Embed Size (px)
Citation preview

Physiology
(1) 27/3/2018
Hala Nsour
This lecture topic is about kidney function, nephron, renal blood flow
(RBF), glomerular filtration (Ma fe da3e trj3/e ll slides)
The doctor started with anatomy of renal system, which we were
supposed to know from anatomy lectures.
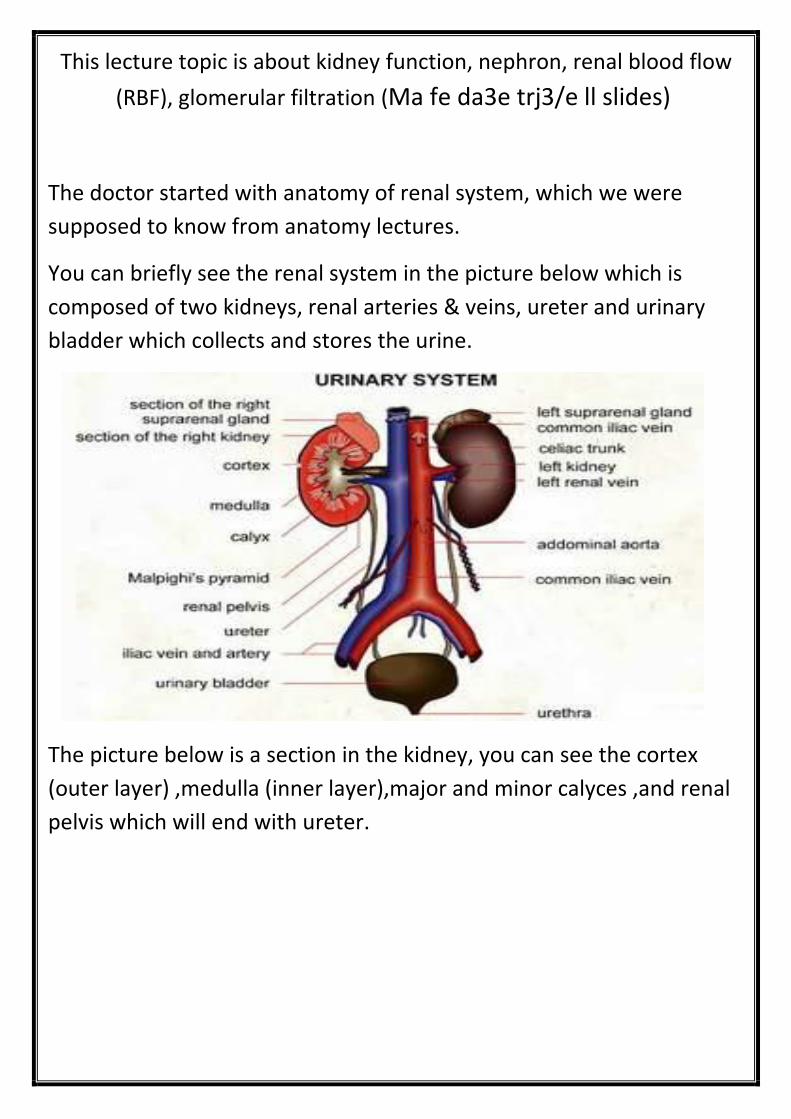
You can briefly see the renal system in the picture below which is
composed of two kidneys, renal arteries & veins, ureter and urinary
bladder which collects and stores the urine.
The picture below is a section in the kidney, you can see the cortex
(outer layer) ,medulla (inner layer),major and minor calyces ,and renal
pelvis which will end with ureter.
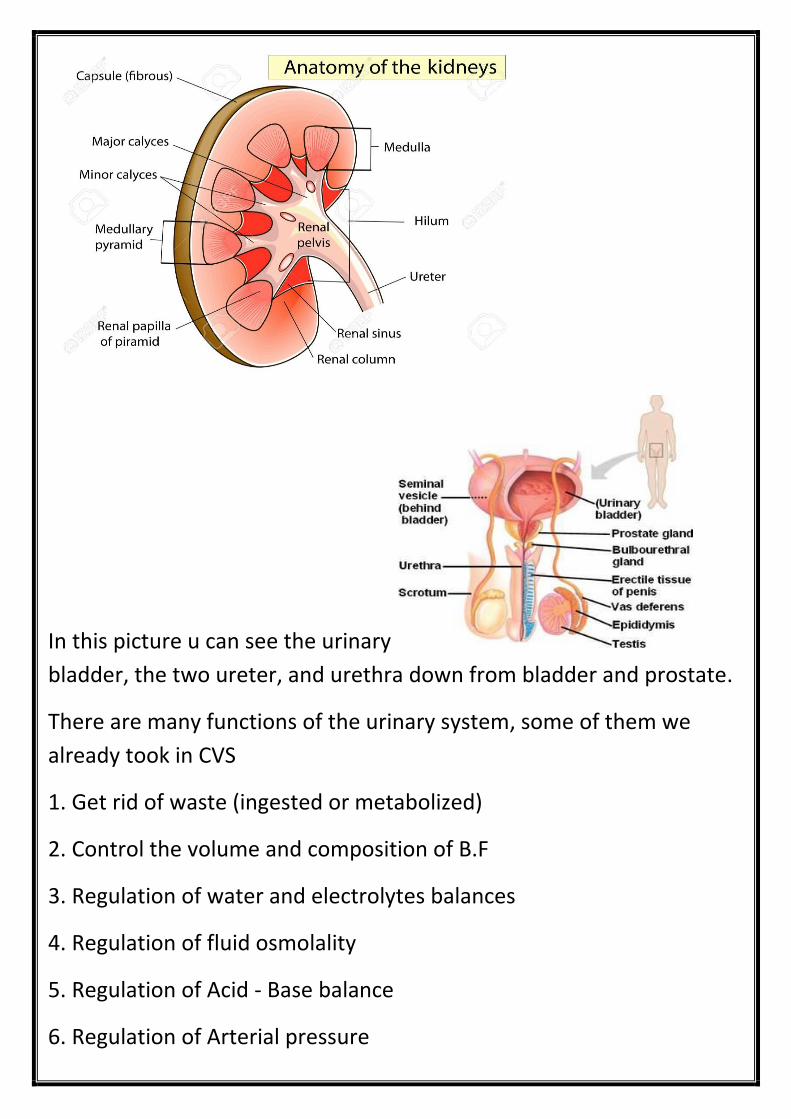
In this picture u can see the urinary
bladder, the two ureter, and urethra down from bladder and prostate.
There are many functions of the urinary system, some of them we
already took in CVS
1. Get rid of waste (ingested or metabolized)
2. Control the volume and composition of B.F
3. Regulation of water and electrolytes balances
4. Regulation of fluid osmolality
5. Regulation of Acid - Base balance
6. Regulation of Arterial pressure
7.Secretion of hormones like the angiotensin hemopoietin (also
called hematopoietin and erythropoietin )
8.Gluconeogenesis :formation of glucose particularly happen
during starvation
9. Producing erythropoietin & renin. Converting vit. D
The doctor explained some of these functions:
Water and electrolyte balance
Eating and drinking habits salts and other electrolytes might
increase 10 fold daily or decrease 1/10 fold daily slight or
modest changes in ECF volume or (Plasma Na)
Part of what we usually excrete from our body fluid volume done by
the kidney, other part is excreted by respiration, skin, vapor ….
*Anything we get during the day must be execrated at the end of the
day
*What's not completed today will be completed the next day
So there must be a balance between the input and the output, any
disturbance, this mean there is pathogenesis, there is some sort of
problem (disease)
The imbalance occurs if 1) we take too much water 2) too much
electrolytes (salts). 3) Shortage of water (starvation) and so on
Despite all this, the kidney still keep the change very minimum
(including the blood volume, extracellular volume, osmolality and
electrolytes)
Excretion of metabolic waste and foreign chemicals
1. Urea is the product from amino acids

2. Creatinine from muscles
3. Uric acid from nucleic acid
4. Bilirubin from Hb breakdown
5. Pesticides, drugs, food additives(toxic material excreted by kidney )
- Regulation of arterial pressure:
As u supposed to remember from the cardiovascular
system we have two mechanisms for regulation blood
pressure by the kidney:
1_ long term:
Excreting Na and water, and if u remember the anti-
diuretic hormones which depends on increase and
decrease of BP
*It takes hour or days
2_short term:
Renin and angiotensin, again if u remember from CVS
angiotensin take about 30 min to be fully active, that's
considered to be short term, the doctor mentioned also
with short term baroreceptors but without
explainnation so to make it easier remember
Short term…..>> regulation blood vessel diameter,
heart rate and contractility.
Long term…>> regulation of blood volume.
Short term regulation mediated by
*nervous system… (by baroreceptor) *chemicals

Regulation of acid-base balance: excreting acid or base urine
(Sulfuric & phosphoric acids)
(Hydrogen and bicarbonate)
Regulation of erythrocyte production: Secrete erythropoietin
Any patient with any renal problem (disease) mostly complain from
anemia (anemia is considered the main sign to renal diseases)
,because the kidney can't secrete erythropoietin so formation of
RBCs will be reduced and this will lead to anemia.
Regulation of 1,25 dihydroxy vitamin D3 production:
Kidneys produce active form of vit. D, by hydroxylating this vitamin
vit D is absorbed in non-active form, and the activation will be in the
kidney.
Glucose synthesis:
From amino acids and other precursors during prolonged fasting
this occur in starvation (prolonged).
**Physiological anatomy as we already mentioned:
150 2 kidneys posterior, outside peritoneal cavity. We have
, size clenched fist. gm
Outer cortex
Inner medulla: renal pyramids papilla renal pelvis major
and minor calyces ureter which ends in the urinary bladder.
(If u want go and see slides 11/12/13, it’s just a pic to kidney
and nephron u can google it)

*The function unit of the kidney is the nephron, structure of the
nephron is composed of different parts, one is the glomerulus,
as u can see in picture we have inside a network of capillary
(arterial capillary), this glomerulus has blood supply from the
renal artery which enters as afferent arteriole then a network of
capillary then leave as efferent arteriole.
Glomerulus surrounded by epithelial cells which are forming
bowman’s capsule which is the first part of renal tubule then
we have proximal tubule, loop of Henle (descending limb then
ascending one) then distal tubule which ends with collecting
tubules which later will be collecting duct & will go to pelvis
then ureter ….
We can see in the pic (slide 12/13) peritubular capillary which is
capillary surrounding the renal tubule, these capillary play a
role in the absorption or secretion.
Renal blood supply:
Renal blood flow is about 22% of C.O (cardiac output) ___ 1200
ml/min and again from anatomy :
Renal artery interlobar arteries arcuate arteries __
interlobular arteries afferent arterioles glomerular
capillaries efferent arteriolesperitubular
capillariesVenous systemInterlobular
arcuateInterlobarRenal vein

This is an actual diagram to the renal blood flow to the kidney, u can
see the cortex (red part) and medulla (pink part)
, its for nutritionis not s blood flow to the kidney purpose of the The
mainly for the regulation of the functions we mentioned before
(filtration, secretion, absorption and also controlling of osmolarity
and blood volume), but there is a very little amount for nutrition.
So regulation is the actual function of the kidney.

Nephron:
Human body have one million nephron in each kidney,
these nephrons will be decreased in function gradually
after the age of 40 years so any disease or damage
affecting the nephron is permanent, it’s not capable to
regenerate, so any problem or disease in kidneys will
make a permanent damage (not curable) and ends up
with renal failure, that’s why people with kidney
disease or diabetes end up with renal failure.
Tubular system
1.Proximal
2.loop of Henle:
a. Descending
b. Ascending (last part thick segment)
3.Distal tubule __ collecting tubule __ cortical collecting tubule
4.cortical collecting duct __ (8 to 10) ducts join to
form single large collecting duct__Medullary
collecting duct__ Renal papillae__Renal
pelvis__Ureter__Bladder (250 large coll.
Ducts/kidney
There are two sets of capillaries in the kidney:
1_ Glomerulus:
Beginning with afferent arteriole then a network of
capillary end with efferent arteriole, this type of
capillary is arterial capillary, as we know all capillaries in

the body consists of artery and vein networks but in
glomerulus of the kidney it is just arterioles.
*Pressure in this capillary is very high it’s about 60
mmhg, normal capillary pressure is about 37mmhg.
Arteriolar capillary is not involved in exchanging
process (reabsorption and secretion) they are mainly
for filtration (filtrate plasma to nephron)
2_ peritubular capillary:
This type of capillary is like other type of capillary in the
rest of the body, this type is involved in the exchange
process (reabsorption and secretion).
We have two type of nephrons (see the pic below)
1_ cortical nephron:
Which originates in the upper cortex, the end of loop of
Henle in the upper part of medulla near to the cortex so
most of it in the cortex and that’s the reason of its
name
2_ medullary nephron: (juxtamedullary)
Starts in the lower end of the cortex, go deep in
medulla even reach near the pelvic inlet, so it’s going
deeper in medulla than cortical type.
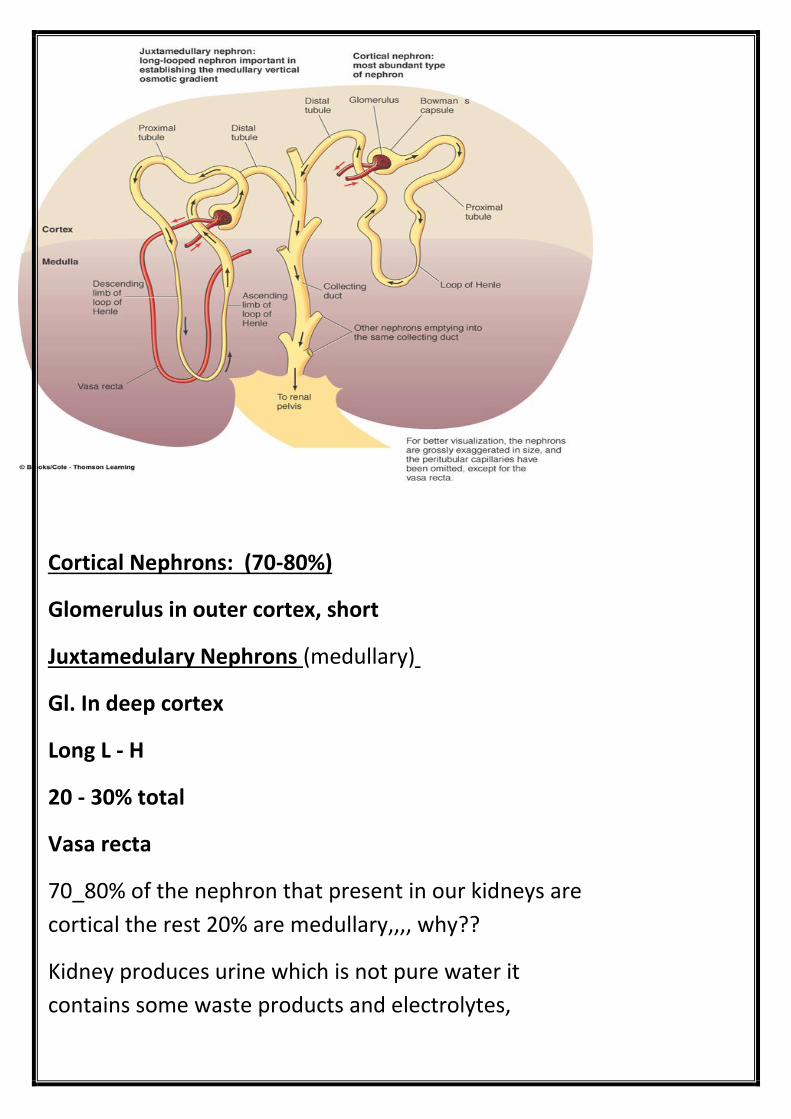
80%)-Cortical Nephrons: (70
Glomerulus in outer cortex, short
(medullary) Juxtamedulary Nephrons
Gl. In deep cortex
Long L - H
20 - 30% total
Vasa recta
70_80% of the nephron that present in our kidneys are
cortical the rest 20% are medullary,,,, why??
Kidney produces urine which is not pure water it
contains some waste products and electrolytes,

normally the kidney uses only cortical nephron, so
regulates normal day input and output
When there is a shortage of water, the osmolarity of
body fluids will be changed in this case other type of
nephrons will be involved.
So when there is a shortage of water, we need water so
anything that is filtrated, most of it must be reabsorbed
Increased absorption of water …..Increasing will get rid
of electrolytes so the kidney will form concentrated
urine.
The principle of forming concentrated urine of diluted
one is related to what we call counter balance and we
will take about it next time in details.
Kidney chooses the type of nephron according to body
needs, the principle function of medullary type is
mainly to produce concentrated urine when there is a
shortage of water.
Body needs is the actual stimulus for the regulation of
the body fluids.
Main function of the kidney is urine formation
(regulation is the upper but that's because of the end
product of kidney main function process urine)
We have four step in urine formation ..1.filtration
2.reabsorbtion 3.secretion 4. Excretion (Final step of
urine formation)

First step of formation the urine is filtration, 20% of CO
coming to kidney in the glomerulus arteriole, the
plasma will filtrate then go to Bowman’s capsule then
to renal tubule
So first thing is filtration, there must be a mechanism to
regulate this huge amount of filtration increase it or
decrease it according to body need
Filtrated fluid is same as the plasma component but
without protein (so no plasma protein present in
filtrated fluid
So what will happen to this filtration?
Normally the plasma(blood ) is re circulate to kidney
the filtrated fluid per day is about 180 liters( passing
through the kidney per day ) so you can imagine how
big it is (the doctor mean that the person cant loose
this big amount of fluid per day , we will die )so part of
this 180L which is 176.5 reabsorbed , all of them
absorbed except of 1.5 L which is the urine
So most of filtrated fluid (mainly all of it ) is reabsorbed
so if there is any imbalance between the output and
input any different of even 1 or 2 milliliter per day this
will make either edema or dehydration so this is prissy
regulated or control each day
So infiltrated fluid through the glomerulus per day
about 180 L

Other possibility that some of the waste product not
filtrated and the body don’t need them so they are
secreted from peritubular capillaries
As we mentioned above four functions (steps) in urine
formation filtration ,absorption, secretion , excretion
…but the major one is the reabsorption because most
of 180L per day is absorbed ,so the bulk is the
absorption so the mechanism of absorption is the main
function part of kidney
Urinary excretion rate (urine output)=
(filter. Rate )- (reabs. Rate )+ secr. Rate

So as we see in the picture below we have four type of
substance which run through the nephron and filtrated
(A,B,C,D)
Type (A) substance :
this represent substances that filtrated and excreted ,they are not
absorbed nor secreted , and these are mainly creatinine and
inulin(examples)
B) substance : )Type
They are filtrated but some of them are absorbed from the tubule to
the peritubuler capillaries because the body need it , so not all of the
filtrated excreted some of it absorbed , most the electrolytes belong to
this type ( Na & k for example or any useful material )
Type (C) substance :

Here what is filtrated all of it absorbed , simple example of this is
glucose
Acc to student question It is clear from the doctor answer to her that
these schemes illustrate the normal situation, but what happens in
patients is different Where we can find glucose in the urine in patients
with diabetes, which is not normal
In other word ….All of amino acids and glucose absorbed again to blood
after filtration so normally we don’t find them in urine
Type (D) substance :
here what filtrated not absorbed but secreted again ,so all of it
excreted in urine , example of this substance is hydrogen
here there is secretion from peritubular capillary add to filtrated
that’s what is called renal handling
A.Freely filtered, not reabs. , no secretion excretion rate = filtration
rate creatinine, inulin
B. Freely filtered, partialy reabs, most electrolytes
C. Freely filtered, not excreted completely reabs., a.a, glucose
D.Freely filtered, not reabs. , but secreted, H
The doctor repeated how kidney handle with substances thousands
times so I guess its very important ( for exam purposes )
Filtration, Reabs. And secretion
Reabs. > secretion : So as we say the major function is for the
reabsorption
Secretion determines K+ and H+ Concentration
But the secretion depend on the body need, if the body need sodium
for example keep it, not need it so secrete it and so on
IF the …Volume of plasma is only 3 L, and the filtration rate is 180, so
the doctor ask how many times this 3 L filtrate in the kidney??
60 time per day the plasma perfuse or filtrate in the kidney
So you can imagine why there is huge GFR
1_Most waste product removed rapidly (effective)
2_Allow all body fluids to be filtered and processed by kidneys
many times each day (precise & rapid control of volume &
composition
So again as we said the main blood supply to the kidney not for
nutrient, less than 1% for nutrition, main (all) blood supply is for
regulation of actual function……..
This is everything for today,,,,,,
I hope it’s clear, and sorry in advance of any mistakes ……..
Best wishes





























