Embed Size (px)
Citation preview

Physiology of AgingNisha Rughwani, MD
Associate Professor
September 13, 2017

Objectives
At the end of this session, participants will be able to:
1. Discuss the characteristics of aging
2. Review the various theories of aging
3. Explore the effects of aging on the different organ
systems

Case: Mrs. LL
Mrs. LL is a 75 year old woman with a h/o osteoporosis and left
hip osteoarthritis. She is transferring her care to you because
she “isn’t getting any younger” and wants to see someone who
specializes in the care of older adults.
At the end of your visit, she asks “Why do people have to get
older anyways?”

Aging
▶ Is not a disease
▶ Occurs at different rates
– Among individuals
– Within individuals
▶ Doesn’t always cause symptoms
4

Characteristics of Mammalian Aging
▶ Cellular and Physiological Deterioration
▶ Increased mortality with age following maturation
▶ Increased vulnerability to disease
▶ Decreased ability to adapt to stress
– Impaired homeostasis
5
From Usual to Successful Aging – a
Clinical Approach
▶ Normalizing
– Adjust to likely changes (e.g. sleep/wake bowels, balance,
benign forgetfulness)
– Identify potential symptoms of disease (sleep apnea, depression,
hypothyroidism, gait disorder, cognitive impairment)
▶ Maintain or improve modifiable causes of age-related change
– Exposures (UV radiation, noise)
– Psychological well being (social isolation)
– Cognition (mental inactivity)
– Nutrition (cholesterol, sodium, calcium)
– Exercise (fitness, strength, balance)
6

Theories of Aging

Characteristics of Aging
Aging is the loss of homeostasis, or a breakdown in maintenance of specific molecular structures and pathways
Biochemical composition of tissue changes
Physiologic capacity decreases
Susceptibility and vulnerability to disease increases
Mortality increases
Both environmental and genetic factorsinfluence the rate of aging

Theories of Aging
▶ Evolutionary Theories of Aging
– Explain historical and evolutionary aspects of aging
▶ Psychosocial Theories of Aging
– Explain behavioral, cognitive, and social features of aging
▶ Physiologic Theories of Aging
– Explain structural and functional age changes and elaborate a framework for translating what is happening on a molecular level to organ system level

Evolutionary Theories of Aging
▶ Mutation Accumulation Theory– Aging viewed as a non-adaptive trait because there is no
selective pressure on older, post-reproductive organisms
– Late acting genes accumulate over time and result in an aging phenotype
▶ Antagonistic Pleiotropy Theory– Pleiotropy: single gene controls or influences multiple traits
– Aging viewed as an adaptive trait
– Genes that can influence several traits are selected for and affect individual fitness in opposite ways at different stages of life

Psychosocial Theories of Aging
▶ Activity Theory– Highlights maintenance of and alerations in regular activities,
roles, and social pursuits as a coping strategy
▶ Life-Course Theory– Aging is the progressive adjustment of older individuals to
changes associated with increasing age, such as declining health, retirement, new living arrangements, etc…
▶ Continuity Theory– Older adults seek to use familiar strategies in familiar areas of
life as an adaptive strategy to deal with changes that occur during normal aging
▶ Gerotranscendence Theory– Shift in perspective from materialistic/rational to more
cosmic/trancendent life view as part of goal of achieving wisdom and maturity

Homeostasis Physiologic Theories of Aging
DNA Integrity and Stability Targeted DNA Damage TheoryMitochondrial DNA Damage TheoryTelomere TheoryTransposable Element Activation TheoryEpigenetic Theory
Synthesis Fidelity Error Catastrophe Theory
Defense Against Free Radicals
Free Radial Theory
Clearance of Defective Components
Accumulation Theory
Physiologic Signaling Endocrine Theory
Response to Pathogens/Injury
Immunologic/Immunosenescence Theory
Physical Reserves Stem Cell Theory
Theories of Aging: DNA Stability
▶ Targeted DNA damage– Cumulative nuclear DNA deletions, mutations and
translocations → altered functional capacity of proteins and cells
▶ Mitochondrial DNA damage– Mitochondrial DNA has higher frequency of mutations →
altered efficiency of respiration/ATP production increased free radicals
▶ Telomere– Loss of telomerase length and activity senescence
Theories of Aging: DNA Stability
▶ Transposable Element Activation– Activation of endogenous transposable elements insertional
mutagenesis, DNA damage, genome rearrangements
▶ Epigenetic– Cumulative errors in RNA/protein synthesis accelerated loss
of function

Theories of Aging: Synthesis Fidelity
▶ Error Catastrophe
– Cumulative errors in RNA/protein synthesis Critical threshold Accelerating loss of function
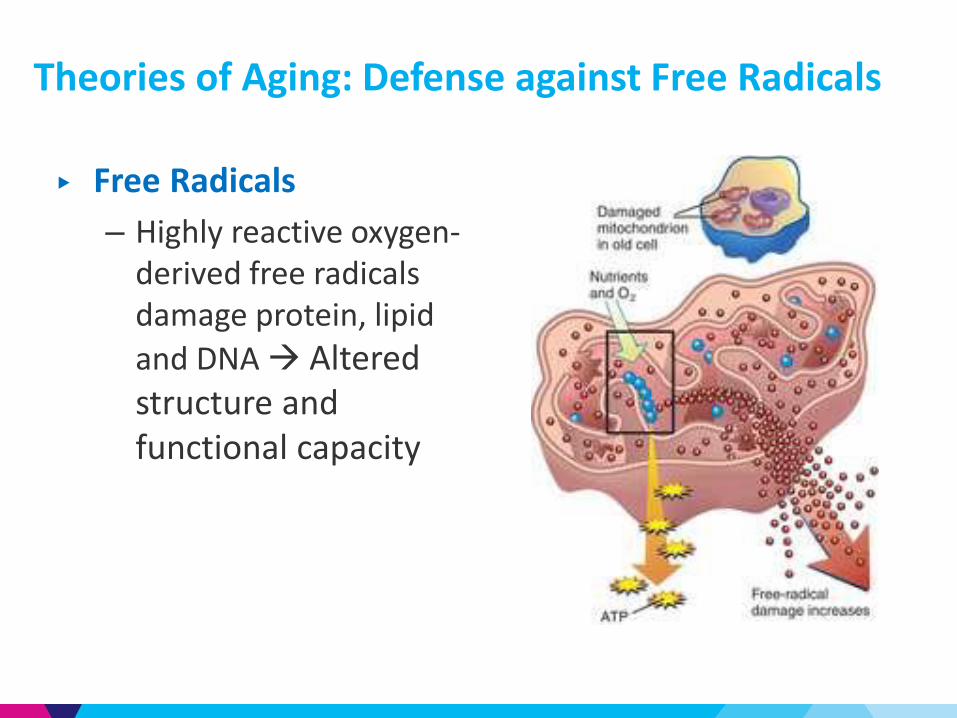
Theories of Aging: Defense against Free Radicals
▶ Free Radicals
– Highly reactive oxygen-derived free radicals damage protein, lipid
and DNA Altered structure and functional capacity

▶ Accumulation Theory: inability to clear defective components– Abnormal proteins, lipids, and/or organelles are not removed
compromised cellular/tissue functional capacity
▶ Rate of Living: changes in energy metabolism– Changes in energy availability, body size, and composition act
independently and in concert to modify life span
▶ Endocrine: changes in physiologic signaling– Age-related changes in the kinetics and levels of hormone
secretion Loss of functional capacity in target organ systems
Theories of Aging

▶ Immunologic, Immunosenescence
– Time-acquired deficits in immune response and T-cell function predisposes to infection and disease
– Accumulation of senescent immune cells increases production of pro-inflammatory cytokines → chronic molecular inflammation with systemic effects
Theories of Aging: Defense against Pathogens, Injury
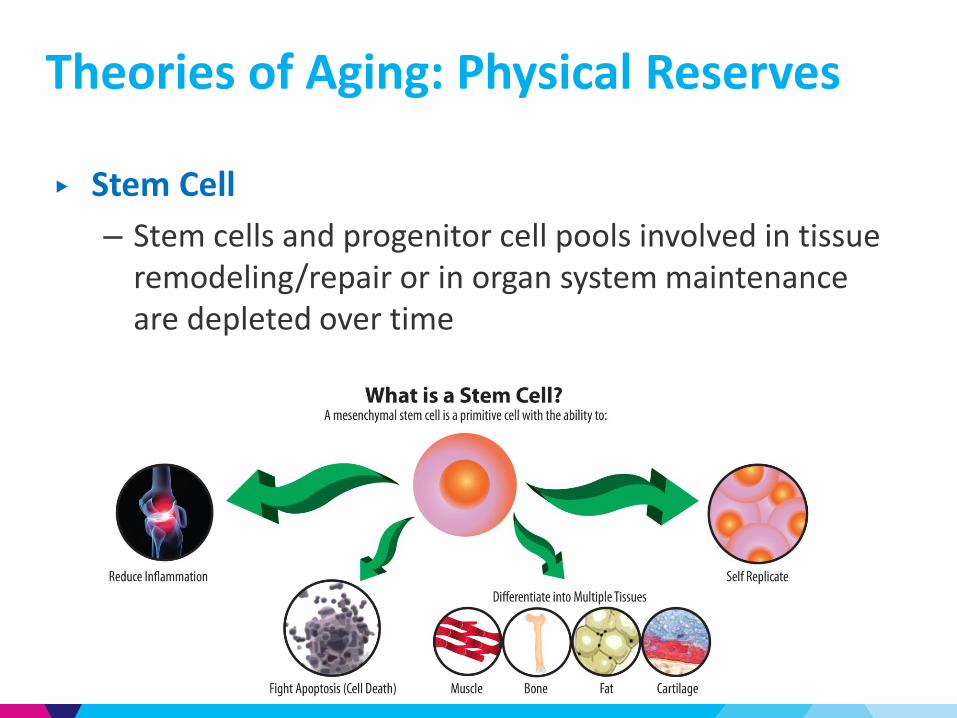
▶ Stem Cell
– Stem cells and progenitor cell pools involved in tissue remodeling/repair or in organ system maintenance are depleted over time
Theories of Aging: Physical Reserves

Sample Boards QuestionIn a report published in 2011, researchers used a transgenic strategy to selectively ablate cells expressing the cyclin-dependent kinase inhibitor and tumor suppressor gene p16-Ink4a, which is known to accumulate with age in various mouse and human tissues. These experiments were conducted on mice with a BubR1 hypomorphic background; the mice exhibit short life span and multiple progressive age-related phenotypes. Administration of a drug to target and continually remove the p16-expressing cells delayed the onset of multiple aging end points, including the onset of skeletal muscle loss, cataracts, and fat. Although the mice in this study did not live longer, they remained healthy for a longer period. These results have raised questions about whether removal of old, senescent cells from aged tissues will improve function, limit tumorigenesis, and increase health span in human beings.
Which one of the following best explains the effects seen from p16 cell clearance in this study?
A) Epigenetic Shifts
B) Attenuation of transposable element activation
C) Change in homeostasis
D) Rate of living theory20

ANSWER C) Change in homeostasisIn the case of tissue and organ deterioration related to cellular senescence and aging, accumulating levels of damaged and stressed cells may deplete various pools of stem and progenitor cells, promote chronic inflammation, and induce aberrant cell differentiation, thereby contributing to overall losses in tissue homeostasis, architecture, and regenerative function. In the case presented, removal of p16-expressing old cells markedly improved preservation of homeostasis of healthy tissue function, even during advanced age.
A) Although epigenetic changes occur with age, there is no evidence here that removal of p16-expressing cells alone would contribute to global epigenetic shifts that favor functional improvement.
B) The possibility that p16 expression might arise as a consequence of transposable element activation in some cells is not well supported in the above scenario. Rate of living theory is likewise not well supported.
D) In the study cited, the impact was on health span, not life span.21
Sample Boards Question

Case: Mrs LL
Mrs LL thanks you for the information. She is committed to eating a healthy diet and continuing with regular exercise to hopefully stave off some of the effects of aging

Effects of Aging on Specific Organ Systems
Case: Mrs LLShe returns to you 6 months later complaining of increasingly severe shortness of breath on exertion over the past 3 months. For the past 20 years, she has walked 30 minutes three times weekly at a fairly rapid pace without symptoms. She has no chest pain, wheezing, or cough. Blood pressure is 140/85 mm Hg. On examination, the lungs are clear and there is no evidence of wheezing. Radiographs of the chest and an electrocardiogram show normal findings. Which of the following additional findings would require further evaluation?
A. Arterial PO2 of 80 mm Hg
B. Decreased cardiac output on ultrasonography
C. Decreased maximum heart rate on stress testing
D. Decreased vital capacity on pulmonary function testing
E. Presence of an S4 gallop

Cardiovascular

Cardiovascular: Changes in Structure
Age-Associated Changes Possible Disease Outcomes
↑ Vascular Intimal Thickening Early stages of atherosclerosis
↑ Vascular Stiffness
Systolic HTN
Stroke
Atherosclerosis
↑ LV Wall Thickness
↓ Early diastolic cardiac filling
↑ Cardiac filling pressure
Lower threshold for dyspnea
↑ Left Atrial Size Atrial Fibrillation

Cardiovascular: Changes in Function
Age-Associated Changes Possible Disease Outcomes
Altered regulation of vascular tone
Vascular stiffening
Hypertension
↓ Cardiovascular Reserve
↓ Threshold for heart failure exacerbation
↑ Severity of heart failure
Pulmonary

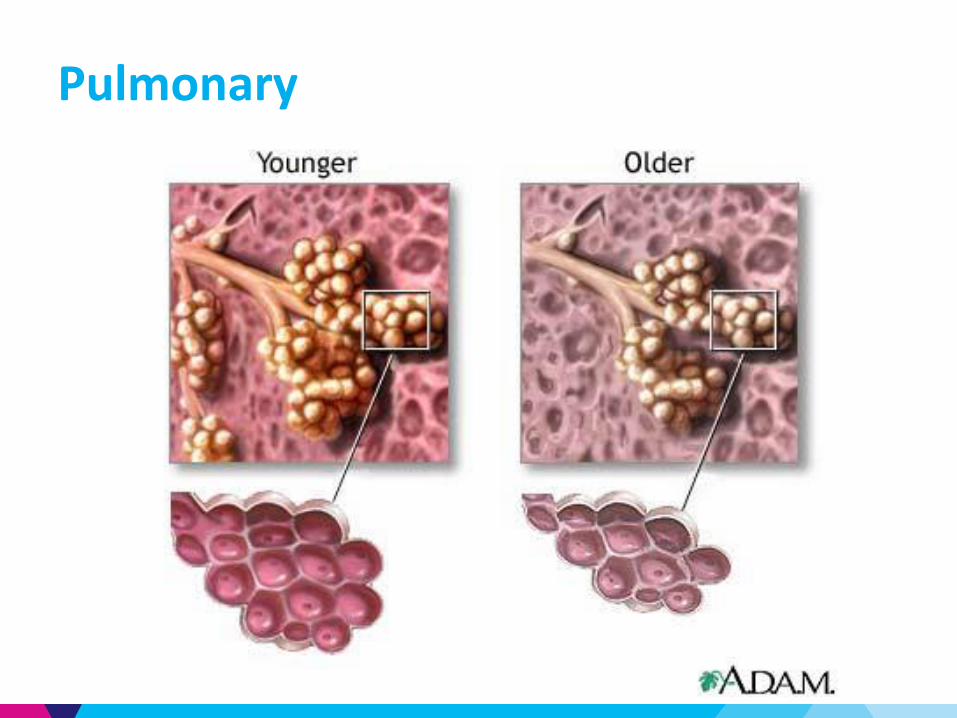
Pulmonary: Changes in Structure
Age-Associated Changes Consequence
↓ Alveoli and lung capillaries ↓ Lung mass
↓ Number and elasticity of parenchymal elastic fibers
↓ Elastic recoil of the lungs
Stiffening of chest wall
↓ Airway size
↓ Effectiveness of ciliary action
Respiratory muscles weaken, including diaphragm by up to 25%

Pulmonary: Changes in Function
Pulmonary: Changes in Function
▶ ↓ FEV1 and FVC
▶ ↑ Residual volume
▶ Ventilation-Perfusion mismatching leads to ↓ PaO2
– Estimated PaO2 = [100 – (0.32 x age)]
▶ ↓ Maximum inspiratory and expiratory pressures
▶ ↓ Diffusion of CO2
▶ ↓ Ventilatory response to hypercapnia
▶ ↓ Effort dependent and independent respiration (quiet and forced breathing)
▶ ↓ Exercise tolerance and pulmonary reserve

Case: Mrs LLShe returns to you 6 months later complaining of increasingly severe shortness of breath on exertion over the past 3 months. For the past 20 years, she has walked 30 minutes three times weekly at a fairly rapid pace without symptoms. She has no chest pain, wheezing, or cough. Blood pressure is 140/85 mm Hg. On examination, the lungs are clear and there is no evidence of wheezing. Radiographs of the chest and an electrocardiogram show normal findings. Which of the following additional findings would require further evaluation?
A. Arterial PO2 of 80 mm Hg
B. Decreased cardiac output on ultrasonography
C. Decreased maximum heart rate on stress testing
D. Decreased vital capacity on pulmonary function testing
E. Presence of an S4 gallop

ANSWER: B) Decreased cardiac output on ultrasonographyCardiac output both at rest and with moderate exercise changes slightly with age (1%/year). A finding of ↓ cardiac output in this patient would suggest an underlying disease.
A) Arterial PO2 ↓ with age because of an age-related increase in ventilation-perfusion mismatch. The age-expected normal Pa O2 is determined by calculating 100 minus (0.325 × patient age).
C) Maximum HR ↓ with age. The age-expected normal maximal heart rate is 220-age
D) Vital capacity ↓ with age. Total lung capacity does not change with age. Residual volume ↑ substantially in older persons.
E) An S4 gallop may occur without underlying disease in persons older than 80 years. ↓ early ventricular filling velocities are caused by aged, less compliant ventricles.

Case: Mrs LLYou order routine labs for Mrs. LL including a complete blood count, comprehensive metabolic panel, erythrocyte sedimentation rate (ESR) lipid panel, and fasting glucose.
Which of the following laboratory findings should lead to further work-up?
A. Erythrocyte sedimentation rate: 45 mm/h
B. Alkaline phosphatase: 130 U/L
C. Total cholesterol: 210 mg/dL
D. 1-hour postprandial glucose: 160 mg/dL
E. Magnesium: 1.4 mg/dL

Renal

Renal: Changes in Structure
Age-Associated Changes Consequence
↓ Kidney size, weight, and number of functional glomeruli
Renal mass ↓ 25%
- mainly cortical
↓ Number/length of functional renal tubules
Impaired permeability
↓ ability to resorb glucose
↓ Reno-vascular bed ↓ Renal Blood flow

Renal: Changes in Function
Age-Associated Changes Consequence
↓ Cr clearance and GFR
(↓ 10mL/decade) ↓ Excretion of drugs, toxins
↓ Concentrating/diluting capacity
↑ Fluid and electrolyte abnormalities
↓ Ability to resorb glucose
↓ Serum renin and aldosterone by 30-50%
↑ Volume depletion
↑ Risk of hyperkalemia
↓ Na and K excretion and conservation
↓ Vitamin D activation Vitamin D deficiency

Gastrointestinal

GI: Changes in Structure
Age-Associated Changes Possible Disease Outcomes
↑ Tongue varicosities
↓ Saliva production
↑ Oral infections
↑ Gum disease
↓ Liver size and blood flowImpaired clearance of drugs requiring phase I metabolism
Impaired response to gastric mucosal injury
↑ Risk of gastric and duodenal ulcers
↓ Pancreatic mass and enzyme reserves
↑ Insulin resistance
↓ Effective colonic contractions ↑ Constipation
↓ Gut-associated lymphoid tissue↑ Risk of gastric & duodenal ulcers

GI: Changes in Function
Age-Associated Changes Possible Disease Outcomes
↓ Stomach acid productionAtrophic gastritis↓ B12 and iron absorption
Impaired acid clearance GERD
Slowing of gastric emptyingProlong gastric distention ↑ Meal-induced satiety
↓ Ca absorption Bone loss
Delay in colonic transit ↓ Rectal wall sensitivity
Constipation
↓ Tensile strength in smooth muscle of colonic wall Diverticulosis
↓ Insulin secretion ↑ Insulin resistance

Endocrine
GlandAge-Associated
ChangesConsequences
Pituitary
↓ Pulsatile secretion pattern (ex: nocturnal secretion of prolactin)
↓ Size of various structures ↓ Lean body mass:fatratio
Pineal ↓ Diurnal melatonin rhythm
Insomnia ↓ Free-radical defenses
ThymusAtrophy↓ Thymosin levels
↓ Immune function↑ Risk of infection and cancer

Endocrine

Endocrine
GlandAge-Associated
ChangesConsequences
Thyroid
Atrophy↑ Fibrosis and nodule formation ↓ T4 production in the very old
↑ Rate of hypo- and hyperthyroidism
Parathyroid
↑ fat deposition without atrophyIn women >40 y/o- ↑ in PTH and ↓ metabolism - ↓ in 1,25 (OH) vitamin D levels - Changes in bone mineral homeostasis
Vitamin D deficiency

Endocrine
GlandAge-Associated
ChangesConsequences
Adrenal ↓ Aldosteronesecretion
Orthostatic hypotension Masculinization of post-menopausal women
Male Gonads
↓ DHEA and DHEA–S, pregnenolone and testosterone levels Change in diurnal rhythm
Changes in skin, hair, muscle and bone. ↓ Body fat
Female Gonads↓ Estrogen and progesterone > 70 y/o ↓ Leptin
Skin changes↑ LDL ↓ Bone minerals↓ Body fat
Hematology
▶ ↓ Hematopoietic tissue in bone marrow
▶ ↓ Stem cells in bone marrow
▶ ↓ Incorporation of iron into RBC slowed erythropoiesis
▶ ↓ (slightly) Average hemoglobin/hematocrit

Case: Mrs LLYou order routine labs for Mrs LL including a complete blood count, comprehensive metabolic panel, erytorcyte sedimentation rate (ESR) lipid panel, and fasting glucose.
Which of the following laboratory findings should lead to further work-up?
A. Erythrocyte sedimentation rate: 45 mm/h
B. Alkaline phosphatase: 130 U/L
C. Total cholesterol: 210 mg/dL
D. 1-hour postprandial glucose: 160 mg/dL
E. Magnesium: 1.4 mg/dL

Case: Mrs LLYou order routine labs for Mrs. LL including a complete blood count, comprehensive metabolic panel, erythrocyte sedimentation rate (ESR) lipid panel, and fasting glucose.
Which of the following laboratory findings should lead to further work-up?
A. Erythrocyte sedimentation rate: 45 mm/h
B. Alkaline phosphatase: 130 U/L
C. Total cholesterol: 210 mg/dL
D. 1-hour postprandial glucose: 160 mg/dL
E. Magnesium: 1.4 mg/dL

ANSWER: (E) Magnesium: 1.4 mg/dL
Mg - 1.4 mg/dL represents a ↓ beyond the amount expected with normal aging and hence should prompt further work-up. Serum Mg ↓ by about 15% between the 20s and 70s.
A) ESR tends to ↑ about 10 to 13 mm/h between the ages of 20 and 80 years and is associated with a similar ↑ in C-reactive protein.
B) The alkaline phosphatase level ↑ by 20% between the 20s and 70s, a change that is unassociated with clinical problems.
C) The total cholesterol level ↑ with age, with a more important ↓ in high-density lipoprotein cholesterol in women as they lose estrogen protection.
D) The postprandial glucose level ↑ with age, a change also reflected in ↑ levels of hemoglobin A1c.
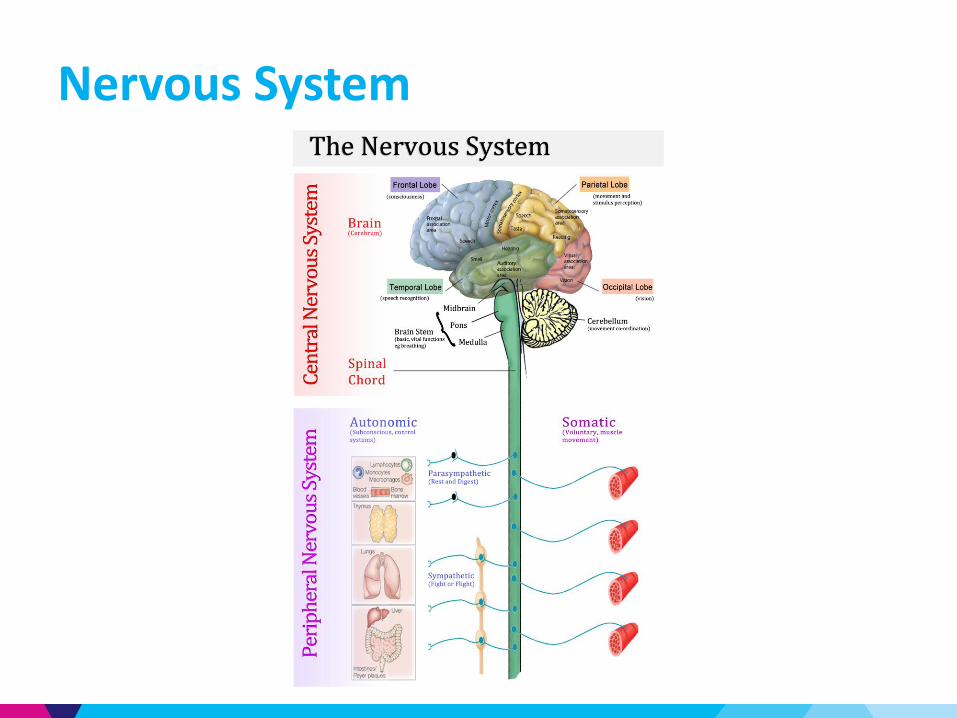
Nervous System

Central Nervous System: Changes in Structure
▶ ↓ Brain Weight
▶ ↓ Cerebral blood flow (20%)
▶ ↓ Number and functioning of CNS neurons
▶ ↑ Neurofibrillary tangles and senile plaques
▶ Altered neurotransmitters
Central Nervous System: Changes in FunctionCognition: maintained until at least 80 y/o
▶ Slowing in central processing → Tasks take longer to perform
Verbal skills: maintained until 70 y/o
▶ ↓ Vocabulary
▶ ↑ Semantic errors
▶ Abnormal prosody
Mentation
▶ Difficulty learning, especially languages and forgetfulness in non-critical areas
▶ Note: does NOT impair recall of important memories or affect ability to function

Peripheral Nervous System
▶ ↓ Spinal motor neurons
▶ Nerve conduction slows
▶ ↓ Vibratory sensation (esp. feet)
▶ ↓ Thermal sensitivity (warm-cool)
▶ ↓ Size of large myelinated fibers

Musculoskeletal

Musculoskeletal: Muscle
▶ ↓ Muscle fibers (type II – fast twitch) → ↓ muscle
mass (sarcopenia) → lean body mass
▶ Infiltration of fat into muscle bundles
▶ ↑ Fatigability
▶ ↓ Basal metabolic rate
– 4%/decade after 50 y/o

Musculoskeletal: Bone
▶ ↓ Bone density (both trabecular and cortical bone)
▶ ↓ Osteoclast bone formation
▶ ↓ Bone remodeling
▶ ↑ Adipocyte formation in bone marrow
▶ Slower healing of fractures
▶ ↓ Vitamin D absorption → ↓ osteoblasts → ↓ bone formation
▶ ↑ Bone loss → Loss of height and dorsal kyphosis
▶ ↓ Bone density and micro-architectural bone deterioration → Osteoporosis

Musculoskeletal: Joints
Non-articular cartilage grows throughout life
Articular cartilage does change
▶ ↓ Thickness of cartilage
▶ ↓ Chondrocytes
▶ Collagen becomes stiffer → Disordered cartilage matrix
As a result, less able to handle mechanical stress

Skin

Skin: Changes in Structure
Epidermal changes
Melanocytes▶ ↓ 15%/decade▶ Density doubles on sun-exposed skin▶ ↑ Lentigines
Langerhans cells▶ ↓ Density▶ ↓ Responsiveness
Dermal Changes▶ ↓ Collagen (1% annual decline) altered fibers▶ ↓ Density▶ Progressive loss of elastic tissue in the papillary dermis

Skin: Changes in Function
Physiologic Decrement Clinical Consequences
↓ Barrier function Dryness
Slower cell replacementRough surface Delayed healing
Ineffective DNA repair ↑ photo-carcinogenesis
↓ Elasticity Lax skin
↓ Immunologic and inflammatory responsiveness
Chronic low-grade skin infectionsInapparent injuries and infections
↓ Melanocytes at base of hair follicles Grey hair

Skin: Changes in Function
Physiologic Decrement Clinical Consequences
Mechanical protection altered↓ Sensory perception
Frequent injuries
↓ Sweating Tendency to hyperthermia
↓ Effectiveness of thermoregulation (vascular) Vulnerability to heat and cold
↓ Vitamin D production Osteomalacia
Impaired wound healing Persistent wounds, weak scars

Immune System

Immune System
Age Associated Changes Consequences
↓ Primary and secondary response
↓ Immune functioning
↑ Autoimmune antibodies ↓ Immune functioning
↓ T-cell function
↓ Naïve Cells
↑ Memory T cells
↓ Response to new pathogens
Atrophy of thymus
↓ T Cells, natural killer cells
↓ Cytokines needed for growth/maturation B cells
63
Five Senses

Sensory: Changes in Vision
Age Associated Changes Consequences
Impaired dark adaptation
↓ Pupil Diameter
↓ Contrast sensitivity
Thickening/Yellowing of lens ↓ Transparency of cornea
↑ Lens size and rigidity due to constant formation of central epithelial cells at front of lens
Inability to focus on near items (Presbyopia)
↓ Lacrimation Dry Eyes

Sensory: Changes in Smell and Thirst
Smell
Thirst
Age Associated Changes Consequences
↓ Detection by 50% ↓ Ability to enjoy food
↓ Appetite
Age Associated Changes Consequences
↓ Thirst drive
Impaired control of thirst by endorphins
↑ Risk of dehydration

Sensory: Changes in Hearing
Age Associated Changes Consequences
Thickened ear drum↑ Conductive deafness (low-frequency range)
↓ Elasticity and efficiency of ossicular articulation
↑ Sensorineural hearing loss (high frequency sounds)
Central processing deficit
Difficulty discriminating source of sound
Impaired discrimination of target from noise

Aging: A State of Chronic Exercise
deficiency?▶ Only 29% of elderly report any regular exercise
67
Physiologic
Characteristic
Aging Exercise
Fat Mass
Bone Mineral
Density
VO2 Max
Muscle Strength
Glucose Tolerance
Insulin Sensitivity
Cholesterol

Benefits of Exercise
▶ Weight Loss
– Decrease central adiposity
– Increase lean body mass▶ Blood pressure decline▶ Aerobic Capacity increase▶ Insulin Sensitivity Increase▶ Increase Bone Mass▶ Increase Muscle Strength▶ Increase perceived well being
68

Life Span Extension
▶ Caloric Restriction (CR)
– Caloric restricted diets demonstrated
• Lower temperature
• Lower insulin levels
– Studies are being conducted in monkeys and non-human primates
– Caveat: caloric restriction (>30% of calories) may be unrealistic in humans
▶ Current studies to search for CR mimics
Studies at NIA, University of Wisconsin, Baltimore Longitudinal Study on Aging

Relevance of Aging to Disability
70

References
▶ Merck Manual of Geriatrics Beers, Mark (2000)
▶ Merck Manual of Health and Aging (2004)
▶ GRS 7th edition – American Geriatrics Society
▶ Geriatric Medicine Cassel, Leipzig, Cohen, Larson,
Meier (4th edition – 2003)

Sample Board QuestionCellular senescence refers to an irreversible state of cell cycle arrest that is triggered in response to various DNA-damaging stressors (eg, telomericerosion, oxidative damage, oncogene activation). This process is believed to halt the proliferation of damaged or potentially transformed cells in the adult. As a potent tumor suppressor, cellular senescence is beneficial early in life and plays a role in tissue remodeling during embryo development. However, there is evidence that senescence may contribute to agerelated declines in tissue regenerative capacity and health, and may even fuel proliferation of premalignant cell populations during biologic aging.
Which one of the following evolutionary theories of aging is most compatible with cellular senescence?
A) Mutation accumulation theory
B) Antagonistic pleiotrophy theory
C) Disposable soma theory
D) Homeostasis theory
74

ANSWER: B) Antagonistic pleiotropy theoryThe antagonistic pleiotropy theory posits that pleiotropic genes or molecular
processes, which may benefit early fitness components in the young, may carry
harmful effects on late-life fitness. Because there is no pressure for natural selection
to favor traits for improving late-life fitness, genes with deleterious effects confined to
late life are less likely to undergo negative selection. If the deleterious aspects confer
more robust survival benefits earlier in life, then their benefits outweigh their harm.
A) Mutation accumulation posits that random, detrimental mutations accumulate over
time and manifest their effects only late in life.
C) Disposable soma theory considers aging to be a tradeoff between an organism’s
efforts to maintain nonreproductive aspects (soma) and the cost of its efforts to
reproduce. Because an organism invests resources into reproduction, over time
mutations and other cellular damage accumulate in the soma because the body
cannot repair all of it.
D) In the example above, cellular senescence is strictly beneficial toward young
organisms and has emerging negative effects on homeostasis with advancing age.
Senescent cells may contribute to homeostenosis in this case, but the process is not
itself considered to be an evolutionary theory of aging.
75

Ames and Snell dwarf mice are classic examples of mouse aging models. They possess
mutations in the Prop1 and Pit1 genes, respectively, and live much longer than their
normal siblings. The mice, which are deficient for growth hormone, prolactin, and
thyroid-stimulating hormone, also exhibit delays in many age-related phenotypes,
such as immune function and connective tissue senescence.
With the various physiologic theories of aging in mind, which one of the following
might NOT be associated with the increased longevity of these animals?
A) Decreased circulating insulin
B) Decreased metabolic rate
C) Suppression of superoxide dismutase (SOD) and catalase activity
D) Reduced plasma glucose
76
Sample Board Question

ANSWER: C) Suppression of superoxide dismutase (SOD) and catalase activityUnder the free-radical theory of aging, suppression of SOD and catalase activity would likely result in lower antioxidant production. However, in the case of the Ames and Snell mice, a loss of antioxidant activity itself would not logically be associated with increased longevity.
A and D) Data support a role for the insulin-like growth factor-1 (IGF-1)/insulin system
in the aging process in various animal models. In such models, diminished activation
of the mTOR pathway is often associated with improved insulin and IGF-1 receptor
sensitivity, thereby promoting relatively lower levels of circulating insulin and IGF-1
bioactivity. This process falls within the general context of the endocrine theory of
aging, which posits that dysregulation in hormone levels and associated signaling are a
major cause of loss of homeostasis. In the specific case of growth hormone–deficient
mice, this supports an environment of insulin decrease and reduced plasma glucose.
B) Decreased metabolic rate is correct with respect to the rate of living theory, which
predicts that lower versus higher metabolic rates favor slower rates of aging and
increased life span. 77

Antagonistic pleiotropy theory suggests that pleiotropic genes or molecular processes
that benefit fitness in the young may carry harmful effects on late-life fitness, because
there is no pressure for natural selection to favor traits that improve late-life fitness. In
other words, genes with deleterious effects confined to late life are less likely to
undergo negative selection. Cellular senescence refers to an irreversible state of cell
cycle arrest that is triggered in response to various DNA-damaging stressors.
Which one of the following findings would best support the role of cellular senescence
in tissue repair and cancer progression?
A) Secreted peptides from senescent cells trigger innate immune responses.
B) During tissue injury and repair, cellular senescence is imposed on resident
myofibroblasts.
C) Removal of senescent cells hinders wound healing response in young animals and
improves healing response in old animals.
D) Secreted peptides from senescent cells induce cell cycle arrest on neighboring cells.
E) Senescent cells accumulate throughout various organs with age.78
Sample Board Question
ANSWER: C) Removal of senescent cells hinders wound healing response in young
animals and improves healing response in old animals.
That removal of senescent cells has different effects in young and old animals supports
the premise of antagonistic pleiotropy. The presence of senescent cells appears to
confer a benefit in young animals, because removal of cells delays and worsens wound
healing, yet the presence of senescence is apparently harmful in old animals.
▶ The triggering of innate immunity by secreted peptides from senescent cells could
be “good for young, bad for old,” but there is no evidence provided in the question
to support this. Immune cell activation could represent a mechanism that
senescent cells use to encourage tissue remodeling, or, alternately, could be a
mechanism to promote their own clearance after activation of an oncogene.
▶ The imposition of cellular senescence on resident myofibroblasts during injury is
not relevant to antagonistic pleiotropy, without knowledge of differential cell
targets between young and old. Although secreted peptides from senescent cells
induce cell cycle arrest on neighboring cells, it does not necessarily follow that a
positive effect ultimately becomes negative.
79

(Cont’d)
▶ Although the age-related accumulation of senescent cells throughout various
organs might be considered to support antagonistic pleiotropy, it is a much weaker
finding than the role of senescent cells in wound healing. It is well established that
senescent cells accumulate throughout multiple organ systems during the aging
process. However, the nature of this accumulation is not fully understood. In some
cases, senescent cells may actively drive aging and age-related disease, through
effects such as reducing stem cell function and producing chronic states of
localized and systemic inflammation. This association alone is not direct evidence
that senescent cells are driving age-related disease; furthermore, it might be true
only for specific organs and tissues. In other cases, the presence of senescent cells
may represent successful imposition of the senescence function, but without
efficient elimination by immune cells. Such various scenarios would need
convincing data showing that accumulated presence alone hastens adverse tissue
function.
80