Embed Size (px)
DESCRIPTION
Physiologic Monitoring of the Surgical Patient. Basic Science Conference 1/26/2010. Background. Latin word monere , which means “to warn, or advise,” is the origin for the English word monitor. - PowerPoint PPT Presentation
Citation preview

Basic Science Conference1/26/2010
BackgroundLatin word monere, which means “to warn, or
advise,” is the origin for the English word monitor.
Patients undergo monitoring to detect pathologic variations in physiologic parameters, in order to give us advance warning of deterioration of one or more organ systems.
GOAL: Use the information to make a timely intervention.
Monitoring also used to guide resuscitation and titrate medications.
Background (cont.)The ultimate goal of hemodynamic monitoring
is to ensure that the flow of oxygenated blood through the microcirculation is sufficient to support aerobic metabolism at the cellular level.
This involves multiple inputs.Oxygen delivery
COHgbO2 satPAO2
Arterial Blood PressureThe pressure exerted by blood in the
systemic arterial system.Hypotension = Shock ?MAP = CO x SVRHow do we measure blood pressure?
Non-invasive (cuff)Invasive
Risks and benefits
NoninvasiveManual and automated means, both of which
use a cuff. The width of the cuff should be about 40% of the circumference.
Korotkoff soundsSystolic- tapping sounds first audibleDiastolic- audible pulsations disappear
Dyna-map
InvasiveFluid-filled tubing to connect an intra-arterial
catheter to external strain-gauge transducer which is transduced as a continuous waveform.
Underdamped –systolic overestimated and diastolic underestimated
Overdamped- systolic underestimated and diastolic overestimated
Use Mean Arterial PressureSystolic pressure higher, diastolic pressure
lower in the radial artery compared to the aorta
Invasive ComplicationsThrombosis (Allen test)Air EmbolismInfection
EKG monitoringContinuous monitoring with three lead EKGImmediate alarm with arrhythmiasCan detect ST elevationNo substitute for 12 lead EKG
Cardiac outputDeterminants of Cardiac Performance
Preload - EDVAfterload-SVRContractility- dependent on preload and
afterload
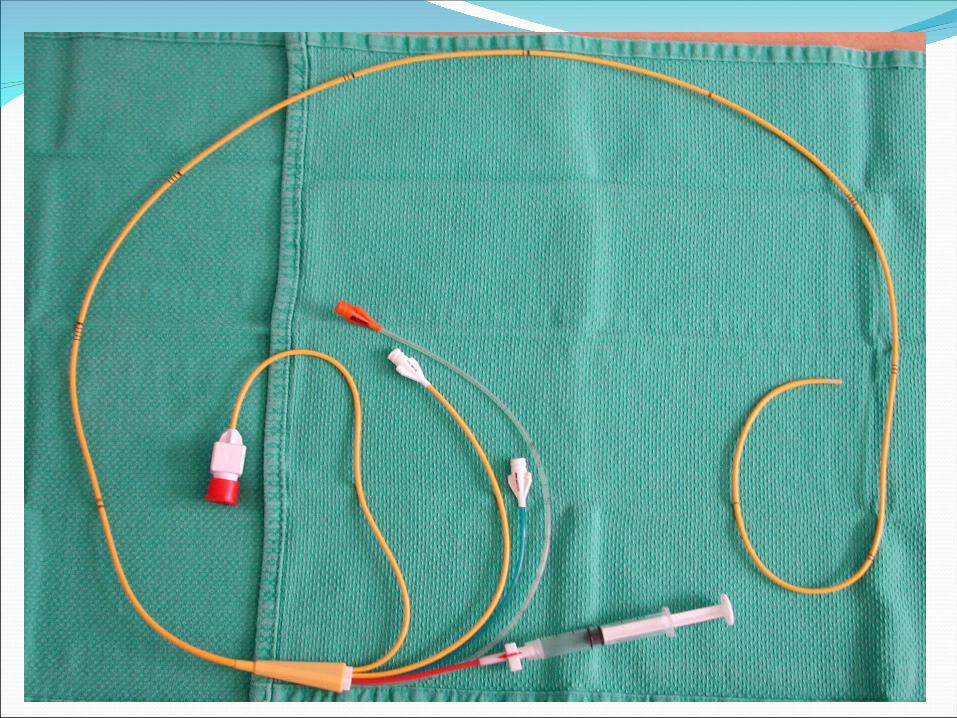
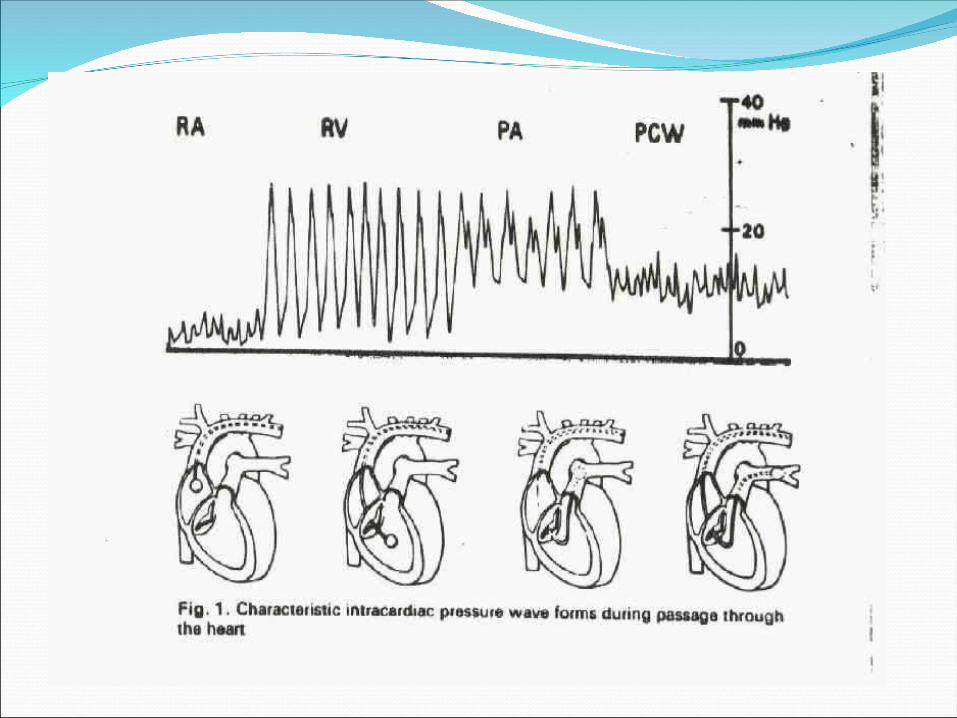
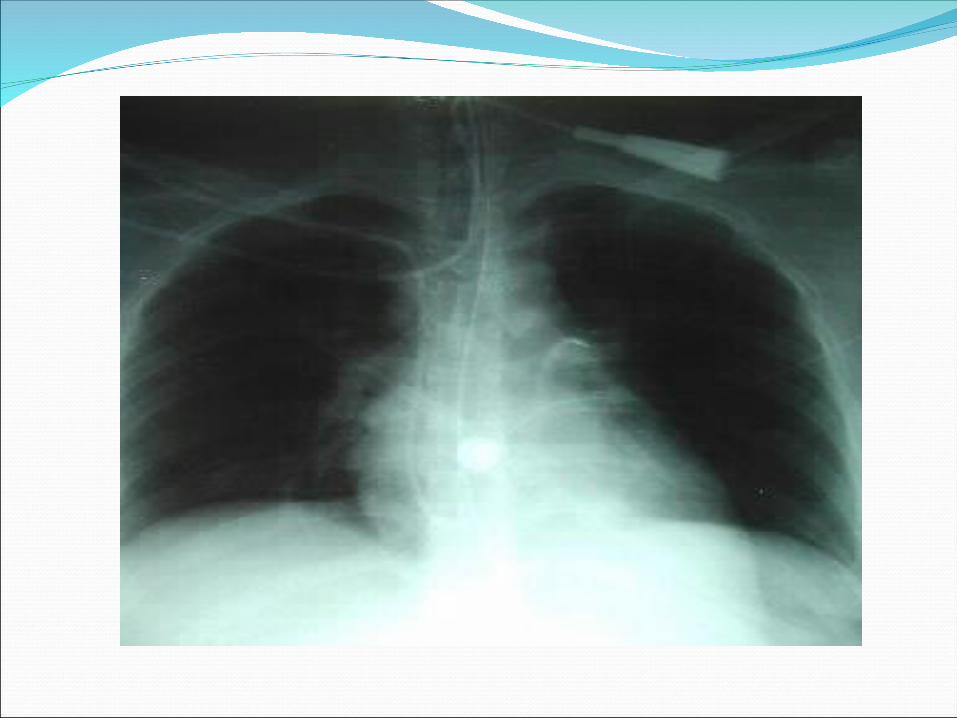
Pulmonary artery catheterPAC has four channelsBalloon (1.5cc)CVP, PAInsertionWaveformsDistance
45 cm RSCV50cm RIJ55cm LSC60cm LIJ
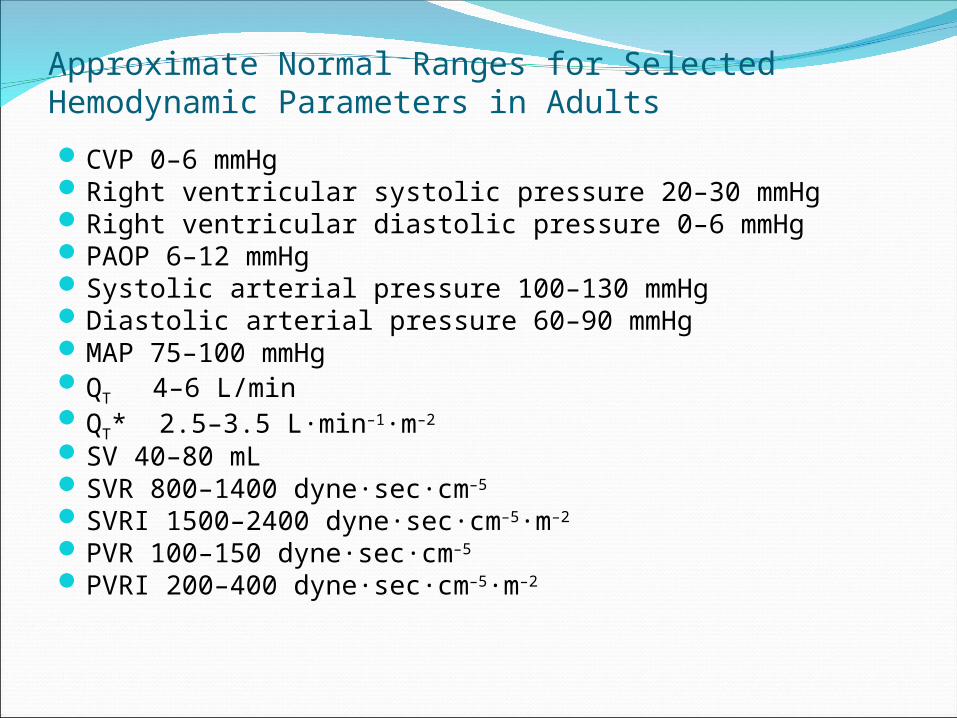
Approximate Normal Ranges for Selected Hemodynamic Parameters in Adults
CVP 0–6 mmHg Right ventricular systolic pressure 20–30 mmHg Right ventricular diastolic pressure 0–6 mmHg PAOP 6–12 mmHg Systolic arterial pressure 100–130 mmHg Diastolic arterial pressure 60–90 mmHg MAP 75–100 mmHg QT 4–6 L/min QT* 2.5–3.5 L·min–1·m–2
SV 40–80 mL SVR 800–1400 dyne·sec·cm–5
SVRI 1500–2400 dyne·sec·cm–5·m–2
PVR 100–150 dyne·sec·cm–5
PVRI 200–400 dyne·sec·cm–5·m–2
Hemodynamic measurementsCardiac output by thermodilutionMixed venous oximetryRV ejection fraction
Types of ShockHemorrhagicSepticCardiogenicNeurogenicHypo adrenal
Risks and benefits of PACsMany studies show no mortality difference
with PAC use and more complications related to the catheter or its placement.
AlternativesDoppler UltrasonographyImpedance cardiographyPulse contour analysisTEE
Respiratory monitoringThe ability to monitor various parameters of
respiratory function is of utmost importance is critically ill patients.
Arterial blood gasesPeak and plateau airway pressurePulse oximetryCO2 monitoring
ABGO2 (PEEP, FIO2)CO2 (RR, TV)O2 satHCO3BE/BD
Airway PressuresIncreased pressure = decreased compliance
Hemo/pneumothoraxAtelectasisPulmonary edemaARDSAbdominal distension
Barotrauma
Renal monitoringUrine outputBladder pressure
Neurologic monitoringIntracranial pressure
CPP= MAP- ICP CPP>60
Allows monitoring and drainageStrategies to decrease ICP
Transcranial doppler ultrasonographyEEGBrain tissue oxygen tension
ConclusionsPhysiologic monitoring provides us with a
multitude of information.Determining what information is beneficial
and using this to positively affect the outcome of the patient is the key.
All of the following are most often associated with a decrease in SVO2 except:Myocardial infarctionCardiac tamponadeHemorrhagic shockSeptic shock
You place a swan ganz catheter in a 709kg adult male through the left subclavian vein and get a wedge pressure. The approximate distance into the patient should be:
45cm50cm55cm 60cm
While trying to treat a patient with severe ARDS, you start to increase the PEEP to improve oxygenation. After doing this, you notice a decrease in urine output. The mechanism of decreased urine output with increased PEEP is:
Compartment syndromeDecreased cardiac outputReduced oxygenationRetained CO2
A patient stops making urine after surgery. All of te following values are consistent with pre-renal renal failure except:
Urine Na 5BUN/Cr ratio >35FeNA=0.1%Urine osmolality 200 mOsm
All of the following concerning pulmonary artery catheters are true except:
Excessive PEEP can artificially increase wedge pressure.
Excessive PEEP can artificially decrease wedge pressure.
Zone III of the lung is the optimal site of placement.
The balloon should be inflated when advancing the catheter.
A critical care patient has the following PAC values: CI 1.8, SVR 3000, and a wedge pressure of 5. This is most consistent with:
Septic shockHypovolemic shockCardiogenic shockNeurogenic shock
A critical care patient has the following PAC values: CI 5.0, SVR 500, and a wedge pressure of 7. This is most consistent with:
Septic shockHypovolemic shockCardiogenic shockNeurogenic shock
A critical care patient has the following PAC values: CI 1.8, SVR 3000, and a wedge pressure of 28. This is most consistent with:
Septic shockHypovolemic shockCardiogenic shockNeurogenic shock
A critical care patient has the following PAC values: CI 2.0, SVR 500, and a wedge pressure of 5. This is most consistent with:
Septic shockHypovolemic shockCardiogenic shockNeurogenic shock
A patient with ARDS following an inhalation injury has an oxygenation saturation of 90% on 90% FiO2 with an SVO2 of 55. The patient’s ABG is pH 7.35, pO2 of 60, and pCO2 60. The patient has a cardiac output of 5, and a Hgb of 8. Oxygen delivery will increase the most by:
Increasing cardiac output by 1Increasing hemoglobin by 2Increasing FiO2 by 10%Decreasing CO2 by 10%
Oxygen delivery = CO x[(Hgb x1.34x O2 sat) + (0.003x PaO2)]





























