Embed Size (px)
Citation preview

J Phys Fitness Sports Med, 4(1): 17-29 (2015)DOI: 10.7600/jpfsm.4.17
JPFSM: Review Article
Physical exercise and renal function
Masato Suzuki
Received: December 20, 2014 / Accepted: February 2, 2015
Abstract The kidneys play an important role in regulating acid-base and water-electrolyte balance disturbances induced by exercise. In sports medicine, research on renal function during exercise in healthy individuals and athletes is less common than other areas of study such as the respiratory, circulatory, and neuromuscular systems as well as metabolism, since renal func-tion has no direct effect on athletic performance. In this study, we reviewed previous research results obtained in our laboratory and other studies as follows: 1) effects of exercise intensity on renal plasma flow and glomerular filtration rate; 2) effects of exercise intensity on plasma hormone responses and urinary excretion of water and electrolytes; 3) effects of aging on renal function following exhaustive exercise; 4) mechanisms underlying exercise-induced diuresis in healthy volunteers; 5) mechanisms underlying exercise-induced proteinuria (EIP) in healthy volunteers; and 6) effects of exercise combined with angiotensin-converting enzyme (ACE) inhibitor (ACE-I) on the progression of diabetic nephropathy (DN) in obese diabetic model rats. The number of obese diabetes patients is increasing in advanced countries, and the num-ber of hemodialysis (HD) patients per capita in Japan is the highest worldwide. Approximately 42% of patients with DN undergo HD treatment every year. However, regular exercise has not been positively recommended for patients with nephropathy despite being an essential clini-cal approach for patients with diabetes. Moreover, the ideal exercise regimen for patients with diabetes complicated by nephropathy has not been investigated much. Therefore, a future study should investigate exercise therapy for patients with DN.Keywords : renal function, exercise intensity, exercise-induced diuresis, proteinuria, diabetic ne-
phropathy
Introduction
The kidneys play an important role in maintaining physiological factors within the body such as pH, osmotic pressure, and electrolyte balance by excreting metabolic waste and noxious products, as well as excreting and reabsorbing water and electrolytes including Na+, K+, and Cl-. These functions are performed by excretion and reabsorption in the renal tubules and quantified as renal plasma flow (RPF) and glomerular filtration rate (GFR). Even if the amounts of excretable noxious products were to increase with an increase in metabolic rate, the RPF would be reduced during exercise. Therefore, physical exercise has a negative effect on the kidneys in terms of maintaining renal function. However, in sports medicine, research on renal function in athletes has been given less importance compared to other areas of study such as the respiratory, circulatory, and neuromuscular systems, as well as glucose and fat metabolism, since it has no direct influence on the performance of exercise. However, ex-ercise is also used in physical therapy for the treatment
of obesity, diabetes mellitus, and minor hypertension. In patients with minor nephritis in whom exercise is not restricted, knowledge of the correlation between exercise and renal function is essential. Although microalbumin-uria (MAU) is used as a useful index for the early detec-tion and diagnosis of diabetic nephropathy (DN), physical activity increases the excretion of MAU into the urine, and the evaluation of MAU of patients with diabetes is invaluable1,2). On the other hand, renal function is important in the maintenance of fluid-electrolyte balance even in healthy persons and athletes during exercise in warm conditions or in water. The purposes of this study are to review the previous literature, present some of our observations on renal function, and discuss the mechanisms underlying the changes in renal function and the roles of the kidneys during and/or after exercise.
Effects of exercise intensity on RPF and GFR
As the muscular oxygen requirement increases during exercise, the distribution of blood changes and blood flow is reduced to the internal organs, including the kidneys. Correspondence: [email protected]
The Jikei University School of Medicine, 3-25-8 Nishi-Shimbashi, Minato-ku, Tokyo 105-8461, Japan

18 JPFSM : Suzuki M
RPF and GFR decrease in response to increases in exer-cise intensity. However, the correlation between exercise intensity and GFR must differ to some extent from that of exercise intensity and RPF. Suzuki3) reported that RPF de-creased from 35% of V・O2max, whereas sodium thiosulfate clearance (Cthi), as one of the indicators of GFR, started to decrease at a V・O2max of 49%. According to the author4), creatinine clearance (Ccr), as an indicator of GFR, showed no immediate change after exercise within a V・O2max of 42.5-60.5%, although Ccr decreased to 47% and 45% im-mediately after a V・O2max of 83% and 100%, respectively. Poortmans5) also reported the absence of a change in GFR at low to medium exercise. However, studies3-5) have suggested that RPF and GFR during exercise were not af-fected by modifications in exercise duration. With regard to the recovery processes of RPF and GFR following exercise, studies3-5) have revealed that low-intensity exercise induced a smaller decrease in and more rapid recovery of RPF following exercise. However, us-ing radionuclide angiography, we6) confirmed that RPF decreased to 46.6% of the pre-exercise level immediately after, to 82.5% 30 min after, and to 78.9% 60 min after exhaustive bicycle ergometer exercise. Moreover, the no-table finding was no significant change in Ccr immediately after moderate intensity (60.5% V・O2max), but a significant increase in Ccr after low-intensity exercise (42.5% V・O2max) until 120 min into the recovery period. With regard to alterations of RPF and GFR, previous observations5,7,8) suggest that enhanced renal sympathetic nerve activity and an increase in catecholamine secretion induces modifications in RPF and GFR during the exer-cise and recovery periods. However, the role of the renin-angiotensin system (RAS) has not been confirmed with regard to the decrease in RPF in response to exercise7-9). Based on these previous studies3-5), it should be recom-mended that daily physical activity within the intensity range of 35-40% of V・O2max is permissible for patients with mild nephritis because RPF and GFR are not decreased during exercise within this intensity range.
Effects of exercise intensity on plasma hormone response and urinary excretion of water and electrolytes
Excretion of water and electrolytes into the urine fol-lowing exercise is affected by an individual’s state of hy-dration5) as well as exercise intensity and duration. In this study, we discuss the effects of exercise intensity. Plasma catecholamine10), angiotensin II (pAng II) and aldosterone (pALD) concentrations increase according to exercise intensity, and significant increases are shown at V・O2max values > 60.5%4). Serum electrolyte concentrations including Na+, K+, and Cl- also show significant increases only immediately after exercise with a V・O2max > 60.5%4). Urine volume (UV) and the urinary excretion of elec-trolytes are affected by changes in RPF, GFR, and plasma hormones related to the regulation of water-electrolyte
balances, which are disturbed by increases in exercise intensity. UV decreases immediately after higher intensity (80-100% V・O2max) exercise as well as decreases in RPF and GFR. Freund, et al.11) reported that changes in urine flow paralleled changes in GFR (r = 0.91, p < 0.001) fol-lowing exercise at 25, 40, 60, and 80% V・O2max. On the other hand, obvious effects of exercise intensity on the urinary excretion of solutes including electrolytes (Na+, K+, Cl-, and PO4
-), urea nitrogen (uUN), lactic acid (uLA-), and urine osmolality (Uosm) are mostly observed 30 min after exercise. Moreover, urinary excretions of UN, Cl-, Na+, and Uosm significantly decreased from low intensity to the highest intensity exercise, and the degrees of these decreases depended on exercise intensity4). Although a change in the urinary concentration of Na+ was largely accompanied by a change in the Cl- concentration (r = 0.756, p < 0.001) throughout exercise with submaximal intensity (80% V・O2max), a remarkable dissociation be-tween changes in the Na+ and Cl- concentrations in the urine was observed 30 min after exhaustive exercise. The reduction in urinary Cl- concentration was 3.6-fold com-pared to that of the Na+ concentration in urine observed 30 min after exhaustive exercise (100% V・O2max)12). At 30 min after exhaustive exercise, there were significant negative correlations between urinary Cl- (uCl-) and uri-nary PO4
- concentration (r = -0.549, p < 0.001) as well as and uCl- and uLA- (r = -0.722, p < 0.001). That is, the significant increases in LA- and PO4
- in the urine were ac-companied by a marked reduction in Cl- concentration in the urine 30 min after exhaustive exercise. The increase in uLA- concentration was due to the increase in blood LA- concentration, and it started to increase once blood lactate (bLA-) concentration exceeded 60 mg/dL (6.7 mM/L)12). Overproduction of LA- in the exercising muscle cell induced by severe exercise led to a pH reduction in the blood, which induced a lower HPO4
2- to H2PO4- con-
centration ratio (HPO42-/H2PO4
-) in the blood. We12) pos-tulated that H2PO4
- and LA- were excreted simultaneously into the renal tubules and resulted in a large concentration of anions in the tubular fluid, and that the ion balance in the tubular fluid might be maintained to enhance reab-sorption of Cl- in the tubule cells12). Later, we will discuss the correlations between enhanced reabsorption of Cl- and the remarkable excretions of albumin and low-molecular-weight proteins into the urine after exhaustive exercise. Meanwhile, no significant relationships between the urinary excretion of water and electrolytes and the plasma responses of hormones related to water-electrolyte bal-ance regulation were observed throughout the exercise of low to high intensity exercise4). However, a significant positive correlation (r = 0.693, p < 0.001) between plasma aldosterone and urinary K+ concentrations and a signifi-cant negative correlation (r = -0.563, p < 0.001) between pALD and urinary Na+ concentration were indicated throughout the moderate intensity exercise in a hot envi-ronment (32.9 ± 1.1°C)13). The renin–angiotensin–aldoste-

19JPFSM : Renal function during exercise
rone (RAA) system became activated and the antidiuretic hormone (ADH) concentration increased remarkably in response to heat exposure (temperature 70-75°C, rela-tive humidity 10-20%), and obvious correlations were observed between the urinary excretion of water and elec-trolytes and the responses of hormones related to the reg-ulation of water-electrolyte balance14). However, the role of these hormones including pAng II, pALD, and ADH, which increased after exercise at greater than submaximal intensity (> 80% V・O2max), is unclear4).
Effects of aging on renal function after exhaustive ex-ercise
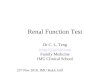
All body functions in healthy individuals decline lin-early starting at 30 years of age15). Poortmans et al.16) reported that the linear estimate of renal function loss averages 0.41% per year on the basis of a literature re-view of studies including 54,272 healthy, nonsmoking human participants of both genders. These studies15,16) also suggested that the older an individual, the greater the renal function impairment after exercise. Therefore, we17) examined the effects of aging on changes in renal function after exhaustive exercise in 162 healthy males 8-80 years of age. Voluntary exhaustive exercise18) was performed using a treadmill. Blood and urine samples were taken before, immediately after, and at 30 and 60 min after exercise. Urinary excretions of albumin (UAlb), lactic acid (ULA), electrolytes (Na+, Cl-, etc.), and Ccr were determined. Fig. 1 shows changes in Ccr (upper panel) and UAlb (lower panel) in different age clusters. The mean resting Ccr in teenagers was significantly low-er than that in adults 20-30 years of age, while the aver-age resting Ccr of participants > 45 years of age tended to decrease with age. The younger the subjects, the greater the reduction of Ccr immediately after exercise, and par-ticipants > 55 years old showed a smaller but significant reduction. The greater the reduction of Ccr, the higher the V・O2max, HRmax, systolic blood pressure (SBP), and bLA- concentration immediately after exhaustive exercise. Thirty minutes after exercise, UAlb remarkably increased in every age cluster. The resting UAlb value was subtracted from the UAlb at 30 min after exercise and defined as ⊿UAlb rec30 min. The value of ⊿UAlb rec30 min was converted to a logarithm that is shown in the lower panel in Fig. 1. ⊿UAlb rec30 min was significantly lower at a mean age of 12.9 (<15) years than mean age of 17.4 (16-19) years. The peak ⊿UAlb rec30 min was at 16-19 years of age and gradu-ally decreased with age. A highly positive correlation (r = 0.819, p < 0.001) was found between UAlb rec30 min and uLA- at 30 min after exercise. On the other hand, a significant negative coefficient of correlation (r = -0.722, p < 0.001) was shown between uCl- and uLA- concentrations. This study17) suggested that the organic acids (lactic acid [LA-] and pyruvic acid [PA-]), produced by exhaustive exercise, might alter renal glomerular permeability and/or inhibit
the reabsorption of albumin at the proximal tubules. We will describe the mechanisms underlying exercise-induced proteinuria (EIP) later. The effects of exercise on the kidneys may lessen with age due to a decreased capacity of energy production during exercise. In this regard, our hypothesis may agree with that of Poortmans et al.16), namely that the exercise impact on some renal functions is related to the absolute load imposed on the individuals.
Mechanisms underlying exercise-induced diuresis in healthy volunteers
The response of UV to exercise occurs as responses in RPF and/or GFR3,4,11), because UV is affected by renal function including RPF, GFR, and the reabsorption of water and other solutes in the renal tubules. However, UV increased 2-3-fold from pre-sprint levels as observed 15-
Fig. 1 Effects of aging on changes in creatinine clearance (Ccr) (upper panel) and urinary albumin excretion (⊿UAlb rec30 min) before and after exhaustive exercise17).
Ccr was measured as an indicator of the glomerular fil-tration rate (GFR).
Subtracting the value of UAlb at rest from the value of UAlb at 30 min after exercise gives ⊿UAlb rec30 min. The value of ⊿UAlb rec30 min was converted to a logarithm.
The data are expressed as the mean ± standard error (±SE). Significance of differences between two values measured: *p < 0.05, **p < 0.01, and ***p < 0.001.
Ccr
(ml/m
in/1
.73m
2 )
Resting
males n=162
**
807060504030201000
20
40
60
80
100
120
140
***********
******
Immediately after
⊿U
Alb
rec3
0 m
in (μ
g/m
in)
Age (years)80706050403020100
0
10
102
103
104**
*
**
****
*
Fig 1. Suzuki. M

20 JPFSM : Suzuki M
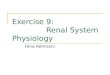
30 min after 200-400 m sprints, although it transiently decreased immediately after the sprints19,20). This phe-nomenon is termed “exercise-induced diuresis (EID)” or “post-exercise diuresis”19,20). However, the mechanisms underlying EID remain unclear. This study21) was performed to examine the mecha-nisms underlying EID caused by a 400 m sprint. The participants were seven healthy male volunteers with no history of cardiovascular disease (age, 22.6 ± 0.6 [± SE] years; weight, 66.5 ± 3.1 kg; height, 173.8 ± 2.2 cm). Each participant performed a 400 m sprint on a running track twice at 60-min intervals. The UV, Ccr, uLA-, uPA-, and other blood and urinary solutes as well as plasma antidiuretic hormone (pADH), pALD, adrenaline (pAd), and noradrenaline (pNorad) were measured before and after each sprint. Fig. 2 shows the responses of UV, Uosm, Ccr, and negative free water clearance (Tc
H2O) to the sprints and standing sessions. A 2.2-3.6 fold increase in UV over the respective pre-sprint level was observed after the first and second sprints. The change in the Uosm showed a mirror-image pattern to the UV change throughout the experiments. There was a negative linear relationship (r = -0.634, p < 0.001) between changes in UV and Uosm. Moreover, the Tc
H2O change occurred in a pattern very similar to that of UV after the first and second sprints. There was also a highly positive correlation coefficient (r = 0.899, p <
0.001) between the UV and TcH2O changes throughout the
experiment. However, the change in Ccr differed from those in UV, Uosm, and Tc
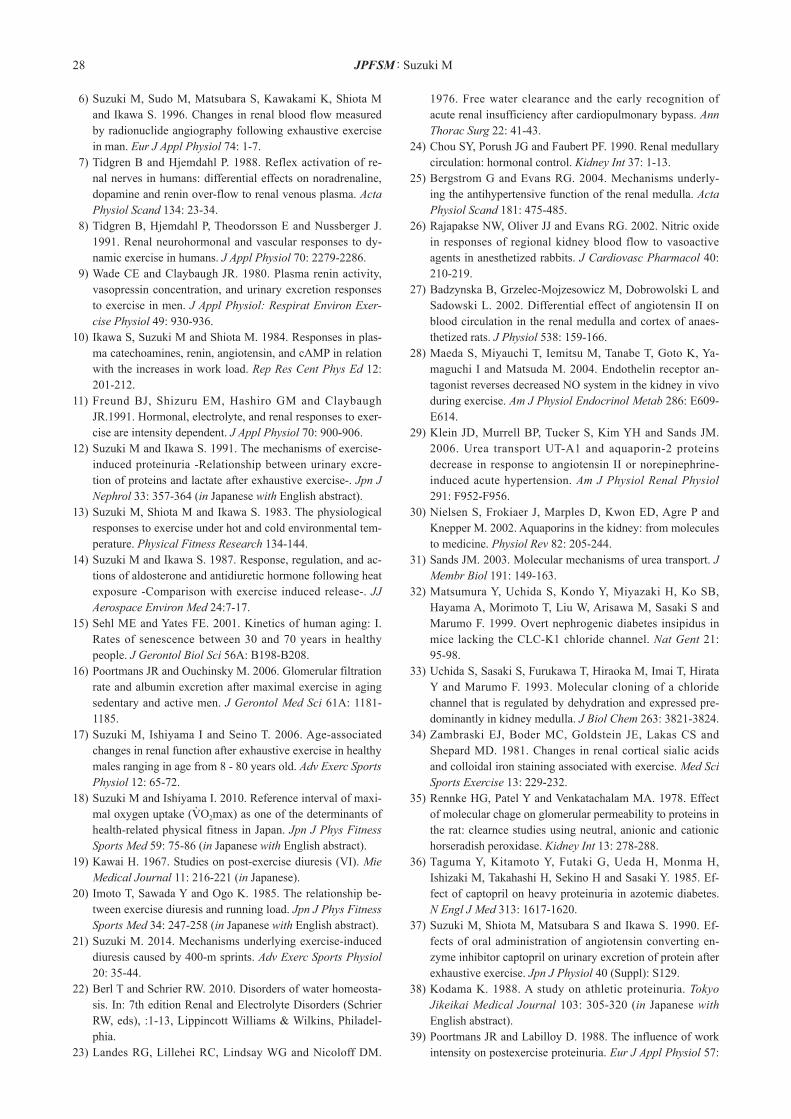
H2O. Fig. 3 shows the responses of urinary electrolytes and organic acids (uLA- + uPA-) to the sprint and standing sessions. The urinary Na+ (uNa+) and uK+ concentrations slightly decreased after the first and second sprints. However, the uCl- concentration decreased remarkably from 15 min to 45 min after both the first and second sprints, and gradually increased thereafter. In contrast, the uLA- and uPA- concentrations increased re-markably after both sprints, and there was a mirror-image pattern seen between uCl- and (uLA- + uPA-) changes throughout the experiment. A higher negative correla-tion coefficient (r = -0.852, p < 0.001) was seen among the uCl- and (uLA- + uPA-) changes. The large amounts of LA- and PA- produced by the sprints were thought to be filtered by the glomeruli and delivered into the renal tubules. Reabsorption of the excess organic acids was in-hibited at the renal tubules, and instead of anions such as LA- and PA-, Cl- were excessively reabsorbed in the renal tubules to maintain the ion balance therein. Inhibition of Cl- excretion may compete with organic acid excretion into the urine. After both sprints, urinary excretion of all of the solutes decreased, except for the organic acids (uLA- and uPA-). Among these solutes, the urinary urea nitrogen (uUN) concentration mostly decreased. The reduction in uUN
Fig 2. Suzuki. M
Uosm
500
700
900
1100
0 30 45 60 75 90 105 120 135 150
mO
sm/k
g ・H
2O
males n = 7
min
1st-sprint 2nd-sprint
: sprint: standing
0
1.2
2.4
3.6UV
mL/
min
males n = 71st-sprint 2nds-sprint : sprint
: standing
100
125
150
175
200Ccr males n = 7
1st-sprint
mL/
min
( 1.7
3 m
2 )
2nd-sprint
: sprint: standing*
mL/
min
0
1
2
3
4
0 30 45 60 75 90 105 120 135 150
males n= 7
min
2nd-sprint
: sprint: standing
1st-sprintTcH2O
~ ~
**
** *
* ***
*
*
**
***
**
****
**
***
*
~ ~
~ ~ ~ ~
### ###†
†
††
††
##
###
###
## ###
##
Fig. 2 Responses of UV, Uosm, Ccr, and TcH2O to the first and second 400 m sprints21)
Note: 1st -sprint, first 400 m sprint; 2nd -sprint, second 400 m sprint; sprint, 1st -400 m and 2nd -400 m sprint experi-ments; standing, 1st and 2nd standing experiments; UV, urine volume; Uosm, urinary osmolality; Ccr, creatinine clearance; Tc
H2O, negative free water clearance. The data are expressed as the mean ± standard error (±SE). *p < 0.05, **p < 0.01, and ***p < 0.001, compared with
the pre-1st-sprint level; ##p < 0.01 and ###, p < 0.001 compared with the pre-2nd -sprint level; †p < 0.05, ††p < 0.01, and †††, p < 0.001 compared with the values at the corresponding times in the sprint experiments.

21JPFSM : Renal function during exercise
accounted for 89.6-92.6% of the decreased Uosm after the first and second sprints. On the other hand, there were no correlative changes between the pADH and UV or pADH and Uosm, although there was a higher negative correlation coefficient (r = -0.699, p < 0.01) between the ratio of Uosm to serum osmolality (Sosm) (Uosm/Sosm) and changes in UV throughout the experiments. The notable and contradic-tory finding of a very similar pattern of change between Tc
H2O and UV (r = 0.899, p < 0.001) after the first and second sprints was observed in this study (Fig. 2). Tc
H2O is an indicator of water reabsorption in the renal tubules22,23). Increased Tc
H2O, which is a decrease in free water clear-ance (CH2O), would result in decreased UV. However, as shown in Fig. 2, the increase in UV was accompanied by an increase in Tc
H2O after the first and second sprints. The Tc
H2O equation was transformed to the following equa-tion22,23): Tc
H2O = UV × (Uosm/Sosm - 1). In this study, the correlation coefficients between Tc
H2O and UV and be-tween UV and (Uosm/Sosm - 1) were 0.899 and -0.771(p < 0.001 both), respectively. Consequently, the contradictory finding of increased UV, despite the increase in Tc
H2O after the sprints, can be explained by the above equation. The value of (Uosm/Sosm - 1) decreased because of a decrease in Uosm and an increase in Sosm after the sprints. Considering the above mentioned findings, the de-creased Uosm and increased UV observed after the first
and second sprints were believed to be due to the im-paired concentrating ability of the renal medullary tubules and collecting ducts caused by supramaximal exercises. The medullary blood flow (MBF), the rate of which can be regulated independently of whole-kidney blood flow, may also affect the renal capacity to both concentrate and dilute urine because preservation of the medullary hypertonicity in the interstitium is dependent on the countercurrent exchange mechanism in the vasa recta24). Approximately 90% of the blood flow delivered to the kidneys remains in the renal cortex to perfuse the peritu-bular capillary bed, whereas only 5-10% of the total renal blood flow reaches the renal medulla via vessels arising from the post-glomerular vasculature of the inner corti-cal or juxtamedullary nephrons22). The effect of Ang II on the MBF is of particular interest because, despite its vasoconstrictor effect, it may elicit paradoxical medullary vasodilatation effects in normotensive animals25,26). MBF increases in response to potent vasoconstrictors such as Ang II22), vasopressin (ADH), or endothelin, whereas cor-tical blood flow (CBF) decreases25-27). Ang II stimulates the medullary production of vasodilators such as prosta-glandins (PGs), nitric oxide (NO), and reactive oxygen species (ROS)25-27); consequently, the interaction of Ang II with these substrates plays an important role in MBF control. Increased MBF may decrease the medullary in-
Fig. 3 Responses of urinary concentrations of electrolytes (uCl-, uNa+, uK+) and organic acids ( uLA- + uPA-) to the first and second 400 m sprints21)
Note: 1st-sprint, first 400 m sprint; 2nd-sprint, second 400 m sprint; sprint, 1st-400 m and 2nd-400 m sprint experi-ments; standing, 1st and 2nd standing experiments; uCl-, urinary chloride; uNa+, urinary sodium; uK+, urinary potas-sium; uLA-, urinary lactic acid; uPA-, urinary pyruvic acid; uLA- + uPA-, the sum of uLA- and uPA+
The data are expressed as the mean ± standard error (±SE). *p < 0.05, **p < 0.01, and ***p < 0.001, compared with the pre-1st-sprint level; ##p<0.01 and ###, p<0.001 compared with the pre-2nd-sprint level; †p<0.05, ††p<0.01, and†††, p<0.001, compared with the values at the corresponding times in the sprint experiments.
0
100
200
300
0
100
200
300
0 30 45 60 75 90 105 120 135 150
0
100
200
300males n = 7
1st -sprint
mm
ol/L
2nd-sprint
min
uK+males n= 7
min
1st-sprint
mm
ol/L
2nd-sprint
uNa+males n = 7
1st-sprint
mm
ol/L
2nd-sprint
: sprint: standing
: sprint: standing
: sprint: standing
uCl-
*** ***
***
*** ***
***
*
~ ~
******
***** *** * *~ ~~ ~
0 30 45 60 75 90 105 120 135 150
uLA-+uPA-males n = 7
1st-sprint
mm
ol/L
2nd-sprint : sprint: standing*** ***
*** ******
***
***
~ ~
0
100
200
300
######
###
#########
## ###
††††††
††† ††† ††††
††† †††
Fig 3. Suzuki. M

22 JPFSM : Suzuki M
tion of the renal arterioles5,7,8). The exercise-induced RPF reduction produces a concomitant effect on the GFR3,5). Moreover, the filtration fraction (FF; GFR/RPF) increases because the GFR decreases relatively less than the RPF during exercise. The increased FF probably enhances the diffusion process of macromolecules into the tubular lu-men. Previous studies34,35) suggest that exercise decreases the glomerular electrostatic barrier and, thereby, could partly explain the enhanced transglomerular passage of macromolecules. On the other hand, the intravenous infu-sion of Norad or Ang II reportedly produced proteinuria, while the oral administration of ACE-I reduced protein-uria in patients with nephropathy36). According to these studies, exercise-induced modifications of renal hemo-dynamics and the FF as well as activation of the renal sympathetic nerve and the RAS are thought to directly or indirectly increase permeability of the glomerular capil-lary membrane to proteins. However, the causes of in-creases in LMWP, such as α1-M and β2-M, concomitantly observed following exhaustive exercise, may not be suf-ficiently explained only by advanced permeability of the glomerular capillary membrane to proteins including high to medium molecular weight proteins. Therefore, we37) tried to confirm that exhaustive ex-ercise produces no increase in urinary excretion of glo-merular type protein, such as Alb, in a state of inhibited increase in pAng II after oral ingestion of ACE-I. We simultaneously observed whether the urinary excretion of tubular-type proteins such as α1-M and β2-M increases after exhaustive exercise. According to the previous study by Kodama et al.38), we used captopril (Capt) as an ACE-I37). Ten healthy male volunteers with no history of any diseases who were 21.6 ± 1.0 (± SD) years of age, weighed 69.7 ± 3.5 kg, and were 175.3 ± 1.7 cm tall participated in this study37). The participants provided informed consent in accordance with the Declaration of Helsinki under careful supervi-sion, including a medical history interview prior to test-ing and the monitoring of electrocardiography and blood pressure throughout the experiment. The subjects were orally administered Capt 50 mg (Sankyo, Tokyo, Japan) in a fasting state the morning after an overnight fast. Thirty minutes later, a maximal voluntary exercise test for 10-12 min was performed using a treadmill. Plasma renin activity (PRA), pAng II, pAd, pNorad, and bLA- concentrations, and urinary excretions of glomerular type proteins such as uAlb and uTP, and tubular-type proteins such as α1-M and β2-M were observed throughout the ex-periment. Fig. 4 shows the responses of plasma hormones (pAd, pNorad, Ang II, PRA), Ccr and urinary proteins (Total protein, uTP; uAlb, β2-M) to exhaustive exercise with administration of Capt and without Capt administration. There were no differences in responses of pAd and pNo-rad following exhaustive exercise between Capt adminis-tration (Capt treatment) and control experiment (without
terstitial osmotic gradient, causing changes in the osmotic forces. In this study21), levels of vasoconstrictors such as pADH and pNorad were measured, whereas the plasma vasoconstrictor Ang II and vasodilator factors such as PGs, NO, and ROS were not. However, many studies9-11) have reported that plasma vasoconstrictors such as the components of the RAS, ADH, and catecholamines in-crease in response to increased exercise intensity. Maeda et al.28) reported that acute exercise enhanced renal tissue RAS, but they did not measure RAS in the tissues of the renal cortical and medullary sites separately. Furthermore, Klein et al.29) reported that the administration of high doses of Ang II or Norad to male Sprague-Dawley rats increased UV and decreased Uosm, urea transporter (UT)-A1, and water channel protein aquaporin-2 (AQP2) in the inner medullary region of rats. UT-A1 is a major protein responsible for reabsorbing urea and NaCl and contribut-ing to the generation of a hypertonic renal medulla, while AQP2 is a major protein regulating water permeability in the collecting duct30,31). Matsumura et al.32) indicated that the chloride channel-K1 (ClC-K1) plays a role in urine concentration and that the countercurrent system in the inner medulla is involved in the generation and mainte-nance of a hypertonic medullary interstitium. The same study32) reported that a specific Cl channel blocker de-creased Cl permeability in the thin ascending limb (TAL). The findings of Matsumura et al.32) and Uchida et al.33) suggest that the remarkable decrease in Cl concentration in the tubular fluid of the TAL contributed to lower med-ullary hypertonicity in the interstitium, and resulted in the observed decrease in Uosm 15 and 30 min after the sprints. The present study’s findings indicated that EID might result from reduced urine concentrating ability, which could be due to washout of the renal medullary interstitial osmotic gradient caused by the increased renal MBF (itself mediated by increased levels of vasodilators released in response to the increased levels of vasoconstrictors) and the remarkable decrease in uCl- concentration after supra-maximal 400 m sprints.
Mechanisms underlying EIP in healthy volunteers
EIP is related to exercise intensity. The maximal rate of protein excretion usually occurs during the first 20-30 min after the cessation of exercise with levels over 70-80% of maximal oxygen intake (V・O2max). EIP involves large to medium molecular weight proteins such as immuno-globulin A, immunoglobulin G, albumin (Alb), total pro-tein (TP), and lower molecular weight proteins (LMWP) such as α1-microglobulin (α1-M) and β2-microglobulin (β2-M). EIP is a mixed glomerular-tubular type due to an increased glomerular permeability and a partial tubular-reabsorption inhibition of LMWP when heavy exercise is performed. It has long been recognized that a reduction of RPF is induced by activation of renal sympathetic nerve and the RAS during exercise, which induces vasoconstric-

23JPFSM : Renal function during exercise
UAlb, and Uβ2-M) between the Capt treatment and control groups; that is, despite the increase in pAng II being in-hibited after oral administration of Capt, a remarkable excretion of mixed glomerular-tubular type proteins was observed in the urine 30 min after exhaustive exercise. Therefore, this study’s findings37) suggest that Ang II does not play an important enough role to induce proteinuria after exhaustive exercise in healthy subjects, since the level of urinary excretion of proteins after exhaustive exercise at a lowered concentration of pAng II caused by
Capt administration). However, PRA gradually and significantly increased up to 30 min after the oral administration of Capt and slightly decreased thereafter, while pAng II also significantly in-creased immediately after exhaustive exercise. However, an increased level of pAng II in the Capt treatment was approximately 45% of that in the control, and this level was comparable with that observed after 60.5% V・O2max intensity exercise4). There were no significant differences in changes of Ccr and urinary excretion of proteins (UTP,
UTPmg/crmg UAlbmg/crmg
Uβ 2-Mµg/crmgml/min
***
Ccr
***
*** *
PRAng/ml/hr
**
***
***
***
** **
pAngIIpg/ml
***
pAdng/ml pNorad: Cont-experiment: Capt-treatment
males n=10ng/ml
0
20
40
60
0
20
40
60
80
100
**
-30 B 30 60 minA -30 B 30 60 minA
***
0
0.05
0.10
0.15
0.20
-30 B 30 60 minA0
1.0
2.0
3.0
-30 B 30 60 minA
*
***
** *
**
*
*
*
0
200
400
600
800
1000
0
200
400
600
800
*
***
*
***
*
******
B 30 90 minA 60 B 30 90 minA 60
0
4
8
12
B 30 90 minA 60
***
*50
80
110
140
B 30 90 minA 60
*** ***
***
Fig 4. Suzuki M
Capt50 mg
Capt50 mg Capt
50 mg
Capt50 mg
Capt50 mg
Capt50 mg
-30 -30
Capt50 mg
Capt50 mg
-30 -30
#
#
###
###
###
Fig. 4 Changes in plasma hormone concentrations (pAd, pNorad, pAngII, PRA), urinary excretion of proteins (UTP, UAlb, Uβ2M) and Ccr following exhaustive exercise with and without the administration of Capt.
Note: B, before exhaustive exercise; A, directly after exhaustive exercise; pAd, plasma adrenarine; pNorad, plasma noradrenaline; pAng II, plasma angiotensin II ; plasma renin activity (PRA); UTP, urinary excretion of total protein; UAlb, urinary excretion of albumin; Uβ2M, urinary excretion of β2-microglobulin; Ccr, creatinine clearance.
The data are expressed as the mean ± standard error (±SE). *p < 0.05, **p < 0.01, and ***p < 0.001, compared with the resting level; #p<0.05, ###p<0.001, compared with the values at the corresponding times in the Cont-experiment.

24 JPFSM : Suzuki M
increases in the urinary excretion of proteins including α1-M, β2-M, uAlb, and uTP following exhaustive exercise than those in the L-uAlb group. It should be noted that the uAlb in the H-uAlb group increased about 10-fold com-pared to that of the L-uAlb group from 30 to 60 min after exercise, although there was no significant difference in the changes of UV and Ccr following exercise between the H-uAlb and L-uAlb groups. However, as shown in Table 2, there were no differences in increases in pAd, pNorad, and pAng II concentrations immediately after exercise between these groups, although the H-uAlb group showed significant higher bLA- concentration immediately and 30 min after exercise than the L-uAlb group. Remarkable differences in the previously mentioned variables observed between the H-uAlb and L-uAlb groups were urinary Cl- and uLA- concentrations at 30 min after exercise and bLA- concentration measured im-
oral administration of Capt was the same as that at higher pAng II concentration without Capt treatment. On the other hand, we12) noticed two groups, one of which showed remarkable excretion of urinary proteins, while the other produced less excretion, although pAng II, pAd, and pNorad concentrations increased to the same levels in both groups after exhaustive exercise. Among the 69 healthy male volunteers who performed the ex-haustive exercise12), we selected two groups of 20 sub-jects, one of which showed the highest excretion of uAlb (H-uAlb, n=20) and the other showed the lowest excre-tion of uAlb (L-uAlb, n=20). Subsequently, to estimate the mechanisms underlying EIP, we compared the levels of V・O2max, bLA, pAng II, pAd and pNorad concentrations, Ccr, uAlb, α1-M, β2-M, electrolytes (Na+, K+, Cl-, PO4
-) and uLA- after exhaustive exercise in both groups. As shown in Table 1, the H-uAlb group showed significantly higher
Table 1. Responses of UV and urinary excretion of proteins (α1-M, β2-M, Alb and TP) in the H-UAlb and L-UAlb groups to exhaustive exercise
pre-ex
H-UAlb (n=20)L-UAlb (n=20)
UAlb µg/min
UV ml/min
β2-M µg/min
α1-M µg/minH-UAlb (n=20)
L-UAlb (n=20)
UTP µg/min
H-UAlb (n=20)
L-UaAlb (n=20)
H-UAlb (n=20)
L-UAlb (n=20)
H-UAlb (n=20)
L-UAlb (n=20)
0.55 ± 0.340.49 ± 0.18
0.86 ± 0.530.75 ± 0.38
0.46 ± 0.160.56 ± 0.24
rec 60 minrec 30 minpost-ex
0.75 ± 0.480.62 ± 0.28
20.6 ± 21.4(3.5~77.7)10.2 ± 10.3
(0.8 ~ 41.8)
148.9 ± 294.7(1.3~1145.3)96.3 ± 107.5(3.1~347.7)
1208.6 ± 1111.9(573.5~5586.0)
125.6 ± 80.8(17.3~234.2)
152.4 ± 184.4(12.6~737.8)
16.3 ± 10.7(7.3~48.1)
4.0 ± 3.6(0.6~16.4)
3.1 ± 2.2(0.4~ 7.5)
3.8 ± 3.9(0.4~14.6)
6.1 ± 5.4(0.9~22.5)
43.6 ± 25.9(14.9~120.5)
22.8 ± 14.0(2.5~56.2)
6.5 ± 8.0(0.9~36.2)
3.1 ± 2.6(0.6~10.4)
0.12 ± 0.10(0.02~0.43)0.07 ± 0.05
(0.01~0.14)
0.45 ± 0.89(0.01~3.66)0.79 ± 1.52
(0.01~6.73)
9.71 ± 10.81(0.08~41.07)
5.03 ± 6.50(0.03~24.95)
0.79 ± 1.14(0.04~5.32)0.47 ± 0.99
(0.03~4.54)
79.7 ± 58.6(19.1~241.3)
77.2 ± 50.9(24.4~188.7)
217.3 ± 404.9(29.9~1853.6)200.6 ± 167.8(21.6~587.4)
1245.7 ± 531.7(697.6~2265.4)
341.8 ± 187.8(75.5~761.5)
223.9 ± 229.2(37.8~1010.2)
96.2 ± 58.8(40.9~244.8)
Table 1. Suzuki. M
*** **
*
***
***
**
*** ***
***
*****
***
***
*
** *
****
***
***
*
UV, urine volume; α1-M, α1-microglobulin; β2-M, β2-microglobulin; UAlb, urinary albumin excretion; UTP, urinary total protein excretion. The data are expressed as the mean ±standard deviation (±SD). *<0.05, **p<0.01, ***p<0.001, compared to pre-exercise level, and difference between two groups.
Table 1. Responses of UV and urinary excretion of proteins (α1-M, β2-M, Alb and TP) in the H-UAlb and L-UAlb groups to exhaustive exercise
UV, urine volume; α1-M, α1-microglobulin; β2-M, β2-microglobulin; UAlb, urinary albumin excretion; UTP, urinary total protein excretion. The data are expressed as the mean ± standard deviation (±SD). *<0.05, **p<0.01, ***p<0.001, compared to pre-exercise level, and difference between two groups.

25JPFSM : Renal function during exercise
mediately after exercise. The uCl- in the H-uAlb group was reduced by 81.5% from resting level, although the L-uAlb group showed a reduction of only 57.4% at 30 min after exhaustive exercise. There was a significant differ-ence (p < 0.001) in uCl- measured at 30 min after exercise between groups. On the other hand, the uLA- concentra-tion measured at 30 min after exercise was significantly higher in the H-uAlb group than in the L-uAlb group. There was a relationship between uLA- and bLA- changes as follows: uLA- = 8.7e0.046・bLA- (r = 0.926, p < 0.001). Moreover, there was a significantly high correlation co-efficient (r = 0.995, p < 0.001) between urinary cation (Na+ + K+) and anion (Cl- + PO4
- + LA-) concentrations. As shown in Fig. 5, higher coefficients of correlation were indicated between uAlb, uβ2-M, and uLA- concentrations. These variables were converted into logarithmic (log) values and are illustrated in Fig. 5. According to the fact that oral administration of ACE-I inhibited an increase in uAlb in patients with nephropa-thy36), it is possible that an increase in glomerular-type proteins such as albumin might be primarily caused by enhanced glomerular membrane permeability due to in-creased Ang II levels. However, EIP involves not only glomerular-type, but also tubular-type proteins such as α1-M and β2-M. The mechanisms underlying the elevated excretion of tubular-type proteins after exhaustive exer-cise could not be explained only by enhanced glomerular membrane permeability caused by increased Ang II. Moreover, there were two characteristic findings observed after exercise, one of which was remarkable excretion of mixed glomerular-tubular type proteins into the urine
Table 2. Responses of blood lactate (bLA), plasma adrenaline (pAd), noradrenaline (pNorad) and angiotensin II (pAngII) concentrations to exhaustive exercise in the H-UAlb and L-UAlb groups.
The data are expressed as the mean ± standard deviation (±SD): significance of differences compared to pre-exercise values and difference between two groups: * p<0.05, ** p<0.01, *** p<0.001
H-UAlb (n=20)L-UAlb (n=20)
H-UAlb (n=20)L-UAlb (n=20)
H-UAlb (n=20)L-UAlb (n=20)
H-UAlb (n=20)L-UAlb (n=20)
12.0 ± 4.910.2 ± 2.7
0.015 ± 0.0080.027 ± 0.016
0.132 ± 0.0580.130 ± 0.044
16.9 ± 12.717.8 ± 10.5
bLA- mg/dl
pAd ng/ml
pNorad ng/ml
pAng II pg/ml
105.3 ± 13.790.1 ± 19.3
0.100 ± 0.0880.110 ± 0.121
1.123 ± 0.9830.978 ± 0.677
71.1 ± 35.571.8 ± 39.7
post-ex rec 30 minpre-ex
59.3 ± 24.842.0 ± 18.3
0.023 ± 0.0150.029 ± 0.024
0.204 ± 0.1180.205 ± 0.112
30.5 ± 24.922.8 ± 12.0
***
***
***
***
******
***
***
***
***
***
*** *
** *
Table 2. Suzuki. M
Table 2. Responses of blood lactate (bLA-), plasma adrenaline (pAd), noradrenaline (pNorad) and angiotensin II (pAngII) concentrations to exhaustive exercise in the H-UAlb and L-UAlb groups.
The data are expressed as the mean ± standard deviation (±SD): significance of differences compared to pre-exercise values and difference between two groups: * p<0.05, ** p<0.01, *** p<0.001
0
1
2
3
4
5
0
1
2
3
4
5
4.03.02.01.00
log [uAlb]
log [uLA-]
n=236 r=0.741
(p<0.001)
µg/ml
µg/l log [uβ2M]n=236 r=0.717
(p<0.001)
mg/dl
Fig 5. Suzuki. M
Fig. 5 Relationships between urinary concentrations of lactic acid (uLA-) and β2-microglobulin (uβ2-M) and albumin (uAlb) before and after exhaustive exercise.
The values of these variables were converted to a loga-rithm and plotted.

26 JPFSM : Suzuki M
to the animals placed on food-restriction in Otsuka Long-Evans Tokushima Fatty (OLETF) rats, which is an animal model of obesity-induced diabetes, the use of an exercise regimen significantly increased the uAlb and kidney weight and enlarged the glomerular and mesangial ar-eas44), although improvements in glucose tolerance and lipid metabolism were seen in both the food-restriction and exercise regimen groups. The progression of nephrop-athy accompanied by an exercise regimen alone might be caused by increased blood pressure (BP) during exer-cise, because the exercise group showed a significantly higher BP than that in the diet regimen group throughout the treatment44). However, some studies45,46) have shown that diet yields a smaller improvement in insulin resis-tance than exercise does, although diet alone is sufficient for decreasing lean body mass. Moreover, our previous study47) suggested that exercise intervention might be an essential option for the improvement of serum lipids since diet alone is not effective. On the other hand, some studies48,49) suggest that the administration of the antihypertensive drug azelnidipine (Azel), a calcium channel blocker, is attractive not only for treating hypertension with accompanying diabetic complications, but also for preventing the development of DN. Therefore, we50) examined the effect of Azel alone or in combination with exercise on BP, kidney morphol-ogy, and urinary protein excretion in OLETF rats. Using 24 male OLETF rats and six normal control Long-Evans Tokushima Otsuka (LETO) rats, these treatments were performed from 21 to 30 weeks of age, an appropriate developmental stage for an exercise regimen for DN. OLETF rats were evenly divided into the following groups: sedentary (OLETF-Sed), Azel (OLETF-Azel), exercise (OLETF-Ex), and Azel plus exercise (OLETF-Azel & Ex). Azel (10 mg/kg/day) was administered in the chow; animals in the exercise groups exercised vol-untarily every day on a rotator wheel (Shinano, Tokyo, Japan), and their running distances were recorded weekly. All groups were allowed access to tap water ad libitum. The effects of 10 weeks of exercise alone and in combi-nation with Azel on BW, BP, glucose tolerance, serum lipid concentrations, kidney morphology, uAlb, and uTP were examined in this study50). Exercise treatment alone decreased BW and improved dyslipidemia and glucose intolerance (GI), but did not decrease BP. Azel treatment alone prevented an increase in SBP in OLETF rats, but did not significantly reduce it. Kurashige et al.51) noted an approximately 80 mmHg decrease in SBP in stroke-prone SHR when Azel 10 mg/kg/day was administered by a technique called oral gavage from 20 to 31 weeks of age. In our study50), Azel was added to the powdered rat chow. This difference in the method of Azel administration might be responsible for the lack of a significant decrease in BP by Azel treatment alone in this study50). Azel treat-ment alone inhibited an increase in BW and decreased serum triglyceride concentration, but did not improve GI.
despite the fact that the increase in pAng II concentration was significantly inhibited after exercise by oral admin-istration of Capt prior to exercise. The other finding was that there were two groups, one of which showed remark-able excretion of uAlb (H-uAlb) and the other produced less excretion (L-uAlb), although pAng II concentration increased to the same level in both groups after exhaus-tive exercise. According to these findings, it seems that elevated pAng II does not play an important enough role to pro-duce a mixed type of proteinuria after exhaustive exercise in healthy subjects. Our previous studies12,37) suggested that an increase in bLA- concentration and a remarkable excretion of LA- into the urine produced by exhaustive exercise are involved in the appearance of postexercise proteinuria, which is a mixed glomerular-tubular type. Meanwhile, Poortmans et al.39) suggested that neither in-creased lactate ion nor decreased pH appears to be related to postexercise proteinuria based on the fact that Cantone et al.40) failed to observe any increase in protein excretion in a resting state during the infusion of a lactate solution leading to 15 mmol/L in the blood. On the other hand, Gardner41) reported that urinary protein excretion in-creased in acidosis by an infusion of 1% NH4Cl solution, and was inhibited in alkalosis. It might be estimated that glomerular membrane per-meability to proteins may be due to changes in charge selectivity in the glomerular basement membrane (GBM). Zambraski et al.42) suggested that exercise may decrease the glomerular capillary electrostatic barrier in rats, and thereby may be an important factor in EIP. It is estimated that the degree of metabolic acidosis due to more in-creased bLA- after exhaustive exercise was significantly higher in the H-uAlb group, and resulted in more change in charge selectivity in the GBM in the H-uAlb than in the L-uAlb group. On the other hand, Poortmans et al.43) reported that the reabsorption of Alb and β2-M at the proximal tubules was inhibited by lysine perfusion in hu-mans. They43) concluded that post-exercise proteinuria is of mixed type after exhaustive short-term exercise, which increased glomerular permeability and partial tubular re-absorption inhibition of proteins. Our previous studies12,37) suggested that the large amounts of LA- and PA- produced by heavy exercise were filtered at the glomerulus, entered the tubular lumen, and inhibited reabsorption of Alb and β2-M at the proximal tu-bules. These may be the leading mechanisms underlying EIP in healthy volunteers, even though the precise mecha-nisms were not clarified.
Effects of exercise combined with ACE-I on the progres-sion of diabetic nephropathy in obese-diabetic model rats
An essential clinical approach for obese diabetes pa-tients is diet and exercise regimens. However, compared

27JPFSM : Renal function during exercise
ideal exercise therapy regimen for patients with DN since physical exercise has been restricted for these patients to date despite regular exercise being an essential clinical approach for obese patients with diabetes.
Conflict of Interests
The author declare that there is no conflict of interests regarding the publication of this article.
The combined treatment of Azel with exercise signifi-cantly decreased BW and BP and improved dyslipidemia and GI. Fig. 6 shows that UAlb did not change in any of the OLETF groups from 10 to 23 weeks of age; rather, it sig-nificantly increased in the OLETF-Sed and OLETF-Ex groups from 23 to 29 weeks of age (higher in the OLETF-Sed group) and was significantly lower in both the OLETF-Azel and OLETF-Azel & Ex groups compared to the OLETF-Sed and OLETF-Ex groups from 26 to 29 weeks of age. Azel, either alone or in combination with exercise, more effectively ameliorated indices of kidney damage, includ-ing mesangial area A
-(M), glomerular volume V
-(G), GBM
thickness, and UAlb and UTP values. In this study50), exercise alone was not as effective at attenuating the indices of nephropathy as was the combi-nation of exercise and Azel despite the fact that it signifi-cantly improved the lipid profile and glucose clearance. Exercise may also exhibit DN progression beyond the preventative effects produced by improvements in dyslip-idemia and glucose metabolism in the exercise treatment alone as observed in this study. Thus, one DN progressive factor may be an elevation in BP during exercise since the urinary excretion of proteins in the OLETF-Ex group was progressively increased during the exercise regimen. This study’s findings50) demonstrate that the combined treatment of regular exercise with the antihypertensive drug Azel produced improvements in GI and dyslipidemia in the absence of the progression of DN. In conclusion, further studies should investigate the
weeks10 15 20 23 26 29 300
5
10
15
20
25
30treatment periodpre-treatment
period
UAlb(mg/day)
X±SE
***
###
***
###
***
###
***
###
**
OLETF -Sed〃 -Ex〃 -Azel〃 -Azel&ExLETO -Sed
21
Fig. 6 Suzuki.MFig. 6 Effects of azelnidipine (Azel) and/or exercise (Ex) on urinary excretion of albumin (UAlb) The data are expressed as the mean ± standard error (±SE). ***p < 0.001, compared to the pre-treatment level (at 20
weeks of age); ###p < 0.001, compared to levels at the same age in OLETF-Azel and OLETF-Azel & Ex groups; *p < 0.05, compared to LETO-Sed group.
Acknowledgements
The author thank Mrs. Tohko Yasumatsu for calculating the data and creating the figures and tables.
References
1) Mogensen CE and Vittinghus E. 1975. Urinary albumin ex-cretion during exercise in juvenile diabetes. A provocation test for early abnormalities. Scand J Clin Lab Invest 35: 295-300.
2) Viberti GC and Keen H. 1984. The patterns of proteinuria in diabetes mellitus. Diabetes 33: 686-692.
3) Suzuki H. 1995. Exercise intensity and renal hemodynam-ics. Jpn J Nephrol 37: 534-542 (in Japanese with English abstract).
4) Suzuki M. 1987. Study on the diagnostic indices in renal function after exercise- Effects of exercise intensity on urinary concentrating ability after exercise in healthy male volunteers- . Tokyo Jikeikai Medical Journal 102: 89-105 (in Japanese with English abstract).
5) Poortmans JR. 1984. Exercise and renal function. Sports Medicine 1: 125-153.
28 JPFSM : Suzuki M
6) Suzuki M, Sudo M, Matsubara S, Kawakami K, Shiota M and Ikawa S. 1996. Changes in renal blood flow measured by radionuclide angiography following exhaustive exercise in man. Eur J Appl Physiol 74: 1-7.
7) Tidgren B and Hjemdahl P. 1988. Reflex activation of re-nal nerves in humans: differential effects on noradrenaline, dopamine and renin over-flow to renal venous plasma. Acta Physiol Scand 134: 23-34.
8) Tidgren B, Hjemdahl P, Theodorsson E and Nussberger J. 1991. Renal neurohormonal and vascular responses to dy-namic exercise in humans. J Appl Physiol 70: 2279-2286.
9) Wade CE and Claybaugh JR. 1980. Plasma renin activity, vasopressin concentration, and urinary excretion responses to exercise in men. J Appl Physiol: Respirat Environ Exer-cise Physiol 49: 930-936.
10) Ikawa S, Suzuki M and Shiota M. 1984. Responses in plas-ma catechoamines, renin, angiotensin, and cAMP in relation with the increases in work load. Rep Res Cent Phys Ed 12: 201-212.
11) Freund BJ, Shizuru EM, Hashiro GM and Claybaugh JR.1991. Hormonal, electrolyte, and renal responses to exer-cise are intensity dependent. J Appl Physiol 70: 900-906.
12) Suzuki M and Ikawa S. 1991. The mechanisms of exercise-induced proteinuria -Relationship between urinary excre-tion of proteins and lactate after exhaustive exercise-. Jpn J Nephrol 33: 357-364 (in Japanese with English abstract).
13) Suzuki M, Shiota M and Ikawa S. 1983. The physiological responses to exercise under hot and cold environmental tem-perature. Physical Fitness Research 134-144.
14) Suzuki M and Ikawa S. 1987. Response, regulation, and ac-tions of aldosterone and antidiuretic hormone following heat exposure -Comparison with exercise induced release-. JJ Aerospace Environ Med 24:7-17.
15) Sehl ME and Yates FE. 2001. Kinetics of human aging: I. Rates of senescence between 30 and 70 years in healthy people. J Gerontol Biol Sci 56A: B198-B208.
16) Poortmans JR and Ouchinsky M. 2006. Glomerular filtration rate and albumin excretion after maximal exercise in aging sedentary and active men. J Gerontol Med Sci 61A: 1181-1185.
17) Suzuki M, Ishiyama I and Seino T. 2006. Age-associated changes in renal function after exhaustive exercise in healthy males ranging in age from 8 - 80 years old. Adv Exerc Sports Physiol 12: 65-72.
18) Suzuki M and Ishiyama I. 2010. Reference interval of maxi-mal oxygen uptake (V・O2max) as one of the determinants of health-related physical fitness in Japan. Jpn J Phys Fitness Sports Med 59: 75-86 (in Japanese with English abstract).
19) Kawai H. 1967. Studies on post-exercise diuresis (VI). Mie Medical Journal 11: 216-221 (in Japanese).
20) Imoto T, Sawada Y and Ogo K. 1985. The relationship be-tween exercise diuresis and running load. Jpn J Phys Fitness Sports Med 34: 247-258 (in Japanese with English abstract).
21) Suzuki M. 2014. Mechanisms underlying exercise-induced diuresis caused by 400-m sprints. Adv Exerc Sports Physiol 20: 35-44.
22) Berl T and Schrier RW. 2010. Disorders of water homeosta-sis. In: 7th edition Renal and Electrolyte Disorders (Schrier RW, eds), :1-13, Lippincott Williams & Wilkins, Philadel-phia.
23) Landes RG, Lillehei RC, Lindsay WG and Nicoloff DM.
1976. Free water clearance and the early recognition of acute renal insufficiency after cardiopulmonary bypass. Ann Thorac Surg 22: 41-43.
24) Chou SY, Porush JG and Faubert PF. 1990. Renal medullary circulation: hormonal control. Kidney Int 37: 1-13.
25) Bergstrom G and Evans RG. 2004. Mechanisms underly-ing the antihypertensive function of the renal medulla. Acta Physiol Scand 181: 475-485.
26) Rajapakse NW, Oliver JJ and Evans RG. 2002. Nitric oxide in responses of regional kidney blood flow to vasoactive agents in anesthetized rabbits. J Cardiovasc Pharmacol 40: 210-219.
27) Badzynska B, Grzelec-Mojzesowicz M, Dobrowolski L and Sadowski L. 2002. Differential effect of angiotensin II on blood circulation in the renal medulla and cortex of anaes-thetized rats. J Physiol 538: 159-166.
28) Maeda S, Miyauchi T, Iemitsu M, Tanabe T, Goto K, Ya-maguchi I and Matsuda M. 2004. Endothelin receptor an-tagonist reverses decreased NO system in the kidney in vivo during exercise. Am J Physiol Endocrinol Metab 286: E609-E614.
29) Klein JD, Murrell BP, Tucker S, Kim YH and Sands JM. 2006. Urea transport UT-A1 and aquaporin-2 proteins decrease in response to angiotensin II or norepinephrine-induced acute hypertension. Am J Physiol Renal Physiol 291: F952-F956.
30) Nielsen S, Frokiaer J, Marples D, Kwon ED, Agre P and Knepper M. 2002. Aquaporins in the kidney: from molecules to medicine. Physiol Rev 82: 205-244.
31) Sands JM. 2003. Molecular mechanisms of urea transport. J Membr Biol 191: 149-163.
32) Matsumura Y, Uchida S, Kondo Y, Miyazaki H, Ko SB, Hayama A, Morimoto T, Liu W, Arisawa M, Sasaki S and Marumo F. 1999. Overt nephrogenic diabetes insipidus in mice lacking the CLC-K1 chloride channel. Nat Gent 21: 95-98.
33) Uchida S, Sasaki S, Furukawa T, Hiraoka M, Imai T, Hirata Y and Marumo F. 1993. Molecular cloning of a chloride channel that is regulated by dehydration and expressed pre-dominantly in kidney medulla. J Biol Chem 263: 3821-3824.
34) Zambraski EJ, Boder MC, Goldstein JE, Lakas CS and Shepard MD. 1981. Changes in renal cortical sialic acids and colloidal iron staining associated with exercise. Med Sci Sports Exercise 13: 229-232.
35) Rennke HG, Patel Y and Venkatachalam MA. 1978. Effect of molecular chage on glomerular permeability to proteins in the rat: clearnce studies using neutral, anionic and cationic horseradish peroxidase. Kidney Int 13: 278-288.
36) Taguma Y, Kitamoto Y, Futaki G, Ueda H, Monma H, Ishizaki M, Takahashi H, Sekino H and Sasaki Y. 1985. Ef-fect of captopril on heavy proteinuria in azotemic diabetes. N Engl J Med 313: 1617-1620.
37) Suzuki M, Shiota M, Matsubara S and Ikawa S. 1990. Ef-fects of oral administration of angiotensin converting en-zyme inhibitor captopril on urinary excretion of protein after exhaustive exercise. Jpn J Physiol 40 (Suppl): S129.
38) Kodama K. 1988. A study on athletic proteinuria. Tokyo Jikeikai Medical Journal 103: 305-320 (in Japanese with English abstract).
39) Poortmans JR and Labilloy D. 1988. The influence of work intensity on postexercise proteinuria. Eur J Appl Physiol 57:

29JPFSM : Renal function during exercise
260-263.40) Cantone A and Cerretelli P. 1960. Effect of training on pro-
teinuria following muscular exercise. Int Z Angew Physiol Arbeitesphysiol 18: 324-329.
41) Gardner KD. 1961. The effect of pH on the filtration, reab-sorption, and excretion of protein by the rat kidney. J Clin Invest 40: 525-535.
42) Zambraski EJ, Bober MC, Goldstein JE, Lakas CS and Shepard MD. 1981. Changes in renal cortical sialic acids and colloidal iron staining associated with exercise. Med Sci Sports Exercise 13: 229-232.
43) Poortmans JR, Brauman H, Staroukine M, Verniory A, De-caestecker C and Leclercq R. 1988. Indirect evidence of glomerular/tubular mixed-type postexercise proteinuria in healthy humans. Am J Physiol 254 (Renal Fluid Electrolyte Physiol 23): F277-F283.
44) Suzuki M, Hodumi N, Kimura M, Nakaya M, Shimizu T, Takao T, Magara T, Mori Y and Machida K. 2000. Effects of exercise and dietary therapies on renal function and morpho-logical findings in the kidney and glucose-fatty metabolism in OLETF rats -Use of OLETF rats as a model of type 2 dia-betes mellitus-. Jpn J Phys Fitness Sports Med 49: 403-418 (in Japanese with English abstract).
45) Ballor DL and Poehlman ET. 1994. Exercise-training en-hances fat-free mass preservation during diet-induced weight loss: A meta-analytical findings. Int J Obes Relat Metab Disord 18: 35-40.
46) Yamanouchi K, Shinozaki T, Chikada K, Nishikawa T, Ito K, Shimizu S, Ozawa N, Suzuki Y, Maeno H, Kato K, Oshida Y and Sato Y. 1995. Daily walking combined with diet therapy is a useful means for obese NIDDM patients not only to re-duce body weight but also improve insulin sensitivity. Dia-betes Care 18: 775-778.
47) Suzuki M, Shindo D, Kimura M and Waki H. 2011. Effects of exercise, diet, and their combination on metabolic-syn-drome-related parameters in OLETF rats. Int J Sport Nutr Exerc Metab 21: 222-232.
48) Kain V, Kumar S, Puranik AS and Sitasawad SL. 2010. Azel-nidipine protects myocardium in hyperglycemia-induced cardiac damage. Cardiovasc Diabetol 9: 82-90.
49) Nagasu H, Satoh M, Fujimoto S, Tomita N, Sasaki T and Kashihara N. 2012. Azelnidipine attenuates glomerular dam-age in Dahl salt-sensitive rats by suppressing sympathetic nerve activity. Hypertens Res 35: 348-355.
50) Matsubara S, Matsuo E, Koike K, Aoyama S, Shindou D and Suzuki M. 2013. Effects of the combination of an anti-hypertensive drug and exercise on glucose-lipid metabolism and diabetic nephropathy in Otsuka Long Evans Tokushima Fatty rats. Adv Exerc Sports Physiol 19: 73-81.
51) Kurashige T, Abe K, Furusu A, Miyazaki M, Obata Y, Xia Z, Nakazawa M, Nakazawa Y, Funakoshi S, Harada T, Koji T and Kohn S. 2008. Renoprotective effects of azelnidipine in rats. Biol Pharm Bull 31: 2237-2244.