Embed Size (px)
Citation preview

Pilbara Health Profile
Planning and Evaluation Unit
September 2015

Pilbara Health Profile 2015
i ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Prepared by Stella Serafino, Campbell Anderson and Nina Waenerberg
Acknowledgements Thanks are extended to our colleagues and specialists in the field who reviewed and commented on the report.

Pilbara Health Profile 2015
1 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Contents Summary ........................................... .................................................................................. 3
Introduction ...................................... .................................................................................. 6
Overview of the region ............................ .......................................................................... 7
Level of remoteness ......................................................................................................... 7
Population ........................................ .................................................................................. 8
Economic, demographic and social factors .......... ........................................................ 12
Socio-Economic Disadvantage ....................................................................................... 12
Private Health Coverage ................................................................................................ 13
Maternal Health Status ............................ ........................................................................ 14
Births .............................................................................................................................. 14
Teenage mothers ........................................................................................................... 14
Smoking in pregnancy .................................................................................................... 15
Alcohol in pregnancy ...................................................................................................... 15
Gestational Diabetes Mellitus ......................................................................................... 16
Health Status - Child and Adolescent .............. .............................................................. 17
Low birth weight ............................................................................................................. 17
Australian Early Childhood Development Census .......................................................... 17
Childhood Vaccinations .................................................................................................. 18
Health and Wellbeing Surveillance System, 0-15 years ................................................. 20
Potentially Preventable Hospitalisations, 0-14 years ...................................................... 22
Injuries, 0-14 years ......................................................................................................... 25
Notifiable Infections, 0-14 years ..................................................................................... 26
Health of Adults .................................. ............................................................................. 27
Self-reported risk factors, 16 years and over .................................................................. 27
Self-reported chronic conditions, 16 years and over....................................................... 28
Self-reported service utilisation, 16 years and over ........................................................ 29
Hospitalisations, 15-64 years ......................................................................................... 31
Alcohol and tobacco related hospitalisations, 15-64 years ............................................. 32
Potentially preventable hospitalisations, 15-64 years ..................................................... 33
Notifiable Infections and Events, 15-64 years ................................................................ 36
Vaccine-preventable diseases, 15-64 years ............................................................... 36
Vector-borne diseases, 15-64 years ........................................................................... 37
Sexually Transmitted Infections, all ages .................................................................... 38
Cancer Incidence, 15-64 years ....................................................................................... 40
Mental Health, 15-64 years ............................................................................................ 41

Pilbara Health Profile 2015
2 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Youth Suicide, 15-24 years ......................................................................................... 41
Mental Health, 16 years and over ............................................................................... 41
Community Mental Health Activity, 15-64 years ......................................................... 41
Mortality, 15-64 years ..................................................................................................... 42
Alcohol and tobacco related mortality, 15-64 years ........................................................ 42
Avoidable Mortality, 15-64 years .................................................................................... 42
Health Status of Older People ..................... .................................................................... 43
Vaccinations, 65 years and over .................................................................................... 43
Hospitalisations, 65 years and over ................................................................................ 43
Potentially Preventable Hospitalisations, 65 years and over .......................................... 44
Mental Health, older people ............................................................................................ 46
Community Mental Health Activity, 65 years and over ................................................ 46
Disability and Carers ............................. .......................................................................... 47
Where Pilbara Residents Accessed Care ............. ......................................................... 47
General Practice ............................................................................................................. 47
Emergency Department Attendances ............................................................................. 48
Hospitalisations .............................................................................................................. 50
Alcohol and tobacco related hospitalisations .............................................................. 51
Potentially preventable hospitalisations ...................................................................... 51
Where Pilbara residents used hospital services ............................................................. 53
Hospitalisations within the region ................................................................................... 54
Mortality ......................................... ................................................................................... 54
Alcohol and tobacco related mortality ............................................................................. 56
Avoidable Mortality, 0-74 years ...................................................................................... 57
Glossary .......................................... .................................................................................. 59
References ........................................ ................................................................................ 61
NOTE:
Unless otherwise stated within this document the term rate refers to an age standardised rate. This means that the differing age and sex structures of the populations have been taken into account enabling two different areas or time periods to be compared.
© Department of Health 201
This document can be made available in alternative formats on request for a person with a disability.

Pilbara Health Profile 2015
3 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Summary This report presents an overview of the health of Pilbara residents to support evidence-based health services. The following areas are recommended for consideration in the planning of primary health services within the Pilbara region.
Population
• The Pilbara region had an Estimated Resident Population (ERP) of 66,298 in 2013. Over the previous five years, the region had an influx of predominantly middle aged males working in mining and construction, plus FIFO workers.
• Based on ABS series B projections (The WA State Government Population Projections), the region’s resident population is projected to taper with only 0.6% per annum between 2014 and 2026.
• The region’s Aboriginal population was 16% in 2011 and has a younger age structure than the non-Aboriginal population.
Economic, demographic and social factors
Based on the 2011 census, the Pilbara region has: • some areas with very low SEIFA (Socio-Economic Indexes for Areas) scores, • less people at school and in tertiary education than other regions, • more people with tertiary qualifications compared with other regions of the State.
Maternal Health
• In 2012, five per cent of births were to Pilbara women aged less than 20 years. This was similar to the State rate. The proportion of births to Aboriginal teenage women in the Pilbara was 21%.
• In 2013, 56% of Aboriginal and 10% of non-Aboriginal women from the Pilbara who gave birth reported smoking during pregnancy. The reported Aboriginal rate increased significantly from 2011.
Child and Adolescent
• In 2012, the proportion of Pilbara children rated as developmentally vulnerable on one or more domains ranged from 5.9% in Paraburdoo to 47% in East Pilbara and remote communities. Five of the 12 communities with valid data had a higher rate of vulnerability than the national average (22%).
• Rates of hearing loss and Otitis Media are higher in Aboriginal children. For 2003-2012, the rate of disease of the ear and mastoid process hospitalisations for Aboriginal children in the Pilbara was one and a half times higher (918 per 100,000) than the non-Aboriginal rate (604 per 100,000).
• For 2008-2013, over half of Pilbara children did not eat the recommended serves of vegetables or do sufficient physical activity while one in five was classified as overweight.
• One in five children reported an injury requiring treatment in the previous year and seven per cent reported having asthma.
• These risk factor and National Health Priority Area proportions were similar to the State.

Pilbara Health Profile 2015
4 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
• The rate of potentially preventable hospitalisations in Pilbara children was significantly (1.2 times) higher compared to children in the State. ‘Dental conditions’, ENT infections and asthma contributed over 70% of potentially preventable hospitalisations.
• For 2008-2012, injury and poisoning hospitalisation rate was significantly (1.3 times) higher compared to children in the State. Leading causes were accidental falls, mechanical forces and transport accidents, together contributing 70% of injury and poisoning hospitalisations and 14% of all hospitalisations in children in the Pilbara.
Adult
• For 2009-2012, Pilbara adults were more likely than the State to report smoking, insufficient fruit intake, drinking at risk of harm and obesity, (behaviours linked with several chronic conditions).
• For 2008-2012, the main cause of hospitalisation for adults aged 15-64 years was renal dialysis (24% of hospitalisations in this age group). The next leading cause was delivery (3% of hospitalisations).
• The rates for alcohol and tobacco-related hospitalisations were significantly higher (1.4 and 1.3 times respectively) than the State rates. For 2003-2012, Pilbara Aboriginal adult rates were significantly higher (9 and 5 times respectively) than non-Aboriginal adult rates.
• For 2008-2012, the potentially preventable hospitalisation (PPH) rate was significantly higher (1.4 times) than the State rate.
• The leading PPH for Pilbara adults was ‘diabetes complications’ (24% of PPH in this age group).
Notifiable Diseases
• For 2007-2011, the notification rate for notifiable diseases for adults aged 15-64 years was significantly higher (1.6 times) in the Pilbara compared with the State.
• The sexually transmitted infection (STI) notification rate (mainly chlamydia and gonorrhoea) was significantly higher (1.9 times), vaccine preventable (mainly influenza and pertussis) was significantly higher (1.3 times) and vector-borne (mainly ross river virus) was significantly higher (1.9 times) than the State rates.
Mental Health
• Females had a higher prevalence of reporting a current mental health problem compared with males (2009-2012), however males had a higher suicide rate than females (2002-2011).
• The leading reason for an occasion of service was serious psychiatric disorders followed by anxiety disorders.
Older People
• For 2008-2012, the leading cause of hospitalisation in older age groups was renal dialysis which was significantly higher (3.7 times) than the State rate.
• The rate of hospitalisation for influenza/pneumonia was significantly higher (3 times) than the State rate.
• The leading PPH was chronic obstructive pulmonary disease (COPD) and the rate was significantly higher (3.8 times) than the State rate.

Pilbara Health Profile 2015
5 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Emergency Departments
• In 2013/14, 74% of attendances to hospitals within the Pilbara were for semi-urgent or non-urgent cases. This was significantly higher than WACHS (66%).
• Around one fifth of patients (22%) were not residents of the Pilbara region.
Hospitalisations
• For 2008-2012, the hospitalisation rate of Pilbara residents was significantly higher (1.03 times) than the State rate.
• For non-Aboriginal Pilbara residents, the leading causes of PPH were dental conditions, diabetes complications, ENT infections and asthma. The asthma PPH rate was significantly higher (1.2 times) than the State non-Aboriginal rate. For Aboriginal Pilbara residents, the leading causes of PPH were diabetes complications, convulsions/epilepsy, COPD and pyelonephritis. Most of these conditions were significantly higher than the State except for convulsions/epilepsy.
• In 2013/14, 78% of Pilbara residents’ hospitalisations to public hospitals occurred within the region. The WACHS average was 75%.
Mortality
• For 2007-2011, the mortality rate of the Pilbara region was significantly higher (1.1 times) than the State rate.
• Just over half of deaths of Pilbara residents under the age of 75 could have potentially been avoided.
• Pilbara Aboriginal people had avoidable death rates that were significantly higher (around 6 times) than non-Aboriginal people, including alcohol and tobacco-related deaths (3-4 times higher).
• The leading causes of avoidable death were ischaemic heart disease, diabetes, lung cancer, alcohol-related conditions and nephritis/nephrosis.

Pilbara Health Profile 2015
6 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Introduction This profile includes regional information on the population, demographics, determinants of health and health statistics such as immunisation rates, mortality and hospitalisation rates for residents of the Pilbara. Where practicable the information is provided in the sequence of the continuity of care, and is provided by age group.
The information can be used to support business cases and to focus services where they can best affect a positive outcome. These regional profiles have been endorsed for public viewing and can be utilised by WACHS staff and key regional stakeholders to inform planning and service development.
Additional information about the region and districts within the region may be found in service plan documents also published on the WACHS Publications page: www.wacountry.health.wa.gov.au. Aboriginal Health Profiles for each region were also produced in 2012 by Aboriginal Health Improvement Unit, WACHS.
We
lln
ess
to
Ill
ne
ss
Public &
Population Health
Services
Mental
Health &
Alcohol &
Drug
Services
Emergency
& Acute
Inpatient &
Clinical
Support Ambulatory
Care Aged Care, Sub-Acute,
Rehabilitation
Health
Maintenance
Hospital Community & Primary Care Centre Community & Health Facility
CONTINUUM OF HEALTH CARE & SERVICES

Pilbara Health Profile 2015
7 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
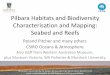
Overview of the region The Pilbara covers 507,896 km² (including offshore islands) and is Western Australia's second most northern health region, with the Indian Ocean to the west and Northern Territory to the east. The region incorporates two Health Districts – West and East Pilbara, with the vast proportion of the population residing in the west (Figure 1). The main population centres of the Pilbara are Port Hedland, Karratha and Newman. During the 1960's approval was given for iron ore deposits to be extracted from the Pilbara, putting the region on the world map. Today, the Pilbara provides Western Australia with its two largest export revenue earners, iron ore and liquefied gasi.
Level of remoteness The Accessibility/Remoteness Index of Australia (ARIA) is a systematic approach by the ABS to classify areas of Australia according to level of remoteness. Within this classification system there are five categories ranging from Major Cities to Very Remote. According to ARIA, most (99.9%) of the Pilbara health region is classified as very remote and the remaining 0.1% is classified as remote. This remote area includes parts of Port Hedland and Roebourneii.
Figure 1: Map of Pilbara showing Health Districts, and relative remoteness
Source: DoH, Epidemiology GIS branch 2015
iii

Pilbara Health Profile 2015
8 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Population
The 2013 Estimated Residential Populationiv (ERP) of the Pilbara is 66,298 which represents 12% of the WACHS population and 2.6% of the State's population. This is an increase of 6.0% (22,209) since 2006.
The Pilbara health region population density is 0.13 people per sq km which is lower than State average (1.0 per sq km; Country: 0.24 per sq km)v.
There is a higher proportion of males (63%) than females in the Pilbara health regioniv.
Pilbara has a younger population compared to other regions. The age structure differs from that of the State by having a smaller percentage of children aged 10-19 years and adults aged 55 years and over and higher proportion of people aged between 20 and 54 years (Figure 2)iv. The reason for this would be the influx of predominately male 20-44 year olds required to work in the mining and construction industries. As well as the resident population, Pilbara has a high number of ‘fly in fly out’ (FIFO) workers. These workers also cause demand for Pilbara health services. The proportion of the population aged 65 years and over is 2% (State 12%)iv. Figure 2: Pilbara Population, Age Distribution, 201 3
0%
2%
4%
6%
8%
10%
12%
14%
16%
Age group
Pilbara population State population
Source: ABS, ERP 2013
iv
Table 1: Pilbara, Estimated Resident Population, 20 13
Age Group 0-14 15-44 45-69 70-84 85+ Grand Total
Number 11,710 37,619 16,279 601 89 66,298
Proportion 18% 57% 25% 1% 0% 100%
Source: ABS, ERP 2013iv

Pilbara Health Profile 2015
9 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Aboriginal people accounted for 16% of the region's population which was greater than the State average (3.8%) based on 2011 ERP. The Aboriginal population has a younger age structure than the non-Aboriginal population (Figure 3)vi.
Figure 3: Pilbara 2011 Estimated Resident Populatio n by Aboriginality
0% 5% 10% 15% 20% 25%
0-9 yrs
10-19 yrs
20-29 yrs
30-39 yrs
40-49 yrs
50-59 yrs
60-69 yrs
70-79 yrs
80 yrs +
Female
0%5%10%15%20%25%
Male
Non Aboriginal Aboriginal
Source: ABS via DoH Rates Calculatorvi
The Pilbara population has undergone rapid growth (6% per year) from 2006 to 2013 after being somewhat stable over the previous five years. From 2014, growth is expected to taper with only 0.6% per annum projected until 2026. The East Pilbara district is projected to increase by 1.3% per annum, but the West Pilbara district is predicted to stabiliseiv.
As can be seen in Figure 4, the ERP for 2013 is more than the 2013 projection. West Pilbara had a larger difference between ERP 2013 and projected 2013 than East Pilbaraiv,vii. Local observations estimated the population has actually dropped during 2014 due to the decreased iron ore price and the completion of the construction phase of some mining projects. The endorsed population projections do not reflect these recent movements. Table 2 shows the projections and any changes from 2014.
The proportion of the younger age groups (15-44 years) in the Pilbara region is projected to decrease while the proportion of other age groups is projected to increase (Figure 5).
Implications for health care service planning:
Pilbara has a high proportion of Aboriginal people. The Aboriginal population of the Pilbara has a much younger age structure than the non-Aboriginal population, with 39% of the population aged under 20 years (compared with 21% for non-Aboriginal). This differing age structure will need to be taken into account in the planning of primary health services and programs.

Pilbara Health Profile 2015
10 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Figure 4: Pilbara population projections
40,000
45,000
50,000
55,000
60,000
65,000
70,000
Pe
rso
ns
ABS series B Projections with WASGPP
Pilbara
ABS B projected
Historic est Pop
Notes:
Limitation of the population projections at LGA level. The endorsed population projections are based at the LGA level from the 2011 ABS census with low migration model. The data for WA is provided as Perth and "rest of WA". The population for each LGA is worked out as a proportion of the total. This proportion is then used to calculate the projection for each LGA over the ensuing years. A variance in any age group in a LGA will not be accounted for. If there is a variance in one LGA in a region which is different to the rest of the LGAs in the region, (i.e. its population changes at a different rate to the others) it will not be picked up in the projection data. Where the 2012 ERP differs from the 2012 projection, and /or the slope of the projection differs from the slope of the historic data, please view the projections with caution.
Limitation of the probable decline in population in the Pilbara: the changes in the last two years (20 14, 2015) haven’t been factored in and therefore these projections must be viewed with caution.
Source: Australian Bureau of Statistics Cat. No. 3222.0 - Population Projections, Australia, 2012 (base) to 2101, November 2013vii
modified using WA Tomorrow band proportions; Presented to WA Health Framework Development & Implementation Steering Committee for endorsement 10 December 2013
Figure 5: Pilbara population projections by age gro up
11,07511,858 11,710
13,902 14,516 15,965
22,70835,125 37,619 31,614 31,108 31,669
9,772 15,127 16,279 15,648 16,520 17,043
470 563 601 1,125 1,485 1,778
6463 89 191 221 266
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2006
ERP
2011
ERP
2013
ERP
2016
Projected
2021
Projected
2026
Projected
Pro
po
rtio
n o
f P
op
ula
tio
n
ABS series B Projections with WASGPP
Age Group, Pilbara Health Region
85+
70-84
45-69
15-44
0-14
WASGPP – WA State Government Population Projections

Pilbara Health Profile 2015
11 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Table 2: Population Projections, Pilbara
Pilbara health region 2014 2021 2026
WASG Population Projection 62,115 63,850 66,720
Population increase 1,735 4,605
Percentage increase 2.8% 7.4%
Average annual increase 0.4% 0.6%
East Pilbara health district
WASG Population Projection 29,038 31,598 33,805
Population increase 2,560 4,767
Percentage increase 8.8% 16.4%
Average annual increase 1.2% 1.3%
West Pilbara health district
WASG Population Projection 33,077 32,252 32,915
Population increase -825 -162
Percentage increase -2.5% -0.5%
Average annual increase -0.4% 0.0% Note: Limitation of the population projections at LGA level, same as listed under Figure 4.
Source: Australian Bureau of Statistics Cat. No. 3222.0 - Population Projections, Australia, 2012 (base) to 2101, November 2013vii
modified using WA Tomorrow band proportions; Presented to WA Health Framework Development & Implementation Steering Committee for endorsement 10 December 2013.
Implications for health care service planning: The overall population of the Pilbara is projected to grow, mainly in East Pilbara but this is dependent on fluctuations in the mining industry, as the population in younger age groups is projected to decrease. The number of people 65 years and over is projected to increase by 61% between 2014 and 2026 (2,179 to 3,505). This changing age structure needs to be taken into account in the commencement and placement of services particularly in Aged Care.

Pilbara Health Profile 2015
12 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Economic, demographic and social factors There are many factors that influence a person’s health, including genetics, lifestyle and environmental, economic and social factorsviii. The demographics within the Pilbara are very diverse. While long travel distances are a common issue, remote communities can differ in function and infrastructure for example a coastal fishing port and harbour will differ from a mining town or a desert Aboriginal community. The level of isolation and impact on health by environmental conditions is often more marked for remote communities than those seen in rural and metropolitan communitiesv.
Table 3 lists some of the socio-demographic factors for Pilbara compared to the rest of the State.
Table 3: Socio Demographic factors, 2011
Measure Metro Country State
Counts % % % %
Born overseas 11,661 19.5 34.9 18.8 30.7
People who don't speak English at home 6,572 11 17.1 7.1 14.5
At primary school 4,491 7.5 8.2 9.2 8.4
At secondary school 1,676 2.8 5.7 5.1 5.5
At TAFE, CAE or Uni 1,836 3.1 7.3 3.5 6.3
Left school aged less than 15 years old 2,896 6 8.1 10.6 8.7
Persons with tertiary qualification 20,158 41.7 45.3 38.3 43.6
Families with annual income < $20,800 298 3 3.9 5.1 4.2
One-parent families 1,040 10.4 14.7 14.1 14.5
Unemployed 839 2.5 4.8 4.4 4.7
Pilbara Health Region
Source: ABS Census 2011 results via DoH, Health Tracksv
Socio-Economic Disadvantage Socio-Economic Indexes for Areas (SEIFA) Index of Relative Socio-Economic Disadvantage scores are calculated from responses to the ABS Census. The more disadvantaged an area, the higher self-reported ill health or risk factors for ill healthix. A score below 1000 indicates an area is relatively disadvantaged.
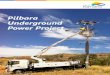
Based on the 2011 Census, the lowest score for a Pilbara LGA is 962 in East Pilbara and the highest is Roebourne with 1,060. However, there is a Statistical Area Level 1 (SA1) within Roebourne with a score of 1,136 and another SA1 within East Pilbara with a score of 496. These East Pilbara residents (around 12,000 people) have scores in the lowest 30% of scores in the State. An indication of the distribution can be seen in the map below (most disadvantaged areas are shown in darkest orange)x.

Pilbara Health Profile 2015
13 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Figure 6: Pilbara SEIFA distribution
Source: DoH, Epidemiology GIS branch, 2015
iii
Note: SEIFA 2011 is released according to the Australian Statistical Geography Standard (ASGS). The ASGS is the new geographical standard developed by the ABS for the collection and dissemination of geographic statistics. It is a hierarchically structured classification with a number of spatial units to satisfy different statistical purposes. The areas used for the Census include Statistical Area Level 1 (SA1) which is the second smallest geographic area defined in the ASGS
xi.
Private Health Coverage An impact of low private health coverage can be related to a low SEIFA Index of Relative Socio-Economic Disadvantage. In 2007-08, around three in ten people, 15 years and over, were covered by private health insurance in Port Hedland and two in five in Roebourne as well, while in Ashburton and East Pilbara there was minimal coverage.
Across Western Australia, one in every two people were covered by private health insurance and less than two in five were covered in country areas of the Statexii.
Implications for health care service planning:
The SEIFA Index of Relative Socio-Economic Disadvantage shows that there are areas within Pilbara with high levels of disadvantage. Services and programs may need to be targeted to these disadvantaged areas, such as in the remote Aboriginal communities of East Pilbara.

Pilbara Health Profile 2015
14 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Maternal Health Status Births Within the Pilbara, there was a 17 per cent increase in births of between 2009/10 and 2013/14, an average annual increase of 4.1 per cent. Non-Aboriginal women had an annual average increase of 5.8 per cent. Aboriginal women in the Pilbara had an annual average decrease of 1.3 per cent (Table 4)xiii.
Table 4: Births by Aboriginal status of mother, Pil bara, 2009/10 to 2013/14
Aboriginal Non-Aboriginal Total
2009/10 155 370 525
2010/11 161 394 555
2011/12 157 448 605
2012/13 145 452 597
2013/14 153 463 616
Increase -1.3% 25% 17%
Average annual increase -0.3% 5.8% 4.1%
Source: WACHS Online data – Obstetric Deliveriesxiii
In 2012, the overall Pilbara age-specific birth rate was 66 per 1000 women which was similar to the State rate (Table 5). For 2008-2012, the age-specific birth rate for Aboriginal women in the Pilbara was 80 per 1,000 women which was significantly higher (1.3 times) than the non-Aboriginal rate (63 per 1,000 women)v.
Table 5: Maternity data, 2012
Maternity dataPilbara Health
RegionMetro State
Age-specific birth rate (per 1,000 women aged 15-44 years, not having had Hysterectomy) 66.3 64.6 66.4
Teenage births (%) 5% 3% 4%
Births in women aged 35 years and older (%) 16% 22% 21% Source: DoH, Health Tracks
v
Teenage mothers In the Pilbara, the proportion of births to women aged less than 20 years was not significantly different from the State figure (Table 5). Between 2007 and 2012, teenage pregnancy has not changed significantly in the Pilbarav.
In 2012, in the Pilbara, the mean maternal age was 24.1 years for Aboriginal women and 29.8 years for non-Aboriginal womenxiv.
The proportion of births to Aboriginal teenage women in the Pilbara was significantly higher (21%) than non-Aboriginal teenage women (2%)xiv.

Pilbara Health Profile 2015
15 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Smoking in pregnancy Smoking during pregnancy is associated with low birth weight, pre-term birth, placental complications and perinatal mortalityxv.
In the Pilbara, the proportion of births to women smoking during pregnancy increased significantly for Aboriginal women in 2013 compared to 2011 while for non-Aboriginal mothers, there was no change. In 2013, the proportion of births to mothers who reported smoking during pregnancy was 56 per cent for Aboriginal mothers and 10 per cent for non-Aboriginal mothers (Figure 7). The WACHS rate for births to Aboriginal mothers was 51 per cent and for births to non-Aboriginal mothers was 14 per centxiv.
Figure 7: Proportion of women smoking during pregna ncy, Pilbara residents, 2011 to 2013
0%
10%
20%
30%
40%
50%
60%
70%
2011 2012 2013
Smoking in Pregnancy
Aboriginal Non-Aboriginal
Notes: The error bars represent the 95% confidence interval of the proportion; 2013 is preliminary data
Source: Midwives Notification Systemxiv
Alcohol in pregnancy Alcohol consumption while pregnant is associated with Fetal Alcohol Spectrum Disorder (FASD) and various other adverse outcomesxv.
A recent report using data from 1980-2010 obtained from the WA Register of Developmental Anomalies and the Midwives Notification System, showed a birth prevalence of FASD in WA of 0.26 per 1000 births. The majority were Aboriginal children (89%). The rate of 4.08 per 1000 for Aboriginal children was significantly higher than non-Aboriginal children (0.03 per 1000). The prevalence rate has doubled over the last 30 years in WAxvi. There have been few studies conducted recently on the consumption of alcohol during pregnancy. A recent ABS study showed that 71 per cent of Indigenous women drink and 77 per cent of non-Indigenous women drink. However, 28.4 per cent Indigenous women of child bearing age (18-44 years) and 42 per cent of non-Indigenous women of child bearing age drink at low risk levels. Also, 11.6 per cent of Indigenous women of child bearing age and 9.5 per cent of non-Indigenous women of child bearing age drink at risky/high risk levelsxvii. The WA Aboriginal Child Health Survey conducted from 2001 to 2002, reported mothers drank alcohol during pregnancy in one in five Aboriginal children in the Western Desert (Warburton) Aboriginal and Torres Strait Islander Commission (ATSIC) region (22%). (The Western Desert

Pilbara Health Profile 2015
16 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
ATSIC Region extends from Nullagine in the north to Coonana in the south with Tjukurla at the most eastern point)xviii. Although there is no direct percentage of women drinking in the Pilbara, given the higher rate of maternal age drinking in Aboriginal women and the high proportion of Aboriginal people in the Pilbara, it could be assumed that Pilbara children are more likely to be at risk of FASD. A recent study on alcohol consumption during pregnancy showed a steady and statistically significant decline in the proportion of Australian women who reported drinking alcohol during pregnancy; 53 per cent reported alcohol use in 2007 compared with 35 per cent in 2011 (Cameron 2013)xix. A number of projects are being conducted across the State to address alcohol use during pregnancy and to find out more about FASD. Details can be obtained from the Australian Aboriginal HealthInfoNet websitexvii.
Gestational Diabetes Mellitus In 2010, AIHW released a report on diabetes in pregnancy discussing its impact on Australian woman and their babies. The report concluded that mothers with diabetes in pregnancy and their babies, were at higher risk of adverse effects of pregnancy, labour and delivery, compared with those not affected by diabetes in pregnancy. Those with pre-existing diabetes who had diabetes in pregnancy, and their babies were at higher risk of developing these adverse effects.
Indigenous mothers and their babies, experienced generally higher rates of the adverse effects of pregnancy, labour and delivery compared with non-Indigenous mothers and their babies. The report also stated that diabetes in pregnancy is an indicator of increased risk of developing Type 2 diabetes later in life.
For 2005-2007, 5.1 per cent of Aboriginal Australian women who gave birth had gestational diabetes mellitus (GDM). The rate of GDM for non-Indigenous Australian women who gave birth was significantly lower at 4.7 per cent xx.
In 2012, another AIHW report on mothers and babies found the rate of women in Western Australia with GDM to be 7.0 per cent of women who gave birth. Other States were between 6.3 and 7.4 per cent xxi.
Implications for primary health care service planni ng: In the Pilbara, Aboriginal women are more likely than non-Aboriginal women to be teenage mothers, to smoke during pregnancy and to have a low birth weight baby suggesting the need for targeted and culturally appropriate health promotion strategies and antenatal services for these women. Alcohol consumption and diabetes in pregnancy are risk factors for all women. Strengthening partnerships with primary care providers, including local GPs and Aboriginal Medical Services is particularly important, given the reasonably high Aboriginal population.
Resources to tackle Aboriginal maternal smoking in WA have been developed such as the Australian Indigenous HealthInfoNet new portal launched recently (Source: Australian Indigenous HealthInfoNet accessed June 2015: http://www.healthinfonet.ecu.edu.au/about/news/3305
http://www.healthinfonet.ecu.edu.au/population-groups/preventing-aboriginal-maternal-smoking).

Pilbara Health Profile 2015
17 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Health Status - Child and Adolescent
Low birth weight Babies born with a low birth weight (less than 2,500g) have a higher risk of health complications. For 2008-2012, the low birth weight rates for Pilbara and State babies were 6 per cent each. The low birth weight rate for Pilbara Aboriginal babies was 12% while the State Aboriginal rate was 14 per cent v.
Australian Early Childhood Development Census The Australian Early Development Census (AEDC) measures how young children are developing when they first enter full time school. A teacher completes a checklist for each child and the scores of all children across Australia are ranked in each of the five areas (domains) of early childhood development. Children ranked in the bottom 10 per cent are classed as “developmentally vulnerable”; those in the top 75 per cent are classed as “on track” and those in between are classed as “at risk”. Results are reported by child’s community of residence.
Across Australia in 2012, one in five children (22%) was developmentally vulnerable on one or more domains of the AEDC. Furthermore, 11 per cent were developmentally vulnerable on two or more domains. The results for the Pilbara local communities are shown below in Table 6.
Around 15 local communities had too few children to publish results but of the 12 for which data have been published, five had a higher proportion vulnerable on one or more domains than the overall Australian proportion. The total published number of children vulnerable in at least one domain was 156 and there would also be additional vulnerable children who were in communities with numbers too low to publish.
Within the Pilbara Communities, the proportion of children rated as developmentally vulnerable varies considerably, and while the percentages may be high within a community, it is also important to consider the numbers of children the percentage represents. The proportion of children rated as developmentally vulnerable on one or more domains ranged from 5.9 per cent (two children) in Paraburdoo to 47 per cent (eight children) in East Pilbara and remote communities. The proportion rated vulnerable on two or more domains ranged from 2.4 per cent (two children) in Newman to 35 per cent (six children) in East Pilbara and remotexxii.

Pilbara Health Profile 2015
18 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Table 6: 2012 AEDC, Pilbara children vulnerable on at least one domain
Local Community Children vulnerable Total children surveyed One or more
domains Two or more
domains
Number % Number % Bulgarra 8 20% 2 4.9% 41 East Pilbara and remote communities 8 47% 6 35% 17 Karratha/Dampier 6 27% 3 14% 22 Newman 9 11% 2 2.4% 84 Nickol/Baynton/Millars Well 45 26% 19 11% 174 Paraburdoo 2 5.9% 1 2.9% 34 Pegs Creek/Stove Hill 12 17% 5 7.2% 69 Port Hedland 15 20% 6 7.8% 77 Roebourne 6 38% 4 25% 16 South Hedland 34 26% 16 12% 133 Tom Price 6 7.3% 3 3.7% 82 Wickham/Point Samson/Cossack 5 16% 2 6.5% 31 Australia 22% 11% Source: AEDC
xxii
Note: Other communities had numbers of children too small to be published. These tables and more information may be found at http://www.aedc.gov.au/
Childhood Vaccinations Immunisation against communicable disease is an effective public health intervention that reduces the mortality and morbidity associated with vaccine preventable conditions. Australian vaccination coverage targets of greater than 90 per cent of children at two years of age and near 100 per cent of children at school entry age are recommended. The coverage needs to exceed 90 per cent to create the community immunity necessary to stop the ongoing transmission of these diseasesxxiii.
In 2014, the childhood vaccination coverage for Pilbara was above 90 per cent for all age groups (Table 7a)xxiv. The overall WACHS coverage was also above 90 per cent for all age groups. The State coverage however, was over 90 per cent for ‘12-<15 months’ only (Table 7b)xxv.
Pilbara Aboriginal immunisation coverage for ‘12-<15 months’ was significantly lower than non-Aboriginal people. For the other age groups, Pilbara Aboriginal people had similar coverage to non-Aboriginal people (Table 7a)xxiv.
Implications for primary health care service planni ng: The AEDC results indicate the need for child development services including access to multidisciplinary teams made up of medical services, child health nurses, speech pathology, physiotherapy and occupational therapy, particularly in the East Pilbara and remote communities and pockets of Roebourne.

Pilbara Health Profile 2015
19 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
For WACHS overall, Aboriginal people had significantly lower coverage than non-Aboriginal people for ‘12-<15 months’ but similar coverage for ’24-<27 months’ and significantly higher coverage for ‘60-<63 months’ (Table 7a)xxiv.
Table 7a: Childhood immunisation, Pilbara Health Re gion, Aboriginality, 2014
Age Group Aboriginal Non-Aboriginal Persons Aboriginal Non-Aborig inal Persons
12-<15 Months 83% 94% 92% 89% 92% 92%24-<27 Months* 91% 94% 93% 89% 91% 91%60-<63 Months 97% 93% 94% 95% 92% 92%
WACHSPilbara Health Region% fully immunised
Source: Australian Childhood Immunisation Register - Coverage Report
xxiv
Table 7b: Childhood immunisation, State and State A boriginal People, 2014
Age Group Aboriginal Persons
12-<15 Months 84% 91%24-<27 Months* 88% 90%60-<63 Months 92% 90%
% fully immunisedState
Source: Immunise Australia Program website, Department of Health, Australian Governmentxxv
*From quarter ending 31 December 2014, meningococcal C (given at 12 months), and dose 2 measles, mumps, rubella (MMR) and dose 1 varicella (given as MMRV at 18 months) was included in the definition of fully immunised for the 24-27 month cohort. The inclusion of these immunisations to the coverage calculation has caused a drop in the 24-27 month coverage rates. The coverage rate has dropped because the criteria to be assessed as fully immunised now includes more vaccines. The more vaccines included in the assessment, the higher the likelihood of reduced coverage rates. This usually resolves over time as the changes become more routine.
In the Pilbara, second quarter of 2013, the majority of vaccinations were provided by community health centres (Table 8)v.
Table 8: Immunisation Provider, Q2, 2013
Immunisation Provider (% of total vaccinations) (Q2 2013)
Pilbara Health Region
Metro State
GPs 24% 71% 63%Community Health Centres 65% 9% 18%
Source: DoH, Health Tracksv

Pilbara Health Profile 2015
20 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Health and Wellbeing Surveillance System, 0-15 years WA conducts a continuous Health and Wellbeing Surveillance System (HWSS). This is a population survey carried out by phone, which is designed to provide results and examine trends at a population level. It is unlikely to be representative of minority groups such as Aboriginal people and the homeless as they are less likely to have phone access. Parents/guardians report on behalf of children aged 0-15 yearsxxvi. Due to the high proportion of Aboriginal people in the Pilbara, the prevalence counts and rates are more likely to be an underestimate of the true amount than other regions.
The HWSS (2008-2013), showed the proportion of either or both parents having smoked during pregnancy was significantly higher for Pilbara children than for children in the State (35% compared with 26%), although the proportion of people who reported their home was smoke free was similar to the State rate at 98 per cent.
A significantly lower proportion reported as having used a dental health care service (50% and 58% respectively) and an allied health care service (17% and 26% respectively) in the last twelve months compared with the State (Table 9).
For the Pilbara health region, the HWSS also showed:
• over half of children (56%) did not eat the recommended daily serves of vegetables • one in four children (28%) did not eat the recommended daily serves of fruit • around half of children (52%) did not do sufficient physical activity • one in five children (20%) reported height and weight measurements that classified them as
overweight.
These proportions were similar to the State.
The prevalence for each of the National Health Priority Area Health Conditions and Injury, for Pilbara children surveyed were similar to the State:
• one in five children (20%) reported an injury requiring treatment from a medical professional in the previous year
• one in fifteen children (7%) had asthma.

Pilbara Health Profile 2015
21 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Table 9: Pilbara Child Population Profile, Health a nd Wellbeing Surveillance System (HWSS), 2008-2013
PilbaraWestern Australia
Significant difference from WA*
Prevalence (%)
Estimated pop ^
Prevalence (%)
Health Enhancing Behaviours
Health is rated excellent or very good 87.0 10,791 86.6 -
Home is smoke free 97.1 12,049 97.7 -
Eats recommended serves of fruit daily (a) (4 years+) 71.6 6,195 70.5 -
Eats recommended serves of vegetables daily (b) (4 years+) 44.1 3,818 45.1 -
Was exclusively breastfed for six months 18.9 2,347 15.1 -
Sufficient physical activity (c) (5 years+) 48.5 3,762 45.6 -Risk FactorsEither or both parents smoked during pregnancy 34.8 4,321 26.4 Higher
Sedentary more than two hours a day (d) (5 years+) 38.8 3,008 38.7 -
Overweight (5 years+) 19.6 1,520 16.7 -
Obese (5 years+) 10.0 + 775 6.2 -Prevalence of National Health Priority Area Health Conditions and Injury
Diabetes 0.0 0 0.2 + n/a
Current asthma 6.6 824 9.0 -
Current respiratory problem (e) 0.5 64 0.7 -
Injury (f) 19.5 2,418 19.7 -Health Service Utilisation in the last 12 months
Used a primary health care service (g) 77.6 9,629 81.5 -
Used a dental health care service 49.7 6,162 58.5 Lower
Used a mental health care service (h) 2.4 + 298 3.5 -
Used an allied health care service (i) 17.4 2,160 25.8 Lower
Used a hospital health care service (j) 27.6 3,428 26.1 -
Used an alternative health care service (k) 1.7 + 210 3.8 Lower Notes:
Results significantly better than the State are highlighted green, significantly worse are highlighted red. Where result could be interpreted as either better or worse, or results similar to the State have not been highlighted.
This information is based on 378 child responses from the Pilbara health region and 6,160 child responses within the State. * Determined by comparing confidence intervals, where intervals that do not overlap are deemed significantly different.
^ Estimated population refers to the estimated number of children with the particular risk factor/condition. It is derived by multiplying the Estimated Resident Population (2011) by the prevalence estimate. Where no children have the condition the estimated population is zero. † Estimates with a relative standard error above 25% are considered unreliable for general use. Therefore, throughout this table, estimates between 25% and 50% have been annotated by a cross and should be used with caution. (a) 2003 guidelines, children aged 4 to 11 years eat one or more serves, children aged 12 years and over eat three or more services of fruit.
(b) 2003 guidelines, children aged 4 to 7 years eat two or more serves, children aged 8 to 11 years eat three or more services and children aged 12 years and over eat
four or more serves of vegetables.
(c) Was physically active for 7 or more sessions and did 60 minutes or more of activity per session.
(d) Watches TV, videos or uses the computer for more than two hours a day.
(e) Respiratory problem other than asthma that has lasted 6 months or more.
(f) Injury in the last 12 months requiring treatment from a health professional.
(g) e.g. medical specialist, general practitioner, community health centre, community or district nurses.
(h) e.g. psychiatrist, psychologist or counsellor.
(i) e.g. optician, physiotherapist, chiropractor, podiatrist, dietician, nutritionist, occupational therapist, diabetes/other health educator.
(j) e.g. overnight stay, accident and emergency department or outpatients.
(k) e.g. acupuncturist, naturopath, homeopath or any other alternative health service.
Source: WA Health and Wellbeing Surveillance Systemxxvi

Pilbara Health Profile 2015
22 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Potentially Preventable Hospitalisations, 0-14 years Hospitalisations are an indicator of severe conditions in the community and assist in targeting primary care resources to prevent hospitalisations. Many hospitalisations result from conditions where hospitalisations could potentially be avoided using preventive care and early disease management. These hospitalisations are known as Potentially Preventable Hospitalisations (PPH) and are grouped into three major categories:
- Acute: This category includes dehydration and gastroenteritis, pyelonephritis (kidney infection), pelvic inflammatory disease, ear, nose and throat (ENT) infections, dental conditions, appendicitis, epilepsy, gangrene and cellulitis (skin infection).
- Chronic: This category includes asthma, diabetes (excluding renal dialysis), chronic obstructive pulmonary disease (COPD), iron deficiency anaemia, nutritional deficiencies and rheumatic heart disease.
- Vaccine preventable: This category includes mumps, measles, rubella, whooping cough, influenza and pneumonia.
Public health measures have the greatest influence on vaccine preventable conditions. Effective clinical care with regular review is essential to reduce avoidable admissions for people with chronic conditions.
For 2008-2012, PPH accounted for 1,627 hospitalisations of Pilbara children aged 0-14 years (18% of all hospitalisations in children). The rate of all PPH was significantly higher (1.2 times) for Pilbara children than for children in the Statev.
Between 2008 and 2012, there was a significant increase in the rate of PPH for children in the Pilbara. Figure 8 compares age-adjusted rates for the Pilbara and State by Aboriginality. The significant increase was mainly due to Aboriginal children as the non-Aboriginal Pilbara child rate remained steady from 2009. Pilbara Aboriginal children had significantly higher rates than non-Aboriginal children and State children for this periodv.
Figure 8: PPH, Pilbara & State by Aboriginality, 0- 14 years, 2008 to 2012
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
2008 2009 2010 2011 2012
AA
R p
er 1
00,0
00 p
erso
n ye
ars
PPH, Age adjusted rates, 0-14 years
Pilbara Aboriginal
State Aboriginal
Pilbara Non-Aboriginal
State Non-Aboriginal
Note: The error bars represent the 95% confidence interval of the rate.
Source: DoH, Health Tracksv

Pilbara Health Profile 2015
23 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Between 2008 and 2012, the Pilbara PPH rate for acute conditions in children was significantly higher than the State from 2009 and for chronic conditions was significantly higher for the whole period. The PPH rate for acute conditions increased significantly. The PPH rate for chronic conditions fluctuated and in 2012 was similar to the 2008 rate (Figure 9)v.
Figure 9: Acute and Chronic PPH, Pilbara, 0-14 year s, 2008 to 2012
0
200
400
600
800
1,000
1,200
1,400
1,600
1,800
2,000
2,200
2,400
2008 2009 2010 2011 2012
AA
R p
er 1
00,0
00 p
erso
n ye
ars
Acute and Chronic PPH Age adjusted rate, 0-14 years
Pilbara acute
State acute
Pilbara chronic
State chronic
Note: The error bars represent the 95% confidence interval of the rate.
Source: DoH, Health Tracksv
Between 2008 and 2012, the leading conditions were dental (acute), ENT infections (acute) and asthma (chronic). The PPH rate for dental conditions increased significantly in 2012 compared with 2008. The State rate did not increase throughout this period. The PPH rate for ENT infections also increased between 2008 and 2012. This trend was similar to the State. The PPH rate for asthma fluctuated while the State rate generally decreased. By 2012, the dental PPH rate was similar to the State rate, whereas ENT and asthma PPH rates were significantly higher than the State rates (Figure 10).
Figure 10: PPH for Dental Conditions, ENT Infection s and Asthma, Pilbara, 0-14 years, 2008 to 2012
0
100
200
300
400
500
600
700
800
900
Pilbara State Pilbara State Pilbara State
Dental ENT Asthma
AA
R p
er 1
00,0
00 p
erso
n ye
ars
PPH for Dental conditions, ENT infections and Asthm a Age adjusted rate, 0-14 years
2008 2009 2010 2011 2012
Note: The error bars represent the 95% confidence interval of the rate.
Source: DoH, Health Tracksv

Pilbara Health Profile 2015
24 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
The overall leading PPH condition for 2008-2012 was dental conditions, which accounted for 26 per cent of all PPH in children in the Pilbara. The PPH rate was similar to the State. This was followed by ENT infections accounting for 25 per cent of PPH (Table 10). The age group most affected by ENT infections is the 0-4 year oldsv.
Figures from a national survey in 2012-13, focussing on Aboriginal populations show that hearing problems and ear diseases, caused by chronic otitis media (middle ear infection) in childhood, is considerably higher among Aboriginal children aged 0-14 years (7%) than non-Aboriginal children (3.6%). This is of key concern as hearing loss resultant from otitis media has significant consequences for child language, social development and educationxxvii.
For 2003-2012, the rate of overall hospitalisations for disease of the ear and mastoid process for Pilbara Aboriginal children aged 0-14 years was significantly higher (1.5 times) than the non-Aboriginal rate, however the Aboriginal rate was similar to the rate for State Aboriginal childrenv.
From 2011 to 2012, the rate of overall hospitalisations for disease of the ear and mastoid process in Pilbara increased significantly for Aboriginal children and decreased significantly for non-Aboriginal childrenv.
The next leading PPH was asthma which was also the leading chronic condition (20% of all child PPH). The PPH rate was significantly higher (1.5 times) than the State rate. Other PPH for children aged 0-14 years in the Pilbara are shown in Table 10v.
Table 10: Leading PPH, Pilbara children aged 0-14 y ears, 2008-2012
PPH ConditionNumber of
PPH% all child
PPHSRR
dental conditions (acute) 416 26% 0.9
ENT infections (acute) 410 25% 1.2asthma (chronic) 330 20% 1.5convulsions and epilepsy (acute) 155 10% 1.3pyelonephritis (acute) 89 5% 1.0
influenza and pneumonia (vaccine) 68 4% 1.9
COPD (chronic) 25 2% 4.7
cellulitis (acute) 22 1% 1.5
rheumatic heart disease (chronic) 21 1% 5.0diabetes complications (chronic) 18 1% 0.6All child PPH 1,627 100% 1.2
Notes:
The standardised rate ratio (SRR) is the ratio between a particular health region (or district) and the state. A ratio of 1 means that the regional rate is the same as the state, and a value of 2 indicates the regional rate is twice that of the state. A ratio of 0.5 indicates that the rate in a region is half that of the State population.
Local rates are compared to the rate of all residents of the State using the standardised rate ratio (SRR) and the 95% confidence interval of the SRR. Those that are significantly different to the state rate (1.0) are coloured. Those between 1 and 1.5 times the state rate are highlighted orange, higher than 1.5 times the state are highlighted red while those rates significantly less than the state are highlighted green.
Source: DoH, Health Tracksv

Pilbara Health Profile 2015
25 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Injuries, 0-14 years For 2008-2012, injury and poisoning hospitalisations in children aged 0-14 years in the Pilbara accounted for 1,265 hospitalisations (14% of all hospitalisations in children). The hospitalisation rate of all injury and poisoning was significantly higher (1.3 times) for Pilbara children (2,185 per 100,000) than for children in the Statev.
The leading causes of injury and poisoning hospitalisations for children in the Pilbara were accidental falls, exposure to mechanical forces and transport accidents. The hospitalisation rates were significantly higher than the State for each of these external causes and transport accidents were more than double (2.2 times) the State ratev.
The rate of hospitalisations for accidental falls in children in the Pilbara was 741 per 100,000 children. While the rate had been fairly constant from 2008 to 2011, it increased significantly from 2011 to 2012 (Figure 10). For children aged 0-4 years, the rate was 576 per 100,000 which was similar to the State ratev.
The rate of hospitalisations for exposure to mechanical forces in children in the Pilbara was 432 per 100,000 and the main forces were cutting/piercing objects, accidentally hit, struck or crushed by an object and animals. The rate increased significantly from 2008 to 2010 then decreased significantly from 2010 to 2012v.
The rate for transport accident hospitalisations in children in the Pilbara was 389 per 100,000. The rate increased significantly from 2008 to 2009 then decreased significantly between 2009 and 2012. Despite this decrease, the rate was still significantly higher than the State rate in 2012 (Figure 11). Motor vehicle/motorcycle accidents were the main transport accident hospitalisations in Pilbara children at 166 per 100,000. The motor vehicle/motorcycle accident hospitalisation rate was significantly higher (2.7 times) than the State ratev.
Figure 11: Hospitalisations for leading causes of i njury and poisoning, Pilbara v State, 0-14 years, 2008 to 2012
0
100
200
300
400
500
600
700
800
900
Pilbara State Pilbara State Pilbara State
Accidental Falls Mechanical Forces Transport Accidents
Age
adj
uste
d ra
te p
er 1
00,0
00 p
erso
n ye
ars
Hospitalisations for Leading Causes of Injury and P oisoning Age adjusted rate, 0-14 years
2008 2009 2010 2011 2012
Note: The error bars represent the 95% confidence interval of the rate.
Source: DoH, Health Tracksv

Pilbara Health Profile 2015
26 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Notifiable Infections, 0-14 years Death and illness resulting from communicable diseases are a major public health problem. Effective containment of many communicable diseases has occurred due to public health legislation requiring reporting of these diseases. ‘Notifiable’ diseases includes a range of vaccine preventable diseases, vector borne diseases, food and water borne diseases, sexually transmitted infections and emerging infections such as Severe Acute Respiratory Syndrome (SARS).
Under the provisions of the WA Health Act 1911 and Health Amendment Act (2006), any medical practitioner or nurse practitioner attending a patient known or suspected to have a notifiable communicable disease has a legal obligation to report the diagnosis to the Department of Health. A complete list of the current notifiable diseases can be accessed at www.public.health.wa.gov.au
For 2007-2011, there were 747 notifiable diseases in children aged 0-14 years in the Pilbara. The notification rate of notifiable diseases (1,215 per 100,000) was significantly higher (1.5 times) for Pilbara children than for children in the State (794 per 100,000)v.
The enteric disease notification rate (463 per 100,000) (salmonellosis, campylobacteriosis, cryptosporidiosis, shigellosis) for Pilbara children was significantly higher (2 times) than State children (Table 11). There was a significant decrease between 2007 and 2010 and a significant increase from 2010 to 2011 for enteric disease notification rates. The rate remained significantly higher (1.8 times) than the State in 2011. The State rate fluctuated throughout 2007 to 2011v.
The vaccine preventable disease notification rate (265 per 100,000) (influenza, pertussis, pneumococcal infection) for children was similar to the State childhood ratev.
Table 11: Disease notifications for Pilbara childre n aged 0-14 years, 2007-2011
Condition Number SRR AAR*
enteric diseases 313 2.0 463
vaccine preventable diseases 162 0.9 265
vector-borne diseases 11 1.0 N/A
blood-borne diseases 7 2.2 N/A
All child notifications 747 1.5 1,215 * Age-adjusted rate per 100,000 persons
Note: The standardised rate ratio (SRR) is the ratio between a particular health region (or district) and the state. A ratio of 1 means that the regional rate is the same as the state, and a value of 2 indicates the regional rate is twice that of the state. A ratio of 0.5 indicates that the rate in a region is half that of the State population.
Note: Local rates are compared to the rate of all residents of the State using the standardised rate ratio (SRR) and the 95% confidence interval of the SRR. Those that are significantly different to the state rate (1.0) are coloured. Those between 1 and 1.5 times the state rate are highlighted orange, higher than 1.5 times the state are highlighted red while those rates significantly less than the state are highlighted green.
Source: DoH, Health Tracksv
For children aged 0-4 years in the Pilbara, the highest rate was for salmonellosis (540 per 100,000), (enteric). The rate was significantly higher (2.9 times) in the Pilbara compared to the State. Cryptosporidiosis, campylobacteriosis and shigellosis (enteric) and influenza (vaccine preventable) were leading notifiable diseases. The notification rates were significantly higher for salmonellosis (2.9 times), cryptosporidiosis (3 times), shigellosis (4.3 times), influenza (1.4 times) and campylobacteriosis (1.4 times) than the State rates.

Pilbara Health Profile 2015
27 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
For 2002-2011, Pilbara Aboriginal children aged 0-4 years had significantly higher (7 times) all-cause notification rates than their non-Aboriginal counterpartsv.
Health of Adults
Self-reported risk factors, 16 years and over Lifestyle factors are particularly important due to their relationship with chronic conditions that are considered to be preventable. Prevention and management of these modifiable risk factors can have a substantial effect on these preventable chronic conditionsviii.
WA conducts a continuous Health and Wellbeing Surveillance System (HWSS). This is a population survey carried out by phone, designed to provide results and examine trends at a population level. It is unlikely to be representative of minority groups such as Aboriginal people and the homeless as they are less likely to have phone accessxxviii.
Results from the HWSS for the Pilbara population are shown in Table 12v. The data for adults aged 16 years and over are for 2009-2012. In summary:
• one in four adults (24%) smoked • over half of adults (53%) did not eat the recommended daily serves of fruit • over half of adults (53%) drank alcohol at risk for long-term harm which • one in four adults (26%) drank alcohol at risk for short-term harm • one in three adults (34%) reported height and weight measurements that classified them as
obese. All these measures were significantly higher than the State. Other findings of concern were: • most adults (90%) did not eat the recommended daily serves of vegetables • nearly half of adults (47%) did not do sufficient physical activity While some risk factors showed no significant difference in the prevalence of Pilbara residents compared with the State, the prevalence is still important because these behaviours are modifiable risk factors for chronic conditions.
Implications for primary health care service planni ng: Pilbara children have higher potentially preventable hospitalisation rates than the State including dental conditions, ENT infections and asthma, and Pilbara Aboriginal children have rates higher than non-Aboriginal children. As potentially preventable conditions can be greatly influenced by public health measures this suggests a need for increased preventative programs as well as maintenance programs and primary health care services. High rates of hospitalisation due to the increasing rate of accidental falls in children highlight the need for public health intervention.

Pilbara Health Profile 2015
28 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Lifestyle risk factor information is not readily available for Aboriginal Pilbara residents. At the national level, Aboriginal people aged 15 years and over were 2.6 times as likely as non-Aboriginal people to be a current daily smoker (40% compared with 15%) and a third (33%) of Aboriginal people have never smoked compared to half of non-Aboriginal people (53%). These differences were statistically significantxxvii.
Furthermore, nationally, at least twice as many Aboriginal people aged 15 years and over reported fair or poor self-assessed health and those aged 18 years and over reported higher levels of psychological stress than non-Aboriginal people (2.7 times)xxvii.
Table 12: Lifestyle and psycho-social risk factors for persons aged 16 years and over by gender, 2009- 2012
Female Male Persons Female Male Persons Female Male Persons
Currently smokes 19.8 26.8 23.9 11,794 12.3 17.7 15.0 Higher Higher Higher
Does not eat two or more serves of fruit daily 49.8 55.5 53.1 26,263 44.4 50.6 47.5 - - Higher
Does not eat five or more serves of vegetables daily 87.2 91.9 89.9 44,444 86.3 91.0 88.7 - - -
Drinks at high risk levels for long-term harm (1) 37.7 64.8 53.4 26,400 25.2 48.2 36.7 Higher Higher Higher
Drinks at high risk levels for short-term harm (2) 16.0 33.2 26.0 12,834 9.7 23.4 16.6 Higher Higher Higher
Insufficient physical activity (3) 49.9 45.1 47.1 23,296 50.0 44.8 47.4 - - -
Current high blood pressure 10.0 9.7 9.8 4,862 16.5 17.0 16.8 Lower Lower Lower
Current high cholesterol 11.4 10.0 10.5 5,212 17.8 20.2 19.0 Lower Lower Lower
Overweight (4) 35.8 41.4 39.1 19,338 32.5 46.4 39.6 - - -
Obese (4) 30.8 36.1 33.9 16,762 26.9 26.9 26.9 - Higher Higher
High or very high psychological distress 9.9 6.0 7.6 3,765 9.5 6.9 8.2 - - -
Lack of control over life in general (5) 6.1 3.9 4.9 2,400 5.0 3.5 4.2 - - -
IndicatorPilbara area Prevalence
EstimatePopulation Estimate^
WA Prevalence Estimate Comparison to WA
Health behaviours, adults 16 years and over
Risk Factors - adults 16 years and over
Note: Results significantly better than the State are highlighted green, significantly worse are highlighted red. Where result could be interpreted as either better or worse, or results similar to the State have not been highlighted.
1. Drinks more than 2 standard drinks on any one day. 2. Drinks more than 4 standard drinks on any one day. 3. Did not do 150 minutes or more of moderate activity over five or more sessions. 4. Self-reported height and weight have been adjusted for under-reporting. BMIs classified as overweight (25≤BMI<30) or obese (BMI≥30). 5. Often or always feels a lack of control over life in general. ^ The estimated population refers to the estimated number of people with the risk factor/condition. It is derived by multiplying the Estimated Resident Population by the persons prevalence estimate.
Source: DoH, Health Tracksv
Self-reported chronic conditions, 16 years and over Chronic conditions refer to long-term conditions that last for six months or more. Not all chronic conditions result in hospitalisations, and hospital data cannot provide a complete picture of the prevalence of chronic conditions in the community. This type of information is more appropriately collected by population based surveys, such as the WA HWSS or Bettering the Evaluation and Care of Health (BEACH) surveys.
The HWSS survey (2009-2012) for self-reported, doctor diagnosed chronic conditions for Pilbara adults found:
• one in four adults reported an injury requiring treatment from a medical professional in the previous year (24%)
• one in seven adults reported a current mental health problem (15%) • one in ten adults reported arthritis (10%). This proportion was significantly lower than the
State. • one in eleven adults reported asthma (8.8%)v.

Pilbara Health Profile 2015
29 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Other than arthritis which was significantly lower than the State, these proportions were similar to those of the State. Nationally, Aboriginal people report a higher prevalence of most chronic conditions compared with non-Aboriginal people. For example, at a national level, after adjusting for age, Aboriginal people were nearly twice as likely to report having asthma, and three times as likely to report having diabetesxxvii. As the HWSS may not be representative of the Aboriginal population, national levels of chronic disease among the Aboriginal population must be factored into estimates of chronic disease in the Pilbara region, given that 16% of the population is Aboriginal.
Self-reported service utilisation, 16 years and over In 2009-2012, Pilbara residents aged 16 years and over, reported their health service utilisation in the previous year (Table 13)v. In summary:
• One in three (34%) reported having used a hospital based health care service which was significantly higher than the State.
• Mean visits to all other health care services were similar to or significantly lower than those of the State.
• Nine in ten (88%) reported having used a primary health care service. • Nearly half of adults (47%) reported having used a dental health care service, which was
significantly lower than the State. • The services accessed at a significantly lower proportion than the State were dental,
allied health, mental health and alternative health care services.
Implications for health care service planning: The rates of modifiable risk factors and self-reported chronic conditions, regardless of prevalence within an area, should be monitored as interventions designed to impact on these behaviours have greatest potential to reduce chronic conditions. Pilbara adults were more likely to report poor health behaviours including smoking, drinking at risk of harm and obesity, which are linked with several chronic conditions and with alcohol-related injury. While specific information regarding the Pilbara Aboriginal population is not available, nationally Aboriginal people are more likely to smoke and to have poorer health than non-Aboriginal people. This demonstrates a need for culturally appropriate and targeted programs and services.

Pilbara Health Profile 2015
30 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Table 13: Self-reported health service utilisation for persons aged 16 years and over by gender, 2009- 2012
Female Male Persons Female Male Persons Female Male Persons
Used a primary health care service (1) 91.2 85.8 88.1 43,541 92.1 84.5 88.3 - - -
Used a dental health care service 49.0 46.1 47.3 23,371 57.2 51.3 54.2 Lower - Lower
Used a mental health care service (2) 8.4 5.1 6.4 3,187 7.4 5.6 6.5 - - -
Used an allied health care service (3) 45.9 39.7 42.3 20,913 52.4 45.8 49.1 Lower - Lower
Used a hospital health care service (4) 38.2 30.7 33.9 16,740 28.2 26.4 27.3 Higher - Higher
Used an alternative health care service (5) 8.5 6.3 7.2 3,572 10.7 5.5 8.1 - - -
Mean visits to primary health care service (1) 5.2 3.5 4.2 - 4.8 3.6 4.2 - - -
Mean visits to dental health care service 1.0 0.8 0.9 - 1.1 1 1 - - -
Mean visits to mental health care service (2) 0.4 0.2 0.3 - 0.5 0.4 0.5 - Lower Lower
Mean visits to allied health care service (3) 2.0 1.9 2.0 - 3.1 2.3 2.7 Lower - Lower
Mean visits to hospital based health care service (4) 0.7 0.6 0.6 - 0.5 0.5 0.5 - - -
Mean visits to alternative health care service (5) 0.3 0.1 0.2 - 0.6 0.3 0.4 Lower - Lower
WA Prevalence Estimate Comparison to WA
Health service utilisation in the past 12 months, a dults 16 years and over
Mean visits in the past 12 months, adults 16 years and over
IndicatorPilbara area Prevalence
EstimatePopulation Estimate
Notes: 1. e.g. medical specialist, general practitioner, community health centre, community or district nurses. 2. e.g. psychiatrist, psychologist or counsellor. 3. e.g. optician, physiotherapist, chiropractor, podiatrist, dietician, nutritionist, occupational therapist, diabetes/other health educator. 4. e.g. overnight stay, accident and emergency department or outpatients. 5. e.g. acupuncturist, naturopath, homeopath or any other alternative health service.
Source: DoH, Health Tracksv
Implications for health care service planning:
Primary health services are particularly important as they provide an opportunity to monitor modifiable risk factors and chronic conditions, and to implement public health programs and interventions, such as vaccinations. A high prevalence of a condition, but a low health service utilisation for that condition may suggest either a lack of access to services, or optimal control of the condition. It is therefore important to look at actual numbers as well as rates of conditions and service provision. Provision of ambulatory and primary health care in partnership with local government, other private and not-for-profit health providers is one means to improve chronic disease management.

Pilbara Health Profile 2015
31 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Hospitalisations, 15-64 years For 2008-2012, the overall hospitalisation rate of Pilbara residents aged 15-64 years was similar to the State rate. However, female hospitalisation rates were significantly higher than the State female rates (Table 14).
Table 14: Hospitalisations, Pilbara residents, 2008 -2012
Number SRR AAR*PilbaraMales 31,629 0.8 24,297
Females 40,176 1.3 50,961Persons 71,805 1.0 34,050StateMales 1,144,142 1 27,886Females 1,466,578 1 37,480Persons 2,610,720 1 32,563
* AAR Age-adjusted rate per 100,000 persons
Notes:
The standardised rate ratio (SRR) is the ratio between a particular health region (or district) and the state. A ratio of 1 means that the regional rate is the same as the state, and a value of 2 indicates the regional rate is twice that of the state. A ratio of 0.5 indicates that the rate in a region is half that of the State population.
Local rates are compared to the rate of all residents of the State using the standardised rate ratio (SRR) and the 95% confidence interval of the SRR. Those that are significantly different to the state rate (1.0) are coloured. Those between 1 and 1.5 times the state rate are highlighted orange, higher than 1.5 times the state are highlighted red while those rates significantly less than the state are highlighted green.
Source: DoH, Health Tracksv
For 2003-2012, the overall hospitalisation rate of Aboriginal Pilbara residents aged 15-64 years was significantly higher (by 10%) than the Aboriginal State rate. This rate was also significantly higher (6.1 times) than the non-Aboriginal Pilbara rate (Table 15). These higher rates highlight the health disparity of residents in the Pilbara compared with those living elsewhere in the State and in particular, the disparity between Aboriginal and non-Aboriginal residentsv.
Table 15: Hospitalisations, Pilbara Aboriginal and non-Aboriginal residents, 15-64 years, 2003-2012
Number SRR AAR*
Aboriginals 58,264 1.1 129,517Non-Aboriginals 68,928 0.7 21,081
* AAR Age-adjusted rate per 100,000 persons
Notes:
The period stated in this table is longer than the previous table to provide more accurate data for Aboriginal people.
The standardised rate ratio (SRR) is the ratio between a particular health region (or district) and the state. A ratio of 1 means that the regional rate is the same as the state, and a value of 2 indicates the regional rate is twice that of the state. A ratio of 0.5 indicates that the rate in a region is half that of the State population.
Local rates are compared to the rate of all residents of the State using the standardised rate ratio (SRR) and the 95% confidence interval of the SRR. Those that are significantly different to the state rate (1.0) are coloured. Those between 1 and 1.5 times the state rate are highlighted orange, higher than 1.5 times the state are highlighted red while those rates significantly less than the state are highlighted green.
Source: DoH, Health Tracksv

Pilbara Health Profile 2015
32 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
For adults aged 15-64 years, across the State for 2008-2012, renal dialysis accounted for 306,085 separations (7% of total separations). Pilbara residents had 17,051 separations for renal dialysis (24%). Leading conditions after renal dialysis were delivery (accounting for 3% of hospitalisations), followed by digestive system symptoms, arthropathies and injuries to head and neck, each accounting for just over two per cent of separationsv.
The leading causes of hospitalisation differed markedly between Aboriginal and non-Aboriginal Pilbara residents aged 15-64 years. Dialysis accounted for the highest number of hospitalisations of Aboriginal Pilbara residents for 2003-2012, at 51 per cent. This was followed by injuries to head and neck (3%), skin infections (2%), injuries to upper limbs (2%) and influenza and pneumonia (2%).
For non-Aboriginal residents in 2008-2012, dialysis was not a leading cause of hospitalisation. Delivery was the leading cause and accounted for four per cent of hospitalisations. Arthropathies (4%), digestive system symptoms (3%), chemotherapy (3%) and diseases of female genital organs (3%) were also leading causesv. The period stated for Aboriginal people is longer to provide more accurate and confidential data.
The top five causes of hospitalisation by major category for 15-64 year olds for 2008-2012 are shown in Table 16. The leading cause of hospitalisation for Pilbara residents was pregnancy and childbirth which accounted for 11% of hospitalisations. This was followed by injury and poisoning (10%), which can include transport accidents, other external accidental injuries, intentional self-harm, assault, and complications of medical and surgical carev.
Table 16: Leading cause of hospitalisation, Pilbara residents, 15-64 years, 2008-2012
RankCause of
HospitalisationNumber
% of all hospitalisations
(15-64yrs)State Rank
1 Pregnancy and childbirth 7,878 11% 22 Injury and Poisoning 6,855 10% 43 Digestive diseases 6,402 9% 14 Ill-defined conditions 4,062 6% 55 Musculo-skeletal diseases 3,571 5% 3
All hospitalisations (15-64yrs) 71,805 100% NOTE: Leading causes exclude ‘Factors influencing health status and contact with health services’ and ‘attending health services for examination and investigation’, reproduction, specific procedures, and other circumstances, and potential health hazards related to communicable diseases, socioeconomic and psychosocial circumstances, family and personal history. This also includes renal dialysis.
Source: DoH, Health Tracksv
Alcohol and tobacco related hospitalisations, 15-64 years For 2008-2012, the hospitalisation rate for alcohol consumption was 1,093 per 100,000 for Pilbara adults aged 15-64 years. This was significantly higher (1.4 times) than the State rate. The tobacco consumption hospitalisation rate was 632 per 100,000 which was also significantly higher (1.3 times) than the State ratev.
For 2003-2012, the rate of alcohol-caused hospitalisations for Aboriginal Pilbara residents aged 15-64 years, was significantly higher (9 times) than the non-Aboriginal rate. The rate of tobacco-caused hospitalisations for Aboriginal people was also significantly higher (5 times) than the non-Aboriginal ratev.

Pilbara Health Profile 2015
33 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Potentially preventable hospitalisations, 15-64 years For 2008-2012, PPH accounted for 4,438 hospitalisations of Pilbara adults aged 15-64 years (6% of all hospitalisations in this age group). The Pilbara PPH rate for 15-64 year olds was significantly higher than the State rate, across all categories (vaccine preventable, acute and chronic conditions)v.
Figure 12 compares age-adjusted potentially preventable hospitalisation rates from 2008 to 2012 for the Pilbara and State by Aboriginality. Pilbara and State non-Aboriginal rates fluctuated a little over this period. The Pilbara Aboriginal rate decreased significantly in 2011 compared with 2009 and increased from 2011 to 2012, although this increase was not significant. The State Aboriginal rate also decreased significantly in 2011 compared with 2008 then increased significantly in 2012. The decrease in 2011 however, was probably due to the change in the definition of diabetes complications. Notwithstanding the diabetes definition, the Pilbara Aboriginal PPH rate was significantly higher than the State Aboriginal rate between 2009 and 2010 and similar in 2008 and between 2011 and 2012v.
Figure 12: PPH, Pilbara & State by Aboriginality, 1 5-64 years, 2008 to 2012
0
2,000
4,000
6,000
8,000
10,000
12,000
2008 2009 2010 2011 2012
AA
R p
er 1
00,0
00 p
erso
n ye
ars
PPH, Age adjusted rates, 15-64 years
Pilbara Aboriginal
State Aboriginal
State Non-Aboriginal
Pilbara Non-Aboriginal
Note: The error bars represent the 95% confidence interval of the rate.
Source: DoH, Health Tracksv
PPH rates for vaccine preventable conditions in Pilbara adults aged 15-64 years are much lower than acute and chronic conditions and fluctuated during the 2008 to 2012 periodv.
Figure 13 shows the trends in PPH rates for acute and chronic conditions for adults in the Pilbara. The Pilbara acute and chronic PPH rates were significantly higher than the respective State rates between 2008 and 2012. The PPH rate for acute conditions decreased from 2008 to 2012 but this was not statistically significantv.
There were significant changes in national coding standards for diabetes complications hence, the numbers and rates are not comparable over the years between 2008 and 2012 for diabetes complications and trends in chronic conditions need to be viewed with caution given diabetes is a chronic conditionv.

Pilbara Health Profile 2015
34 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
For 2008-2012, the overall leading PPH condition in the Pilbara was diabetes complications, which accounted for 24 per cent of all PPH in adults aged 15-64 years. The PPH rate was significantly higher (2.1 times) than the State (Table 17)v.
Figure 13: Acute and Chronic PPH, Pilbara & State, 15-64 years, 2008 to 2012
500
600
700
800
900
1,000
1,100
1,200
1,300
2008 2009 2010 2011 2012
AA
R p
er 1
00,0
00 p
erso
n ye
ars
Acute and Chronic PPHAge adjusted rate, 15-64 years
Pilbara Chronic Conditions
Pilbara Acute Conditions
State Acute Conditions
State Chronic Conditions
Note: The error bars represent the 95% confidence interval of the rate.
Source: DoH, Health Tracksv
The change in rate for diabetes complications between 2008 and 2012 was due to the change in national coding standards as mentioned earlier. Notwithstanding changes to the definition, Pilbara rates were significantly higher than the State rates (Figure 14)v.
The PPH rate for dental conditions fluctuated for Pilbara 15-64 year olds while the State rate increased significantly over the 2008 to 2012 period. In 2011 and 2012, the Pilbara rate was significantly lower than the State ratev.
The PPH rate for pyelonephritis increased between 2008 and 2012 for Pilbara and the State. This increase was only statistically significant for the State. Despite the increase not being significant, the rate for Pilbara was significantly higher than the State between 2008 and 2012 (Figure 14). The Aboriginal rate for 15-64 year olds was significantly higher than the non-Aboriginal rate for both the Pilbara (6.8 times) and State (5.1 times) (2003-2012)v.
The female PPH rate for pyelonephritis was significantly higher than the male rate for both Pilbara (10 times) and State (4.3 times) 15-64 year olds, (2008-2012)v.

Pilbara Health Profile 2015
35 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Figure 14: Top 3 PPH, Pilbara, 15-64 years, 2008 to 2012
0
100
200
300
400
500
600
700
800
900
Pilbara State Pilbara State Pilbara State
Diabetes complications Dental conditions Pyelonephritis
AA
R p
er 1
00,0
00 p
erso
n ye
ars
Leading PPH, Age adjusted rates, 15-64 years
2008 2009 2010 2011 2012
Note: The error bars represent the 95% confidence interval of the rate.
Source: DoH, Health Tracksv
Other leading PPH for adults aged 15-64 years in the Pilbara are shown in Table 17. Most of these conditions have rates significantly higher than the State ratesv.
Table 17: Leading Potentially Preventable Hospitali sations, Pilbara, 15-64 years, 2008-2012
PPH Condition Number % all PPH
(15-64 years)SRR
diabetes complications (chronic) 1,086 24% 2.1dental conditions (acute) 454 10% 0.8pyelonephritis (acute) 436 10% 1.3convulsions and epilepsy (acute) 367 8% 1.3ENT infections (acute) 319 7% 1.6asthma (chronic) 268 6% 1.6congestive cardiac failure (chronic) 216 5% 2.8COPD (chronic) 206 5% 1.5influenza and pneumonia (vaccine) 205 5% 2.1gangrene (acute) 154 3% 3.3cellulitis (acute) 139 3% 1.5iron deficiency anaemia (chronic) 126 3% 0.6pelvic inflammatory disease (acute) 108 2% 1.5dehydration and gaestroenteritis (acute) 96 2% 0.8appendicitis and generalised peritonitis (acute) 59 1% 0.9All PPH (15-64yrs) 4,438 100% 1.4 Notes:
The standardised rate ratio (SRR) is the ratio between a particular health region (or district) and the state. A ratio of 1 means that the regional rate is the same as the state, and a value of 2 indicates the regional rate is twice that of the state. A ratio of 0.5 indicates that the rate in a region is half that of the State population.
Local rates are compared to the rate of all residents of the State using the standardised rate ratio (SRR) and the 95% confidence interval of the SRR. Those that are significantly different to the state rate (1.0) are coloured. Those between 1 and 1.5 times the state rate are highlighted orange, higher than 1.5 times the state are highlighted red while those rates significantly less than the state are highlighted green.
Source: DoH, Health Tracksv

Pilbara Health Profile 2015
36 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Notifiable Infections and Events, 15-64 years For 2007-2011, communicable disease notification rates for Pilbara health region residents aged 15-64 years were significantly higher than the State rates overall and specifically for sexually transmitted infections (STI) , vaccine preventable and vector-borne diseases. The rates for STI and vector-borne notifications were nearly double the State rates. The number of STI accounted for 68 per cent of all communicable disease notifications in 15-64 year olds in the Pilbara (Table 18)v.
Table 18: Pilbara resident communicable disease not ification rates, 15-64 years, 2007-2011
Condition Number SRR AAR*
sexually transmitted diseases 2,966 1.9 1,415
vaccine preventable diseases 583 1.3 279
vector-borne diseases 325 1.9 146
enteric diseases 308 0.9 139
blood-borne diseases 192 0.7 88
All notifications (15-64yrs) 4,393 1.6 2,076 * Age-adjusted rate per 100,000 persons
Notes:
The standardised rate ratio (SRR) is the ratio between a particular health region (or district) and the state. A ratio of 1 means that the regional rate is the same as the state, and a value of 2 indicates the regional rate is twice that of the state. A ratio of 0.5 indicates that the rate in a region is half that of the State population.
Local rates are compared to the rate of all residents of the State using the standardised rate ratio (SRR) and the 95% confidence interval of the SRR. Those that are significantly different to the state rate (1.0) are coloured. Those between 1 and 1.5 times the state rate are highlighted orange, higher than 1.5 times the state are highlighted red while those rates significantly less than the state are highlighted green.
Source: DoH, Health Tracksv
Vaccine-preventable diseases, 15-64 years The vaccine preventable diseases notification rate in the Pilbara health region for 15-64 year olds was significantly higher (1.3 times) than the State rate. Most of these notifications were for Influenza (66%) and pertussis notifications (22%). The age group most affected by influenza and pertussis was the 25-64 year age groupv.
Figure 15: Influenza Virus notifications, Pilbara a dults aged 15-64 years, 2007-2011
0
100
200
300
400
500
600
2007 2008 2009 2010 2011
AA
R p
er
10
0,0
00
pe
rso
n y
ea
rs
Influenza notifications, Age adjusted rate, 15-64 years
Pilbara Influenza
State Influenza
Note: The error bars represent the 95% confidence interval of the rate.
Source: DoH, Health Tracksv

Pilbara Health Profile 2015
37 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Vector-borne diseases, 15-64 years The average number of vector-borne disease related notifications in the Pilbara health region for 15-64 year olds was around 50 persons per year between 2007 and 2011 except in 2009 where there were 121 notifications. Most (71%) of the vector-borne notifications for this period were for Ross River Virus (RRV)v.
The notification rate for RRV fluctuated over 2007 to 2011 for both the Pilbara and the State and it remained significantly higher in Pilbara residents aged 15-64 years compared with the State over this period (Figure 15)v.
Figure 16: Ross River Virus notifications, Pilbara adults aged 15-64 years, 2007-2011
0
50
100
150
200
250
2007 2008 2009 2010 2011
AA
R p
er
10
0,0
00
pe
rso
n y
ea
rs
Ross River Virus Notifications, Age adjusted rate, 15-64 years
Pilbara RRV
State RRV
Notes:
The 2007 Pilbara rate has been suppressed due to an unreliable rate derived from a low count.
The error bars represent the 95% confidence interval of the rate.
Source: DoH, Health Tracksv

Pilbara Health Profile 2015
38 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Sexually Transmitted Infections, all ages
Notifiable sexually transmitted infection information for Pilbara residents is shown in Figures 17 and 18 and Table 19. Information for this section presents all age groups combined as per the data source.
Figure 17: ASR of Chlamydia and Gonorrhoea notifica tions by Public Health Unit, WA, 2012
Source: The Epidemiology of Notifiable Sexually Transmitted Infections and Blood-Borne Viruses in Western Australia 2012xxix.

Pilbara Health Profile 2015
39 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
The age-standardised rate of all notifiable communicable diseases was significantly higher (1.5 times) among Pilbara residents compared with the State, in particular STI which was 1.9 times higher (Figure 18). The trend for STI in the Pilbara remained fairly steady between 2007 and 2011 except in 2009 when it dropped significantlyv.
Figure 18: Sexually transmitted notification rates, Pilbara, 2007-2011
0
200
400
600
800
1,000
1,200
1,400
2007 2008 2009 2010 2011
AS
R p
er
10
0,0
00
pe
rso
n y
ea
rs
Sexually Transmitted Infection Notification Rates
Pilbara Health Region
State
The error bars represent the 95% confidence interval of the rate.
Source: DoH, Health Tracksv
There are noticeable differences in the rate of some notifiable diseases in the Aboriginal compared with non-Aboriginal populations. Table 19 shows the Pilbara STI and Blood-borne virus notification ratesxxix.
Table 19: Notifiable disease by Aboriginality, Pilb ara residents, 2012
No. ASR No. ASR No. ASRSexually Transmitted Infections (STI) Chlamydia 181 1,758 207 346 417 645 Gonorrhoea 160 1,529 30 45 190 311Blood Borne Virus (BBV)* Hepatitis B 7 83 9 19 16 25 Hepatitis C 5 58 14 22 20 29
PersonsAboriginal Non-Aboriginal
* includes newly acquired and unspecified. ASR = Age-standardised notification rate per 100,000 population
Source: The Epidemiology of Notifiable Sexually Transmitted Infections and Blood-Borne Viruses in Western Australia 2012xxix
Chlamydia is the most commonly notified STI and gonorrhoea is the second most commonly notified STI in WA. There was an increase in the chlamydia notification rate for the Pilbara region from 2003 to 2012 of 5 per cent per year, compared with 11per cent per year for WA. The Pilbara gonorrhoea notification rate fluctuated from 2003 to 2012 and peaked in 2006xxix.
The Hepatitis B notification rate for Pilbara has fluctuated from 2003 to 2012 while the State rate has remained fairly steady. The hepatitis C notification rate fluctuated throughout this period. From 2008 to 2012, the rate decreased significantly for both Pilbara and the Statexxix.

Pilbara Health Profile 2015
40 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Cancer Incidence, 15-64 years Cancer is the leading cause of the total burden of disease and injury in Australia. In 1996, it was declared a National Health Priority Area. In 2008, five cancers (bowel, breast, cervical, lung and melanoma) were included in the health performance indicator ‘Incidence of selected cancers’ as part of the National Healthcare Agreement (NHA)xxx. Since then, the incidence of prostate cancer has increased throughout the State, and is one of the most common cancers in the Pilbara. The Pilbara rates for prostate cancer and breast cancer are significantly lower than the State. Other non-NHA cancers are included for the Pilbara as they are ranked in the top five (Table 20)v.
Table 20: Pilbara Cancer incidence, 15-64 years, 20 08-2012
Rank Condition N % all cases(15-64yrs)
SRR
1 breast 59 13% 0.5
1 melanoma (skin) 59 13% 0.8
1 prostate gland 59 13% 0.8
2 colorectal 40 9% 0.8
3 lymphoma 28 6% 0.9
4 lung, bronchus & trachea 26 6% 0.9
5 thyroid 21 5% 0.8450 100% 0.8All cancer incidence (15-64yrs)
Notes:
The standardised rate ratio (SRR) is the ratio between a particular health region (or district) and the state. A ratio of 1 means that the regional rate is the same as the state, and a value of 2 indicates the regional rate is twice that of the state. A ratio of 0.5 indicates that the rate in a region is half that of the State population.
Local rates are compared to the rate of all residents of the State using the standardised rate ratio (SRR) and the 95% confidence interval of the SRR. Those that are significantly different to the state rate (1.0) are coloured. Those between 1 and 1.5 times the state rate are highlighted orange, higher than 1.5 times the state are highlighted red while those rates significantly less than the state are highlighted green.
Source: DoH, Health Tracksv
Implications for health care service planning: The number and trend of notifiable diseases, particularly sexually transmitted infections need to be considered for health promotion programs and screening opportunities. These notifications point to unsafe sexual behaviour that places the individual at risk not only of these infections, but of others, such as HIV/AIDS, and unplanned pregnancies. Notification rates for STI are higher in the younger population and Aboriginal people. Specific screening may help to reduce the spread of notifiable diseases. Health regions should consider the recommendations and five key strategies of the “Third National Transmissible Infections Strategy 2014-2017” when planning targeted programs for this population (Source: Department of Health, July 2014, Third National Sexually Transmissible Infections Strategy 2014-2017 at http://www.health.gov.au/internet/main/publishing.nsf/Content/ohp-bbvs-sti: accessed December 2014. Australian Government. Canberra)

Pilbara Health Profile 2015
41 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Mental Health, 15-64 years
Youth Suicide, 15-24 years The youth suicide rate in the Pilbara region was similar to the State for both males and females for 2007-2011v. Table 21 shows the youth suicide rates for males and females over a longer period to preserve confidentiality.
The suicide rate for males aged 15-24 years in the Pilbara region was 20.6 per 100,000 and for females was 3.2 per 100,000v.
Table 21: Youth suicide rates by gender, Pilbara re sidents, 15-24 years, 2002-2011
Youth suicides (per 100,000 persons)* Pilbara Health Region
Metro State
(2002 - 2011)Males (15-24 years) 20.6 15.6 19.9
Females (15-24 years) 3.2 5.4 6.0
* These rates have been age-standardised to the Australian 2001 population.
Source: DoH, Health Tracksv
Mental Health, 16 years and over For 2009-2012, HWSS found that one in seven (15%) Pilbara adults aged 16 years and over reported having a current diagnosed mental health problem, with the prevalence nearly twice as high among females than males. However, only six per cent reported having used a mental health care service in the last year. These figures were similar to the Statev.
HWSS also collects information regarding psychological distress and perceived lack of control, which are both related to mental health and can have adverse effects on health. Eight per cent of Pilbara adults reported high or very high psychological distress, while five per cent reported lack of control over their life in general. These figures were similar to the Statev.
While this information is not available for the Pilbara Aboriginal population, nationally the Aboriginal population aged 18 years and over has been found to report higher levels of psychological stress, 2.7 times higher than their non-Aboriginal counterpartsxxvii.
Community Mental Health Activity, 15-64 years For 2008-2012, Pilbara residents aged 15-64 years accessed community mental health services at a significantly lower rate than the State, accounting for 47,203 occasions of service. The leading occasion of service was for serious psychiatric disorders (48%) followed by anxiety disorders (10%).
For 2003-2012, Pilbara Aboriginal residents aged 15-64 years accessed community mental health services three and a half times the rate of non-Aboriginal residentsv
.

Pilbara Health Profile 2015
42 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Mortality, 15-64 years Mortality is an important indicator of the health of the population. Knowledge of the reasons for mortality can help to focus primary and community care services to prevent avoidable mortality.
For 2007-2011, in the Pilbara, the mortality rate for 15-64 year olds was similar to the State rate. The leading cause for 15-64 year olds was ‘Ischaemic heart diseases’. The age group most affected by Ischaemic heart disease deaths is the 45-64 year olds. ‘Transport accidents’ was the next leading cause of death for 15-64 year olds in the Pilbarav.
Alcohol and tobacco related mortality, 15-64 years For 2007-2011 compared with the State, Pilbara residents aged 15-64 years had similar mortality rates due to alcohol consumption (21 per 100,000) and tobacco consumption (22 per 100,000).
For 2002-2011, Aboriginal people had a significantly higher rate for alcohol deaths (102 per 100,000; 8 times) than non-Aboriginal people in the Pilbara, in this age group. The tobacco death rate (107 per 100,000) was also significantly higher (7 times) for Aboriginal people than non-Aboriginal people, in this age groupv.
Avoidable Mortality, 15-64 years Avoidable mortality is defined as deaths before the age of 75 years from conditions which are potentially avoidable given the present health system, available knowledge about social and economic policy impacts and health behaviours. Categories are identified using underlying cause of death ICD–10 codes in the WA cause of death database as defined by the Australian Institute of Health and Welfare, National Healthcare Agreement: PI 20-Potentially avoidable deaths, 2011 and are divided into two categories:
• potentially preventable deaths - those amenable to screening and primary prevention such as immunisation
• deaths from potentially treatable conditions - those amenable to therapeutic interventions.
The rate of avoidable deaths for 15-64 year olds in the Pilbara region was similar to the State rates for both preventable deaths (55 per 100,000) and deaths from treatable conditions (46 per 100,000). The leading causes of avoidable deaths were:
• ischaemic heart disease
• accidental poisonings
• diabetes
• alcohol-related disease, and
• selected invasive bacterial and protozoal infectionv.

Pilbara Health Profile 2015
43 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Health Status of Older People Vaccinations, 65 years and over Annual flu vaccinations and five yearly pneumonia vaccinations are recommended for people aged 65 years and over and are an important primary health intervention.
Influenza vaccinations
For 2011-2013, 54 per cent of Kimberley/Pilbara residents aged 65 years and over, reported having a seasonal influenza vaccination since the 1st March of the year of interview. The influenza vaccination rate for the State was 58 per cent.
Kimberley and Pilbara are combined as there were insufficient numbers in the Pilbara itself to generate meaningful statistics.
Pneumonia vaccinations
For 2009-2013, 38 per cent of Kimberley/Pilbara region residents aged 65 years and over, reported having a pneumonia vaccination in the previous five years. This result was significantly lower than that of the State (47%)xxxi.
Hospitalisations, 65 years and over Pilbara residents aged 65 years and over had 7,835 hospitalisations for 2008-2012. The rate was significantly higher (1.3 times) than the State rate. Half of the hospitalisations for Pilbara residents were for renal dialysis. Other leading causes of hospitalisations for older Pilbara residents that had higher rates than the State were COPD, influenza/pneumonia, injuries to lower limbs and diabetes (Table 22)v.
Table 22: Leading causes of hospitalisation, Pilbar a residents, 65 years and over, 2008-2012
ConditionNumber of
hospitalisations
% all hospitalisations(65yrs and over)
SRR
Dialysis 3,926 50% 3.7COPD 264 3% 3.8Diseases of the eye & adnexa 249 3% 0.6Chemotherapy 158 2% 0.3Influenza & pneumonia 151 2% 3.0Ischaemic heart diseases 112 1% 0.7Arthropathies 112 1% 0.6Injuries to lower limbs 101 1% 1.7Symptoms involving the digestive system & abdomen 95 1% 0.7Diabetes & impaired glucose regulation 93 1% 1.4All hospitalisations (65yrs and over) 7,835 100% 1.3 Notes: The standardised rate ratio (SRR) is the ratio between a particular health region (or district) and the state. A ratio of 1 means that the regional rate is the same as the state, and a value of 2 indicates the regional rate is twice that of the state. A ratio of 0.5 indicates that the rate in a region is half that of the State population.
Local rates are compared to the rate of all residents of the State using the standardised rate ratio (SRR) and the 95% confidence interval of the SRR. Those that are significantly different to the state rate (1.0) are coloured. Those between 1 and 1.5 times the state rate are highlighted orange, higher than 1.5 times the state are highlighted red while those rates significantly less than the state are highlighted green.
Source: DoH, Health Tracksv

Pilbara Health Profile 2015
44 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Potentially Preventable Hospitalisations, 65 years and over For 2008-2012, PPH accounted for 779 hospitalisations of Pilbara people aged 65 years and over (10% of all hospitalisations in older people). The rate of all PPH was significantly higher for Pilbara residents aged 65 years and over (1.3 times) than for the State and for each category (chronic, acute and vaccine preventable)v.
Figure 19 shows the trend between 2008 and 2012 for PPH for Pilbara residents aged 65 years and over. The PPH rate and numbers followed the same trend which was a significant decrease from 2008 to 2010. The rate then increased significantly in 2011 and decreased significantly in 2012. This trend was partly influenced by the change in definition of diabetes complications mentioned in previous sectionsv.
Figure 19: Potentially Preventable Hospitalisations , Pilbara, 65 years and over, 2008 to 2012
0
20
40
60
80
100
120
140
160
180
200
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
2008 2009 2010 2011 2012
num
ber
of P
PH
per
yea
r
AA
R p
er 1
00,0
00 p
erso
n ye
ars
PPH: Pilbara age 65+ trend
N
AAR
The error bars represent the 95% confidence interval of the rate.
Source: DoH, Health Tracks v
Figure 20 compares age-adjusted rates of PPH from 2008 to 2012 for the Pilbara and State by Aboriginality. Aboriginal people aged 65 years and over had significantly higher PPH rates than non-Aboriginal people for both the Pilbara and the Statev.
Pilbara Aboriginal people aged 65 years and over had a significantly higher PPH rate than State Aboriginal people from 2008 to 2011. Pilbara non-Aboriginal people had a significantly lower PPH rate than State non-Aboriginal people between 2008 and 2012 except for 2011 where it was similarv.

Pilbara Health Profile 2015
45 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Figure 20: PPH, Pilbara & State by Aboriginality, 6 5 years and over, 2008 to 2012
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
45,000
50,000
55,000
2008 2009 2010 2011 2012
AA
R p
er 1
00,0
00 p
erso
n ye
ars
PPH, Age adjusted rates, 65 years and over
Pilbara Aboriginal
State Aboriginal
Pilbara Non-Aboriginal
State Non-Aboriginal
The error bars represent the 95% confidence interval of the rate.
Source: DoH, Health Tracksv
For 2003-2012, the PPH rates for Aboriginal people aged 65 years and over for all categories were significantly higher (1.4 times) in Pilbara compared to the State Aboriginal peoplev.
As mentioned earlier, the vaccination rate for influenza in the Kimberley/Pilbara regions was similar to the State during 2011-2013 and the pneumonia vaccination rate was significantly lower than the State rate during 2009-2013xxxi. This is reflected in the PPH rate for influenza and pneumonia in the Pilbara which was three times higher than the State ratev.
The overall leading PPH condition for 2008-2012 for Pilbara people aged 65 years and over was COPD. This accounted for 33 per cent of all PPH in this age group in the Pilbara and was nearly four times the State rate. The next leading PPH condition was diabetes complications at 21 per cent of all PPH in this age group. These rates were significantly higher than the State rates for this age group (Table 23)v.
The PPH rate for COPD in Pilbara residents in this age group fluctuated from 2008 to 2010 and decreased significantly from 2010 to 2012. The change in PPH rate for diabetes complications between 2008 and 2012 is not comparable due to changes in national coding standardsv.
All top five leading conditions for Pilbara residents had rates significantly higher than the State rates for this age group (Table 23)v.

Pilbara Health Profile 2015
46 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Table 23: Leading PPH, Pilbara adults aged 65 years and over, 2008-2012
Condition PPH% all PPH
(65 yrs and over) SRR
COPD (chronic) 257 33% 3.8diabetes complications (chronic) 162 21% 1.4congestive cardiac failure (chronic) 73 9% 1.4pyelonephritis (acute) 72 9% 1.8convulsions and epilepsy (acute) 27 3% 3.1
All PPH (65 yrs and over) 779 100% 1.9 Notes:
The standardised rate ratio (SRR) is the ratio between a particular health region (or district) and the state. A ratio of 1 means that the regional rate is the same as the state, and a value of 2 indicates the regional rate is twice that of the state. A ratio of 0.5 indicates that the rate in a region is half that of the State population.
Local rates are compared to the rate of all residents of the State using the standardised rate ratio (SRR) and the 95% confidence interval of the SRR. Those that are significantly different to the state rate (1.0) are coloured. Those between 1 and 1.5 times the state rate are highlighted orange, higher than 1.5 times the state are highlighted red while those rates significantly less than the state are highlighted green.
Source: DoH, Health Tracksv
Mental Health, older people
Community Mental Health Activity, 65 years and over There were 1,119 occasions of service for Mental Health in those aged 65 years and over in the Pilbara for 2008-2012. The rate of mental health occasions of service for Pilbara was significantly lower than the State ratev.
Implications for primary health care service planni ng: High levels of respiratory hospitalisations in the older age groups suggest a need to ensure influenza and pneumonia vaccinations are available and promoted. Strengthening partnerships with all primary care providers, including local GPs and Aboriginal Medical Services will assist in managing these conditions in the community. The high potentially preventable hospitalisation rates of chronic conditions in the Aboriginal community, often noted at a younger age, may indicate increased frailty, disability and functional decline at a younger than expected age.
There are several HACC services and Home Care Packages (HCP’s) in the Pilbara region which have a significant impact on maintaining the older populations in the community.

Pilbara Health Profile 2015
47 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Disability and Carers In the Pilbara health region, one per cent of residents have a core need for assistance in activities of daily living while four per cent provide unpaid care to a person with a disability. The numbers in each age group are provided in Table 24.
Overall, residents in the Pilbara have a significantly lower proportion of people needing assistance (1%) compared to WACHS (3.5%) however, Pilbara residents aged 65 years and over have a significantly higher proportion of people needing assistance compared to WACHS residents aged 65 years and over (Table 24)xxxii.
Table 24: Pilbara residents with a core need for as sistance, or who provide unpaid care to a person wi th a disability
Have Core Need for
Assistance
% WACHS %
Provide Unpaid Care
% WACHS %
0-14years 104 0.9% 1.6% - - -
15-44 years 142 0.4% 1.3% 1564 4.7% 7.0%
45-64 years 168 1.2% 3.4% 717 5.1% 12%
65-74 years 91 9.9% 7.5% 66 7.2% 11%
Over 75 years 90 37% 25% 12 4.9% 7.3%
All ages 595 1.0% 3.5% 2359 3.9% 7.2%
Source: ABS table builder, Census 2011xxxii
Where Pilbara Residents Accessed Care
General Practice Visits to General Practices not only provide necessary primary care to the population, but offer opportunities for the provision of public health programs, such as vaccinations, and the early intervention and management of chronic conditions.
It can be difficult to access GPs across the Pilbara region particularly in more remote locations. Various mechanisms have been used to increase access including establishment of a S19(2) exemption site at Onslow. These are placed at eligible locations to enable State health providers to access Medicare item numbers. In addition medical outreach into communities is a common method of primary health care service delivery where a resident general practice would not be viable.
There were more than 130,000 GP attendances recorded by Pilbara GP Network in 2012/13, giving a rate of 1,997 per 1,000 people in the area (Table 25). In comparison, the State rate was 3,715 per 1,000 people. This demonstrates the reduced access to GPs within the Pilbara region which can negatively impact on health outcomes.

Pilbara Health Profile 2015
48 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Data by local government area for 2009/10 showed a rate of:
• 3,985 per 1,000 in Port Hedland • 3,569 per 1,000 in Roebourne • 3,420 per 1,000 in East Pilbara • 3,292 per 1,000 in Ashburtonxxxiii.
Table 25: Medicare GP professional attendances, Pil bara Division of General Practice (614), 2012/13
Number Crude Rate /1000 persons
GP Attendances -total 132,429 1,997
$ benefit $5,247,667 $79,153
after hours 1,712 26
Multidisciplinary Care Plans 2,435 37
Health Assessments 2,279 34
Mental Health Care Plans 1,043 16
Source: Medicarexxxiii
(rates based on ABS, ERP 2013)
Emergency Department Attendances Pilbara hospitals
In 2013/14, there were 59,233 Emergency Department (ED) attendances in Pilbara hospitals. Of these attendances, 22 per cent were for patients who were not residents of the regionxxxiv.
In regional areas where workforce shortages and challenges can mean that there are insufficient GPs, many residents use the hospital services for primary care. The ED attendances at hospitals within Pilbara are shown by triage category in Figure 21.
The majority of attendances (74% in 2013/14) were classified as semi or non-urgent (triage 4 or 5), suggesting issues that could be dealt with by GPs and primary health care services. The proportion was significantly higher than WACHS (66%)xxxiv.
Figure 21: Pilbara hospitals emergency attendances by triage category
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
1. Resuscitation 2. Emergency 3. Urgent 4. Semi-urgent 5. Non-urgent
ED
Atte
ndan
ces
Triage Category
2009/10 2010/11 2011/12 2012/13 2013/14
Source: WACHS online ED pivot as at end of October 2014
xxxiv

Pilbara Health Profile 2015
49 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
The top five reasons for ED attendances to hospitals in Pilbara for 2013/14 are shown in Table 26.
Table 26: Leading Cause of Emergency Attendance at hospitals in Pilbara, 2013/14
Major Disease CategoryNumber of ED attendances
% of Total
Musculoskeletal System And Connective Tissue 9,225 16%
Skin, Subcutaneous Tissue And Breast 8,346 14%
Injuries, Poison And Toxic Effect of Drugs 6,494 11%
Ear, Nose, Mouth And Throat 5,723 10%
Digestive System 5,713 10%
Total ED attendances 59,233 100%
Source: WACHS online ED pivot as at end of October 2014xxxiv
Aboriginal people were over-represented in the ED attendances, accounting for 30 per cent of all ED attendances in 2013/14, but only 16 per cent of the populationxxxiv. Also, across the Pilbara there are several Aboriginal Community Controlled Health Organisations (ACCHOs) that provide health services to the Pilbara region.
Pilbara residents
For 2008-2012, the proportion of ED attendances for triage 4 and 5 in the Pilbara was 75 per cent and for the State was 63 per cent. The proportion for triage 4 and triage 5 were significantly higher (2.0 and 3.3 times respectively) than the State proportionsv.
Implications for health care service planning:
Pilbara residents present at high rates to emergency departments, particularly in the semi and non-urgent attendances. The region also sees a high proportion of attendances from non-residents. This is usually an indication of a need for increased primary health services such as increased GP and population health services. Co-location of a range of health services and collaborative service models between GP primary care, non-government health providers (e.g. Silver Chain and Aboriginal organisations) and WACHS population health/primary health services has the potential to reduce the demand for non-urgent attendances at ED.

Pilbara Health Profile 2015
50 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Hospitalisations For 2008-2012, the overall hospitalisation rate of Pilbara residents was significantly higher than that of the State. This was due to the females as they had a rate 1.29 times higher than the State female rate while the male rate was lower than the State male rate (Table 27)v.
Table 27 : Hospitalisations, Pilbara residents, 2008-2012
Number SRR ASR per 100,000 person yearsPilbara
Males 41,108 0.88 32,566
Females 47,769 1.29 53,001
Persons 88,877 1.03 39,914
State
Males 2,115,186 1 37,823
Females 2,309,166 1 39,434
Persons 4,424,352 1 38,317 Notes:
The standardised rate ratio (SRR) is the ratio between a particular health region (or district) and the state. A ratio of 1 means that the regional rate is the same as the state, and a value of 2 indicates the regional rate is twice that of the state. A ratio of 0.5 indicates that the rate in a region is half that of the State population.
Local rates are compared to the rate of all residents of the State using the standardised rate ratio (SRR) and the 95% confidence interval of the SRR. Those that are significantly different to the state rate (1.0) are coloured. Those between 1 and 1.5 times the state rate are highlighted orange, higher than 1.5 times the state are highlighted red while those rates significantly less than the state are highlighted green.
Source: DoH, Health Tracksv
For 2003-2012, the overall hospitalisation rate of Aboriginal Pilbara residents was significantly higher (1.05 times) than the Aboriginal State rate. This rate was also over five times higher than the non-Aboriginal Pilbara rate (Table 28). These higher rates highlight the health disparity of residents in the Pilbara compared with those living elsewhere in the State and in particular, the disparity between Aboriginal and non-Aboriginal residentsv.
Table 28 : Hospitalisations, Pilbara Aboriginal and non-Aborig inal residents
Number SRRASR per 100,000 person
years
Pilbara
Aboriginals 71,806 1.05 120,785Non-Aboriginals 83,977 0.67 23,347
Source: DoH, Health Tracksv
Across the State for 2008-2012, renal dialysis accounted for 574,963 separations (13% of total separations). Pilbara residents had 20,977 separations for renal dialysis (24% of the total). Leading conditions after renal dialysis were delivery, injuries to upper limbs, injuries to head and neck, symptoms of digestive system, skin infections and arthropathies, each accounting for around two per cent of separationsv.
The leading cause of hospitalisation differs markedly between Aboriginal and non-Aboriginal Pilbara residents. Dialysis accounts for nearly half the hospitalisations of Aboriginal Pilbara residents for 2003-2012 (47%)v.

Pilbara Health Profile 2015
51 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
For non-Aboriginal Pilbara residents, dialysis hospitalisations were around three per cent for 2008-2012. The period stated for Aboriginal people in the Pilbara is longer to provide more accurate datav.
The top five causes of hospitalisation by major category for 2008-2012 are shown in Table 29. The leading cause of hospitalisation for Pilbara residents was ‘injury and poisoning’, (which can include transport accidents, other external accidental injuries, intentional self-harm, assault, and complications of medical and surgical care). These accounted for nine per cent of hospitalisations. This was followed by pregnancy and childbirth (9%)v.
Table 29: Leading cause of hospitalisation, Pilbara residents, 2008-2012
Rank Cause of Hospitalisation Number % of Total State R ank1 Injury and Poisoning 8,411 9% 42 Pregnancy and childbirth 7,889 9% 63 Digestive diseases 7,522 8% 14 Respiratory diseases 5,288 6% 95 Ill-defined conditions 4,946 6% 3
All hospitalisations 88,877 100% Note: Leading causes exclude ‘Factors influencing health status’ and ‘contact with health services’ and ‘attending health services for examination and investigation’, reproduction, specific procedures, and other circumstances, and potential health hazards related to communicable diseases, socioeconomic and psychosocial circumstances, family and personal history. This also includes renal dialysis.
Source: DoH, Health Tracksv
Alcohol and tobacco related hospitalisations For 2008-2012, Pilbara residents had significantly higher hospitalisation rates due to alcohol and tobacco consumption (1.4 times each), compared with the State. The hospitalisation rate due to tobacco consumption for Pilbara Aboriginal residents was higher (1.2 times) than the State while the rate for alcohol-related hospitalisations was similar to the State (for 2003-2012)v
.
For 2003-2012, the rate of alcohol-caused hospitalisations for Aboriginal Pilbara residents was significantly higher (7 times) than the non-Aboriginal Pilbara rate. The rate of tobacco-caused hospitalisations for Aboriginal Pilbara residents was significantly higher (4 times) than the non-Aboriginal ratev
.
Potentially preventable hospitalisations Many hospitalisations result from conditions where hospitalisations could potentially be avoided using preventive care and early disease management. These hospitalisations are known as Potentially Preventable Hospitalisations (PPH) and are grouped into three major categories as discussed in ‘Health Status - Child and Adolescent’ section.
For 2008-2012, PPH accounted for 6,844 hospitalisations of Pilbara residents (8% of all hospitalisations). The PPH rate for Pilbara residents was significantly higher (1.4 times) than the State rate. PPH rates for each category were significantly higher than the State (acute 1.2 times, chronic 1.7 times, vaccine preventable 2 times)v.
The leading PPH condition for Pilbara residents was diabetes complications, which accounted for 18 per cent of PPH. Other conditions are shown in Figure 22. All of these conditions apart from dental have rates significantly higher than the State rates, with diabetes complication rates 1.9 times higherv.

Pilbara Health Profile 2015
52 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Figure 22: Pilbara residents leading potentially pr eventable hospitalisations, 2008-2012
730
446
359
280
111
315
224
141
162
536
439
385
341
486
234
264
157
130
diabetes complications
dental conditions
ENT infections
asthma
pyelonephritis
convulsions and epilepsy
chronic obstructive pulmonary disease
influenza and pneumonia
congestive cardiac failure
Males Females
Source: DoH, Health Tracks
v
Most leading conditions were the same for both Aboriginal people and non-Aboriginal people in the Pilbara, however in a different order (Table 30 & Table 31). For non-Aboriginal people (for 2008-2012), the leading condition was ‘dental conditions’ accounting for 19% of all PPH and for Aboriginal people (for 2003-2012), the leading condition was diabetes complications (25%)v.
Most of the PPH rates for leading conditions for non-Aboriginal people were similar or lower than State non-Aboriginal rates. Asthma, COPD and influenza/pneumonia had significantly higher PPH rates than the State non-Aboriginal people (Table 30). For Aboriginal people in the Pilbara, most leading conditions were higher than State Aboriginal rates (for 2003-2012) (Table 31)v.
Table 30: Leading causes of PPH of Pilbara non-Abor iginal residents, 2008-2012
Condition Number % all PPH SRR
dental conditions (acute) 632 19% 0.8
diabetes complications (chronic) 476 14% 1.0
ENT infections (acute) 445 13% 1.1
asthma (chronic) 328 10% 1.2
pyelonephritis (acute) 288 9% 0.8
COPD (chronic) 216 6% 1.5
convulsions and epilepsy (acute) 188 6% 0.7
influenza and pneumonia (vaccine) 133 4% 1.4
iron deficiency anaemia (chronic) 102 3% 0.5
dehydration and gaestroenteritis (acute) 87 3% 0.8
All PPH 3,341 100% 0.9

Pilbara Health Profile 2015
53 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Table 31: Leading causes of PPH of Pilbara Aboriginal residen ts, 2003-2012
Condition Number % all PPH SRR
diabetes complications (chronic) 1,673 25% 1.2convulsions and epilepsy (acute) 757 11% 0.9COPD (chronic) 567 8% 1.3pyelonephritis (acute) 556 8% 1.2asthma (chronic) 536 8% 1.2
ENT infections (acute) 508 8% 1.0congestive cardiac failure (chronic) 431 6% 1.3
dental conditions (acute) 430 6% 1.0
influenza and pneumonia (vaccine) 311 5% 1.2cellulitis (acute) 202 3% 1.3
All PPH 6,771 100% 1.1
Notes:
The standardised rate ratio (SRR) is the ratio between a particular health region (or district) and the state. A ratio of 1 means that the regional rate is the same as the state, and a value of 2 indicates the regional rate is twice that of the state. A ratio of 0.5 indicates that the rate in a region is half that of the State population.
Local rates are compared to the rate of all residents of the State using the standardised rate ratio (SRR) and the 95% confidence interval of the SRR. Those that are significantly different to the state rate (1.0) are coloured. Those between 1 and 1.5 times the state rate are highlighted orange, higher than 1.5 times the state are highlighted red while those rates significantly less than the state are highlighted green.
Source: DoH, Health Tracksv
Where Pilbara residents used hospital services Pilbara residents were seen in hospitals across the State. The proportion of resident hospitalisations in public hospitals that occur within the region is known as self-sufficiency. The Pilbara public self-sufficiency was 78 per cent. The WACHS average was 75 per cent (Table 32)xxxv.
Table 32: Place of hospitalisation, Pilbara residen ts, 2013/14
Place of HospitalisationNumber of
Hospitalisations % of total Beddays
Karratha 2,970 18% 5,300
Newman 655 3.9% 954
Onslow 294 1.8% 534
Paraburdoo 57 0.3% 60
Port Hedland 8,677 52% 13,126
Roebourne 137 0.8% 307
Tom Price 261 1.6% 450
Pilbara Total 13,051 78% 20,731
Other WACHS 210 1.3% 839
Royal Perth Hospital 1,430 8.6% 5,676
Sir Charles Gairdner Hospital 444 2.7% 2,267
Other Metropolitan 1,518 9.1% 6,855
Total 16,653 100% 36,368 Note: Excludes unqualified neonates and boarders
Source: HMDSxxxv

Pilbara Health Profile 2015
54 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Hospitalisations within the region Historic activity at hospitals within the Pilbara region is shown in Figure 23. Between 2011/12 and 2014/15, hospital separations decreased at an average of one per cent per year. Total bed days decreased over the period, by an annual average of two per cent.
The proportion of activity for non-residents of the region in 2014/15 was 9%. For the three years prior, it was between 10 per cent and 12 per cent.
Figure 23: Hospitalisations within the Pilbara regi on, 2011/12 to 2014/15
0
5,000
10,000
15,000
20,000
25,000
30,000
2011/12 2012/13 2013/14 2014/15
Number
Financial Year
Separations Beddays
Note: Excludes unqualified neonates and boarders
Source: HMDSxxxvi
Implications for health care service planning:
Aboriginal Pilbara residents have a much greater need for ED and inpatient services than non-Aboriginal residents therefore culturally appropriate services and programs are necessary in partnership with ACCHOs and other providers. An increase in the GP sector, combined with co-located and collaborative service models between GP primary care, other non-government health providers (e.g. Silver Chain and Aboriginal organisations) and WACHS ED and population health/primary health services are strongly recommended.

Pilbara Health Profile 2015
55 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Mortality
Mortality is an important indicator of the health of the population. Knowledge of the reasons for mortality can help to focus primary and community care services to prevent avoidable mortality.
State level ABS data from 2011 to 2013 shows life expectancy at birth has increased for the total population to 80.3 years for males and 84.8 years for femalesxxxvii, compared with the 2008 to 2010 figures of 79.7 years and 84.3 years respectivelyxxxviii.
Aboriginal people in Western Australia have a significantly lower life expectancy compared with their non-Aboriginal counterparts. The gap in 2010-2012 was estimated by ABS to be 15.1 years for males and 13.5 years for females (Figure 22)xxxix.
Figure 24: Western Australian life expectancy at bi rth by Aboriginality, 2010-2012
65.0 70.2
80.1 83.7
0
10
20
30
40
50
60
70
80
90
Males Females
Age Aboriginal Non-Aboriginal
Source: ABS Life Tablesxxxix
Death rates have fallen state-wide and in Australia overall from 2003 to 2013. The Australian Aboriginal death rate however, remained steady during this 10-year period (Table 33)xl.
Table 33: Australian standardised death rates, 2003 , 2012, 2013
Population 2003 2012 2013
Western Australia 6.3 5.4 5.2
Australia 6.5 5.5 5.4
Aboriginal (Australia) 10.1 9.8 10.0
Note: Deaths per 1,000 standard population. Standardised death rates use the age distribution of total persons in the Australian population at 30 June 2001 as the standard population.
Source: ABS Deathsxl

Pilbara Health Profile 2015
56 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
When considering mortality within a region, a longer time period is required to ensure anonymity and accuracy.
For 2007-2011, there were 535 deaths for Pilbara residents. The region’s mortality rate was significantly higher (1.1 times) than that of the State. The top five causes of mortality for 2007-2011 are shown in Table 34. For this period, the leading cause of death of Pilbara residents was ischaemic heart disease which had a rate similar to the State. The next leading cause was transport accidents which was significantly higher (1.8 times) than the State rate. Diabetes and unknown causes both had rates significantly higher (around 4 times) than the State ratesv.
Table 34: Leading cause of mortality, Pilbara resid ents, 2007-2011
Rank ConditionNumber of
deaths% all deaths SRR
1 Ischaemic heart diseases 62 12% 1.2
2 Transport accidents 50 9% 1.8
3 Diabetes & impaired glucose regulation 40 7% 3.5
4 Unknown causes of morbidity & mortality 35 7% 4.4
5 Cerebrovascular diseases 25 5% 1.5
All deaths 535 100% 1.1 Notes:
The standardised rate ratio (SRR) is the ratio between a particular health region (or district) and the state. A ratio of 1 means that the regional rate is the same as the state, and a value of 2 indicates the regional rate is twice that of the state. A ratio of 0.5 indicates that the rate in a region is half that of the State population.
Local rates are compared to the rate of all residents of the State using the standardised rate ratio (SRR) and the 95% confidence interval of the SRR. Those that are significantly different to the state rate (1.0) are coloured. Those between 1 and 1.5 times the state rate are highlighted orange, higher than 1.5 times the state are highlighted red while those rates significantly less than the state are highlighted green.
Source: DoH, Health Tracksv
For 2002-2011, there were 1,211 deaths for Aboriginal Pilbara residents. The Aboriginal Pilbara mortality rate was significantly higher compared to the State. The five leading causes of mortality for Aboriginal Pilbara residents were ischaemic heart disease (IHD), diabetes and impaired glucose regulation, transport accidents, cerebrovascular diseases and unknown causes. These death rates were significantly higher than the State except for IHD and cerebrovascular diseases which were similar to the State ratesv.
Over the 2007-2011 period, the five leading causes for non-Aboriginal residents were IHD, transport accidents, lung cancer, intentional self-harm and CVD. These deaths rates were similar to the State except for intentional self-harm which was significantly lower than the Statev.
Alcohol and tobacco related mortality For 2007-2011, the mortality rate due to alcohol consumption in Pilbara residents was 27 per 100,000 and tobacco consumption was 94 per 100,000. These rates were similar to State rates.
The mortality rates for alcohol and tobacco consumption were also similar to the State for Aboriginal residents in the Pilbara (for 2002-2011). However, Aboriginal Pilbara residents had significantly higher mortality rates for both alcohol (4.4 times) and tobacco consumption (2.5 times) compared with non-Aboriginal Pilbara residentsv.

Pilbara Health Profile 2015
57 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Avoidable Mortality, 0-74 years Avoidable mortality is defined as deaths before the age of 75 years from conditions which are potentially avoidable given the present health system, available knowledge about social and economic policy impacts and health behaviours, as described in ‘Avoidable Mortality, 15-64 years’ section.
For 2007-2011, over half (56%) of the Pilbara resident deaths under the age of 75 years were classified as avoidable, and the rate was significantly higher than the State. The use of screening and primary prevention could potentially have avoided over half of avoidable deaths in Pilbara residents and better treatment measures could potentially have avoided just under half of avoidable deaths (Table 35)v.
Table 35: Avoidable mortality before the age of 75 years, Pilbara residents, 2007-2011
Condition Number% of all deaths
(<75yrs)SRR
Treatable 115 25% 1.3Preventable 143 31% 1.2All avoidable deaths (<75yrs) 257 56% 1.2All deaths (<75yrs) 455 100% 1.2
Notes:
The standardised rate ratio (SRR) is the ratio between a particular health region (or district) and the state. A ratio of 1 means that the regional rate is the same as the state, and a value of 2 indicates the regional rate is twice that of the state. A ratio of 0.5 indicates that the rate in a region is half that of the State population.
Local rates are compared to the rate of all residents of the State using the standardised rate ratio (SRR) and the 95% confidence interval of the SRR. Those that are significantly different to the state rate (1.0) are coloured. Those between 1 and 1.5 times the state rate are highlighted orange, higher than 1.5 times the state are highlighted red while those rates significantly less than the state are highlighted green.
Source: DoH, Health Tracksv
The higher rate in the Pilbara region can be attributed to a higher Aboriginal population. The rates for treatable and preventable avoidable deaths for Aboriginal people in the Pilbara were significantly higher than in Pilbara non-Aboriginal people (7 and 5 times respectively) (Table 36)v. Table 36: Avoidable mortality before the age of 75 years, Pilbara residents by Aboriginality, 2002-201 1
Number AAR* Number AAR*
Treatable 131 309.1 87 41.3
Preventable 153 368.4 137 81.5
All avoidable deaths(<75yrs)
284 677.4 223 122.9
Aboriginal Non-Aboriginal
*AARs are standardised with the Australian 2001 population and expressed per 100,000 person years.
Source: DoH, Health Tracksv
The leading cause of avoidable mortality for Aboriginal Pilbara residents for 2002-2011, was ischaemic heart disease, which accounted for one in seven deaths (14%), followed by diabetes (10%).
The leading cause of avoidable mortality for non-Aboriginal Pilbara residents was ischaemic heart disease (14%), followed by lung cancer (6%), for 2007-2011 (Table 37)v.

Pilbara Health Profile 2015
58 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Table 37: Leading cause of avoidable mortality by A boriginal status, Pilbara residents, 0-74 years
Aboriginal, 2002-2011 Number% of all deaths
(<75yrs)SRR
ischaemic heart disease (preventable proportion) 33 7% 1.1
ischaemic heart disease (treatable proportion) 33 7% 1.1
diabetes (preventable proportion) 24 5% 1.3
diabetes (treatable proportion) 24 5% 1.3
alcohol related disease (preventable) 17 3% 0.9
nephritis and nephrosis (treatable) 17 3% 1.5
selected invasive bacterial and protozoal infection (treatable) 16 3% 1.1
lung cancer (preventable) 11 2% 0.9
road traffic injuries, other transport injuries (preventable) 11 2% 1.8
All avoidable deaths (<75yrs) 284 57% 1.1
All deaths (<75yrs) 501 100% 1.2
Non-Aboriginal, 2007-2011 Number% of all deaths
(<75yrs)SRR
ischaemic heart disease (preventable proportion) 15 7% 1.1
ischaemic heart disease (treatable proportion) 15 7% 1.1
lung cancer (preventable) 12 6% 0.6
accidental poisonings (preventable) 8 4% 0.6
breast cancer (females only) (treatable) 7 3% 0.6
alcohol related disease (preventable) 5 2% 0.9
melanoma of skin (treatable) 5 2% 0.9
All avoidable deaths (<75yrs) 120 59% 0.8All deaths (<75yrs) 204 100% 0.7
Persons, 2007-2011 Number % of all deaths (<75yrs)
SRR
ischaemic heart disease (preventable proportion) 29 6% 1.5
ischaemic heart disease (treatable proportion) 29 6% 1.5
lung cancer (preventable) 18 4% 0.8
diabetes (preventable proportion) 17 4% 3.8
diabetes (treatable proportion) 17 4% 3.8
alcohol related disease (preventable) 11 2% 1.3
nephritis and nephrosis (treatable) 11 2% 3.7
All avoidable deaths (<75yrs) 257 56% 1.2
All deaths (<75yrs) 455 100% 1.2 Notes:
The period stated in this table for Aboriginal people is longer than the other populations to provide more accurate data.
The standardised rate ratio (SRR) is the ratio between a particular health region (or district) and the state. A ratio of 1 means that the regional rate is the same as the state, and a value of 2 indicates the regional rate is twice that of the state. A ratio of 0.5 indicates that the rate in a region is half that of the State population.
Local rates are compared to the rate of all residents of the State using the standardised rate ratio (SRR) and the 95% confidence interval of the SRR. Those that are significantly different to the state rate (1.0) are coloured. Those between 1 and 1.5 times the state rate are highlighted orange, higher than 1.5 times the state are highlighted red while those rates significantly less than the state are highlighted green.
Source: DoH, Health Tracksv

Pilbara Health Profile 2015
59 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Implications for health care service planning: Just over half of the deaths of Pilbara residents under the age of 75 years were classified as avoidable. Ischaemic heart disease, diabetes, lung cancer and alcohol-related disease were leading causes of avoidable mortality. As the majority of deaths from these conditions are avoidable through the use of primary and secondary interventions such as public health programs and screening, greater focus on these interventions in the Pilbara will improve health and wellbeing. In particular, smoking, physical inactivity, excess weight, excess alcohol use and poor diet are modifiable risk factors for these conditions. Aboriginal Pilbara residents had a significantly higher proportion of deaths classified as avoidable compared with non-Aboriginal residents and there were differences in the causes of death. Diabetes was a leading cause only for Aboriginal residents, highlighting the need for targeted, culturally appropriate programs and services.

Pilbara Health Profile 2015
60 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
Glossary ABS Australian Bureau of Statistics
ACCHO Aboriginal Community Controlled Health Organisations
AEDC Australian Early Development Census
ARIA Accessibility/Remoteness Index of Australia
ASR Age-standardised rate
ATSIC Aboriginal and Torres Strait Islander Commission
CI 95% Confidence Interval of a rate or proportion
DoH Department of Health WA
ENT Ear, nose and throat infections
ERP Estimated Residential Population
GDM Gestational Diabetes Mellitus
HMDS Hospital Morbidity Data System
HWSS Health and Wellbeing Surveillance System
LGA Local Government Area
PPH Potentially Preventable Hospitalisations
SA1 Statistical Area Level 1
SEIFA Socio-Economic Indexes for Areas
STI Sexually transmitted infections
SRR Standardised rate ratio
WA Tomorrow, 2012 Department of Planning Population Projections from 2006 Census
WACHS Western Australia Country Health Service
WASG Western Australia State Government
WASGPP Western Australia State Government Population Projections

Pilbara Health Profile 2015
61 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
References i WACHS Pilbara internet, http://www.wacountry.health.wa.gov.au/index.php?id=494, (accessed July 21, 2015) ii Department of Health Australia, 2001.Measuring Remoteness: Accessibilty/Remoteness Index of Australia (ARIA) iii Department of Health WA, Epidemiology Geographic Information System branch, 2015 iv Australian Bureau of Statistics (ABS), 3235.0 Population by Age and Sex, Regions of Australia v Department of Health WA, Health Tracks - Epidemiology Branch (PHI) in collaboration with the Cooperative Research Centre for Spatial Information (CRC-SI) vi Department of Health WA, Rates Calculator - Epidemiology Branch (PHI) based on ABS ERP 2011 vii ABS 2013, 3222.0 - Population Projections, Australia, 2012 (base) to 2101 viii Radomiljac, Ali and Joyce, Sarah 2014. Health and Wellbeing of Adults in Western Australia 2013, Overview and Trends. Department of Health, Western Australia ix ABS, 2008 Socio-Economic Indexes for Areas (SEIFA) - Technical Paper, 2006. Cat No. 2039.0.55.001
x ABS, Census of Population and Housing: Socio-Economic Indexes for Areas (SEIFA), Australia, 2011 (cat. no. 2033.0.55.001). xi ABS, 2901.0 - Census Dictionary, 2011. xii Public Health Information Development Unit (PHIDU). http://www.adelaide.edu.au/phidu/maps-data/data/ xiii WACHS Online data – Obstetric Deliveries (HCARe, webPAS & TOPAS via Data Extracts) xiv Midwives Notification System (via WACHS Safety, Quality and Performance)
xv Australian Institute of Health and Welfare 2012. A picture of Australia’s children 2012. Cat. no. PHE 167. Canberra: AIHW. xvi Raewyn CM, Watkins R and Bower C, 2014. Fetal alcohol spectrum disorders: Notifications to the Western Australian Register of Developmental Anomalies. Journal of Paediatrics and Child Health. doi: 10.1111/jpc.12746. xvii Australian Indigenous Alcohol and Other Drugs Knowledge Centre at http://www.aodknowledgecentre.net.au/aodkc/alcohol/fasd/fasd-key-facts#_ENREF_17 accessed December 2014. Australian Indigenous HealthInfoNet. Australian Government Department of Health. xviii Institute of Child Health Research, Western Australia Aboriginal Child Health Survey 2001. Western Desert (Warburton) ATSIC Regional Profile, Volume 1: The Health of Aboriginal Children and Young People. (Zubrick SR, Lawrence DM, Silburn SR, Blair E, Milroy H, Wilkes T, Eades S, D'Antoine H, Read A, Ishiguchi P and Doyle S, 2004. The Western Australian Aboriginal Child Health Survey: The Health of Aboriginal Children and Young People, Telethon Institute for Child Health Research, Perth). xix Cameron CM, Davey T, Kendall E, Wilson A, McCLure RJ. Changes in alcohol consumption in pregnant Australian women between 2007 and 2011. Medical Journal of Australia, 2013. Vol 199:Iss 5 p355-7. xx AIHW 2010. Diabetes in pregnancy: its impact on Australian women and their babies. Diabetes series no. 14. Cat. no. CVD 52. Canberra: AIHW. Viewed 23 December 2014. http://www.aihw.gov.au/publication-detail/?id=6442472448. xxi Hilder L, Zhichao Z, Parker M, Jahan S, Chambers GM 2014. Australia’s mothers and babies 2012. Perinatal statistics series no. 30. Cat. no. PER 69. Canberra: AIHW.

Pilbara Health Profile 2015
62 ONCE PRINTED THIS DOCUMENT MAY BECOME OUT OF DATE Trim Record No: ED-CO-15-51706 REFER TO THE ONLINE SOURCE FOR THE CURRENT VERSION
xxii Australian Early Development Census, 2012 http://www.aedc.gov.au/ xxiii 4813.0.55.001 - Occasional Paper: Vaccination Coverage in Australian Children - ABS Statistics and the Australian Childhood Immunisation Register (ACIR), 2001
xxiv Australian Childhood Immunisation Register - Coverage Report. Communicable Disease Control Branch, Department of Health, Western Australia.
xxv Immunise Australia Program website, Department of Health, Australian Government, accessed July 29, 2015. http://www.immunise.health.gov.au/internet/immunise/publishing.nsf/Content/acir-ann-cov-hist-data.htm http://www.immunise.health.gov.au/internet/immunise/publishing.nsf/Content/acir-ann-hist-data-ATSI-child.htm xxvi Epidemiology Branch, 2014, WA Country Health Region Child Health Profiles, HWSS 2008-2013, WA Department of Health: Perth. xxvii ABS, 2013. Australian Aboriginal and Torres Strait Islander Health Survey: First Results, Australia, 2012-13 cat. no. 4727.0.55.001 http://www.abs.gov.au/ausstats/[email protected]/Lookup/4727.0.55.001main+features12012-13 xxviii Radomiljac, Ali and Joyce, Sarah 2014. Health and Wellbeing of Adults in Western Australia 2013, Overview and Trends. Department of Health, Western Australia xxix The Epidemiology of Notifiable Sexually Transmitted Infections and Blood-Borne Viruses in Western Australia 2012. Communicable Disease Control Directorate, Department of Health, Western Australia. xxx Australian Institute of Health and Welfare 2014. Australia’s health 2014. Australia’s health series no.14. Cat. no. AUS 178. Canberra: AIHW. xxxi Epidemiology Branch, 2014, Pneumonia and Flu Vaccination Prevalence by Health Region, HWSS 2009-2013, WA Department of Health: Perth. xxxii ABS, Census 2011 via Table Builder xxxiii Medicare Australia, 2010. Divisions of General Practice Statistics Reports http://medicarestatistics.humanservices.gov.au/statistics/div_gen_prac.jsp xxxiv WACHS Online ED pivot xxxv Hospital Morbidity Data System (HMDS, Inpatient pivot 2008/09 to 2013/14), accessed Nov 2014 xxxvi Hospital Morbidity Data System (Inpatient Separation Details as at end July 2015 (2010/11 to 2014/15 YTD)) xxxvii ABS 3302.0.55.001 - Life Tables, States, Territories and Australia, 2011-2013 xxxviii ABS 3302.5.55.001 - Life Tables, Western Australia, 2008-2010 xxxix ABS, 2013. Life tables for Aboriginal and Torres Strait Islander Australians, 2010–2012. ABS cat. no. 3302.0.55.003. Canberra: ABS. xl ABS 3302.0 - Deaths, Australia, 2013