Embed Size (px)
Citation preview

Continuing EducationHOURS2.1
32 AJN ▼ December 2009 ▼ Vol. 109, No. 12 ajnonline.com
By Kathleen A. Whitney, BSN, RN, CEN
Placental Site Trophoblastic TumorA case demonstrates the importance of looking beyond a positivepregnancy test for corroborating clinical manifestations.

[email protected] AJN ▼ December 2009 ▼ Vol. 109, No. 12 33
of being there for the two children I already had.Afterward, I felt compelled to share the knowledgeI had gotten from late nights reading over case stud-ies and research articles in the hope that I could shedlight on this rare and little-known disorder.
CASE IN POINTIn preparation for the smallpox vaccination that wasrequired before my military deployment, I was givena qualitative pregnancy blood test for beta humanchorionic gonadotropin (hCG) and received posi-tive results (see Using Serum hCG Tests To DetectPregnancy1). I was 34 years old. I’d been pregnanttwice and given birth twice, most recently sevenmonths before, and I’d recently stopped nursing myinfant. I was on day 13 of my first menstrual periodsince my most recent pregnancy, and the flow wasquite heavy. A follow-up quantitative study showed mybeta hCG trending downward, from 42 to 35 mIU/mLover a period of five days (below 5 mIU/mL is con-sidered normal, or not pregnant).1 My bleedingde creased over a period of two weeks, and I waspre sumed to have had a complete spontaneous abor-tion. Dilation and curettage were not performed.
Within 12 weeks of the miscarriage, however, Ibegan to experience fatigue and mild nausea. I hadalready been deployed, and the physician at the mil-itary base ordered another quantitative pregnancyblood test, which showed my beta hCG level to be544.5 mIU/mL. When told that I was pregnant again,I knew it wasn’t possible. I hadn’t had intercoursesince military deployment had separated me from myhusband almost four months before. I was havingintermittent spotting but hadn’t had a normal men-strual cycle since the miscarriage. I had no fever orcramping, so it was unlikely that I’d retained anyproducts of conception from the miscarriage.
A repeated quantitative test one week latershowed my beta hCG trending downward again, to510.3 mIU/mL. A pelvic ultrasound was negative for
Nurses have learned to suspect the veracity ofsuch statements as, “There’s no way I couldbe pregnant.” It’s not that we’re overly cyni-
cal, but we have to maintain enough suspicion to keepour patients safe—and the safest course of action isto assume that every female patient of childbearingage is pregnant until proven otherwise. But when wereceive positive results of a pregnancy test given to apatient who says pregnancy is an impossibility, shouldwe automatically assume that she’s naive or has beenless than honest with us?
I’d never heard of placental site trophoblastictumor (PSTT) until I received that diagnosis in 2006.My background was in emergency nursing, not oncol -ogy or gynecology. As far as I knew, the only formsof trophoblastic disease were hydatidiform mole andchoriocarcinoma. As an ED nurse, I’d seen morethan one young woman come through triage swear -ing that she’d never been sexually active and couldn’tpossibly be pregnant, only to be rushed into labor anddelivery, where she’d give birth to a full-term infantwithin the hour.
When I received a positive result on my pregnancytest, although I knew I couldn’t be pregnant, I alsoknew that my physician would probably find my ex -planation suspect. I was stationed on a military post,where husbands and wives were separated by lengthydeployments. No one wanted to admit to infidelity.To their credit, my military physicians never insinu -ated that I was being untruthful and seemed to takethe situation seriously.
When given the diagnosis of PSTT, I immediatelystarted doing research. Although my physician reas -sured me that there was a low risk of metastasis andthat PSTT was easily curable, the studies I read wereless reassuring. There were many contradictionsamong them and little agreement as to how to pre-dict the risk of metastasis.
It was a tough decision, but in the end, I sacrificedmy dream of a large family to improve my chances
When the author received a positive pregnancy test at a time she knew she couldn’t pos-sibly be pregnant, it caused her to rethink the healthy skepticism her years of nursinghad engendered. This case reminds nurses that positive pregnancy tests can result from
medical conditions other than pregnancy, including various cancers, such as placental site tropho-blastic tumor, the focus of this article. It also serves as a reminder that any positive pregnancy testthat isn’t accompanied by corresponding clinical evidence needs to be evaluated further.
OVERVIEW

retained products of conception and ectopic preg-nancy but revealed an indistinct endometrial outline.(Endometrial and myometrial boundaries are normallydistinct.) I was referred to a gynecologic oncologist,who performed an endometrial biopsy. Pathologicstudies revealed scattered trophoblastic cells thatstained positive for hCG, a finding consistent with apresumptive diagnosis of PSTT, which was sup-ported by dilation and curettage.
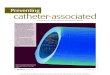
UNDERSTANDING THE TROPHOBLASTThe human blastocyst forms four to five days afterfertilization, travels down the fallopian tube, andimplants in the uterus (Figure 1). It’s during preim-plantation blastocyst formation that cell differenti-ation begins. The blastocyst comprises an inner cellmass, which becomes the embryo and extraembry-onic tissue, and an outer layer of cells known as thetrophoblast, which forms the placenta.
The trophoblast can be divided into three types ofcells: cytotrophoblasts, the mononuclear cells that
form the inner layer of the trophoblast and differ-entiate into all other trophoblastic cells; the syncy-tiotrophoblasts, individual cells with multiple, diversenuclei, which create the trophoblast’s continuousouter layer and, ultimately, the chorionic villi, allow -ing fetal and maternal circulations to exchange gasand nutrients without mixing; and intermediatetrophoblasts, invasive cells that leave the placentato penetrate and remodel uterine spiral arteries, allow -ing for increased blood flow to the placental bed.It’s the intermediate trophoblasts that are primarilyresponsible for PSTT formation.2 Their prolifera-tive and invasive nature, which is strictly controlledin a normal pregnancy, is similar to that of manymalignant cells. Research suggests that in PSTT theintermediate trophoblasts have an abnormal expres -sion of cyclins, particularly cyclin A, and the p53protein.3
WHAT IS PSTT?Gonadotropic disease, a family of benign and malig-nant tumors characterized by abnormal chorionictissue growth, includes hydatidiform mole, invasivemole, partial hydatidiform mole, choriocarcinoma,and PSTT.4 PSTT, the rarest of these, occurs whenintermediate trophoblastic cells invade the myo -metrium at the site of implantation.3, 5, 6
34 AJN ▼ December 2009 ▼ Vol. 109, No. 12 ajnonline.com
PSTT can occur after any normal, aborted, ormolar pregnancy, although one study found that it’smore likely to occur after pregnancy with a femalefetus.7 As of 2000, fewer than 100 cases of PSTThad been reported in the medical literature, and only72 of those reports included clinical and pathologicdetails.7
Because of its rarity and vague symptoms, PSTTcan be difficult to diagnose. Levels of beta hCG areusually lower than in choriocarcinoma.6, 8 The mostcommon symptoms of PSTT are irregular vaginalbleeding and amenorrhea, although uterine enlarge-ment has also been reported as a primary symptom.6, 9
A chart review of all PSTT cases recorded in theNew England Trophoblastic Disease Center databasebetween 1982 and 1999 (13 cases) found the mean ageat diagnosis to be 31 years.10
Overall, imaging studies of PSTT have been non-specific, and the majority of cases are diagnosed onthe basis of curettage specimens.11 Ultrasonographyor magnetic resonance imaging, however, may be useful
in distinguishing between hypovascular PSTT and thehypervascular type,12 which carries an increased riskof massive hemorrhage with surgery (such as dila-tion and curettage or uterine resection).13
In a 1998 case in Norway, PSTT was transmit-ted from mother to infant. The infant died at fivemonths of age from multiorgan failure, less thantwo months after the onset of symptoms. An autopsyrevealed multiple tumors in the infant’s lungs, liver,mesentery, and kidney. Shortly thereafter, the motherwas diagnosed with PSTT. Curettage specimenswere found to be of the same origin as the infant’stumors.14
TREATMENT AND PROGNOSISUnlike other forms of gonadotropic disease, PSTTgrows slowly and is slow to metastasize.15 Earlydiagnosis and treatment are associated with a lowrate of metastasis.6 Its slow development, however,makes PSTT resistant to chemotherapy, which tar-gets rapidly dividing cells.9 For this reason, PSTT isusually treated surgically, most frequently withhysterectomy—either partial (removal of the uterusalone), total (removal of the uterus and cervix), orradical (removal of the uterus, cervix, fallopian tubes,ovaries, oviducts, top portion of the vagina, and lymphnodes)—although some women choose instead to
PSTT is usually treated surgically, most frequently with hysterectomy—although
some women choose instead to have a local uterine resection in order to retain
childbearing capability.

[email protected] AJN ▼ December 2009 ▼ Vol. 109, No. 12 35
have a local uterine resection in order to retain child -bearing capability. (Prior to resection, tumor bound-aries are identified with magnetic resonance imagingor other imaging technology.13)
Reported rates of metastasis vary greatly, from aslow as 14%9 to as high as 53%.6 Metastatic PSTTcan be unpredictable, aggressive, and difficult to treat,even with intensive multimodal therapy.9 The mostcommon sites of metastasis are the lung and vagina,although metastasis to the lymph nodes, brain, liver,ovary, kidney, pancreas, and bladder have also beenreported.15 Metastasis is treated aggressively witha multidrug regimen of etoposide, methotrexate,dactinomycin, cyclophosphamide, and vincristine.Although this drug combination is widely acceptedas the most effective regimen for treating metastaticPSTT, in one study of seven patients it had a complete
response rate of only 28%.16 Feltmate and colleagueshave reported on cases in which metastasis wastreated effectively with brachytherapy and (in onecase) with external beam radiation therapy.10 In atleast one other case of metastatic PSTT, external beamradiation therapy succeeded in achieving remissionafter both surgery and multiagent chemotherapy hadfailed. Although data on the use of radiation therapyto treat PSTT are limited, it may be considered forlocal tumor control and palliative care.9
Like other forms of gonadotropic disease, whencaught early, PSTT has an excellent prognosis. Nev -ertheless, all patients who achieve PSTT remissionrequire lifelong follow-up, usually taking the formof serial serum beta hCG monitoring.
There is some debate over which factors areprognostic in the course of PSTT. Although many
FIGURE 1. Blastocyst at six days’ gestation. In a normal pregnancy the trophoblasts (the cells on theoutside wall of the blastocyst) attach to the endometrium and burrow into the uterine wall. Eventually theydevelop into the placenta. In rare cases, after a pregnancy (regardless of whether it resulted in a birth oran abortion) trophoblasts can infiltrate the myometrium and grow into a PSTT. Illustration by Anne Rains.
Blastocyst
Embryoblast
Cytotrophoblast
Uterine wall
Endometrium
Myometrium
Fibrinoid material
Syncytiotrophoblast

clinicians use the International Federation of Gy -necology and Obstetrics staging score or the WorldHealth Organization prognostic score, some authorsclaim they’re irrelevant to PSTT.5, 6 Two factors com-monly used as prognostic indicators are the elapsedtime from antecedent pregnancy to diagnosis, withintervals of two years or more said to indicate poorprognosis, and the mitotic rate of the tumor (thatis, the proportion of tumor cells undergoing mitosis),with mitotic counts of more than five mitoses per10 high-power fields said to correlate with poor out-come.10, 17
NURSING INTERVENTIONSBecause PSTT is a rare condition with which fewpatients are familiar, patient education is paramount.Inform patients of the treatment choices availableas well as the benefits and risks of each. Encouragethem to discuss all viable options with their physi-cian. Stress the importance of lifelong follow-upwith serum beta hCG monitoring.
As with any cancer diagnosis, providing psy-chosocial support is a crucial nursing intervention.Although PSTT is easily treated in most cases, can-cer is always a life-changing event. Ask patients whattypes of social support are available to them. Reassurethem that this type of cancer has a low rate of metas-tasis when detected in its early stages.
Because patients with PSTT tend to be of child-bearing age, and first-line treatment includes hysterec-tomy, be open to listening to patients’ concerns aboutfamily planning and help them explore their options.If a patient is adamant about retaining her fertility,encourage her to discuss the possibility of uterineresection with her physician. Be sure that she under-stands the risks that this procedure carries, includingthe likelihood that hysterectomy will be necessary ifshe fails to achieve remission through the resection.
Because chemotherapy and radiation are not first-line treatments for PSTT, related education tends notto be useful at diagnosis and may be overwhelming tothe patient. After surgical treatment, patients requirepain control, wound care to prevent infection, andencouragement of early ambulation to reduce the riskof postsurgical complications.
A FAVORABLE OUTCOMEAfter I received a definitive diagnosis of PSTT, I wasscheduled for a total hysterectomy and lymph noderesection, which was performed in January 2007,little more than a year after the antecedent pregnancy.Pathologic examination of the uterus showed a 2.5-cmtumor with some extension into the lymphovascularspace, but my lymph nodes were negative for metas-tasis. Within one month of surgery, my beta hCG lev-els had trended downward, reaching 1.9 mIU/mL(meaning negative for disease). Two years after sur-gery, I am disease free with negative results on serumbeta hCG testing.
Under normal circumstances, hCG is secreted bythe placenta during pregnancy. This article has exam-ined one condition, PSTT, that can cause beta hCGlevels to rise. Positive serum beta hCG results can alsobe produced by other forms of gonado tropic disease;other germ-cell cancers; cancers of the lung, liver, andpancreas; as well as by anticonvulsant, antiparkin-sonian, hypnotic, and phenothiazine drugs. A possi-ble cause of false-positive serum beta hCG results is aphenomenon known as “phantom hCG,” which canoccur when an hCG assay is not specific for hCG orbeta hCG but detects a wide range of hCG-relatedmolecules that are not indicative of pregnancy. Sus -pected false-positive results should be followed upwith a urine hCG test because the urine test targetsthe beta-core fragment, or the terminal degradationproduct, of hCG.4 Any case in which serial beta hCGtesting doesn’t conform to the normal pattern, orany positive result that isn’t accompanied by corre-lating clinical evidence, should be further evaluated
36 AJN ▼ December 2009 ▼ Vol. 109, No. 12 ajnonline.com
USING SERUM hCG TESTS TODETECT PREGNANCY
Human chorionic gonadotropin, or hCG,is a glycoprotein secreted shortly after
conception by trophoblastic cells and, later,by the placenta. Its function is to preventdegeneration of the corpus luteum. In theblood of nonpregnant women ages 18 to 40,beta hCG is normally present at a level below5 mIU/mL.1 In a normal single-gestation preg-nancy, levels rise six to 18 days after ovu-lation (when they can be detected in urine),doubling every other day until they peak atabout 10 weeks’ gestation, and then slowlydecline from a median level of 60,000mIU/mL to about 12,000 mIU/mL by week20, remaining relatively constant until deliv-ery. (Note that levels vary widely, and mul-tiple gestation raises levels 30% to 50%.)The hCG glycoprotein consists of an alphaand beta subunit, the latter being the mostsensitive, and therefore most commonlyused, marker of pregnancy.
Pregnancy tests can be either qualitative,providing a positive or negative answer, orquantitative, indicating the level of betahCG present in the blood. The quantitativebeta hCG test, drawn serially, is most use-ful because it indicates whether levels arerising at an appropriate rate or declining,as they would in a miscarriage or with fetaldeath.

[email protected] AJN ▼ December 2009 ▼ Vol. 109, No. 12 37
because it may indicate pregnancy complications oranother diagnosis. ▼
Kathleen A. Whitney is an ED nurse at Texas Health HarrisMethodist Hospital Fort Worth. Contact author: [email protected]. The author of this article has no significant ties,financial or otherwise, to any company that might have aninterest in the publication of this educational activity.
REFERENCES 1. Snyder JA, et al. Diagnostic considerations in the measure-
ment of human chorionic gonadotropin in aging women.Clin Chem 2005;51(10):1830-5.
2. Shih IM, Kurman RJ. The pathology of intermediate tro-phoblastic tumors and tumor-like lesions. Int J GynecolPathol 2001;20(1):31-47.
3. Ichikawa N, et al. Immunohistochemical analysis of cellcycle regulatory gene products in normal trophoblast andplacental site trophoblastic tumor. Int J Gynecol Pathol1998;17(3):235-40.
4. Li AJ. Gestational trophoblastic neoplasms. In: Gibbs RS,et al., editors. Danforth’s obstetrics and gynecology. 10thed. Philadelphia: Wolters Kluwer/Lippincott Williams andWilkins; 2008. p. 1073-85.
5. Kim SJ. Placental site trophoblastic tumour. Best Pract ResClin Obstet Gynaecol 2003;17(6):969-84.
6. Papadopoulos AJ, et al. Twenty-five years’ clinical experiencewith placental site trophoblastic tumors. J Reprod Med 2002;47(6):460-4.
7. Hui P, et al. Pathogenesis of placental site trophoblastic tumormay require the presence of a paternally derived X chromo-some. Lab Invest 2000;80(6):965-72.
8. Eckstein RP, et al. Placental site trophoblastic tumour (tro-phoblastic pseudotumour): a study of four cases requiringhysterectomy including one fatal case. Histopathology1982;6(2):211-26.
9. Finkler NJ, et al. Clinical experience with placental site tro-phoblastic tumors at the New England TrophoblasticDisease Center. Obstet Gynecol 1988;71(6 Pt 1):854-7.
10. Feltmate CM, et al. Placental site trophoblastic tumor: a 17-year experience at the New England TrophoblasticDisease Center. Gynecol Oncol 2001;82(3):415-9.
11. Sumi Y, et al. Placental site trophoblastic tumor: imagingfindings. Radiat Med 1999;17(6):427-30.
12. Sakamoto C, et al. Sonographic appearance of placental sitetrophoblastic tumor. J Ultrasound Med 1990;9(9):533-5.
13. Garner E. Malignant gestational trophoblastic disease: stag-ing and treatment. Waltham, MA: Wolters Kluwer Health/UpToDate 2008.
14. Monclair T, et al. Placental site trophoblastic tumor (PSTT)in mother and child: first report of PSTT in infancy. MedPediatr Oncol 2002;38(3):187-91; discussion 92.
15. Chang YL, et al. Prognostic factors and treatment for pla-cental site trophoblastic tumor—report of 3 cases andanalysis of 88 cases. Gynecol Oncol 1999;73(2):216-22.
16. Swisher E, Drescher CW. Metastatic placental site tro-phoblastic tumor: long-term remission in a patient treatedwith EMA/CO chemotherapy. Gynecol Oncol 1998;68(1):62-5.
17. Schmid P, et al. Prognostic markers and long-term outcomeof placental-site trophoblastic tumours: a retrospectiveobservational study. Lancet 2009;374(9683):48-55.
For more than 15 additional continuing nursingeducation articles related to the topic of women’shealth, go to www.nursingcenter.com/ce.
GENERAL PURPOSE: To provide registered professionalnurses with information on positive pregnancy tests thatresult from medical conditions other than pregnancy,including placental site trophoblastic tumors.
LEARNING OBJECTIVES: After reading this article andtaking the test on the next page, you will be able to• summarize the etiology, risk factors, and characteris-
tics regarding placental site trophoblastic tumors.• outline the diagnostic measures, treatment modalities,
and outcomes of placental site trophoblastic tumors.
TEST INSTRUCTIONSTo take the test online, go to our secure Web site at www.nursingcenter.com/ce/ajn.To use the form provided in this issue, • record your answers in the test answer section of the
CE enrollment form between pages 40 and 41. Eachquestion has only one correct answer. You may makecopies of the form.
• complete the registration information and courseevaluation. Mail the completed enrollment form andregistration fee of $21.95 to Lippincott Williams andWilkins CE Group, 2710 Yorktowne Blvd., Brick, NJ08723, by December 31, 2011. You will receive yourcertificate in four to six weeks. For faster service, includea fax number and we will fax your certificate withintwo business days of receiving your enrollment form.You will receive your CE certificate of earned contacthours and an answer key to review your results. Thereis no minimum passing grade.
DISCOUNTS and CUSTOMER SERVICE• Send two or more tests in any nursing journal published
by Lippincott Williams and Wilkins (LWW) together, anddeduct $0.95 from the price of each test.
• We also offer CE accounts for hospitals and otherhealth care facilities online at www.nursingcenter.com.Call (800) 787-8985 for details.
PROVIDER ACCREDITATIONLWW, publisher of AJN, will award 2.1 contact hours forthis continuing nursing education activity.
LWW is accredited as a provider of continuing nursingeducation by the Commission on Accreditation of theAmerican Nurses Credentialing Center (ANCC).
This activity is also provider approved by the CaliforniaBoard of Registered Nursing, Provider Number CEP11749 for 2.1 contact hours. LWW is also an approvedprovider of continuing nursing education by the District ofColumbia and Florida #FBN2454. LWW home studyactivities are classified for Texas nursing continuingeducation requirements as Type I.
Your certificate is valid in all states.The ANCC’s accreditation status of the LWW Department
of Continuing Education refers to its continuing nursingeducational activities only and does not imply Commissionon Accreditation approval or endorsement of any commercialproduct.
TEST CODE: AJN1209A
Continuing Education
EARN CE CREDIT ONLINEGo to www.nursingcenter.com/ce/ajn and receive a certificate within minutes.
2.1 HOURS