Embed Size (px)
Citation preview

ANTIMICROBLAL AGENTS AND CHEMOTHERAPY, Dec. 1978, p. 829-8370066-4804/78/0014-0829$02.00/0Copyright © 1978 American Society for Microbiology
Vol. 14, No. 6
Printed in U.S.A.
Piperacillin: Human Pharinacokinetics After Intravenous andIntramuscular Administration
T. B. TJANDRAMAGA,l* A. MULLIE,' R. VERBESSELT,' P. J. DE SCHEPPER,' AND L. VERBIST2Division of Clinical Pharmacology, Department ofPharmacology and Medicine,' and Department ofBacteriology,2 Academic Hospitat St. Rafael, Katholieke Universiteit Leuven, B-3000 Leuven, Belgium
Received for publication 21 September 1978
The phannacokinetics of piperacillin were studied in a total of 26 Caucasiannormal male volunteers. Single intramuscular doses of 0.5, 1.0, and 2.0 g weregiven to three groups, each containing eight volunteers. Mean peak serumconcentrations of 4.9, 13.3, and 30.2 jig/ml were assayed at 30 to 50 min, andmeasurable levels were present up to 4, 6, and 8 h, respectively, after dosing.Single intravenous bolus doses of 1.0, 2.0, 4.0, and 6.0 g were given to four groupsof five subjects, and mean serum concentrations of 70.7, 199.5, 330.7, and 451.8,jg/ml were measured at the end of the injections. The antibiotic had a meanterminal serum half-life of 60 to 80 min after the intramuscular doses and 36 to 63min after intravenous administrations, depending on the dose. The apparentdistribution volume was 20 to 24 liters/1.73 m2, and distribution volume at steadystate was 16 to 19 liters/1.73 M2. Mean urinary recovery in 24 h was 74 to 89% forthe intravenous doses and 57 to 59% for the intramuscular doses. The piperacillin-creatinine clearance ratios indicated that the proportion of renal excretion ofpiperacillin through tubular secretion was 56 to 73%, and this was confirmed bythe renal clearance data from eight volunteers receiving probenecid treatmentbefore the piperacillin dose. Probenecid (1 g given orally before administration ofpiperacillin) increased peak serum concentration by 30%, terminal serum half-lifeby 30%, and the area under the plasma concentration curve by 60%, and itdecreased the apparent distribution volume by 20% and the renal clearance of theintramuscularly administered (1 g) antibiotic by 40%. Injections of piperacillin byboth parenteral routes were well tolerated.
Piperacillin (T-1220) is the generic name forsodium 6-[D(-)-a (4-ethyl-2,3-dioxo-1-piperazin-ylcarbonyl-amino)-a-phenylacetamido] penicil-linate, a new semisynthetic aminobenzyl penicil-lin derivative with an unusually wide spectrumof activity (2, 7, 9). In vitro testing showedpiperacillin to be active against all members ofthe Enterobacteriaceae, including Klebsiella (ofwhich 58% were inhibited by 8 ,ig/ml), and alsoagainst Pseudomonas aeruginosa. The activityof piperacillin was at least equivalent, but gen-erally superior to, that of ampicillin and carben-icillin, especially against Enterobacter species,Klebsiella species, Serratia marcescens, all Pro-teus species, including the indole-positive spe-cies, and Providencia species. Most striking wasits activity on P. aeruginosa, of which 50% wereinhibited by 2 ,ug/ml and 83% were inhibited by4 jig/ml (9).
Klebsiella pneumoniae, Escherichia coli, P.aeruginosa, Enterobacter species, and, increas-ingly, S. marcescens are, the major organismscausing life-threatening infections in debilitatedpatients. The activity of ampicillin is virtually
limited to E. coli; that of carbenicillin is ex-tended to Enterobacter species, S. marcescens,and P. aeruginosa, but the majority of the latterspecies are only inhibited by carbenicillin atconcentrations of 32 jug/ml or above. The sub-stantially higher activity and wider spectrum ofpiperacillin made it important to conduct humanpharmacokinetic studies, which are presented inthis paper.
Preliminary pharmacokinetic studies in labo-ratory animals (mice, rats, rabbits, dogs) and inhumans, employing both labeled and unlabeledpiperacillin, have indicated that the drug ispoorly absorbed orally but is well absorbed afterparenteral adninistration. It is bound to serumproteins by approximately 22%, and only mini-mal amounts of the drug appear to be metabo-lized in the body because most of the adminis-tered dose is excreted unchanged, primarily(66%) through the kidneys. The animal studiesalso disclose the presence of a wide range ofvariation among species but a significant biliaryexcretion of the drug (1). Previous pharmacoki-netic and clinical evaluations of this antibiotic
829
on April 10, 2019 by guest
http://aac.asm.org/
Dow
nloaded from

830 TJANDRAMAGA ET AL.
were performed in Japan with both normal vol-unteers and patients receiving this drug.The present study was designed to evaluate
both tolerance to piperacillin and the pharrna-cokinetics of the antibiotic after single intrave-nous (i.v.) and intramuscular (i.m.) doses of thisdrug given to a group of Caucasian healthyvolunteers. Data on the effect of probenecid onthe pharnacokinetics of piperacillin after i.m.injection are also included in this report.
(A preliminary report of this work was pre-sented at the 17th Interscience Conference onAntimicrobial Agents and Chemotherapy, NewYork, N.Y., 12-14 October 1977.)
MATERLALS AND METHODS
Subjects. The pharmacokinetic studies were car-ried out in 26 Caucasian subjects after informed con-sent. All were healthy male volunteers, ranging in agefrom 18 to 29 years (mean ± standard error of themean, 22 ± 0.42 years) and in weight from 60 to 85 kg(mean ± standard error of the mean, 70.4 ± 1.41 kg).Physical examinations, hematological and biochemicalindexes (peripheral blood count, renal and liver func-tion tests, complete urinary examination), chest Xrays, and electrocardiograms were normal. None wasaltered after administration of the antibiotic. None ofthe subjects was taking any drug therapy for at least2 weeks before the start of the study and during thewhole course of piperacillin studies. Subjects with ahistory of drug allergy were excluded.Drugs and routes ofadministration. Piperacillin
as the sodium salt was made available in vials of 1,000mg by American Cyanamid Co., Lederle LaboratoriesDiv., Pearl River, N. Y. Solutions were prepared im-mediately before injection by dissolving the antibioticin pyrogen-free sterile water for injections. Final vol-umes for the various dose of i.m. (0.5 and 1 g) and i.v.(1 to 4 g) injections were 4 ml and up to 20 ml (dilutedwith 5% dextrose) for the 6-g i.v. dose. Groups of eightvolunteers received piperacillin as single i.m. admin-istrations deep into the buttock in doses of 0.5, 1, and2 g. The i.v. administrations were given as slow bolusinjections over 3 min, with single doses of 1, 2, 4, and6 g in groups of five subjects each. Subjects partici-pating in more than one trial had an interval of atleast 1 week between two subsequent studies.The influence of probenecid was studied in a cross-
over design involving eight subjects. Probenecid wasgiven orally in a single dose of 1 g (two 0.5-g Benemidtablets; Merck Sharp & Dohme) at approximately 1 hbefore the i.m. administration of 1 g of piperacillin.Before each study, all subjects were fasted overnightand hydrated (water intake, 750 ml) 30 min beforepiperacillin administration.Blood and urine coliections for antibiotic as-
say. Venous blood samples (10 ml) were withdrawnfrom an arm vein through an indwelling butterflyneedle into collection tubes for clotted blood before,just at the end of, and at specified intervals afterpiperacillin injection; these samples were taken at 5,10, 20, 30, 60, and 90 min and 2, 3, 4, and 6 h after the
i.v. dose and 15, 30, and 60 min and 2, 3, 4, 6, and 8 hafter the i.m. dose.
In subjects receiving probenecid treatment, an ad-ditional blood sample was obtained at 24 h for proben-ecid assay. Blood specimens were allowed to stand incold environment (crushed ice) for about 1 h. Aftercentrifugation serum was removed and frozen (-20°C)before assay (within 1 to 2 weeks).
Urine was collected before the start of the experi-ment and during the periods 0 to 2 h, 2 to 4 h, 4 to 6h, 6 to 12 h, and 12 to 24 h after the piperacillin dose.All urine volumes were measured, and samples werestored at -20°C before analysis. The excretion ofcreatinine in the urine collected over 24 h was mea-sured, and its clearance was calculated. Creatinine wasmeasured by using the autoanalyzer modification ofthe method of Jaffe.Antibiotic assay. Concentrations of piperacillin in
serum and urine were determined by an agar wellmethod with the test organism Bacillus subtilis ATCC6633 in spore suspension (Difco Laboratories, Detroit,Mich.) incorporated in seed agar medium (BaltimoreBiological Laboratory, Cockeysville, Md.) adjusted topH 6.0. Further details of this method have beendescribed in a previous paper (8). For standards, pi-peracillin of certified potency from Lederle ResearchLaboratories was used. All samples were assayed induplicate and calculated according to the regressionlines of the standards in serum or in phosphate buffer(pH 6.0) in final concentrations of 50, 25, 12.5, 6.25,3.12, 1.56, 0.78, and 0.39 ,tg/ml. Samples were dilutedwhen necessary with pooled human serum (for serumsamples) or with phosphate buffer at pH 6.0 (for urinesamples) until concentrations were in the range of thestandard curves.The correlation coefficients of the regression lines
varied from r = 0.9967 to r = 0.9999 in serum and fromr = 0.9978 or r = 0.9999 in buffer. The sensitivity ofthe assay was limited to 0.4 yg/ml. All serum and urineblanks were negative.Pharmacokinetic analysis. Piperacillin serum
level data after i.v. administrations were analyzed bythe two-compartment open pharmacokinetic modeldesigned for rapid injection of a drug into the vascularcompartment (11).The decline in piperacillin serum concentration
after i.v. administration was fitted by a computerprogram for each subject by using the least-squaresregression analysis and the method of residuals to thesum of the two exponentials: C,' = Ae" + Be-',where Cp' represents the serum concentration at timet after the dose, a and /? are the first-order rateconstants of the fast and slow disposition processes,respectively, andA and B are the zero-time interceptsof the two components of the biexponential curves.These constants were estimated from the postinjectionplasma concentration data in the usual fashion (as-forrapid i.v. administration) because drug administrationof over 3 min in the present study was not sufficientlylong to attain steady state. Specific first-order rateconstants for distribution into (k12) and out of (k2l) theperipheral compartment and for elimination from thebody (k.0), as well as volume parameters describingthe disposition of i.v.-administered piperacillin accord-ing to the two-compartment open model, were calcu-
ANTIMICROB. AGENTS CHEMOTHER.
on April 10, 2019 by guest
http://aac.asm.org/
Dow
nloaded from

PHARMACOKINETICS OF PIPERACILLIN 831
lated from the usual equations (3, 6, 10). The areaunder the serum concentration-time curve (AUC) wasderived from the expression AUCi.v. = (A/a) + (B/f?)or determined by the trapezoidal rule (after either i.v.or i.m. dosing) and extrapolated to infinity. After i.m.administrations, the terminal serum half-life (t1/2 P) ofthe antibiotic was estimated by using the equationt1/2 = In 2/,8. Each regression line was based on atleast four points of serum concentrations from the 1-to 8-h data. The apparent volume of distribution (Vdarea) was calculated from the equation Vd area =(F.Do)/(AUCo c *,B), where Fis the fraction of the doseentering the systemic circulation as unchanged drug(F = 1 after i.v. dose). Because the fractional absorp-tion F derived from AUCi.m./AUCi.v. calculation was0.767, our calculations were based on the assumptionthat the i.m.-administered doses of piperacillin were77% available. Total clearance (CITO.) values were es-timated from ClTot = (F.Do)/AUC0.
Renal clearance (CIR) was calculated from: CIR =Xuo -t/AUCo-t. The binding of piperacillin to humanplasma proteins was reported to be 22% (1). Assumingthat the bound portion is not filtered during its passagethrough the glomerulus, the following equations canbe used to apportion the renal excretion of the anti-biotics in both: (i) percentage filtered by glomerulus(PFG) = (endogenous creatinine clearance/renalclearance of drug) x (percentage of drug not bound toplasma proteins); and (ii) percentage secreted by tu-bules = 100 - PFG. Nonrenal clearance (CINR) can bederived from the equation CINR = CITot - ClR. Whereappropriate, results have been standardized to 1.73 m2body surface area. The results are presented as mean± standard error of the mean in the text and thetables. Statistical analyses were performed by usingStudent's t test, and a P value of 0.05 or less wasconsidered to be statistically significant.
1000_
500
E - CeE
z 100#a: "
CL,50-'' \z
O L \\
X 10
z 5~.4
RESULTS
Tolerance to piperacillin and safety involunteers. The three parts of the presentstudy in which parenteral piperacillin doses (i.v.and i.m.) as well as i.m. doses of the antibioticwith and without probenecid were used weresatisfactorily completed with all the 26 healthyvolunteers. Both the i.v. and i.m. injections ofpiperacillin were well tolerated without any ad-verse local or systemic effects, and no abnor-malities in any of the hematological or biochem-ical indexes or in urinalysis were observed.Administration by i.v. injection. The av-
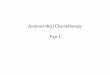
erage serum levels of piperacillin obtained fromthe normal subjects receiving single i.v. injec-tions of the antibiotic (1, 2, 4, and 6 g) are shownin Fig. 1. As can be seen, the serum levels declinein a biexponential manner. An initial rapid fallover the first 1 h was followed by a monoexpo-nential decline over the remaining period ofobservation. The mean phannacokinetic param-eters estimated from serum and urine data afterthe i.v. doses are shown in Table 1. The averageconcentrations immediately at the end of the 3-min slow bolus injection for the four doses were71, 199,331, and 452 ,tg/ml. Mean concentrationsat 3 h were 0.9, 4.7, 17.7, and 32.8 jLg/ml, respec-tively, after the four increasing doses and 1.4,ug/ml at 8 h after the 6.0-g dose.The mean tl/2 # for these doses were 36, 54, 61,
and 63 min, respectively, showing clearly pro-longed tl/2 ,g values with increasing doses from 1to 4 g, whereas the additional increase of the
Dose NIGm3
0__ _* 5>- 2 5*U 5
6 5
Mean t SEM
6 7 8
FIG. 1. Mean serum concentrations ofpiperacillin after single i.v. injections of increasing doses offrom 1
to 6 g in four groups offive normal volunteers. S.E.M., Standard error of the mean.
0 1 2 3 4 5TIME -After single dose (hours)
VOL. 14, 1978
I
,IL
on April 10, 2019 by guest
http://aac.asm.org/
Dow
nloaded from

832 TJANDRAMAGA ET AL. ANTIMICROB. AGENTS CHEMOTHER.
TABLE 1. Pharmacokinetic data ofpiperacillin in healthy volunteers after i.v. administration
Dose Serum concn at A a t1/2a B pDose end of injection (jug/m1) (h-') h(/Ag/MI) (h-1)() (jig/mi)h mi
1.0 70.7 ± 12.7a 32.7 ± 3.5 -5.51 ± 1.74 0.17 ± 0.03 10.0 ± 1.9 34.5 ± 4.6 -1.19 ± 0.10(n= 5)
2.0 199.5 ± 37.4 131.6 ± 19.4 -3.93 ± 0.37 0.18 ± 0.02 10.9 ± 1.1 52.6 ± 4.4 -0.79 ± 0.07(n= 5)
4.0 330.7 ± 67.8 252.7 ± 76.4 -4.40 ± 0.81 0.18 ± 0.03 10.7 ± 1.7 134.7 ± 5.9 -0.69 ± 0.04(n= 5)
6.0 451.8 ± 21.8 314.1 ± 100.9 -2.75 ± 0.80 0.32 ± 0.06 19.0 ± 3.4 218.1 ± 18.5 -0.67 ± 0.04(n= 5)
t1/2,0 Distribution volumes (liters/1.73 m2)Dose AUC0x(g) h min (ug/ml-h) V, (central com- V2 (peripheral Vd,. (steady
partment) compartment) state)1.0 0.60 ± 0.05 35.8 ± 3.1 36.0 ± 1.0 14.5 ± 1.3 4.6 ± 0.5 19.0 ± 1.4(n= 5)
2.0 0.90 ± 0.08 54.0 ± 4.7 102.0 ± 11.5 10.9 ± 1.3 7.4 ± 0.6 18.3 ± 1.9(n= 5)
4.0 1.02 ± 0.05 61.2 ± 3.1 250.3 ± 12.5 11.2 ± 1.9 7.4 ± 1.1 18.6 ± 1.1(n = 5)
6.0 1.05 ± 0.07 63.0 ± 4.4 437.9 ± 21.6 11.9 ± 1.6 4.2 ± 1.0 16.1 ± 1.3(n = 5)
Dose Vde Intercompartmental rate constants (h-') ClTot CIR1 2 (ml/min per 1.73 (ml/min per 1.73
(g) (liters/1.73m' k,2 k2, kel m2) m2)
1.0 21.6 ± 1.7 1.30 ± 0.58 3.55 ± 1.12 1.86 ± 0.16 408.6 ± 16.8 303.6 ± 29.5(n= 5)
2.0 24.3 ± 3.1 1.18 ± 0.12 1.71 ± 0.16 1.84 ± 0.18 301.8 ± 32.3 245.7 ± 30.3(n= 5)
4.0 24.3 ± 1.3 1.61 ± 0.54 1.96 ± 0.10 1.51 ± 0.24 254.2 ± 19.3 203.7 ± 19.5(n = 5)
6.0 20.2 ± 1.5 0.76 ± 0.43 1.44 ± 0.16 1.22 ± 0.23 209.6 ± 8.3 186.9 ± 17.5(n = 5)
DoseCINR Endogenous creat- Ratio of piper- Proportion of % of dose recovered in urine (un-Dose 1(ml/mnper 173 inine clearance acillin to cre- renal excretion changed form) at:(g) in2) (ml/min per 1.73 atinine clear- via tubules
m mi2) ance (%) -2 h -24 h
1.0 105.1 ± 26.3 101.8 ± 4.6 3.0 ± 0.3 72.9 ± 2.9 49.0 ± 12.1 74.1 ± 6.3(n= 5)
2.0 54.7 ± 13.7 86.5 ± 10.2 3.1 ± 0.7 69.7 ± 6.5 65.3 ± 4.3 81.4 ± 4.5(n= 5)
4.0 53.8 ± 2.6 86.5 ± 5.0 2.4 ± 0.4 65.4 ± 4.1 61.6 ± 3.6 79.8 ± 2.3(n= 5)
6.0 24.3 ± 15.2 103.1 ± 10.0 1.8 ± 0.2 56.4 ± 3.7 64.2 ± 3.2 89.1 ± 7.5(n = 5)a Values given are mean ± standard error of the mean.
dose to 6.0 g did not result in further prolonga- tered dose, in particular with the higher doses oftion of the half-life. 2, 4, and 6 g. This relationship, however, did notThe mean areas under the concentration- hold for the 1-g dose, which resulted in a dispro-
time curves (AUC00) were 38.3, 110.4, 254.8, and portionately smaller AUC value of less than one-452.2 ,ug/ml . h, respectively, showing that the third of that achieved after a 2-g dose (Fig. 1).area is reasonably proportional to the adminis- The Vd area of piperacillin was not signifi-
on April 10, 2019 by guest
http://aac.asm.org/
Dow
nloaded from

PHARMACOKINETICS OF PIPERACILLIN 833
cantly altered with increasing dose; the meanvolumes were 21.6, 24.3, 24.3, and 20.2 liters/1.73In2. The corresponding AUCs at steady statewere 19.0, 18.3, 18.6, and 16.1 liters/1.73 m2,respectively.
Piperacillin was rapidly excreted in high con-centrations through the kidney. Approximately50 to 65% of the dose was recovered in the urinewithin 2 h after the i.v. injection, and the cu-mulative urinary excretion in 24 h amounted tofrom 75 to 90% of the dose. The CIR of pipera-cillin was more rapid with the lower dose anddecreased with increasing dosage; the meanclearance rates adjusted to a body surface areaof 1.73 m2 were 303.6, 245.7, 203.7, and 186.9ml/min after doses of 1, 2, 4, and 6 g, respec-tively. In all subjects, the CIR rate of piperacillinwas found to be more rapid than the simulta-neously measured endogenous creatinine clear-ance, thus indicating the presence of an activetubular secretion of the drug in addition to glo-merular filtration. Mean ratios of piperacillin tocreatinine clearance were 3.0 and 3.1 for the 1-and 2-g doses, respectively, but they were low-ered to 2.4 and 1.8 with the increased doses of 4and 6 g, respectively. Taking into account a 22%protein binding of piperacillin, these data indi-cate that between 73 and 56% of the drug ex-creted by the kidneys is cleared by tubular se-cretion (Table 1).Administration by i.m. injection. For the
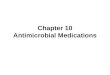
three i.m. doses the mean serum concentrationcurves are shown in Fig. 2, and the mean phar-
100t
50t
I
Ez 1000-
l 5zwUJz0
C-)uIrwUnz 054wI
macokinetic data of piperacillin are given inTable 2. Average peak serum concentrationsafter 0.5-, 1.0-, and 2.0-g injections were 4.9, 13.3,and 30.2 ,tg/ml, respectively. The mean times topeak concentrations occurred at approximately30 to 50 min after the i.m. doses. The mean t1/2,Bfor the three increasing doses were 60.2, 68.7,and 80.6 min (differences not statistically sig-nificant).
Disproportionately lower values of the AUCwith decreasing doses were also observed afteri.m. doses, the mean areas being 85.2 ,ug/ml.hafter the 2-g dose, 29.2 ,ug/ml.h after the 1-gdose, and only 10.3 ,ug/mlh after the lowestdose tested, 0.5 g (Fig. 2). Comparison of theAUC values of piperacillin achieved through thei.v. and i.m. routes disclosed an available fractionof approximately 70 to 80% for the i.m. admin-istered dose. The Vd area of piperacillin appearsto be decreased with increasing i.m. dose, themean Vd areas being 51.5, 41.1, and 33.1liters/1.73 M2. Approximately 60% of the i.m.doses were recovered in urine after 24 h.
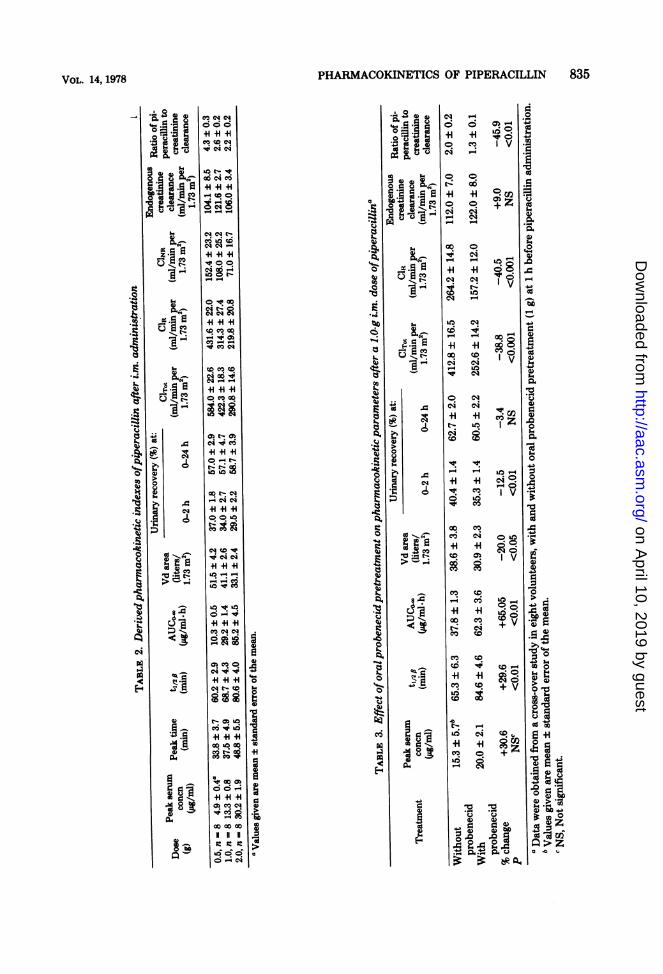
Effects of probenecid. Probenecid (1.0 g),given orally approximately 1 h before i.m. piper-acillin administration (1.0 g), had a clear effecton several pharinacokinetic parameters (Table3). Concomitant probenecid administration re-sulted in a significantly increased mean peakserum concentration (30%), an increased totalAUC (65%), as well as a prolonged terminalserum half-life (30%). It decreased the Vd areaof the drug by 20% and its CIR by 40%. Lowering
Dose N(GM)
_-* 05 80- -o 1 8ii _ 4 2 8
M*an * SEM
0.10 1 2 3 l 5 6 7 8 9 10 11 12
TIME - After single dose (hours)
FIG. 2. Mean serum concentrations ofpiperacillin after i.m. injection of 0.5, 1.0, and 2.0 g in three groupsof eight normal volunteers. S.E.M., Standard error of the mean.
VOL. 14, 1978
on April 10, 2019 by guest
http://aac.asm.org/
Dow
nloaded from

so:
50
0 -
1--r 5 ~ Probenecid WITHz Probenecid
z0
w
O,-ts \z< 0.5S I
N B normal subjects
lMean t S.E.M.
O 1 2 3 4 5 6 7 8TIME - After single dose (hours)
FIG. 3. Piperacillin serum concentrations after i.m. injection of) g ofpiperacillin from a cross-over studywith and without probenecid pretreatment (I g orally at 1 h before piperacillin dose) in eight normalvolunteers. S.E.M., Standard error of the mean.
of the urinary excretion by probenecid was es-pecially noticeable during the first 4 to 5 h afterprobenecid administration. However, there wasonly a delay, not a significant decrease in thetotal 24-h urinary excretion of the antibiotic(62.7% of the dose without probenecid and 60.5%with concomitant probenecid). The ratio of pi-peracillin to creatinine clearance was signifi-cantly lowered (from 2.4 to 1.3) by oral proben-ecid treatment.
DISCUSSIONThe pharmacokinetics of parenterally admin-
istered piperacillin were analyzed in the presentstudy by using a two-compartment kinetic model(i.v. doses) and a one-compartment model (i.m.doses).The 2-g i.v. dose in our study functioned as a
reference when considering our pharmacokineticdata after bolus i.v. doses of 1, 2, 4, and 6 g ofpiperacillin given to Caucasian healthy volun-teers. After a slow (3-min) i.v. bolus injection of2 g, piperacillin appears to be rapidly distributed(average half-life for distribution [t1/2 .] = 10.8min) within the extracellular fluids (V1 = 10.9liters/1.73 m2) and to some extent within theperipheral tissue compartment (V2 = 7.4liters/1.73 m2). The Vd area of the drug was 24.3liters, and its distribution volume at steady state(Vd.) was 18.3 liter/1.73 M2. The mean serumhalf-life during the fl-elimination phase was 54min, and the AUC0o. was 102.0 ,g/ml*h. ClTot ofthe antibiotic averaged 301.8 ml/min per 1.73
mi2, whereas the CIR rate was approximately 20%lower (245.7 ml/min per 1.73 m2), indicating thatpiperacillin undergoes biotransformation or ex-trarenal elimination to some extent in additionto renal excretion. Approximately 80% of theadministered dose was recovered in urine after24 h.The ClR rate values consistently exceed their
corresponding glomerular filtration rate, as es-timated by the endogenous creatinine clearance;average ratios of piperacillin to creatinine clear-ance were 3.1 after the 2-g i.v. dose, thus sug-gesting that active renal tubular secretion of theantibiotic does take place.The binding of piperacillin to human plasma
proteins is reported to be 22% (1). Assuming thatthe bound fraction is not filtered during its pas-sage through the glomerulus, about 70% of therenal excretion of piperacillin after the 2-g i.v.dose would seem to be by tubular secretion(Table 1), the remainder being by glomerularfiltration. This finding is supported by our stud-ies with probenecid in which peak serum con-centrations and tl/2 (after i.m. injections of 1 gof piperacillin) increased by 30%, AUC0oD in-creased by 65%, and CIR decreased by 40%(Table 3).The kinetic data obtained after the lower i.v.
dose of 1 g suggest that piperacillin is clearedfrom plasma by both the kidneys and nonrenalmechanisms in a greater proportion than it is inthe case of the higher doses; CIR was 304 ml/minper 1.73 m2 after the 1-g dose and 246, 204, and
834 TJANDRAMAGA ET AL. ANTIMICROB. AGENTS CHEMOTHER.
on April 10, 2019 by guest
http://aac.asm.org/
Dow
nloaded from
PHARMACOKINETICS OF PIPERACILLIN 835
CU
C's
0
04
.-
5..
5.
0
0
_0
fi4)
54
4)
4)
1
Go
N
I
4)4)
I
aw
.is 4) 8't I .
0 ,I
'43 go .24 & 0
N 4) 4)kC)a .10 .s
0, a I m0) '-. ti.- V-4
3 0 d
k
N
A S1-4
u m
11-1 ti
I-
k
N
4.1 e- 4 mU "I t-
d -4
p4C.)4)8>
C%c
4c
el
c
N.4
tN
cr v-
OI V
o60
cOC44eq4
O0_ _
44
NO eq
_
c.6 4CD 0_
0. co I ?
t eq
o. cq
c eq 1Ci
L8
0.
00 CY)Co e-
9s
V-401 v
0
eq 0iI v
cys
00 mc
eo so
CO CD
CD*
m w
(0ct
n4
-4
O
co ,
+
10 l
jI1101104)4
0 .0 .0
C.)
0s
.4(4
0D
b4
$oZ
VOL. 14, 1978
51:113ji:""4
54&z e-c) .-
I
U e
Id
ei
+ +1 +
&o Cq 4
cs
-H
peq _
+1
'q.
e"!q q
C4 8
0' t-
-
o.4s 0
+1 +
0.0-uX
t eq
C4 V co
04- -Co
qCeq
eq -q q
V0404-
44+1444
_i _ C4u:-0rA
ci C Uoq _ s+1 +1" es cs
°9 0
t co o.
co co
N 1
ci O U
It
..
9.
-S.)
L.
'.2
CIA
Cs
C.)
E9
144
;Ib
)IIiII9Iii.b 1-
9I.
It
3A
3A
k4)3zob
4ki.4:0oc-1
4I
t
1.
r
I
on April 10, 2019 by guest
http://aac.asm.org/
Dow
nloaded from

836 TJANDRAMAGA ET AL.
187 ml/min after the three subsequent higherdoses of 2, 4, and 6 g, respectively, whereas thecorresponding CINR values were 105 ml/min(after 1 g), 55 ml/min (after 2 g), 54 ml/min(after 4 g), and 24 ml/min (after 6 g). Thepresence of disproportionately higher clearancevalues for the lower doses of piperacillin is re-
flected in the disproportionately lower AUCoxwhich were 36, 102, 250, and 438 ,tg/ml h afterdoses of 1, 2, 4, and 6 g, respectively. The mean
t1/2 of piperacillin after the four increasing i.v.doses were 36, 54, 61, and 63 min, respectively,showing that the half-life is clearly shortened inthe case of the lowest dose tested (1 g), whereasthe values obtained after 4- and 6-g doses were
similar (half-life of approximately 1 h), suggest-ing some saturation process in the clearancemechanisms. Obviously higher clearance rates(CIR and CINR) of piperacillin with the lowerdoses were also observed after the three increas-ing i.m. doses tested (0.5, 1, and 2 g). ClR was
432 ml/min per 1.73 m2 after the 0.5-g i.m. dose,compared with 314 and 220 ml/min after the 1-
and 2-g doses, respectively, and the correspond-ing ClNR values were 153, 108, and 71 ml/min(Table 2). The peak serum concentrations were
achieved within 30 to 50 min after i.m. injection.The 0.5-g dose resulted in disproportionatelylower peak serum levels and AUCs comparedwith the higher doses (Table 2). Bioavailabilitiesof piperacillin after i.m. administration, as
judged from the area under the curve ratios(i.m./i.v.) after the 1- and 2-g doses, were ap-proximately 70 to 80%. Thus, piperacillin doesindeed appear to be rapidly and reliably ab-sorbed after i.m. administration.The 24-h urinary recovery of the antibiotic
averaged 57 to 58% after i.m. administration(Table 2) and 74 to 89% after the i.v. route(Table 1). This lower urinary recovery implies a
larger proportion of nonrenal mechansm of elim-ination when piperacillin is administeredthrough the i.m. route.The fact that the ratio ofthe CIR of piperacillin
to the CIR of creatinine was significantly higherthan 1 indicates that piperacillin, in addition tobeing excreted by glomerular filtration, is alsosecreted by renal tubules. This is strongly sup-
ported by the inhibiting effect of oral probenecidadministration (Table 3). The CIR of piperacillinwas significantly (40%) lowered, and the ratio ofpiperacillin clearance to creatinine clearance de-creased from 2.4 to 1.3 after probenecid treat-ment. The 24-h urinary recovery of piperacillinafter a 1-g i.m. dose was not significantly alteredby probenecid; recovery was 62.7% in the ab-sence and 60.5% in the presence of probenecid,
indicating that probenecid delayed but did notdecrease the urinary excretion.The pharmacokinetic data with and without
probenecid treatment (Table 3) show that pro-benecid diminishes the CIR of piperacillin by40.5%, which is consistent with its usual effectson organic acid transport in the kidney. Mostunusual, however, was the fact that a concomi-tant decrease of 35.9% in the CLNR of piperacillinduring probenecid treatment was observed inthe present study. These two alterations shouldthus be responsible for the observed increases inplasma piperacillin concentrations, i.e. a 30%increase in the peak serum concentrations, a 30%prolongation of serum half-life, and a 65% in-crease in AUCox. As has been reported earlierfor several other penicillin derivatives, e.g., am-picillin, ancillin, nafcillin, and cephaloridine (4),a similar apparent decrease in the distributionparameters was observed for piperacillin (20%decrease in Vd area) in the presence of proben-ecid. Such a decrease in the Vd area parameterhas been shown to be an artifactual findingresulting from the reduced elimination rate ofpenicillin during probenecid treatment, whichallows more drug to reach the tissue compart-ment (5). Such an apparent decrease in Vd areaappears to be a reflection that the system wascloser to reaching steady-state equilibrium withprobenecid.The good human tolerance to parenteral pi-
peracillin and the favorable pharmacokineticproperties comparable to those known for otherpenicillin compounds, together with its good an-tibacterial activity, suggest that extensive clini-cal trials with this antibiotic are highly desirablefor the evaluation of its usefulness in treatingbacterial infections in humans.
ACKNOWLEDGMENTSThe authors are grateful to M. Phyfferoen from Cyanamid
Benelux, Brussels, Belgium, for her advice and help during theinvestigations and to M. Bareau for her secretarial assistance.
LITERATURE CITED1. American Cyanamid Co. 1977. Clinical investigators
brochure. American Cyanamid Co., Lederle Laborato-ries Div., Pearl River, N. Y.
2. Fu, K. P., and H. C. Neu. 1978. Piperacillin, a newpenicillin active against many bacteria resistant to otherpenicillins. Antimicrob. Agents Chemother. 13:358-367.
3. Gibaldi, M., and D. Perrier. 1975. Pharmacokinetics.Marcel Dekker, Inc., New York.
4. Gibaldi, M., and M. A. Schwartz. 1968. Apparent effectof probenecid on the distribution of penicillins in man.Clin. Pharmacol. Ther. 9:345-349.
5. Jusko, W. J., and M. Gibaldi. 1972. Effects of change inelimination on various parameters of the two-compart-ment open model. J. Pharm. Sci. 61:1270-1273.
6. Riegelman, S., J. C. K. Loo, and M. Rowland. 1968.Shortcomings in pharmacokinetic analysis by conceiv-
ANTIMICROB. AGENTS CHEMOTHER.
on April 10, 2019 by guest
http://aac.asm.org/
Dow
nloaded from

PHARMACOKINETICS OF PIPERACILLIN 837
ing the body properties of a single compartment. J.Pharm. Sci. 57:117-123.
7. Ueo, K., Y. Fukuoka, T. Hayashi, T. Yasuda, H. Taki,M. Tai, Y. Watanabe, I. Saikawa, and S. Mitsu-hashi. 1977. In vitro and in vivo antibacterial activityof T-1220, a new semisynthetic penicillin. Antimicrob.Agents Chemother. 12:455-460.
8. Verbist, L, 1974. Triple crossover study on absorptionand excretion of ampicillin, pivampicillin, and amoxy-
cillin. Antimicrob. Agents Chemother. 6:588-593.
9. Verbist, L 1978. In vitro activity of piperacillin, a newsemisynthetic penicillin with an unusually broad spec-trum of activity. Antimicrob. Agents Chemother.13:349-357.
10. Wagner, J. G. 1975. Fundamentals of clinical pharma-cokinetics. Drug Intelligence Publications, Hamilton,m.
11. Wagner, J. G., and J. I. Northam. 1967. Estimation ofvolume of distribution and half-life of a compound afterrapid intravenous injection. J. Phann. Sci. 56:529-531.
VOL. 14, 1978
on April 10, 2019 by guest
http://aac.asm.org/
Dow
nloaded from