Embed Size (px)
Citation preview
1
PK-PD and ANTIBIOTIC RESISTANCE Lessons Learned
24 September 2014
Paul G. Ambrose, Pharm.D, FIDSA Institute for Clinical Pharmacodynamics
Latham, New York
WHERE WE’RE GOING TODAY
Some Important Questions
• Does the presence or absence of a resistance determinant(s)
predict outcome?
• What is the relationship between drug exposure and resistance emergence?
• Can we alter the shape of drug exposure to increase our
chances of attaining positive outcomes?
• How big a challenge is effect site penetration and associated
variability?
• Is the answer simply the “not so simple” combination therapy?
2
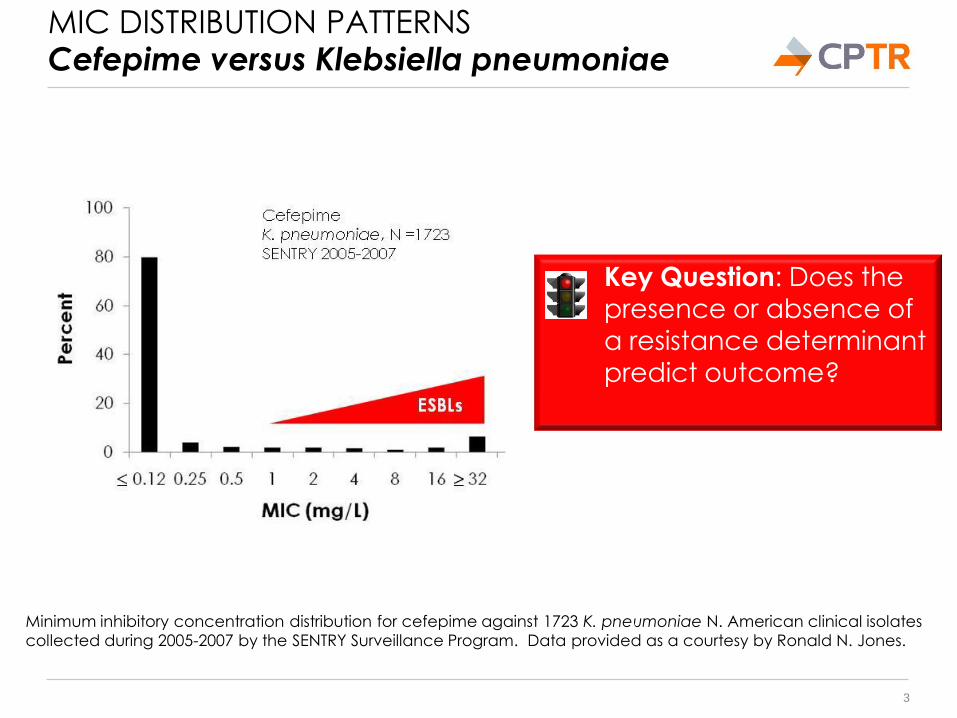
MIC DISTRIBUTION PATTERNS Cefepime versus Klebsiella pneumoniae
3
Key Question: Does the
presence or absence of
a resistance determinant predict outcome?
Minimum inhibitory concentration distribution for cefepime against 1723 K. pneumoniae N. American clinical isolates
collected during 2005-2007 by the SENTRY Surveillance Program. Data provided as a courtesy by Ronald N. Jones.
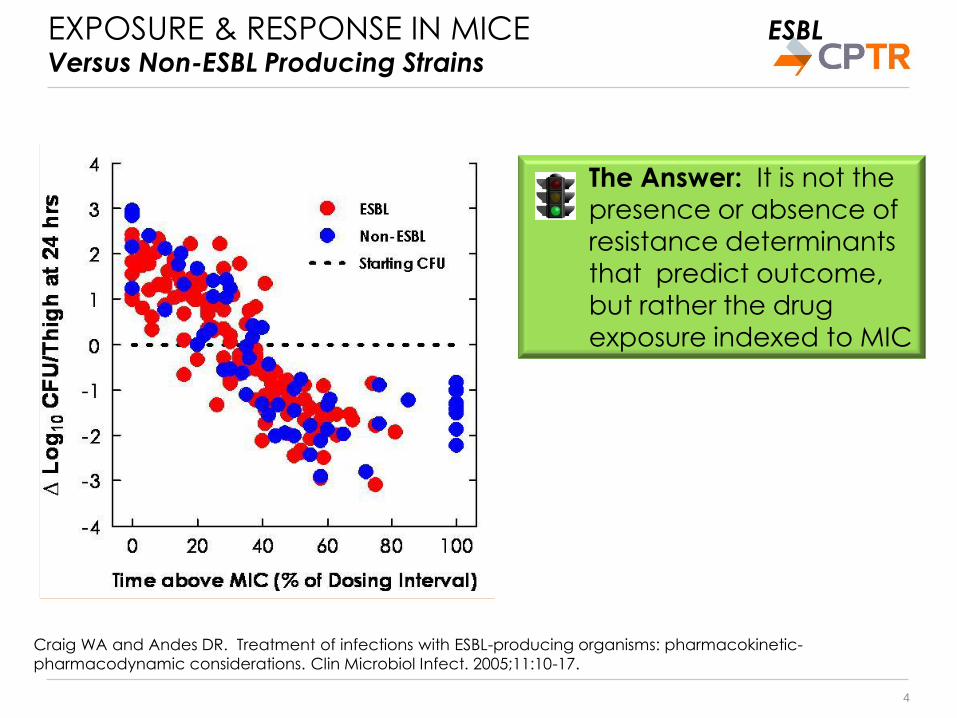
EXPOSURE & RESPONSE IN MICE ESBL
Versus Non-ESBL Producing Strains
4
The Answer: It is not the
presence or absence of
resistance determinants
that predict outcome,
but rather the drug
exposure indexed to MIC
Craig WA and Andes DR. Treatment of infections with ESBL-producing organisms: pharmacokinetic-
pharmacodynamic considerations. Clin Microbiol Infect. 2005;11:10-17.
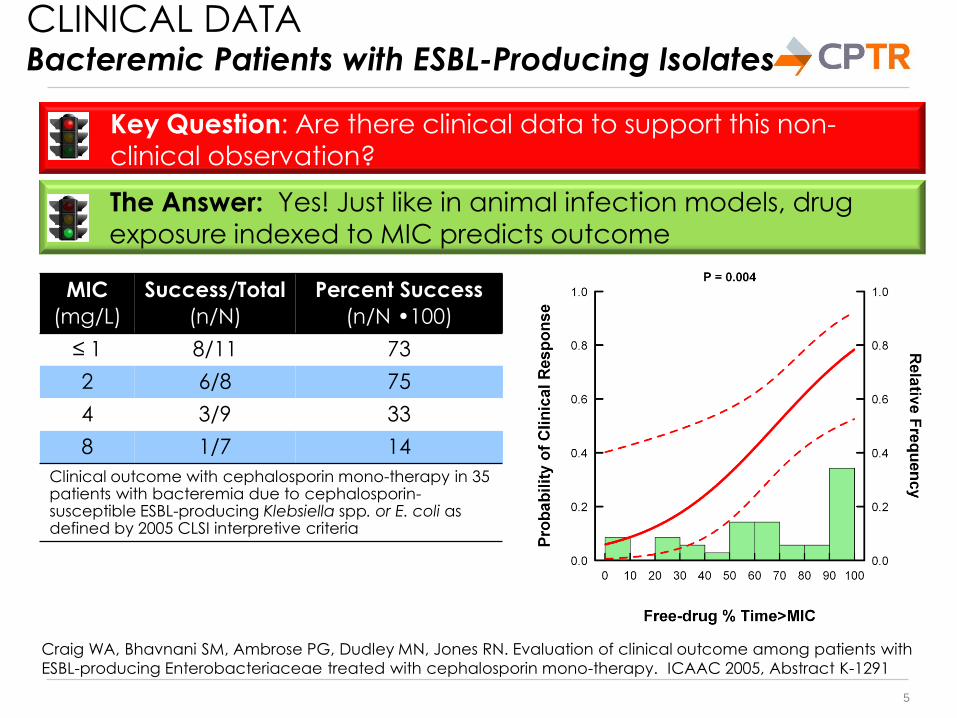
CLINICAL DATA Bacteremic Patients with ESBL-Producing Isolates
5
The Answer: Yes! Just like in animal infection models, drug
exposure indexed to MIC predicts outcome
Key Question: Are there clinical data to support this non-clinical observation?
MIC
(mg/L)
Success/Total
(n/N)
Percent Success
(n/N •100)
≤ 1 8/11 73
2 6/8 75
4 3/9 33
8 1/7 14
Clinical outcome with cephalosporin mono-therapy in 35 patients with bacteremia due to cephalosporin-susceptible ESBL-producing Klebsiella spp. or E. coli as defined by 2005 CLSI interpretive criteria
Craig WA, Bhavnani SM, Ambrose PG, Dudley MN, Jones RN. Evaluation of clinical outcome among patients with
ESBL-producing Enterobacteriaceae treated with cephalosporin mono-therapy. ICAAC 2005, Abstract K-1291
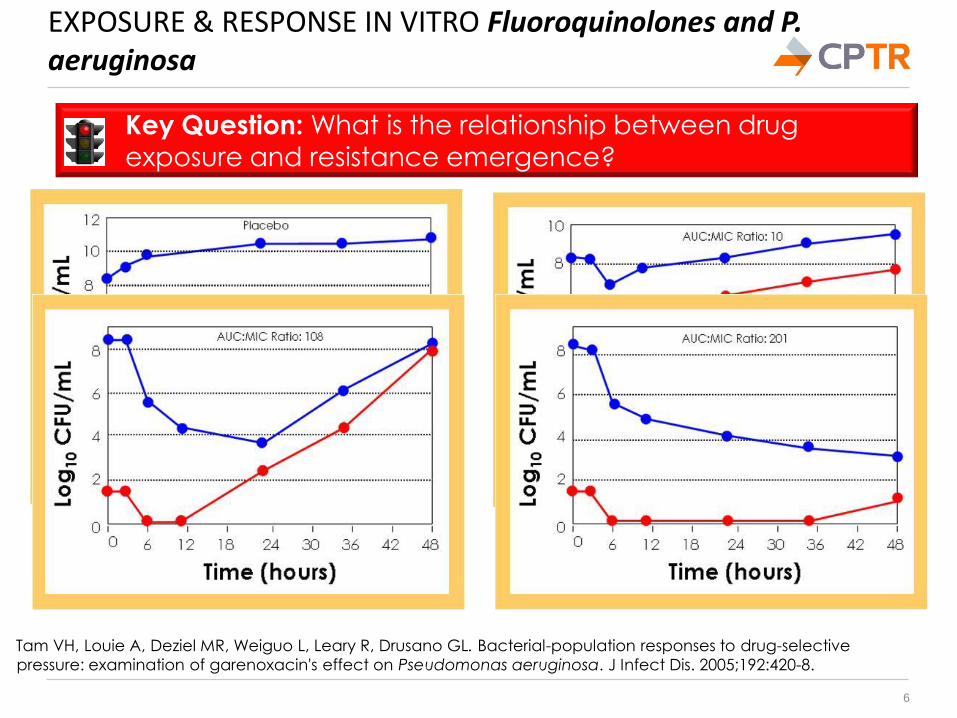
EXPOSURE & RESPONSE IN VITRO Fluoroquinolones and P. aeruginosa
6
Tam VH, Louie A, Deziel MR, Weiguo L, Leary R, Drusano GL. Bacterial-population responses to drug-selective
pressure: examination of garenoxacin's effect on Pseudomonas aeruginosa. J Infect Dis. 2005;192:420-8.
Key Question: What is the relationship between drug
exposure and resistance emergence?
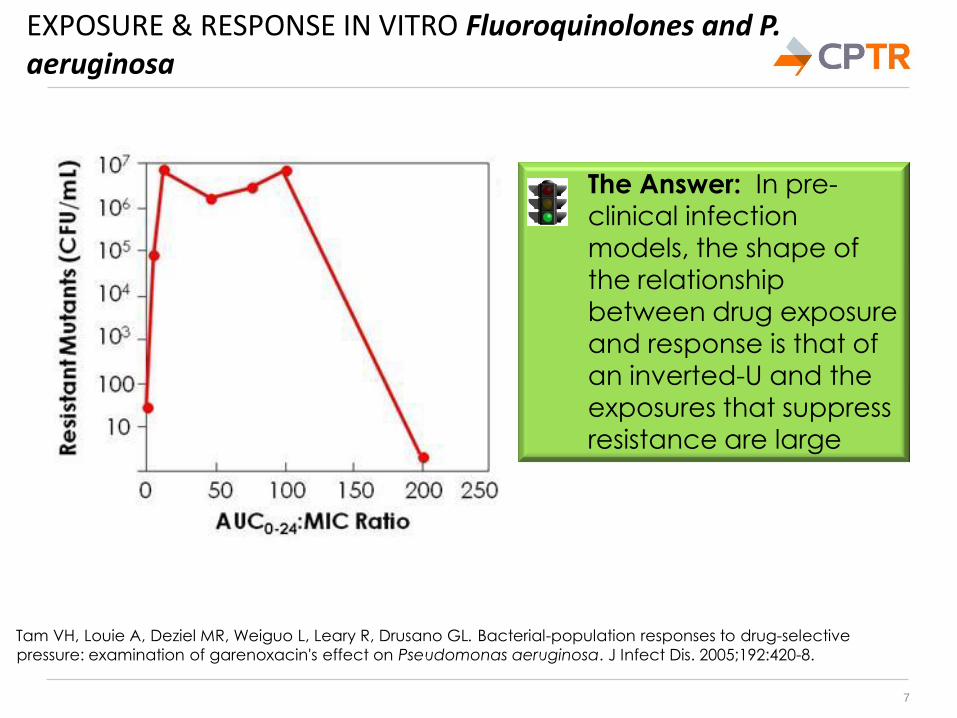
EXPOSURE & RESPONSE IN VITRO Fluoroquinolones and P. aeruginosa
7
Tam VH, Louie A, Deziel MR, Weiguo L, Leary R, Drusano GL. Bacterial-population responses to drug-selective
pressure: examination of garenoxacin's effect on Pseudomonas aeruginosa. J Infect Dis. 2005;192:420-8.
The Answer: In pre-
clinical infection
models, the shape of the relationship
between drug exposure
and response is that of
an inverted-U and the exposures that suppress
resistance are large
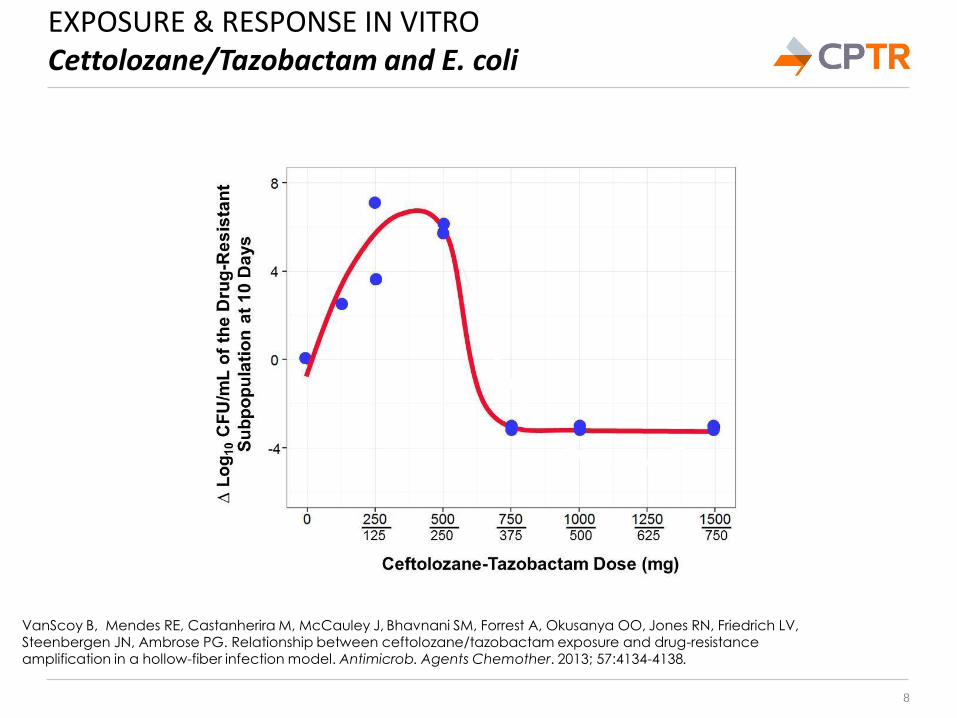
EXPOSURE & RESPONSE IN VITRO Cettolozane/Tazobactam and E. coli
8
VanScoy B, Mendes RE, Castanherira M, McCauley J, Bhavnani SM, Forrest A, Okusanya OO, Jones RN, Friedrich LV, Steenbergen JN, Ambrose PG. Relationship between ceftolozane/tazobactam exposure and drug-resistance amplification in a hollow-fiber infection model. Antimicrob. Agents Chemother. 2013; 57:4134-4138.
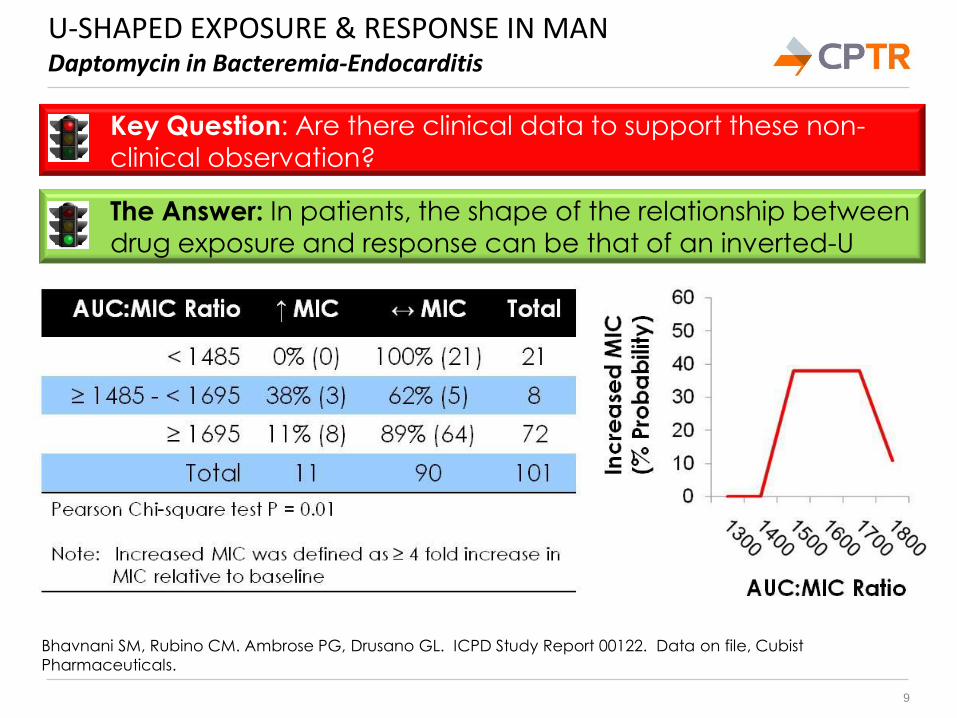
U-SHAPED EXPOSURE & RESPONSE IN MAN Daptomycin in Bacteremia-Endocarditis
9
Bhavnani SM, Rubino CM. Ambrose PG, Drusano GL. ICPD Study Report 00122. Data on file, Cubist
Pharmaceuticals.
The Answer: In patients, the shape of the relationship between
drug exposure and response can be that of an inverted-U
Key Question: Are there clinical data to support these non-clinical observation?
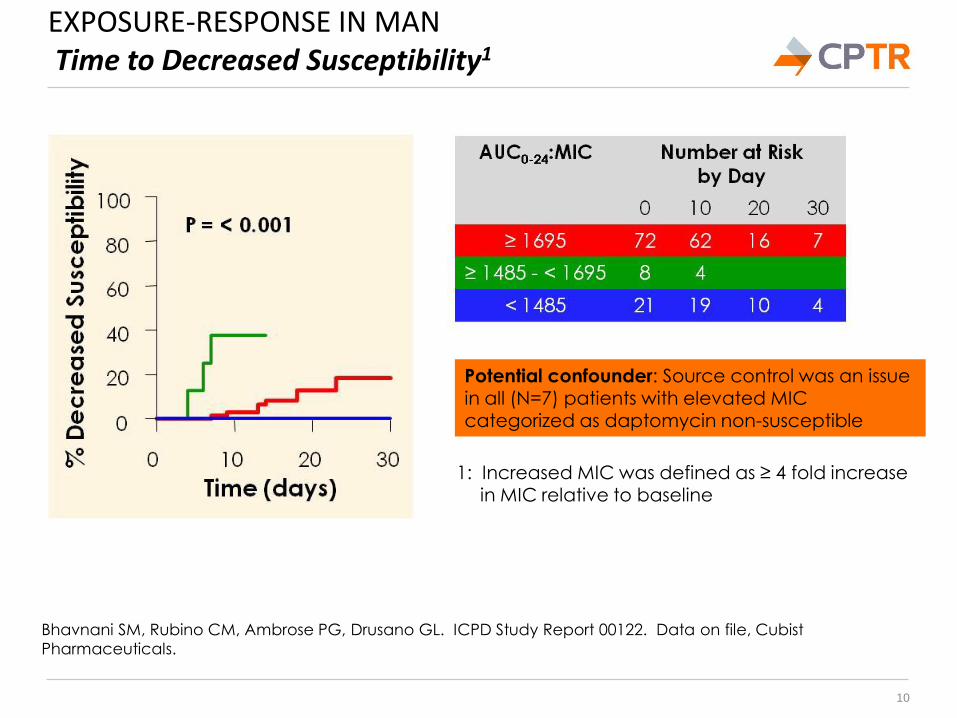
EXPOSURE-RESPONSE IN MAN Time to Decreased Susceptibility1
10
Bhavnani SM, Rubino CM, Ambrose PG, Drusano GL. ICPD Study Report 00122. Data on file, Cubist
Pharmaceuticals.
Potential confounder: Source control was an issue in all (N=7) patients with elevated MIC
categorized as daptomycin non-susceptible
1: Increased MIC was defined as ≥ 4 fold increase in MIC relative to baseline
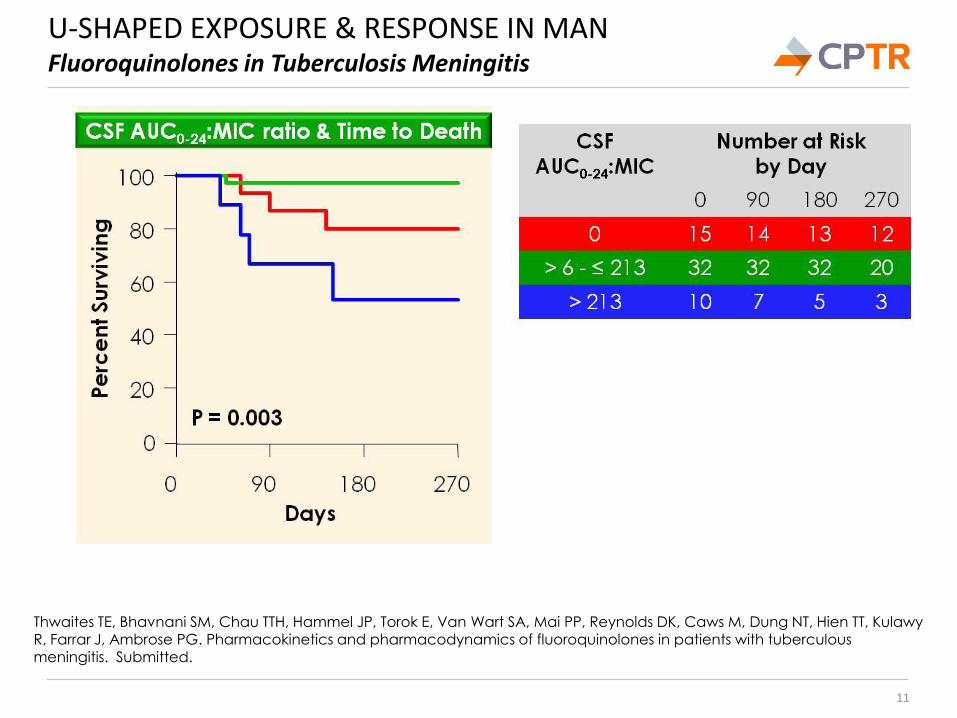
U-SHAPED EXPOSURE & RESPONSE IN MAN Fluoroquinolones in Tuberculosis Meningitis
11
Thwaites TE, Bhavnani SM, Chau TTH, Hammel JP, Torok E, Van Wart SA, Mai PP, Reynolds DK, Caws M, Dung NT, Hien TT, Kulawy R, Farrar J, Ambrose PG. Pharmacokinetics and pharmacodynamics of fluoroquinolones in patients with tuberculous
meningitis. Submitted.
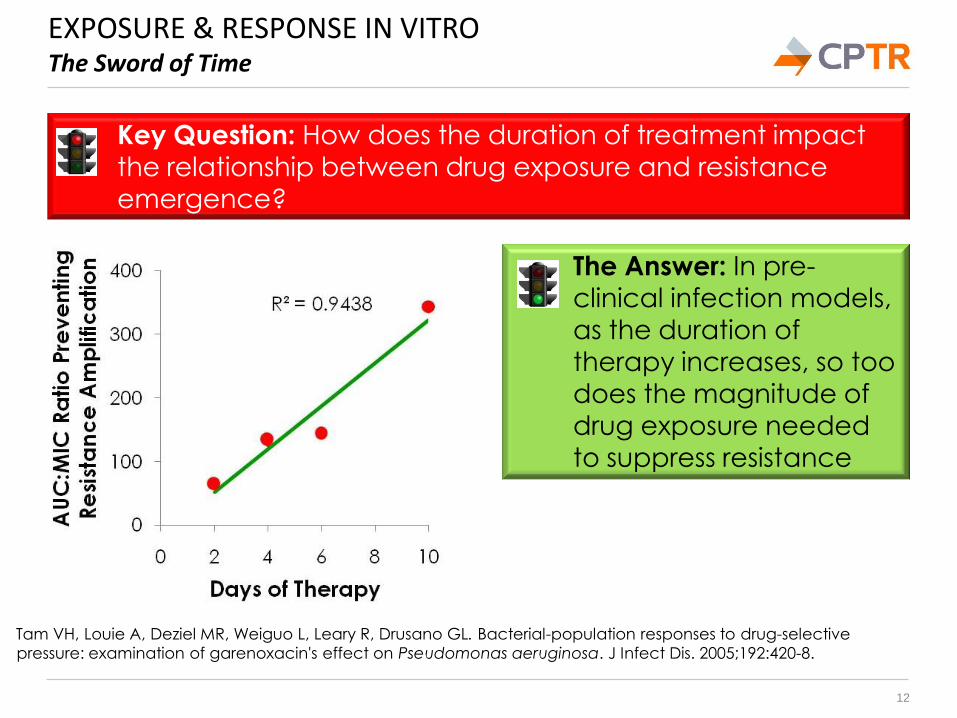
EXPOSURE & RESPONSE IN VITRO The Sword of Time
12
Key Question: How does the duration of treatment impact
the relationship between drug exposure and resistance emergence?
Tam VH, Louie A, Deziel MR, Weiguo L, Leary R, Drusano GL. Bacterial-population responses to drug-selective
pressure: examination of garenoxacin's effect on Pseudomonas aeruginosa. J Infect Dis. 2005;192:420-8.
The Answer: In pre-clinical infection models,
as the duration of
therapy increases, so too
does the magnitude of
drug exposure needed to suppress resistance
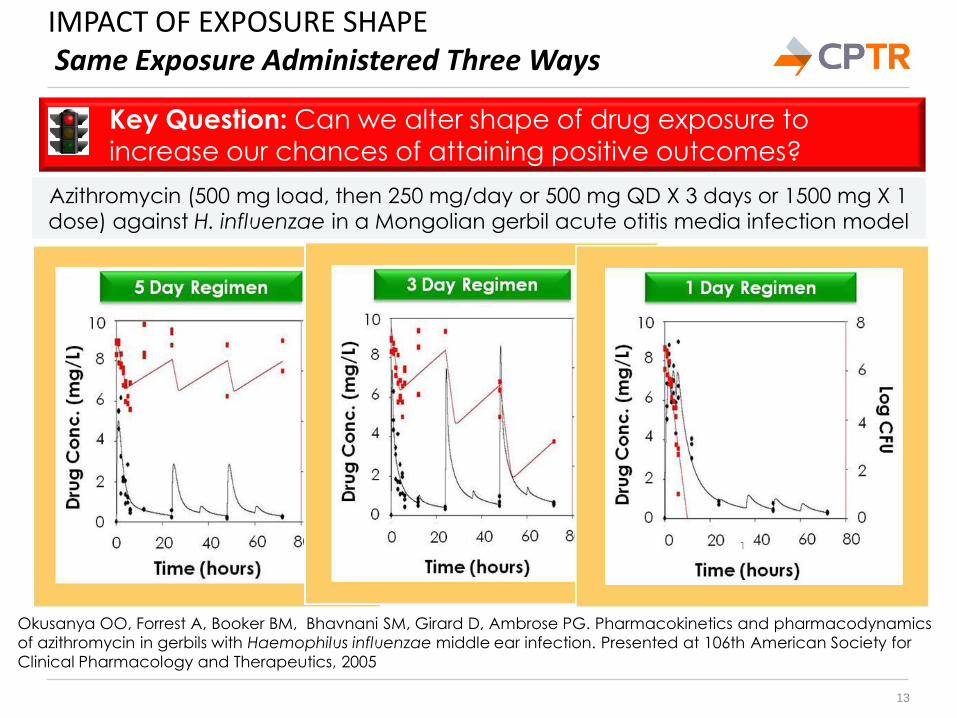
IMPACT OF EXPOSURE SHAPE Same Exposure Administered Three Ways
13
Okusanya OO, Forrest A, Booker BM, Bhavnani SM, Girard D, Ambrose PG. Pharmacokinetics and pharmacodynamics
of azithromycin in gerbils with Haemophilus influenzae middle ear infection. Presented at 106th American Society for
Clinical Pharmacology and Therapeutics, 2005
Key Question: Can we alter shape of drug exposure to increase our chances of attaining positive outcomes?
Azithromycin (500 mg load, then 250 mg/day or 500 mg QD X 3 days or 1500 mg X 1
dose) against H. influenzae in a Mongolian gerbil acute otitis media infection model
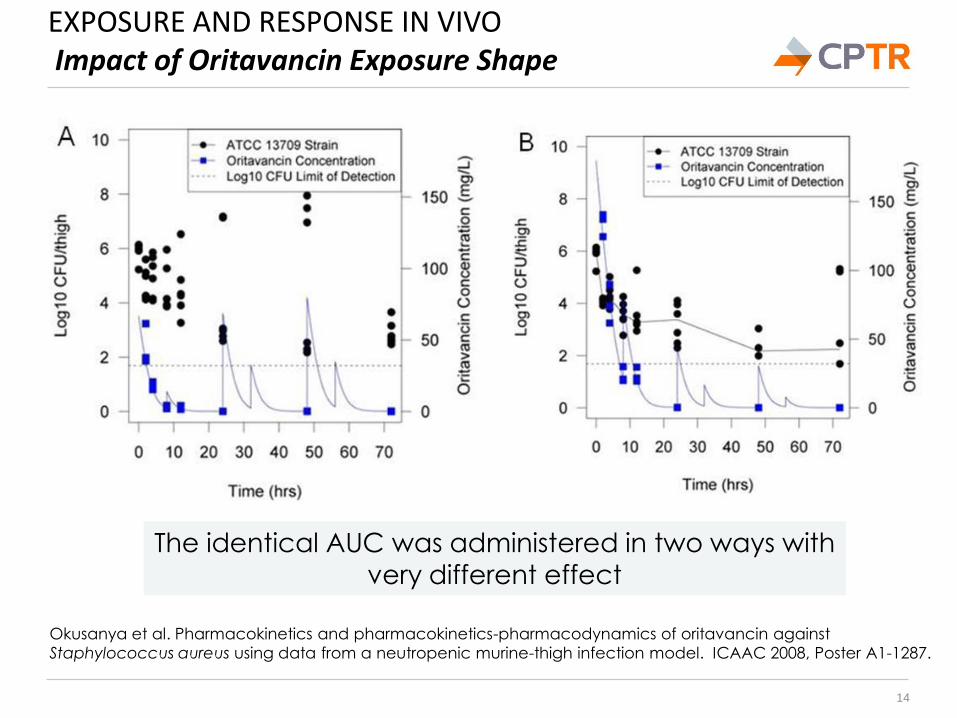
EXPOSURE AND RESPONSE IN VIVO Impact of Oritavancin Exposure Shape
14
Okusanya et al. Pharmacokinetics and pharmacokinetics-pharmacodynamics of oritavancin against
Staphylococcus aureus using data from a neutropenic murine-thigh infection model. ICAAC 2008, Poster A1-1287.
The identical AUC was administered in two ways with
very different effect
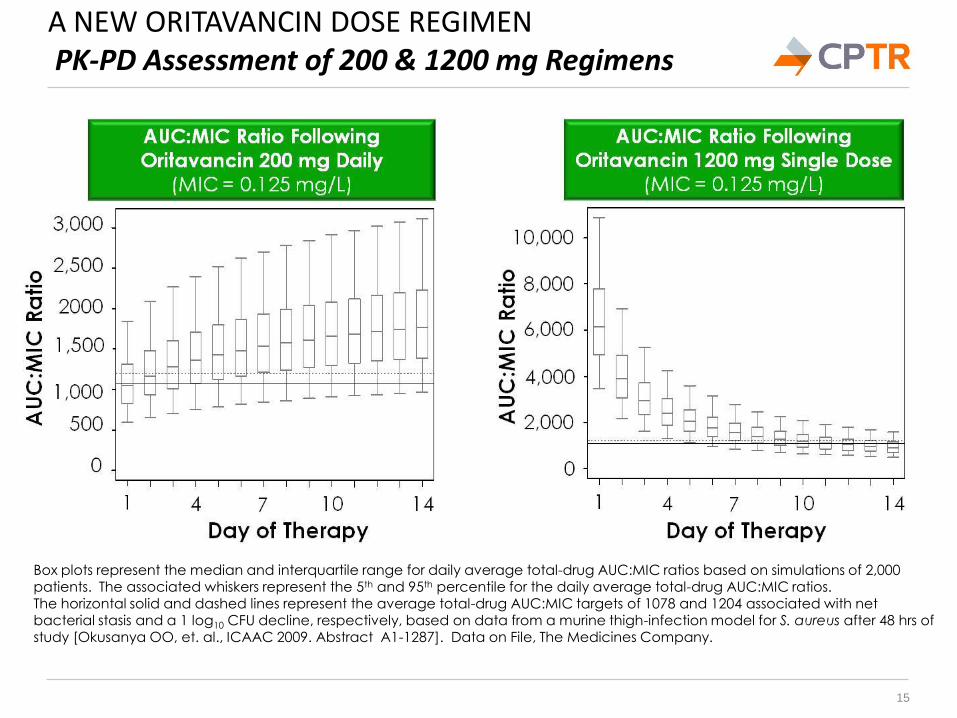
A NEW ORITAVANCIN DOSE REGIMEN PK-PD Assessment of 200 & 1200 mg Regimens
15
Box plots represent the median and interquartile range for daily average total-drug AUC:MIC ratios based on simulations of 2,000 patients. The associated whiskers represent the 5th and 95th percentile for the daily average total-drug AUC:MIC ratios. The horizontal solid and dashed lines represent the average total-drug AUC:MIC targets of 1078 and 1204 associated with net bacterial stasis and a 1 log10 CFU decline, respectively, based on data from a murine thigh-infection model for S. aureus after 48 hrs of study [Okusanya OO, et. al., ICAAC 2009. Abstract A1-1287]. Data on File, The Medicines Company.
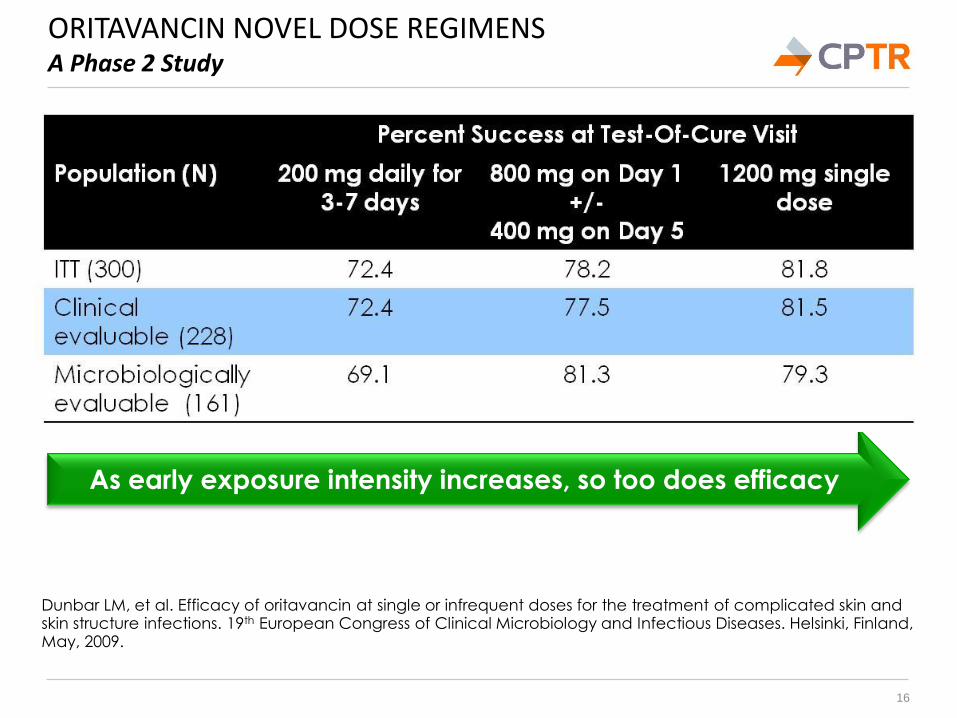
ORITAVANCIN NOVEL DOSE REGIMENS A Phase 2 Study
16
Dunbar LM, et al. Efficacy of oritavancin at single or infrequent doses for the treatment of complicated skin and skin structure infections. 19th European Congress of Clinical Microbiology and Infectious Diseases. Helsinki, Finland, May, 2009.
As early exposure intensity increases, so too does efficacy
PREVENTING RESISTANCE EMERGENCE Mission Impossible?
17
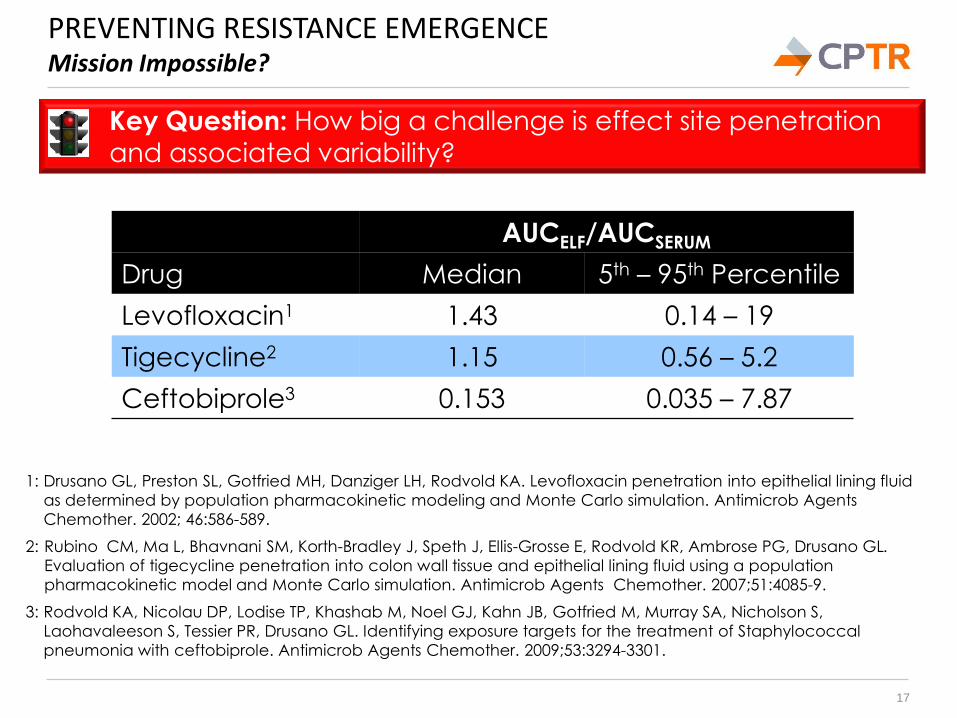
1: Drusano GL, Preston SL, Gotfried MH, Danziger LH, Rodvold KA. Levofloxacin penetration into epithelial lining fluid
as determined by population pharmacokinetic modeling and Monte Carlo simulation. Antimicrob Agents
Chemother. 2002; 46:586-589.
2: Rubino CM, Ma L, Bhavnani SM, Korth-Bradley J, Speth J, Ellis-Grosse E, Rodvold KR, Ambrose PG, Drusano GL.
Evaluation of tigecycline penetration into colon wall tissue and epithelial lining fluid using a population
pharmacokinetic model and Monte Carlo simulation. Antimicrob Agents Chemother. 2007;51:4085-9.
3: Rodvold KA, Nicolau DP, Lodise TP, Khashab M, Noel GJ, Kahn JB, Gotfried M, Murray SA, Nicholson S,
Laohavaleeson S, Tessier PR, Drusano GL. Identifying exposure targets for the treatment of Staphylococcal
pneumonia with ceftobiprole. Antimicrob Agents Chemother. 2009;53:3294-3301.
Key Question: How big a challenge is effect site penetration and associated variability?
AUCELF/AUCSERUM
Drug Median 5th – 95th Percentile
Levofloxacin1 1.43 0.14 – 19
Tigecycline2 1.15 0.56 – 5.2
Ceftobiprole3 0.153 0.035 – 7.87
PREVENTING RESISTANCE EMERGENCE Mission Impossible?
18
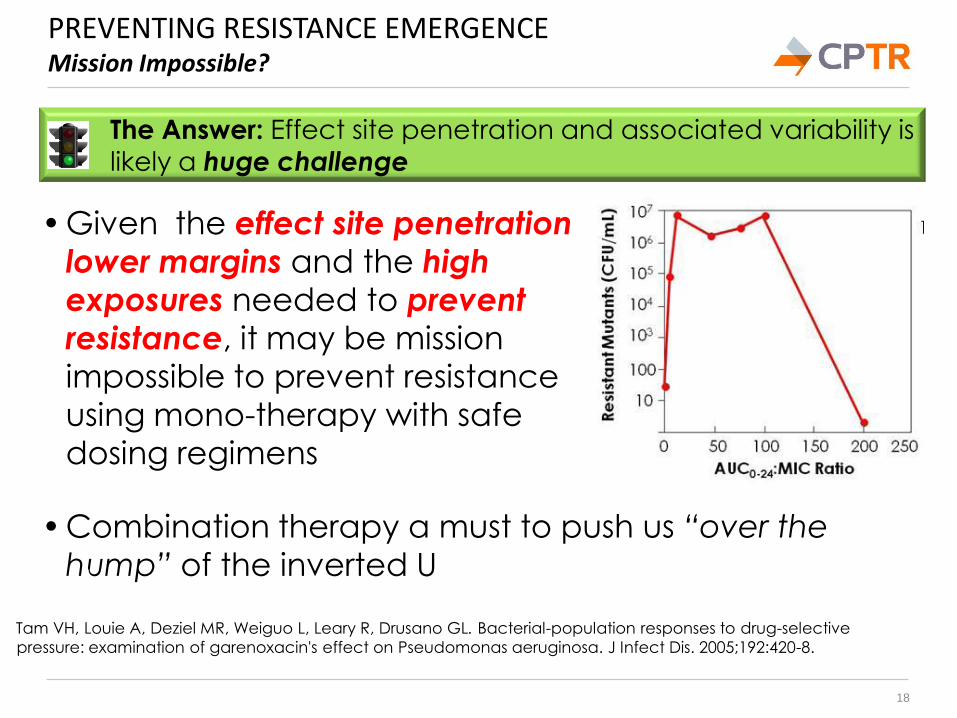
• Combination therapy a must to push us “over the
hump” of the inverted U
The Answer: Effect site penetration and associated variability is likely a huge challenge
• Given the effect site penetration
lower margins and the high
exposures needed to prevent
resistance, it may be mission
impossible to prevent resistance
using mono-therapy with safe
dosing regimens
Tam VH, Louie A, Deziel MR, Weiguo L, Leary R, Drusano GL. Bacterial-population responses to drug-selective
pressure: examination of garenoxacin's effect on Pseudomonas aeruginosa. J Infect Dis. 2005;192:420-8.
COMBINATION THERAPY Is The Answer as Simple as it Sounds?
19
Key Question: Should we be simply administering drug
combinations that are synergistic or at least additive?
• Traditionally, we think of antimicrobial interactions as
synergistic, additive or antagonistic
o While interesting, these categories miss the point
o Synergistic agents can have horrible activity and visa versa
• Vancomycin and rifampin are often antagonistic
o Rifampin wildly active but resistance emerges rapidly;
o Vancomycin prevents rifampin resistance emergence; and
o Together are a more active regimen than either alone
The Answer: What makes or breaks a regimen is not the
presence or absence of synergy but is regimen activity
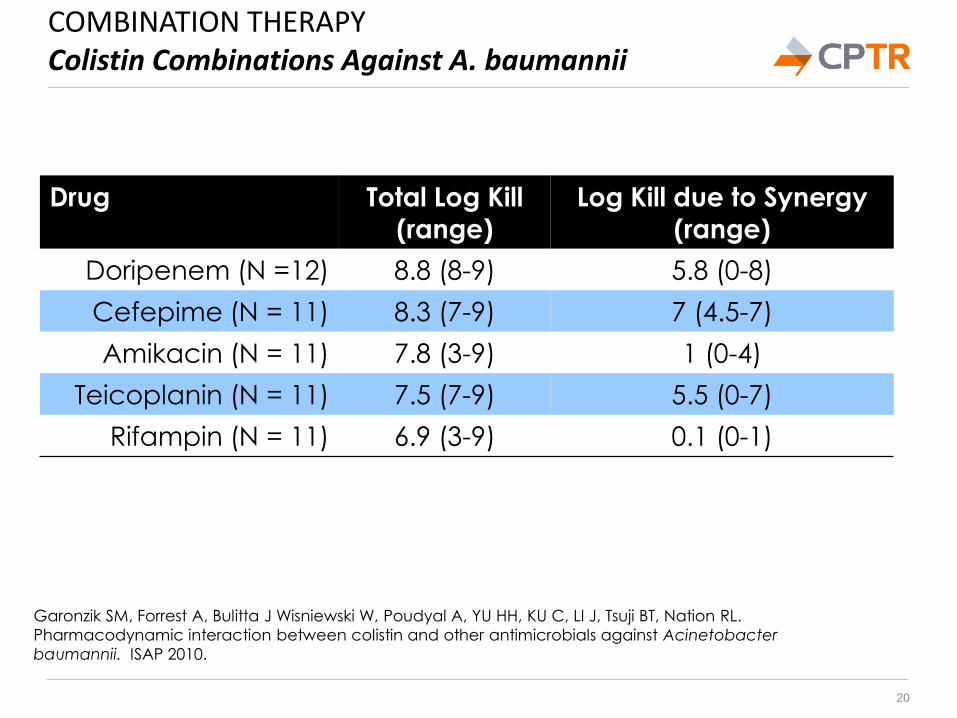
COMBINATION THERAPY Colistin Combinations Against A. baumannii
20
Drug Total Log Kill (range)
Log Kill due to Synergy (range)
Doripenem (N =12) 8.8 (8-9) 5.8 (0-8)
Cefepime (N = 11) 8.3 (7-9) 7 (4.5-7)
Amikacin (N = 11) 7.8 (3-9) 1 (0-4)
Teicoplanin (N = 11) 7.5 (7-9) 5.5 (0-7)
Rifampin (N = 11) 6.9 (3-9) 0.1 (0-1)
Garonzik SM, Forrest A, Bulitta J Wisniewski W, Poudyal A, YU HH, KU C, LI J, Tsuji BT, Nation RL.
Pharmacodynamic interaction between colistin and other antimicrobials against Acinetobacter
baumannii. ISAP 2010.
TAKE HOME MESSAGES It’s About the Magnitude, Shape and Duration of Drug Exposure!
• Drug exposure indexed to MIC, rather than the presence or absence of resistance determinants,
predicts response
o Think about magnitude of drug exposure when designing regimens for drug-resistant pathogens
o The trade-off may be, but not necessarily, more toxicity
• Think about manipulating drug exposure shape to take advantage of each drug’s PK-PD profile to provide:
o Best chance to maximize bacterial kill,
o Best chance to maximize positive clinical outcomes,
o Best chance to reduce spontaneous mutation, and
o Best chance to eliminate a pre-existing resistant
subpopulations
21
TAKE HOME MESSAGES It’s About the Magnitude, Shape and Duration of Drug Exposure!
• Relationships between drug exposure and resistance
emergence are U-shaped and time-dependent
o Just don’t think about magnitude and shape, but also
therapy duration
o Consider front-loading exposure and shortening therapy for
antibiotics with high resistance potential
• Effect site penetration variability is high and often will
necessitate the need for combination therapy
• Consider regimens, not simply drugs
o Consider multiple, combination administration routes
o Consider combining multiple new active drugs rather than
one new active drug with less active old ones
22
23
THANK YOU FOR YOUR ATTENTION Questions, Comments or Wise Remarks?





























