Embed Size (px)
Citation preview

Wright, 2012 1
Pharmacology Pearls: What I Wish I Knew Years Ago
Wendy L. Wright, MS, RN, ARNP, FNP, FAANPFamily Nurse Practitioner
Owner - Wright & Associates Family Healthcare
Amherst, New Hampshire
Partner – Partners in Healthcare Education, LLC
Objectives
• Upon completion of this lecture, the participant
will be able to:
– Discuss 10 -20 “pharmacology” pearls of practice
related to various disease states
– Identify techniques to incorporate these
pharmacology pearls into practice
Wright, 2012
Pharmacology/Drug
Interaction Pearls
Wright, 2012
Malpractice Suits
• Drug interactions
–Drug interactions: Now the 4th leading
cause of death in the United States
–Now: 6th leading cause of malpractice
suits against nurse practitioners,
physician assistants, and physicians
Wright, 2012
Many Common Complaints Can Occur From a
Drug/Drug Interaction
• Fatigue
• Constipation or diarrhea
• Confusion
• Incontinence
• Falls
• Depression
• Weakness or tremors
• Excess drowsiness or dizziness
• Agitation or anxiety
• Decreased sexual behavior
Wright, 2012
3 Mechanisms For Drug Interactions
• Drug Interactions
– 1. Drug interactions occur when medications
utilize the same enzyme in the liver for
metabolism
– 2. Can also occur if one medication interferes
with another medication’s excretion through
the kidneys
– 3. Can occur if multiple “highly protein bound
drugs” are given to a patient
Wright, 2012

Wright, 2012 2
Let’s Start With
Drug Interactions
Which Occur
Through CYP 450
Wright, 2012
Cytochrome P450
• History of CYP450
– Not much was known about this drug
metabolism system until Seldane and
erythromycin began to producing Torsade de
Pointe
• CYP450: Enzymes, found within the liver,
which metabolize various medications
• Many medications utilize these pathways
for metabolismWright, 2012
CYP450
• Purpose of this enzyme system is to
metabolize a substance so that it
may be broken down and excreted or
so that it may be delivered to the
tissues on which it will act
Wright, 2012
Pathways
• There are > 100 enzymes or pathways
– 1A2
– 2C9
– 2C19
– 3A4
– 2D6
Wright, 2012
Terminology
• Substrates
–Metabolized by the isoenzyme
• Inhibitors
–Block the activity of the isoenzyme
• Inducers
–Accelerate the activity of the isoenzyme
Wright, 2012
Examples of Common Drug Interactions
CY P450 Isoenzyme
Drug Substrate Drug Inhibitor Drug
Inducer
1A2 Caffeine
Theophylline
Cimetidine
Fluvoxamine (Luvox)
Ticlopidine (Ticlid)
Fluoroquinolones
Tobacco
Nicotine
Wright, 2012Adapted from: Abramowicz, M. (1999). Drug Interactions. The Medical Letter on Drugs and Therapeutics. 41(1056) 61-62.

Wright, 2012 3
Let Us Look At An Example!
• Patient drinks 4 cups of coffee per day
– Caffeine is a substrate
• You prescribe ciprofloxacin
– Ciprofloxacin is an inhibitor
• What happens to the caffeine levels?
• About what will the patient complain?
Wright, 2012
Another Example
• Patient is on theophylline for COPD
– Substrate
• Smoking (Nicotine)
– Nicotine is an inducer
• What have you had to do with the theophylline
to get this patient to a therapeutic goal?
• Patient develops AECB and quits smoking
• What happens to theophylline levels?
Wright, 2012
CY P450 3A4
• This is the location of most drug-drug
interactions
• 50% of medications are metabolized
through this pathway
Wright, 2012
Examples of Common Drug Interactions
CY P450 Isoenzyme
Drug Substrate
Drug Inhibitor
Drug Inducer
3A4 Amiodarone
Diltiazem
Felodipine
Nifedipine
Verapamil
Lovastatin
Simvastatin
Amiodarone
Clarithromycin
Erythromycin
Fluconazole
Itraconazole
Ketoconazole
Barbiturates
Carbamazepine
Phenytoin
Rifampin
Phenobarbital
St. John’s Wort
Wright, 2012Adapted from: Abramowicz, M. (1999). Drug Interactions. The Medical Letter on Drugs and Therapeutics. 41(1056) 61-62.
Examples of Common Drug Interactions
CY P450 Isoenzyme
Drug Substrate
Drug Inhibitor
Drug Inducer
3A4 Atorvastatin
Quinidine
Alprazolam
Diazepam
Methadone
Sildenafil
Grapefruit juice
Ritonavir
Fluoxetine
Nefazodone
Barbiturates
Carbamazepine
Phenytoin
Rifampin
Phenobarbital
St. John’s Wort
Wright, 2012Adapted from: Abramowicz, M. (1999). Drug Interactions. The Medical Letter on Drugs and Therapeutics. 41(1056) 61-62.
Also Important
• Drugs that are substrates of the same
CYP 450 substrate can inhibit each
other’s metabolism, possibly resulting in
drug toxicity
Wright, 2012

Wright, 2012 4
Let Us Look At Another Patient• 78 year-old woman with asthma, hypertension,
hyperlipidemia, obesity, osteoarthritis
– Currently on numerous medications including Zocor (simvastatin) 80 mg qhs
• Develops chest pain, rules-in for an MI and undergoes a 6-vessel CABG
– Started on Amiodarone
• 4 weeks later: Creatinine 3.0; LFTs-2x upper limits of normal (had all been normal in patient and before surgery)
– Cardiology consulted – recommend gastroenterology evaluation; Gastro said it was a reaction to the Zocor
• 1 week later – Creatinine 3.2
• What really is going on?Wright, 2012
Drugs Frequently Involved in Interactions
• Statins
– Lova, simva, atorva
• Amiodarone
• Telithromycin, erythromycin, clarithromycin
• -Azoles
• -Antivirals
Wright, 2012
Ideally, a Medication Would Use Multiple
Pathways for Metabolism
Wright, 2012
• Some medications use multiple
pathways
• This is ideal
–If one pathway is being utilized by
multiple medications, the medication
can be metabolized by the other
pathway
Another Example
Wright, 2012
CW
• CW is a 52-year-old woman who presents to discuss her recent cholesterol profile
– Lab results are as follows:
• Total cholesterol: 286
• HDL: 46
• LDL: 199
• Triglycerides: 154
• Risk ratio: 6.22
• LFT’s: normal
Wright, 2012
Treatment
• CW has been on a diet and exercise plan for the last 3 months attempting to lower her cholesterol without pharmacotherapy
• At today’s visit, atorvastatin therapy initiated
• Dosage: 20 mg qhs
Wright, 2012

Wright, 2012 5
HMG Co-A Reductase Inhibitors• Metabolized through the liver
– Liver is the primary site of elimination for the majority of medications on the market
– Statins are no exception
– The liver contains numerous enzymes that oxidize or conjugate drugs
• CYP450 is involved in the metabolism of most statins
– In fact, most statins use the 3A4 pathway
– Pravastatin is one exception; it is not metabolized through the CY P450 system; Crestor (rosuvastatin –2C9)
Wright, 2012
Caution: CY P450 3A4
• Caution: Medications using CY P450 3A4
– Avoid azole medications (rhabdomyolysis)
– Avoid concomitant gemfibrozil
(rhabdomyolysis)
– Avoid erythromycin and clarithromycin
(increases statin AUC by 50%)
Wright, 2012
6 Months Later
• CW calls complaining of cramping in her feet only at night
• It is occurring every night
• This is new; she has never had anything like this before and because of our discussion regarding potential side effects of the statin class, she decided to call
• She was advised to stop atorvastatin and come into the office for an evaluation and a few additional laboratory tests
Wright, 2012
Rhabdomyolysis
• Concern regarding rhabdomyolysis
– Fatigue
– Myalgias
– Cramping
– If these occur:
• Discontinue the drug
• CK (Done to exclude muscle involvement)
• LFTs (full liver panel is recommended because we are now potentially dealing with a significant problem)
Wright, 2012
CW’s Labs
• Physical examination: normal; no evidence of tender or edematous muscles
• CK: 3305 (normal level: 20-170)
• Chemistry panel: normal
• Urinalysis: normal
• CBC with differential: normal
Wright, 2012
Rhabdomyolysis
• Laboratory Features:
– Elevated CK-MM** Most sensitive test
• With rhabdo, range is often: 500 ->100,000 units/L
• Degree of elevation roughly correlates with the risk of renal failure
Wright, 2012

Wright, 2012 6
What Changed?
• Why did this happen?
• CW went to a walk-in center
• Diagnosed with “walking pneumonia”
• Given a prescription for clarithromycin
Wright, 2012
Remember CY P450 3A4
• Atorvastatin is a substrate
• Clarithromycin is an inhibitor
• Blocks 3A4 enzyme causing atorvastatin levels
to increase significantly (50%)
Wright, 2012
What Psychiatric Medications Can Do
The Same Thing?
• Nefazodone
• Alprazolam
Wright, 2012
Interactions
Involving Renal
System
Wright, 2012
Lithium
Wright, 2012
CF
• CF is a 62-year-old female with bipolar disorder
• Currently maintained on Lithium 300 mg 2 tablets po bid
• Has been on this dosage x years and doing relatively well; moods are stabilized
• Employed in a steady job; marriage going well
• Presented to family physician for bilateral knee pain
• Diagnosed with osteoarthritis; started on naproxen
Wright, 2012

Wright, 2012 7
CF Presents 3 Weeks Later
• Husband is concerned
• Seems more confused
• Complaining of dizziness, nausea, and tremor
• Began approximately 1 week ago and seems to be worsening
• CBC with diff, CMP, UA, Lytes, Lithium level, TSH and CT scan obtained
Wright, 2012
Laboratory Values
• CBC with diff: normal
• CMP: normal
• Lytes: normal
• UA: normal
• Lithium level: 2.2 mEQ/L (normal: 0.8 mEq/L – 1.2 mEq/L)
• CT scan: normal
Wright, 2012
What Changed???
• What caused a
sudden change in
this woman?
– Is this delirium?
– Medication
– TIA?
– CVA?
Wright, 2012
Lithium
• Lithium is cleared completely through the renal
system
• Drugs and conditions that influence renal
excretion stand the potential for increasing
serum lithium concentrations
• Such drugs include: thiazide diuretics, NSAIDs,
ACE inhibitors, Calcium channel blockers
(diltiazem and verapamil), Caffeine
Wright, 2012
Let’s Talk About NSAIDs and
Lithium
• NSAIDs
– Have been associated with increasing lithium plasma levels to toxic levels
– OTC medications can produce the same effect yet it is not seen as much as anticipated when they went OTC
– ? Lower dosage
– If you need to use an NSAID in a patient with lithium: consider aspirin and sulindac
– Less likely to cause toxicityWright, 2012
Thiazides and Lithium
• In fact, concomitant use of diuretics has long been
associated with the development of lithium
toxicity
– Thiazide diuretics are thought to be the worst
because they act distally on the renal tubule
(same location as lithium is cleared) causing an
increase in the re-absorption of lithium
Wright, 2012
Wright, 2012 8
Think of All the Antihypertensives
• Most antihypertensives now have
HCTZ in them
• Easy for a drug interaction to
occur
Wright, 2012
Other Drugs Can Lower Lithium Levels
• Osmotic diuretics enhance lithium excretion and are often used for lithium toxicity
• Caffeine and theophylline also decrease lithium levels and therefore need to be monitored if used concomitantly
Wright, 2012
Other Labs to Monitor in Patients
Taking Lithium
• TSH (lithium decreases thyroxine production by interfering with iodine absorption)
• Calcium (increased levels)
• Glucose (increased levels)
• Potassium (increased levels)
• If patient is on a stable dosage, can monitor these every year
Wright, 2012
Other Medications Which Can Alter
The TSH
• Amiodarone
• Lithium
• Interferon
• Why??
Wright, 2012
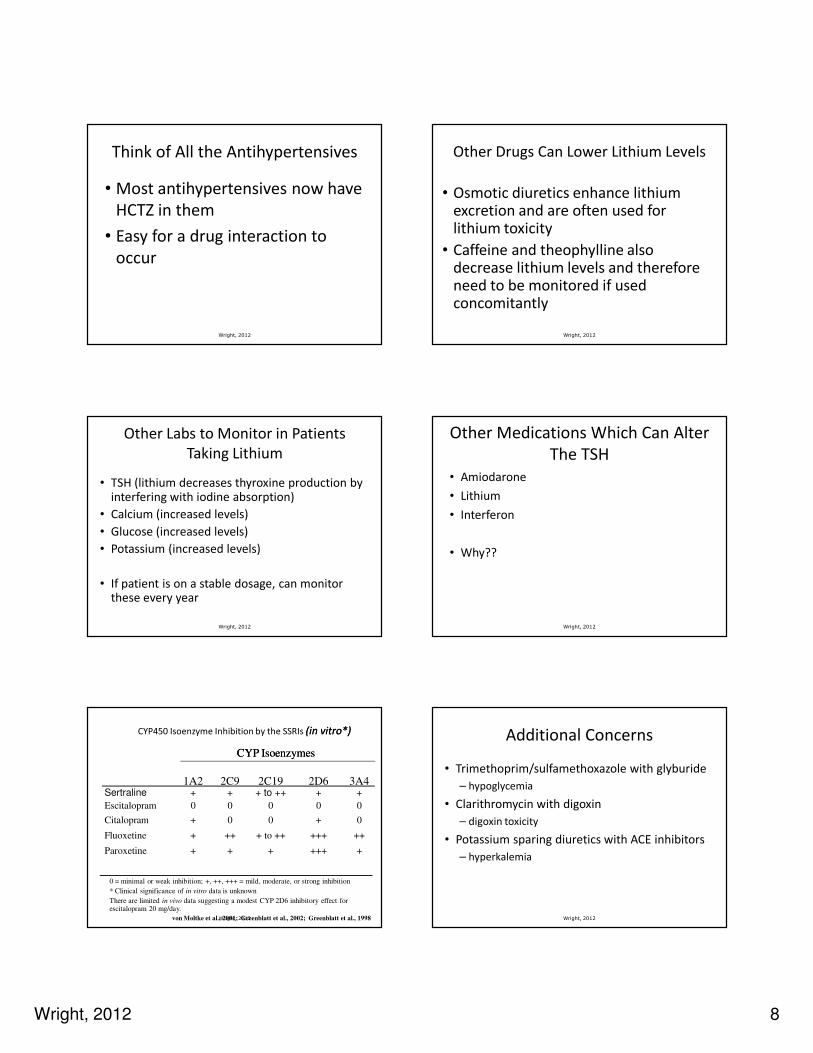
CYP450 Isoenzyme Inhibition by the SSRIs (in vitro*)(in vitro*)
Wright, 2012
0 = minimal or weak inhibition; +, ++, +++ = mild, moderate, or strong inhibition
* Clinical significance of in vitro data is unknown
There are limited in vivo data suggesting a modest CYP 2D6 inhibitory effect for escitalopram 20 mg/day.
1A2 2C9 2C19 2D6 3A4Sertraline + + + to ++ + +
Escitalopram 0 0 0 0 0
Citalopram + 0 0 + 0
Fluoxetine + ++ + to ++ +++ ++
Paroxetine + + + +++ +
CYP IsoenzymesCYP Isoenzymes
von Moltke et al., 2001; Greenblatt et al., 2002; Greenblatt et al., 1998
Additional Concerns
• Trimethoprim/sulfamethoxazole with glyburide
– hypoglycemia
• Clarithromycin with digoxin
– digoxin toxicity
• Potassium sparing diuretics with ACE inhibitors
– hyperkalemia
Wright, 2012

Wright, 2012 9
Other Areas of Risk
• Case in NH
• NP wrote RX for Elocon for eczema; large tube
with 5 refills
• Refilled 6 months later
• Patient sued; had been using the steroid cream as
a moisturizer
• Developed striae over lower extremities
• What could have been done differently?
Wright, 2012
Techniques to Avoid Errors
• Clear writing and documentation
• EHR, if available
• Double check dosages
• Avoid writing RX’s when patient is talking to
you or sitting in front of you
• Have a list of high risk drugs; when you see
this list – bells should go off in your head
• Double check interactions
Wright, 2012
HEENT Pearls
Wright, 2012
Internal Hordeola
Wright, 2012
Blepharitis
Wright, 2012
• Mycoplasma
• Intensely painful
• Treatment is with a
macrolide
Bullous Myringitis
Wright, 2012

Wright, 2012 10
Allergic Facies
Wright, 2012
ABRS Treatment Guidelines
Adult: Mild ABRS
No antibiotic use in 4 – 6 weeks
Adult: Mild ABRS
No antibiotic use in 4 – 6 weeks
No improvement or worsening at 72
hours
Amoxicillin (1.5 – 4.0 g)/day
Amox/clav (1.75 – 4.0g/250mg)/day
Cefpodoxime (Vantin)
Cefuroxime (Ceftin)
Cefdinir (Omnicef)
Amox/clavulantate (4g/day)
Levofloxacin (Levaquin)
Moxifloxacin (Avelox)
Wright, 2012Sinus and Allergy Health Partnership Guidelines
Otolaryngol Head Neck Surg. 2004;130:1-
ABRS Treatment Guidelines
Adult: Mild ABRS
No antibiotic use in 4 – 6 weeks
Beta-Lactam Allergy
Adult: Mild ABRS
No antibiotic use in 4 – 6 weeks
Beta-Lactam Allergy
No improvement or worsening at 72
hours
TMP/SMX (Bactrim)
Doxycycline
Azithromycin (Zithromax)
Clarithromycin (Biaxin)
Erythromycin
Levofloxacin (Levaquin)
Moxifloxacin (Avelox)
Clindamycin (Cleocin) with rifampin
Wright, 2012Sinus and Allergy Health Partnership Guidelines
Otolaryngol Head Neck Surg. 2004;130:1-
ABRS Treatment Guidelines
Adult: Mild ABRS and recent antibiotic
usage or moderate ABRS
+/- antibiotic use in 4 – 6 weeks
Adult: Mild ABRS and recent antibiotic
usage or moderate ABRS
+/-antibiotic use in 4 – 6 weeks
No improvement or worsening at 72
hours
Levofloxacin (Levaquin)
Moxifloxacin (Avelox)
Amox/clavulanate (4g/day)
Ceftriaxone (Rocephin)
Clindamycin with rifampin
Re-evaluate
Consider complication
Wright, 2012Sinus and Allergy Health Partnership Guidelines
Otolaryngol Head Neck Surg. 2004;130:1-
ABRS Treatment Guidelines
Adult: Mild ABRS and recent antibiotic
usage or moderate ABRS
+/- antibiotic use in 4 – 6 weeks
Beta-Lactam Allergy
Adult: : Mild ABRS and recent antibiotic
usage or moderate ABRS
+/- antibiotic use in 4 – 6 weeks
Beta-Lactam Allergy
No improvement or worsening at 72
hours
Levofloxacin (Levaquin)
Moxifloxacin (Avelox)
Clindamycin (Cleocin) with rifampin
Re-evaluate patient
Consider complication
Wright, 2012Sinus and Allergy Health Partnership Guidelines
Otolaryngol Head Neck Surg. 2004;130:1-
Wright, 2012
Fluoroquinolone Side Effects
• Associated with tendonitis and spontaneous
tendon rupture
– Rupture may occur during or after use
– Discontinue with any tendon pain
**Clinical Pearl: Biggest risk factor is concomitant oral
steroid use
– Give magnesium 325 mg (Magnesium oxide) 6 hours
before fluoroquinolone dose
Lecture Lecture –– Paul Iannini, MD; Worcester, MA, 2006Paul Iannini, MD; Worcester, MA, 2006

Wright, 2012 11
Pulmonary Pearls
Wright, 2012 Wright, 2012
IDSA/ATS 2007 Guidelines
for CAP in Adults
• Practice Guidelines for the Management of
Community-Acquired Pneumonia in Adults
– Revised and published in Clinical Infectious Diseases
2007;44:S27 – S72
http://www.medscape.com/viewarticle/546317 accessed 01-28-2010
Wright, 2012
IDSA/ATS CAP
Outpatient Treatment
• Classification
– Previously healthy, no recent (within past 3
months) antibiotic use
• Likely causative pathogens
– S. pneumoniae (Gm pos) with low DRSP risk
– Atypical pathogens (M. pneumoniae, C.
pneumoniae)
– Respiratory virus including influenza A/B, RSV,
adenovirus, parainfluenza
IDSA/ATS CAP
Outpatient treatment
• Strong recommendation
– Macrolide such as azithromycin, clarithromycin, or
erythromycin
Or
• Weak recommendation
– Doxycycline
Wright, 2012
IDSA/ATS CAP
Outpatient treatment
• Classification
– Comorbidities including: COPD, diabetes,
renal or heart failure, asplenia, alcoholism,
immunosuppressing conditions or use of
immunosuppressing medications,
malignancy or use of an antibiotic in past 3
months
Wright, 2012
IDSA/ATS CAP
Outpatient treatment• Likely causative organism
– S. pneumoniae (Gm pos) with DRSP risk
– H. influenzae (Gm neg)
– Atypical pathogens (M. pneumoniae, C.
pneumoniae, Legionella)
– Respiratory virus as mentioned above
Wright, 2012
Wright, 2012 12
Wright, 2012
IDSA/ATS CAP classification for
outpatient treatment• Respiratory fluoroquinolone
OrOr
• Advanced macrolide (azithro- or
clarithromycin) plus b-lactam such as HD
amoxicillin (3- 4 g/d), HD amoxicillin-
clavulanate (4 g/d), ceftriaxone (Rocephin),
cefpodoxime (Vantin), cefuroxime (Ceftin)
• Alternative to macrolide: doxycycline
Wright, 2012
Treated With...
• Macrolide x 5 days
• Clinical improvement within 48 hours
• Chest x-ray repeated in 12 weeks to confirm
resolution
– R/O any underlying pathology
Wright, 2012
Length of Therapy
• Shortened to 5 days
• Provided that the patient is afebrile by 48 – 72
hours
Neurological Pearls
Wright, 2012
Treatments for Migraines
Look How Far We Have Come
• BC: trephination
• 1850: bromide
• 1883: ergotamine
• 1897: aspirin
• 1963: methysergide
• 1975: DHE
• 1993: sumatriptan
• 1998-2003: other triptansTrephination
Wright, 2012
Acute Migraine Management
Evidence-Based Guidelines
• Adopted by AAFP, ACP-ASIM, AAN
– NSAIDs as first-line therapy
– Triptans (or dihydroergotamine) indicated for those who fail to
tolerate or respond to NSAIDs
– No evidence to support the use of butalbital compounds in
acute migraine
– Little evidence to support the use of isometheptene compounds
in migraine
– Opioids “reserved for use when other medications cannot be
used”Snow V, et al. Ann Intern Med 2002;137:840-849.Wright, 2012

Wright, 2012 13
Abortive Medications
The Triptans
Cady R, Dodick DW. Mayo Clin Proc. 2002;77:255-261.
Selective 5-HT1 agonists (the
triptans) have emerged as the gold
standard
for acute migraine therapy.
Hargreaves RJ. Cephalalgia. 2000;20(suppl 1):2-9.
Migraine-Specific Therapy:
The Mechanism of Action
Wright, 2012
Headache Experts Agree That the Optimal Headache Experts Agree That the Optimal
Treatment Strategy Is to Treat Early, Treatment Strategy Is to Treat Early, Before Central Sensitization OccursBefore Central Sensitization Occurs
Adapted from Cady RK. Clin Cornerstone. 1999;1(6):21-32.
Phases of a Migraine Attack
Premonitory/Prodrome
Aura MildModerate to Severe HA Postdrome
Pre-HA Post-HAHeadache
Time
Intensity
TREAT EARLY!
Wright, 2012
Stratified Care vs Step Care
28*†
53*†
69*
20
37
74
0
20
40
60
80
100
1 Hour 2 Hours 4 Hours
Stratified Care
Step Care Within Attacks (All 6 Attacks)
*P < .001 for stratified care vs step care across attacks.†P < .001 for stratified care vs step care within attacks.
Adapted from Lipton RB et al. JAMA. 2000;284:2599-2605.
Attacks (%)
Time Postdose
Step Care Across Attacks (All Attacks)
20
41
55
Headache Response
Wright, 2012
Too Much of a Good Thing….
• Use of any product more than 3 times per week
will result in rebound headaches
• Medication Overuse Headache
– Worsening of head pain caused by frequent and
excessive use of immediate relief medications
– Bilateral, diffuse headache
– Waxes and wanes
– Associated with fatigue, n/v, restlessness
– Will never get better on any medications until
rebounding is eliminatedWright, 2012

Wright, 2012 14
Controller Pharmacologic Therapies
• Beta Adrenergic Receptor Antagonists
– Propranolol 40-240mg qd
– Nadalol 20-80mg qd
– Atenolol 50-150mg qd
– Metoprolol 50-300mg qd
Up to 70% - 80% reduction in severity and frequency of migraine headaches
Wright, 2012
Controller Pharmacologic Therapies
• Calcium Channel Blockers
– Verapamil 120-480 mg qd
– Diltiazem 90 - 180 mg qd
– Nifedipine 30 - 120 mg qd
• Mechanism of Action
– Blocks vasoconstriction and increases cerebral blood
flow
Wright, 2012
Controller Pharmacologic Therapies
• Tricyclic Antidepressants
– Amitriptyline 10-120mg qhs
– Nortriptyline 10-150mg qhs
– Doxepin 10-200mg qhs
– Imipramine 10-200mg qhs
• Mechanism of Action
– Believed to inhibit 5–HT receptors, thus interfering with the
impulse of pain
• Efficacy
– Approximately 40 – 60% of patients experience improvement
within 1-2 monthsWright, 2012
Controller Pharmacologic Therapies
• SSRI’s
– Fluoxetine 10-30mg qd
• Other Agents
– Neurontin 600- 2400 qd
– Phenytoin 300-800 mg qd (macrocytosis)
– Depakote 750-1500 mg qd (pancreatitis, hepatic issues)
– Carbamazepine 200-800 mg qd (macrocytosis, thrombocytopenia)
– Topiramate 50 mg bid (sedation/fatigue/metabolic acidosis)
– Pregabalin 100 -150 mg daily
Wright, 2012
Difficulty With Medications
• Managing side effects
– Paresthesias and memory loss: topiramate
• Dose once daily
– Fatigue and dizziness: pregabalin, gabapentin
• Dose at night
Wright, 2012
Alternative or Other Therapies
• ACE Inhibitor– Lisinopril (Prinivil)
• Alpha-2 Agonist Group– Tizanidine (Zanaflex)
• Riboflavin (B2) 400 mg qd
• Magnesium 600 mg qd
• Coenzyme Q-10 150 mg – 300 mg qd
• Feverfew
• Butterbur Extract
Not evaluated by the US Headache Consortium
Wright, 2012

Wright, 2012 15
What Other Therapies
Are Being Done?
• Botulism injections
• Trigger point injections
• Massage
• Chiropractic manipulation
• Consider “headache clinic” for drug
detoxification
Wright, 2012
Cluster Headaches
• Abortive treatment
– Injectable triptans
– 7L O2 via mask
• Preventative Options
– Lithium
Wright, 2012
My Medication Doesn’t Work...
• Prednisone
– 60, 40, 20 mg/day
• Analgesic
– Ketorolac in office or pain medication
• Antiemetic
– Suppository
– Orally dissolving tablet
Wright, 2012
Another Option
• Ketorolac 15 mg, 30 mg or 60 mg
• Monitor blood pressure
• Consider IV fluids
• Consider antiemetic
Wright, 2012
Case Study: June 2009
• SG is 17 year-old female; referred by school nurse
• Presents with mom who is concerned:
– Daily headaches; requiring medication daily (5 – 6 days per week);
using NSAIDs primarily
– Headaches wax and wane; some days worse than others
• Bilateral, pressure. Hard to concentrate. No neuro symptoms
• Has not had a day in 6+ months without headache
– Occasional (1x per week), horrible headaches requiring nurse visit
and frequently, discharge from school
• These are associated with n/photo/phono; occasional vomiting
– Headaches present x 2 – 3 years but worsening
Wright, 2012
Case Study
• Meds: as above
• Allergies: NKDA or NKFA
• PE – completely normal
• Assessment: What is your diagnosis
Wright, 2012

Wright, 2012 16
Chronic Migraine: Diagnostic Criteria
Not Not
attributable attributable to another to another
disorderdisorder
Meets the Meets the
IHS criteria IHS criteria for migraine for migraine
without aurawithout aura
Occurs Occurs ≥≥ 15 days per month for 15 days per month for ≥≥ 3 months3 months
Usually begins as migraine without aura and Usually begins as migraine without aura and progressesprogresses
As chronicity develops, headache tends to lose its As chronicity develops, headache tends to lose its attackattack--like presentationlike presentation
When medication overuse is present, it is the When medication overuse is present, it is the likely cause of the chronic symptoms likely cause of the chronic symptoms
(Medication overuse headache (Medication overuse headache –– MOH)MOH)
Migraine Fulfilling the Criteria BelowMigraine Fulfilling the Criteria Below
Olesen J et al. Cephalalgia. 2004;24(suppl 1):1-151.Wright, 2012
Common Pitfalls in Migraine Diagnosis:
Importance of Medication Overuse
• MOH is common, but
widely unrecognized
• MOH is almost always
transformed migraine
• Ask patients about all pain
medication use!Patients With CDHPatients With CDH
Patients With HAPatients With HA
General General
PopulationPopulation1%1%11
5%5%--10%10%11
>60%>60%22
1. Diener HC and Katsarava Z. Curr Med Res Opin 2001;17(suppl 1):S17-S21.2. Bigal ME, et al. Neurology 2004;63(5):843-847.Wright, 2012
MOH Diagnosis
• Patients typically overuse multiple
medications simultaneously
– Mean tablets/day = 5.2
– Most commonly overused drugs are
• Butalbital combinations (48%)
• Acetaminophen (46%)
• Opioids (33%)
• ASA (32%)
• Triptans (18%)
Bigal ME, et al. Cephalalgia 2004;24:483-490.Wright, 2012
MOH Diagnosis (cont’d)
• Both diagnosis and treatment require time
– Diagnosis is confirmed in retrospect
– Offending medications must be stopped and
prophylactic medications started
Smith TR and Stoneman J. Drugs 2004;64:2503-2514.Wright, 2012
How Do You Break This Cycle?
• Depends upon what the drug of overuse is
• Prednisone: 20 mg two times daily x 10 days
• Introduce preventative drug
• Absolutely no pain medication
• Consider long-acting NSAID for prophylaxis
• Phenobarbital may be used if overusing butalbital
• Headache diary
Wright, 2012
What Will Happen?
• Abortive meds begin to work better
• Fewer and fewer headaches
• Migraine will return to its acute nature
• Sooner you can treat, more likely to have
success
Wright, 2012

Wright, 2012 17
SG
• March 2010 visit: Review of headache diary
– Migraine: 1x in past three months; lasted < 1 hour with
medication management. Triggered by too little sleep
– Riboflavin 400 mg once daily; tolerating well
– Triptan available for acute migraine treatment
– No use of NSAIDs in 3 months
– Daily headaches gone
– Working with massage therapist re: tension in neck
– Eating three meals daily rather than skipping meals
– Working on biofeedback
Wright, 2012
Genitourinary Pearls
Wright, 2012
Gorbach et al, 1999 Guidelines for Infections in Primary Care.
Complicated UTIE coli
Proteus
Klebsiella
Enterococci
Pseudomonas
Mixed
Other
S epidermidis
E coli 32%
Enterococci 22%Pseudomonas 20%
S epidermidis 15%
Complicated UTI: Pathogens
Wright, 2012
Pathogens: A Discussion
• E. Coli:
– Most common cause of both uncomplicated and
complicated UTI’s
• Enterococci:
– Most common gram positive cause of UTI
– Often associated with recent antibiotic therapy
– Consider recent urologic procedure
– Often cause in the patient with an obstructive
pathologyWright, 2012
http://emediciine.medscape.com/article/245559-overview accessed 03-11
Pathogens: A Discussion
• Staphylococcus saphrophyticus
– Gram positive organism
– Second most common cause in sexually active
woman
• Pseudomonas
– Often seen in the individual with an obstructive
pathology
Wright, 2012
http://emediciine.medscape.com/article/245559-overview accessed 03-11
cUTI Pathogens
• Proteus and Klebsiella
– Predispose the patient to stone formation and are
more often than not seen in patients with calculi
• Tend to be polymicrobial in the setting of an
indwelling catheter or stent placement
Kasper, D.L. (2005). Harrison’s Manual of Medicine (16th ed.). New York, NY.:
McGraw-Hill Companies, Inc. Wright, 2012

Wright, 2012 18
Complicated UTI:
Antimicrobial Choices
• Trimethoprim-sulfamethoxazole (TMP-SMX)
• Fluoroquinolones (ciprofloxacin, ofloxacin,
levofloxacin)
• Aminoglycosides (gentamicin, tobramycin,
amikacin)
• Third-generation cephalosporins (ceftriaxone)
Wright, 2012
Mild – Moderate cUTI
• Guidelines pertain if patient is not residing in
long-term care facility or recently received
fluoroquinolones
– Levofloxacin 250 mg - 500 mg orally once daily
– Ciprofloxacin 250 mg - 500 mg two times daily or
1000 mg XR once daily
http://prod.hopkins-abxguide.org/diagnosis/genitourinary/urinary_tract_infection_complicated accessed 04/12/2009
Wright, 2012
Dosage Adjustment
• Must make sure to account for CrCl in older
population
• May need to reduce dosage based upon level of
kidney disease
Wright, 2012
Culture and Sensitivity
• Once C&S has returned, may narrow spectrum
of antibiotic
• Consider blood cultures
• Consider CBC
• Consider hospitalization, based upon
presentation
http://prod.hopkins-abxguide.org/diagnosis/genitourinary/urinary_tract_infection_complicated accessed 02/01/2012
Wright, 2012
Guidelines for Treatment
• Severely ill, recent FQ or long-term care facility
resident
– Imipenem
– Piperacillin-tazobactam
– Tobramycin or Gentamycin
http://prod.hopkins-abxguide.org/diagnosis/genitourinary/urinary_tract_infection_complicated accessed 04/12/2009
Wright, 2012
Abdominal Pearls
Wright, 2012

Wright, 2012 19
Differentiating Signs and Symptoms of
Chronic Constipation (CC) and IBS-C
*3 BMs/day to 3 BMs/week is considered range of normal stool frequency1. Brandt LJ, et al. Am J Gastroenterol. 2005;100(suppl 1):S5-S21. 2. Delvaux M. Best Pract Res Clin Gastroenterol.
Chronic constipationChronic constipation
IBS with constipation
++-- Abdominal Pain/Discomfort1
++-- Visceral Hypersensitivity2
<3 BMs/Week Normal Stool Frequency*1,3
• Most products will not work until:
– You have cleaned out the patient’s bowel with
colonic cleansing
Chronic Constipation
Wright, 2012
Traditionally Used IBS TreatmentsTreatment
Bulking Agents (eg, wheat bran, corn fiber, psyllium)
Water
Antispasmodics (eg, hyoscyamine, dicyclomine)
Antidepressants (eg, TCAs, SSRIs*)
• Most traditionally used
treatments have little
evidence to support
benefit
TCA, tricyclic antidepressant; SSRI, selective serotonin reuptake inhibitorSpiller R, et al. Gut 2007;56;1770-1798.
Thank You
I Would Be Happy To Entertain Any Questions
Wright, 2012
Wendy L. Wright, MS, RN, ARNP, FNP, FAANP
Wright & Associates Family Healthcare
Wright, 2012


![AZOLES - [DePa] Departamento de Programas Audiovisualesdepa.fquim.unam.mx/amyd//archivero/SINTESISYREACCIONESAZOLES-1,2Y1... · Dakin-West utilizando piridina como el disolvente,](https://img.pdfslide.net/doc/110x75/5bcc0c4009d3f2e1348d30cc/azoles-depa-departamento-de-programas-2y1-dakin-west-utilizando-piridina.jpg)