Embed Size (px)
Citation preview

Philippine Dermatological Society
Officers and Board Members 2001 - 2002
PresidentVice President
SecretaryTreasurer
Members of the Board
Immediate Past President
Rm. 1015 Front Tower, Cathedral Heights Complex, St. Lukes Medical Center, E. Rodriguez Sr., Ave., Quezon CityEmail: [email protected] Website: www.pds.org.phTel/Fax. No.: 727-7309; Fax No.: 932-9269
Elizabeth Amelia V. Tianco, M.D.Francisca C. Roa, M.D.Benjamin B. Bince, M.D.Georgina C. Pastorfide, M.D.
Ma. Lorna F. Frez, M.D. Daisy K. Ismael, M.D. Evelyn R. Gonzaga, M.D. Sylvia S. Jacinto, M.D. Vermen M. Verallo-Rowell, M.D.
Clarita C. Maaño, M.D.

ECZEMA CpM4THEDITION
Guidelines in the Diagnosis & Treatment of EczemaPrepared byVermén M. Verallo-Rowell, M.D.Board Member and Past President, Philippine Dermatological Society
Eczema and eczematous dermatitis refer to an in-flammatory condition of the skin characterized by the exudation of serous matter in lesions that appear and evolve in a very similar manner. These skin changes frequently rank among the top 5 - 10 that bring patients to a doctor’s office. A wide variety of unrelated causes produce eczema. Each of these have different pathoge-netic characteristics that differentiate one type of eczema from all the others. Treatment becomes successful when the guidelines are targeted towards specific aspects of Pathogenesis. CommonFeaturesofEczematousDermatitis(ED)
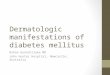
The primary clinical presentation of acute ED begins with an itchyedematousandredpatch which then develops tiny bumps or bubbles within the patch. These bumps/bubbles become fluid-filled vesicles or larger bullae, which break down, become eroded, often with more itching, sometimes pain, redness and edema of the patch, Fig. 1:
Figure 1
Almost immediately, secondary changes develop. The fluid filled vesicles or blisters turn into a wet crust,then into adryscab,resulting in adry,scalypatch.The inevitable scratching and excoriations of the itchy
patch lead to varying degrees of infection which further lead to thickening or lichenification, and post-inflam-matoryhyperorhypopigmentationoftheinvolvedskin,Fig.2:
Figure 2
The series of primary and secondary changes re-occur at the initial patch, or spread to other areas depending on the continued activity or presence of the primary cause in subacute ED, Fig. 3:
Figure 3
Common conditions with these sequence of skin events, but with different causes, pathogenesis, and clinical evolution, are: • Atopic Dermatitis • Contact Dermatitis • Photosensitivity Dermatitis • Palmo-plantar Vesicular Eczema • Nummular Eczema • Asteatotic Eczema of the elderly, and • Gravitational Eczema. 1,2,3
Itchy edematousand red patch
Vesicle
Bumps or bubbles
Crust
open, eroded blister
Vesicles
ECZEMA

CpM4THEDITION ECZEMA
DIsEAsEs
ATOpICDErMATITIs(Eczema)(AD)
primaryCause/pathogenesis•Familial • Inheritance Pattern, autosomal dominant • Polygenic • Flare-ups associated with Allergens which act
either as Antigens – (need cellular processing), or as superantigens (no prior processing), induc-ing IgE synthesis, TH2-like cell expansion, mast cell degranulation, and injury to keratinocytes. All contribute to the inflammation and cutaneous hyperresponsiveness in AD
Allergensare: • Environmental contactants by direct skin contact:
on the face of babies: tomatoes, citrus fruits; soaps, detergents, wool, acrylics. Inhalants by airborne exposure, Indoors/Outdoors: Dander, housedust mites, pollens
• Foodallergens - a subset is known to exist but in most, this is unsubstantiated
• Microbes - Staphylococci, P. ovate, T. rubrum
CONTACTDErMATITIs(CD)
primaryCause/pathogenesis • Acquired and specific • Reaction to a substance in direct contact with the
skin. • AllergicCD:the contactant is processed by antigen
– presenting cells at the epidermis, followed by a TH-1 or delayed type immune response
CommonContactAllergens: Metals: Chrome, Nickel. Perfume ingredients.
Rubber chemicals. Dyes; Formaldehyde resins formaldehyde releasing preservatives.
• IrritantCD: Non-immunologic, based on the ir-ritability of the skin and amount of the contactant present.
strongContactIrritants: Ethylene Oxide used for gas sterilizations; Hy-
drofluoric acid used in electronics/semi-conduc-tors; Wet cement
MildtomoderateContactIrritants Soaps, solvents, detergents, fiberglass, metalwork-
ing fluids, bleaches, grease removers, insecticides, fertilizers, rodenticides, waxes and polishers
someallergensinhighconcentrations
pHOTOsENsITIvITyDErMATITIs(pD)CON-TACT(CpD)&Drug(DpD)
primaryCause/pathogenesis • Acquired and specific • Reaction to a contactant or drug which is stimulated
by light exposure Common Contact photoallergens: • Dyes and fragrance ingredients in household
products, toiletries, and cosmetics • Therapeutic tars, pitch, creosote • Some plants:celery, lime, lemon, garlic, chrysanthemum, dill, parsnip • Halogenated salicylanilides used as anti-
bacterial ingredients • Whiteners in household products • Sunscreens Common Drug photoallergens: • Antibiotics: Griseofulvin, nalidixic acid, sulfanilamide, tetracyclines, doxycycline, quinolones: cipro-, oflo-, norfloxacin, urologi-
cals • NSAIDS: Benoxaprofen, piroxicam, naproxen, ketoprofen, mefenamic acid • Anti-diabetic drugs:Sulfonylureas • Diuretics: Furosemide, thiazides • Cardiac medicines: Quinidine, amiodarone • BP medicines: Enalapril, diltiazem • Antidepressants • Anxiolytics • Antipsychotics • Chemotherapeutic drugs: Dacarbizine, 5-FU,vinblastine • Lipid lowering drugs: Fenofibrate, benzofi-
brate
PAlmo-PlAntAr VesiculAr eczemA(ppvE):This includes the broadened concept of Pom-pholyx or Dyshidrotic Eczema
primaryCause/pathogenesis•AcquiredandMultifactorial • Atopic history as in AD – allergens acting as an-
tigens or superantigens. Atopichistory20-30%, Familyhistory59%
• Contact Dermatitis Most commoncontactants: • Nickel, chrome, PPDA, fragrance • Ingested allergens: Ni, Cobalt, chromates Balsams Neomycins, other drugs Foods Poison oak or poison ivy related to mango, lac-
quer tree oil for furniture (Japan, China, India), cashew nut shells and oils.
• Implanted metals • Contact with proteins
table 1 - DIFFErENTCAusEsANDpATHOgENETICFEATurEsOF 7COMMONECZEMATOusDErMATOsEs
ECZEMA

ECZEMA CpM4THEDITION
• Secondary to distant focus of infections which clear when primary is treated. Fungal Infection: Dermatophytid Bacterial: Bacterid
NuMMulArECZEMA(NE)Or[DIsCOIDECZEMA]
primaryCause/pathogenesis• AcquiredandMultifactorial • Unrelated to Atopy IgE level Normal • Bacteria as primary cause or through hypersensitiv-
ity, but actual role of staphylococcus or streptococ-cus not definite
• Related to dry skin – from obsessive use of soap several times a day, long hours of direct fan expo-sure or low-set air conditioning
• Some worsen in the summer, exacerbated by heat and humidity
• Other associations of flare-ups: wool, topical medicines including topical steroids varicosities, autosensitization
• Drugs: Gold, methyldopa, streptomycin, aminosali-cylic acid, INH
AsTEATOTICECZEMA(AE)orECZEMACrAquElATuM
primaryCause/pathogenesis• Acquired,duetoXerosiscausedby: • Aging • Post-inflammatory change
ATOpICDErMATITIs(ECZEMA)(AD)
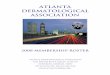
• Infants and children: Facial (Figure 4a) and extensors (Figure 4b) with secondary staphylococcal impetig-inization of lesions.
Figure 4a
• Post-use of irritants • Low ambient humidity from seasonal change of
weather, prolonged airplane flights, air-condition-ing
• Frequent bathing using soaps with high or alkaline pH.
• Diminished use of emollients • Familial tendency for dry skin • Occasionally a presenting sign of hypothy-
roidism, • Lymphoma, other systemic diseases.
grAvITATIONAlECZEMA(gE) oldtermforstasisDermatits
primaryCause/pathogenesis•Acquired,duetochronic, venous, hypertension from
poor venous drainage due to: • Obesity • Trauma • Venous thrombosis from pelvic/lower abdominal
operations, prolonged recumbency, leg injuries, varicose veins, thrombophlebitis
• Multiple pregnancies • Heredity for incompetent valves,causing backflow
of blood • Common in wheelchair bound patients • All other situations with decreased muscle pump
function for assisting blood return
table 2 - DIFFErENTIATINgFEATurEsOFprIMArylEsIONsANDDIsTrIBuTIONpAT-TErNsOF7COMMONECZEMATOusDErMATOsEs
Figure 4b
ECZEMA

CpM4THEDITION ECZEMA
Figure 5a, affecting antecubital spaces
Figure 5b, affecting popliteal spaces
• Adult AD: Flexural distributioin, often with licheni-fication is very common, Fig. 5 a and b.
• Airborne CD due to contactants such as pollens, house-dust, perfume/insecticide sprays, affect exposed areas, spare covered areas. This is similar to the distribution of photocontact dermatitis. The difference is involve-ment of eyelids, inner arms creases of the neck. Fig 6a:
• Plants: Linear pattern from leaf, or plant markings, Fig. 7:
• Clothing-related allergens affect covered areas es-pecially posterior aspect of neck, upper back, lateral thorax, flexor surfaces, axilla. Fig. 8 is contact due to exposure to leather below the abdomen bulge.
CONTACTDErMATITIs(CD)
• Involvement of the chin and under the chin areas, Fig 6b:
Figure 6b
Figure 7
Figure 8
ECZEMA

ECZEMA CpM4THEDITION
Dermatitis of the face, ears, neck are often due to com-ponents of facial, scalp cosmetics, other products for grooming on areas of application, Fig. 9:
Figure 9
• Deodorants can also cause CD, Fig. 10:
• Topical medications commonly produce Contact Dermatitis. These eczematous lesions were produced by allergy to petrolatum, used as a moisturizer and in an ointment : Fig. 11a on the thighs:
Figure 10
Figure 11a
Figure 11b, on the legs
CONTACTpHOTOsENsITIvITy(CpD)andDrug(DpD)
• The pattern in Photosensitivity whether due to a Drug
or Contactant, remains the same, and is similar to airborne CD.
• Exposed areas are affected but differ from airborne CD by sparing the eyelids and the area below the jawline, Fig. 12a:
• Spares the area under the chin, Figure 12b
Figure 12a
Figure 12b
ECZEMA

CpM4THEDITION ECZEMA
AsTEATOTICECZEMA(AE)orECZEMACrAquElATuM
• Older patients: Appearance of a cracked river bed with
poorly defined borders• Primarily on the extensor aspects of the limbs and
trunk (Figure 14).
grAvITATIONAlECZEMA(gE) old term forstasisDermatitis
• Rarely before middle age• Scaling, erythema pigmentation, scarring, often with
pruritus and eczematous changes from scratching, topical medicines used, Fig. 15a and Fig. 15b
Figure 15a
Figure 15b
• Affects the exposed areas of the dorsa of ankles and feet, Fig. 12c
Figure 12c
NuMMulArECZEMA(NE)or[DIsCOIDECZEMA]
• In men: 55 - 56 peak age. In women peak age at 15 - 25
• Rare in children• Single, multiple or episodic, and recurrent at previ-
ously affected sites• Start as discrete vesicles, papules become confluent,
coin-shaped usually up to 10 cm. size (Figure 13a) extend peripherally (Figure 13b)
Figure 13a
Figure 13b
Figure 14
ECZEMA

ECZEMA CpM4THEDITION
PAlmo-PlAntAr VesiculAr eczemA (ppvE):This includes the broadened concept ofpompholyxorDyshidroticEczema
• Minor, mainly affects sides of fingers with or without palms or soles Fig. 16a
• Classic, rare, explosive large coalescent blisters• Relapsing, acute, subacute, and chronic Fig. 16b
Figure 16a
Figure 16b
OTHErAssOCIATEDFEATurEs
ATOpICDErMATITIs(ECZEMA)(AD)• Pruritus, intense• Xerosis / Ichtyosis, common, usually severe• Cutaneous infections often• Pityriasis alba• Non-specific hand and feet dermatitis• Asthma, allergic rhinitis may develop as AD is out-
grown in 30% of children• Commonest inflammatory skin disease of childhood
(15% in the UK)• Less common in adults (1-2%) but more severe and
chronic
CONTACTDErMATITIs(CD)
• HighdegreeofawarenessandsuspicionneededtorecognizepatternsofCD
• Persistent questioning yields results about exposure to contactants
• Habitually used contactants often least recog-nized
• Occupational Diseases – Contact Dermatitis ranks among the top
CONTACT(CpD)andDrug(DpD)pHOTO-sENsITIvITyDErMATITIs(pD)
• HighdegreeofawarenessandsuspicionneededtorecognizepatternsofpD
• Persistent questioning yields results about exposure to the photoallergen
• Familiarity with the generic family of chemicals, needed to recognize cross-reactions.
PAlmo-PlAntAr VesiculAr eczemA (ppvE):This condition includes the broadened concept ofDyshidroticEczema(orpompholyx)
• Affects adolescents and young adults• Discomfort and itching precedes development of
vesicles, small sago-like• Dry out, resolve, often without rupturing• Secondary infections common
NuMMulArECZEMA(NE)or[DIsCOIDECZEMA]
• Acute edema exudation• Chronic: scaling, lichenification, excoriations, itch-
ing, mild to moderate• Legs usually, also upper extremities, especially dor-
sum of hands, trunk• Drug history
AsTEATOTICECZEMA(AE)orECZEMACrAquElATuM
• Bed-ridden or confined indoors especially with con-stant air-conditioning
lABOrATOryDATA
ATOpICDErMATITIs(ECZEMA)(AD)• Elevated serum IgE for foods, aeroallergens, micro-
organisms, bacterial toxins• KOH of skin scrapings for fungi; fungal culture• Microbiology by Giemsa staining, Bacterial culture• skinBiopsy: Eczematous Dermatitis with mild to
ECZEMA

CpM4THEDITION ECZEMA
ground• KOH skin scrapings for fungi/fungal culture• Microbiology by: Giemsa staining, Bacterial culture• skinBiopsy: Eczematous Dermatitis with mild Eosi-
nophilia
NuMMulAr ECZEMA (NE) Or [DIsCOIDECZEMA]
• Bacterial culture• CBC, ASO titer, ESR• skinBiopsy: Subacute Eczematous Dermatitis
AsTEATOTICECZEMA(AE)OrECZEMACrAquElATuM
• Thyroidfunction tests• Organs check-up as indicated by history and Physical
Examination• skinBiopsy: Hyperkeratosis with a thin granular layer
similar to Ichtyosis
grAvITATIONAlECZEMA(gE)oldtermforstasisDermatitis
• venousultrasonography to rule out DVT in cases with acute onset
• skinBiopsy shows dilated capillaries with thick walls, abundant melanin and hemosiderin pigment deposi-tion
spECIFICTrEATMENTTArgETEDATCAusEsIDENTIFIED
ATOpICDErMATITIs(ECZEMA)(AD)
Improvementofambienthumidity• Avoid over air-conditioning• place a bowl of water or a steamer beside the bed• Avoiddirect exposure to fansDecreasesweating• Improveair circulation• Avoidhot baths• Takecooling drinks• Exercisemoderately, cooldownimmediately• Avoidexcesseslessenskindryness• Takeshort cool showers• usesuperfatted soaps sparingly, and minimally use
at the creases• usethe mildest non-scented laundry soaps for cloth-
ing and beddings• Avoidexposure to specific allergens • use Barrier creams
CONTACTDErMATITIs(CD)
• Identifycontactant by history or by Patch testing• Observe for prompt improvement when contactant is
moderate Eosinophilia
CONTACTDErMATITIs(CD);CONTACT(CpD)ANDDrug(DpD)pHOTOsENsITIvITyDEr-MATITIs(pD)
• sampleofrelevant(+)patchtests(Figure17) in a patient with the pattern of clothing CD, Cosmetic CD and CPD
Left side Right side
Comparison reading of two patch test trays:Chemotechnique Tray: (L), Patch #2 (++)Skin Science Laboratory, Inc. Tray (R): Patch #4 (+++) Both patches are p-phenylenediamine base 1% in Petrolatum Relevance: Exposure: +, and Current to dyes for the hair, clothing, newspaper ink and recently to the ink of a photo exposed tattoo applicationClose up of multiple (+) patch tests mimics the ecze-
matous clinical lesions, Fig.18:
Conclusion: PPDA is both a contactant and a photo contactant in this patient
• skin Biopsy: dermal infiltrate with marked eosi-nophilia
PAlmo-PlAntAr VesiculAr eczemA (ppvE):includesDysHIDrOTICECZEMA
• Elevated serum IgE demonstrates atopic back-
Figure 18
ECZEMA

ECZEMA CpM4THEDITION
to use of air conditioning/fans.• use emollients liberally, frequently and massage well
into moistened skin• Wrap with flexible plastic overnight to increase
moisture content of skin• Diminish use of soaps• Correct irritation and trauma immediately
grAvITATIONAlECZEMA(gE)oldtermforstasisDermatitis
Weightreduction• Minimizetrauma especially from excoriationsDecreasevenousHypertensions• use of support hose for prevention of varicosities in
those with (+) family history for VV and/or early VV development
• use of properly fitted hosiery once varicosities de-velop
• Avoid irritants and contactants including antibiotic, stabilizer and steroid ingredients in topical medications
non-sPecific treAtment tArgeted AtsTAgE&TypEOFsKINlEsIONs
TOpICAl
Acute Exudative lesions: Tub baths, or cold water compresses using old T-shirt or soft towels. Saturate with tap water, NSS, Burrows Solution (1:20 dilution) 15 – 30 mins twice a day. Add mineral or bath oil 10 minutes after start of bath or compress. Keep bullae in-tact, do not prick unless very large and tense. If infected, potassium permanganate 1:25,000 – 1:50,000 dilution, benzalkonium chloride 1:5,000 aqueous solution (may also cause Contact Dermatitis); 5% acetic acid aqueous solution especially for Pseudomonas infection
non-steroidAl, Anti-PruriticprEpArATIONs
subacute:Antipruritic soothing lotions: Calamine lo-tion (8% zinc oxide/8% calamine); Witch Hazel Solu-tion; Camphor 1% - 3%; Coal tar solution 3% - 10% , Menthol 0.25% - 2.00%; Phenol 0.5% - 1.5%; Salicylic acid 1.0 – 2.0%
Chronicdry thickened lesions:Soak affected areas 5 min in water. Immediately apply a hydrophilic oint-ment (Petrolatum) liberally, massage into the skin thoroughly.Occlude using a thin flexible plastic (Glad®, Saran®, Nanya®)
Intralesional steroid Injections to more rapidly thin down thick dry patches
discontinued, slow or no improvement when another cross-reacting product is still used.
• usebarrier creams including petrolatum jelly when exposure to contact allergen cannot be avoided, or use cotton gloves under plastic gloves, not rubber gloves
• Irritants: forceful and prolonged irrigation with water
• Teach Good Housekeeping Practice at work: Proper storage of raw materials, frequent disposal of
wastes, prompt removal of spillage, a neat and clean environment
CONTACT(CpD)ANDDrug(DpD)pHOTO-sENsITIvITyDErMATITIs(pD)
• Identifyphotocontactant by history or by Photopatch testing
• Observe for prompt improvement when photoaller-gen is discontinued, unless there is a cross-sensitivity with other products still used.
• useof sunscreen (SS) with a High Protection Factor (PF) to UVA, UVB, Indoor lights. At least an SPF of 30, PFA of 4, with Titanium dioxide, Zinc and Iron oxide for outdoor and indoor artificial light protec-tion.
ContinueSS beyond time of stopping of allergens until patient is no longer photosensitive.
• AVOID outdoor sun and indoor light• Use clothing protection
PAlmo-PlAntAr VesiculAr eczemA (ppvE):Thisconditionincludesthebroadenedcon-ceptofDyshidroticEczema(orpompholyx)
• Trialof suspected allergen withdrawal and/or chal-lenge
• Treatmentof suspected or identified infection: bacte-rial or fungal
• useofprotectantsZinc oxide Paste/Ointment, Pet-rolatum jelly, Stokogard Cream, Pure cotton gloves for dry work, plastic or rubber glove on top of cotton gloves for wet work
NuMMulArECZEMA(NE)Or[DIsCOIDECZEMA]
• Trialof suspected allergen withdrawal and/or chal-lenge
• Treatmentof suspected or identified infection: bacte-rial or fungal
• Improveambient humidity. Avoid over air-condition-ing, water compresses
AsTEATOTICECZEMA(AE)OrECZEMACrAquElATuM
• Correcthyperthyroidism medically• Correctenvironment to increase humidity in regards
ECZEMA

CpM4THEDITION ECZEMA
TosuppresstheImmunesystemanddecreaseskinhy-per-reactivity, refer to a Dermatologist for photothera-pyusing: UVB, Broad band or narrow band; UVA, PUVA.
sysTEMICMEDICATIONsAntihistamines at bedtime, Hydroxyzine or Benad-
ryl;Daytime, a non-sedating antihistamine
Role of antihistamines in controlling itching in AD. Remains to be defined (this may also apply to other Eczemas). Effects may be peripheral and/or central (sedation). Questions remain on choice of sedating vs. non-sedating antihistamines, for how long, and the pos-sible side effect of hyperactivity in children.4
OralAntibioticsorantifungals if infected or to reduce bacterial or fungal population of dermatitic skin
oral anti-viral medications when viral infections oc-cur.
Oralsteroids: short term for acute, severe, or general-ized Eczema
In more severe/acute AD or PPVE, very carefully moni-tor the use of: Cyclosporin A & Mycophenolate
references:
1. Epstein JH. Phototoxicity and Photoallergy. SEMIN CUTAN MED SURG 1999 Dec 18 (4) 274 – 84
2. Riescherl RL, Fowler Jr., JF, eds. FISHER’S CONTACT DERMA-TITIS FOURTH EDITION, Williams and Wilkins, US, 1995
3. Freedberg IM, Eisen AZ, Wolff K, Austen KF, Goldsmith LA, Katz SI, Fitzpatrick TB. FITZPATRICK’S DERMATOLOGy IN GENERAL MEDICINE FIFTH EDITION, Numular Eczema, Chapter 125; Atopic Eczema, Chapter 124; Vesicular Palmo-plantar Eczema, Chapter 127; Gravitational Eczema and Asteatotic Eczema, Chapter 146, McGraw-Hill Companies, Inc., US 1999
4. Eysenbach G, Williams H, Diepgen TL. Antihistamines for Atopic Eczema (Protocol) Completed Review, Cochrane Skin Group Page (http://nottingham.ac.uk/~muzd)
5. Hoare C, Leonard T, Williams HC. Chinese Herbal Medicine for Atopic Eczema (Protocol) Cochrane Skin Group Page (http://not-tingham.ac.uk/~muzd)
6. Scheman AJ, Severson DL. MEDICATIONS USED IN DERMA-TOLOGy SIXTH EDITION. Lippincott Williams and Wilkins, US 1999
Herbal medicines – CAUTION: Be sure these do not contain steroids; are notirritants5
Tar: 10% Liquor Carbonis DetergentsSalicylic Acid: 3-6%Antibiotic creams, ointmentsAntifungal creams, ointments, sprays
new non-steroidAl immunomodulA-TINgDrug for moderate to severe AD.
Tacrolimus Ointment (PROTOPIC)
TOpICAlCOrTICOsTErOIDs
Anti-Inflammatory medicationslotions or creams for subacute lesions; ointments for chronic. Prescribe use of steroids only for severe, acute or gen-eralized lesions. Instruct patients about side effects and to avoid prolonged/repeated use.
Use topical steroids according to strength and class Class strength 1 = Strongest 7 = Weakest
1. Clobetasol propionate – Dermovate (0.05%) scalp lotion, cream, ointment
2. Bethamethasone dipropionate – Diprolene (0.05%) cream, lotion, ointment; Diprosone cream, oint-ment
Mometasone furoate – Elica (0.1%) cream, ointment, lotion
Fluocinonide – Lidex (0.05%) cream, ointment; Lidemol (0.05%) ointment
Desoximethasone – Esperson (0.25%) ointment, scalp application
3. Betamethasone valerate – Betnovate (0.1%) cream, lotion, ointment
Fluticasone propionate – Cutivate (0.005%) oint-ment
4. Fluocinolone acetonide – Aplosyn (0.025%) cream; Synalar 25 cream, ointment
5. Hydrocortisone butyrate – Locoid (0.1%)6. Desonide – Desowen (0.05%) cream, lotion, oint-
ment7. Hydrocortisone – Lacticare HC (1%) lotion; Hy-
drotopic (1%) cream Hydrocortisone aceponide – Efficort cream, lipo-
cream
ECZEMA

ECZEMA CpM4THEDITION
Drugs Mentioned in the Treatment GuidelineThis index lists drugs/drug classifications mentioned in the treatment guideline. Prescribing Information of these drugs can be found in the Philippine Pharmaceutical Directory (PPD) 8th edition. Opposite the brand name is its page number in the PPD 8th edition.
AntihistaminesAstemizole
Hismanal C23Diphenhydramine
Alertuss C23 Benadryl C23 Biogenerics Diphenhydramine C23 Dramelin C23 Europharma Diphenhydramine C23 Hizon Diphenhydramine Inj C23
Hydroxyzine Iterax C23
Loratadine Claritin C23 Loradex C24
OralAntibiotics Amoxicillin
Aldemox D37 Amoclav* D37 Amoxil D37 Amoxsteryl D37 Amoxtrex D37 Amusa D37 AstraZeneca Amoxicillin D38 Athenalyn D38 Augmentin* D38 Axmel D38 Biogenerics Amoxicillin D38 Cilfam D39 Clearamox D39 Curamox D39 Daisamox D39 DLI-Amoxicillin D39 Drugmakers Amoxicillin D39 Eleomox D39 Europharma Amoxicillin D39 Glamox D40 Glenox D40 Globamox D40 Harvimox D40 Himox D40 IHC-Amoxicillin D40 Intermox D40 Jamox/Jamox Forte D40
Littmox D40 Medimoxil D40 Megamox D40 Metaxyl D40 Montecil D41 Moxillin D41 Neomox D41 Oramox/Oramox Forte D41 Pediamox D41 Pharex Amoxicillin D42
Pharmamox D42 Polymox D42 Servimox D42 Shinamox D42 Sumoxil D43 Teramoxyl D43 UL Amoxicillin D43 Valmox D44 Wyamox D44 yugoxil D44 Zymoxyl D45
Ampicillin Ampedia D37 Ampicin D37 Ampimycin D37 Ampin D37 Amplivacil D37 Apamicin D38 Bactimed D38 Biogenerics Ampicillin D38 Celidam D39 Cloxamicin* D39 DLI-Ampicillin D39 Drugmakers Ampicillin D39 Eurotrexil D39 Genaxcin D39 Leoplex D40 Metadyl D40 Penbritin D41 Pensyclox* D41 Pensyn D41 Pentrexyl D42 Saloxin D42 Shinapen D42 UL Ampicillin D43
Azithromycin Zithromax D36Bacampicillin
Bacacil D38 Penglobe D41Cefaclor Ceclor/Ceclor BID/
Ceclor CD D29Cefadroxil Duracef D30Cefalexin Bacilexin D28 Biogenerics Cefalexin D28 Bloflex D28 Cefalexin-Vamsler D28 Cefalin D28 Ceporex D28 Cidoxine D28 Cromlex D28 Drugmakers Cefalexin D28 Eliphorin D28 Europharma Cefalexin D28 Exel D28 Fevenil D28 Genflex D28 Gesenal D28 Halcepin D28 Harvexyl D28 Keflex D28 Lexum D28 Lyceplix D28 Medilexin D28 Medoxine D28 Oneflex D28 Oranil D29 Pectril D29 Pharex-Cefalexin D29 Servispor D29 VCP Cefalexin D29 Xinflex D29 Zeporin D29Cefatrizine Zanitrin D31Cefdinir Omnicef D32Cefprozil Procef D30Cefradine Velosef D31Cefuroxime Zinacef D31
ECZEMA

CpM4THEDITION ECZEMA Zinnat D31Ciprofloxacin Ciprobay D45Clarithromycin Klaricid D36Clindamycin Biogenerics Clindamycin D34 Clindal D34 Dalacin C HCl/Dalacin C
Palmitate/Dalacin C Phosphate D34
Inprosyn-HP D34Cloxacillin
Biogenerics Cloxacillin D38 Cloxamicin* D39 Cloxigen D39 Drugmakers Cloxacillin D39 Encloxil D39 Europharma Cloxacillin D39 IHC-Cloxacillin D40 Interclox D40 Medix D40 Myrex Cloxacillin D41 Orbenin D41 Pensyclox* D41 Pharex Cloxacillin D42 Prostaphlin-A D42
Cotrimoxazole Bacidal D47 Bactille Forte D47 Bactille-TS D47
Bactrim D47 Bacxal D47 Biogenerics Cotrimoxazole D48 Cotrexel D48 Cotrimoxazole-Vamsler D48 DLI-Cotrimoxazole D48 Doctrimox D48 Drugmakers Cotrimoxazole D48 Genoxzole/ Genoxzole Forte D48 Genzaprim/ Genzaprim Forte D48 Globec/Globec Forte D48 Gutrisul D48 Intrafort D48 Kathrex D48 Lagatrim Forte D48 Macromed D48 Microbid/Microbid DS D48 Onetrim D48 Pharex-Cotrimoxazole D48
Rimezone D48 Septrin D48 Servitrim D49 Syndal D49 Synerzole D49 Thoprim D49 Triglobe D49 Trim-S D49 Trimephar D49 Trimetazole/ Trimetazole DS D49 Trizine D49 Trizole Suspension D49 UL Cotrimoxazole D49
Dirithromycin Dynabac D35 Onzayt D36Doxycycline Atrax D50 Doryx D50 Doxicon D50 Doxin D50 Drugmakers Doxycycline D50 Harvellin D50 Servidoxyne D50 Vibramycin D50Enoxacin Abenox D45Erythromycin
Ditron D35 DLI-Erythromycin D35 Drugmakers Erythromycin D35 Ery-max D35 Erybron* D35 Erycin D35 Erythrocin/ Erythrocin DS D35 Erythrolan D35 Ethiocin D35 Europharma Erythromycin D35 Gentrocin D35 Ilosone D35 Macrocin D36 Pharex-Erythromycin D36 Sefavex D36 Servitrocin D36 UL Erythromycin D36
Fleroxacin Roquinol D46Flucloxacillin Na Stafloxin D42Levofloxacin
Floxel D45Lincomycin Harvivin D34 Lincocin D35Loracarbef Lorabid/Lorabid DS
Suspension/Lorabid Pulvules D51
Moxifloxacin Avelox D45Nafcillin Na Vigopen D44Ofloxacin Inoflox D45 Qinolon D46Oxytetracycline DLI-Oxytetracycline HCl D50 Noxebron D50 Terramycin D50Roxithromycin Macrol/Macrol Kiddie D36 Rulid D36Sultamicillin Unasyn Oral D44Tetracycline DLI-Tetracycline HCl D50 Tetracycline-B D50 UL Tetracycline D50 Unimycin D50Tosufloxacin Tosacin D46
OralAntifungalsFluconazole Diflucan D52Griseofulvin Grisovin-FP D52Itraconazole Sporanox D52Ketoconazole Nizoral Tablet D52Terbinafine Lamisil D52
OralsteroidsBetamethasone Betnelan P221
Betneton* C26 Celestamine C26 Celestone P221
Dexamethasone Decilone P221 UL Dexamethasone P223Methylprednisolone
ECZEMA

ECZEMA CpM4THEDITION
Medrol P222Prednisolone Liquipred P222 UL Prednisolone P223Prednisone DLI-Prednisone P221 Drazone P221 Drugmakers Prednisone P221Triamcinolone Kenacort P222
protectantsZinc oxide
Bioderm Ointment* I135 Pevaryl HP* I137
TopicalCorticosteroidsBetamethasone Betnovate I142 Betnovate Scalp I142
Betnovate-C* I149 Betnovate-N* I148 Clotrasone* I148 Diproform* I149 Diprogenta* I148 Diprolene I143 Diprosalic* I149 Diprosone I143 Fucicort* I149 Quadriderm* I148 Quadrotopic Cream* I148 Steroderm I145 Triderm* I148
Clobetasol Clobederm I147
Clobederm-N* I147 Dermovate I143 Dermovate NN* I147 Dermovate Scalp I143
Desonide Desowen I143
Sterax I144Fluocinolone
Aplosyn C/ Aplosyn N* I148 Aplosyn/Aplosyn HP I142 Neo-Synalar 10/ Neo-Synalar 25* I149 Synalar/Synalar HP I145
Fluocinonide Lidemol I144 Lidex I144 Lidex NGN* I147
Fluticasone Cutivate I142
Hydrocortisone Cortizan I142
Daktacort* I149 Eczacort I143 Efficort I143 Eurax-Hydrocortisone* I139 Hydrotopic I143 Hytone I143 Lacticare-HC Lotion I144 Terra-Cortril Topical* I149 Trimycin-H* I148
Mometasone furoate Elica I143 Elocon I143
ECZEMA