Embed Size (px)
Citation preview
Physiologie et Sémiologie
Cérébelleuses
Pr Fabien Zagnoli
Hôpital d’Instruction des Armées
Brest
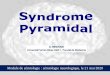
Cervelet:
Régulation du mvt volontaire
Noyaux gris:
Régulation du mvt automatique
Systèmes en dérivation
Rôle Moteur:
• Maintien équilibre
• Régulation du tonus
• Coordination action volontaire
• Programmation motrice
Rôle Non Moteur
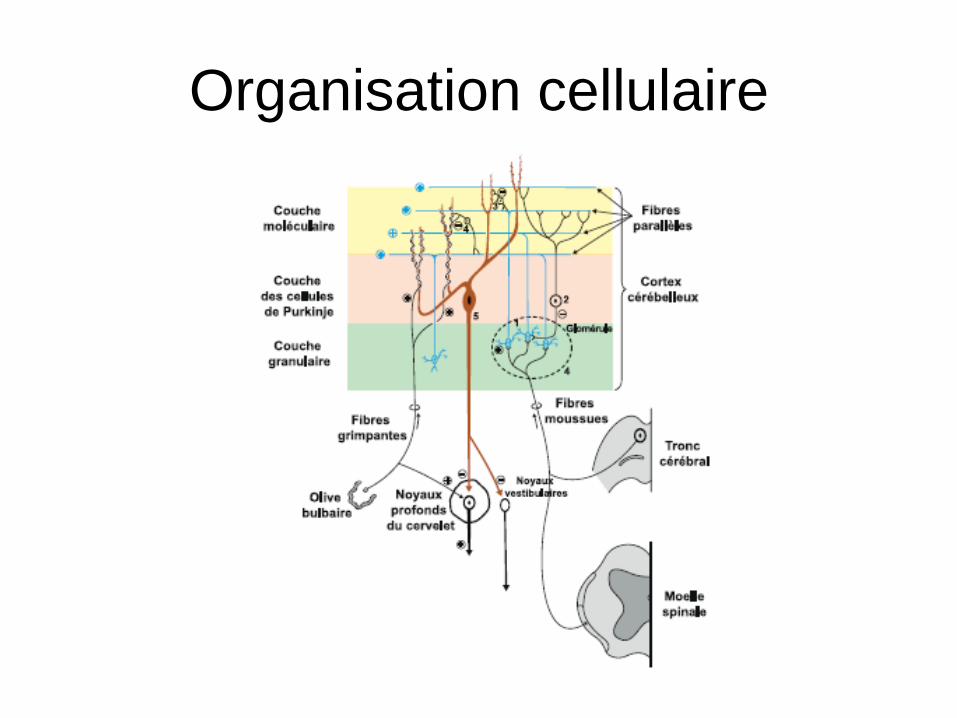
Organisation cellulaire
Couche moléculaire
Couche des c. de Purkinje
Couche des grains
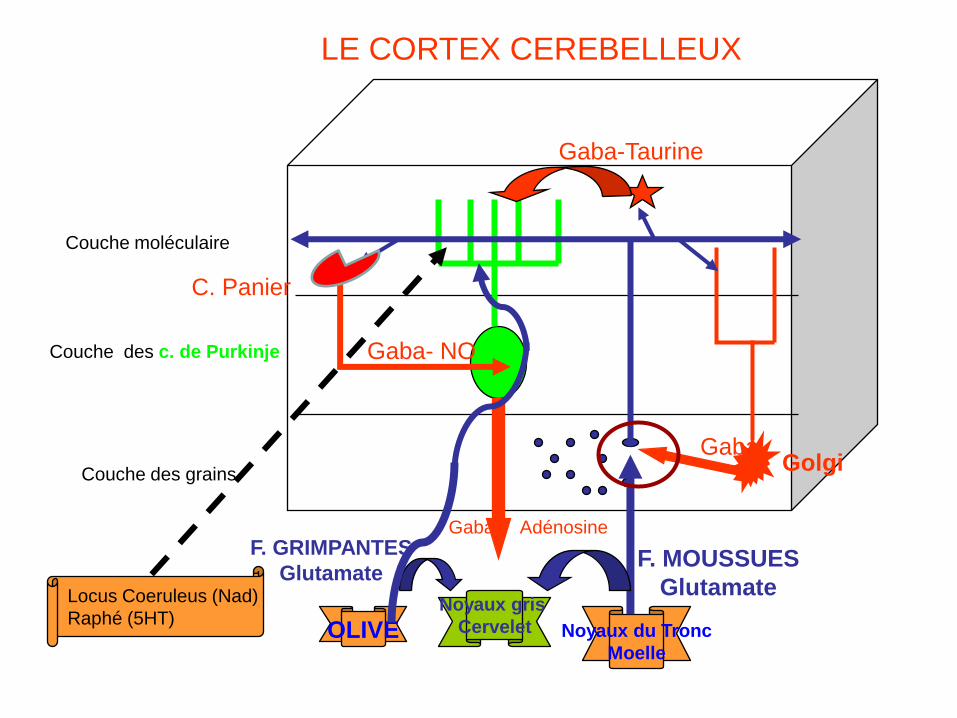
LE CORTEX CEREBELLEUX
OLIVE Noyaux du Tronc
Moelle
Noyaux gris
Cervelet
F. GRIMPANTES
GlutamateF. MOUSSUES
Glutamate
Gaba-Taurine
Gaba- NO
Gaba- Adénosine
Golgi
C. Panier
Gaba
Locus Coeruleus (Nad)
Raphé (5HT)
Couche moléculaire
Couche des c. de Purkinje
Couche des grains
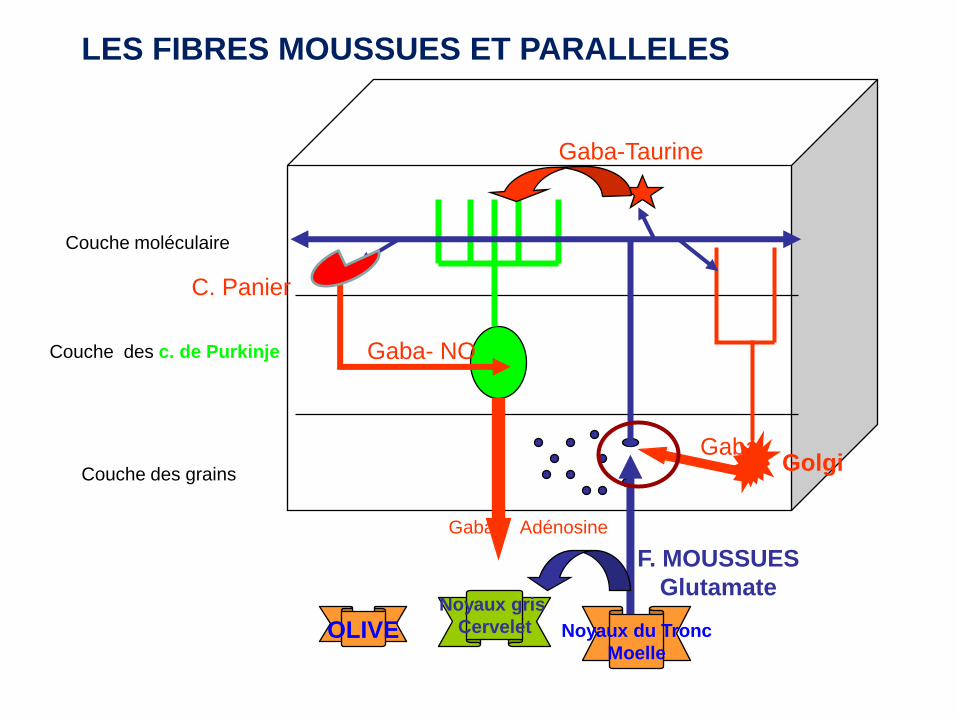
LES FIBRES MOUSSUES ET PARALLELES
OLIVE Noyaux du Tronc
Moelle
Noyaux gris
Cervelet
F. MOUSSUES
Glutamate
Gaba-Taurine
Gaba- NO
Gaba- Adénosine
Golgi
C. Panier
Gaba
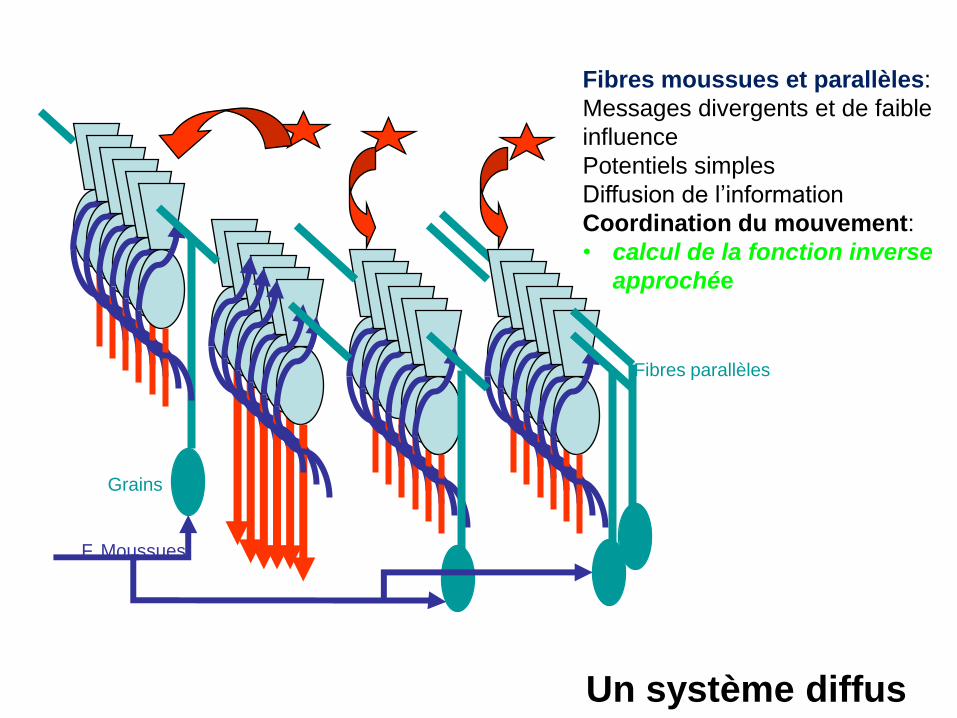
F. Moussues
Grains
Fibres parallèles
Fibres moussues et parallèles:
Messages divergents et de faible
influence
Potentiels simples
Diffusion de l’information
Coordination du mouvement:
• calcul de la fonction inverse
approchée
Un système diffus
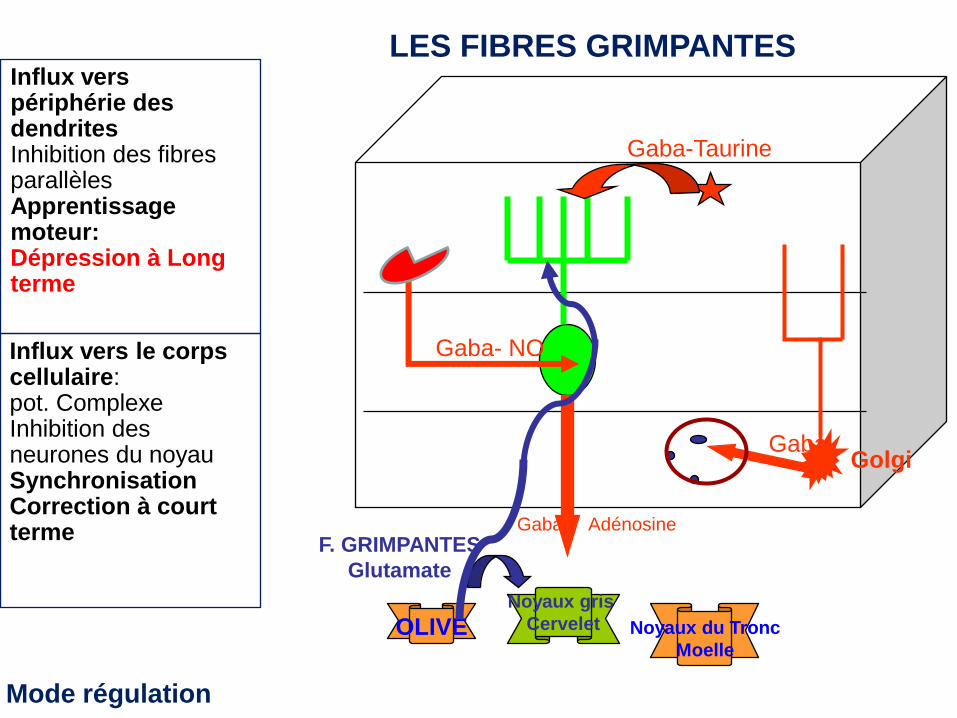
LES FIBRES GRIMPANTES
OLIVE Noyaux du Tronc
Moelle
Noyaux gris
Cervelet
F. GRIMPANTES
Glutamate
Gaba-Taurine
Gaba- NO
Gaba- Adénosine
GolgiGaba
Influx vers périphérie des dendritesInhibition des fibres parallèlesApprentissage moteur: Dépression à Long terme
Influx vers le corps cellulaire: pot. ComplexeInhibition des neurones du noyau SynchronisationCorrection à court terme
Mode régulation
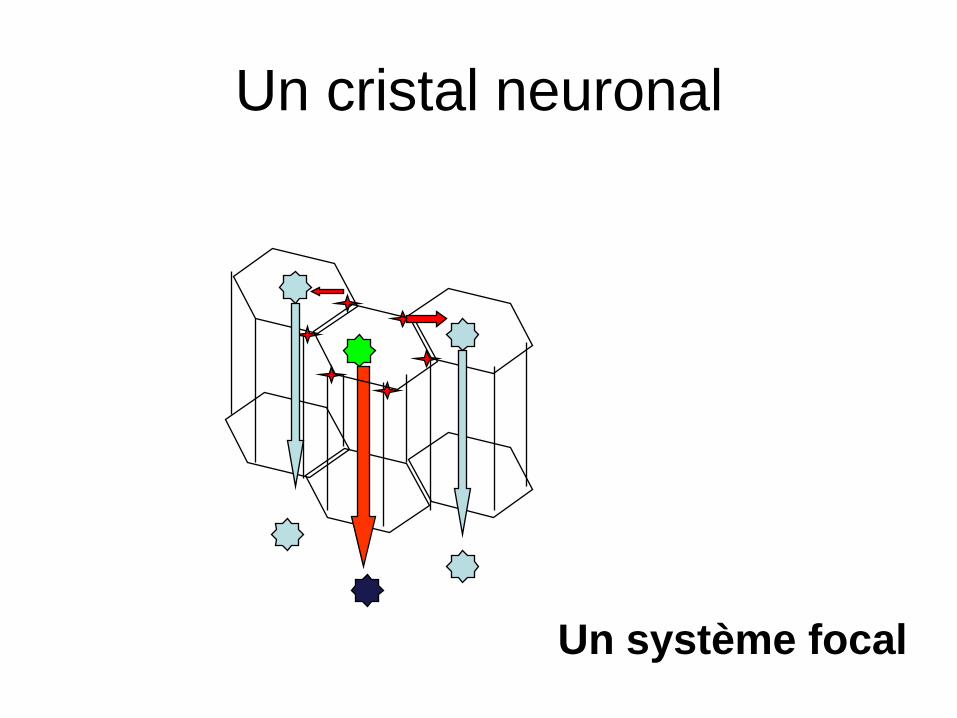
Un cristal neuronal
Un système focal

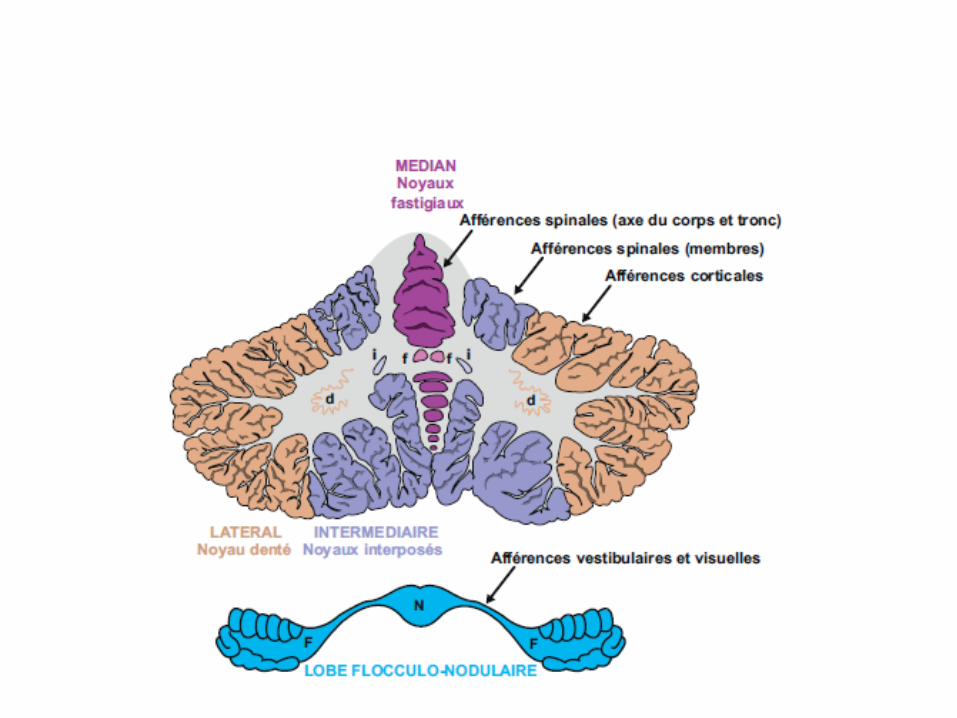
Noyaux Cérébelleux
OliveNoyaux Tronc
Moelle
F. Grimpantes
+ -
SPECIFICITE D ’ACTIVATION
F. Moussues
+
F. Parallèle
-Pot. SimplePot.complexe
-
+
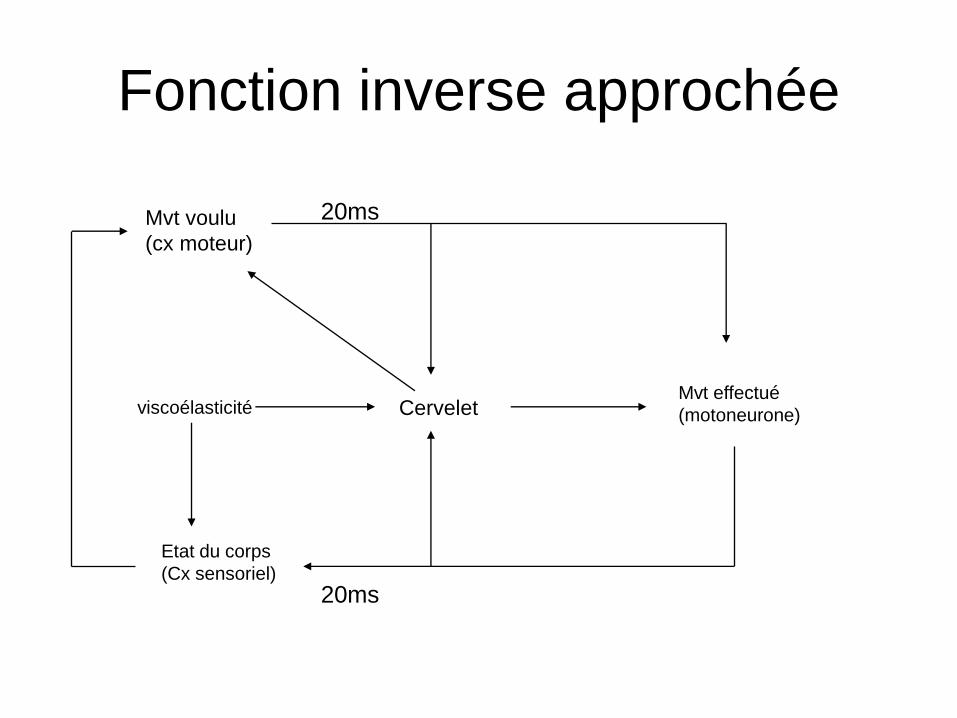
Fonction inverse approchée
Mvt voulu
(cx moteur)
Mvt effectué
(motoneurone)
Etat du corps
(Cx sensoriel)
20ms
20ms
viscoélasticité Cervelet
Fonction inverse approchée
• Traitement en continu de l’info sensori- motrice
• Intégration de la constante de temps
• Intégration de l’espace extérieur (trajectoire)
• Intégration de l’état intérieur
• Correction en continu et par anticipation de
l’ordre moteur
• Mouvement conforme au mouvement voulu
Apprentissage moteur
• Dépression à long terme
• Mémoire procédurale de gestes
complexes
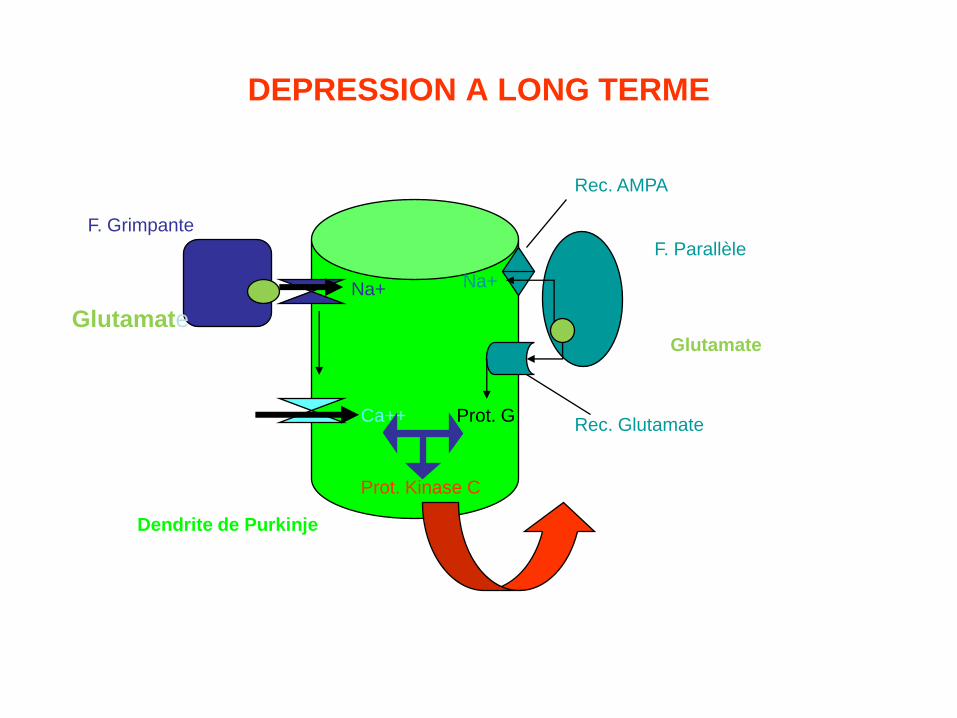
DEPRESSION A LONG TERME
F. Grimpante
Glutamate
Na+
Ca++
Dendrite de Purkinje
F. Parallèle
Glutamate
Na+
Rec. AMPA
Rec. GlutamateProt. G
Prot. Kinase C
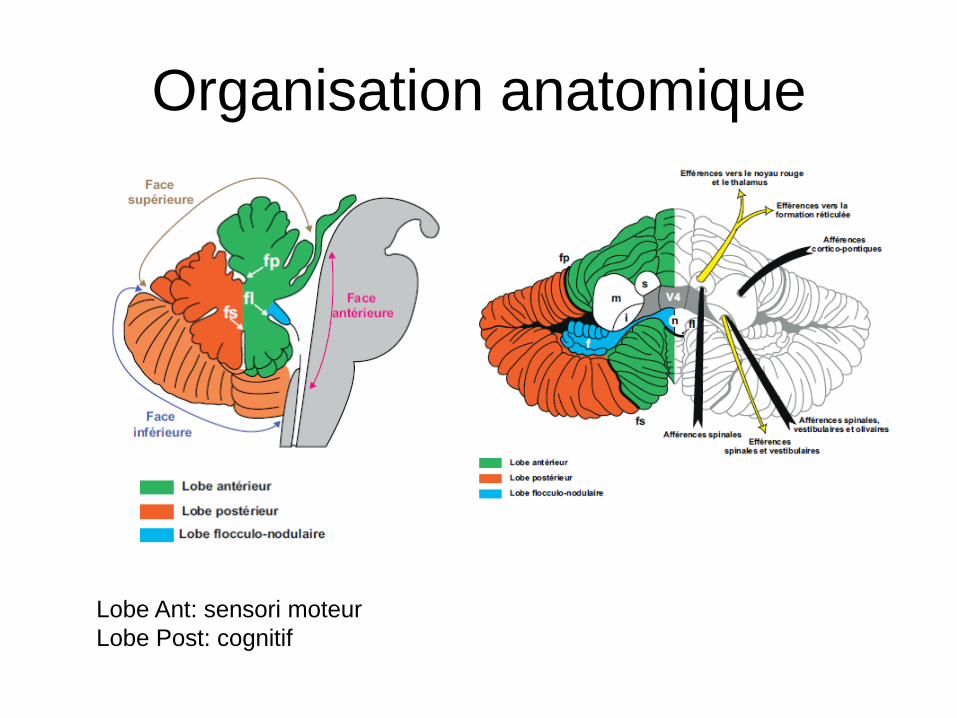
Organisation anatomique
Lobe Ant: sensori moteur
Lobe Post: cognitif
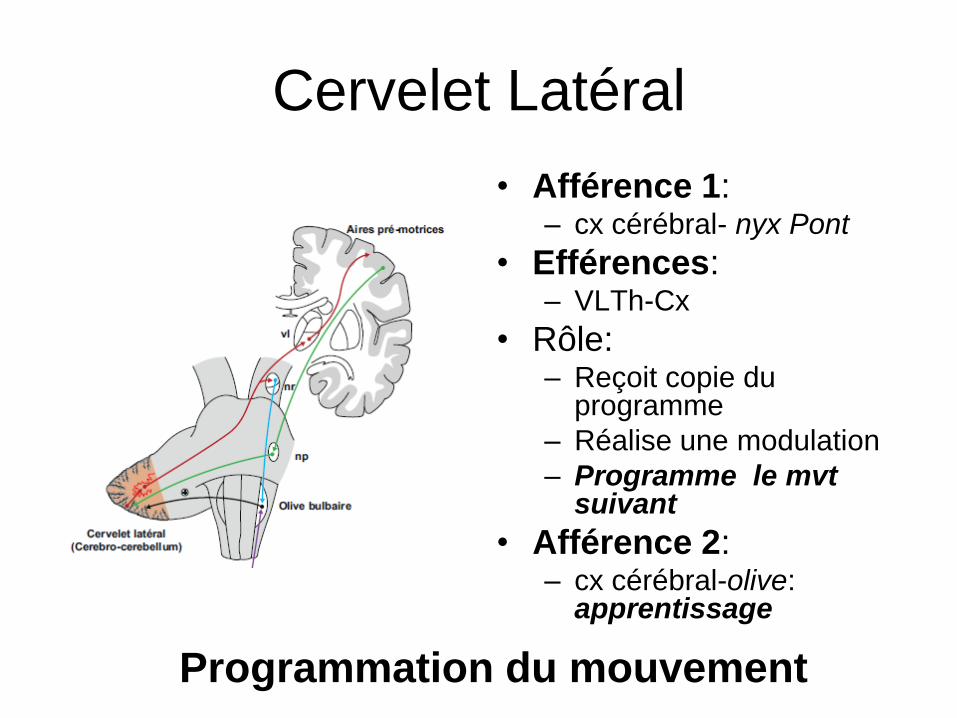
Cervelet Latéral
• Afférence 1: – cx cérébral- nyx Pont
• Efférences: – VLTh-Cx
• Rôle:– Reçoit copie du
programme
– Réalise une modulation
– Programme le mvtsuivant
• Afférence 2: – cx cérébral-olive:
apprentissage
Programmation du mouvement
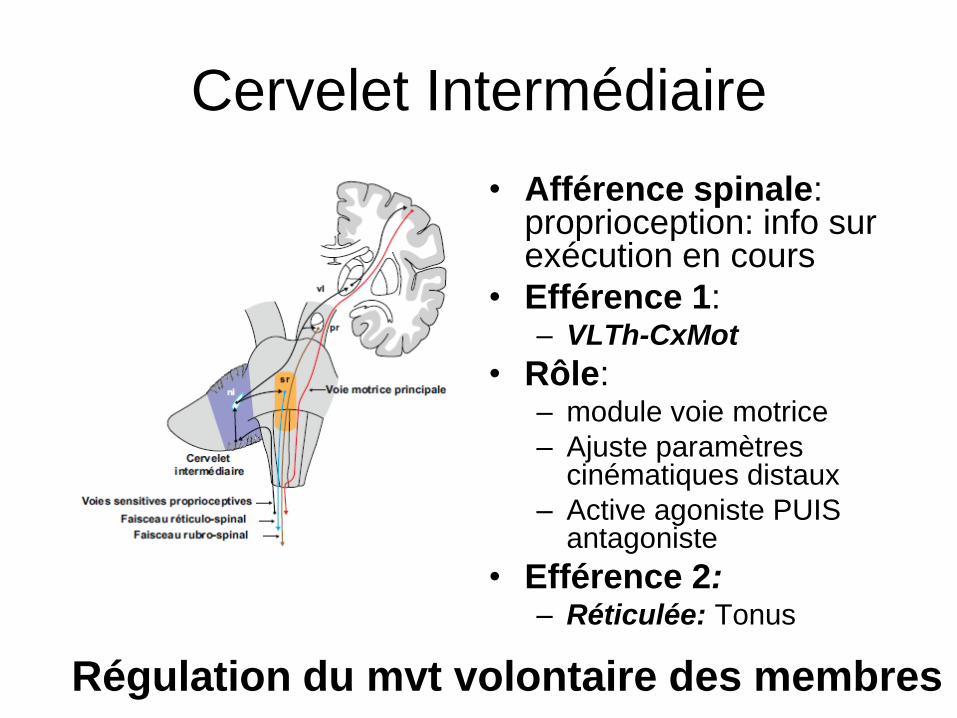
Cervelet Intermédiaire
• Afférence spinale: proprioception: info sur exécution en cours
• Efférence 1: – VLTh-CxMot
• Rôle: – module voie motrice
– Ajuste paramètres cinématiques distaux
– Active agoniste PUIS antagoniste
• Efférence 2:– Réticulée: Tonus
Régulation du mvt volontaire des membres

• Afférences:
– Spinale (proprioception)
– Réticulée
• Efférences:
– Vestibulo spinal: muscles paravertébraux et
proximaux: équilibre postural
– Réticulo spinal: tonus
– Réticulo Pontin: Ny oculomot: saccades
Contrôle muscles proximaux et axiaux:
érection du rachis et maintien de la tête
Cervelet Médian
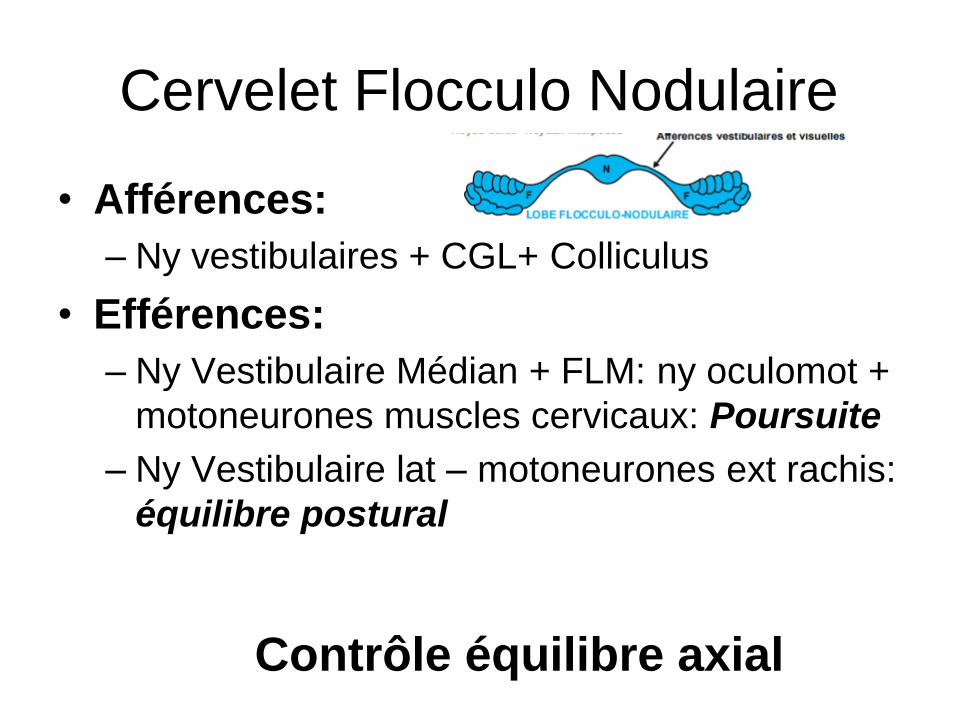
Cervelet Flocculo Nodulaire
• Afférences:
– Ny vestibulaires + CGL+ Colliculus
• Efférences:
– Ny Vestibulaire Médian + FLM: ny oculomot +
motoneurones muscles cervicaux: Poursuite
– Ny Vestibulaire lat – motoneurones ext rachis:
équilibre postural
Contrôle équilibre axial
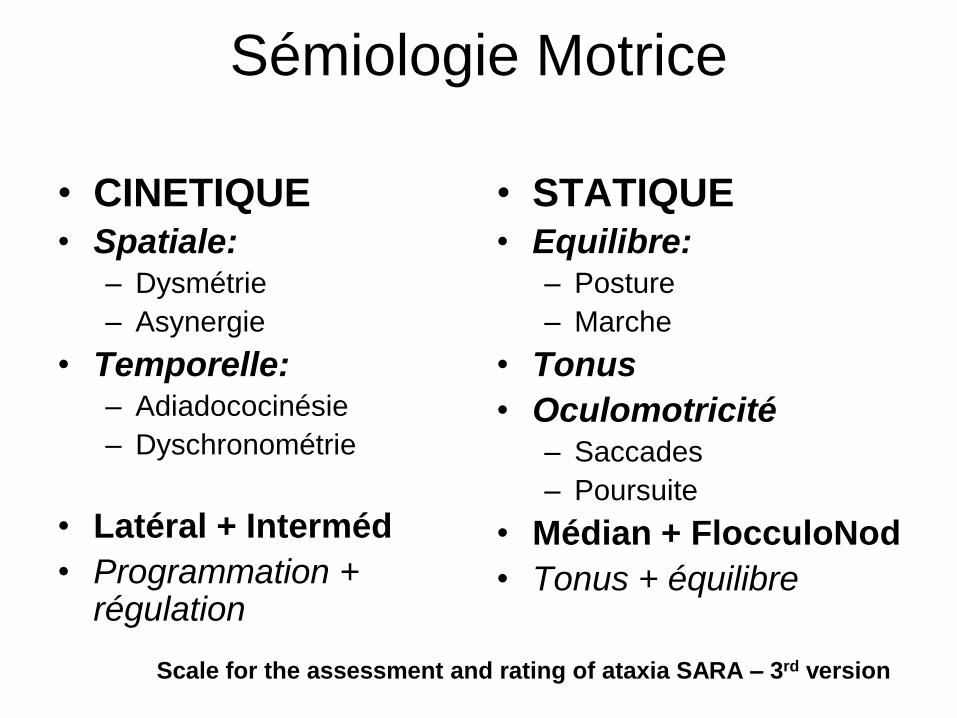
Sémiologie Motrice
• CINETIQUE
• Spatiale:– Dysmétrie
– Asynergie
• Temporelle:– Adiadococinésie
– Dyschronométrie
• Latéral + Interméd
• Programmation + régulation
• STATIQUE
• Equilibre:– Posture
– Marche
• Tonus
• Oculomotricité– Saccades
– Poursuite
• Médian + FlocculoNod
• Tonus + équilibre
Scale for the assessment and rating of ataxia SARA – 3rd version
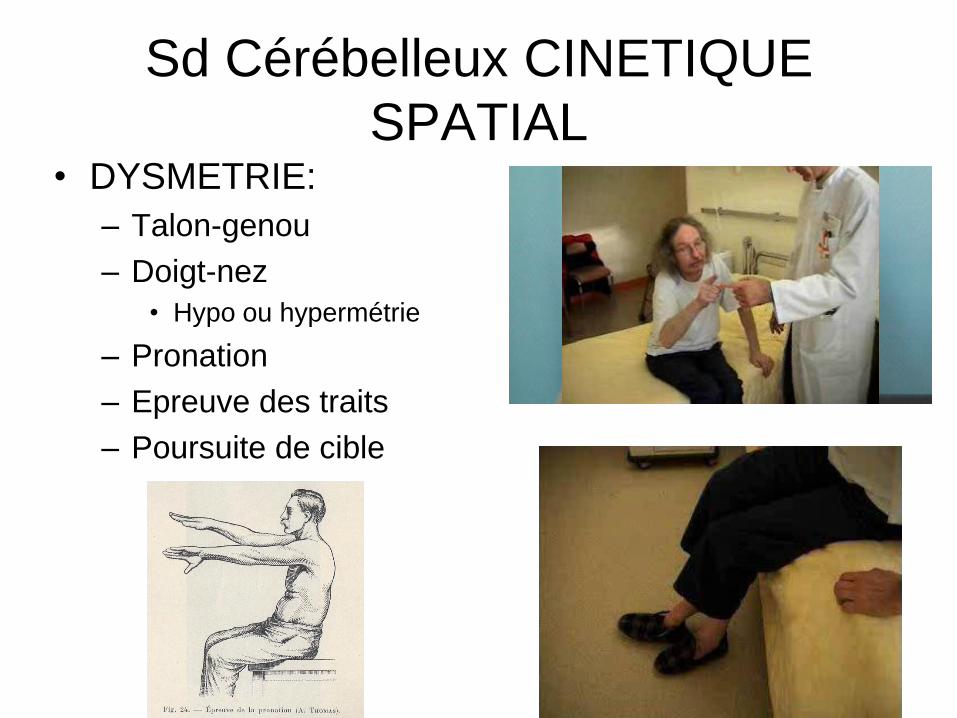
Sd Cérébelleux CINETIQUE
SPATIAL• DYSMETRIE:
– Talon-genou
– Doigt-nez
• Hypo ou hypermétrie
– Pronation
– Epreuve des traits
– Poursuite de cible

Poursuite de cible
• 5: Finger chase:
• Proband sits comfortably. If necessary, support of feet and trunk is allowed.
• Examiner sits in front of proband and performs 5 consecutive sudden and fast pointing movements in unpredictable directions in a frontal plane, within 50 % of proband´s reach.
• Movements have an amplitude of 30 cm and a frequency of 1 movement every 2 s.
• Proband is asked to follow the movements with his index finger, as fast and precisely as possible.
• Average performance of last 3 movements is rated.
• Slow and hypometric movement is rated 0 as long as patient is able to perform 5 pointing movements.
0 Normal,
1 Hypermetriaovershooting target<5
2 Hypermetria,< 15 cm
3 Hypermetria,> 15 cm
4 Unable to perform 5 pointing movements due to any reason
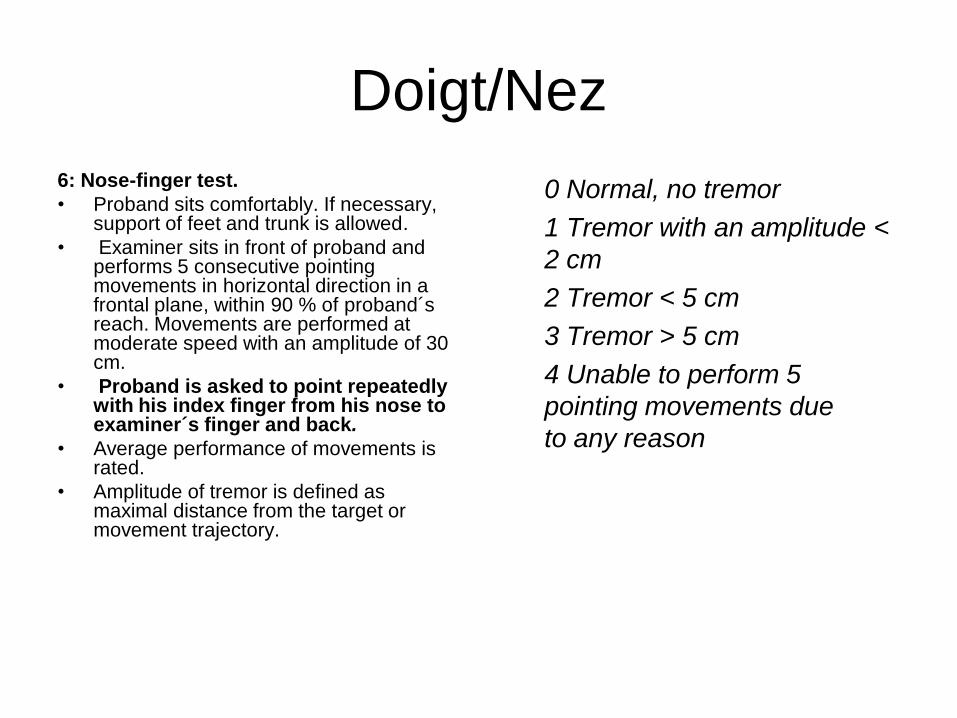
Doigt/Nez
6: Nose-finger test.
• Proband sits comfortably. If necessary, support of feet and trunk is allowed.
• Examiner sits in front of proband and performs 5 consecutive pointing movements in horizontal direction in a frontal plane, within 90 % of proband´sreach. Movements are performed at moderate speed with an amplitude of 30 cm.
• Proband is asked to point repeatedly with his index finger from his nose to examiner´s finger and back.
• Average performance of movements is rated.
• Amplitude of tremor is defined as maximal distance from the target or movement trajectory.
0 Normal, no tremor
1 Tremor with an amplitude <
2 cm
2 Tremor < 5 cm
3 Tremor > 5 cm
4 Unable to perform 5
pointing movements due
to any reason

Talon/genou
8) Heel-shin slide:
• rated separately for each side
• Proband lies on examination bed, without vision of his legs.
• Proband is asked to lift one leg, point with the heel to the opposite knee, slide down along the shin to the ankle, and to lay the leg back on the examination bed.
• The task is performed 3 times.
• Slide-down movements should
be performed within1 s.
• 0 Normal
• 1 Slight difficulties, contact to shin maintained
• 2 Clear difficulties, goes off shin up to 3 times during 3 cycles
• 3 Severely unstable, goes off shin 4 or more times during 3 cycles
• 4 Unable to perform the task
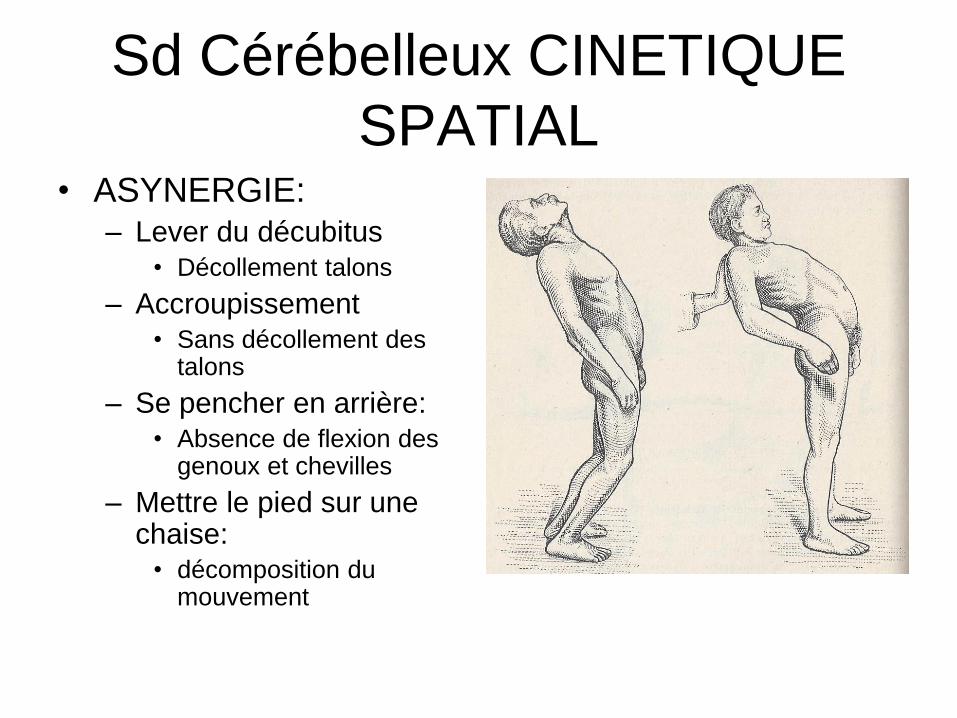
Sd Cérébelleux CINETIQUE
SPATIAL• ASYNERGIE:
– Lever du décubitus
• Décollement talons
– Accroupissement
• Sans décollement des talons
– Se pencher en arrière:
• Absence de flexion des genoux et chevilles
– Mettre le pied sur une chaise:
• décomposition du mouvement
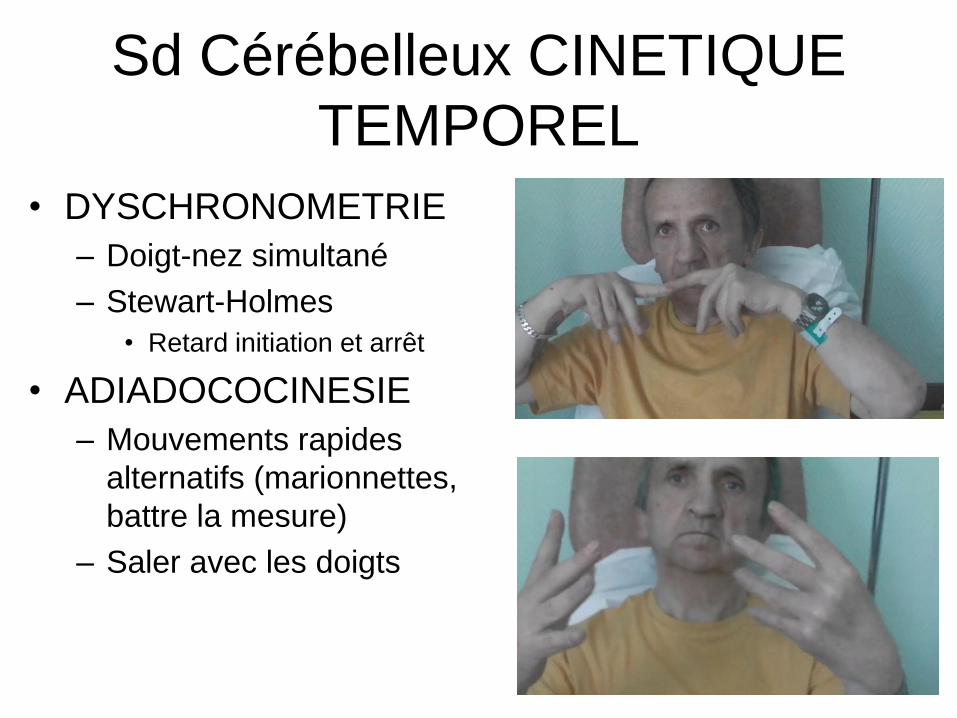
Sd Cérébelleux CINETIQUE
TEMPOREL
• DYSCHRONOMETRIE
– Doigt-nez simultané
– Stewart-Holmes
• Retard initiation et arrêt
• ADIADOCOCINESIE
– Mouvements rapides
alternatifs (marionnettes,
battre la mesure)
– Saler avec les doigts
Adiadiococinésie
7) Fast alternating hand movements:
rated separately for each side
• Proband sits comfortably. If necessary, support of feet and trunk is allowed.
• Proband is asked to perform 10 cycles of repetitive alternation of pro- and supinations of the hand on his/her thigh as fast and as precise as possible.
• Movement is demonstrated by examiner at a speed of approx. 10 cycles within 7 s.
• Exact times for movement execution have to be taken.
0 Normal, no irregularities (performs <10s)
1 Slightly irregular (<10s)
2 Clearly irregular, single movements difficult to distinguish or relevant interruptions (performs <10s)
3 Very irregular, single movements difficult to distinguish or relevant interruptions, >10s
4 Unable to complete 10 cycles due to any reason
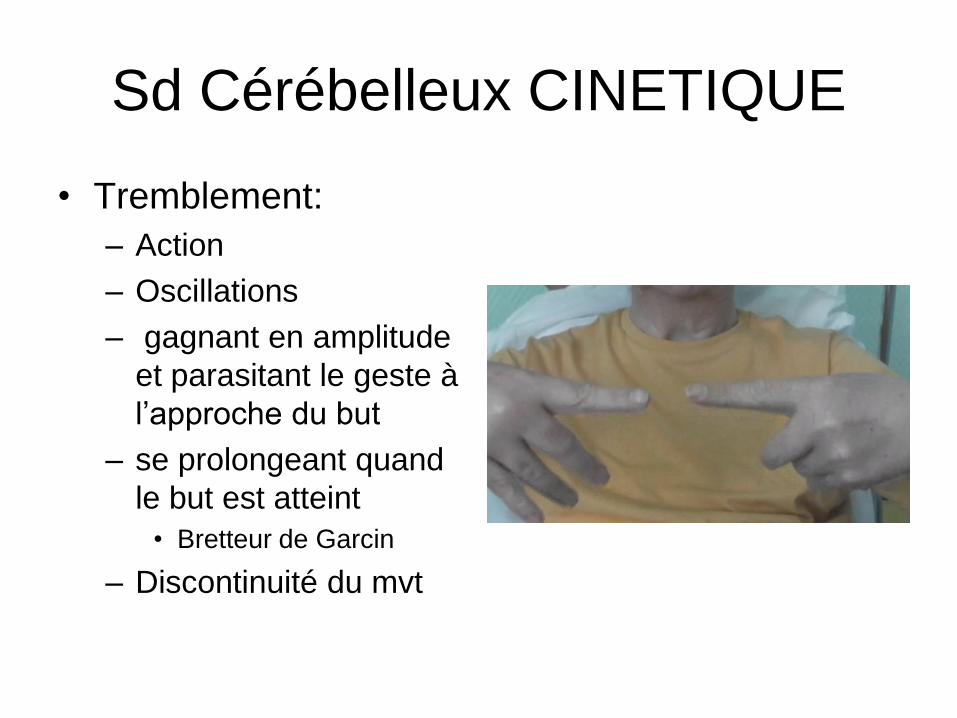
Sd Cérébelleux CINETIQUE
• Tremblement:
– Action
– Oscillations
– gagnant en amplitude
et parasitant le geste à
l’approche du but
– se prolongeant quand
le but est atteint
• Bretteur de Garcin
– Discontinuité du mvt
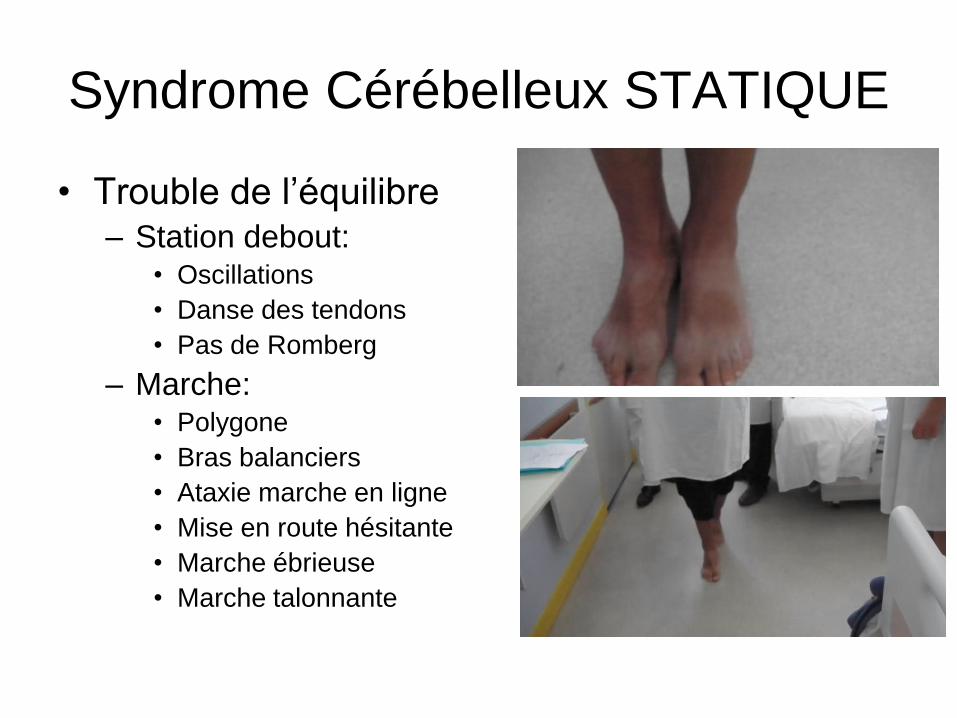
Syndrome Cérébelleux STATIQUE
• Trouble de l’équilibre– Station debout:
• Oscillations
• Danse des tendons
• Pas de Romberg
– Marche:• Polygone
• Bras balanciers
• Ataxie marche en ligne
• Mise en route hésitante
• Marche ébrieuse
• Marche talonnante
Marche
1) Gait
– Proband is asked
– (1) to walk in safe
distance from a wall
including a half-turn
(2) to walk in tandem
(both feet on one line,
no space between
heel and toes).
0: Normal, no difficulties in walking, turning or walking tandem (up to one misstep allowed)
1 Slight difficulties, only visible when walking 10
consecutive steps in tandem
2 Clearly abnormal, tandem walking >10 steps not possible
3 Considerable staggering, difficulties in half-turn, but without support
4 Marked staggering, intermittent support of the wall required
5 Severe staggering, permanent support of one stick or light support by one arm required
6 Walking > 10 m only with strong support (two special sticks or stroller or accompanying person)
7 Walking < 10 m only with strong support (two special sticks or stroller or accompanying person)
8 Unable to walk, even with accompanying person
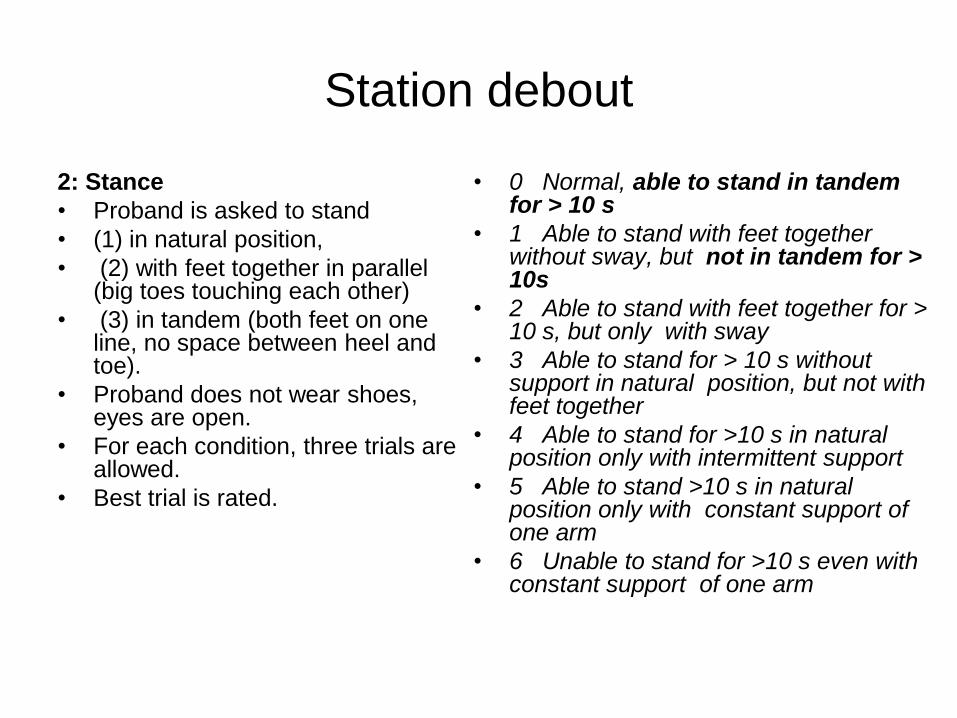
Station debout
2: Stance
• Proband is asked to stand
• (1) in natural position,
• (2) with feet together in parallel (big toes touching each other)
• (3) in tandem (both feet on one line, no space between heel and toe).
• Proband does not wear shoes, eyes are open.
• For each condition, three trials are allowed.
• Best trial is rated.
• 0 Normal, able to stand in tandem for > 10 s
• 1 Able to stand with feet together without sway, but not in tandem for > 10s
• 2 Able to stand with feet together for > 10 s, but only with sway
• 3 Able to stand for > 10 s without support in natural position, but not with feet together
• 4 Able to stand for >10 s in natural position only with intermittent support
• 5 Able to stand >10 s in natural position only with constant support of one arm
• 6 Unable to stand for >10 s even with constant support of one arm

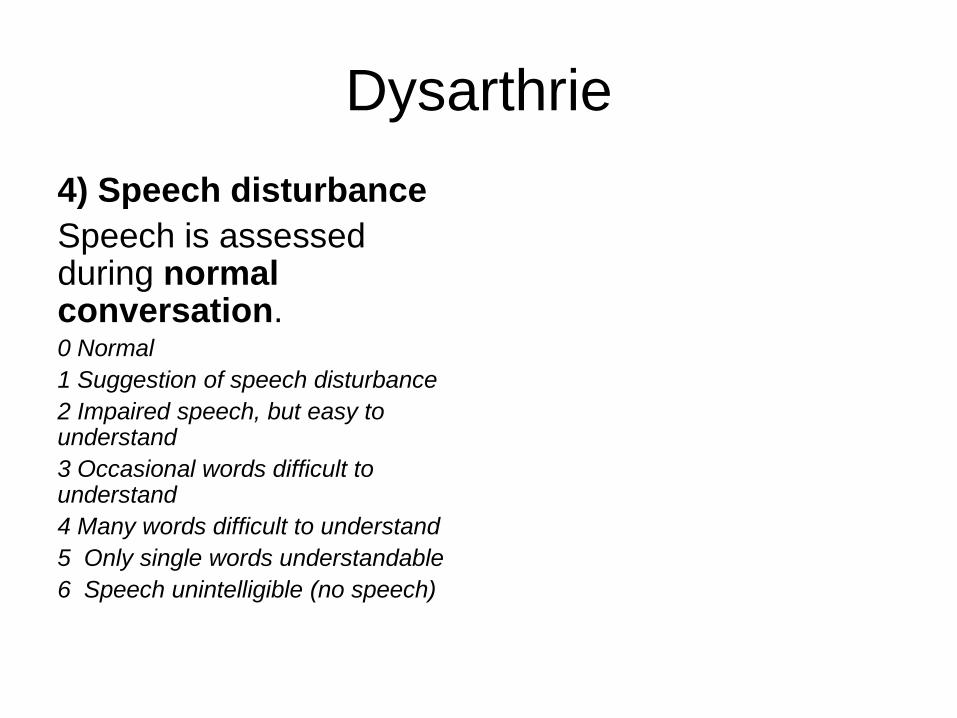
Dysarthrie
4) Speech disturbance
Speech is assessed during normal conversation.0 Normal
1 Suggestion of speech disturbance
2 Impaired speech, but easy to understand
3 Occasional words difficult to understand
4 Many words difficult to understand
5 Only single words understandable
6 Speech unintelligible (no speech)
Autres Troubles
• Hypotonie:
– Atteinte réticulospinale
– Cervelet médian
• ROT pendulaires
Autres échelles
• FARS: Friedreich Ataxia Rating Scale
• ICARS: International Coopérative Ataxia Rating Scale (16 items)– Mvt yeux
– Atteinte bulbaire
– Dysarthrie
– Neuropathie périphérique
– Coordination • Bretteur
• Doigt Nez
• Dysmétrie
• Adiadococinésie
• Talon/genou
• Pointage
• Stabilité posturale (pieds joints/ tandem)
• Marche (normale, tandem)
• Ecriture