Embed Size (px)
DESCRIPTION
farmakologi GIT
Citation preview

Pharmacological Pharmacological aspect of upper aspect of upper gastrointestinal gastrointestinal
diseases diseases
Nico L Lumbuun, dr., SpFKNico L Lumbuun, dr., SpFK
Faculty of MedicineFaculty of Medicine
UPHUPH

CaseCase
A 22 yo medical student, noted A 22 yo medical student, noted a burning pain a burning pain in his in his upper abdomen upper abdomen since 2 weeks ago. This sensation since 2 weeks ago. This sensation occurs 1 to occurs 1 to 2 hrs after eating2 hrs after eating. He is actually in a good . He is actually in a good health before, although he health before, although he smokessmokes approximately 2 approximately 2 packs of cigs & drink 5 cups of packs of cigs & drink 5 cups of coffee a daycoffee a day. He is . He is currently currently under stress under stress because of his bachelor exam. because of his bachelor exam. He also been taking 1-2 tabs He also been taking 1-2 tabs aspirin daily aspirin daily for the past for the past 2 months because of headache.2 months because of headache.
The pain frequently awakens him at midnight. His The pain frequently awakens him at midnight. His pain usually relieved by eating and by taking antacid.pain usually relieved by eating and by taking antacid.
What is the most likely problem?What is the most likely problem?
What is the most appropriate treatment?What is the most appropriate treatment?

Meaning of numbers1. Body of stomach 2. Fundus 3. Anterior wall 4. Greater curvature 5. Lesser curvature 6. Cardia 9. Pyloric sphincter 10. Pyloric antrum 11. Pyloric canal 12. Angular notch 13. Gastric Canal 14. Rugal folds
Anatomy



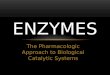
ProglumideACh
PGE2
Histamine Gastrin
Adenyl cyclase
_+
ATP cAMP
Protein Kinase (Activated)
Ca++
+
Ca++
Proton pump
KK+ H+
Gastric acid
Parietal cell
Lumen of stomach
AntacidOmeprazole
Ranitidine
H2M3
Misoprostol
_
__
_
+
PGE receptor
+
+
Gastrin receptor+
+
+

Antacids
Weak bases that react with gastric hydrochloric acid to form a salt and water.
Principal mechanism of action is :
reduction of intragastric acidity.
Acid-neutralization capacity among different proprietary formulations highly variable, depend on:
rate of dissolution (tablet versus liquid)
water solubility
rate of reaction with acid
rate of gastric emptying.

► Sodium bicarbonate (NaHCO3) reacts rapidly with HCl. NaHCO3 + HCl CO2 + NaCl + H2O pH gastric .
► Formation of CO2 results in gastric distention & belching. ► NaCl absorption may exacerbate fluid retention in patients with
heart failure, hypertension, and renal insufficiency. ► Unreacted alkali (NaHCO3) is readily absorbed potentially causing metabolic alkalosis when given in high
doses or to patients with renal insufficiency.
► Calcium carbonate (CaCOOH) less soluble, reacts slowly.
CaCOOH + HCL CO2 + CaCl2 + H2O► Also may cause belching or metabolic alkalosis. ► Other indications : bone mineralization.► Excessive doses + calcium-containing dairy products can lead
to hypercalcemia, renal insufficiency, and metabolic alkalosis (milk-alkali syndrome)
Antacids – cont…

► Present day antacids : Aluminium Hydroxide Magnesium Hydroxide
React slowly with HCl magnesium chloride or aluminum chloride and water.
No gas is generated, belching does not occur.Metabolic alkalosis is also uncommon
because of the efficiency of the neutralization reaction.
OTC drug for symptomatic rapid relief of dyspepsia
Antacids – cont…

Antacids – cont…
Duration of action : 30 min when taken in empty stomach 2 hrs when taken after a meal
Side effects :
Al3+ antacids – constipation (As they relax gastric smooth muscle & delay gastric emptying)
Mg2+ antacids – Osmotic diarrhoea . Both magnesium and aluminum are absorbed and
excreted by the kidneys. Hence, patients with renal insufficiency should not take these agents long-term.
In renal failure Al3+ antacid – Aluminium toxicity &
Encephalopathy

Antacids – Common additives
Simethicone – Decrease surface tension, reduce bubble formation Added to prevent reflux .Alginates is a viscous gum that is abundant in the cell walls of
brown algae. – Form a layer of foam/gel on
top of gastric contents &
reduce reflux
Oxethazaine – Surface anaesthetic (Strocain®)

Antacid - Interactions
Adsorb drugs (binding the drug) and form insoluble complexes that are not absorbed (ex.tetracycline, quinolone)
Increasing intragastric pH so that the drug's dissolution or solubility (especially weakly basic or acidic drugs) is altered.(ketocanazole, iron)
Clinical importance :
Interactions can be avoided by taking antacids 2 hrs before or after ingestion of other drugs .

Is it rational to combine aluminium hydroxide and magnesium hydroxide in antacid preparations ?

Combination provides a relatively fast and sustained neutralising capacity .
(Magnesium Hydroxide – Rapidly acting
Aluminium Hydroxide - Slowly acting )
Combination preserves normal bowel function.
(Aluminium Hydroxide – constipation
Magnesium hydroxide – diarrhoea )

Histamine H2 Receptor Antagonist
Reversible competitive inhibitors of H2 receptor
Highly selective, No action on H1 or H3 receptors
Very effective in inhibiting nocturnal acid secretion ( as it depends largely on Histamine )
Modest impact on meal stimulated acid secretion (As it depends on gastrin, acetyl choline and histamine)

Cimetidine Ranitidine Famotidine Nizatidine
Bioavailability 80 50 40 >90
Relative Potency 1 5 -10 32 5 -10
Half life (hrs) 1.5 - 2.3 1.6 - 2.4 2.5 - 4 1.1 -1.6
Duration of 6 8 12 8
action (hrs)
Inhibition of 1 0.1 0 0 CYP 450
Dose mg(bd) 400 150 20 150

H2 Blockers–Side effects & Interactions
Extremely safe drugs
Cimetidine causes gynecomastia, galactorrhea (as it is antiandrogenic & increases
prolactin level)
Cimetidine inhibits CYP450 (specifically CYP1A2,
CYP2C9, CYP2C19, CYP2D6, CYP2E1, and CYP3A4) & increases conc. of Warfarin, Theophylline, Phenytoin, Ethanol.

Proton Pump Inhibitors
Most effective drugs in antiulcer therapy
Irreversible inhibitor of H+ K+ ATPase
Prodrugs requiring activation in acid environment
Lipophilic , weakly basic drugs & so accumulate in canaliculi of parietal cell
Activated in canaliculi & binds covalently to extracellular domain of H+ K+ ATPase
Acid secretion resumes only after synthesis of new molecules

Proton Pump Inhibitors
Omeprazole 20 mg o.d. (Once Daily)
Esomeprazole 20 - 40 mg o.d.
Lansoprazole 30 mg o.d.
Pantoprazole 40 mg o.d.
Rabeprazole 20 mg o.d.

Proton Pump Inhibitors – Kinetics
PPI are administered as inactive prodrugs.
To protect the acid-labile prodrug from rapid destruction within the gastric lumen, oral products are formulated for delayed release as acid-resistant, enteric-coated tablet or capsule formulations.
Esomeprazole, lansoprazole, and pantoprazole
also given intravenously
Half life – 1.5 hrs
Since it requires acid for activation - given 1 hr before meals
Other acid suppressing agents not coadministered

P.P.I. – Side effects & Interactions
Extremely safe drugs
Causes hypergastrinemia which leads to carcinod tumor (ECL cell hyperplasia) in rats, but no evidence of such tumors in man
Inhibit CYP 450 & hence metabolism of warfarin, phenytoin, etc
Pantoprazole & Rabeprazole have no significant interactions

A patient comes to your clinic at midnight complaining of heart burn. You want to relieve his pain immediately. What drug will you choose?

Answer :
Antacids
Explanation :
Antacids neutralise the already secreted acid in the stomach. All other drugs act by stopping acid secretion and so may not relieve symptoms at least for 45 min.

Mucosal Protective Agents
Sucralfate
Misoprostol
Colloidal Bismuth compounds

Sucralfate
Salt of sucrose complexed to sulfated aluminium hydroxide
In acidic pH polymerizes to viscous gel that adheres to ulcer crater & stimulates mucosal prostaglandin
Taken on empty stomach 1 hr. before meals
Concurrent antacids, H2 antagonist avoided
( as it needs acid for activation )

Misoprostol
PGE analogue
Modest acid inhibition Stimulate mucus & bicarbonate secretion
Enhance mucusal blood flow
Approved for prevention of NSAID induced ulcer
Side effect : Diarrhoea & cramping abd. pain – 20 %
Not so popular as P.P.I are more effective & better tolerated

Colloidal Bismuth Compounds
Coats ulcer, stimulates mucus & bicarbonate secretion
Direct antimicrobial activity against H.pylori
May cause blackening of stools & tongue
Not used for long periods – bismuth toxicity
Available compounds :
Bismuth subsalicylate – in USA (IndScantoma)
Bismuth subcitrate – in Europe
Bismuth dinitrate

A pregnant lady (first trimester) comes to you with peptic ulcer disease. Which drug will you prescribe for her ?

Answer :
Antacids or Sucralfate
Explanation ;
H2 antagonists cross placenta and are also secreted in breast milk. Safety of Proton pump inhibitors not established in pregnancy. Misoprostol causes abortion .

Eradication of H.pylori

Triple Therapy
The BEST among all the Triple therapy regimen is
Omeprazole / Lansoprazole - 20 / 30 mg bd
Clarithromycin - 500 mg bd
Amoxycillin / Metronidazole - 1gm / 500 mg bd
Given for 14 days followed by P.P.I for 4 – 6 weeks
Short regimens for 7 – 10 days not very effective??
Newest 7 days…

Triple Therapy – cont …
Bismuth subsalicylate – 2 tab qid
Metronidazole - 250 mg qid
Tetracycline - 500 mg qid
Some other Triple Therapy Regimens are
Ranitidine /Bismuth citrate - 400 mg bd
Tetracycline - 500 mg bd
Clarithromycin / Metronidazole - 500 mg bd

Quadruple Therapy
Given when Triple Therapy fails
Omeprazole / Lansoprazole - 20 / 30 mg bd
Bismuth subsalycilate - 2 tabs qid
Metronidazole - 250 mg qid
Tetracycline - 500 mg qid

Drugs causing peptic ulcer
Non Steroidal Anti Inflammatory Drugs (NSAIDs)
Glucocorticoids
Cytotoxic agents
Stress induced ulceration after head trauma (ICP) = Cushing’s ulcer
Stress induced ulceration after severe burns
= Curling’s ulcer

AntiemeticsAntiemetics

Vomiting Centre (medulla)
Cerebral cortex
Anticipatory emesisSmellSight
Thought
Vestibular nucleiMotion
sickness
Pharynx & GIT
Chemo & radio therapy Gastroenteritis
Chemoreceptor Trigger Zone
(CTZ)
Cancer chemotherapyOpioids
Muscarinic, 5 HT3 & Histaminic H1
5 HT3 receptors
Dopamine D2,
5 HT3,Opioid Receptors
Muscarinic Histaminic H1
Pathophysiology of Emesis

Now answer this question
Which group of drugs can be used as antiemetics ?
Serotonin 5 HT3 Antagonists
Dopamine D2 Antagonist
Anticholinergics
H1 Antihistaminics
Cannabinoids

Serotonin 5 HT3 Antagonist
Potent antiemetics
Even though 5 HT3 receptors are present in vomiting centre & CTZ, the antiemetic action is restricted to emesis caused by vagal stimulation.
High first pass metabolism
Excreted by liver & kidney
No dose reduction in renal insufficiency but needed in hepatic insufficiency
Given once or twice daily – orally or intravenously.

Drugs Available
Ondansetron 32 mg / day
Granisetron 10 g / kg / day
Dolasetron 1.8 mg / kg / day
Indications
Chemotherapy induced nausea & vomiting – given 30 min. before chemotherapy.
Postoperative & postradiation nausea & vomiting

Adverse EffectsExcellent safety profile
Headache & constipation
All three drugs cause prolongation of QT interval, but more pronounced with dolasetron.

Dopamine D2 Antagonist
Antagonise D2 receptors in CTZ.
Drugs available
Metoclopramide 10 mg tid
Domperidone 10 mg tid
Both drugs are also prokinetic agents due to their 5 HT4 agonist activity.
Domperidone – oral ; Metoclopramide – oral & i.v
Metoclopramide crosses BBB but domperidone cannot.

Now answer this question
Which is a better antiemetic – Metoclopramide or Domperidone ?
As CTZ is outside BBB both have antiemetic effects.
But as metoclopramide crosses BBB it has adverse effects like extrapyramidal side effects.
Domperidone is well tolerated.

Phenothiazines & Butyrophenones
Phenothiazines
Prochlorperazine
Promethazine
Phenothiazines are antipsychotics with potent antiemetic property due to D2 antagonism.
Butyrophenone
Droperidol
Droperidol used for post-op. nausea & vomiting, but cause QT prolongation.

H1 Antihistaminics
Most effective drugs for motion sickness
Drugs available
Betahistine
Meclizine
Cyclizine
Dimenhydrinate
Diphenydramine
Promethazine – Used in pregnancy,
used by NASA for space motion sickness

AnticholinergicsScopolamine (hyoscine) – used as oral or
transdermal patch for motion sickness
Cannabinoids
Dronabinol – used as adjuvant in chemotherapy induced vomiting.It is a psychoactive substance
Nabilone

Now answer this question
A physician prescribed Tab.Ondansetron for prophylaxis of motion sickness. Even though ondansetron is a potent antiemetic it didn’t produce any effect in this patient. Can you explain why ?

Explanation :
Vestibular nuclei has only muscarinic and H1 histaminic receptors.

GERD GERD (Gastroesophageal Reflux (Gastroesophageal Reflux
Disease)Disease) ► Chronic symptoms or mucosal damage produced
by the abnormal reflux in the esophagus due to incompetence of the lower esophageal sphincter (LES), transient LES relaxation, impaired expulsion of gastric reflux from the esophagus, or a hiatal hernia
► Symptom :Symptom :Heartburn, cough, hoarseness, voice changes, chronic ear ache, burning chest pains, nausea & vommiting & vommiting

► Principle Management :Principle Management : lifestyle modifications lifestyle modifications weight loss and elevating the head of the bedweight loss and elevating the head of the bed avoiding eating two hours before bed avoiding eating two hours before bed
► Certain foods & lifestyle are considered to promote reflux:Certain foods & lifestyle are considered to promote reflux: Coffee, alcohol, and excessive amounts of Vitamin C supplements Coffee, alcohol, and excessive amounts of Vitamin C supplements
stimulate gastric acid secretion. Taking these before bedtime stimulate gastric acid secretion. Taking these before bedtime especially can cause evening refluxespecially can cause evening reflux
Foods high in fats and smoking reduce lower esophageal Foods high in fats and smoking reduce lower esophageal sphincter competence, so avoiding these tends to help. Fat also sphincter competence, so avoiding these tends to help. Fat also delays stomach emptyingdelays stomach emptying
Large meals Large meals Carbonated soft drinks (regular or diet). Carbonated soft drinks (regular or diet). Chocolate and peppermintChocolate and peppermint Acidic foods, such as oranges and tomatoes Acidic foods, such as oranges and tomatoes Cruciferous vegetables: onions, cabbage, cauliflower, broccoli, Cruciferous vegetables: onions, cabbage, cauliflower, broccoli,
spinach, brussels sprouts spinach, brussels sprouts Milk and milk-based products contain calcium and fat, and should Milk and milk-based products contain calcium and fat, and should
be avoided before bedtime. be avoided before bedtime.
GERD GERD (Gastroesophageal Reflux (Gastroesophageal Reflux
Disease)Disease)

► Drug treatmentDrug treatment Proton pump inhibitors Proton pump inhibitors are the most effective in reducing gastric are the most effective in reducing gastric
acid secretion. These drugs stop acid secretion at the source of acid secretion. These drugs stop acid secretion at the source of acid production.acid production.
Antacids before meals or symptomatically after symptoms begin Antacids before meals or symptomatically after symptoms begin can reduce gastric acidity (increase pH). can reduce gastric acidity (increase pH).
Alginic acid may coat the mucosa as well as increase pH and Alginic acid may coat the mucosa as well as increase pH and decrease reflux.decrease reflux.
Gastric H2 receptor blockers can reduce gastric secretion of acid. Gastric H2 receptor blockers can reduce gastric secretion of acid. They relieve complaints in about 50% of all GERD patients.They relieve complaints in about 50% of all GERD patients.
Prokinetics strengthen the LES and speed up gastric emptying. Prokinetics strengthen the LES and speed up gastric emptying. Sucralfate is also useful as an adjunct in helping to heal and Sucralfate is also useful as an adjunct in helping to heal and
prevent esophageal damage caused by GERD, however it must be prevent esophageal damage caused by GERD, however it must be taken several times daily and at least 1-2 hours apart from meals taken several times daily and at least 1-2 hours apart from meals and medications. and medications.
GERD GERD (Gastroesophageal Reflux (Gastroesophageal Reflux
Disease)Disease)