Embed Size (px)
Citation preview
C L A U D I N E L A N G - H O D G E P H A R M D , B C P P C L I N I C A L P H A R M A C I S T
A L B E R T A C H I L D R E N ’ S H O S P I T A L S E P T 1 0 , 2 0 1 6
C L A U D I N E . L A N G - H O D G E @ A H S . C A
Physical Effects of Antipsychotics
Disclosures
I have no current or past relationships with commercial entities
Speaking Fees for current program:
– I have received a complimentary registration for today’s conference

Objectives
Review of antipsychotic pharmacology/uses
Discuss metabolic side effects of APs
Discuss movement side effects of APs
Highlight emergency reactions to APs
Determine monitoring/treatment for side effects
Antipsychotics: 1st Generation
• Also known as “Typical Antipsychotics”
• Introduced between 1955-1980 Haldol (haloperidol)
Loxapac (loxapine)
Clopixol (zuclopenthixol)
Orap (pimozide)
Fluanxol (flupenthixol decanoate)
Modecate (fluphenazine decanoate)
Piportil (pipotiazine palmitate)
Largactil (chlorpromazine)
Nozinan (methotrimeprazine)
Antipsychotics: 2nd Generation
Also called “Atypical Antipsychotics” Newer, only available since 1990
- Clozaril (clozapine) - Riperdal (risperidone) - Zyprexa (olanzapine) - Seroquel (quetiapine) - Invega (paliperidone) - Zeldox (ziprasidone) - Saphris (asenapine) - Latuda (lurasidone)
• 3rd generation
- Abilify (aripiprazole)
(NIMH) Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE)
“To the extent that antipsychotics differ, it is more in their side effects than therapeutic effects.”
LIEBERM, J.A, STROUP, T..S.; Commentary :Am J Psychiatry 168:8, August 2011
Antipsychotic Uses
Schizophrenia Schizoaffective d/o Bipolar mania Depression Acute agitation/aggression Sleep Anxiety Dementia Eating disorders Tics
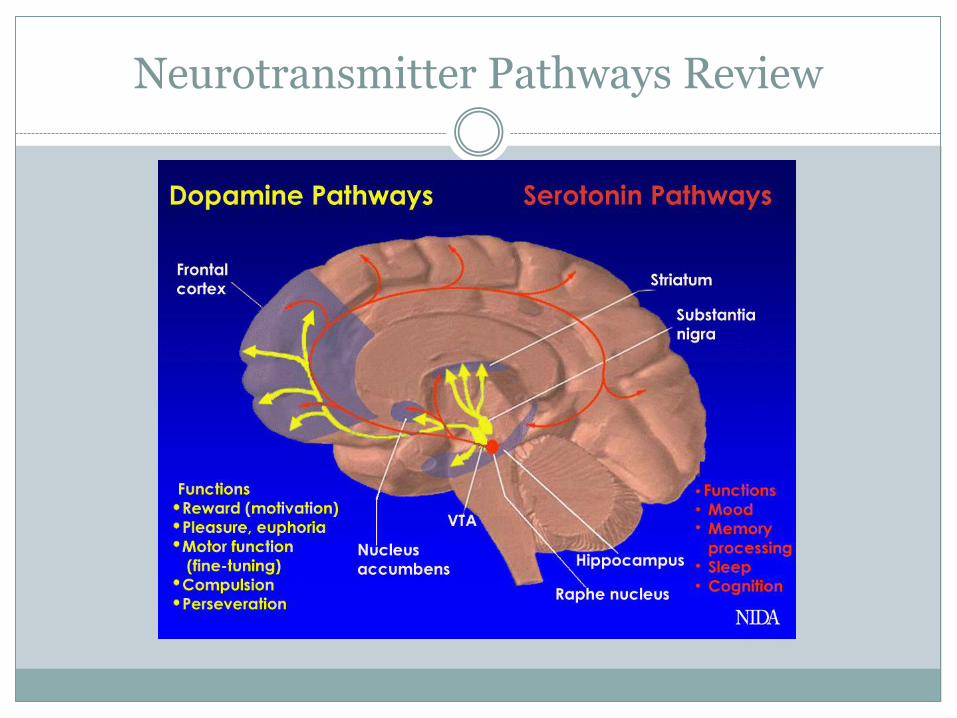
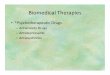
Neurotransmitter Pathways Review
Schizophr Bull, image, viewed May2016 <http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2669582/figure/fig1/>
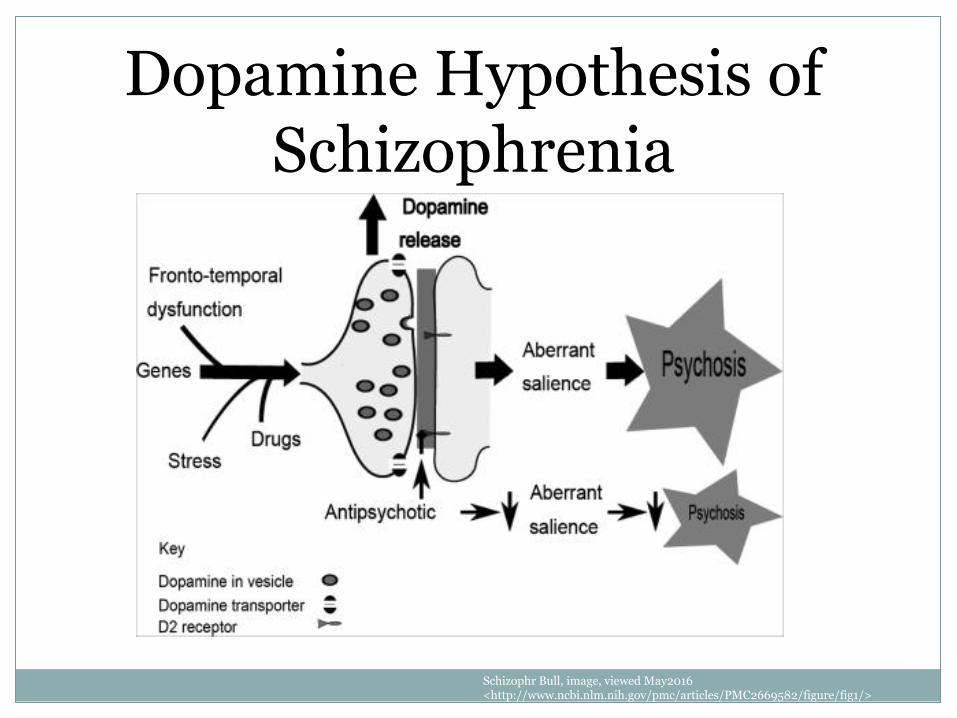
Dopamine Hypothesis of Schizophrenia
Medication Overview: Antipsychotics
Excessive dopamine in specific areas of the brain causes psychoses
Antipsychotics: block various dopamine receptors in the brain
Attempt to regulate: Positive symptoms
Negative symptoms
Mood
Mechanism of Action of Antipsychotics
Exact mechanisms of action are unknown
The primary actions have been attributed to D2 dopamine blocking
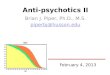
3rd generation (aripiprazole) acts as partial agonist
The different actions at the neurotransmitters account for the different efficacy and side effect profiles
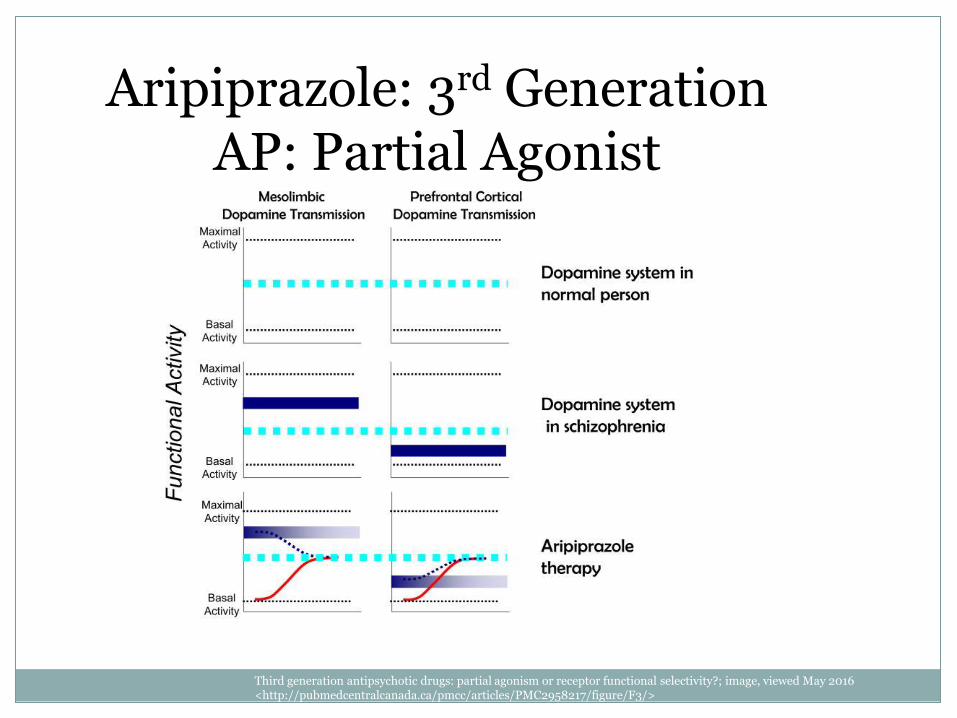
Aripiprazole: 3rd Generation AP: Partial Agonist
Third generation antipsychotic drugs: partial agonism or receptor functional selectivity?; image, viewed May 2016 <http://pubmedcentralcanada.ca/pmcc/articles/PMC2958217/figure/F3/>
Pharmacological Effects of APs on Neurotransmitters/Receptors
• Dopamine Blockade D2
• in mesolimbic =antipsychotic effect (controlling positive symptoms of schizophrenia) • in nigrostriatal tract=EPS and TD • in tuberoinfundibular area= prolactin elevation
• Histamine Blockade Sedation, drowsiness, hypotension, weight gain, antiemetic
• Acetylcholine Blockade Dry mouth, blurred vision, constipation, urinary retention, anticholinergic delirium
• Serotonin Blockade May decrease negative symptoms of schizophrenia, anxiolytic, antidepressant, modulate EPS,
hypotension, sedation, weight gain
• Alpha Blockade Hypotension, reflex tachycardia, sedation, hypersalivation, sexual disturbance
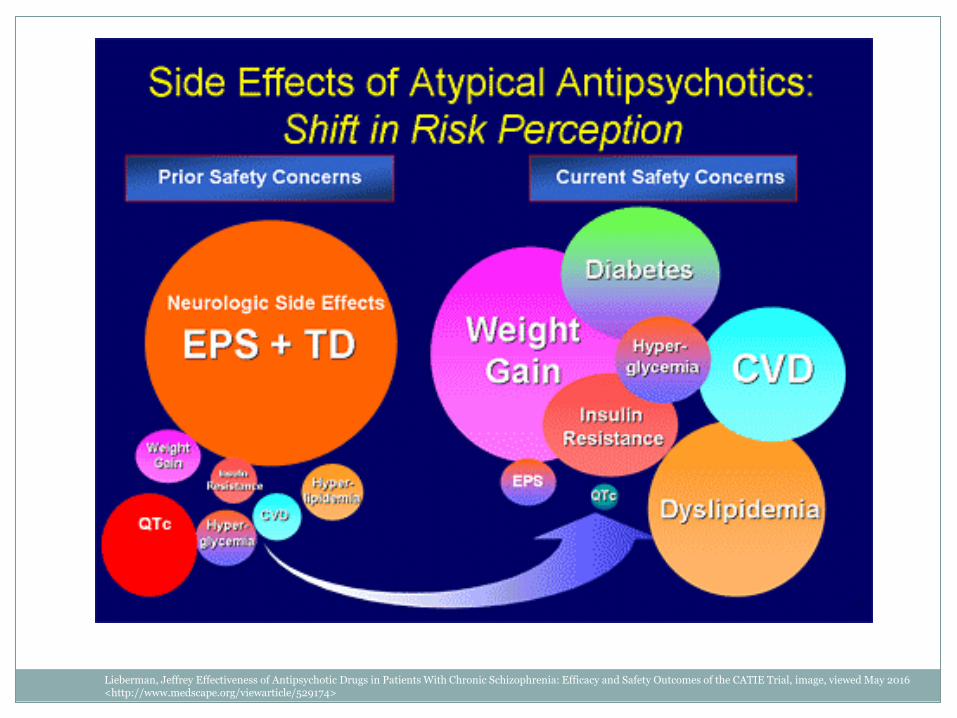
Lieberman, Jeffrey Effectiveness of Antipsychotic Drugs in Patients With Chronic Schizophrenia: Efficacy and Safety Outcomes of the CATIE Trial, image, viewed May 2016 <http://www.medscape.org/viewarticle/529174>
Organ Systems Affected by Antipsychotics
• Endocrine system
• Central nervous system CNS Effects
EPS
Neuroleptic Malignant Syndrome
Seizures
• Cardiovascular system
• Hepatic system
• Dermatologic system
• Hematologic system
• Genitourinary system
Organ Systems Affected by Antipsychotics
• Endocrine system
• Central nervous system CNS Effects
EPS
Neuroleptic Malignant Syndrome
Seizures
• Cardiovascular system
• Hepatic system
• Dermatologic system
• Hematologic system
• Genitourinary system
Endocrine System Effects
Metabolic Effects
Prolactin Effects
Metabolic Effects of APs
• Weight gain
• Increased blood pressure
• Increased lipids Increased total cholesterol
Increased LDL
Increased triglycerides
Decreased HDL
• Increased fasting glucose Increased risk for insulin resistance, type 2 DM
• Increased prolactin
Monitoring for Metabolic Effects
Baseline monitoring: before start of medication or as soon as possible
This includes Personal and family history of obesity, diabetes, dyslipidemia,
hypertension, or cardiovascular disease
Weight and height (so that BMI can be calculated)
Waist circumference (at the level of the umbilicus)
Blood pressure
Fasting plasma glucose
Fasting lipid profile
+/- Prolactin level (depending on medication)
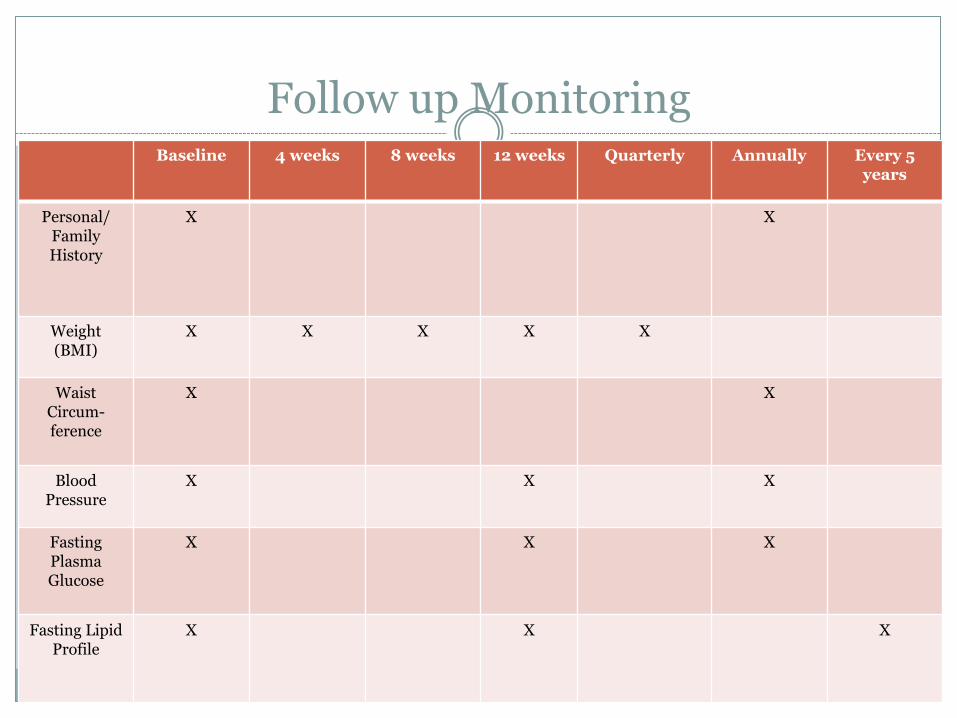
Follow up Monitoring Baseline 4 weeks 8 weeks 12 weeks Quarterly Annually Every 5
years
Personal/ Family History
X X
Weight (BMI)
X X X X X
Waist Circum- ference
X X
Blood Pressure
X X X
Fasting Plasma Glucose
X X X
Fasting Lipid Profile
X X X
Pediatric/Adolescent Metabolic Monitoring
CAMESA Guidelines Canadian Alliance for Monitoring Effectiveness and Safety of
Antipsychotics in Children
CAMESA is led by Dr. Tamara Pringsheim, neurologist and clinical epidemiologist at the University of Calgary
http://camesaguideline.org/
Metabolic Monitoring Form
Example: Risperidone
http://camesaguideline.org/information-for-doctors
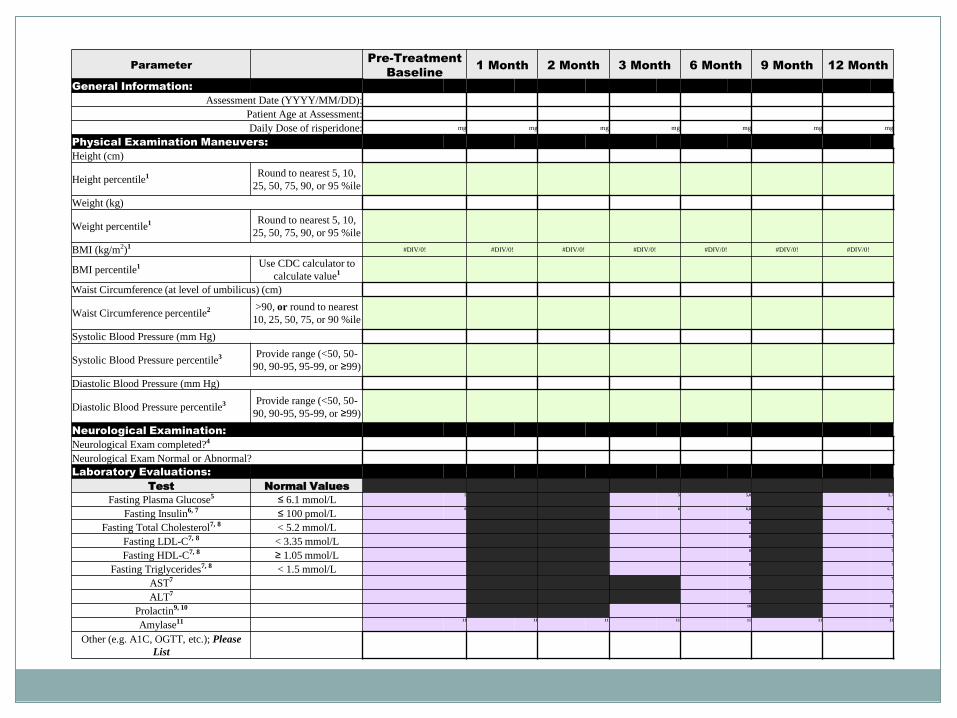
Parameter Pre-Treatment
Baseline 1 Month 2 Month 3 Month 6 Month 9 Month 12 Month
General Information:
Assessment Date (YYYY/MM/DD):
Patient Age at Assessment:
Daily Dose of risperidone: mg mg mg mg mg mg mg
Physical Examination Maneuvers:
Height (cm)
Height percentile1 Round to nearest 5, 10,
25, 50, 75, 90, or 95 %ile
Weight (kg)
Weight percentile1 Round to nearest 5, 10,
25, 50, 75, 90, or 95 %ile
BMI (kg/m2)1 #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0! #DIV/0!
BMI percentile1 Use CDC calculator to
calculate value1
Waist Circumference (at level of umbilicus) (cm)
Waist Circumference percentile2 >90, or round to nearest
10, 25, 50, 75, or 90 %ile
Systolic Blood Pressure (mm Hg)
Systolic Blood Pressure percentile3 Provide range (<50, 50-
90, 90-95, 95-99, or ≥99)
Diastolic Blood Pressure (mm Hg)
Diastolic Blood Pressure percentile3 Provide range (<50, 50-
90, 90-95, 95-99, or ≥99)
Neurological Examination:
Neurological Exam completed?4
Neurological Exam Normal or Abnormal?
Laboratory Evaluations:
Test Normal Values
Fasting Plasma Glucose5 ≤ 6.1 mmol/L 5
5
5,8
5,7
Fasting Insulin6, 7 ≤ 100 pmol/L 6
6
6,8
6, 7
Fasting Total Cholesterol7, 8 < 5.2 mmol/L 8
7
Fasting LDL-C7, 8 < 3.35 mmol/L 8
7
Fasting HDL-C7, 8 ≥ 1.05 mmol/L 8
7
Fasting Triglycerides7, 8 < 1.5 mmol/L 8
7
AST7 7
7
ALT7 7
7
Prolactin9, 10 10
10
Amylase11 11
11
11
11
11
11
11
Other (e.g. A1C, OGTT, etc.); Please
List
Prolactin Effects
D2 blockade in tuberoinfundibular area in brain
risp=pali>FGA>olanz>zipr>quet≥cloz>arip
In women can lead to: galactorrhea, amenorrhea, irregular menses, anovulation, osteoporosis
In men: impotence and azoospermia, and gynecomastia with or without lactation
Prolactin Elevation
If asymptomatic, typically watch and wait No intervention
If symptomatic, preferred treatment is to switch to another antipsychotic agent with reduced risk- caution with relapse potential
Other options:
Add aripiprazole – D2 partial agonist
Add other dopamine agonists: bromocriptine, cabergoline
Organ Systems Affected by Antipsychotics
• Endocrine system • Central nervous system
CNS Effects EPS Neuroleptic Malignant Syndrome Seizures
• Cardiovascular system • Hepatic system • Dermatologic system • Hematologic system • Genitourinary system
CNS Effects of Antipsychotics
CNS Effects
Drowsiness, sedation
Insomnia, agitation
Movement Disorders
Extrapyramidal symptoms
Neuroleptic Malignant Syndrome (NMS)
Seizures
All APs lower the seizure threshold, use with caution in patients with seizure disorder (typically dose related)
Higher risk with chlorpromazine and clozapine
CNS Effects of Antipsychotics
CNS Effects
Drowsiness, sedation
Insomnia, agitation
Movement Disorders
Extrapyramidal symptoms
Neuroleptic Malignant Syndrome (NMS)
Seizures
All APs lower the seizure threshold, use with caution in patients with seizure disorder (typically dose related)
Higher risk with chlorpromazine and clozapine
Movement Disorders Associated with Antipsychotics (EPS)
D2 Blockade in nigrostriatal tract leads to extrapyramidal symptoms
Extrapyramidal Symptoms (EPS)
Drug induced movement disorders that include acute and tardive symptoms Dystonia – continuous spasms and muscle contractions
Akathisia – state of excessive restlessness
Pseudoparkinsonism – rigidity, bradykinesia, tremor
Tardive dyskinesia – abnormal involuntary movement
The Extrapyramidal Symptom Rating Scale (ESRS) to assess four types of drug-induced movement disorders
FGA> risp=pali>olan=zipr=arip>quet>cloz
Chouinard, G, Margolese HC: Manual for the Extrapyramidal Symptom Rating Scale (ESRS); Schizophr Res,2005 Jul 15;76(2-3):247-65. Epub 2005 Apr 18
Extrapyramidal Symptoms (EPS)- Dystonia
Dystonia (10-30%)
Rapid onset 1 or 4 days of start or increase of antipsychotics
Prolonged muscle spasms / contractions
- Oculogyric crisis – rotating of eyeballs
- Opisthotonus- tension in neck, spine, arching
- Tongue spasms or protrusion
- Torticollis – twisted neck
- Trismus-unable to open mouth (forced jaw opening)
- Pharyngeal-laryngeal spasm https://www.youtube.com/watch?v=2krwEbm5hBo
Extrapyramidal Symptoms (EPS)-Dystonia
Treatment/ Recommendation for Acute Dystonia
Anticholinergics:
- Benztropine (PO,IM,IV)
- Procyclidine (PO)
- Trihexyphenidyl (PO)
Diphenhydramine (PO,IM,IV)
Reduce dose of antipsychotics
Symptoms will resolve within minutes with IV therapy
Extrapyramidal Symptoms (EPS)-Akathisia
Akathisia (20-40%)
Usually in first 10 days of start or increase of antipsychotics
Restlessness, pacing, fidgeting, subjective jitteriness, associated with suicide
Most common: Movements affecting the legs
May describe vague sensations of internal restlessness, discomfort, or anxiety
Resembles psychotic agitation, agitated depression
Extrapyramidal Symptoms (EPS)- Akathisia
Treatment / Recommendations for Akathisia
Lower antipsychotic dose if possible
- Greater risk with high dose vs. lower dose
Change to different drug (atypical antipsychotic)
- Higher risk with FGA
- Quetiapine, clozapine – less EPS
Beta-blocker (propranolol)
Benzodiazepines
Extrapyramidal Symptoms (EPS) Pseudoparkinsonism
Pseudoparkinsonism (15-35%)
Onset may be as late as 30 days after initiation/increase
Represents symptoms of Parkinson’s disease:
akinesia, bradykinesia, decreased movement initiation, shuffling gait
micrographia, decreased arm swing, masklike faces
postural abnormalities
Extrapyramidal Symptoms (EPS) -Pseudoparkinsonism
Treatment /Recommendation for Pseudoparkinsonism
Lower antipsychotic dose if possible - SGA
Change to different drugs
- Low risk with SGAs and TGA
Antiparkinsonian medications (anticholinergics)
– Benztropine, trihexphenidyl, or procyclidine
Extrapyramidal Symptoms (EPS)-Tardive Dyskinesia
Tardive Dyskinesia (5%) Late onset: after 3 or more months of treatment Abnormal involuntary movements: - Often begins with tongue or fingers –> face -> limbs -> gait -> trunk -> posture - Tongue thrusting, fly catching, lateral jaw movement, abnormal hand movement - Can interfere with eating/swallowing Major risk factors:
-High doses, long duration of treatment, increased age, history of parkinsonian side effects
-https://www.youtube.com/watch?v=BRbjRctgj_k&list=PLz27Rlp3y6XvE3f-GYukCjfI5ArXjAoJ6&index=65
Extrapyramidal Symptoms (EPS)-Tardive Dyskinesia
Treatment / Recommendation for Tardive Dyskinesia
Remission: likely with prompt discontinuation of antipsychotic therapy
No treatment with proven efficacy
- suggestion: switch to an SGA or TGA
- clozapine?
Discontinue anticholinergic med if pt is taking concurrently (benztropine, trihexphenidyl, or procyclidine)
CNS Effects of Antipsychotics
CNS Effects
Drowsiness, sedation
Insomnia, agitation
Movement Disorders
Extrapyramidal symptoms
Neuroleptic Malignant Syndrome (NMS)
Seizures
All APs lower the seizure threshold, use with caution in patients with seizure disorder (typically dose related)
Higher risk with chlorpromazine and clozapine
Neuroleptic Malignant Syndrome
Life threatening neurologic emergency associated with a class of medications that block dopamine transmission
Characterized by fever, severe muscle rigidity, and autonomic and mental status changes
Incidence of 0.01-0.02% of pts treated with antipsychotics
Mortality estimated 10-20% (was 76% in 1960s)
Neuroleptic Malignant Syndrome
Pathophysiological mechanism
Antipsychotic-induced dopamine blockade likely plays a pivotal triggering role in the condition - central dopamine receptor blockade in the hypothalamus =
hyperthermia and other signs of dysautonomia
- Interference with nigrostriatal D2 blockade = rigidity, tremor
Neuroleptic Malignant Syndrome
Associated Medications
Neuroleptic agents
- Greater risk: High potency FGA (haloperidol, fluphenazine)
Other drugs with anti-dopaminergic activity
- eg, Antiemetic drugs – metoclopramide, promethazine, domperidone
Withdrawal of L-dopa or dopamine agonist therapy
Neuroleptic Malignant Syndrome
Onset of symptoms
Within first two weeks of initiation or change in dose of neuroleptics
Predisposing factors
Increased use of higher doses, rapid dose escalation, a greater number of IM injections (long acting)
However, NMS usually occurs within the therapeutic dosage range of antipsychotics
Neuroleptic Malignant Syndrome
Tetrad of distinctive Clinical Features: (DSM-V Diagnostic Features)
ever
utonomic Instability
Severe Muscle igidity
ental status changes
Mental status changes
Rigidity Hyperthermia Autonomic dysfunction
o Analysis of 340 Cases: 70% of patients followed the symptoms below in order:
Neuroleptic Malignant Syndrome
Differential diagnosis Prime importance because NMS is a diagnosis of exclusion
Lab abnormalities Elevated serum CK >1000IU/L
Leukocytosis: WBC count 10,000 to 40,000/mm
Mild elevations of lactate dehydrogenase, alkaline phosphatase, liver transaminases
Electrolytes abnormalities: hypocalcemia, hypomagnesemia, hypernatremia, hyperkalemia, metabolic acidosis
Myoglobinuric acute renal failure resulting from rhabdomyolysis
Low serum iron conc
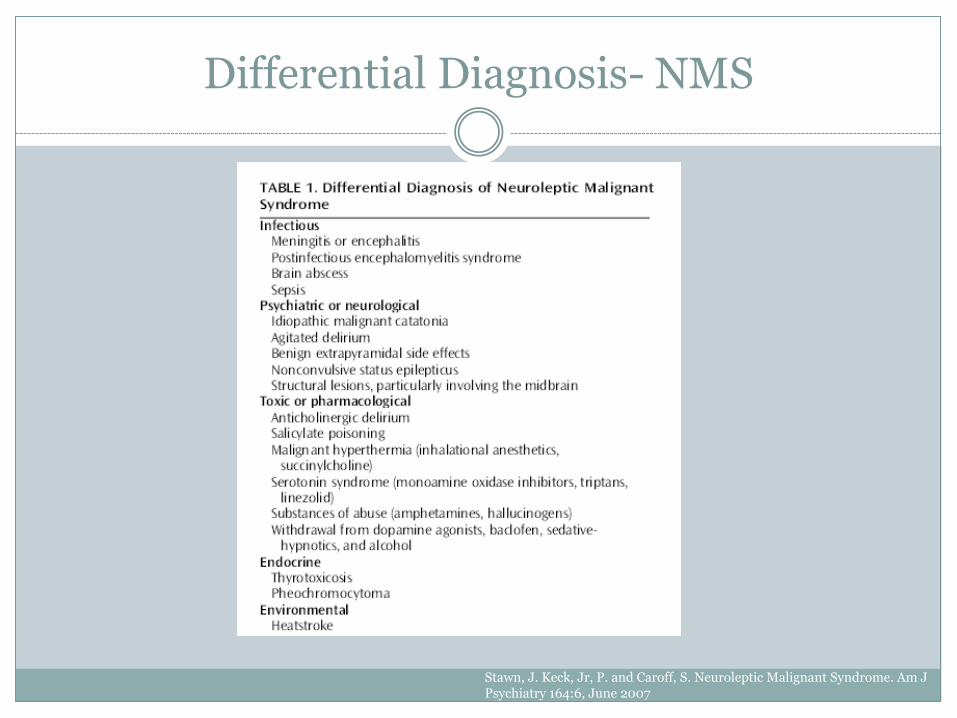
Differential Diagnosis- NMS
Stawn, J. Keck, Jr, P. and Caroff, S. Neuroleptic Malignant Syndrome. Am J Psychiatry 164:6, June 2007
Neuroleptic Malignant Syndrome
Treatment Discontinue antipsychotic drug (do not taper)
Supportive Care/Hydration
- eg. control of fever, intravenous fluid support, correction of electrolyte abnormalities
Use benzodiazepines to control agitation, if necessary
Specific pharmacotherapy:
- Dopaminergic agents
bromocriptine
amantadine
dantrolene (especially, for patients with extreme temperature elevations and rigidity)
ECT
Neuroleptic Malignant Syndrome
Drug Treatment for NMS Bromocriptine – start with 1 or 2.5mg doses. If ineffective,
increase to 15-20mg TID or QID
Amantadine – 100mg once daily to TID
Dantrolene – 4-8mg/day IV divided QID or 25-600mg/day PO
Once patients respond to drug treatment it should be continued for 1-2 weeks.
NMS- Prognosis
• Most episodes resolve within two weeks
• Reported mean recovery time 7-11 days
• Cases persisting for 6 months with residual catatonia and motor signs are reported
• Risk factors for a prolonged course: depot antipsychotic use and concomitant structural brain disease
• Most patients recover without neurologic sequelae except severe hypoxia or grossly elevated temperatures for long duration
NMS- Restarting Antipsychotics
Minimize risk by: Waiting for at least 2 weeks before restarting therapy
Using low-potency rather than high-potency drugs
Starting with low doses and titrating upward slowly
Avoiding concomitant lithium
Avoiding dehydration
Carefully monitoring for symptoms of NMS
CNS Effects of Antipsychotics
CNS Effects
Drowsiness, sedation
Insomnia, agitation
Movement Disorders
Extrapyramidal symptoms
Neuroleptic Malignant Syndrome (NMS)
Seizures
All APs lower the seizure threshold, use with caution in patients with seizure disorder (typically dose related)
Higher risk with chlorpromazine and clozapine
Seizures
Most agents lower seizure threshold and may produce seizures
Predisposing factors for antipsychotic induced seizures:
Pre-existing seizure disorder
Abnormal EEG without a history of seizure
Pre-existing CNS pathology
Rapid increases in antipsychotic dosage
Clozapine greatest risk of 2nd gen AP (dose dependent)
Organ Systems Affected by Antipsychotics
• Endocrine system
• Central nervous system CNS Effects
EPS
Neuroleptic Malignant Syndrome
Seizures
• Cardiovascular system
• Hepatic system
• Dermatologic system
• Hematologic system
• Genitourinary system
Cardiovascular Effects of APs
QTc prolongation
Tachycardia
Orthostatic hypotension
Cardiomyopathy (reported with clozapine)
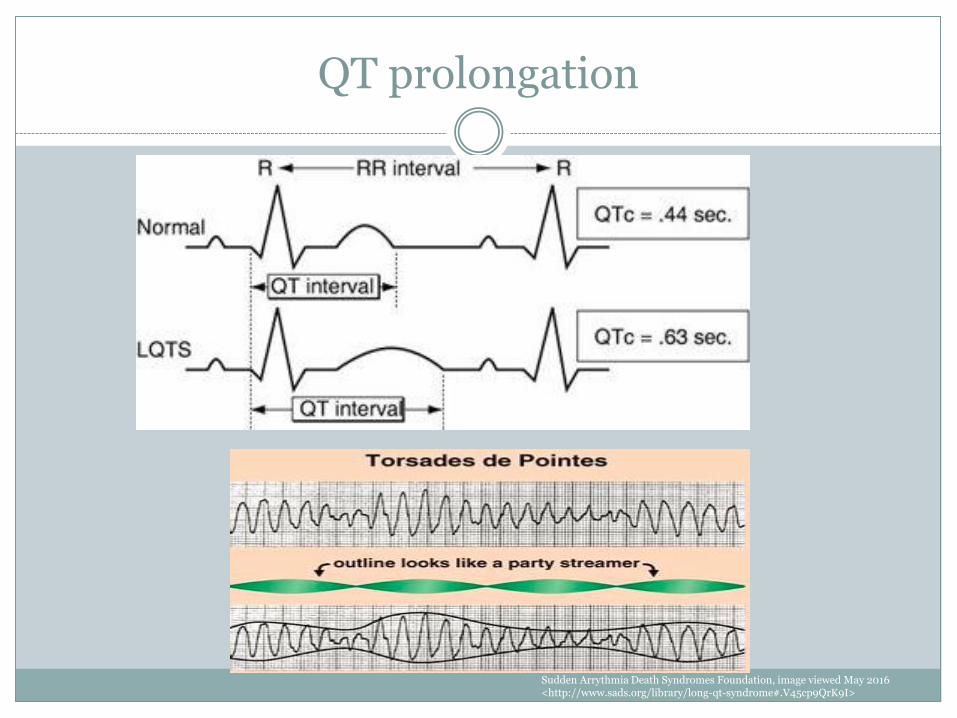
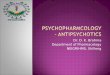
QT prolongation
Sudden Arrythmia Death Syndromes Foundation, image viewed May 2016 <http://www.sads.org/library/long-qt-syndrome#.V45cp9QrK9I>
Normal QTc intervals
• Mean daily variation is approximately 75msec
• Males: Prolonged if >440msec
• Female: Prolonged if >450msec
• Or any increase of >40ms from baseline for either gender
• If >500ms, at increased risk for Torsade de pointes (4x greater risk)
Risk Factors for QTc prolongation
• Hypokalemia
• Hypomagnesemia
• Age
• Female sex
• Advanced heart disease
• Congenital and acquired long-QT syndromes
• Family history of sudden death
• Anorexia
• Bradycardia
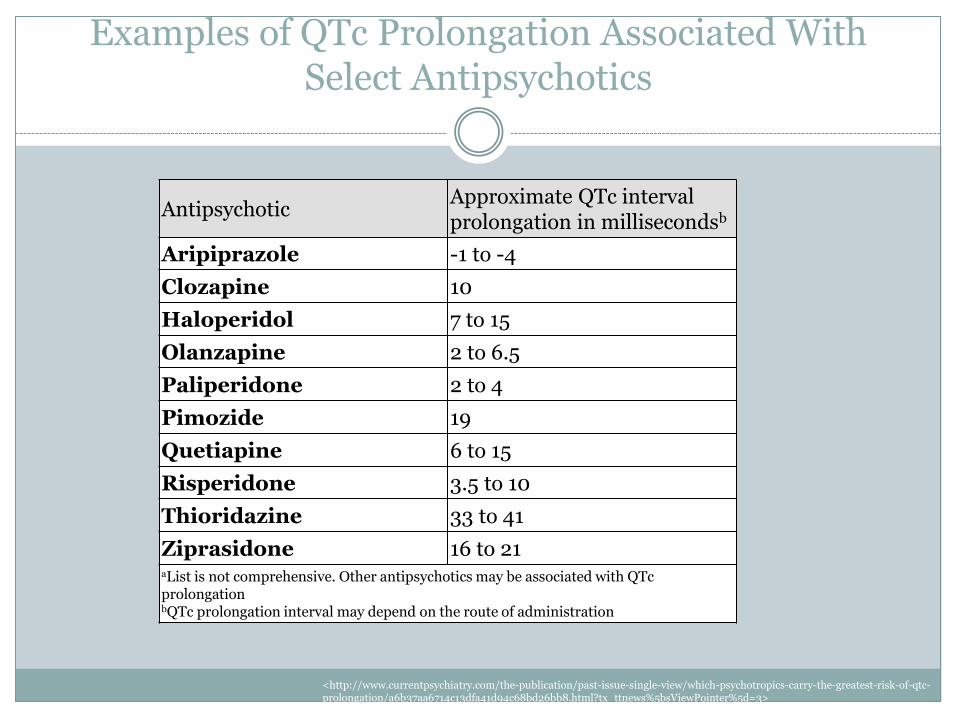
Examples of QTc Prolongation Associated With Select Antipsychotics
Antipsychotic Approximate QTc interval prolongation in millisecondsb
Aripiprazole -1 to -4
Clozapine 10
Haloperidol 7 to 15
Olanzapine 2 to 6.5
Paliperidone 2 to 4
Pimozide 19
Quetiapine 6 to 15
Risperidone 3.5 to 10
Thioridazine 33 to 41
Ziprasidone 16 to 21 aList is not comprehensive. Other antipsychotics may be associated with QTc prolongation bQTc prolongation interval may depend on the route of administration
<http://www.currentpsychiatry.com/the-publication/past-issue-single-view/which-psychotropics-carry-the-greatest-risk-of-qtc-prolongation/a6b37aa6714c13dfa41d94c68bd26bb8.html?tx_ttnews%5bsViewPointer%5d=3>
Monitoring for QTc Prolongation
Obtain history for congenital or acquired long QT syndromes
Identify other QT prolonging medications (crediblemeds.org)
Obtain baseline ECG
If borderline prolongation or combining with other QT prolonging agents, obtain second ECG after initiation
Usually wait for steady state (3-5 days) before repeating
If concern, can repeat sooner
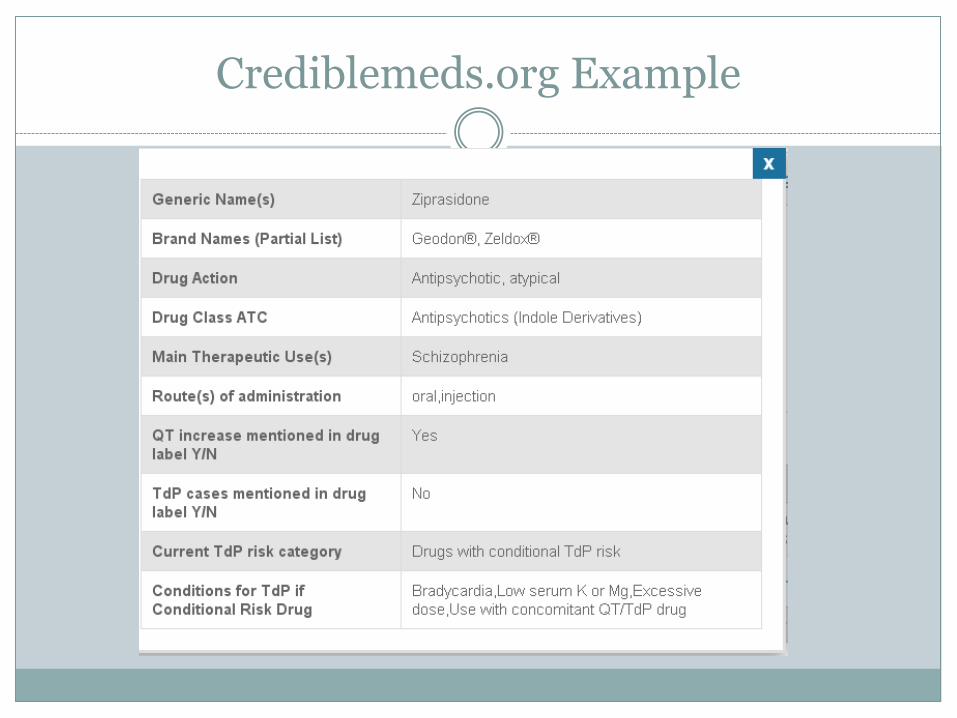
Crediblemeds.org Example
Recap: Objectives
Review of antipsychotic pharmacology/uses
Discuss metabolic side effects of APs
Discuss movement side effects of APs
Highlight emergency reactions to APs
Determine monitoring/treatment for side effects
References
1. Alvarez PA, Pahissa J. QT alterations in psychopharmacology: proven candidates and suspects. Curr Drug Saf. 2010;5(1):97-104. 2. American Psychiatric Association. Desk Reference to the Diagnostic Criteria from DSM-5TM. London: American Psychiatric Publishing;
2013 3. Bezchlibnyk-Butler KZ, Virani AS. Clinical Handbook of Psychotropic Drugs for Children and Adolescents. 3rd ed. Ashland: Hogrefe &
Buber Publishers 4. Boyer EW, Shannon M. The Serotonin Syndrome. N Engl J Med 2005;352:1112-20 5. Boyer EW. Serotonin Syndrome. 2015 UpToDate [cited 2015 Sep 14] 6. Chouinard, G, Margolese HC. Manual for the Extrapyramidal Symptom Rating Scale (ESRS); Schizophr Res,2005 Jul 15;76(2-3):247-65.
Epub 2005 Apr 18 7. Consensus Development Conference on Antipsychotic Drugs and Obesity and Diabetes. Diabetes Care February 2004vol. 27 no. 2 596-601 8. Elbe, Dean et al. Clinical Handbook of Psychotropic Drugs for Children and Adolescents, 3rd edition, 2015 Hogrefe Publishing 9. Leucht S et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis.
www.thelancet.com Vol 382; September 14, 2013 10. Lieberman JA. Managing Anticholinergic Side Effects. Prim Care Companion J Clin Psychiatry. 2004; 6(suppl 2): 20-23. 11. Muench J, Hamer AM. Adverse Effects of Antipsychotic Medications. American Family Physician. March 1, 2010. Volume 81, No 5 12. Nielsen J, Graff C, Kanters JK, et al. Assessing QT interval prolongation and its associated risks with antipsychotics. CNS Drugs.
2011;25(6):473-490. 13. Pringsheim T. Extrapyramidal Symptoms Associated with Second Generation Antipsychotic Use 14. Strawn JR, Keck PE, Caroff SN. Neuroleptic Malignant Syndrome. AM J Psychiatry 164:6, June 2007 15. Taylor DM. Antipsychotics and QT prolongation. Acta Psychiatr Scand. 2003;107(2):85-95. 16. Vieweg WV. New generation antipsychotic drugs and QTc interval prolongation. Prim Care Companion J Clin Psychiatry. 2003;5(5):205-
215. 17. Weiden PJ. EPS Profiles: The Atypical Antipsychotics Are Not All the Same. Journal of Psychiatric Practice Vol. 13, No. 1. January 2007 18. Wenzel-Seifert K, Wittmann M, Haen E. QTc prolongation by psychotropic drugs and the risk of torsade de pointes. Dtsch Arztebl Int.
2011;108(41):687-693. 19. Wijdicks E. Neuroleptic malignant syndrome. 2015 UpToDate [cited 2015 Sep 14] 20. Yatham, LN et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) and international Society of CANMAT guidelines for
the management of patients with bipolar disoder: update 2013. Bipolar Disorders 2013: 15:1-44
Questions?