Embed Size (px)
Citation preview

Vascular Intervention
, Placement of Mechanically Detachable 1 Spiral Coils in the Endovascular Treat- 1 ment of Intracranial Aneurysms. Work in Progress1
lsil Saatci, MD H. Saruhan Cekirge, MD Murat M. Firat, MD Ferhun Balkanci, MD Tuncalp Ozgen, MD Vural Bertan, MD Suleyman Saglam, MD
Index terms: Aneurysm, intracranial, 1731.73,1753.73 Aneurysm, therapy, 1731.757,1753.757 Interventional proce- dures, technology
JVIR 1996; 7:75-79
Abbreviations: GDC = Guglielmi de- tachable coil, MDS = mechanically detach- able spiral coil
'From the Departments of Radiology (I.S., H.S:C., M.M.F., F.B.) and Neurosurgery (T.O., V.B., S.S.), Hacettepe University Hospital, Sihhiye, Ankara 06100, Turkey. Received January 30,1995; revision re- quested April 3; revision received July 17; accepted July 25. Address correspon- dence to I.S.
O SCVIR. 1996
PURPOSE: To determine the usefulness of mechanically detachable spiral tungsten coils (MDSs) in the endovascular, endosaccular oc- clusion of intracranial aneurysms. MATERIALS AND METHODS: Anterior communicating artery aneu- rysms shown at angiography in two patients and a basilar tip aneu- rysm shown in one patient were treated with MDSs. RESULTS: In the basilar artery aneurysm, eight coils were deliv- ered. Two additional coils were placed at 3 months because of filling of the residual aneurysm neck. Angiography at 1 year showed no re- canalization. The smaller aneurysm in the anterior communicating artery was totally occluded by a single coil. Angiography at 6 months showed no recanalization. The other aneurysm was occluded by two coils, with a small amount of residual filling. A third coil was with- drawn before detachment. The patient had aspiration pneumonia and electrolyte imbalance, but he was in stable condition 3 weeks later and was discharged. CONCLUSION: The pliable, soft, retrievable MDS system provides instantaneous release of a spiral coil.
TREATMENT of intracranial aneu- rysms with preservation of the par- ent artery may be performed by us- ing either open surgical clipping or an endovascular, endosaccular tech- nique (I) , but the endovascular treatment has not yet been proved to be as effective as the surgical treat- ment. The endovascular approach to aneurysm occlusion has been limited to balloon embolization (2). Recent development of detachable coils has increased the number of alternatives available for the endovascular thera- peutic management of intracranial aneurysms. One recently described retractable coil system is the Gugli- elmi detachable coil (GDC) (Target Therapeutics, San Jose, Calif) (3). The detachment mechanism of the GDC system is controlled with an electric current that induces detach- ment by means of electrolysis, a pro- cess that requires a variable amount
of time. Another mechanical system that allows immediate but still con- trollable detachment has recently been developed. We describe the treatment of three intracranial an- eurysms with mechanically detach- able spiral coils (MDSs) (Balt Extru- sion, Montmorency, France), with midterm follow-up.
1 MATERlALS AND METHODS Three patients, two with anterior
communicating artery aneurysms and one with a basilar tip aneurysm, were first seen with subarachnoid hemorrhage and underwent treat- ment with endovascular, endosaccu- lar occlusion with MDSs. The pa- tients were men aged 31,44, and 54 years. They had no neurologic defi- cits. In the patient with a basilar tip aneurysm, an attempt at surgical clipping had failed. In the remaining

76 Journal of Vascular and Interventional Radiology
January-February 1996
a.
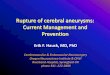
Figure 1. (a) Illustration of the MDS system; 1 = pusher attached to the spiral coil, 2 = transparent introducing tube, 3 = Y-connector, 4 = MAG 3-Fl2-F catheter, and 5 = spiral coil. (Fig la courtesy of Balt.) (b) Illustration of a magnified view of the spiral coil being attached to the pusher. The small ball at the end of the coil sits within the open center of the leading end of the pusher. The coil and the pusher are then pulled back into the transparent introducing tube as a unit.
two patients with anterior communi- cating artery aneurysms, no previ- ous surgical intervention had been ~erformed: the decision to use MDSs h a s made 'on the basis of patients7 preferences after full explanation of the alternatives. Use of the MDS system was approved by the investi- gational committee of the Ministry of Health and the ethical board at our hospital.
Diagnostic angiograms showed a wide-neck, 1.5 x 2-cm aneurysm at the tip of the basilar artery and two anterior communicating artery an- eurysms that were 0.6 and 1 cm in diameter. The patients were treated within 3 days after admission.
The procedures were performed with patients under general anes- thesia. A 7-F introducer sheath was placed into the right common femo- ral artery, and a 6-F guiding cath- eter was used in all patients. A MAG microcatheter (Balt) with a 3- F shaft tapering to 2 F at the lead- ing end (3-Fl2-F) was included in the introduction system for the MDSs and was introduced coaxially. Road- mapping guidance was used to ad- vance the microcatheter tip into the sac of the aneurysm. A 0.016-inch gold-tip micro-glide wire (Terumo, Tokyo, Japan) was used when neces- sary.
The mechanical detachment sys- tem is composed of an MAG 3-Fl2-F or MAG 5-F catheter, a pusher, a Y-adaptor, and a transparent intro- ducer tube (Fig la), which are used to place the spiral tungsten coils. The coils are 2-11 mm in diameter and range from 25 to 150 mm in
length when straightened. The pri- mary helix diameter is 0.36 mm (0.014 inch) in coils of all sizes. The spiral, with a tiny ball at one end, is attached to the pusher (Fig lb); a magnifying glass may be needed for the attachment process. The con- nected spiral coil and pusher are pulled back into the transparent in- troducer tube as a unit. The intro- ducing tube is used to load the coil into the microcatheter, the tip of which has been previously placed in the aneurvsm sac. There are two radiopaque markers at the leading end of the microcatheter. The coil at- tached to the pusher may be ad- vanced until the marker on the lead- ing end of the pusher is superim- posed on the proximal marker of the microcatheter. When necessary, the spiral coil can be easily retrieved be- fore the superimposition of these two markers, and it may be pushed forward again. At the point of super- imposition of the markers, the spiral coil is released with slight rotational movement of the pusher, aided by a torque device. After detachment of the first coil, it may be difficult to vi- sualize the coil-pusher junction of second and subsequent coils within the mesh. Similar to the mechanism of the GDC system, the trailing radiopaque markers (outside the an- eurysm) allow precise placement of the coil-pusher junction within the aneurysm, even when the actual junction cannot be visualized. The same pusher can be used multiple times by mechanically attaching new spiral coils.
Care was taken to fill the dome of
the aneurysm with coils first and to provide bridging of the mesh of the coils across the neck. Before the re- lease of each of the spirals, the posi- tion and proper coiling of the spirals in the sac and the filling of the aneu- rvsm were ensured bv means of con- trast-material injection at fluoros- copy to guard against impingement on or protrusion of the coils into the parent artery or adjacent arteries.
Early detachment, which may cause coils to become trapped within the catheter, did not occur.
The patients were given 5,000 IU of heparin, administered intrave- nously, when the coaxial system was introduced. Administration of a 2,500-IU dose was repeated every hour during the procedure. Intrave- nous heparin was continued, with administration of a total dose of 500 IUkg in a 24-hour period during the first 3 days to avoid any thromboem- bolic complications. The patients continued to take oral phenytoin for seizure prophylaxis, a therapy that was started at the time of admis- sion.
RESULTS In the basilar artery aneurysm,
eight coils were delivered, for a total length of 89 cm (9 x 150 mm, 7 x 100 mm, 5 x 150 mm, 4 x 120 mm [n = 3],3 x 80 mm, 3 x 50 mm). The im- mediate posttreatment angiogram revealed minimal amounts of con- trast material in the neck of the an-

Saatci et a1 77 Volume 7 Number 1
Figure 2. Wide-necked basilar artery aneurysm. (a) Left vertebral angiogram in Towne projection shows the basilar tip aneu- rysm. (b) Same projection as in a shows occlusion of the aneurysm with minimal filling of contrast material at the base of the an- eurysm. (c) Twelfth-month control angiogram in Towne projection (magnified view [x2]) shows no filling of contrast material.
Figure 3. Anterior communicating artery aneurysm. (a) Left internal carotid angiogram in left oblique Towne projection shows the aneurysm. (b) Angiogram obtained by using the same projection after coil occlusion shows that filling by contrast material adjacent to the aneurysm on the left, at the junction of A1 and A2 segments, is not residual filling but a vascular loop (arrow- head). (c) Sixth-month control angiogram obtained in the same projection (magnified view [x1.51) shows no recanalization. The right A2 segment was filled with contrast material at the right internal carotid injection (not shown).
eurysm (Fig 2). The posttreatment clinical course was uneventful. The follow-up angiogram obtained a t 3 months showed slight enlargement and continued filling of the residual aneurysm neck. Two additional coils were packed in the aneurysm neck. An angiogram obtained a t 1 year showed no recanalization (Fig 2c), and the patient was considered to be cured.
The smaller aneurysm in the an- terior communicating artery was to- tally occluded by a single 3 x 80-mm coil (Fig 3a, 3b). The patient was discharged a week after the proce-
dure in good condition. The control angiogram obtained a t 6 months showed no recanalization (Fig 3c).
The other aneurysm in an ante- rior communicating artery was filled by two coils, for a total length of 22 cm with a small amount of residual filling. During placement of a third 3 x 50-mm coil, i t was seen to extend into the right A1 segment, and the coil was withdrawn before detach- ment. The procedure was termi- nated without complication. The pa- tient, however, had aspiration pneu- monia and electrolyte imbalance; he was discharged 3 weeks later in
stable condition. A follow-up angio- gram will be obtained a t 6 months.
DISCUSSION Endovascular, endosaccular oc-
clusion of intracranial aneurysms of- fers several advantages compared with direct surgical clipping. Occlu- sion allows preservation of the par- ent artery. Also, craniotomy and brain manipulation are avoided. The medical condition of the patient does not affect the timing or performance of the procedure, which may be used in patients in whom direct surgical

78 Journal of Vascular and Interventional Radiology January-February 1996
clipping has failed. Until recently, the only method of endovascular an- eurysm occlusion has been balloon embolization (2,4). The fragile wall of the aneurysm, however, undergoes stress while it adapts to the shape of the balloon. Thus, there is a risk of aneurysm rupture (4,5). Other risks include rupture of the balloon, in- ability to navigate the balloon into the proper position, and migration of the balloon after placement into clot within the aneurysm (2,4,6).
Conventional coils not directly at- tached to a coil pusher take the place of the balloons in endosaccular occlu- sion of aneurysms (7). These coils, however, cannot be retrieved once they are released into an aneurysm or blood vessel. Therefore, the re- leased coil may protrude into a par- ent vessel (7,8) and cannot be reposi- tioned or retracted when it is un- stable in a blood vessel (9).
Detachable coils have been devel- oped recently that offer less trau- matic and safer treatment of intra- cranial aneurysms. The GDC is a re- tractable coil that is detached by means of electrolysis; it has been in use since 1990 and has had promis- ing early results (3,5,10). In the GDC system, the coil is separated from the coil-pusher segment by means of electrolysis; the uninsulated, most distal portion of stainless steel core wire dissolves with the application of direct electric current, and the coil is liberated. Separation of the initial coils may require less time (average, 1-2 minutes), but as more coils are placed, more time is required for separation with electrolysis (5). Soft- ness, retrievability, and atraumatic detachment are the reported safety features of the GDC (10). Thrombo- sis that takes place during detach- ment of the coils by electrolysis is considered to contribute to the achievement of complete aneurysm occlusion (10). Guglielmi et a1 (10) reported the results of endosaccular treatment of posterior circulation an- eurysms with GDCs in a multicenter study. The morbidity and mortality were 4.8% and 2.4%, respectively.
Mechanically detachable coils have been available for only a short time. Apart from an experimental study by Marks et a1 ( l l ) , to our
knowledge there are no published clinical data regarding mechanically detachable coils. Marks et a1 (11) re- ported the results of in vitro and in vivo animal testing of coils recently developed by Target Therapeutics. They emphasized the immediate re- lease feature of the mechanically de- tachable coil design and disputed the role of electrothrombosis pro- vided by the GDC system in the oc- clusion of the aneurysmal sac. Be- cause the endovascular-coil proce- dures are generally performed with systemic anticoagulation with hep- arin to impede blood-clot formation at the time of placement, they doubted whether there was an ad- vantage to having thrombus form at the time of each coil placement.
The MDSs used in this study are constructed of tungsten. Thev are - supple and easily recoil in the aneu- rysm sac without displacing the tip of the microcatheter during the pushing action. Their excellent radiopacity allows for easy fluoro- scopic monitoring. We found that spiral coils can be retracted after partial ejection. Therefore, if an in- correct coil size is chosen or if a coil is in an unstable nosition in the an- eurysm sac or blood vessel, the coil can be removed before it is released. The spiral coils are nonferromag- netic and thus are compatible with magnetic resonance imaging. The mechanical detachment mechanism offers immediate but controllable re- lease. No waiting period is required like with the GDC system. The rela- tive importance of current-induced thrombosis in the obliteration of an aneurysm sac with a GDC is still controversial, because it is not clear how much of the observed thrombo- sis is the result of electrothrombosis and how much is due to vascular stasis caused by the packing of coils into a vascular space (11).
Although, to our knowledge, no long-term results of endovascular coil occlusion have been published, we do know that aneurysms treated with GDCs may recanalize (12). If recanalization is seen on follow-up angiograms, the technique still of- fers the same opportunity to re-treat residual aneurysm as is offered with the MDS system. Larger series will
be needed to compare the recanali- zation rate of the MDS system with that of the GDC svstem. Recanaliza- tion rates of aneurysms treated with surgical clipping also are not well known, primarily because midterm and long-term follow-up angiogra- phy are not routinely performed.
In conclusion, the pliable, soft, re- trievable MDS system provides in- stantaneous release of a spiral coil. It may eventually be used as an al- ternative in the treatment of endo- vascular aneurysm.
References 1. Higashida RT, Halbach W, Hie-
shima G. Endovascular therapy of intracranial aneurysms. In: Vinuela F, Halbach W, Dion JE, eds. Inter- ventional neuroradiology: endovas- cular therapy of the central nervous system. New York, NY: Raven, 1992; 87-106.
2. Higashida RT, Halbach W, Dowd CF, Barnwell SL, Hieshima GB. Intracranial aneurysms: intenen- tional neurovascular treatment with detachable balloons-results in 215 cases. Radiology 1991; 178:663-670.
3. Guglielmi G, Vinuela F, Dion J , Duckwiler G. Electrothrombosis of saccular aneurysms via endovascu- lar approach. 11. Preliminary clini- cal experience. J Neurosurg 1991; 7553-14.
4. Moret J . Endovascular treatment of berry aneurysms by endosaccular occlusion. Acta Neurochir 1991; 53(suppl):48-49.
5. Guglielmi G. Endovascular treat- ment of intracranial aneurysms. Neuroimag Clin North Am 1992; 2:269-278.
6. Higashida RT, Halbach W, Cahan CD, Hieshima GB, Konishi Y. De- tachable balloon embolization ther- apy of posterior circulation intracra- nial aneurysms. J Neurosurg 1989; 71:512-519.
7. Casasco AE, Aymard A, Gobin P, et al. Selective endovascular treat- ment of 71 intracranial aneurysms with platinum coils. J Neurosurg 1993; 79:3-10.
8. Knuckey KW, Haas R, Jenkins R, Epstein MH. Thrombosis of diffi- cult intracranial aneurysms by the endovascular placement of plati- num-Dacron microcoils. J Neuro- surg 1992; 77:43-50.
9. Nancarrow PA, Fellows KE, Lock JE. Stability of coil emboli: an in vitro study. Cardiovasc Intervent Radio1 1987; 10:226-229.

Saatci et a1 79 Volume 7 Number 1
10. Guglielmi G, Vinuela F, Duckwiler 11. Marks MP, Chee H, Liddell RP, et G, et al. Endovascular treatment al. A mechanically detachable coil of posterior circulation aneurysms for the treatment of aneurysms and by electrothrombosis using electri- occlusion of blood vessels. AJNR cally detachable coils. J Neurosurg 1994; 15:821-827. 1992; 77:515-524. 12. Houdart E, Casasco A, George B,
Cophignon J , Merland JJ. Our ex-
perience in therapeutic manage- ment of 159 intracranial aneurysms by GDC coils (abstr). Neuroradiol- ogy 1994; 36(suppl 1):82.