Embed Size (px)
Citation preview

ARTICLE IN PRESS
PIN ARTHRODESIS OF THE WRIST –
A MODIFIED TECHNIQUEK. KUMAR and Q. G. N. COX
From the Department of Orthopaedics, Raigmore Hospital, Inverness IV2 3UJ, UK
An intramedullary pin is commonly used for wrist arthrodesis in patients with rheumatoid arthritis.
However, pin migration is a recognized complication of this technique. We report the results ofwrist fusion in 15 patients using a modified technique with a transverse blocking screw inserted intothe metacarpal distal to the intramedullary pin to prevent distal migration and backing out of theintramedullary pin. The procedure is simple to perform, does not add significantly to the operatingtime and has not been associated with any complications.Journal of Hand Surgery (British and European Volume, 2005) 30B: 5: 461–463Keywords: wrist, arthrodesis, closed, intramedullary pin
INTRODUCTION
Wrist arthrodesis, using a variety of techniques, is arecognized procedure for the management of therheumatoid wrist, aiming to provide a stable, pain freejoint. Use of an intramedullary pin was first describedby Clayton (1965) and has subsequently been modified(Mannerfelt and Malmsten, 1971; Millender and Nale-buff, 1973; Stanley et al. (1986). Intramedullary rod orpin techniques have the advantage of decreased opera-tive time, simplicity of technique and lower cost.However, distal pin migration (Fig 1) is a recognizedcomplication of this technique and may necessitatesecondary operative procedures.In this paper, we describe the results of wrist fusion
using a modified technique to prevent distal pinmigration.
Fig 1 Radiograph showing distal migration of the intramedullary pin.
PATIENTS AND METHODS
Between 2000 and 2002, 15 patients with establishedrheumatoid arthritis of the wrist underwent wrist fusion.There were 10 women and 5 men, with a mean age of 57(range 40–68) years. The right wrist was fused in ninepatients and the left in six. In 14 patients, closed wristarthrodesis was performed using our modification of theoriginal technique described by Clayton. A Stanley pinwas used in all the cases (Stanley et al., 1986). In the firstpatient, the original technique was used but the pinbacked out. The patient needed a secondary procedure,in which the modified technique was used. In thispatient, two screws were used. Subsequently, only onescrew has been used. In all the cases, excision of thedistal ulna was performed concomitantly for rheuma-toid disease of the distal radioulnar joint.
Surgical technique
The wrist is placed in a neutral position with the forearmin pronation. A longitudinal incision is made over the
461
metacarpophalangeal joint of the middle or, occasion-ally, the index finger. A Stanley pin 3 or 4mm indiameter and an appropriate length (90–150mm) isintroduced through the head of the metacarpal. Underfluoroscopic control, the pin is advanced through themetacarpal across the carpus and into the radius untilthe distal end is finally seated in the isthmus of themetacarpal. The wrist joint is not opened routinely.

ARTICLE IN PRESS
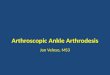
Fig 2 Postoperative radiograph showing a blocking screw distal to the
intramedullary pin.
Fig 3 Radiograph showing an intramedullary pin which has migrated
distally and is abutting against the blocking screw.
THE JOURNAL OF HAND SURGERY VOL. 30B No. 5 OCTOBER 2005462
A 2.0mm cortical screw is inserted transversely acrossthe metacarpal shaft distal to the Stanley pin (Fig 2).Postoperatively, the wrist is immobilized in a cast for 6weeks.
RESULTS
All patients had satisfactory relief of pain and clinicalstability at the time of plaster removal. Patients werefollowed up for a mean of 6.5 (range 4–10) months. Thesymptoms continued to improve at the most recentreview. Wrists were not routinely radiographed after 6weeks and we do not feel that bony arthrodesis isessential for a satisfactory clinical result. There were noinfections and none of the implants had to be removed.One patient complained of discomfort from the screwhead, but this did not necessitate the removal of thescrew.
DISCUSSION
Use of an intramedullary pin was first described in 1965by Clayton, who used a Steinmann pin. Mannerfelt and
Malmsten (1971) described a technique using Rush pins.More recently, Stanley and his colleagues modified theoriginal Clayton technique and modified some of theinstrumentation for pin insertion (Stanley et al., 1986).The use of an intramedullary pin for wrist fusion has
been associated with distal migration of the pin causingpain and necessitating its removal. In a series of 60patients, Millender and Nalebuff (1973) experienced 12distal migrations of the pin requiring subsequentremoval of the pin. Stanley et al. (1986) reported aseries of 71 wrist arthrodeses in 66 patients with hismodified pin and instruments, but no complicationswere reported. Christodoulou et al. (1999) reporteddistal migration of the pin in four of 22 wrist fusions.Feldon et al. (1993) recommend tapping cancellous boneinto the medullary canal prior to introducing the pin toprevent it from backing out.We feel that our technique of inserting a transverse
screw distal to the intramedullary pin produces a definitemechanical block that prevents any migration of the pin,as observed in a case when this technique was not used.

ARTICLE IN PRESS
PIN ARTHRODESIS OF THE WRIST 463
Standard wrist fusion using an intramedullary Stanleypin was performed. However, the pin backed out. It wasreinserted and two 2.0mm blocking screws were insertedin the metacarpal distal to the pin. Subsequent radio-graphs showed that the pin had migrated distally again,but any further migration was prevented by the blockingscrew (Fig 3). We have found that, on average, it addsabout 10min to the surgical time. Use of the transversescrew has not been associated with any significantcomplication. One patient had slight discomfort fromthe screw. In subsequent patients, we have inserted thescrew as transversely as possible to minimize the screwhead prominence on the dorsum of the hand.In patients requiring subsequent implant arthroplasty
of the metacarpophalangeal joints the screw can beremoved without any difficulty.
References
Christodoulou L, Patwardhan MS, Burke FD (1999). Open and closedarthrodesis of rheumatoid wrist using a modified (Stanley)Steinmann pin. The Journal of Hand Surgery, 24B: 662–666.
Clayton ML (1965). Surgical treatment at the wrist in rheumatoidarthritis. Journal of Bone and Joint Surgery, 47A: 741–750.
Feldon PG, Millender LH, Nalebuff EA. Rheumatoid arthritis. In:Green DP (Ed.), Operative Hand Surgery, New York, ChurchillLivingstone, 1993, Vol. 2: 1587–1690.
Mannerfelt L, Malmsten M (1971). Arthrodesis of the wrist inrheumatoid arthritis. A technique without external fixation.Scandinavian Journal of Plastic and Reconstructive Surgery, 5:124–130.
Millender LH, Nalebuff EA (1973). Arthrodesis of the rheumatoidwrist. Journal of Bone and Joint Surgery, 55A: 1026–1034.
Stanley JK, Gupta SR, Hullin MG (1986). Modified instruments forwrist fusion. The Journal of Hand Surgery, 11B: 245–249.
Received: 24 June 2004Accepted after revision: 3 May 2005Mr K. Kumar, 9 Edgehill Road, Aberdeen, AB15 5JG, UK. Tel.: +44 7876196523.E-mail: [email protected]
r 2005 The British Society for Surgery of the Hand. Published by Elsevier Ltd. All rightsreserved.doi:10.1016/j.jhsb.2005.05.001 available online at http://www.sciencedirect.com