Embed Size (px)
Citation preview

Physician decision-making regarding medication use in patients with dementia
at the end of life
Dr Carole ParsonsSchool of Pharmacy
Queen’s University Belfast

Introduction
• Studies in populations with a reduced life expectancy have highlighted the prevalence of suboptimal and inappropriate medication use
• Little discussion regarding medication use in patients with advanced dementia nearing the end of life
• No attempt to define decision-making processes for physicians in determining which of the dying dementia patient’s medications should be withheld or discontinued
Introduction Method Results Discussion Acknowledgements

Introduction
• Study funded by CARDI
• Cross-border and inter-disciplinary collaboration with University College Cork, practitioners in nursing, medicine and pharmacy, representatives from the voluntary sector
• Aim: To evaluate, using a factorial design with vignette-based survey methodology, the extent to which patient-related factors and physician country of practice influence decision-making among Northern Ireland (NI) and Republic of Ireland (RoI) physicians with respect to medication use in patients with end-stage dementia
Introduction Method Results Discussion Acknowledgements

Method
• 3x2x3 factorial survey design• Four different patient clinical scenarios (vignettes) • Each vignette prefaced with statement indicating doctor is caring for
a patient with advanced dementia nearing the end of life• Drug regimen for patient outlined
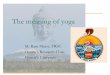
Vignette Medical Issues
Vignette 1: patient with pneumonia and fever
How to manage? Start or withhold antibiotic?Change any of patient’s other medications?
Vignette 2: patient taking acetylcholinesterase inhibitor and memantine
Continue or discontinue acetylcholinesterase inhibitor and/or memantine?Change any of patient’s other medications?
Vignette 3: patient taking statin Continue or discontinue statin?Change any of patient’s other medications?
Vignette 4: patient taking atypical antipsychotic
Continue or discontinue antipsychotic?Change any of patient’s other medications?
Table 1: Summary of vignettes and issues considered
Introduction Method Results Discussion Acknowledgements

Method
Suppose that you are seeing Mrs. Mary Jones today. Mrs Jones is an 82 year-old retired seamstress who is <RANDOM ASSIGNMENT: “resident in a nursing home” OR “cared for in her own home.” She has developed pneumonia with severe respiratory failure and has a fever of 38.9°C. She was diagnosed with Alzheimer’s Disease seven years ago. RANDOM ASSIGNMENT: “She has a signed advance directive expressing a preference for supportive care, rather than for more aggressive treatment measures, at the end-of-life”. OR “There is no advance directive concerning treatment.” Recently her mental condition has declined. Although she is alert, she is no longer orientated in terms of time, place and situation. She displays little spontaneous speech and when she does speak, her speech is unintelligible with the exception of single random words. She is totally dependent on her caregiver for all activities of daily living. She can no longer walk since suffering a series of falls three months ago and refuses food and fluids often, slapping at the hand of the person attempting to feed her. She has lost 7% of her body weight in the last two months. RANDOM ASSIGNMENT: “Mrs. Jones’ family desires active treatment measures be taken to save her life in the event of a life-threatening condition.” OR “Mrs. Jones’ family desires supportive treatment measures be taken to provide symptomatic relief only and make her comfortable.” OR “There is no family involvement.”
Introduction Method Results Discussion Acknowledgements

Method
• Physician asked to indicate whether he/she would make any changes to patient’s prescribed medication in the scenario• Patient-related factors were systematically manipulated in the vignettes
– Place of residence of patient (community-dwelling, resident in nursing home, hospital inpatient)– Signed advance directive (present or absent)– Level of family involvement (desire for active treatment measures, desire for supportive treatment measures or no family involvement)
• Dependent variables assessed were whether the physician chose to 1. initiate an antibiotic2. continue or discontinue donepezil hydrochloride3. continue or discontinue memantine hydrochloride4. continue or discontinue simvastatin5. continue or discontinue quetiapine
Introduction Method Results Discussion Acknowledgements

Method
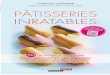
Advance Directive
No Advance Directive
Family desires active measures
Family desires supportive measures
No family involved
Family desires active measures
Family desires supportive measures
No family involved
Vignettes for hospital
physicians
Figure 1: Variants of vignettes for hospital physicians
Introduction Method Results Discussion Acknowledgements

Method
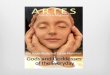
Figure 2: Variants of vignettes for GPs
Introduction Method Results Discussion Acknowledgements
Vignette for GPs
Patient resident in own home
Patient resident in nursing home
Advance Directive
No Advance Directive
Advance Directive
No Advance Directive
Family desires active measures
Family desires supportive measures
No family involved
Family desires active measures
Family desires supportive measures
No family involved
Family desires active measures
Family desires supportive measures
No family involved
Family desires active measures
Family desires supportive measures
No family involved

• Physicians randomly assigned one variant of each vignette appropriate to their practice
• Questionnaire also gathered demographic information and included a series of open questions
• Piloted with 4 hospital physicians and 5 GPs
• Ethical approval granted by the Office for Research Ethics Committees Northern Ireland (ORECNI) and the Irish College of General Practitioners Research Ethics Committee
• Questionnaires mailed to all hospital physicians in geriatric medicine (NI n= 73; RoI n= 86) and all GPs (NI n= 1161; RoI n= 1900) with a reminder three weeks later
Method
Introduction Method Results Discussion Acknowledgements

• All responses coded and entered into SPSS® Version 18.0
• Logistic regression analysis examined impact of patient-related factors and physician country of practice on decision-making about key medications
• P ≤ 0.05
• Qualitative analysis of free text responses
Method - Analysis
Introduction Method Results Discussion Acknowledgements

Results
• Response rates
– Hospital physicians: NI: n = 38 (52.1%); RoI: n = 31 (36.2%)
– GPs: NI: n = 245 (21.1%); RoI: n = 348 (18.3%)
Introduction Method Results Discussion Acknowledgements
Medication of interest NI hospital
physicians
RoI
hospital
physicians
All hospital
physicians
NI GPs RoI GPs All GPs
Antibiotic (prescribed)15/36
(41.7%)12/30
(40.0%)27/66
(40.9%)126/237 (53.2%)
189/329 (57.4%)
315/566 (55.7%)
Donepezil hydrochloride 10 mg
nocte (discontinued)
15/38 (39.5%)
22/31 (71.0%)
37/69 (53.6%)
131/230 (57.0%)
185/339 (54.6%)
316/569 (55.5%)
Memantine hydrochloride 10 mg
bd (discontinued)
7/38 (18.4%)
14/31 (45.2%)
21/69 (30.4%)
101/225 (44.9%)
139/336 (41.4%
240/561 (42.8%)
Simvastatin 20mg nocte
(discontinued)
32/37 (86.5%)
30/31 (96.8%)
62/68 (91.2%)
176/236 (74.6%)
232/337 (68.8%)
408/573 (71.2%)
Quetiapine 100mg bd
(discontinued)
12/36 (33.3%)
7/29 (24.1%)
19/65 (29.2%)
61/232 (26.3%)
54/336 (16.1%)
115/568 (20.2%)
Table 2. Frequency and percentage of GPs and hospital physicians who recommended initiating/discontinuing the five key medications of interest

Results
Outcome variable Χ2 (df) p (Cox & Snell) R2
% decisions regarding drug initiation/continuation
correctly classifiedBefore IVs
enteredAfter IVs entered
Antibiotic initiated 48.340 (8) <.001 .073 54.1 61.2
Donepezil
continued
19.190 (10) .038 .030 57.7 55.3
Memantine
continued
14.789 (8) .063 .023 58.9 58.6
Simvastatin
continued
36.222 (10) <.001 .055 73.3 73.3
Quetiapine
continued
26.011 (6) <.001 .040 78.8 78.8
Table 3: Logistic regression model statistics for the five key medications of interest
IV – independent variable
Introduction Method Results Discussion Acknowledgements

Results
• Regression models only explained a small percentage of the variance in physicians’ prescribing decisions
• Across the five medications of interest, patient place of residence and physician’s country of practice appeared to have the strongest and most consistent effects on decision-making (of those factors examined in the study), albeit yielding small effect sizes.
• When the patient was resident in hospital (compared to resident at home or in a nursing home) it was less likely that an antibiotic would be prescribed, and more likely that simvastatin and quetiapine would be discontinued.
• If the physician practised in RoI (compared to NI), it was less likely that quetiapine would be discontinued.
• If the physician practised in hospital in the RoI (compared to NI), it was more likely that donepezil hydrochloride and memantine hydrochloride would be discontinued.
• An antibiotic was more likely to be prescribed when the patient did not have an advance directive, or when the patient’s family desired active treatment measures
Introduction Method Results Discussion Acknowledgements

Results - free text responses
• Discontinuation of donepezil hydrochloride and memantine hydrochloride: little clinical benefit
“Patient is not going to get long term benefit of Alzheimer's drugs (not much use anyway), and if used, should only be in early stages of disease. Pointless now.” (RoI physician 302, GP)
• Discontinuation of simvastatin: primary/secondary prevention inappropriate, little clinical benefit
“I would discontinue any medication used for longer term secondary prevention because of advanced stage of dementia” (RoI physician 352, hospital physician)
• Discontinuation of quetiapine: lack of indication, possibility of side-effects
“Hold quetiapine as may be making her confusion worse” (RoI physician 126, GP)
“No clinical benefit ….. risk of adverse effects” (NI physician 112, GP)• Other reasons for discontinuing medications: focus on patient comfort or symptom
management, reduce polypharmacy, recognition of distress caused by medication
“Stop all preventative treatment as not necessary for providing comfort or support and may increase distress” (NI physician 169, GP)
“No compelling reason to continue, relative meds benefit now minimal. Reduce polypharmacy and risk of mistakes” (NI physician 231, GP)
Introduction Method Results Discussion Acknowledgements

Discussion
• Considerable variability exists in NI and RoI physician decision-making regarding medication use in patients with advanced dementia who are nearing the end of life
• Uncertainty exists with regard to prescribing antibiotics, discontinuing donepezil hydrochloride and memantine hydrochloride
• Less variability exists in decision-making regarding simvastatin and quetiapine
• Patient place of residence and physician country of practice had the strongest and most consistent effects on decision-making
Introduction Method Results Discussion Acknowledgements

Discussion
• Study limitations
– Low response rates, using vignette approach
• Future research to
– clarify how patient place of residence and physician country of practice impact on prescribing decisions
– identify other factors which may account for unexplained variance in decision-making
• Development and clarification of the evidence base regarding prescribing for patients with end-stage dementia required
Introduction Method Results Discussion Acknowledgements

Acknowledgements
• Dr Noleen McCorry
• Prof Carmel Hughes
• Prof Peter Passmore
• Dr Susan Patterson
• Mr Gordon Kennedy
• Mrs Valerie Megraw
• Mrs Anne Olver
• Dr Stephen Byrne
• Dr Denis O’Mahony
• Mr David O’Sullivan
• Mr Kevin Murphy
• Ms Mary Hickey
• Ms Ursula Collins
All hospital physicians and GPs who responded to the questionnaires
Centre for Ageing Research and Development in Ireland
Introduction Method Results Discussion Acknowledgements

Discussion
• Considerable variability exists in NI and RoI physician decision-making regarding medication use in patients with advanced dementia who are nearing the end of life
• Uncertainty exists with regard to prescribing antibiotics, discontinuing donepezil hydrochloride and memantine hydrochloride
• Less variability exists in decision-making regarding simvastatin and quetiapine• Patient place of residence and physician country of practice had the strongest
and most consistent effects on decision-making• Future research to
– clarify how patient place of residence and physician country of practice impact on prescribing decisions
– identify other factors which may account for unexplained variance in decision-making
• Development and clarification of the evidence base regarding prescribing for patients with end-stage dementia required