Embed Size (px)
Citation preview
HAL Id: hal-00902408https://hal.archives-ouvertes.fr/hal-00902408
Submitted on 1 Jan 1996
HAL is a multi-disciplinary open accessarchive for the deposit and dissemination of sci-entific research documents, whether they are pub-lished or not. The documents may come fromteaching and research institutions in France orabroad, or from public or private research centers.
L’archive ouverte pluridisciplinaire HAL, estdestinée au dépôt et à la diffusion de documentsscientifiques de niveau recherche, publiés ou non,émanant des établissements d’enseignement et derecherche français ou étrangers, des laboratoirespublics ou privés.
Pharmacokinetics of penicillin G in plasma andinterstitial fluid collected with dialysis fiber bundles in
sheepIm Cooke, Rf Bevill, Dr Nelson, Gd Koritz
To cite this version:Im Cooke, Rf Bevill, Dr Nelson, Gd Koritz. Pharmacokinetics of penicillin G in plasma and interstitialfluid collected with dialysis fiber bundles in sheep. Veterinary Research, BioMed Central, 1996, 27(2), pp.147-160. <hal-00902408>
Original article
Pharmacokinetics of penicillin G in plasmaand interstitial fluid collected
with dialysis fiber bundles in sheep
IM Cooke RF Bevill DR Nelson GD Koritz 2
1 Department of Environmental Health and Safety;2 Department of Veterinary Biosciences;
3 Department of Veterinary Clinical Medicine, University of Illinois, Urbana, IL 61801, USA
(Received 19 July 1995; accepted 16 November 1995)
Summary - A new method of collection of interstitial fluid (ISF) (the site of most bacterial infections)was developed for the determination of free (unbound) penicillin G concentrations in sheep. Dialysisfiber bundles for the collection of ISF were first characterized in vitro and subsequently implanted in thesubcutaneous fascia of the dorsal thorax parallel to the vertebral column in sheep. The sheep were thendosed intravenously with 26.4 and 52.9 mg/kg of sodium penicillin G using a crossover experimentaldesign. Plasma and ISF dialysate were collected after dosing for determination of penicillin G con-centrations using high pressure liquid chromatography (HPLC) The concentration of penicillin G in theISF dialysate was calculated with the recovery ratio determined for each fiber bundle. The decline ofpenicillin G concentrations in ISF dialysate paralleled the disappearance of the drug from plasma pro-viding evidence for the rapid diffusion of penicillin G into the fiber bundles. Pharmacokinetic analysisdetermined that the disposition of penicillin G was best described by a two-compartment open modelwith penicillin concentrations in plasma (Cp) defined by two biexponential equations, Cp = 170.64e-! !sr+ 31.04e-i 5sr for the low dose and Cp = 418.1 9e-6.15t + 59.85e-1.56t for the high dose.
penicillin G / pharmacokinetics / interstitial fluid / sheep / dialysis fiber bundle
Résumé ― Pharmacocinétique de la pénicilline G prélevée à l’aide de faisceaux de fibres de dia-lyse dans le plasma et le liquide interstitiel chez le mouton. Une nouvelle méthode de déterminationde la concentration de pénicilline G libre (non-liée) dans le liquide interstitiel - site de la plupart des infec-tions bactériennes - a été développée. Des faisceaux de fibres de dialyse destinées aux prélève-ments du liquide interstitiel ont été initialement calibrés in vitro. Les fibres de dialyse ont ensuite étéimplantées chez le mouton dans le fascia sous-cutané du thorax dorsal parallèlement à la colonne ver-
* Correspondence and reprints

tébrale. Les moutons ont ensuite reçu par voie intraveineuse 26 et 52 mglkg de pénicilline G sodiqueen utilisant un plan expérimental croisé. Du plasma et des dialysats de liquide interstitiel ont été col-lectés et les concentrations de pénicilline G ont été déterminées par chromatographie liquide à hauteperformance. La concentration de pénicilline G dans les dialysats de liquide interstitiel a été calculéeen utilisant le rapport de récupération déterminé pour chaque faisceau de fibres. La diminution desconcentrations de pénicilline G dans le dialysat interstitiel était parallèle à celle du médicament dansle plasma, suggérant une diffusion rapide de la pénicilline G dans les fibres de dialyse. L’analysepharmacocinétique a conduit à décrire la disposition de la pénicilline G selon un modèle bicompartimentalouvert. Les concentrations de pénicilline dans le plasma ont été décrites par deux équations biexpo-nentielles, Cp = 170,64e-7, 161 + 31,04e-l,56t pour la dose inférieure et CP = 418,19e-s. 151 + 59,85e-1.56tpour la dose supérieure.
pénicilline Glpharmacocinétiquelliquide interstitiellmoutonlfaisceau de fibres de dialyse
INTRODUCTION
Pharmacokinetic investigations to optimizeantibacterial dosage regimens are oftenbased on plasma or serum drug concen-tration versus time profiles. However, suchstudies disregard the free (unbound) andtherefore active drug concentrationsachieved at the site of bacterial infectionwhich is of fundamental importance to theoptimization of antibiotic dosage regimens.This need to understand the distribution ofantibacterial agents in tissues was recog-nized shortly after the introduction of peni-cillin when antibiotic concentrations werefound to persist in infected wound exudates(Eagle et al, 1953).
Since most bacterial infections occur in
interstitial fluid (ISF), many techniques weredeveloped to sample the fluid for the deter-mination of antibiotic concentrations. The
implanted fibrin clot was one of the earliestapproaches (Weinstein et al, 1951 Skinwindows and skin blisters techniques werealso developed to sample tissue fluid (Rae-burn, 1971; Harding and Eilon, 1977; Gilletteand Wise, 1978; Schreiner et al, 1978; Wiseet al, 1980; Findlay et al, 1981 However,the prolonged penetration of drug into theblister fluid and the small fluid volumesobtained limited sampling frequency. Paperdiscs implanted subcutaneously (Bergeronet al, 1977) were limited by small sample
volume and the inability to obtain multiplesamples. Techniques were also developedin both humans (Engeset et al, 1973; Berganand Engeset, 1987) and other animals(Smith et al, 1970; Staub et al, 1975; Cohenet al, 1984) to obtain peripheral lymph sam-ples as a representative of ISF (Courtice,1971 ). A variety of tissue chambers for ISFcollection were subsequently developed(Guyton, 1963; Burke, 1964; Calnan et al,1972; Chisholm et al, 1973; Ryan, 1978;Bergan, 1981; Guyton, 1981; Beadle et al,1989), which varied considerably in size,shape and diameter (Gardner et al, 1973;Carbon et al, 1977; Bengtsson et al, 1984;Clarke, 1989). High chamber surface area tointernal volume ratios and long diffusionalpaths, however, resulted in unacceptablylong equilibration times between drug con-centrations in ISF and those in chamberfluid. Dialysis tubes that filter either ISF orserum through a semipermeable membranehave also been used for fluid collection
(Peterson and Gerding, 1978; Gerding etal, 1982). Although several units may beimplanted subcutaneously to facilitate mul-tiple sampling, this increases the variabilityin the data (Dan et al, 1981 Lastly, a micro-dialysis fiber system incorporating small hol-low dialysis fibers was introduced to over-come limitations of the larger dialysis tubes(Bunnett et al, 1983, 1984; Ruckebusch etal, 1985; Pairet et al, 1986; Ruckebuschand Malbert, 1987). Rapid equilibration was

achieved as a result of the short diffusional
distances and multiple samples could beobtained from the same fiber bundle.
The purpose of this study was to developa simple and reliable technique using dial-ysis fiber bundles to sample ISF without thelimitations of previous methods and to usethe technique to determine the disposition ofan antibacterial drug in ISF in vivo. Peni-cillin G and the sheep were chosen as themodel antibacterial drug and test species,respectively.
MATERIALS AND METHODS
Fiber construction
Spectra/Por« hollow fiber bundles (SpectrumMedical Industries Inc, Los Angeles, CA, USA)with a molecular weight cut off of 9 000 Da andworking volumes of 654 pL were used. This inter-nal volume plus a flush volume of 1 mL provideda final sample volume sufficient to permit analy-sis of penicillin G concentrations by high pres-sure liquid chromatography (HPLC). Each bundleconsisted of 176 fibers with an exposed lengthof 21 cm and an internal diameter of 150 pm. A6.25 cm piece of heat shrink tubing was appliedaround the injection end of the bundle cap. Astopcock was then fitted into the free end of thetubing. The tip of the stopcock was inserted asclose to the fiber ends within the tubing as pos-sible to minimize dead space. A 3.75 cm pieceof heat shrink tubing was also applied to the oppo-site collection end of the bundle and plugged witha removable stylet. Two surgical clips were gen-tly applied at one third and two thirds of the lengthof the fiber bundle to spread the fibers. The con-trolled force applied to the clips did not result inocclusion of the fibers.
Fiber characterization
The permeability of the fibers to penicillin G wasfirst characterized in vitro. The equilibration timeand percent recovery for penicillin G concentra-tions within the fibers in relation to those con-centrations in fluid bathing the fibers were deter-
mined for six fiber bundles. The equilibration timewas defined as the middle collection interval ofthe consecutive collection intervals for which therewas no significant difference in sequential ratiosof penicillin G concentrations in fiber dialysateand bath fluid. The percent recovery was calcu-lated as the ratio of penicillin G concentrationsin fiber dialysate and bath fluid when equilibriumwas attained. The experiment was designed as athree-way factorial design. The order in whicheach fiber bundle, collection interval and con-centration was used was completely randomized.
The dialysis fibers were filled with isotonicsaline and immersed in a beaker containing abath of isotonic saline with 0.2% bovine serumalbumin (Sigma, Saint Louis, MO, USA) to simu-late the drug binding phenomena occurring inISF (Bunnett et al, 1983) and fortified with 5, 25 or50 pg/mL of penicillin G. The solution was con-tinuously stirred with a magnetic stirrer (CorningHot Plate Stirrer PC-351, Corning Lab Products,Corning, NY, USA) to ensure an even distribu-tion of penicillin G. The 9 000 Da molecular exclu-sion limit of the fibers excluded protein-bounddrug from the dialysate. Samples of dialysatewere collected at intervals of 0, 1, 2, 5 and 10 0min by flushing the fiber bundle with saline toobtain 1 mL of saline and dialysate in the collec-tion syringe. The sampling procedure was com-pleted within 15 s. Subsequently, the fiber bundlewas flushed with 5 mL of saline, the stopcockwas closed, and the stylet plugs replaced at theinjection and collection ends of the fiber bundle.The dialysate and beaker fluid were then ana-lyzed for penicillin G by HPLC. The concentra-tion of penicillin G in the dialysate was dividedby the concentration of penicillin G in the beakerfluid to obtain ratios of penicillin G inside and out-side the fibers at the different collection times.
Pharmacokinetic study
Six male Suffolk-cross sheep (44-64 kg) weredetermined to be healthy by clinical examinationprior to the start of the experiment. The animalswere acclimated to their surroundings for a week,and then each was surgically implanted with adialysis fiber bundle which had been sterilizedwith ethylene oxide. The animals were not pro-vided food or water during the 24 h interval priorto surgery. Anesthesia was induced with a1.1 mL/kg iv bolus injection of 500 mg ketamine(Ketaset, Fort Dodge Laboratories Inc, Fort

Dodge, IA, USA) and 50 mg xylazine (Rompun,Mobay Corporation, Shawnee, KS, USA) in500 mL of 5% glycerol guaiacolate (Gecolate,Summit Hill Laboratories, Navesink, NJ, USA).Endotracheal tubes were placed in the sheepand anesthesia was maintained with halothane
during the surgical procedure. The skin over thedorsal thorax was clipped and scrubbed in prepa-ration for surgery. Two small skin incisions weremade 22 cm apart in the dorsal thorax parallel tothe vertebral column on the left side. A hollowstainless steel trocar equipped with a cutting edgewas tunneled through the subcutaneous fasciabetween the incisions. The fiber bundle wasinserted in the trocar which was then gently pulledout leaving the fiber bundles in position subcu-taneously. The ends of the fiber bundles weresutured to the skin and flushed daily with saline.
Sixteen hours prior to dosing, food was with-held and a 16 g, 8.3 cm catheter (Angiocath,Deseret Medical Inc, Sandy, UT, USA) with aninternal volume of 0.2 mL was implanted in thejugular vein for both dosing and blood collection.The sheep were dosed with sodium penicillin G(Sigma, Saint Louis, MO, USA) 48 h aftersurgery. Three sheep were dosed with the lowdose of penicillin G (26.4 mg/kg or 44 000 IU/kg)followed by the high dose (52.9 mg/kg or 88 000IU/kg), 2 days after the first. The other threesheep received the high dose of penicillin G fol-lowed by the low dose. The order in which eachsheep was dosed with the low or high dose wasrandomized. The dose was injected during a 30 sinterval via the jugular catheter followed by a10 mL flush with saline which had been shown to
prevent carryover of penicillin to subsequentblood samples. Blood and ISF dialysate sam-ples were collected before dosing (control) and at10, 20, 30, 45 min and 1, 1.5, 2, 3, 4 and 5 h
post-dosing. Blood samples (5 mL) were col-lected in 1% heparin after withdrawing and dis-carding 2 mL of blood from the catheter. Saline(5 mL) was injected to replace the blood volumefollowed by 1.5 mL of heparinized saline to main-tain catheter patency between collections. Bloodsamples were centrifuged and plasma collected.ISF dialysate was collected by flushing the fiberbundle with saline to obtain 1 mL of the ISF
dialysate within 15 s. The fiber bundle was thenflushed with 5 mL saline and refilled. All sam-
ples were analyzed for penicillin G concentra-tions by HPLC.
The fiber bundle was removed from the sheepat the end of the experiment, 7 days after implan-tation. To remove the bundle, the sheep were
tranquilized with xylazine (0.11 mg/kg) intra-venously. The fiber bundles were cut off at oneend and easily withdrawn. The open wound wasthen sutured.
Penicillin G analysis
A HPLC assay developed by Tyckowska andAronson (1988) was modified to improve thedetection and quantitation of penicillin G. A HPLCsystem from Waters Associates (Milford, MA,USA), consisting of a pump (Model 6000 A), anautomated injector (Model 712) and a variablewavelength detector (Model 484), was used forthe isocratic separation, detection and quantitationof penicillin G in all samples. A Brownlee Spheri-5 phenyl column (250 x 4.6 mm) equipped with aphenyl Newguard column (Brownlee Laborato-ries Inc, Santa Clara, CA, USA) was used to sep-arate penicillin G from plasma components. Thecolumn was heated and maintained at 50 °C witha water jacket (All Tech Associates, ArlingtonHeights, IL, USA) and a Haake constant tem-perature water bath equipped with an externalcirculation pump (Cole Parmer Instrument Com-pany, Chicago, IL, USA). A Hewlett Packard(Rolling Meadows, IL, USA) recording integrator(Model 3396 A) and disc drive (Model 9114 B)were used to record and store the chromatogramsand print reports of each analysis.
The standard, penicillin G sodium salt, wasfrom Sigma (Saint Louis, MO, USA). Acetonitrileand orthophosphoric acid (85%) were from FisherScientific (Fairlawn, NJ, USA); triethylamine andoctanesulfonate were from Regis Chemical Com-pany (Morton Grove, IL, USA); methanol wasfrom American Burdick and Jackson (Muskegon,MI, USA). All solvents were HPLC grade. Thereagents were analytical grade. Deionized glass-distilled water was used for all preparations. Themobile phase was prepared by dilution of 300 mLacetonitrile with 680 mL water, 5 mL triethylamine,5 mL phosphoric acid and 10 mL of a 0.5 Moctanesulfonate solution. The eluant used forextraction and concentration of the sample wasprepared by dilution of 90 mL acetonitrile with10 mL of modified mobile phase prepared asdescribed above but without acetonitrile.
Plasma and ISF dialysate samples wereextracted and concentrated with prepacked resincolumns (Bond-Elut, Analytichem International,Harbor City, CA, USA). The columns were pre-

conditioned with two 1 mL methanol washes fol-lowed by two 1 mL phosphate buffer washes. Avacuum (17.5 cm of mercury) was used toincrease the flow of solvents and reduce elutiontime. The sample (1 mL) was added to the con-ditioned column followed by two 1 mL buffer
washes. A vacuum was applied to the columnoutlet to remove free liquid from the resin. Peni-cillin G was extracted from the resin with 200 p Lof the eluant. Centrifugation (2.5 min at 140 y)was used to increase movement of the fluids
through the column. The extraction was repeatedwith 100 »L of eluant to obtain a 3.33-fold con-centration of penicillin G in the sample. The com-bined eluates were then transferred to an injectionvial equipped with a 0.3 mL limited volume insert(Crom Tech, Inc, Apple Valley, MN, USA). Com-plete recovery (100%) of penicillin G was obtainedwith this method.
The processed sample (25 yL) was placedin the automated injector and introduced into themobile phase being delivered to the reversephase HPLC column. The mobile phase flowwas 1.2 mL/min. The ultraviolet absorption ofthe mobile phase as it emerged from the columnwas monitored at 210 nm. Changes in absorptionwere integrated, recorded and stored on the discdrive.
Standards containing 1, 2, 4, 8 and 16 6 jrg/mLof drug in sheep plasma were analyzed for peni-cillin G concentrations, and standard curves cor-
relating penicillin G concentrations to peak integralareas under UV absorption response curves wereestablished. This correlation was defined by aregression equation which was subsequentlyused to calculate penicillin G concentrations inan unknown sample. Samples with penicillin Gconcentrations greater than 16 6 j<g/mL were dilutedwith eluant after extraction to achieve a concen-
tration within the range of the standard curve.The standard curves were linear within the rangeof 0.5 to 16 6 j<g/mL and passed through the origin.The coefficients of correlation obtained when theareas of the eluted peaks were compared to thepenicillin G concentrations were always greaterthan 0.995. The level of quantitation of the assaywas found to be 0.5 ,llg/mL. The limit of detec-tion of the assay was 1 ¡lg/mL. Absence of otherinterfering peaks confirmed the specificity of theassay. Reliability of the assay was determinedto be 0.9906. Reproducibility of the assay wasalso excellent as indicated by coefficient of vari-ation values which were all less than 10°° for
duplicate samples.
Data analysis
Fiber characterization
A multiple regression analysis (with dummy cod-ing used for fiber identity) was used to determineif there were any significant differences in theratios obtained between the collection intervals,fibers and penicillin G concentrations. If a signif-icant difference was found, the least significantdifference between collection intervals was deter-mined (Snedecor and Cochran, 1980). P 5 0.05
was required for statistical significance.
Pharmacokinetic study
The Autoan computer program (Sedman and Wag-ner, 1976) was used to determine which expo-nential equation best fit the plasma and ISFdialysate data and to obtain initial estimates of thepharmacokinetic parameters. An F-test in the com-puter program determined which exponential equa-tion best fitted each animal’s data. The SAAM27
curve-fitting computer program based on nonlineariterative least-squares regression analysis (Bermanand Weiss. 1977) was subsequently used to obtainfinal values of the rate constants and volumes
using the initial estimates obtained with the Autoanprogram. Drug concentrations were weighted bythe reciprocal of each observation for the Autoanand SAAM27 fitting procedures. Pharmacokineticparameters (A, B, u, (i, t1/2u, t1!21), VDarea’ Vc, Vss,CL and AUC) were calculated using standard for-mulas (Gibaldi and Perrier, 1982). These phar-macokinetic parameters are defined according toBaggot (1977) (see table II below). Free drug con-centrations in plasma were calculated after cor-rection of the plasma penicillin G concentrations for30% protein binding (Ziv and Sulman, 1972). Apaired t-test was used to determine whether therewere any significant differences in the CL. Vp!,ea!Vss and after the administration of the low and
high dose of penicillin G. P <_ 0.05 was requiredfor statistical significance.
RESULTS
Fiber characterization
The ratios of the concentrations of penicillinG in the dialysate to the beaker bath solution
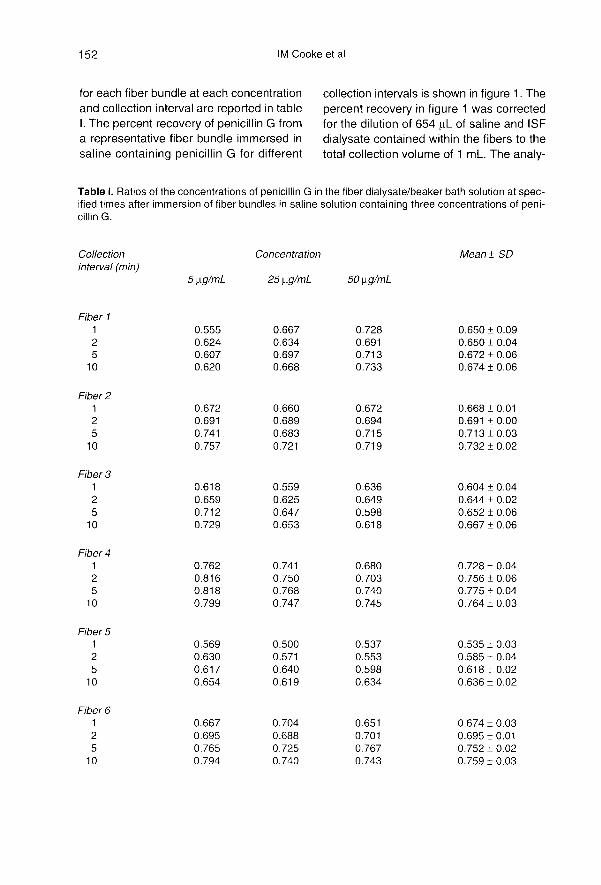
for each fiber bundle at each concentration
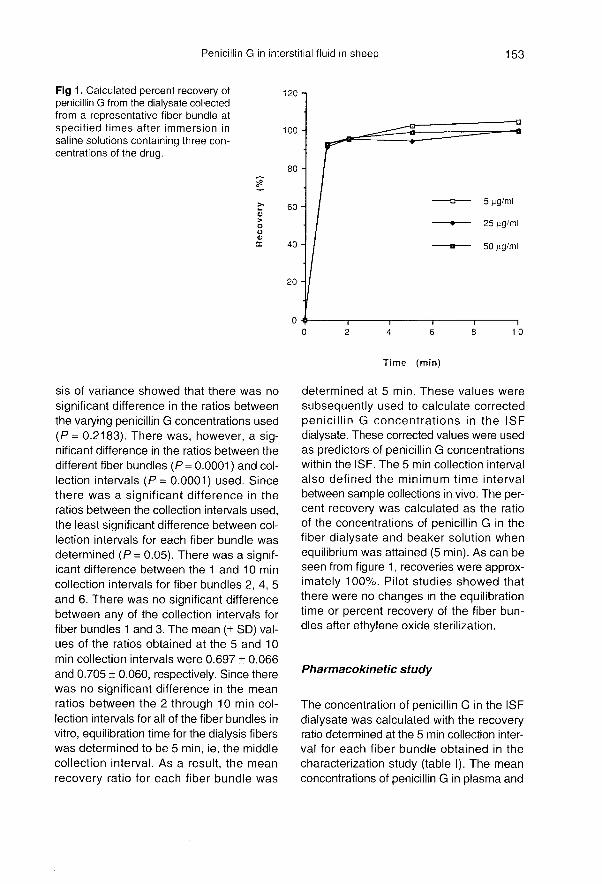
and collection interval are reported in tableI. The percent recovery of penicillin G froma representative fiber bundle immersed insaline containing penicillin G for different
collection intervals is shown in figure 1. Thepercent recovery in figure 1 was corrected
for the dilution of 654 pL of saline and ISFdialysate contained within the fibers to thetotal collection volume of 1 mL. The analy-
sis of variance showed that there was no
significant difference in the ratios betweenthe varying penicillin G concentrations used(P = 0.2183). There was, however, a sig-nificant difference in the ratios between thedifferent fiber bundles (P= 0.0001 ) and col-lection intervals (P= 0.0001) used. Sincethere was a significant difference in theratios between the collection intervals used,the least significant difference between col-lection intervals for each fiber bundle wasdetermined (P = 0.05). There was a signif-icant difference between the 1 and 10 min
collection intervals for fiber bundles 2, 4, 5and 6. There was no significant differencebetween any of the collection intervals forfiber bundles 1 and 3. The mean (± SD) val-ues of the ratios obtained at the 5 and 10 0min collection intervals were 0.697 ± 0.066and 0.705 ± 0.060, respectively. Since therewas no significant difference in the meanratios between the 2 through 10 min col-lection intervals for all of the fiber bundles in
vitro, equilibration time for the dialysis fiberswas determined to be 5 min, ie, the middlecollection interval. As a result, the meanrecovery ratio for each fiber bundle was
determined at 5 min. These values were
subsequently used to calculate correctedpenicillin G concentrations in the ISF
dialysate. These corrected values were usedas predictors of penicillin G concentrationswithin the ISF. The 5 min collection intervalalso defined the minimum time intervalbetween sample collections in vivo. The per-cent recovery was calculated as the ratioof the concentrations of penicillin G in thefiber dialysate and beaker solution whenequilibrium was attained (5 min). As can beseen from figure 1, recoveries were approx-imately 100%. Pilot studies showed thatthere were no changes in the equilibrationtime or percent recovery of the fiber bun-dles after ethylene oxide sterilization.
Pharmacokinetic study
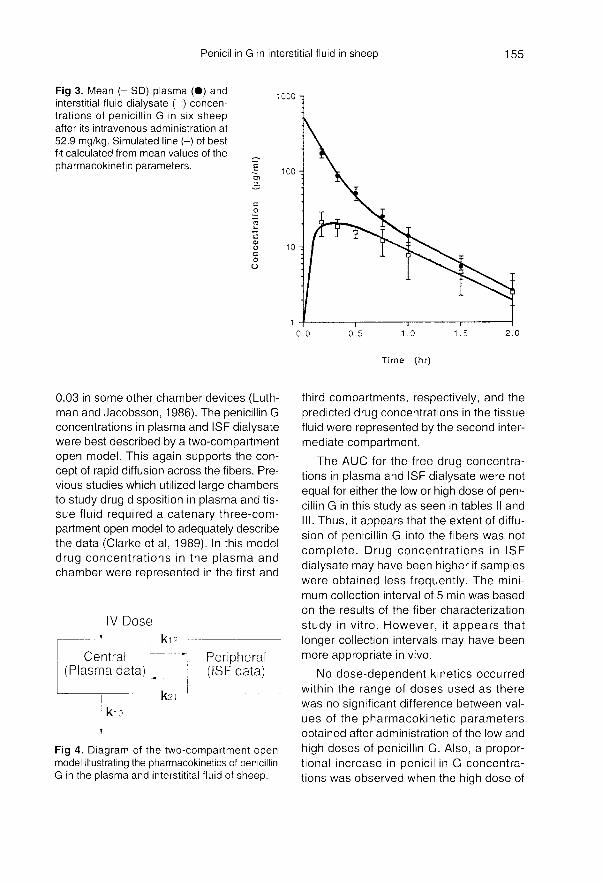
The concentration of penicillin G in the ISFdialysate was calculated with the recoveryratio determined at the 5 min collection inter-val for each fiber bundle obtained in thecharacterization study (table I). The meanconcentrations of penicillin G in plasma and
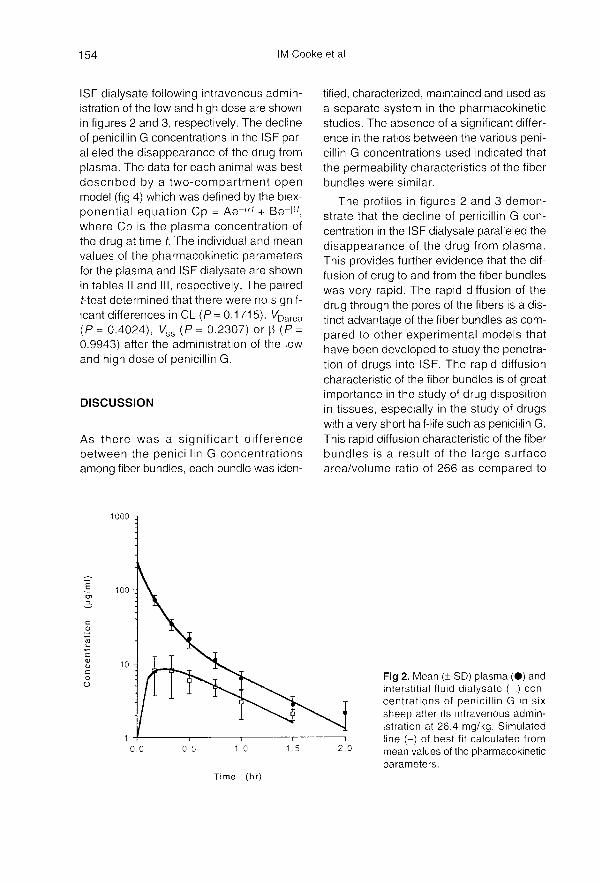
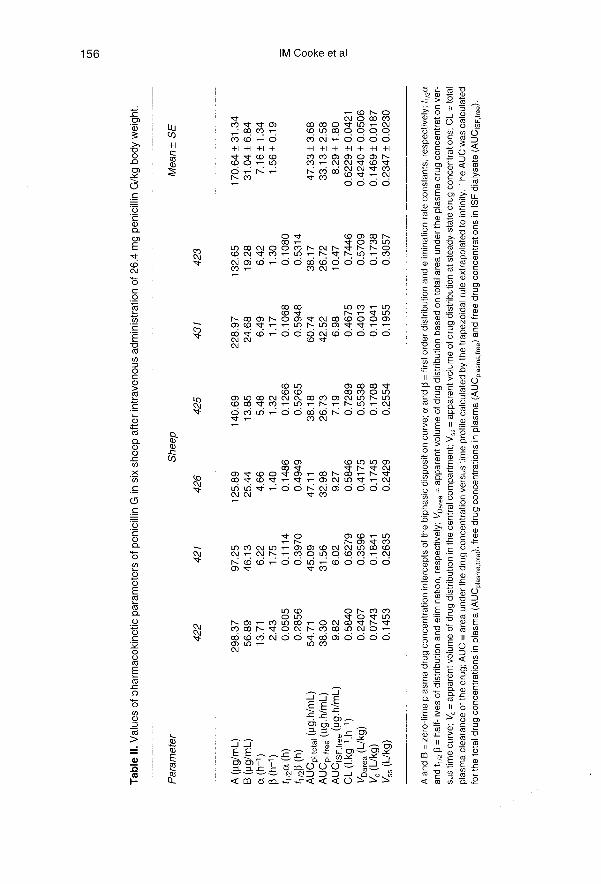
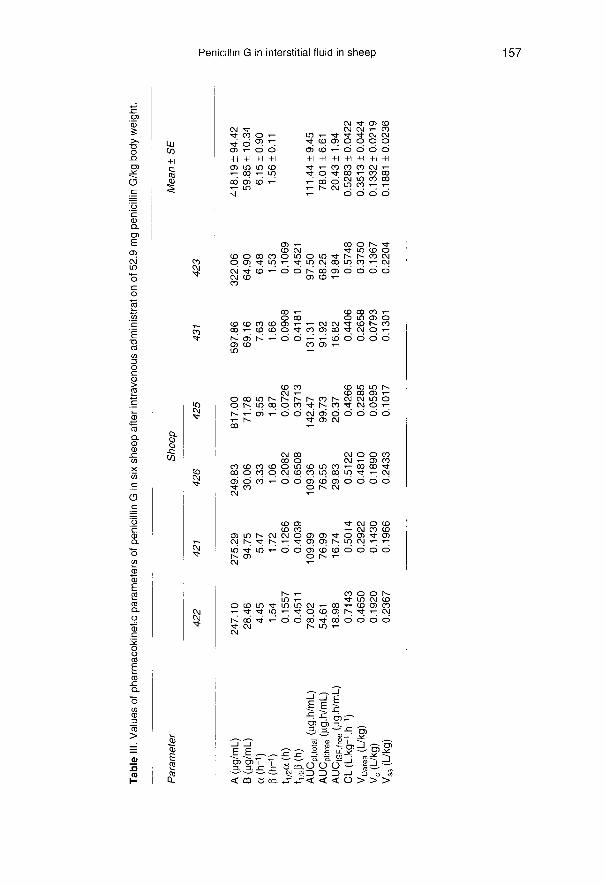
ISF dialysate following intravenous admin-istration of the low and high dose are shownin figures 2 and 3, respectively. The declineof penicillin G concentrations in the ISF par-alleled the disappearance of the drug fromplasma. The data for each animal was bestdescribed by a two-compartment openmodel (fig 4) which was defined by the biex-ponential equation Cp = Ae-«r + Be-I1t,where Cp is the plasma concentration ofthe drug at time t. The individual and mean
values of the pharmacokinetic parametersfor the plasma and ISF dialysate are shownin tables II and III, respectively. The pairedt-test determined that there were no signif-icant differences in CL (P= 0.1715), VDarea(P = 0.4024), VSS (P = 0.2307) or !3 (P =
0.9943) after the administration of the lowand high dose of penicillin G.
DISCUSSION
As there was a significant differencebetween the penicillin G concentrationsamong fiber bundles, each bundle was iden-
tified, characterized, maintained and used asa separate system in the pharmacokineticstudies. The absence of a significant differ-ence in the ratios between the various peni-cillin G concentrations used indicated that
the permeability characteristics of the fiberbundles were similar.
The profiles in figures 2 and 3 demon-strate that the decline of penicillin G con-centration in the ISF dialysate paralleled thedisappearance of the drug from plasma.This provides further evidence that the dif-fusion of drug to and from the fiber bundleswas very rapid. The rapid diffusion of thedrug through the pores of the fibers is a dis-tinct advantage of the fiber bundles as com-pared to other experimental models thathave been developed to study the penetra-tion of drugs into ISF. The rapid diffusioncharacteristic of the fiber bundles is of greatimportance in the study of drug dispositionin tissues, especially in the study of drugswith a very short half-life such as penicillin G.This rapid diffusion characteristic of the fiberbundles is a result of the large surfacearea/volume ratio of 266 as compared to
0.03 in some other chamber devices (Luth-man and Jacobsson, 1986). The penicillin Gconcentrations in plasma and ISF dialysatewere best described by a two-compartmentopen model. This again supports the con-cept of rapid diffusion across the fibers. Pre-vious studies which utilized large chambersto study drug disposition in plasma and tis-sue fluid required a catenary three-com-partment open model to adequately describethe data (Clarke et al, 1989). In this modeldrug concentrations in the plasma andchamber were represented in the first and
third compartments, respectively, and thepredicted drug concentrations in the tissuefluid were represented by the second inter-mediate compartment.
The AUC for the free drug concentra-tions in plasma and ISF dialysate were notequal for either the low or high dose of peni-cillin G in this study as seen in tables II and
I 1 Thus, it appears that the extent of diffu-
sion of penicillin G into the fibers was notcomplete. Drug concentrations in ISF
dialysate may have been higher if sampleswere obtained less frequently. The mini-mum collection interval of 5 min was based
on the results of the fiber characterization
study in vitro. However, it appears that
longer collection intervals may have beenmore appropriate in vivo.
No dose-dependent kinetics occurredwithin the range of doses used as therewas no significant difference between val-ues of the pharmacokinetic parametersobtained after administration of the low and
high doses of penicillin G. Also, a propor-tional increase in penicillin G concentra-tions was observed when the high dose of
penicillin G was administered. Drug con-centrations increased twofold in plasmaand ISF dialysate when the dose was dou-bled.
Implanted dialysis fibers provided a sim-ple, convenient and reliable technique todetermine free antibiotic concentrations in
ISF dialysate. The main advantages of thistechnique were the ease of use, rapid dif-fusion characteristic and the ability to obtainmultiple samples. In addition, the dialysisfiber bundles can be easily adapted for avariety of potential applications. The fiberbundles may be implanted at different sites,organs or tissues. For example, they mightbe implanted in the peritoneal cavity fordetermination of drug concentrations dur-ing peritonitis. They might also be implantedin various muscles, organs or fat to detecttissue residue concentrations of drugs. Thiswould obviate the animal sacrifices typical ofconventional drug residue studies. Alterna-tively, the fibers could be used to create alocalized site of infection in the body. Bac-teria inoculated within implanted fibers wouldremain trapped due to the small size of thefiber pores and could serve as a model to
study the antibacterial action of an antibi-otic dosage regimen. The limitations in theuse of the fiber bundle may be related more
to assay requirements than any intrinsic lim-itation of the fiber bundle.
REFERENCES
Baggot JD (1977) Principles of Drug Disposition inDomestic Animals: the Basis of Veterinary ClinicalPharmacology. WB Saunders Company, Philadel-phia. PA, USA
Beadle RE, Short CR, Corstvet RE et al (1989) Char-acterization of a soft-tissue infection model in the
horse and its response to intravenous cephapirinadministration. J Vet Pharmacol Therap 12, 73-86
Bengtsson B, Luthman J, Jacobsson SO (1984) Evalu-ation of a tissue cage model for use in cattle. Acta Vet
Scand 25. 480-494
Bergan T (1981) Pharmacokinetics of tissue penetra-tion of antibiotics? Rev Infect Dis 3 (suppl 1 ), 45-66
Bergan T, Engeset A (1987) Does serum protein bindinginhibit tissue penetration of antibiotics. Rev InfectDis 9 (suppl 4), 713-718 8
Bergeron M, Nguyen BM, Trottier S, Gauvreau L (1977)Penetration of cefamandole, cephalothin, and
desacetyl-cephalothin into fibrin clots. AntimicrobAgents Chemother 12, 682-687
Berman M, Weiss MF (1977) Users’ manual for SAAM.Laboratory of Theoretical Biology, National CancerInstitute, National Institutes of Health, Bethesda,MD, USA
Bunnett NW, Walsh JH. Debas HT, Kauffman GL,Golanska EM (1983) Measurement of prostaglandinE2 in interstitial fluid from the dog stomach afterfeeding and indomethacin. Gastroenterology 85,1391-1398
Bunnett NW, Mogard M, Orloff MS, Corbet HJ, ReeveJR, Walsh JH (1984) Catabolism of neurotensin ininterstitial fluid of the rat stomach. Am J Physiol26,675-682
Burke JF (1964) An implanted reservoir for continuoussampling of interstitial fluid. J Surg Res 4, 195-199
Calnan J, Ford PM, Holt PJL, Pflugg JJ (1972) Implantedtissue cages―a study in rabbits. Br J Plast Surg 25,164-174
Carbon C, Contrepois A, Brian N, Lamotte-Barrillon S(1977) Penetration of cefazolin, cephaloridine andcefamandole into interstitial fluid in rabbits. Antimicrob
Agents Chemother 1 1, 594-598
Chisholm GD, Waterworth PM, Calnan JS, Garrod LP
(1973) Concentration of antibacterial agents in inter-stitial fluid. Am Med J 1, 569-573
Clarke CR (1989) Tissue-chamber modeling systems―applications in veterinary medicine. J Vet PharmacolTher 12. 349-368
Clarke CR, Short CR, Bourne DWA, Usenik EA (1989)Subcutaneously implanted tissue chambers―a phar-macokinetic study. J Vet Pharmacol Ther 12, 312-389
Cohen SH, Hoeprich PD. Demling R, Gunther R et al(1984) Entry of four cephalosporins into the ovinelung. J Infect Dis 149 (suppl 2), 264-270
Courtice FC (1971) Lymph and plasma proteins: barriersto their movement throughout the extracellular fluid.Lymphology 4, 9-17 7
Dan M, Halkin H, Rubinstein E (1981) Interstitial fluid
concentrations of aminoglycosides. J AntimicrobChemother7, 551-558
Eagle H, Fleischman R, Levy M (1953) ’Continuous’ vsdiscontinuous’ therapy with penicillin: the effect of theinterval between injections on therapeutic efficacy. N
Engl J Med 248, 481-488
Engeset A, Hager B, Nesheim A, Kolbenstvedt A (1973)Studies on human peripheral lymph. Lymphology6,1-5
Findlay CD, Wise R. Allcock JE, Durham SR (1981) Thetissue penetration as measured by a blister tech-nique and pharmacokinetics of cefulodin comparedwith carbenicillin and ticarcillin J Antimicrob
Chemother7, 637-642
Gardner WG, Prior RB, Perkins RL (1973) Fluid andpharmacological dynamics in a subcutaneous cham-ber implanted in rats. Antimicrob Agents Chemother4, 196-197
Gerding DN, Van Ette LL. Peterson LR (1982) Role ofserum protein binding and multiple antibiotic doses inthe extravascular distribution of ceftizoxime and cefo-
taxime. Antimicrob Agents Chemother 22, 844-847
Gibaldi M, Perrier D (1982) Pharmacokinetics. In:
Drugs and the Pharmaceutical Sciences. Vol 15 5
(J Swarbrick, ed), Marcel Dekker Inc. New York,NY, USA
Gillette AP. Wise R (1978) Penetration of four
cephalosporins into tissue fluid in man. Lancet I.962-964
Guyton C (1963) A concept of negative interstitial pres-sure based on pressures in implanted perforatedcapsules. Circ Res 12, 399-414 4
Guyton C (1981) Capillary dynamics and exchange offluid between the blood and interstitial fluid. In
Textbook of Medical Physiology, 6th ed (C Guy-ton, ed), WB Saunders Co, Philadelphia. PA, USA,358-369
Harding SM, Eilon LA (1977) Clinical pharmacology ofcefuroxime. In: The Early Evaluation of Cefuroxime(ES Snell et al, ed), Glaxo Research Ltd, Granford,UK, 57-68
Luthman J, Jacobsson SO (1986) Distribution of penicillinG in serum and tissue cage fluid in cattle. Acta Vet
Scand 27, 313-325
Pairet M, Meirieu 0, Bardon T, Ruckebusch Y (1986)Cholinergic modulation of the release of serotoninin the gastric interstitial fluid. Gastroenterology 911250-1257
Peterson LR, Gerding DN (1978) Prediction of cefa-zolin into high and low protein containing extravas-cular fluid: new method for performing simultane-ous studies. Antimicrob Agents Chemother 14,533-538
Raeburn JA (1971) A method for studying antibiotic con-centrations in inflammatory exudates. J Clin Pathol24, 633-635
Ruckebusch M, Malbert CH (1987) Availability of 5-HTPin duodenal interstitial fluid of sheep and dogs. J VetPharmacol Ther 10. 254-256
Ruckebusch Y, Meineu O, Von Ritter C, Blum AL (1985)Measurement of monoamines and their metabolites
in the interstitial fluid of the gut. J Pharmacol Meth-ods 13, 167-177
Ryan DM (1978) Implanted tissue cages: a critical eval-uation of their relevance in measuring tissue con-centrations of antibiotics. Scan J Infect Dis [Suppl] 14.225-227
Schreiner A, Hellum KB, Digranes A, Bergman I (1978)Transfer of penicillin G and ampicillin into humanskin blisters induced by suction. Scand J Infect Dis[Suppl] 14, 233-237
Sedman AJ, Wagner JG (1976) Autoan, a decision-mak-ing pharmacokinetic computer program. PublicationDistribution Service. Ann Arbor, MI, USA
Snedecor GW, Cochran WG (1980) Statistical Meth-ods. Iowa State University Press, Ames, IA, USA,233-234
Smith JB, Mcintosh GH. Morris B (1970) The traffic ofcells through tissues: a study of peripheral lymph insheep. J Anat 107 (suppl 1 ), 87-100
Staub NC, Bland RD, Brigham KL. Demling R, Erd-mann J, Woolverton WC (1975) Preparation ofchronic lymph fistulas in sheep. J Surg Res 19, 315-320
Tyckowska K, Aronson AL (1988) lon-pair liquid chro-matographic determination of some penicillins incanine and equine sera. JAssoc OffAnal Chem71(suppl 4), 773-775
Weinstein L. Daikos GK, Perrin TS (1951) Studies onthe relationship of tissue fluid and blood levels ofpenicillin. J Lab Clin Med 38; 712-718
Wise R, Gillette AP, Cadge B, Durham SR, Baker S (1980)The influence of protein binding upon tissue levels ofsix [3-lactam antibiotics. J Infect Dis 142, 77-82
Ziv G, Sulman FG (1972) Binding of antibiotics to bovineand ovine serum. Antimicrob Agents Chemother 2,206-213 3





























