Embed Size (px)
Citation preview

Udgivet i samarbejde medDansk Cardiologisk Selskabwww.cardio.dk
Dansk Cardiologisk SelskabHauser Plads 101127 København [email protected]
Copyright © Jakob Gerhard Stegger
Tryk: AKA-PRINT A/SJuni 2012
ISBN: 978-87-92010-39-1
Ph.D. thesis
Anthropometry and polymorphisms in
inflammatory genes in relation to acute
coronary syndrome
Jakob Gerhard SteggerPh.D. thesis ● Jakob G
erhard Stegger
Faculty of Health Sciences,University of Aarhus
AARHUS UNIVERSITY AU
Omslag-Jakob Gerhard Stegger-TRYK.indd 1 29-06-2012 10:04:01

Ph.D. thesis
Anthropometry and polymorphisms in inflammatory genes in relation to acute coronary syndrome Jakob Gerhard Stegger

Academic advisors Kim Overvad PhD Department of Cardiology, Centre for Cardiovascular Research, Aalborg Hospital, Aarhus University Hospital, Aalborg, Denmark Section of Epidemiology, Department of Public Health, Aarhus University, Aarhus, Denmark Erik Berg Schmidt DMSc Department of Cardiology, Centre for Cardiovascular Research, Aalborg Hospital, Aarhus University Hospital, Aalborg, Denmark Thorkild I. A. Sørensen DMSc Institute of Preventive Medicine, University of Copenhagen, Co-penhagen, Denmark Members of the assessment committee Steen Dalby Kristensen, DMSc (chairman) Department of Cardiology B, Aarhus Univesity Hospital Ruth Frikke-Schmidt, PhD, DMSci Department of Clinical Biochemistry Section for Molecular Genetics, Rigshospitalet Professor Tobias Pischon, MD, MPH Molecular Epidemiology Group Max Delbrück Center for Molecular Medicine, Berlin Charité University Medicine Berlin The Faculty of Health Science, Aarhus University, Denmark has approved this PhD dissertation for public defense. The public lecture and defense will take place June 19th, 2012 at 14.00 in the Auditorium at Aalborg Hospital Science and Innovation Center.

Anthropometry and polymorphisms in inflammatory genes in relation to acute coronary syndrome 3
Preface
The present thesis is based on studies conducted during my em-ployment as a PhD student at the Department of Cardiology at Aalborg Hospital, Aarhus University Hospital from 2009 until 2012. During this time I have received excellent guidance from my supervisors. You have used your experience to guide me into the world of research, and even though your extensive knowledge has been requested from many sides; you have always found time for me, when I needed it. I have been privileged to work with a group of very skilled do-mestic and foreign co-authors. You have all shown great interest in my work, and your comments have been much appreciated. I am grateful for all the help I have received from everybody at the statistics department. You have all taken the time to explain the answers to my endless questions in a way that made sense. Also, I would like thank my current and previous colleagues at Aalborg Hospital Science and Innovation Center. Your positive spirits have created a pleasant and fun atmosphere. I have enjoyed your everyday company and most of you have, in one way or an-other, contributed to my work. The financial support from the Danish Heart Association and Danish Obesity Research Centre has given me the opportunity to focus full time on my research. A special thanks to my family, Tine, Emil and Oskar. Your smiles and hugs mean the world to me. Jakob Gerhard Stegger, March 2012

4 Jakob Gerhard Stegger
Table of Contents
Abbreviations 4 Introduction 5 Hypotheses 5 Background Acute coronary syndrome 6 Adipose tissue 6 NF-κB 6 Interleukin 1B 6 Study Populations Diet, Cancer and Health 7 US Cohorts 8 Statistics Variables 9 Models 9 Biological Interaction 10 RERI with one Continuous Variable 11 Studies Study I 13 Study II 15 Study III 17 Discussion 18 Conclusions 20 Perspectives 21 English Summary 22 Dansk Resumé 23 References 24 Papers Paper I 26 Paper II 27 Paper III 28
List of Papers This thesis was based on the following papers: 1. Stegger JG, Schmidt EB, Obel T, Berentzen TL, Tjønneland A, Sørensen TIA, Overvad K: Body composition and body fat distribu-tion in relation to later risk of acute myocardial infarction: a Danish follow-up study. Int J Obes 2011; 35: 1433-41 2.Stegger JG, Schmidt EB, Berentzen TL, Tjønneland A, Vogel U, Rimm E, Sørensen TIA, Overvad K, Jensen MK: Interaction between obesity and NFKB1 -94ins/delATTG promoter polymorphism in relation to incident ischemic heart disease: a follow up study in three independent cohorts. Submitted for internal (Channing) review 3. Stegger JG, Schmidt EB, Tjønneland A, Kopp TI, Sørensen TIA, Vogel U, Overvad K: Single Nucleotide Polymorphisms in IL1B and the Risk of Acute Coronary Syndrome: a Danish Case-Cohort Study. Accepted for publication (PLoSONE)
Abbreviations
ACS Acute coronary syndrome BMI Body mass index WC Waist circumference HC Hip circumference LBM Lean body mass BIA Bioelectric impedance analyses BFM Body fat mass MI Myocardial infarction DCH Diet, cancer and health NHS Nurses’ Health Study HPFS Health Professionals Follow-up Study BFP Body fat percentage SNP Single nucleotide polymorphism WHR Waist to hip ratio NF-κB Nuclear factor kappa-light-chain-enhancer of activated B
cells IL-1B Interleukin 1B ICD International classification of diseases

Anthropometry and polymorphisms in inflammatory genes in relation to acute coronary syndrome 5
Introduction
Obesity is a well-known risk factor for acute coronary syndrome (ACS)(1-5), and it may become even more important to society in the future as obesity seems to develop in epidemic propor-tions(6,7). The association between obesity and ACS has been investigated for decades. In the beginning, measures of general obesity like body mass index (BMI) and skin fold thickness were used(8). More recently, it became clear that visceral adipose tissue secretes a relatively greater amount of pro-inflammatory and pro-thrombotic proteins than subcutaneous adipose tissue(9), and that these active proteins could influence the inflammatory processes in the artery wall leading to atherosclerosis(10,11). Since then, the inves-tigational focus turned towards different measures of body fat distribution like waist circumference (WC) and hip circumference (HC)(8,12,13). WC is a measure of abdominal fat accumulation(3), and its strong association with ACS has been well established in both men and women(12-14). HC, on the other hand, is negatively associated with ACS when adjusted for WC or BMI(14,15). HC might represent gluteofemoral fat deposits, but HC could also represent gluteal muscle mass, which is the largest muscle group of the human body. HC could therefore be associated to lean body mass (LBM) that might protect against ACS either on its own or as a surrogate indicator of a healthy lifestyle. The association between BMI and total mortality is U-shaped, and the increased risk associated with a low BMI has been related to a low LBM, while the increased risk in subjects with a high BMI has been related to a high fat mass (16). Bioelectrical impedance analyses (BIA) provide estimates of LBM and body fat mass (BFM), and investigation of the associations between the more detailed results of BIA of body composition and incident ACS may further illuminate the association between obesity and ACS. Inflammation may be an important link between obesity and ACS. As obesity develops, the release of adipose tissue-derived cytokines increases (5), and the resulting state of chronic low-grade inflammation may accelerate atherosclerosis and lead to ACS (5,10,11). However, many obese people do not experience ACS, indicating that other factors may affect the implications of obesity. Several genes encoding pro-inflammatory or anti-inflammatory proteins in both adipose tissues and atherosclerotic plaques are regulated by the NF-κB transcription factor family (5,17-19), and interleukin-1B (IL-1B) is a key pro-inflammatory cytokine(20,21). Both of these proteins have been associated with atherosclerosis (17,22-27), and genetic variation in the expression of NF-κB or IL-1B may modify the effect of obesity, thus explaining part of the inconsistent effect of obesity on ACS. The possible identification of genotypes more or less suscepti-ble to the pathological effects of obesity could be important in determining otherwise healthy obese subgroups that could be in special need of preventive measures.
Hypotheses and aims
The aim of the present thesis was to explore the association with incident ACS for different anthropometric measures including measures of body composition obtained by BIA that had not previ-ously been investigated in large prospective studies. Another aim was to explore the role of inflammation as a pathway between obesity and incident ACS The following hypotheses were tested:
1. Anthropometric measures of body fatness obtained by BIA are positively associated with incident ACS.
2. LBM is negatively associated with ACS.
3. Genetic variation in NFKB1 or IL1B modifies the ef-
fect of obesity on ACS risk according to body fat dis-tribution.
Information on anthropometric data and polymorphisms in candidate genes were used to conduct studies within the Danish Diet, Cancer and Health cohort and the two US-based cohorts the Nurses’ Health study and the Health Professionals Follow-up Study.

6 Jakob Gerhard Stegger
Background
Acute coronary syndrome ACS is a state of acute ischemia of the cardiac muscle tissue due to occlusion of the coronary artery. Thrombus formation within the coronary artery initiated by the rupture of an atherosclerotic plaque is the underlying cause of the vast majority of ACS cas-es(10,28,29). Atherosclerotic plaques develop as low-density lipo-proteins trapped in the arterial wall undergo oxidative modifica-tion and initiate a local inflammatory reaction that activates endo-thelial cells and attracts inflammatory cells. Monocytes migrate into the arterial wall and differentiate into macrophages that scav-enge the oxidized low-density lipoprotein(10,29). Persistent in-flammatory stimulation by perturbation of low-density lipoprotein cholesterol and by endogenous pro-inflammatory cytokines may cause a vicious circle of continuing inflammation leading to accu-mulation of inflammatory cells and lipids, which make up the core of the atherosclerotic plaque(10,29). A cap of smooth muscle cells and collagen seals the lipid laden core of the plaque, but continu-ing inflammation may weaken the cap causing it to rupture, expos-ing the very pro-thrombotic core to circulating blood. This may lead to thrombus formation causing acute ischemia and eventually infarction downstream(28,29). Adipose tissue The function of adipose tissue through evolution has been to store excess energy as fatty acids in good times and release the free fatty acids during periods of starvation. Furthermore, adipose fat deposits have insulated and protected the body. However, adipose tissue has been increasingly recognized also as an active endocrine organ secreting cytokines and hormones that influence various functions as food intake, lipid and glucose metabolism, blood pressure, haemostasis, and inflammation(5,9,30). Adipose tissue consists mainly of adipocytes, but several other cell types including macrophages are present within the stroma(5,30). As obesity develops, the adipocytes increase in size and secrete more free fatty acids which stimulate macrophages to an increased produc-tion of active inflammatory proteins that again stimulate the adi-pocytes to also secrete pro-inflammatory cytokines(5). Thus, obesi-ty establishes a local paracrine loop in the adipose tissue that leads to an increased production and secretion of pro-inflammatory cytokines; a state of adipose tissue dysfunction or adiposo-pathy(5,30). This increased release of adipocyte-derived pro-inflammatory cytokines may induce a systemic state of low-grade inflammation which may accelerate the development of atherosclero-sis(5,10,11,30). Adipose tissue can be divided into visceral adipose tissue and subcutaneous adipose tissue, and the release of adipocyte-derived cytokines varies extensively between these compartments, i.e. visceral fat releases more IL-6, PAI-1, resistin, angiotensinogen, and angiotensinogen converting enzyme, whereas subcutaneous fat releases more leptin, adiponectin and IL-10(5,9,30,31). In the pre-sent thesis we use terms abdominal obesity (high WC) synonymous with excess visceral adipose tissue and gluteofemoral obesity (high
HC) synonymous with excess subcutaneous adipose tissue alt-hough e.g. increased WC also may be due to increased subcutane-ous adipose tissue located abdominally. NF-κB Many genes encoding pro-inflammatory and some genes encoding anti-inflammatory proteins in both adipose tissues and atheroscle-rotic plaques are regulated by the NF-κB transcription factor fami-ly(5,17-19). The NF-κB family consists of heterodimeric or ho-modimeric combinations of five subunits (p50, p100, RelA(p65), RelB and c-Rel), and different combinations have different target genes. The p50/p50 homodimer represses transcription of pro-inflammatory cytokines like TNFalpha and IL-12 and promotes transcription of the anti-inflammatory IL-10(18,19). The NFKB1 -94ins/delATTG promoter polymorphism is an insertion/deletion of four bases in the promoter region of the NFKB1 gene encoding the p50 subunit. It is the only functional polymorphism in NFKB1, and the variant allele containing the deletion produces lower transcript levels of the p50 subunit(32). The NFKB1 -94ins/delATTG promoter polymorphism has been associated with both the inflammatory marker CRP and several inflammatory diseases including ACS(32-34). The NFKB1 -94ins/delATTG promoter polymorphism is not a single nucleotide polymorphism and thus not detected by genome-wide association scans. Interleukin 1B Interleukin-1B (IL-1B) is a key pro-inflammatory cytokine that induces the production of other cytokines, adhesion molecules, and metalloproteinases(20,21). The IL-1 signaling pathway has been associated with the development of atherosclerosis in animal studies(23,24,26), and IL-1B mRNA is increased in human athero-sclerotic arteries(27). Low release of IL-1B due to a single nucleo-tide polymorphism (SNP) in IL-1B has been associated with a rela-tively low risk of MI at young age(25,35). The entire IL1B gene has been sequenced, and several SNPs have been identified in the promoter region, but only four of them (T-31C, C-511T, G-1464C, and C-3737T) seem to be of clinical interest due to their prevalence and functionality(36). However, T-31C and C-511T are in complete linkage in Danes(37), leaving only three functional polymorphisms in this population. The SNPs are all located in the same promoter region and are therefore tightly linked(35). This indicates the need for analyses of functional SNP haplotypes as they exist in the hu-man genome to address the combined effects of concurrent SNPs.

Anthropometry and polymorphisms in inflammatory genes in relation to acute coronary syndrome 7
Study populations
Diet, Cancer and Health Diet, Cancer and Health (DCH) is a Danish prospective study, which was undertaken from December 1993 to May 1997, when all men and women aged 50-64 years, born in Denmark, living in the great-er Copenhagen or Aarhus areas, and with no previous cancer diag-nosis registered in the Danish Cancer Registry were invited to participate in the study. Potential participants were identified from the Civil Registration System in Denmark in which every Danish citizen was identified by a unique ten-digit number. With the mailed invitation, a semiquantitative food frequency questionnaire was enclosed. In total, 57,053 (35%) persons accepted to partici-pate. Among the participants 276 were later excluded due to a cancer diagnosis (other than non-melanoma skin cancer) that was not registered in the Danish Cancer Registry at the time of invita-tion (due to processing delay). The DCH study was approved by the National Committee on Health Research Ethics and the Danish Data Protection Agency. Written informed consent was obtained from all participants to search information from medical registers. A detailed description of the study design and measurement procedures has been pub-lished elsewhere(38). Endpoint assessment The Danish National Patient Registry(39) holds information on diagnoses and procedures, e.g. percutaneous coronary interven-tion, in relation to all hospital ward admissions since 1977. All visits at outpatient clinics and emergency rooms have been registered since 1995. The Danish Causes of Death Registry contains diagno-ses for all deaths since 1943. Patients were registered in both registries in accordance with international classification of diseases (ICD) 8th edition until January 1st 1995 and subsequently according to ICD 10th edition. Danish registries are known to be of high inter-national quality, but a declining autopsy rate and general registra-tion bias make registries like the National Patient Registry and the Cause of Death Registry less valid. A study by Joensen et al. docu-mented the validity of ACS diagnoses (ICD 8: 410-410.99 and 427.27 and ICD 10: I20.0, I21.0-I21.9 and I46.0-I46.9) in the Na-tional Patient Registry and the Causes of Death Registry(40). Of 1,654 participants in DCH, who had been registered with a first-time event of ACS until December 31, 2003, only 1,050 (63,5%) could be validated as cases after meticulously reviewing all the medical records and characterizing them in accordance with the guidelines of the American Heart Association and the European Society of Cardiology. The study showed that the positive predic-tive value varied extensively, with the unstable angina pectoris diagnosis being as low as 16%, whereas a diagnosis of MI given in a ward had a positive predictive value above 90%(40). Valid endpoints are of outmost importance and for our studies regarding the time period until ultimo 2003 (Study II and III), we used only the validated cases. For Study I we extended the follow-up period until April 27, 2008, and thus we needed to validate potential new cases. This validation process was performed by the
author, and as the procedure was only briefly mentioned in the article, it will be described more thoroughly here. Due to the low positive predictive value we did not use the unstable angina diagnosis as an endpoint beyond 2003, but only included patients with MI. From January 1, 2004 and until April 27, 2008 we accepted all participants with an MI diagnosis from a ward as cases, and all other possible cases i.e. MI given in the emergency department or sudden cardiac death, were validated separately by going through diagnoses and procedure codes in the National Patient Registry and the Cause of Death Registry. If the patient chart clearly suggested a non-coronary reason for admit-tance, i.e. if a participant was given the diagnose sudden cardiac arrest with successful resuscitation in the emergency room, but later, in the same admittance, was coded as ruptured abdominal aortic aneurysm and was given the procedure code for the opera-tion thereof, then the participant was classified as non-case. If there was strong indices that the diagnosis was correct, for exam-ple if a participant was given an MI diagnosis after being brought to a cardiology ward with cardiac arrest, then the patient was catego-rized as a case. Finally, if a prior or subsequent diagnosis did not provide evidence to either clearly discard or confirm the diagnosis, then the participant was also accepted as a case. Of the 55,547 participants in DCH after exclusions, 1,087 partic-ipants had a previous validated diagnosis. The chart for 137 partic-ipants had not previously been available for validation, but accord-ing to the National Patient Registry the participants had been given an MI diagnosis in a ward in the time from inclusion and until December 31, 2003. Furthermore, 678 participants had been given an MI diagnosis in a ward in the time from January 1, 2004 and until April 27, 2008. These 1,902 (1,087+137+678) participants were all accepted as cases without further validation. The charts for 37 participants had not previously been available for validation, but the participants had been given a sudden cardiac death diagnosis in the time from inclusion and until December 31, 2003. Sixty eight participants had been given a sudden cardiac death diagnosis in the time from January 1, 2004 and until April 27, 2008 according to the National Patient Registry. Finally, 178 partic-ipants had died in a non-hospital setting, and therefore the inci-dent had not been registered in the National Patient Registry, but the participants had been given an endpoint diagnosis in the Cause of Death Registry. The diagnoses of these 283 (37+68+178) partici-pants were reviewed, and 202 participants were accepted as cases. Anthropometry All anthropometric data were collected by trained laboratory tech-nicians. Height was measured to the nearest 0.5 cm with the par-ticipants standing without shoes. Weight was measured using a digital scale with the participants wearing light clothing and rec-orded to the nearest 0.1 kg. WC was recorded to the nearest 0.5 cm and measured at the narrowest part between the lower rib and the iliac crest. Bioelectrical impedance was obtained using a 50 Hz single frequency device (BIA 101-F, Akern/RJL, Florence, Italy), with

8 Jakob Gerhard Stegger
the participants lying relaxed on a couch with their legs 45° apart and arms 30° from the torso. Estimates of body fat percentage (BFP), BFM, and LBM were obtained by sex-specific equations obtained from a comparable population(41,42). Polymorphisms Blood samples were collected from each participant at baseline, and lymphocytes were isolated and frozen within 2 h. Genotyping was performed in 2004, and in order to preserve biological materi-al, only cases validated by December 31, 2003 and members of a sex-stratified subcohort drawn randomly from the entire cohort at the end of 2003 were genotyped. DNA was isolated from the fro-zen lymphocytes(43-45), and the IL1B T-31C (rs1143627), IL1B G−1464C (rs1143623), and IL1B C−3737T (rs4848306) genotypes were determined on an ABI 7900HT using allelic discrimination (Applied Biosystems, Birkerød, Denmark) as previously de-scribed(37,43). Genotypes of NFKB1 ATTG ins/del (rs28362491) were determined by Taqman allelic discrimination (ABI 7500, Ap-plied Biosystems)(46). Controls with known genotypes were in-cluded in each run, and repeated genotyping of 10% of the sam-ples yielded identical results. Cases and controls were mixed during genotyping, and the case status of samples was blinded during genotyping. Confounders At the baseline visit all participants filled in a food frequency ques-tionnaire and a background questionnaire containing detailed questions concerning socio-demographic factors, lifestyle, and health including information regarding family history of heart disease, physician-diagnosed prevalent disease, and medications. To avoid missing or unclear information both questionnaires were checked by an interviewer together with the participant. Design In all studies, data from DCH were analyzed by a follow-up design, and all analyses were stratified by sex. In Study I we used the en-tire cohort, whereas in Study II and III, we were restricted to geno-typed participants who included all cases validated by December 31, 2003 and a sex-stratified subcohort randomly drawn from the entire cohort including cases. As the subcohort represented the entire cohort, we used a case-cohort design. In all studies we excluded participants for whom information was missing on one or more variables. The Nurses’ Health Study and the Health Professionals Follow-up Study The Nurses’ Health Study (NHS) was established in 1976 at the Channing Laboratory of the Brigham and Women’s Hospital, Bos-ton, MA, US. The study included married, female, registered nurses aged 30–55 years residing in one of 11 larger US states. The Health Professionals Follow-up Study (HPFS) was estab-lished at the Harvard School of Public Health in 1986. The HPFS is a longitudinal study of male health workers (dentists, optometrists, osteopathic physicians, pharmacists, podiatrists, and veterinarians) in the US aged 40-75 years at enrollment. Endpoint assessment In both the NHS and the HPFS, cases of ACS were defined as MI and fatal coronary heart disease. Potential cases were participants who
reported incident ACS events on the follow-up questionnaires and deceased participants. Deaths were identified from state vital records and the National Death Index or reported by the partici-pant’s next of kin or the postal system. Cases were validated pri-marily through review of medical records by physicians blinded to the participant’s questionnaire reports(47). The diagnosis of MI was confirmed on the basis of the criteria of the World Health Organization (symptoms plus either diagnostic electrocardiograph-ic changes or elevated levels of cardiac enzymes), and fatal ACS was confirmed by an examination of hospital or autopsy records, by the listing of ACS as the cause of death on the death certificate, or if ACS was the underlying and most plausible cause. Between blood draw and June 2004, 512 female incident cases of ACS were identified in the NHS, and 454 male cases were identi-fied in the HPFS. After exclusion of participants for whom infor-mation on the NFKB1 genotype, BMI, and covariate data was miss-ing, the NHS comprised 471 cases of incident ACS and 922 controls, while the HPFS comprised 427 cases and 873 controls. Anthropometry Self reported information on height and weight was obtained at baseline, and self-reported measures of WC and HC were obtained in 1986 and 1987 in the NHS and the HPFS, respectively. However, information on WC and HC was not available for all participants, and thus analyses regarding waist and hip circumference only included 426 cases and 679 controls and 382 cases and 821 con-trols in the NHS and the HPFS, respectively. Polymorphisms In the NHS, blood samples were collected in 1989-1990 from par-ticipants free of cardiovascular disease and cancer. Participants underwent local phlebotomy and returned samples to the labora-tory via overnight courier. Upon arrival, whole blood samples were centrifuged and stored in cryotubes as plasma, buffy coat, and red blood cells. DNA was extracted from the buffy coat fraction of centrifuged blood with the QLAmp Blood Kit (Qiagen, Chatsworth, CA, USA). The primary genotyping technique was Taqman SNP allelic discrimination by means of an ABI 7900HT (Applied Biosys-tems, Foster City, CA, USA)(48). Similarly, blood samples were collected from participants free of cardiovascular disease and cancer in the HPFS in 1993-1995. Confounders In both studies, the participants returned questionnaires at base-line and received follow-up questionnaires biennially to update information on lifestyle factors, body weight, and newly diagnosed illnesses. Covariate data for Study II were derived from question-naires administered at blood draw (1990 in the NHS and 1994 in the HPFS), with missing information substituted from previous questionnaires(49,50). Design In both the NHS and the HPFS, we used nested case-control de-signs. Using risk-set sampling, controls were selected randomly and matched in a 2:1 ratio on age, smoking, and month of blood return, among participants who were free of cardiovascular disease at the time ACS was diagnosed in the case patient(51). Participants for whom information was missing were excluded.

Anthropometry and polymorphisms in inflammatory genes in relation to acute coronary syndrome 9
Statistics
In Study I, the incidence rate ratios of ACS were analyzed by Cox proportional hazards regression models with age as the underlying time variable(52). The observation time was censored by death from other causes than ACS, emigration, or end of follow-up April 2008. Age may be one of the strongest risk factors for ACS, and we therefore chose age as time axis to achieve best possible control for potential confounding hereof. On the other hand, we consid-ered time in study to be of only minor importance; the question-naires at the baseline visit may have caused participants to recon-sider their lifestyle, which could alter their risk of ACS, but the effect would most likely have been minor and random. In Study II and III we used a case-cohort design for the DCH data, and the incidence rate ratios in DCH were analyzed by weighted Cox proportional hazards regression models(53). For the NHS and the HPFS data in Study II we used a nested case-control design, and incidence rate ratios were calculated by logistic regres-sion models. Conditional logistic regression would be the natural choice for case-control studies, but a significant number of cases were missing a match in the conditional analyses due to missing exposure/covariate information, and in order to maintain the highest possible statistical power, we chose to provide results from unconditional analyses. Crude conditional and unconditional analyses (adjusted for matching factors) provided very similar results. The proportionality assumptions of the Cox proportional hazards models were evaluated graphically using log-log plots in all analyses. Variables The description of variables varied according to nature of the variable and the context in which the variable was used. Most variables were by nature categorical (SNPs, haplotypes, smoking status, education, hypertension, diabetes mellitus, hypercholes-terolemia, and, for women, menopausal status and hormonal substitution therapy). Physical activity was included as a continu-ous variable expressed in terms of metabolic equivalent (MET)-hours in the NHS and the HPFS, whereas in DCH it was described in three categories (<0.5 hour/week, 0.5 - 3.5 hours/week or >3.5 hours/week). The first category included participants with a very sedentary lifestyle, and the remaining participants were divided according to the recommendation of the Danish Department of Health of 0.5 hours/day. The effects of continuous variables (anthropometric variables, alcohol consumption, total energy intake, and intake of fruit and vegetables) were described linearly or by centered restricted cubic splines. The modeling of a restricted cubic spline is dependent on the number of knots, i.e. a higher number of knots allows the spline to follow the observations more closely. Thus, a high number of knots, e.g. 7, will describe the observations more accurately, but this may lead to non-physiological “bumps” on the curve that most likely represents random variation, but also could be due to bias. On the other hand, a low number of knots, e.g. 3, will result in a smooth curve that may better describe the “true” association as it
would be seen in a perfect dataset, but it will not describe the actual observations as precisely as a spline with a higher number of knots. Likewise, a spline with k number of knots uses k-1 number of degrees of freedom, and that should be considered in small datasets. In all tables in our studies the reported effects are based on a linear or categorical description of the reported exposure variable. Figures were based on an effect of the reported exposure variable modeled by centered restricted cubic splines with 3 knots. All confounder covariates described by splines were included by centered restricted cubic splines with 5 knots. All knots were placed as suggested by Harrel(54). Models There are many potential risk factors for ACS associated with obe-sity, and the large number of cases in all studies gave us statistical power to conduct separate analyses in men and women with ex-tensive confounder control. In all studies we had the same overall analyses strategy to explore associations in three models: Model A1: Crude analyses. In DCH adjusted for age due to the time axis of the Cox proportional hazards model, and in the NHS and the HPFS adjusted for matching factors if unconditional logistic regression models were used. Model A2: Main analyses. Adjusted for all relevant confounders, e.g. smoking status, fruit and vegetables intake, alcohol consump-tion, physical activity, educational level, and, for women, meno-pausal status and hormone replacement therapy. Model B: As A2, but further adjusted for the possible intermedi-ate variables hypercholesterolemia, diabetes mellitus, and hyper-tension. Hypertension, diabetes mellitus, and hypercholesterolemia can be seen as intermediate variables in analyses regarding anthropome-try and ACS, and their inclusion in multivariate analyses contracts the outcome to associations through other pathways, but analyses without these adjustments may imply confounding from other causes to these intermediate variables. To evaluate the effect of these, intermediate variables analyses like model B were per-formed in all three studies, but overall adjustments for both con-founders and intermediate variables had only limited effect on the associations suggesting that residual confounding was unlikely to have played a major role for our findings.

10 Jakob Gerhard Stegger
Biological interaction We investigated possible interaction on an additive scale by calcu-lating the relative excess risk due to interaction (RERI) as suggested by Rothman(55). In all studies, the first exposure was a measure of obesity, and the other exposure was LBM in Study I, the NFKB1 -94ATTG promoter polymorphism in Study II, and haplotypes of SNP’s in the promoter region of IL1B in Study III. Due to the nature of these variables, we used the term biological interaction. The formula for calculating the RERI given by Rothman only applies to two categorical variables, which works well for tables. However, the basis for our assumption of biological interaction was that the investigated variables e.g. obesity and the NFKB1 -94ATTG promoter polymorphism affect the same mediator for ACS. In our studies this mediator is inflammation, but one problem is that the true association between the level of inflammation and the risk of ACS is unknown i.e. it could be linear or, more likely, it could be S-shaped with a lower threshold below which inflammation does not contribute to the risk of ACS, a more or less steep middle part at which changes in the level of inflammation would alter the risk of ACS, and an upper threshold above which the curve flattens, and further increase in inflammation does not result in an concurrent increased risk of ACS. The RERI depends on where on this unknown curve the two exposure variables are, which can be demonstrated by the following example. Assume that the true association between inflammation and ACS risk is S-shaped as explained above. We use a categorical BMI variable with three levels (normal weight, overweight, and obese) as one exposure and the NFKB1 -94ATTG promoter polymorphism as the other. Let the normal weight non-carriers of the variant allele be the reference group with an inflammation level of zero and thus no risk of ACS. Let the variant allele of the NFKB1 -94ATTG promoter polymorphism result in a moderate increase in inflam-mation i.e. by itself the variant allele would put a normal weight
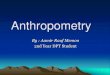
participant close to the lower threshold, but not above, and thus normal weight carriers of the variant allele would not have an increased risk of ACS. Now, let the effect of obesity in the over-weight (middle) group result in an increase in inflammation equal to the middle section of the curve, then the increase in inflamma-tion caused by addition of the NFKB1 -94ATTG promoter polymor-phism would result in an increase in ACS risk i.e. an overweight carrier of the variant allele would have a higher risk of ACS than an overweight non-carrier. In this case the RERI would be positive as the risk of ACS (e.g. hazard rate ratio) among the jointly exposed would be higher than the sum of the individual effects of over-weight and the NFKB1 -94ATTG promoter polymorphism. Now, if the effect of obesity in the obese (highest) group results in an increase in inflammation equal to a point above the upper thresh-old, then the increase in inflammation caused by adding the NFKB1 -94ATTG promoter polymorphism would not result in an increase in ACS risk, and in this case the RERI would again be zero. Thus, the calculated RERI’s are dependent on an unknown curve and thus dependent on the categorization of the exposure variables. In order to avoid this dependency, the obesity exposure variable could be described continuously, e.g. by a spline, and the RERI’s could then be demonstrated graphically. This would give a truer picture of the association between the common mediator and the outcome. In the work of the present thesis we developed a method for calculating the RERI with a continuous variable, but graphically presentation of the RERI was removed from the articles prior to submission. Therefore, I have included a figure (originally used on a poster) that demonstrates a graphically presentation of the RERI among the jointly exposed based on the NFKB1 -94ATTG promoter polymorphism and BMI described by a cubic spline with 3 knots (Figure 1)
0.5
11.
52
RE
RI
22 24 26 28 30 32
Body mass index
Wildtype/Wildtype Wildtype/Variant Variant/Variant
Figure 1

Anthropometry and polymorphisms in inflammatory genes in relation to acute coronary syndrome 11
Relative excess risk due to interaction (RERI) with one continuous variable We have not previously published the mathematics underlying the figure, and therefore it is presented in the following. Let a dichotomous variable G (0/1) (e.g. the presence of a polymorphism in a dominant gene model) and a continuous variable x (e.g. BMI) describe the systematic variation in a multiplicative model for time to event described by a proportional hazards model. Furthermore, let Ck be additional confounders. Then, the hazard rate at a given time )(tλ would be described as;
∑=+++
k kk CGxxGx ett γβββλλ 321)()( 01
(1)
Where )(0 tλ describes the hazard rate for an unexposed (i.e. G=0 and x=0) participant at time (t), and Gx3β describes the potential
interaction between G and x. The hazard rate ratio (‘hazard ratio’, HR) for a participant with the SNP ‘G’ and a BMI of x would be;
∑==
+++k kk CGxxGx
x ettHR γβββ
λλ 321
)()(
0
11 (2)
Now, let )(1 txλ , )(01 txλ , )(0 txλ and )(
00 txλ describe the hazard rates with and without the dichotomous variable, and at a random
x and a reference level x0 of the continuous variable. In a setting without interaction, we can then describe the combined effect of the two exposure variable as the sum of the individual effects;
))()(())()(()()(0000 000101 tttttt xxxxxx λλλλλλ −+−=−
In accordance with Rothman & Greenland (55), the presence of additive interaction (INT) could be described;
INTtttttt xxxxxx +−+−=− ))()(())()(()()(0000 000101 λλλλλλ
))()(())()(())()((0000 000101 ttttttINT xxxxxx λλλλλλ −−−−−= (3)
According to (1) the individual differences would be;
∑−∑=−++++
k kkk kk CxCGxxGxx etettt γβγβββ λλλλ 02321
0)()()()( 0001
)()()()( 02321
0 001xGxxGC
xx eeettt k kk ββββγλλλ −∑=− ++ (4)
and;
∑−∑=−++++
k kkk kk CxCGxxGxx etettt γβγβββ λλλλ 0203021
00)()()()( 0001
)()()()( 0203021
00 001xGxxGC
xx eeettt k kk ββββγλλλ −∑=− ++ (5)
and;
∑−∑=−++
k kkk kk CxCxxx etettt γβγβ λλλλ 022
0)()()()( 0000
)()()()( 022
0 000xxC
xx eeettt k kk ββγλλλ −∑=− (6)

12 Jakob Gerhard Stegger
By insertion of (4), (5) and (6) in (3) we get;
)()()()()()( 022020302102321000
xxCxGxxGCxGxxGC eeeteeeteeetINT k kkk kkk kk ββγββββγββββγ λλλ −∑−−∑−−∑= ++++
)()( 0220203021023210
xxxGxxGxGxxGC eeeeeeetINT k kk ββββββββββγλ +−+−−∑= ++++
)()( 022030213210
xxGxxGGxxGC eeeeetINT k kk ββββββββγλ +−−∑= ++++ (7)
The relative excess risk due to interaction (RERI) is defined by Rothman & Greenland as;
0λ
INTRERI = (8)
By insertion of INT from (7) and 00xλ from (1) we get;
∑
+−−∑=
+
++++
k kk
k kk
Cx
xxGxxGGxxGC
xet
eeeeetRERI
γβ
ββββββββγ
λ
λ02
02203021321
0
)(
)()(
0
0
02
02203021321
0)(
)()(
0
0
xC
xxGxxGGxxGC
xeet
eeeeetRERIk kk
k kk
βγ
ββββββββγ
λ
λ∑
+−−∑=
++++
02
02203021321
0 x
xxGxxGGxxG
x eeeeeRERI β
ββββββββ +−−=
++++
)()()()( 002020300213021
0
xxxxGxxxGGxxxGx eeeeRERI −−+−++−+ +−−= ββββββββ
1)()( 020313021
0+−−= −++−+ xxGxGGxxxG
x eeeRERI ββββββ (9)
1011 00+−−= xxxx HRHRHRRERI
Where 0xRERI denotes that the underlying hazards are ratios in relation to hazard for the reference level x0 for the continuous variable,
i.e. the reference level for e.g. BMI does not have to be zero, but it can be a more relevant level, e.g. 20 kg/m2. Note that, as seen in formu-
la (9), if G=0 or 0xx = then 00=xRERI .

Anthropometry and polymorphisms in inflammatory genes in relation to acute coronary syndrome 13
STUDY I
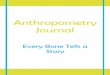
BIA provides information on LBM and BFM, and inclusion of BIA in the assessment of ACS risk could give insight into the individual effects of fat mass and muscle mass. The aim was to investigate the associations between BIA of body composition in relation to ACS defined as incident MI. We conducted our analyses in the DCH cohort and for the final analyses there were 53,884 participants (25,769 men and 28,115 women) including 2,028 cases of incident MI in 1,487 men and 541 women. BFM adjusted for height showed positive associations with incident MI in both sexes as would be expected for a measure of general obesity. Further adjustment of BFM for HC (which makes
BFM a measure of abdominal obesity, like WC) resulted in steeper curves. However, when we adjusted BFM for WC, there was no longer any clear association (Figure 2). Both WC and HC were associated with MI, but the associations were opposite. WC was positively associated with ACS, whereas HC was negatively associated (Table 3, Paper I). The results regarding indices of body fatness obtained by BIA supported the importance of adipose tissue in relation to incident MI. However, the results for WC and HC confirmed the importance body fat distribution. Measures of body fatness (BFM) obtained by BIA seemed not to provide additional information over WC regard-ing the adverse effect of obesity.
Figure 2. Splines of multivariable¹ Cox proportional hazards ratios for the associations between baseline bioelectrical impedance analyses of body composition and incident acute myocardial infarction. Diet, Cancer and Health, Denmark, 1993-2008.
¹) Crude association. ²) Adjusted for smoking status, fruit and vegetable intake, alcohol consumption, physical activity, total energy intake and educational level. Women also adjusted for hormone replacement therapy

14 Jakob Gerhard Stegger
For low LBM (adjusted for BFM and WC) we observed the hy-pothesized negative association with MI, but surprisingly we did not find the expected negative association for high LBM (Figure 3).
Our interaction studies indicated that the almost U-shaped association between LBM and MI mostly represents the obese participants, whereas a more consistent negative association seemed to be present among the participants with normal BFM (data shown in Table 5, Paper I).
Figure 3. Splines of multivariable¹ Cox proportional hazards ratios for the associations between baseline bioelectrical impedance analyses of body composition and incident acute myocardial infarction. Diet, Cancer and Health, Denmark, 1993-2008.
¹) Crude association. ²) Adjusted for smoking status, fruit and vegetable intake, alcohol consumption, physical activity, total energy intake and educational level. Women also adjusted for hormone replacement therapy and menopausal status.

Anthropometry and polymorphisms in inflammatory genes in relation to acute coronary syndrome 15
STUDY II
The NF-κB transcription factor family regulates several genes en-coding pro-inflammatory and some genes encoding anti-inflammatory proteins in both adipose tissues and atherosclerotic plaques, and in the second study, we investigated whether genetic variation in NFKB1 due to the NFKB1 -94ins/delATTG promoter polymorphism interact with obesity in relation to the risk of ACS. The analyses were conducted according to the case-cohort design in DCH and as nested case-control studies in the NHS and the HPFS. We conducted sex-stratified analyses that included 1,202 male and 708 female cases of incident ACS, and the results are presented below in Table 1. There was no substantial interaction between either general, abdominal, or gluteofemoral obesity and the NFKB1 -94ins/delATTG promoter polymorphism in relation to the risk of incident ACS; however, joint exposure to general or abdominal obesity and the variant allele was associated with the highest risk of ACS.

16 Jakob Gerhard Stegger
Table
1. R
R* w
ith 95
% co
nfide
nce i
nterva
l in br
acke
ts for
the c
ombin
ed ef
fect o
f glut
eofem
oral o
besit
y and
the N
FKB1
-94AT
TG po
lymop
hism
in rel
ation
to ac
ute co
ronary
synd
rome.
Diet,
Can
cer a
nd H
ealth
, Hea
lth P
rofes
siona
ls Fo
llow-
up S
tudy (
HPFS
), and
Nurs
es H
ealth
Stud
y (NH
S).
MEN
Varia
bleBo
dy m
ass i
ndex
< 25 k
g/m²
1.00
(ref.
)1.1
4(0
.85;1
.53)1
.10(0
.73;1
.66)
1.00
(ref.
)1.0
4(0
.72;1
.50)0
.79(0
.46;1
.35)
1.00
(ref.
)1.1
0(0
.88;1
.38)0
.97(0
.70;1
.35)
25 - 2
9 kg/m
²1.1
5(0
.86;1
.52)1
.40(1
.07;1
.84)1
.71(1
.24;2
.37)
1.21
(0.80
;1.85
)1.65
(1.11
;2.44
)1.07
(0.60
;1.89
)1.1
7(0
.92;1
.48)1
.48(1
.18;1
.84)1
.52(1
.15;2
.02)
> 29 k
g/m²
1.49
(1.08
;2.05
)1.61
(1.20
;2.18
)1.98
(1.35
;2.91
)1.0
4(0
.59;1
.82)1
.83(1
.11;3
.04)1
.50(0
.68;3
.27)
1.36
(1.03
;1.80
)1.67
(1.29
;2.15
)1.88
(1.33
;2.65
)W
aist c
ircum
feren
ce< 9
4 cm
1.00
(ref.
)1.0
9(0
.84;1
.42)1
.04(0
.71;1
.52)
1.00
(ref.
)1.0
5(0
.68;1
.63)0
.84(0
.45;1
.59)
1.00
(ref.
)1.0
8(0
.86;1
.35)0
.98(0
.71;1
.36)
94 - 1
02 cm
1.04
(0.78
;1.38
)1.29
(0.99
;1.69
)1.56
(1.14
;2.15
)1.3
5(0
.83;2
.18)1
.17(0
.74;1
.85)0
.77(0
.37;1
.59)
1.11
(0.87
;1.42
)1.26
(1.00
;1.59
)1.39
(1.04
;1.86
)> 1
02 cm
1.37
(0.98
;1.91
)1.55
(1.12
;2.15
)2.00
(1.35
;2.95
)0.9
8(0
.56;1
.71)1
.54(0
.94;2
.54)1
.10(0
.58;2
.08)
1.25
(0.94
;1.67
)1.55
(1.18
;2.03
)1.70
(1.22
;2.37
)Hi
p circ
umfer
ence
> 103
.5 cm
1.00
(ref.
)1.2
3(0
.93;1
.63)1
.56(1
.11;2
.20)
1.00
(ref.
)1.3
2(0
.86;2
.01)1
.14(0
.65;2
.00)
1.00
(ref.
)1.2
6(0
.99;1
.59)1
.43(1
.07;1
.92)
98 - 1
03.5
cm0.9
6(0
.70; 1
.30)1
.04(0
.78;1
.38)1
.42(1
.02;1
.99)
1.39
(0.84
;2.31
)1.53
(0.94
;2.50
)0.76
(0.37
;1.55
)1.0
6(0
.81;1
.38)1
.15(0
.90;1
.47)1
.27(0
.94;1
.72)
< 98 c
m1.0
7(0
.77;1
.48)1
.25(0
.91;1
.71)0
.99(0
.64;1
.54)
1.29
(0.75
;2.23
)1.16
(0.69
;1.96
)0.97
(0.45
;2.10
)1.1
2( 0
.85;1
.49)1
.23(0
.94;1
.61)0
.98(0
.67;1
.44)
WOME
N
Varia
bleBo
dy m
ass i
ndex
< 24 k
g/m²
1.00
(ref.
)0.9
6(0
.59;1
.55)0
.69(0
.32;1
.47)
1.00
(ref.
)0.9
7(0
.66;1
.42)1
.02(0
.60;1
.76)
1.00
(ref.
)0.9
6(0
.71;1
.30)0
.90(0
.58;1
.39)
24 - 2
8 kg/m
²1.1
5(0
.67;1
.97)1
.25(0
.80;1
.97)0
.91(0
.44;1
.86)
1.23
(0.79
;1.91
)1.22
(0.81
;1.84
)1.31
(0.77
;2.23
)1.2
0(0
.85;1
.69)1
.24(0
.91;1
.67)1
.15(0
.75;1
.77)
> 28 k
g/m²
1.47
(0.88
;2.45
)1.79
(1.10
;2.89
)2.43
(1.35
;4.37
)1.6
7(1
.08;2
.58)2
.08(1
.34;3
.22)1
.59(0
.84;3
.03)
1.58
(1.14
;2.21
)1.94
(1.41
;2.69
)2.00
(1.30
;3.09
)W
aist c
ircum
feren
ce< 8
0 cm
1.00
(ref.
)0.9
2(0
.57;1
.48)0
.84(0
.42;1
.69)
1.00
(ref.
)0.8
5(0
.57;1
.27)0
.97(0
.57;1
.67)
1.00
(ref.
)0.8
8(0
.65;1
.20)0
.92(0
.60;1
.41)
80 - 9
1 cm
1.69
(0.99
;2.89
)1.68
(1.03
;2.76
)0.96
(0.47
;1.95
)0.8
7(0
.51;1
.48)0
.70(0
.41;1
.21)0
.72(0
.35;1
.46)
1.21
(0.83
;1.77
)1.13
(0.79
;1.63
)0.83
(0.50
;1.37
)> 9
1 cm
2.07
(1.09
;3.95
)3.53
(1.96
;6.35
)5.50
(2.53
;12.0
)1.2
0(0
.64;2
.26)2
.04(1
.05;3
.99)1
.45(0
.59;3
.57)
1.57
(1.00
;2.46
)2.78
(1.79
;4.33
)3.11
(1.73
;5.60
)Hi
p circ
umfer
ence
> 104
cm1.0
0(r
ef.)
1.21
(0.74
;2.00
)1.32
(0.63
;2.78
)1.0
0(r
ef.)
1.30
(0.80
;2.09
)0.85
(0.44
;1.63
)1.0
0(r
ef.)
1.25
(0.89
;1.77
)1.03
(0.63
;1.68
)98
- 104
cm1.2
9(0
.72;2
.32)1
.49(0
.87;2
.54)1
.64(0
.88;3
.07)
1.01
(0.55
;1.88
)1.04
(0.58
;1.89
)1.16
(0.53
;2.56
)1.1
5(0
.75;1
.76)1
.27(0
.85;1
.89)1
.44(0
.88;2
.35)
< 98 c
m2.3
3(1
.27;4
.26)2
.05(1
.16;3
.62)1
.21(0
.51;2
.89)
1.59
(0.91
;2.79
)1.15
(0.66
;2.00
)1.61
(0.81
;3.19
)1.9
0(1
.26;2
.86)1
.52(1
.02;2
.27)1
.44(0
.84;2
.47)
¹) Ad
justed
for a
ge, s
mokin
g stat
us, a
lcoho
l con
sump
tion,
phys
ical a
ctivit
y, ed
ucati
onal
level,
and w
aist c
ircum
feren
ce. W
omen
also
adjus
ted fo
r men
opau
sal s
tatus
.²)
Adjus
ted fo
r age
, smo
king s
tatus
, alco
hol c
onsu
mptio
n, ph
ysica
l acti
vity,
and w
aist c
ircum
feren
ce. W
omen
also
adjus
ted fo
r men
opau
sal s
tatus
and h
ormon
e rep
lacem
ent th
erapy
.*)
RR es
timate
d by C
ox pr
oport
ional
haza
rds re
gress
ion in
DCH
and l
ogist
ic reg
ressio
n in N
HS an
d HPF
S.
wt/w
twt
/var
var/v
ar
Diet,
Can
cer a
nd H
ealth
¹NH
S²Me
taana
lysis
Metaa
nalys
isNF
KB1
NFKB
1NF
KB1
wt/w
twt
/var
Diet,
Can
cer a
nd H
ealth
¹
NFKB
1wt
/wt
wt/va
r
var/v
arwt
/wt
HPFS
²
NFKB
1va
r/var
wt/w
t
wt/va
rva
r/var
NFKB
1wt
/wt
wt/va
rva
r/var
wt/va
rva
r/var

Anthropometry and polymorphisms in inflammatory genes in relation to acute coronary syndrome 17
STUDY III
In the third study we further explored the possible interaction between genetic variation in inflammation and obesity in relation to the risk of ACS. In Study II we investigated a transcription factor complex that regulates several genes, but in Study III we focused on one gene and examined the possible interaction between ge-netic variation in the IL1B gene encoding the key pro-inflammatory cytokine interleukin-1B (IL-1B)(20,21). The IL-1 signaling pathway has been associated with the devel-opment of atherosclerosis and MI(23-27). The aims of this study were to examine the main effects of individual SNPs as well as SNP haplotypes and haplotype combinations in IL1B in relation to inci-dent ACS in a prospective study. Furthermore, we explored the
potential interaction with obesity and the NFKB1 -94 ATTG ins/del polymorphism. The study was based on the DCH cohort, and the analyses were conducted according to the case-cohort design. For the final anal-yses we had 989 cases of incident ACS (755 male cases and 234 female cases). We observed no associations between individual IL1B SNPs, SNP haplotypes, or haplotype combinations and incident ACS (Data shown in Table 3 and 4, Paper III). Likewise, we found no evidence of interaction between haplotypes of IL1B haplotypes and risk of ACS on an additive scale (Table 2).
Table 2. Relative excess risk due to interaction (RERI) with 95% confidence interval in brackets for the associationbetween baseline anthropometric measures, IL1B SNP haplotypes and incident acute coronary syndrome.Median follow up 7.2 years. Diet, Cancer and Health, Denmark, 1993-2003.
Men Women
IL1B SNP haplotype 1 IL1B SNP haplotype 1Variable 0 copy 2 copies Variable 0 copy 2 copiesBody mass index Body mass index
< 25 n/a n/a < 24 n/a n/a25 - 29 n/a 0.62 (-0.64;1.88) 24 - 29 n/a -0.53 (-2.96;1.89)> 29 n/a 1.02 (-1.30;3.33) > 29 n/a -1.21 (-4.31;1.89)
Waist circumference Waist circumference< 93 n/a n/a < 80 n/a n/a93 - 102 n/a 0.23 (-0.97;1.43) 80 - 91 n/a 0.90 (-2.47;4.27)> 102 n/a 1.64 (-1.55;4.83) > 91 n/a -1.08 (-5.23;3.07)
Hip circumference Hip circumference> 103 n/a n/a > 105 n/a n/a98 - 103 n/a -0.82 (-2.54;0.91) 98 - 105 n/a 1.15 (-1.50;3.80)< 98 n/a -0.99 (-2.65;0.66) < 98 n/a 0.79 (-2.17;3.75)
Men Women
IL1B SNP haplotype 2 IL1B SNP haplotype 2Variable 0 copy 2 copies Variable 0 copy 2 copiesBody mass index Body mass index
< 25 n/a n/a < 24 n/a n/a25 - 29 n/a -0.05 (-0.91;0.81) 24 - 29 n/a 0.02 (-1.62;1.66)> 29 n/a -0.46 (-1.95;0.99) > 29 n/a -1.02 (-3.75;1.71)
Waist circumference Waist circumference< 93 n/a n/a < 80 n/a n/a93 - 102 n/a -0.21 (-0.99;0.57) 80 - 91 n/a 1.01 (-0.85;2.86)> 102 n/a -0.23 (-1.64;1.19) > 91 n/a 0.03 (-6.12;6.17)
Hip circumference Hip circumference> 103 n/a n/a > 105 n/a n/a98 - 103 n/a -0.03 (-0.73;0.66) 98 - 105 n/a 0.79 (-0.49;2.07)< 98 n/a 0.01 (-0.72;0.74) < 98 n/a 0.82 (-0.86;2.49)
NFKB1snp(-94 ATTG ins/del)
NFKB1snp(-94 ATTG ins/del)
Wild/Wild n/a n/a Wild/Wild n/a n/aWild/variant n/a -0.14 (-0.96;0.67) Wild/variant n/a -1.96 (-4.50;0.58)Variant/Variant n/a -0.31 (-1.50;0.89) Variant/Variant n/a 0.24 (-2.42;2.89)
Men Women
IL1B SNP haplotype 3 IL1B SNP haplotype 3Variable 0 copy 2 copies Variable 0 copy 2 copiesBody mass index Body mass index
< 25 n/a n/a < 24 n/a n/a25 - 29 n/a -1.26 (-2.63;0.11) 24 - 29 n/a 0.95 (-0.53;2.43)> 29 n/a 0.64 (-1.67;2.94) > 29 n/a 1.85 (-1.11;4.81)
Waist circumference Waist circumference< 93 n/a n/a < 80 n/a n/a93 - 102 n/a -0.45 (-1.74;0.84) 80 - 91 n/a -1.78 (-3.56;0.06)> 102 n/a -0.13 (-1.84;1.58) > 91 n/a 1.08 (-5.79;7.95)
Hip circumference Hip circumference> 103 n/a n/a > 105 n/a n/a98 - 103 n/a -0.41 (-1.46;0.64) 98 - 105 n/a -2.54 (-5.49;0.42)< 98 n/a -0.03 (-1.31;1.25) < 98 n/a -2.39 (-5.41;0.63)
Age used as time axis. All adjusted for smoking status and alcohol consumption.Women also adjusted for menopausal status.Waist circumference and hip circumference mutually adjusted.n/a: Not applicable.

18 Jakob Gerhard Stegger
Discussion
In Study I, we investigated associations between anthropometry and incident ACS defined as MI. The anthropometric measures were the classical indices of general obesity (weight and BMI) and body fat distribution (WC and HC). Furthermore, measures of body composition (BFM, BFP and LBM) obtained by BIA were included. We demonstrated strong positive associations with incident MI for the classical measures of general and abdominal obesity, which was in line with the results of recent meta-analyses(2,56). WC indicates abdominal fat accumulation(3), but the amount of visceral fat may differ among persons with similar WC(57). WC adjusted for BMI has been used as an estimate of visceral fat(58) and has been reported to be positively associated with MI(2). In this adjustment, BMI was an estimate of general obesity, but BMI is also influenced by LBM, and general obesity may be more pre-cisely estimated by BFM. We therefore investigated WC adjusted for BFM as an estimate of visceral adipose tissue and found a slightly stronger positive association with MI compared to WC not adjusted for other anthropometric measures. However, the associ-ation was not as strong as WC adjusted for HC, indicating that the latter may be a better measure for the adverse effect of abdominal obesity regarding ACS risk. Furthermore, the interpretation of WC adjusted for a measure of general obesity like BMI or BFM is diffi-cult, i.e. for an equal BMI a larger WC results in the HC being small-er, and then the exposure could be either a larger WC or a smaller HC. The quest for precise, easy to use, and cheap anthropometric measures has been long, and in their 1997 review, Williams et al.(8) describe the pros and cons of the many different anthropo-metric measurements which have been used during the last half a century. They concluded that body weight and skin fold measure-ment were poorly associated to ACS, and skin fold measurement was susceptible to inter- and intra-observer variability. Further-more, they stated that BMI was moderately associated with ACS, but the waist to hip ratio (WHR) was found to be more strongly associated. Canoy et al(2) found a positive association with ACS for BMI, WC and WHR and a negative association between HC and ACS in the Norfolk cohort of the EPIC study. They concluded that the association was greater and more consistent for WHR. The INTERHEART Study(1) found that abdominal obesity meas-ured as WHR explained 20% of population attributable risk for MI. In their original work, Yusuf et al. examined both BMI and WHR and found that BMI was significantly associated with the occur-rence of MI, but the association became non-significant when WHR was included in a multivariate analysis. On the other hand WHR retained its significance even after multivariate adjustment includ-ing BMI and was therefore chosen as a marker of abdominal adi-posity. The associations for different indices of adiposity (BMI, WC, HC, and WHR) were further examined in an INTERHEART sub-study(59). The authors concluded that BMI had the weakest positive associa-tion with MI, WC was more strongly associated, and WHR had the strongest association. Again, HC was negatively associated with MI.
Furthermore, the authors discussed that some of the limitations of these indices were their lack of ability to distinguish between LBM and fat, and the fact that it is unknown whether HC is a measure of subcutaneous fat and/or of muscle mass. In previous studies the strongest association between anthro-pometry and MI/ACS was observed for WHR. However, the strength of association is not an indication of how well the variable predicts the outcome. A comparison of the strength of the associa-tions for different anthropometric measures may thus not be of particular interest. We did not use WHR as the WHR is ambiguous, i.e. a WHR of 1.0 may be due to a WC and HC of 70, or a WC and HC of 110, and those two scenarios are far from identical. Furthermore, WHR assumes that HC counteracts all the adverse effects of WC, i.e. a 10% increase in both WC and HC equals an unchanged WHR and thereby unchanged risk of ACS, i.e. gluteofemoral fat counteracts abdominal fat. This may partly be true regarding the lipolytic activi-ty of abdominal fat, whereas gluteofemoral fat may function as a buffer removing the free fatty acids from the circulation. However, the visceral fat is releasing the free fatty acids directly into the portal circulation and the hepatic effect of the free fatty acids– atherogenic lipid profile and decreased insulin-clearance(5) – can-not be counterbalanced completely by the subcutaneous fat. Fur-thermore, the release of adipocyte-derived proteins varies exten-sively between visceral and subcutaneous fat, i.e. visceral fat re-leases more IL-6, PAI-1, resistin, angiotensinogen, and angiotensin-ogen converting enzyme, whereas subcutaneous fat produces more leptin and adiponectin(5,9,30,31,60). Thus, WHR may not be a good measure for abdominal obesity, but it may be a good measure of body fat distribution. If the body fat distribution is determined by an underlying (unknown) factor that also plays an important role in the development of adipose dysfunction (adiposopathy), then WHR could be seen as a measure of adipose dysfunction, and thus a measure for adipose tissue-related ACS risk. This could explain the consistent findings for WHR in relation to ACS risk, but further studies are warranted to investi-gate this hypothesis. BFM adjusted for height showed a positive association with ACS, but after additional adjustment for WC, BFM was not signifi-cantly associated with ACS. This was in contrast to WC that re-mained significantly associated with ACS after adjustment for BFM. This indicats that BFM provided no additional information to WC with respect to the risk of incident MI. BFP is a measure of general obesity like BMI, but while high muscle mass would lead to a high BMI and thereby give a false indication of a higher risk of ACS, high muscle mass diminishes BFP, thereby indicating a lower risk. Thus BFP held information on body composition, but it did not provide any information on body fat distribution. Besides alternative measures of obesity like BFM and BFP, BIA also provided a measure for LBM. We hypothesized that LBM, as a surrogate for muscle mass, would be negatively associated with ACS risk, but on the contrary LBM was monotonously positively associated with incident MI in both men and women. However,

Anthropometry and polymorphisms in inflammatory genes in relation to acute coronary syndrome 19
when we also adjusted for BFM and WC as measures of total body fat and body fat distribution, a low LBM was associated with a higher risk of incident ACS. However, the negative association was not consistent, and there was no protective effect of a high LBM. The higher risk of ACS associated with low LBM suggested that the adverse effect of a small HC, at least partly, could be explained by muscle mass. The conclusion of Study I was that abdominal and gluteofemo-ral adipose tissues are different and discrimination between them is important in relation to ACS risk. As estimates of obesity achieved by BIA did not seem to add information to the classical anthropometric measures, we used BMI as a measure for general obesity, WC, and HC mutually adjusted as measures for abdominal (visceral) and gluteofemoral (subcutaneous) obesity in Study II and Study III. The association between obesity and ACS is strong, but the physiological pathways through which obesity results in ACS are complex. Obesity can be seen as an underlying risk factor for ACS raising the risk through other risk factors. However, in a review, Bogers in 2007(25) concluded that adjusting the association be-tween obesity measured as BMI and ACS for intermediary factors like hypercholesterolemia and high blood pressure only diminished the association by 45% indicating that obesity is a risk factor per se. This is in line with the findings of our studies, where adjustment for possible common causes of obesity and ACS like total energy in-take and physical activity as well as possible intermediate variables as hypertension, hypercholesterolemia, and diabetes mellitus had only minor influence on the associations. Furthermore, the abun-dant secretion of proteins makes adipose tissue an active player during the development of atherosclerosis. In order to investigate inflammation as a pathway between obesity and ACS we explored the possible interaction between obesity and the NFKB1-94ins/delATTG promoter polymorphism in Study II. The polymorphism leads to lower transcript levels of the NF-κB p50 subunit and thus affect both the availability of the anti-inflammatory p50/p50 NF-κB homodimer and the pro-inflammatory p50/p65 NF-κB heterodimer(19,32). Therefore, the effect of polymorphisms may vary between different tissues. We hypothesized that in participants with a high HC, the net effect of the NFKB1-94ins/delATTG promoter polymorphism may be a preferential depletion of anti-inflammatory cytokines and a reduction in the protective effect of gluteofemoral fat deposits. Likewise, the combined effect of abdominal obesity and homozy-gote variant carrier status may be more than additive due to an excess secretion of pro-inflammatory cytokines as well as an in-creased inflammatory response to cytokines in atherosclerotic plaques. Our results did show a tendency of positive interaction for abdominal obesity and negative interaction for gluteofemoral obesity and thus support the above mentioned biological hypothe-sis; however, the potential interaction between genetic variation in NFKB1 and obesity was not substantial and did not seem to be of clinical importance. In Study III we further explored the inflammatory link between obesity and ACS, as we investigated the possible interaction be-tween individual SNPs in and SNP haplotypes of the promoter region of IL1B and incident ACS. However, there was no evidence that the investigated SNP haplotypes modified the effect of obesity on the risk of ACS. We also investigated the main effects, but found no significant associations between individual SNPs or SNP haplo-types in the promoter region of the IL1B gene and incident ACS.
Confidence limits show that it is quite unlikely that a possible true clinically important association could have given rise to the esti-mates found. The biological effect of the investigated SNPs on IL1B expres-sion(36) and release of IL-1B(25) is well established. The -511T SNP (which in our cohort was in complete linkage disequilibrium with the investigated C-31T(37)) and haplotypes containing this SNP have been associated with a relatively low risk of myocardial in-farction at young age(25,35), but our results suggest that IL-1B may have a limited role in the development of ACS in men and women above the age of 50 years. Strengths and limitations of the individual studies are men-tioned in the articles, and only general issues will be discussed here. Due to the high level of data ascertainment in DCH only few participants were excluded because of missing variables. However, as we investigated incident ACS, we also excluded participants with prevalent ACS, and because the participants were at least 50 years old at inclusion, this amounted to a significant proportion (in Study I we excluded 900 participants due to prevalent ACS). The exclu-sion was necessary for several reasons. Prevalent ACS could have influenced the participants’ lifestyle including several parameters that could have affected anthropometry and thus produced re-verse causation. Furthermore, participants with prevalent ACS would receive several medications that modify future risk of ACS. Finally, only persons who survived their ACS event could later become eligible for participation in our cohort. The exclusions may have influenced our results, as we cannot rule out a “healthy par-ticipant effect” since participants who had “survived” until inclu-sion without sustaining ACS might have had a reduced susceptibil-ity to the investigated variables. In all our studies we used incident ACS as output. ACS was considered the result of the rupture of a vulnerable atherosclerotic plaque, but atherosclerosis may also lead to stroke and peripheral artery disease. The inflammatory mechanisms leading to athero-sclerosis are mainly the same in arteries in different regions, and thus, exposures leading to increased atherosclerosis in coronary arteries may also lead to a higher incidence of strokes and periph-eral artery disease. Thus, death from stroke or peripheral artery disease was a competing risk. If the examined exposures also lead to a higher risk of fatal stroke and/or peripheral artery disease, then we would underestimate the effect of the exposures on the risk of ACS. This is because; more participants would experience death from these other atherosclerotic diseases and thus not live long enough to develop ACS. Consequently, to investigate the full effect of our exposures on the risk of plaque rupture, it might have been more correct to have used a composite endpoint encompass-ing ACS, stroke, and peripheral artery disease. Furthermore, if the atherosclerotic plaque was stable, it could progress without rupture to a size where it limited the blood flow in the coronary artery. This would have led to stable angina pector-is, and in addition to possible direct coronary intervention the patient would have received medical treatment that would have modified the risk of ACS in the patient. We did not include stable angina pectoris as an outcome as the biology leading to a stable plaques and vulnerable plaques may be different.

20 Jakob Gerhard Stegger
Main conclusions
In the present thesis we investigated the association with incident ACS for different anthropometric measures including measures of body composition obtained by BIA that had not previously been investigated in large prospective studies. The anthropometric measures of body fatness obtained by BIA (BFM and BFP) were positively associated with incident ACS. The associations were statistically significant and consistent in both men and women and the results emphasize the importance of obesity in the develop-ment of ACS. However, the endocrine differences between abdominal and gluteofemoral adipose tissues make obesity an ambiguous con-cept, and in a biologically perspective abdominal and gluteofemo-ral obesity should be set apart. This was confirmed by the opposite associations for WC and HC with incident ACS. The lacking ability of BIA to describe body fat distribution suggests that WC and HC may be better estimates of obesity in relation to ACS. We furthermore explored the association between LBM and ACS, and we hypothesized that LBM would be negatively associat-ed with ACS. Our results indicate that low LBM may indeed be associated with a higher risk of incident ACS (especially in women), but there was no clear association between high LBM and ACS. Thus, LBM does not seem to play an important role in the devel-opment of atherosclerosis and ACS. The inflammatory properties of adipose tissues and the im-portant role of inflammation in the development of the atheroscle-rotic plaque suggest that inflammation may be an important path-way between obesity and ACS. Another aim of the thesis was to
explore this possible pathway by investigating possible interaction between obesity and genetic variation in two candidate genes encoding key proteins in the inflammatory system. We hypothe-sized that altered expression of the candidate genes due to poly-morphisms would modify the effect of obesity on ACS risk accord-ing to body fat distribution. This first candidate gene was NFKB1 and we investigated the -94ins/delATTG promoter polymorphism. The variant allele had been associated to high CRP and inflammatory diseases including ACS. We observed a tendency towards positive interaction for abdominal obesity and negative interaction for gluteofemoral obesity with ACS. However, the magnitude of the interaction was small and not statically significant. IL1B was the second candidate gene, and we investigated all functional SNPs as well as SNP haplotypes in the promoter region. We observed no association with ACS for the main effect of any SNP or haplotype. Likewise, we found no interaction between SNP haplotypes and general, abdominal, or gluteofemoral obesity. The functionality of all investigated polymorphisms was well established and the conclusion could be that the lack of interaction between any of the polymorphisms and obesity indicates that neither p50 subunit-dependent NF-κB transcription factors nor IL-1B is important in the possible inflammatory pathway between obesity and ACS. However, it was more likely that the pathways between obesity and ACS are complex, and that none of the inves-tigated factors by themselves significantly modifies the association between obesity and ACS.

Anthropometry and polymorphisms in inflammatory genes in relation to acute coronary syndrome 21
Perspectives
The acute treatment of ACS and subsequent secondary prophylaxis in order to reduce the risk of recurrent ACS has improved markedly in the last two decades. However, there remains a high risk of irreversible invalidating sequelae (e.g. heart failure) or even death associated to a first time ACS event and better primary prevention is still needed. The associations between classic anthropometric measures like BMI, WC and HC and ACS are well established, and our studies further support the hypothesis that the adverse or protective effects of general, abdominal and gluteofemoral obesity are well described by these measures. However, it may be that the endo-crine properties of the different adipose tissues are more im-portant than amount of adipose tissue and further studies are warranted to investigate the patho-physiology of adipose tissue dysfunction (adiposopathy). Especially it would be interesting to investigate WHR as a measure of adipose tissue dysfunction. Furthermore, a better understanding of the pathways between obesity and disease including ACS is crucial. Identification of im-portant factors in this association would allow us to institute better preventive measures. We explored the association for two important factors in the inflammatory system. However, the inflammatory system is ex-tremely complex and studies of other factors as well as further studies of NF-κB and IL-1B are warranted to clarify the biological implications of genetic variations. Despite our incomplete understanding of the many implications of obesity, the increased morbidity and premature mortality asso-ciated with obesity cannot be questioned, and prevention of the evolving obesity epidemic is of outmost importance.

22 Jakob Gerhard Stegger
English summary
Obesity is a risk factor for acute coronary syndrome ACS, and in Study I, we investigated the associations between detailed anthro-pometric measures and incident ACS. Inflammation plays a major role in the development of ACS and may be an important pathway between obesity and ACS. In Study II and Study III, we investigated the possible interaction between different measures of obesity and polymorphisms in two major inflammatory genes. In the first Study I, we investigated the associations for classical anthropometric measures like body mass index (BMI), waist cir-cumference (WC), and hip circumference (HC), as well as bioelec-trical impedance analyses (BIA) of body composition including body fat mass (BFM), body fat percentage, (BFP) and lean body mass (LBM). The study was conducted in the Danish prospective study Diet, Cancer and Health (DCH) encompassing 27,148 men and 29,863 women, aged 50 to 64 year at baseline including 2,028 cases of incident ACS (mainly myocardial infarction). We found that general and abdominal obesity was positively associated and glu-teofemoral obesity negatively associated with ACS. Estimates of obesity achieved by BIA did not add additional information to the classical anthropometric measures, whereas both high and low LBM may be positively associated with ACS. In the Study II, we investigated the possible interaction be-tween obesity and the NFKB1 -94ins/delATTG polymorphism in the promoter region of the NFKB1 gene. The NF-κB transcription fac-tor family regulates several genes encoding pro-inflammatory and anti-inflammatory proteins in adipose tissues and in atherosclerot-ic plaques, and the variant allele carrying the deletion has been associated with the risk of several inflammatory diseases including ACS. The study was conducted as a case-cohort study in DCH and
as case-control studies in the two US-based cohorts; the Nurses’ Health Study and the Health Professionals Follow-up Study. We conducted sex-stratified analyses that included 1,202 male and 708 female cases of incident ACS. We observed no substantial interac-tion between obesity and the NFKB1 -94ins/delATTG promoter polymorphism in relation to the risk of incident ACS. In the Study III, we investigated the associations for all func-tional single nucleotide polymorphisms (SNPs) and SNP haplotypes in the promoter region of IL1B gene encoding interleukin-1B (IL-1B) in relation to incident ACS. Furthermore, we investigated the pos-sible interaction between SNP haplotypes and obesity in relation to ACS. IL-1B is a key pro-inflammatory cytokine that has been associ-ated with the development of atherosclerosis and myocardial infarction. The study was conducted as a case-cohort study in DCH, and for the analyses we had 755 male and 234 female cases. Indi-vidual IL1B SNPs, SNP haplotypes, or haplotype combinations were not significantly associated with incident acute coronary syndrome, and, likewise, we found no evidence of interaction between haplo-types of IL1B haplotypes and risk factors for ACS on an additive scale. In conclusion, obesity was a risk factor for ACS, but even though inflammation may be an important pathway between obesity and ACS, we found no substantial interaction between obesity and genetic variation in the investigated genes encoding key inflamma-tory proteins. Further studies are needed to provide a better understanding of the pathways between obesity and disease including ACS. Identi-fication of important factors in this association would allow us to institute better preventive measures.

Anthropometry and polymorphisms in inflammatory genes in relation to acute coronary syndrome 23
Dansk resume
Fedme er en betydende risikofaktor for akut koronart syndrom (AKS), og i Studie I i denne tese undersøgte vi sammenhængen mellem detaljerede mål for kropsbygning og kropssammensætning og førstegangstilfælde af AKS. Inflammation spiller en stor rolle i udviklingen af den åreforkalkning, der ligger til grund for AKS, og kan være et vigtigt bindeled mellem fedme og AKS. I Studie II og Studie III undersøgte vi derfor mulig interaktion mellem fedme og genetisk variation i to gener, der hver især koder for proteiner med markant inflammatorisk betydning. I Studie I undersøgte vi sammenhæng mellem klassiske mål for fedme og fedtfordeling såsom body mass index (BMI), livvidde (WC) og hoftevidde (HC) samt mål for fedme og kropssammensæt-ning udledt ved bioimpedansmålinger (BIA) såsom total kropsfedt (BFM), fedtprocent (BFP) og fedtfri masse (LBM). I studiet brugte vi data fra kohorten Kost, Kræft og Helbred (KKH), der indeholder data fra 27.148 mænd og 29.863 kvinder i alderen 50-64 år ved indgang i studiet. I løbet af 11,9 års opfølgning identificerede vi 2028 nye cases af førstegangs AKS. Resultaterne viste, at generel fedme målt ved BMI og livvidde var positivt associeret med risiko for AKS, hvorimod hoftevidde var negativt associeret med AKS-risiko. De detaljerede mål for kropssammensætning udledt ved BIA syntes ikke at bidrage med yderligere information end de klassiske mål for fedtfordeling i relation til AKS. Overraskende synes både høj og lav LBM at være positivt associeret med risikoen for AKS. I Studie II undersøgte vi den mulige interaktion mellem fedme og NFKB1 -94ATTG polymorfien lokaliseret i promotor regionen af NFKB1-genet. NF-κB er en transkriptionsfamilie, der regulerer mange pro-inflammatoriske og en del anti-inflammatoriske gener, og variant allelen af NFKB1-94ATTG polymorfien har været associe-ret med flere inflammatoriske sygdomme herunder AKS. Dette
studie blev udført med data fra KKH samt data fra de to amerikan-ske befolkningsundersøgelser Nurses’ Health Study og Health Professionals Follow-up Study. Vi udførte kønsopdelte analyser blandt 1202 mandlige og 708 kvindelige cases. Vi fandt ingen bety-dende interaktion mellem fedme og NFKB1-94ATTG polymorfien. I Studie III undersøgte vi sammenhængen mellem alle funktio-nelle enkeltnukleotidpolymorfier (SNP) og SNP-haplotyper i IL1B-genet, der koder for interleukin-1B (IL-1B) og AKS. Desuden under-søgte vi en mulig interaktion mellem SNP-haplotyper og fedme i relation til AKS. IL-1B er et vigtigt pro-inflammatorisk protein, der er vist at være betydende for udvikling af åreforkalkning og blod-propper i hjertets kranspulsårer. Studiet blev udført som et case-kohorte design på baggrund af data fra KKH, og til de endelige analyser havde vi 755 mandlige og 234 kvindelige cases. Ingen af de enkelte polymorfier eller haplotyperne var associeret med AKS, og der var ingen tegn på interaktion mellem SNP-haplotyperne og AKS. Vi kan på baggrund af vores studier konkludere, at fedme var en risikofaktor for førstegangstilfælde af AKS, men selvom inflamma-tion kan være et betydende bindeled mellem fedme og AKS, fandt vi ingen betydende interaktion mellem fedme og genetisk variation i de undersøgte gener kodende for betydende inflammatoriske proteiner. Der er fortsat behov for yderligere studier, der kan give en bedre forståelse for sammenhængen mellem fedme og AKS. Identi-fikation vigtige faktorer i denne association kunne give mulighed for bedre præventive tiltag.

24 Jakob Gerhard Stegger
References
(1) Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, et al. Effect of potentially modifiable risk factors associated with myocardial in-farction in 52 countries (the INTERHEART study): case-control study. Lancet 2004 Sep 11-17;364(9438):937-952.
(2) Canoy D. Distribution of body fat and risk of coronary heart disease in men and women. Curr Opin Cardiol 2008 Nov;23(6):591-598.
(3) Chan DC, Watts GF, Barrett PH, Burke V. Waist circumference, waist-to-hip ratio and body mass index as predictors of adipose tissue com-partments in men. QJM 2003 Jun;96(6):441-447.
(4) Grundy SM. Obesity, metabolic syndrome, and cardiovascular disease. J Clin Endocrinol Metab 2004 Jun;89(6):2595-2600.
(5) Hajer GR, van Haeften TW, Visseren FL. Adipose tissue dysfunction in obesity, diabetes, and vascular diseases. Eur Heart J 2008 Dec;29(24):2959-2971.
(6) Berghofer A, Pischon T, Reinhold T, Apovian CM, Sharma AM, Willich SN. Obesity prevalence from a European perspective: a systematic re-view. BMC Public Health 2008 Jun 5;8:200.
(7) Obesity and overweight. 2010; Available at: http://www.who.int/dietphysicalactivity/publications/facts/obesity/en/.
(8) Williams SR, Jones E, Bell W, Davies B, Bourne MW. Body habitus and coronary heart disease in men. A review with reference to methods of body habitus assessment. Eur Heart J 1997 Mar;18(3):376-393.
(9) Kershaw EE, Flier JS. Adipose tissue as an endocrine organ. J Clin Endocrinol Metab 2004 Jun;89(6):2548-2556.
(10) Ross R. Atherosclerosis--an inflammatory disease. N Engl J Med 1999 Jan 14;340(2):115-126.
(11) Ridker PM, Morrow DA. C-reactive protein, inflammation, and coro-nary risk. Cardiol Clin 2003 Aug;21(3):315-325.
(12) Larsson B, Svardsudd K, Welin L, Wilhelmsen L, Bjorntorp P, Tibblin G. Abdominal adipose tissue distribution, obesity, and risk of cardiovas-cular disease and death: 13 year follow up of participants in the study of men born in 1913. Br Med J (Clin Res Ed) 1984 May 12;288(6428):1401-1404.
(13) Lapidus L, Bengtsson C, Larsson B, Pennert K, Rybo E, Sjostrom L. Distribution of adipose tissue and risk of cardiovascular disease and death: a 12 year follow up of participants in the population study of women in Gothenburg, Sweden. Br Med J (Clin Res Ed) 1984 Nov 10;289(6454):1257-1261.
(14) Canoy D, Boekholdt SM, Wareham N, Luben R, Welch A, Bingham S, et al. Body fat distribution and risk of coronary heart disease in men and women in the European Prospective Investigation Into Cancer and Nu-trition in Norfolk cohort: a population-based prospective study. Circu-lation 2007 Dec 18;116(25):2933-2943.
(15) Parker ED, Pereira MA, Stevens J, Folsom AR. Association of hip cir-cumference with incident diabetes and coronary heart disease: the Atherosclerosis Risk in Communities study. Am J Epidemiol 2009 Apr 1;169(7):837-847.
(16) Heitmann BL, Erikson H, Ellsinger BM, Mikkelsen KL, Larsson B. Mortal-ity associated with body fat, fat-free mass and body mass index among 60-year-old swedish men-a 22-year follow-up. The study of men born in 1913. Int J Obes Relat Metab Disord 2000 Jan;24(1):33-37.
(17) de Winther MP, Kanters E, Kraal G, Hofker MH. Nuclear factor kappaB signaling in atherogenesis. Arterioscler Thromb Vasc Biol 2005 May;25(5):904-914.
(18) Pereira SG, Oakley F. Nuclear factor-kappaB1: regulation and function. Int J Biochem Cell Biol 2008;40(8):1425-1430.
(19) Cao S, Zhang X, Edwards JP, Mosser DM. NF-kappaB1 (p50) homodi-mers differentially regulate pro- and anti-inflammatory cytokines in macrophages. J Biol Chem 2006 Sep 8;281(36):26041-26050.
(20) Dinarello CA. Immunological and inflammatory functions of the inter-leukin-1 family. Annu Rev Immunol 2009;27:519-550.
(21) Dinarello CA. A clinical perspective of IL-1beta as the gatekeeper of inflammation. Eur J Immunol 2011 May;41(5):1203-1217.
(22) Vogel U, Jensen MK, Due KM, Rimm EB, Wallin H, Nielsen MR, et al. The NFKB1 ATTG ins/del polymorphism and risk of coronary heart dis-ease in three independent populations. Atherosclerosis 2011 Jun 17.
(23) Chamberlain J, Francis S, Brookes Z, Shaw G, Graham D, Alp NJ, et al. Interleukin-1 regulates multiple atherogenic mechanisms in response to fat feeding. PLoS One 2009;4(4):e5073.
(24) Bhaskar V, Yin J, Mirza AM, Phan D, Vanegas S, Issafras H, et al. Mono-clonal antibodies targeting IL-1 beta reduce biomarkers of atheroscle-rosis in vitro and inhibit atherosclerotic plaque formation in Apolipo-protein E-deficient mice. Atherosclerosis 2011 Jun;216(2):313-320.
(25) Iacoviello L, Di Castelnuovo A, Gattone M, Pezzini A, Assanelli D, Lorenzet R, et al. Polymorphisms of the interleukin-1beta gene affect the risk of myocardial infarction and ischemic stroke at young age and the response of mononuclear cells to stimulation in vitro. Arterioscler Thromb Vasc Biol 2005 Jan;25(1):222-227.
(26) Kirii H, Niwa T, Yamada Y, Wada H, Saito K, Iwakura Y, et al. Lack of interleukin-1beta decreases the severity of atherosclerosis in ApoE-deficient mice. Arterioscler Thromb Vasc Biol 2003 Apr 1;23(4):656-660.
(27) Olofsson PS, Sheikine Y, Jatta K, Ghaderi M, Samnegard A, Eriksson P, et al. A functional interleukin-1 receptor antagonist polymorphism in-fluences atherosclerosis development. The interleukin-1beta:interleukin-1 receptor antagonist balance in atherosclerosis. Circ J 2009 Aug;73(8):1531-1536.
(28) Davies MJ, Thomas AC. Plaque fissuring--the cause of acute myocardi-al infarction, sudden ischaemic death, and crescendo angina. Br Heart J 1985 Apr;53(4):363-373.
(29) Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med 2005 Apr 21;352(16):1685-1695.
(30) Bays HE. Adiposopathy is "sick fat" a cardiovascular disease? J Am Coll Cardiol 2011 Jun 21;57(25):2461-2473.
(31) Hamdy O, Porramatikul S, Al-Ozairi E. Metabolic obesity: the paradox between visceral and subcutaneous fat. Curr Diabetes Rev 2006 Nov;2(4):367-373.
(32) Karban AS, Okazaki T, Panhuysen CI, Gallegos T, Potter JJ, Bailey-Wilson JE, et al. Functional annotation of a novel NFKB1 promoter polymorphism that increases risk for ulcerative colitis. Hum Mol Genet 2004 Jan 1;13(1):35-45.
(33) Van der Heiden K, Cuhlmann S, Luong le A, Zakkar M, Evans PC. Role of nuclear factor kappaB in cardiovascular health and disease. Clin Sci (Lond) 2010 Feb 23;118(10):593-605.
(34) Vogel U, Jensen MK, Due KM, Rimm EB, Wallin H, Nielsen MR, et al. The NFKB1 ATTG ins/del polymorphism and risk of coronary heart dis-ease in three independent populations. Atherosclerosis 2011 Jun 17.
(35) Latella MC, de Gaetano M, Di Castelnuovo A, Napoleone E, Lorenzet R, Gattone M, et al. Interleukin 1 gene cluster, myocardial infarction at young age and inflammatory response of human mononuclear cells. Immunol Invest 2009;38(3-4):203-219.
(36) Chen H, Wilkins LM, Aziz N, Cannings C, Wyllie DH, Bingle C, et al. Single nucleotide polymorphisms in the human interleukin-1B gene af-fect transcription according to haplotype context. Hum Mol Genet 2006 Feb 15;15(4):519-529.

Anthropometry and polymorphisms in inflammatory genes in relation to acute coronary syndrome 25
(37) Vangsted AJ, Klausen TW, Abildgaard N, Andersen NF, Gimsing P, Gregersen H, et al. Single nucleotide polymorphisms in the promoter region of the IL1B gene influence outcome in multiple myeloma pa-tients treated with high-dose chemotherapy independently of relapse treatment with thalidomide and bortezomib. Ann Hematol 2011 Feb 24.
(38) Tjonneland A, Olsen A, Boll K, Stripp C, Christensen J, Engholm G, et al. Study design, exposure variables, and socioeconomic determinants of participation in Diet, Cancer and Health: a population-based prospec-tive cohort study of 57,053 men and women in Denmark. Scand J Pub-lic Health 2007;35(4):432-441.
(39) Andersen TF, Madsen M, Jorgensen J, Mellemkjoer L, Olsen JH. The Danish National Hospital Register. A valuable source of data for mod-ern health sciences. Dan Med Bull 1999 Jun;46(3):263-268.
(40) Joensen AM, Jensen MK, Overvad K, Dethlefsen C, Schmidt E, Rasmus-sen L, et al. Predictive values of acute coronary syndrome discharge diagnoses differed in the Danish National Patient Registry. J Clin Epi-demiol 2009 Feb;62(2):188-194.
(41) Heitmann BL. Prediction of body water and fat in adult Danes from measurement of electrical impedance. A validation study. Int J Obes 1990;14:789-802.
(42) Kyle UG, Piccoli A, Pichard C. Body composition measurements: inter-pretation finally made easy for clinical use. Curr Opin Clin Nutr Metab Care 2003 Jul;6(4):387-393.
(43) Vangsted AJ, Klausen TW, Ruminski W, Gimsing P, Andersen NF, Gang AO, et al. The polymorphism IL-1beta T-31C is associated with a longer overall survival in patients with multiple myeloma undergoing auto-SCT. Bone Marrow Transplant 2009 Apr;43(7):539-545.
(44) Vogel U, Christensen J, Dybdahl M, Friis S, Hansen RD, Wallin H, et al. Prospective study of interaction between alcohol, NSAID use and pol-ymorphisms in genes involved in the inflammatory response in rela-tion to risk of colorectal cancer. Mutat Res 2007 Nov 1;624(1-2):88-100.
(45) Vogel U, Christensen J, Wallin H, Friis S, Nexo BA, Raaschou-Nielsen O, et al. Polymorphisms in genes involved in the inflammatory response and interaction with NSAID use or smoking in relation to lung cancer risk in a prospective study. Mutat Res 2008 Mar 1;639(1-2):89-100.
(46) Vangsted AJ, Klausen TW, Gimsing P, Andersen NF, Abildgaard N, Gregersen H, et al. A polymorphism in NFKB1 is associated with im-proved effect of interferon-{alpha} maintenance treatment of patients with multiple myeloma after high-dose treatment with stem cell sup-port. Haematologica 2009 Sep;94(9):1274-1281.
(47) Rimm EB, Giovannucci EL, Willett WC, Colditz GA, Ascherio A, Rosner B, et al. Prospective study of alcohol consumption and risk of coronary disease in men. Lancet 1991 Aug 24;338(8765):464-468.
(48) Jensen MK, Rimm EB, Mukamal KJ, Edmondson AC, Rader DJ, Vogel U, et al. The T111I variant in the endothelial lipase gene and risk of coro-nary heart disease in three independent populations. Eur Heart J 2009 Jul;30(13):1584-1589.
(49) Rimm EB, Giovannucci EL, Stampfer MJ, Colditz GA, Litin LB, Willett WC. Reproducibility and validity of an expanded self-administered semiquantitative food frequency questionnaire among male health professionals. Am J Epidemiol 1992 May 15;135(10):1114-26; discus-sion 1127-36.
(50) Rimm EB, Stampfer MJ, Colditz GA, Chute CG, Litin LB, Willett WC. Validity of self-reported waist and hip circumferences in men and women. Epidemiology 1990 Nov;1(6):466-473.
(51) Jensen MK, Mukamal KJ, Overvad K, Rimm EB. Alcohol consumption, TaqIB polymorphism of cholesteryl ester transfer protein, high-density lipoprotein cholesterol, and risk of coronary heart disease in men and women. Eur Heart J 2008 Jan;29(1):104-112.
(52) Korn EL, Graubard BI, Midthune D. Time-to-event analysis of longitu-dinal follow-up of a survey: choice of the time-scale. Am J Epidemiol 1997 Jan 1;145(1):72-80.
(53) Kalbfleisch JD, Lawless JF. Likelihood analysis of multi-state models for disease incidence and mortality. Stat Med 1988 Jan-Feb;7(1-2):149-160.
(54) Harrel J, F.E. Regression modeling strategies. United States of Ameri-ca: Springer-Verlag New York, Inc; 2001.
(55) Rothman KJ GS. Modern Epidemiology. 2nd ed. Philadelphia: Lip-pincott Williams and Wilkins; 1998.
(56) Bogers RP, Bemelmans WJ, Hoogenveen RT, Boshuizen HC, Woodward M, Knekt P, et al. Association of overweight with increased risk of cor-onary heart disease partly independent of blood pressure and choles-terol levels: a meta-analysis of 21 cohort studies including more than 300 000 persons. Arch Intern Med 2007 Sep 10;167(16):1720-1728.
(57) Fujimoto WY, Bergstrom RW, Boyko EJ, Chen KW, Leonetti DL, Newell-Morris L, et al. Visceral adiposity and incident coronary heart disease in Japanese-American men. The 10-year follow-up results of the Seat-tle Japanese-American Community Diabetes Study. Diabetes Care 1999 Nov;22(11):1808-1812.
(58) Janssen I, Heymsfield SB, Allison DB, Kotler DP, Ross R. Body mass index and waist circumference independently contribute to the pre-diction of nonabdominal, abdominal subcutaneous, and visceral fat. Am J Clin Nutr 2002 Apr;75(4):683-688.
(59) Yusuf S, Hawken S, Ounpuu S, Bautista L, Franzosi MG, Commerford P, et al. Obesity and the risk of myocardial infarction in 27,000 partici-pants from 52 countries: a case-control study. Lancet 2005 Nov 5;366(9497):1640-1649.
(60) Iwaki M, Matsuda M, Maeda N, Funahashi T, Matsuzawa Y, Makishima M, et al. Induction of adiponectin, a fat-derived antidiabetic and anti-atherogenic factor, by nuclear receptors. Diabetes 2003 Jul;52(7):1655-1663.

26 Jakob Gerhard Stegger
Paper I

Anthropometry and polymorphisms in inflammatory genes in relation to acute coronary syndrome 27
Paper II
Interaction between Obesity and the NFKB1 -94ins/delATTG Promoter Polymorphism in Relation to Incident Acute Coronary Syndrome: a Follow-up Study in Three Independent Cohorts
Jakob Gerhard Stegger MD1, Erik Berg Schmidt DMSc1, Tina Landsvig Berentzen PhD2, Anne Tjønneland DMSc3, Ulla Vogel PhD4, Eric Rimm ScD5, Thorkild I. A. Sørensen DMSc2, Kim Over-vad PhD1,6, Majken K Jensen PhD1,7
1Department of Cardiology, Center for Cardiovascular Research, Aalborg Hospital, Aarhus University Hospital, Aalborg, Denmark 2Institute of Preventive Medicine, University of Copenhagen, Copenhagen, Denmark 3Institute of Cancer Epidemiology, Danish Cancer Society, Co-penhagen, Denmark 4National Research Centre for the Working Environment, Co-penhagen, Denmark 5Departments of Nutrition and Epidemiology, Harvard School of Public Health, Boston, MA, USA 6Section of Epidemiology, Department of Public Health, Aarhus University, Aarhus, Denmark 7Department of Nutrition, Harvard School of Public Health, Boston, MA, USA Correspondence to: Jakob Gerhard Stegger, Department of Cardiology, Center for Cardiovascular Research, Aalborg Hospital, Aarhus University Hospital, Sdr. Skovvej 15, DK-9000 Aalborg, Denmark, Tel.: +45 9932 1111, email address: [email protected]
ABSTRACT Introduction The NF-κB transcription factor family regulates several genes encoding pro-inflammatory and anti-inflammatory proteins in adipose tissues and in atherosclerotic plaques. The deletion variant allele of the NFKB1 -94ins/delATTG promoter polymor-phism leads to lower transcript levels of the p50 subunit, and has been associated with the risk of several inflammatory dis-eases including coronary heart disease. The objective of this study was to explore the potential inter-action between the NFKB1 -94ins/delATTG promoter polymor-phism and general, abdominal, and gluteofemoral obesity in relation to the risk of incident acute coronary syndrome (ACS) in three large independent cohorts. Methods and Results The analyses were conducted in the Danish prospective study Diet, Cancer and Health and the two US-based cohorts; Nurses’ Health Study and Health Professionals Follow-up Study. We conducted sex-stratified analyses that included 1202 male and 708 female cases of incident ACS. We observed a positive association for general and ab-dominal obesity with risk of incident ACS, independent of geno-type in both sexes. Gluteofemoral obesity was negatively associ-ated with ACS risk in women independent of genotype, whereas there was no clear association for men. We calculated the rela-tive excess risk due to interaction (RERI) and observed a tenden-cy towards an excess risk among participants jointly exposed to general or abdominal obesity and the NFKB1 -94ATTG polymor-phism, whereas there was a tendency towards subadditivity for gluteofemoral obesity. The excess risks were, however, small and generally not statistically significant. Conclusion The NFKB1 -94ins/delATTG promoter polymorphism did not substantially modify the association between obesity and inci-dent ACS. Keywords: NF-kappaB, acute coronary syndrome, inflammation, obesity, gene-environment interaction

28 Jakob Gerhard Stegger
Paper III
Single Nucleotide Polymorphisms in IL1B and the Risk of Acute Coronary Syndrome: a Danish Case-Cohort Study Jakob Gerhard Stegger MD1, Erik Berg Schmidt DMSc1, Anne Tjønneland DMSc2, Tine Iskov Kopp3 MSc, Thorkild I. A. Sørensen DMSc4, *Ulla Vogel PhD5 / Kim Overvad PhD1,6
1Department of Cardiology, Center for Cardiovascular Research, Aalborg Hospital, Aarhus University Hospital, Aalborg, Denmark 2Danish Cancer Society Research Center, Copenhagen, Denmark 3National Food Institute, Technical University of Denmark, Soborg, Denmark 4Institute of Preventive Medicine, University of Copenhagen, Copenhagen, Denmark 5National Research Centre for the Working Environment, Co-penhagen, Denmark 6Department of Epidemiology, School of Public Health, Aarhus University, Aarhus, Denmark *Ulla/Kim contributed equally Correspondence to: Jakob Gerhard Stegger, Department of Cardiology, Aalborg Hospital, Aarhus University Hospital, Sdr. Skovvej 15, 9000 Aal-borg, Denmark, Tel.: +45 9932 1111, email address: [email protected] Word count: Abstract: 258 Article: 2537, exclusive of title page, abstract and tables. ABSTRACT Introduction Interleukin-1B (IL-1B) is a key pro-inflammatory cytokine that has been associated with the development of atherosclerosis and myocardial infarction. However, the prospective associa-tions between functional single nucleotide polymorphisms (SNPs) in IL1B and incident acute coronary syndrome (ACS) have not been thoroughly investigated. The aims of this study were to examine the associations between individual SNPs in and SNP haplotypes of the promoter region of IL1B and incident ACS in a prospective study. Further-more, we wanted to explore potential interactions with other risk factors for ACS on an additive scale.
Methods and Results The present study was based on the Danish prospective study Diet, Cancer and Health comprising more than 57 000 partici-pants aged 50-64 at baseline. During a median follow-up of 7.2 years we identified 989 cases of incident ACS (755 men and 234 women). All cases were validated by review of medical records, and information on covariates was collected by study techni-cians. The study was conducted according to a case-cohort study design including ACS cases and a sex-stratified sub cohort of 1663 participants drawn randomly from the entire cohort. Weighted Cox proportional hazard models with age as time axis were used in the statistical analyses. Individual IL1B SNPs, SNP haplotypes, or haplotype combina-tions were not significantly associated with incident ACS, and, likewise, we found no evidence of interaction on an additive scale between IL1B haplotypes and risk factors, respectively. Conclusion Genetic variation in the promoter region of IL1B may not be associated with incident ACS in men or women above the age of 50 years. Keywords: IL-1B; acute coronary syndrome; in-flammation; obesity; gene-environment interaction.

Udgivet i samarbejde medDansk Cardiologisk Selskabwww.cardio.dk
Dansk Cardiologisk SelskabHauser Plads 101127 København [email protected]
Copyright © Jakob Gerhard Stegger
Tryk: AKA-PRINT A/SJuni 2012
ISBN: 978-87-92010-39-1
Ph.D. thesis
Anthropometry and polymorphisms in
inflammatory genes in relation to acute
coronary syndrome
Jakob Gerhard Stegger
Ph.D. thesis ● Jakob Gerhard Stegger
Faculty of Health Sciences,University of Aarhus
AARHUS UNIVERSITY AU
Omslag-Jakob Gerhard Stegger-TRYK.indd 1 29-06-2012 10:04:01