficacy of some cytotoxic chemotherapeuticagents, the National Cancer Institute is developing BSO as anadjuvant to cancer chemotherapy. The present studies were
5385
Research. on August 16, 2019. © 1989 American Association for Cancercancerres.aacrjournals.org Downloaded from

BSO PHARMACOKINETICS AND TOXICITY
designed to describe the pharmacokinetics of BSO and toevaluate the toxicity of BSO and its effect on the toxicity ofmelphalan in BALB/c x DBA/2 F, (hereafter called CD2F,)mice, in preparation for clinical trials of this combinationchemotherapy.
MATERIALS AND METHODS
Animals. CD2F, mice were supplied by Charles River Laboratories,Inc., through the Animal Genetics and Production Branch, Developmental Therapeutics Program, Division of Cancer Treatment, NationalCancer Institute. Mice were maintained on a 12-h light, 12-h dark cycleand had free access to food and water.
Chemicals. L-Buthionine(S,R)sulfoximine (NSC 326231) and melphalan (NSC 8806) were clinical formulations supplied by the Pharmaceutical Resources Branch, Developmental Therapeutics Program,Division of Cancer Treatment, National Cancer Institute. All otherchemicals were obtained from commercial sources.
Pharmacokinetic and Bioavailability Studies. BSO or vehicle (0.9%sodium chloride) was administered either p.o. by gavage or i.v. in thetail vein. Blood samples were obtained by cardiac puncture into aheparinized syringe. Plasma was isolated by centrifugation, removed,pooled, and either frozen at —¿�20°Cfor plasma BSO determination or
immediately processed for plasma GSH determination. Liver, lung,and kidney were removed, rinsed, weighed, frozen in liquid nitrogen,and stored at —¿�70°Cfor tissue GSH determination. BSO plasma
concentrations were analyzed by standard pharmacokinetic techniques(34). The area under the plasma concentration versus time curve andthe first moment curve were determined by the linear trapezoidal rule.Half-lives were determined from the best fit of a biexponential equationto the plasma concentration-time profile. The fit was determined witha nonlinear regression routine. Other parameters were calculated asindicated in Table 1.
Plasma BSO Analysis. Pooled plasma BSO was determined by themethod described by Duff and Murrill (35). Briefly, plasma samples(0.5 ml) were placed in culture tubes with Teflon-lined caps andmethanol (2 ml) was added to precipitate macromolecules. After centrifugation, a 1.0 nil aliquot of the supernatant was removed and addedto 0.2 ml of the derivatizing reagent. The derivatizing reagent wasprepared by dissolving 200 mg of o-phthalaldehyde in 5 ml of methanol,adding 0.2 ml of 2-mercaptoethanol, and diluting with 0.01 M sodiumborate buffer (pH 9.5) to 50 ml. After derivatization, samples werefiltered through an unwetted Sep-PaK C,8 solid phase extraction cartridge and a 0.5-ml aliquot of the derivatized samples was spiked with0.1 ml of butyrophenone (1.3 mg/liter methanol) as the internal standard. Standard curves were prepared by spiking untreated mouse plasmasamples with 0 to 100 mg BSO/ml plasma. Separation of BSO fromother plasma constituents was performed by high pressure liquid chro-matography on an Altex Ultrasphere C,8 column using an isocraticgradient solvent system. Solution A (0.005 M tetrabutylammoniumhydroxide adjusted to pH 7.4 with phosphoric acid) and solution B(100% methanol) were used for the mobile phase. The elution programwas initiated with a solvent ratio of 51% solution A/49% solution B,which ran for 40 min. This was followed by a linear gradient for thenext 10 min to reach a solvent ratio of 30% solution A/10% solutionB. This ratio was held for 5 min before returning to initial conditions.Derivatized BSO was detected by fluorescence at excitation wavelengthof 340 nm and emission wavelength of 491 nm; the internal standardwas detected by UV absorbance at 254 nm.
Clutathione Analysis. Pooled plasma (0.5 ml) was mixed with cold25% perchloric acid (0.125 ml) to precipitate proteins. The mixturewas centrifuged and the supernatant was removed. An aliquot of thesupernatant was buffered to pH 7.0 with 2 N KOH/0.3 M 2-(N-morpholino) ethanesulfonic acid, the samples were centrifuged, andsupernatants were removed for GSH determinations. Frozen tissuesamples were homogenized in 4 volumes of cold 5% perchloric acid.After centrifugation, supernatant was removed and diluted 10- to 20-fold with 0. l Mphosphate buffer (pH 7.4). Glutathione was determinedby the method described by Akerboom and Sies (36), as modified bySmith and Boyd (37).
BSO Toxicity Studies. Male and female CD2F, mice (6-8 weeks old)were treated with either 400, 800, or 1600 mg/kg BSO or VCTL i.v.every 4 h for a total of six doses. Liver glutathione was determined inone group of mice five BSO-treated male mice from each BSO dosegroup and five vehicle-treated male mice) l h after the fifth dose ofBSO or VCTL. The other groups of mice were observed daily foradverse clinical signs and mortality. Blood samples for clinical pathology determinations (consisting of hematology and clinical chemistryparameters) were taken on study days 2, 8, 15, 22, and 29. Hematologyparameters measured were RBC count, hemoglobin, hematocrit, platelet count, reticulocyte count, total WBC, differential leukocyte count,and nucleated RBC count. Clinical chemistry parameters determinedwere blood urea nitrogen, serum alanine transaminase, serum aspartatetransaminase, and total protein. Complete gross pathological and his-topathological evaluations were done on animals necropsied on studydays 2 and 29. Tissues [bone (femur), bone marrow, brain, colon,duodenum, gonads (ovaries, testes), heart, ileum, jejunum, kidney, liver,lung, lymph nodes, pancreas, spleen, stomach, and thymus] were fixedin buffered formalin and 5-^m paraffin sections were stained withhematoxylin and eosin.
In the BSO plus melphalan combination study, 400, 800, or 1600mg/kg BSO or VCTL was administered i.v. every 4 h for a total of sixdoses. One h after the fifth dose of BSO, 5 mg/kg (15 mg/m2) melphalan
was administered at 4 p.m. on study day 1. Before melphalan administration, five BSO-treated male mice from each dose group and fiveVCTL-treated male mice were used for liver glutathione determinations. Blood samples for clinical pathology determinations were takenon study days 2, 4, 6, 11, 17, and 30. Complete gross pathological andhistopathological evaluations were done on mice necropsied on studydays 2, 6, and 30.
Statistical Methods. Statistical analyses were performed by comparing control group data with treated using either paired / tests or oneway analysis of variance coupled with Duncan's multiple range test.
RESULTS
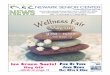
The plasma concentration versus time curve (Fig. 1) after i.v.dosing revealed a biexponential disappearance for BSO. Thehalf-life of the initial phase was 4.9 min, while the half-life ofthe terminal phase was 36.7 min (Table 1). The AUC of theinitial phase accounted for approximately 94% of the total areaunder the curve, while the AUC of the terminal phase accountedfor only 6% of the total AUC. The steady state volume ofdistribution (Kdss)was 280 ml/kg and was severalfold smallerthan the terminal volume (Fdlcrm).Since the elimination of BSOfrom plasma occurred during the initial phase, the ydsswas felt
to be the more appropriate term to represent the distribution
10,000
1000
100
10
40 60TIME (minutes)
100
Fig. 1. Plasma BSO elimination in male CD2F, mice. A dose of 800 mg/kgBSO was administered i.v. Plasma from six mice was collected at the indicatedtimes and the plasma from three mice was pooled for drug level analysis. Eachline represents the BSO concentration obtained from the pooled plasma fromthree mice.
5386
Research. on August 16, 2019. © 1989 American Association for Cancercancerres.aacrjournals.org Downloaded from

BSD PHARMACOKINETICS AND TOXICITY
Table 1 Pharmacokinelic analysis of plasma BSO concentrations in CD2F, miceafter 800 mg/kg i. v. dose of BSO
Parameters (units)" Calculation Estimated
AUC (fig/ml xmin)Cl(ml/min/kg)rWA(min)rWB(min)AUMC
(jig/ml xmin2)>,,.
(min)Ki"(ml/kg)K,"'m
(ml/kg)C*DTD/AUCC*DTAUMC/AUCt^-ciCY/(0.693/IKB)28,50028.14.8936.7284,0009.962801,490
°C, BSO plasma concentration; CI, plasma clearance; D, dose (mg); Õ,AA,half-life of initial disposition phase; r*,B,half-life of terminal disposition phase; AUMC,area under the first moment curve; tm, mean residence time; Ki", apparent volumeof distribution at steady state; K,1"™,apparent volume of distribution during the
terminal phase.
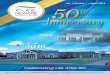
Fig. 2. Sample chromatogram of plasma BSO high pressure liquid chroma-tography analysis.. I. Sample chromatogram of mouse plasma spiked with 20 nnof BSO; B, chromatogram of plasma BSO concentration 60 min after a singlei.v. dose of 800 mg/kg BSO.
volume of BSO. Plasma clearance of BSO in CD2F, mice was28. 1 ml/min/kg. Interestingly, the two stereoisomers of BSOform a double peak in this chromatography system (Fig. 2).These peaks are approximately the same height in spikedplasma samples and in the plasma samples drawn soon afterdosing (e.g., 2-min sampling time). However, the two stereoisomers disappeared from the plasma very differently. The ster-eoisomer which élûtesfirst disappears more quickly than thesecond. Oral administration of BSO (800 mg/kg) did not resultin measurable plasma drug levels except at l h after dosing (1 1
Plasma and liver GSH levels after p.o. and i.v. dosing areshown in Fig. 3. Liver GSH depletion was similar to plasmaGSH depletion after p.o. and i.v. BSO administration. Maximum depletion of 64-67% (33-36% of control values) wasobserved in liver GSH 2-4 h after i.v. and 2-8 h after p.o. BSOadministration. Liver GSH levels returned to control values 8-12 h after i.v. or p.o. doses of BSO. Maximum plasma gluta-thione depletion was 78% (22% of control values) after bothp.o. and i.v. administered BSO. Recovery of plasma GSH afteri.v. administration of BSO was relatively rapid; levels were notdifferent from control values 16 h after BSO. Kidney GSHlevels were depleted by 78 and 77% (22 and 23% of controlvalues) and lung GSH levels were depleted by 29 and 20% (71and 80% of control values), respectively, 4 h after a single i.v.or p.o. dose of BSO (Table 2).
Clinically, it is proposed that multiple i.v. doses of BSO beadministered to produce maximal GSH depletion before theadministration of a cytotoxic chemotherapeutic agent, such asmelphalan. Therefore, the toxicity of BSO was evaluated inCD2P! mice following multiple i.v. doses to produce and maintain maximal GSH depletion. The data in Fig. 3 indicate thatmaximal plasma and liver GSH depletion occurs 4 h after asingle i.v. 800 mg/kg dose of BSO. The administration of 400,800, or 1600 mg/kg BSO i.v. every 4 h for a total of six dosesresulted in an 85-89% reduction in liver GSH, measured l hafter the fifth dose of BSO. Each of the three dose levels ofBSO produced a quantitatively similar amount of liver GSHdepletion; thus there is no apparent dose response. The onlytoxicity produced by multiple doses of BSO was a substantial75% decrease in WBC 12 h following the last dose of BSO infemale mice given 1600 mg/kg (Fig. 4). This WBC depressionwas not associated with histopathological evidence of bonemarrow atrophy or aplasia and WBC values had returned toand remained in the control range beginning on study day 8.There were no clinical signs of toxicity or changes in clinicalchemistry parameters and no gross or histopathological lesionswere detected after BSO was given by this dosing regimen.
Melphalan administered at a dose of 5 mg/kg ( 15 mg/m2)
produced microscopic evidence of gastrointestinal toxicity onday 2 and a reversible depression of peripheral WBC values inmale and female mice (Table 3; Fig. 5). Histopathologically,thymic atrophy was present in all melphalan-treated mice onday 6, but no bone marrow atrophy occurred after the administration of this dose of melphalan. Pretreatment of mice withup to 800 mg/kg BSO i.v. every 4 h for a total of five dosesprior to melphalan administration and an additional BSO doseafter melphalan administration did not potentiate melphalan-induced leukopenia (Fig. 5). In mice given doses of 1600 mg/kg BSO every 4 h for a total of six doses, BSO did not affectthe WBC nadir but did appear to delay the recovery of WBCvalues after melphalan administration in both male and femalemice. In this dose group, 30% of the mice had histopathologicalevidence of bone marrow atrophy accompanied by splenic mye-loid tissue atrophy on day 6 (Table 3). In addition, melphalanadministration to mice treated with multiple doses of 1600 mg/kg BSO produced a rise in blood urea nitrogen (peak levels,47-117 mg/dl) and histopathological evidence of renal tubularnecrosis on day 6 (Fig. 6). The tubular necrosis was characterized by loss of nuclear and cytoplasmic detail and was accompanied by regeneration/hyperplasia. The incidence of renaltubular necrosis was very high, occurring in 80% of the male
•¿�.«.uÄ
aI.iifeJi
iili
Ed1r0
1EOO
mg.VB >VBOO
mgfcgpòRil2
4 8 12IflTIME
(HOURS)1
1-,20
240 1 24 6 12 16 20 24
TIME IHOURS)
Fig. 3. Effect of a single i.v. or p.o. dose of BSO on liver and plasma GSH.Male CD2F| mice were treated with 800 mg/kg BSO and liver (left) and plasma(right) GSH levels were determined at the indicated times. Liver GSH values arethe mean ±SE of six determinations. Plasma from three mice was pooled forGSH determination. Plasma values are the average of two determinations. *,mean significantly (P < 0.05) different from the control values.
5387
Research. on August 16, 2019. © 1989 American Association for Cancercancerres.aacrjournals.org Downloaded from

BSO PHARMACOKINETICS AND TOXICITY
Table 2 Comparison of liver, lung, and kidney glulalhione levels
GSH level
TissueLiver
LungKidneyVCTL/jmol/g5.88
±0.86* (4)r
2.31 ±0.17 (4)3.03 + 0.42 (4)%of
control100
100100i.V."/xmol/g1.96
±0.42 (4)1.63 + 0.20(4)0.68 ±0.08 (4)%of
control33"
71"22"p.o.°iimol/g2.12+ 0.56(4)
1.84 + 0.09(4)0.69 ±0.02 (4)%of
control36"
80"23"
" Tissue samples were taken 4 h after 800 mg/kg i.v. or p.o. dose of BSO.' Mean ±SD.e Numbers in parentheses, number of mice.d Mean values are statistically different from the VCTL (P < 0.05).
DAY IN STUDY
10 15 20
DAY IN STUDY
Fig. 4. Effect of multiple doses of BSO on WBC levels. Mice were treatedwith the indicated i.v. doses of BSO every 4 h for a total of six doses. Blood wasobtained and WBC levels were determined in male (left) and female (right) CD2F¡mice. Values represent mean + SE of five determinations. *, mean significantly
(P < 0.05) different from control values.
mice and 20% of the female mice. All lesions were reversible,nonprogressive, and completely resolved by study day 30.
DISCUSSION
There is substantial clinical interest in evaluating the effectof BSO-induced tumor tissue GSH depletion on the efficacy ofchemotherapeutic agents used in the treatment of cancer (1,3).The present studies were designed to describe the pharmacoki-netics of BSO in mouse plasma, correlate them with tissue GSHdepletion, and evaluate the toxicity of multiple doses of BSOalone and in combination with melphalan, a potent bifunctionalalkylating agent used to treat a variety of neoplastic diseases.
We have shown that BSO administered i.v. is cleared veryrapidly from mouse plasma, whereas plasma BSO levels afterp.o. administration of the drug were much lower and at mosttimes undetectable. These data suggest that BSO is either (a)poorly absorbed from the gastrointestinal system or (b) absorbed but rapidly removed and/or metabolized by the liver orother tissues. Since quantitatively similar GSH depletion occurred after comparable p.o. and i.v. doses of BSO in all tissues
examined (lung, liver, and kidney), effective amounts of BSOmust have been absorbed from the gastrointestinal tract. Thereare several possibilities which could explain the apparent absorption of effective BSO doses in the absence of detectableplasma concentrations. It is possible that (a) very small plasmaconcentrations of BSO (below the limit of detection of theanalytical method) are necessary for GSH depletion or (b) BSOcould be metabolized to a metabolite which is also able toinhibit GSH synthesis. Plasma BSO pharmacokinetic parameters or plasma BSO levels did not correlate with the amount ofGSH depletion, due to the rapid removal of BSO from plasmaafter i.v. administration and unmeasurable plasma BSO levelsafter p.o. administration. Therefore, measuring plasma BSOlevels does not permit one to estimate the degree of GSHdepletion, at least preclinically.
The toxicity of BSO and the resultant GSH depletion hasnot been widely addressed. BSO administered p.o. in drinkingwater to mice, at concentrations up to 30 HIM for 30 daysproduced up to 60% reduction in tissue GSH, depending onthe tissue measured, with no evidence of acute toxicity (38).Single i.p. or p.o. doses of 5 g/kg BSO have also been reportedto be nontoxic (33). In other preclinical studies in CD2F, mice,p.o. administration of up to 800 mg/kg/dose of BSO givenevery 8 h for a total of 15 doses (5 days) did not induce anyclinical signs of toxicity, hematological or clinical chemistrychanges, or histopathological lesions (39). The present studiessuggest that BSO administered i.v. at doses up to 800 mg/kg/dose every 4 h for a total of six doses also produced substantialGSH depletion with no measurable acute toxicity. The onlyevidence of toxicity was WBC depletion, which occurred whenmultiple i.v. doses of 1600 mg/kg/dose were administered tofemale CD2F| mice (Fig. 4). This WBC depletion was mild andtransient and was unaccompanied by histopathological evidenceof bone marrow atrophy. Other investigators have reported thatBSO alone did not produce any WBC depletion in mice (13,33, 40) and in these studies there were no adverse effects onbone marrow stem cells (31, 33, 40). Therefore, BSO alone isnot myelotoxic, except potentially at very high, multiple i.v.doses of drug.
Table 3 Toxicity of BSO alone and in combination with melphalan
BSOO,* mei- BSO400,phalan5f melphalan0Microscopic
lesions"NoneBone
marrowatrophyRenalnecrosisSmall
intestinalnecrosisSplenicmyeloidatrophyThymicatrophyM"5/55/5F
MF5/5
5/55/55/5BSO400,
BSO 800, BSO 800, BSO1600,BSO1600,melphalan5 melphalan 0 melphalan 5 melphalan 0 melphalan5M5/55/5F
M5/55/55/5F M5/55/55/5F M5/55/55/5F M5/52/54/55/52/55/5F1/51/55/51/55/5
°Incidence of lesion occurrence as number of mice with lesion/total number of mice examined.* Dose of BSO (mg/kg/dose) or VCTL administered i.v. every 4 h for a total of six doses.' Dose of melphalan (mg/kg) or VCTL administered i.v. l h after the fifth dose of BSO.d M, male; F, female
5388
Research. on August 16, 2019. © 1989 American Association for Cancercancerres.aacrjournals.org Downloaded from

BSO PHARMACOKINETICS AND TOXICITY
10 15 20 25 30 35
DAY IN STUDY
10 15 20 25 30
DAY IN STUDY
Fig. 5. Effect of multiple doses of BSO on melphalan-induced WBC depletion.Mice were treated with the indicated doses of BSO every 4 h for a total of sixdoses. One h after the fifth dose of BSO, melphalan (5 mg/kg, 15 mg/m;) was
administered i.V. Blood was obtained and WBC levels were determined in male(left) and female (right) CD2Fi mice. Values represent mean ±SE of fivedeterminations. *, mean significantly (P < 0.05) different from control values.
Combining BSO with cytotoxic chemotherapeutic agents presents a different set of toxicological questions. Theoretically,BSO-induced GSH depletion could potentiate known toxicitiesof the chemotherapeutic agent or the combination of BSO andthe chemotherapeutic agent could produce new types of dose-limiting toxicities. Only a few studies have addressed the effectof BSO pretreatment and the resultant GSH depletion on thetoxicity of antineoplastic agents. Methylcyclohexylchloroethyl-nitrosourea, a potent alkylating nitrosourea, has been shown tobe nephrotoxic, but not hepatotoxic, when administered toFischer 344 rats. BSO pretreatment potentiates the nephrotox-icity of methylcyclohexylchloroethylnitrosourea and, additionally, the combination produces hepatotoxicity in Fischer 344rats (41). Conversely, Mayer et al. (42) provide evidence thatBSO pretreatment decreases the nephrotoxicity of cisplatin,even though another study suggested that GSH depletion produced by administration of diethylmaleate, a compound thatdirectly binds to GSH, potentiates the nephrotoxicity of cisplatin (43). Kramer et al. (13) suggested that BSO pretreatmentdid increase the lethality of melphalan but the potentiation oflethality was dependent on the route of BSO administrationand the extent of GSH depletion. Additionally, much higher(10-40 mg/kg) i.p. doses of melphalan were used in thesestudies than were used in the present study. Therefore, it isclear that GSH depletion can markedly affect the toxicity ofcertain cancer chemotherapeutic agents in animal models.
Clinically, i.v. doses of melphalan produce a dose-limitingmyelosuppression, characterized by both leukopenia andthrombocytopenia. High doses of melphalan produce dose-limiting gastrointestinal toxicity in cancer patients given bonemarrow transplants to offset the myelosuppressive effects ofthe drug (44). Myelosuppression and gastrointestinal toxicityare produced in mice by doses of melphalan (15 mg/m2) which
are comparable to the doses that produce similar toxicity inhumans (20 mg/m2). The similarity in the pattern of toxicity at
similar doses of melphalan suggests that CD2F, mice are anacceptable preclinical animal model to evaluate melphalan-induced toxicity.
BSO treatment at doses up to 800 mg/kg/dose (every 4 h fora total of six doses) did not have any effect on the myelosuppression produced by melphalan administration. However, pretreatment of mice with multiple doses of 1600 mg/kg/dose of BSOsignificantly altered the pattern of melphalan toxicity. Firstly,the myelotoxicity of melphalan was potentiated by BSO treatment, as evidenced by histologically identifiable bone marrow
B
.
•¿�
Fig. 6. Effect of BSO and melphalan on renal histopathology. A, Representative photomicrograph of a stained section of renal cortex taken from a mousetreated with multiple 1600 mg/kg doses of BSO (every 4 h x 6) and one 5 mg/kg dose of melphalan l h after the fifth dose of BSO. Note the areas of necrosis(open arrow) characterized by loss of nuclear and cytoplasmic detail. Tubularregeneration/hyperplasia (solid arrow) is characterized by cytoplasmic basophiliaand increased numbers of tubular epithelial cells. B, Higher magnification oftubular necrosis (open arrow) and mild regeneration (solid arrow).
atrophy accompanied by splenic myeloid tissue atrophy, eventhough there appeared to be no significant change in the peripheral WBC nadir. The recovery of WBC counts to controllevels was delayed in mice treated at the highest dose level ofBSO and melphalan, which has been observed and reported byother investigators (13). The potentiation of bone marrow toxicity was considered to be relatively slight, since the incidencewas low (30%), the bone marrow lesions were not severe andwere readily reversible, and there was no drug-induced mortality
caused by this combination.Surprisingly, the combination of melphalan with multiple
1600 mg/kg doses of BSO was nephrotoxic, as evidenced byincreases in blood urea nitrogen and histopathological lesions.Evidence of renal toxicity did not occur with either agent alone.The incidence of the nephrotoxicity was very high in male mice(80%) and it was readily reversible. The only suggestion in theclinical literature that melphalan administration is linked to
5389
Research. on August 16, 2019. © 1989 American Association for Cancercancerres.aacrjournals.org Downloaded from

BSO PHARMACOKINETICS AND TOXICITY
renal toxicity appeared in a study in which high doses ofmelphalan were administered with other cytotoxic agents (cy-clophosphamide, cisplatin, and bis-chloroethylnitrosourea)with bone marrow transplantation support (45). From this ' '
clinical study, it is impossible to determine whether melphalanis responsible for the observed renal toxicity: (a) melphalan 12administered as a single agent at similar doses has not beenreported to be nephrotoxic (44); and (b) cisplatin, one of theother agents administered, is a known nephrotoxic agent. The 13
authors suggest that the addition of melphalan to the combination produced the nephrotoxicity but melphalan may be '•»
potentiating the nephrotoxicity produced by any or all of theagent(s) in this combination or, conversely, one or all of theother agent(s) may be inducing the nephrotoxicity by mei- 15
phalan.The renal toxicity produced by BSO pretreatment and mei- 16
phalan administration did not appear to be related to theamount of glutathione depletion, since multiple doses of 400to 1600 mg/kg/dose of BSO produced comparable reductionsof tissue GSH concentrations. Renal toxicity was noted only '<!
after a combination of melphalan and 1600 mg/kg/dose ofBSO; therefore, GSH depletion cannot explain the effect of this '9
combination on the kidneys. This information suggests that,clinically, dose escalation of BSO above levels needed for maximal GSH depletion should be approached cautiously.
In summary, BSO did not alter the dose-limiting toxicity ofmelphalan in preclinical studies ¡nCD2F, mice except at extremely high (1600 mg/kg/dose) multiple i.v. doses of BSO. 21
This combination of high multiple doses of BSO prior to asingle dose of melphalan produced nephrotoxicity and increased 22the myelotoxicity of melphalan.
ACKNOWLEDGMENTS
The authors would like to thank Karen McNeill, Diane Habash, andKate Colling at Battelle Columbus Division and Todd Merriman andDr. Kevin Michlewicz at Springborn Life Sciences for their excellenttechnical assistance. The authors would also like to thank Dr. WilliamCollins, Jr., at Springborn Life Sciences for reading the histology slidesand Dr. Michael Stedham at Pathology Associates, Inc., for makingthe photomicrographs.
REFERENCES
20.
23.
24.
26.
27.
28.1. Ozols, R. F., Masuda, II.. and Hamilton, T. C. Keynote address: mechanisms
of cross-resistance between radiation and antineoplastic drugs. Nati. CancerInst. Monogr., 6: 159-165, 1988. 29-
2. Gottesman, M. M.. and Pastan, I. Resistance to multiple chemotherapeuticagents in human cancer cells. Trends Pharmacol. Sci., 9: 54-58, 1988.
3. Fojo, A., Hamilton, T. C., Young, R. C., and Ozols, R. F. Multidrugresistance in ovarian cancer. Cancer (Phila.), 60: 2075-2080, 1987. 30.
4. Meister, A. Selective modification of glutathione metabolism. Science (Wash.DC), 220: 472-477, 1983.
5. Meister, A., and Anderson, M. E. Glutathione. Annu. Rev. Biochem., 52: 31.711-760, 1983.
6. Hamilton, T. C., Young, R. C., Louie, K. G., Behrens. B. C., McKoy, W.M., Grotzinger, K. R., and Ozols, R. F. Characterization of a xenographmodel of human ovarian carcinoma which produces ascites and intra-abdom- 32.ina) carcinomatosis. Cancer Res., 44: 5286-5290, 1984.
7. Hamilton, T. C., Winker, M. A., Louie, K. G., Batist, G., Behrens, B. C.,Tsuruo, T., Grotzinger, K. R., McKoy, W. M., Young, R. C., and Ozols, R. 33.F. Augmentation of adriamycin, melphalan, and cisplatin cytotoxicity indrug-resistant and -sensitive human ovarian carcinoma cell lines by buthion-ine sulfoximine mediated glutathione depletion. Biochem. Pharmacol., 34: 34.2583-2586, 1985.
8. Ozols, R. F. Pharmacologie reversal of drug resistance in ovarian cancer.Semin. Oncol., 12 (Suppl. 4): 7-11, 1985. 35.
9. Green, J. A., Vistica, D. T., Young, R. C., Hamilton, T. C., Rogan, A. M.,and Ozols, R. F. Potentiation of melphalan cytotoxicity in human ovariancancer cell lines by glutathione depletion. Cancer Res.. 44: 5427-5431,1984.
10. Louie, K. G., Behrens, B. C., k insci la. T. J., Hamilton, T. C., Grotzinger, 36.
5390
K. R., McKoy, W. M., Winker, M. A., and Ozols, R. F. Radiation survivalparameters of antineoplastic drug-sensitive and -resistant human ovariancancer cell lines and their modification by buthionine sulfoximine. CancerRes., ¥5:2110-2115, 1985.Suzukake, K., Vistica, B. P., and Vistica, D. T. Dechlorination of L-phenyl-alanine mustard by sensitive and resistant tumor cells and its relationship tointracellular glutathione content. Biochem. Pharmacol., 32: 165-167, 1983.Somfai-Relle, S., Suzukake, K., Vistica, B. P., and Vistica, D. T. Reductionin cellular glutathione by buthionine sulfoximine and sensitization of murinetumor cells resistant to L-phenylalanine mustard. Biochem. Pharmacol., 33:485-490, 1984.Kramer, R. A., Greene. K., Ahmad, S., and Vistica, D. T. Chemosensitizationof L-phenylalanine mustard by the thiol-modulating agent buthionine sulfoximine. Cancer Res., 47:1593-1597, 1987.Friedman, H. S., Skapek, S. X., Colvin, O. M., Elion, G. B., Blum, M. R.,Savina, P. M., Hilton, J., Schold, S. C., Kurtzberg, J., and Bigner, D. D.Melphalan transport, glutathione levels, and glutathione-5-transferase activity in human medulloblastoma. Cancer Res., 48: 5397-5402, 1988.Meister, A., and Griffith, O. W. Effects of methionine sulfoximine analogson the synthesis of glutamine and glutathione: possible chemotherapeuticimplications. Cancer Treat. Rep., 63: 1115-1121, 1979.Arrick, B. A., and Nathan, C. F. Glutathione metabolism as a determinantof therapeutic efficacy: a review. Cancer Res., 44:4224-4232, 1984.Griffith, O. W. Mechanism of action, metabolism and toxicity of buthioninesulfoximine and its higher homologs, potent inhibitors of glutathione synthesis. J. Biol. Chem., 257: 13704-13712, 1982.Lee, F. Y. F., Allalunis-Turner, M. J., and Siemann, D. W. Depletion oftumour versus normal tissue glutathione by buthionine sulfoximine. Br. J.Cancer, 56: 33-38, 1987.Ono, K., and Shrieve, D. C. Enhancement of EMT6/SF tumor cell killingby mitomycin c and cyclophosphamide following in vivo administration ofbuthionine sulfoximine. Int. J. Radial. Oncol. Biol. Phys., 12: 1175-1178,1986.Ozols, R. F., Louie, K. G., Plowman, J., Behrens, B. C., Fine, R. L., Dykes,D., and Hamilton, T. C. Enhanced melphalan cytotoxicity in human ovariancancer in vitro and in tumor-bearing nude mice by buthionine sulfoximinedepletion of glutathione. Biochem. Pharmacol., 36: 147-153, 1987.Dorr, R. T. Reduced thiol content in I 1210 cells treated with BSO increasesDNA cross-linking by melphalan. Biochem. Biophys. Res. Commun., 144:47-52, 1987.Skapek, S. X., Colvin, M., Griffith, O. W., Elion, G. B., Bigner, D. D., andFriedman, H. S. Enhanced melphalan cytotoxicity following buthioninesulfoximine-mediated glutathione depletion in human medulloblastoma xenograph in athymic mice. Cancer Res., 48: 2764-2767, 1988.Tsutsui, K., Komuro, C., Ono, K., Nishida, T., Shibamoto, Y., Takahashi,M., and Abe, M. Chemosensitization by buthionine sulfoximine in vivo. Int.J. Radiât.Oncol. Biol. Phys., 12:1183-1186, 1986.Tomashefsky, P., Astor, M., and White, R. D. Relationship between thioldepletion and Chemosensitization in transplantable murine bladder tumor. J.Nati. Cancer Inst., 74: 1233-1238, 1985.Ono, K., Komuro, C., Tsutsui, K., Shibamoto, Y., Nishidai, T., Takahashi,M., Abe, M., and Shrieve, D. C. Combined effect of buthionine sulfoximineand cyclophosphamide upon murine tumours and bone marrow. Br. J.Cancer, 54: 749-754, 1986.DeGraff, W. G., and Mitchell, J. B. Glutathione dependence of neocarzinos-tatin cytotoxicity and mutagenicity in Chinese hamster V-79 cells. CancerRes., 45: 4760-4762, 1985.Hodgkiss, R. J., and Middleton, R. W. Effects of glutathione depletion usingbuthionine sulfoximine on the cytotoxicity of nitroaromatic compounds inmammalian cells in vitro. Biochem. Pharmacol., 34: 2175-2178, 1985.Lee, F. Y. F., Vessey, A. R., and Siemann, D. W. Glutathione as a determinant of cellular response to doxorubicin. Nati. Cancer Inst. Monogr., 6:211-215, 1988.Dethlefsen, L. A., Biaglow, J. E., Peck, V. M., and Ridinger, D. N. Toxiceffects of extended glutathione depletion by buthionine sulfoximine on murine mammary carcinoma cells. Int. J. Radiât.Oncol. Biol. Phys., 12: 1157-1160, 1986.Dorr, R. T., Liddil, J. D., and Soble, M. J. Cytotoxic effects of glutathionesynthesis inhibition by L-buthionine-S./f-sulfoximine on human and murinetumor cells. Invest. New Drugs, 4: 305-313, 1986.Ono, K., and Shrieve, D. C. Effect of glutathione depletion by L-buthioninesulfoximine on the cytotoxicity of cyclophosphamide in single and fractionated doses to EMT6/SF mouse tumors and bone marrow. J. Nati. CancerInst., 79:811-815, 1987.Soble, M. J., and Dorr, R. T. Lack of enhanced antitumor efficacy for L-buthionine sulfoximine in combination with carmustine, cyclophosphamide,doxorubicin or melphalan in mice. Anticancer Res., S: 17-22, 1988.Soble, M. J., and Dorr, R. T. Lack of enhanced myelotoxicity with buthioninesulfoximine and sulfhydryl-dependent anti-cancer agents in mice. Res. Commun. Chem. Path. Pharmacol., 55: 161-180, 1987.Gilbaldi, M., and Perrier, D. Pharmacokinetics. In: J. Swarbrick (ed.), Drugsand the Pharmaceutical Sciences, pp. 45-111. New York: Marcel Dekker,Inc., 1982.Duff, R., and Murrill, E. Determination of L-buthionine-S,A-sulfoximine inplasma by high-performance liquid chromatography with o-phthalaldehydederivatization and fluorometric detection. J. Chromatogr., 385: 275-282,1987.Akerboom, T. P. M., and Sies, H. Assay of glutathione, glutathione disulfide
Research. on August 16, 2019. © 1989 American Association for Cancercancerres.aacrjournals.org Downloaded from

BSO PHARMACOKINETICS AND TOXICITY
and glutathione mixed disulfides in biological samples. Methods Enzymol.,77:372-382, 1981.
37. Smith, A. C., and Boyd, M. R. Preferential effects of 1,3-bis-(2-chloroethyl)-1-nitrosourea (BCNU) on pulmonary glutathione reducÃaseand glutathione/glutathione disulfide ratios: possible implication for lung toxicity. J. Phar-macol. Exp. Ther., 229: 658-663, 1984.
38. Sun, J. D., Ragsdale, S. S., Benson, J. M., and Henderson, R. F. Effects ofthe long-term depletion of reduced glutathione in mice administered L-buthionine-5,/?-sulfoximine. Fundam. Appi. Toxicol., 5: 913-919, 1985.
39. Page, J. G., Carlton, B. D., Smith, A. C., Kastello, M. D., and Grieshaber,C. K. Preclinical toxicology and pharmacokinetic studies of buthioninesulfoximine (BSO, NSC-326231) in CD2F1 mice. Proc. Am. Assoc. CancerRes., 28: 440, 1987.
40. Russo, A., Tochner, A., Phillips, T., Carmicheal, J., DeGraff, W., Friedman,N., Fisher, J., and Mitchell, J. B. In vivo modulation of glutathione bybuthionine sulfoximine: effect on marrow response to melphalan. Int. J.Radial. Oncol. Biol. Phys., 12: 1187-1189, 1986.
41. Kramer, R. A., Schuller, H. M., Smith, A. C, and Boyd, M. R. Effect of
buthionine sulfoximine on the nephrotoxicity of l-(2-chloroethyl)-3-(frans-4-methylcyclohexyl)-l-nitrosourea (MeCCNU). J. Pharmacol. Exp. Ther.,234: 498-506, 1985.
42. Mayer, R. I).. Lee, K.. and Crockett, A. T. K. Inhibition of cisplatin-inducednephrotoxicity in rats by buthionine sulfoximine, a glutathione synthesisinhibitor. Cancer Chemother. Pharmacol., 20: 207-210, 1987.
43. Litterst, C. L., Bertolero. F., and Uozumi, J. The role of glutathione andmetallothionein in the toxicity and subcellular binding of cisplatin. In: D. C.H. McBrien and T. F. Slater (eds.), Biochemical Mechanisms of PlatinumAntitumor Drugs, pp. 227-254. Oxford, England: IRL Press, Ltd., 1986.
44. Sarosy, G., Leyland-Jones, B., Soochan, P., and Cheson, B. D. The systematicadministration of intravenous melphalan. J. Clin. Oncol., 6: 1768-1782,1988.
45. Antman, K., Eder, J. P., Elias, A., Shea, T., Peters, W. P., Andersen, J.,Schryber, S., Henner, W. P., Findberg, R., Wilmore, D. et al. High-dosecombination alkylating agent preparative regimen with autologous bonemarrow support. The Dana-Farber Cancer Institute/Beth Israel Hospitalexperience. Cancer Treat. Rep., 71: 119-125, 1987.
5391
Research. on August 16, 2019. © 1989 American Association for Cancercancerres.aacrjournals.org Downloaded from

1989;49:5385-5391. Cancer Res Adaline C. Smith, James T. F. Liao, John G. Page, et al. Its Effect on Melphalan-induced Toxicity in MicePharmacokinetics of Buthionine Sulfoximine (NSC 326231) and
Updated version
http://cancerres.aacrjournals.org/content/49/19/5385
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/49/19/5385To request permission to re-use all or part of this article, use this link
Research. on August 16, 2019. © 1989 American Association for Cancercancerres.aacrjournals.org Downloaded from