Embed Size (px)
Citation preview

Physical Therapists
and Physicians
Working Together for Optimal Patient
Outcomes
2018 Spine Care and Physiatry Symposium

Objectives1. Understand key points from Providence system spine pathway work,
particularly related to appropriate patients for physical therapist services
2. Psychosocial risk stratification and how it helps improve success and efficiency in treating people with back pain
3. Gain a greater understanding of how Providence Rehab Services is working to improve outcomes for your patients with back pain
– Overview of evidence-based physical therapist services for identification of back pain subgroup and matched treatment for optimal results
– Providence Rehab Services options for people with back pain
4. Working together to optimize patient outcomes
5. Time to address your questions


People with Back Pain
• Common reason for seeking care in primary care,
physiatry, and physical therapy
• Pain is a multidimensional experience
• Controversy continues to exist regarding most
effective treatment
• Wide variability in treatment and referral patterns
affects health care costs

Providence/Swedish System Spine Pathway
• Work groups
– Primary care
– Physiatry and neurology
– Surgery
– Pain
– Physical therapy
– Pharmacy
• 37-page document outlining best practice guidelines
– Right provider, right time
– Guidelines for pharmacy, imaging, surgical implants

Proposed
System
Spine
Pathway


Providence Oregon Rehab Services
Back pain best practice
• Screening for rapidly progressive neurological deficit
and red flags
• Psychosocial risk stratification
• Back pain subgroups with matched treatment
• Multiple service options

Physical therapist services
• 1:1 clinic-based PT
• Persistent pain services
• Pain education class
• STEP
• Telehealth pilot
→ Long-term self-management maintenance
program

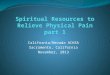
Patient with back pain
Entry to PT services
Rapidly progressing neurological deficits: send to emergency department
Red flags: refer for medical follow-up
Radiculopathy: consult with neurology or physiatry; consider MRI
STarT Back Screening ToolPT as needed
Low Risk Medium Risk High Risk
Education, reassurance,
medication (PCP)
Possible PT
Same as low risk+
Best practice PT
Same as medium risk+
Biopsychosocially-minded care
+MD & Behavioral Health
If improved, discharge Improving but goals not yet met, reassess POC/continue
If not improving in 4-8 weeks, refer back to MD
Physical
Therapy
Pathway

Back pain best practice
Psychosocial risk stratification

STarT Back Screening Tool
Thinking about the past two weeks, mark your response to the following questions:Disagree Agree
My back pain has spread down my leg(s) in the past two weeks □ □
I have had pain in the shoulder or neck at some time in the last two weeks □ □
I have only walked short distances because of my back pain □ □
In the last two weeks, I have dressed more slowly than usual because of back pain □ □
It’s not really safe for a person with a condition like mine to be physically active □ □
Worrying thoughts have been going through my mind a lot of the time □ □
I feel that my back pain is terrible and it’s never going to get any better □ □
In general, I have not enjoyed the things I used to enjoy □ □
Overall, how bothersome has your back pain been in the last two weeks? Not at all Slightly Moderately Very much Extremely
□ □ □ □ □
Total score (all 9): __________ Psych subscore (questions 5-9): __________
©Keele University 1/8/2007. Funded by Arthritis Research UK.

Psychosocial complexity stratification
High complexity → High risk

Treatment tailored to high psychosocial
complexity
• Focus on cognitive, emotional, and behavioral
responses
• Multidisciplinary care, including behavioral health
• Gradual return to activity
• Tools for self-management

Back pain best practice
Back pain subgroups

Back pain subgroups
• Evidence-based classification
• Matched treatment

Identifying
back pain
subgroups

Physical Therapy Low Back Pain Clinical Practice Guidelines – Matching Treatment to Back Pain Subgroup
Subgroup Clinical Picture Key Matched Treatments
Low back pain with movement coordination
impairments
Hypermobility and/or weakness is the main
problem
Needs strengthening, conditioning
Low back pain with mobility deficits Stiffness is the main problem
May be deconditioned
Needs stretching and mobilization
May need strengthening & cardio
Acute low back pain with related lower
extremity pain (somatic referral)
Non-radicular referral to the LE(s).
Often similar to the “movement coordination
impairments” (hypermobile/weak) group
May respond to McKenzie/MDT
(repeated exercise)
May need strengthening
Low back pain with radiating pain Radicular referral to the LE(s) Screen for red flags/progressive
neurological deficits
Be aware of neural mobility –
protect in acute phase,
mobilize in chronic phase
Low back pain with related cognitive or
affective tendencies
Pain and psychosocial issues are the main
problem
Treat objective impairments as well
as addressing psychosocial and
pain education needs
Gentle cardiovascular exercise
Multidisciplinary care
Chronic low back pain with related
generalized pain
Matched Treatment

Back pain best practice
Persistent pain services

Persistent Pain Services
• All therapists in Rehab Services have basic pain
training
• Pain specialists
• Other services

Pain Education Class
• Free for current Rehab Services patients
– One-time, two hour class
• Understanding pain helps calm pain
– Current understanding of pain neurophysiology
– Self-management strategies and resources
– Understanding pain reduces pain – there is hope

Oregon Pain Management Commission
Pain Care Resources
• http://www.oregonpainmodule.org/regApp/menu.asp

Back pain best practice
STEP

STEP: Spine Therapy Exercise Program
• Supervised exercise therapy for people with back and neck pain– Failed previous therapies, including surgery, injections, PT, etc.
– Need a strength and conditioning program to enable them to perform their daily and work activities
– Number of treatments varies between 4 and 12, based on psychosocial complexity (STarT score)
• Goal is to establish a long-term, independent resistive exercise program
https://www.youtube.com/watch?v=NM4jBGMb5s8

Not sure?Failed
previous therapies
Ready for supervised
exercise
Patient with
persistent pain
“Typical” PT back
pain patient
PT referral;PT will get the patient
to the appropriate specialist/program
PT referral STEP referral
STEP referral
PT referral;PT will get the patient
to the appropriate specialist/ program
How do I know whether to refer to PT or to STEP?

Back pain best practiceLong-term self management

Long-term exercise program
• Strong evidence that exercise alone or in combination with education reduces the frequency, duration, and severity of future episodes of back pain
• Building and maintaining capacity
• Physical activity is not associated with back pain flare-ups,
but sitting, stress, and depression are
Pradeep S, Rainville J, de Schepper E, Martha J, Harigan C, Huner DJ. Do physical activites trigger flare-ups during an acute low back pain episode? A longitudinal case-crossover feasibility study. Spine 2018:43(6);427-422.
Steffens D, Maher CG, Pereira LSM, Stevens ML, Oliveira VC, Chapple M, Teixeira-Salmela LF, Hancock MJ. Prevention of Low Back Pain: A Systematic Review and Meta-analysis. JAMA Intern Med. doi:10.1001/jamainternmed.2015.7431. Published online January 11, 2016.

Back pain best practice
Working together for optimal outcomes

Working together for optimal patient outcomes
Patient

Working together for optimal patient
outcomes
• Talking about to patients about their back pain
• Talking about imaging
• What to expect in PT
• Realistic expectations
• Fostering hope

Talking about imaging
• Early imaging
– Evidence shows that early imaging is not helpful for most
people with back pain and that simple guidelines indicate
when it’s appropriate
• Persistent symptoms
– Guidelines often indicate that imaging is appropriate
• Cultural beliefs about imaging have repercussions

Talking about imaging

Talking about imaging

Working together for optimal patient outcomes
Establishing realistic expectations
“You have had this for a long time.
It’s not going to go away immediately, but you will learn
exercises and strategies to take better care of your
condition.
You will probably be able to move better and do more before
your pain goes down.
It will be important to continue with what you learn even after
you start to feel better.”

Working together for optimal patient outcomes
Fostering hope
– Reinforcing idea that back pain is normal
– Imaging doesn’t tell the whole story
– The body has great potential to heal
– People can learn the tools they need to manage their
condition better
– Regular exercise helps prevent back pain

Take home messages
1. A message of hope is important and builds self-
efficacy
– Imaging results don’t mean you can’t get better
– With a little work, you can learn to manage this better
2. PT offers a wide variety of services
– Evidence-based treatment
– Pain education
3. Long-term exercise and self-management

Questions?

Thank You!

References“Back Boot Camp – breaking down back pain.” https://www.youtube.com/watch?v=NM4jBGMb5s8 Accessed on 4/17/18.
Brinjikji W et al. Systematic literarture review of imaging features of spinal degeneration in asymptomatic populations. AJNR Am J Neuroradiol 2015:36:811–16.
Childs JD, Flynn TW, Wainner RS. Low back pain: do the right thing and do it now. J Orthop Sports Phys Ther 2012;42(4):296-299.
Chou R, Qaseem A, Owens DK, Shekelle P. Diagnostic imaging for low back pain: advice for high-value health care from the American College of Physicians. Ann Intern Med. 2011;154:181-189
Delitto A, George SZ, Van Dillen L, Whitman JM, Sowa G, Shekelle P, Denninger TR, Godges JJ. Low back pain clinical practice guidelines linked to the international classification of functioning, disability, and health from the orthopaedic section of the American Physical Therapy Association. J Orthop Sports Phys Ther 2012;42(4):A1-A57.
Downie A et al. Red flags to screen for malignancy and fracture in patients with low back pain: systematic review. BMJ 2013;347:f7095 doi: 10.1136/bmj.f7095
Flynn TW, Smith B, Chou R. Appropriate use of diagnostic imaging in low back pain: a reminder that unnecessary imaging may do as much harm as good. J Orthop Sports Phys Ther 2011;41(11):838-846, Epub 3 June 2011. doi:10.2519/jospt.2011.3618
Fritz JM, Brennan GP, Hunter SJ. Physical therapy or advanced imaging as first management strategy following a new consultation for low back pain in primary care: associations with future health care utilization and charges. Health Services Research 2015 Mar 16. doi: 10.1111/1475-6773.12301.
Fritz JM, Childs JD, Wainner RS, Flynn TW. Primary care referral to patients with low back pain to physical therapy: impact on future health care utilization and costs. Spine 2012;37(25):2114-2121.
Fritz, JM, Cleland JA, Childs JD. Subgrouping patients with low back pain: evolution of a classification approach to physical therapy. J Orthop Sports Phys Ther 2007;37(6):290-302.
Hadler N, Meira E, Hilton S. I am a placebo: and interview with Dr Nortin Handler MD. Pain Science and Sensibility Podcast. 12/28/17.
Hill JC, Whitehurst DG, Lewis M, et al. Comparison of stratified primary care management for low back pain with current best practice (STarT Back): a randomised controlled trial. Lancet. 2011;378(9802):1560-1571. doi:10.1016/S0140-6736(11)60937-9.
Karran EL, Hillier SL, Yau Y, McAuley JH, Moseley GL. A quasi-randomised, controlled, feasibility trial of GLITtER (Green Light Imaging Interpretation to Enhance Recovery)—a psychoeducational intervention for adults with low back pain attending secondary care. PeerJ 2018:e4301 https://doi.org/10.7717/peerj.4301
Karlen EK. Implementation of evidence-informed physical therapy and chiropractic care improves value for patients. SpineLine 2015;Jan-Feb:15-20.
Keele STarT Back Screening Tool – Matched Treatments. Available at: http://www.keele.ac.uk/sbst/matchedtreatments/. Accessed on April 9, 2018.
Pradeep S, Rainville J, de Schepper E, Martha J, Harigan C, Huner DJ. Do physical activites trigger flare-ups during an acute low back pain episode? A longitudinal case-crossover feasibility study. Spine 2018:43(6);427-422.
Sackett, DL, Rosenberg, WM. On the need for evidence-based medicine. Journal of Public Health 1995;17:330-334.
Srinivas SV, Deyo RA, Berger ZD. Application of “less is more” to low back pain. Arch Intern Med. 2012;172:1016-1020. Published online June 4, 2012. DOI:10.1001/archinternmend.2012.1838.
Stevans JM, Bise CG, McGee JC, Miller DL, Rockar P, Delitto A. Evidence-based practice implementation: case report of the evolution of a quality improvement program in a multicenter physical therapy organization. PhysTher 2015;95:588-599.