Embed Size (px)
Citation preview

Archives ofDisease in Childhood 1990; 65: 977-983
Plasma prolactin and clinical outcome in preterminfants
A Lucas, B A Baker, T J Cole
AbstractPlasma prolactin was measured weekly in 280preterm infants. The complex gestational agedependent pattern of postnatal prolactinrelease has been defined and reference stan-dards provided. Plasma prolactin was higherin girls, with increasing divergence betweenthe sexes from the third week onwards, andhigher after two weeks, in infants of motherswith pregnancy related hypertension. Diet,assigned randomly, exerted a major effect onplasma prolactin, with significantly highervalues in infants fed donor breast milk or stan-dard formula than in those fed a protein,energy, and mineral enriched preterm for-mula. After adjusting for confounding factors,infants with the lowest plasma prolactin con-centrations (<1000 mU/l, 32-9 jig/l) occurringusually at a nadir between days 5 and 12,showed a 120% increase in the duration ofventilatory assistance required, a 20%increase in the number of days to attain fullenteral feeds, and a 30% decrease in lengthgain.We suggest preterm birth disrupts the nor-
mal perinatal pattern of prolactin release andthat those infants who develop relatively lowplasma concentration have an adverse out-come. Our data add to the broader debate onwhether preterm infants require multipleendocrine replacement treatment.
MRC DunnNutrition Unitand UniversityDepartment ofPaediatrics,CambridgeA LucasB A BakerT J ColeCorrespondence to:Dr A Lucas,Dunn Nutrition Unit,Downhams Lane,Milton Road,Cambridge CB4 1XJ.Accepted 27 April 1990
Prolactin has a central role in stimulating milkproduction. Numerous and diverse actions forprolactin have been proposed in animals andman, however,' 2 and in recent years the possi-bility has been raised that prolactin is importantfor developmental events in the perinatalperiod>-7High plasma prolactin concentrations are
found in the fetal circulation and in amnioticfluid.5 8 Plasma values considerably in excess ofthose seen in adults have been found in neonatesand persist up to three months postnatally infull term infants and longer still in infants bornpreterm.?" Prolactin may be important forlung maturation and surfactant synthcsis,12'17and the possibility that low plasma concen-
tration might be of aetiological importance inhyaline membrane disease in preterm infantshas been suggested and debated by severalgroups.7 12-15 18-22 Further evidence, alsodebated, points to a possible role for prolactin inthe growth of the gut and its mucosal func-tion and the intestinal absorption of fluidand ions.26
Because of the uncertainty about the physi-
ological actions of prolactin in early life and itspotential importance in preterm neonates, wehave studied plasma prolactin concentrationslongitudinally in a large cohort of intensivelymonitored premature infants, taking part in amulticentre feeding trial.27 Firstly, we havederived standards for plasma prolactin concen-trations, taking into account postnatal age, ges-tation, and sex. Secondly, we have investigatedthe effect of diet and possible influence of otherperinatal factors on prolactin release. Finally, inview of the observations above, we haveexplored, using regression analysis to adjust forconfounding factors, whether postnatal plasmaprolactin concentrations relate to selected clini-cal outcome responses potentially linked to thedevelopment of the lung or gut. These out-comes include duration of severe respiratorydisease, necrotising enterocolitis, days to attainfull enteral feeds, and growth performance.
Subjects and methodsLongitudinal data derived from a large multi-centre infant feeding study were analysed.27 Atotal of 280 neonates were studied in five centreswith a mean (SE) gestational age of 30 3 (0-2)weeks and a mean birth weight of 1330 (18) g.All were less than 1850 g at birth. Extensivedata were collected on their biochemical pro-files. Growth data were collected as describedpreviously.27
In three centres infants whose motherselected not to provide their own milk wereassigned randomly27 to receive either bankedpooled donor breast milk or a preterm formula(Oster-Prem, Farley Health Products) as solediets (trial 1). When mothers expressed theirown 'preterm' milk the infants were assignedrandomly to receive either donor breast milk orpreterm formula as supplements in volumesaccording to the mother's success in expressingher milk (trial 2). In the remaining two centresinfants were assigned randomly to receive eithera standard 'ierm' formula (Osterfeed, FarleyHealth Products) as sole diets (trial 3) or assupplements to mothers milk (trial 4). The pro-tein, energy, and sodium contents of the pre-term formula were: 2-0 g/100 ml, 0-33 MJ (80kcal)/100 ml, and 19-6 mmol/l, and of the stan-dard formula: 145 g/100 ml, 0-28 MJ (68kcals)/100 ml, and 8-3 mmol/l, respectively.
In each subject plasma prolactin was measuredweekly until discharge from hospital or until aweight of 2000 g was exceeded; the mean (SD)duration in study was 37-3 (20 6) days. Databeyond week 7 are presented as the mean ofvalues from week 8 onwards for each subject
977
on Septem
ber 5, 2021 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.9.977 on 1 Septem
ber 1990. Dow
nloaded from

Lucas, Baker, Cole
still in the study. The population of infantsremaining in the study fell with postnatal age; ofthe 280 subjects, 160 remained beyond week 4and 56 beyond week 8. An additional cross sec-tional analysis was performed on valuesobtained within two day blocks of time fromdays 1-2 up to day 13-14.Venous samples were collected in cooled
heparinised tubes, centrifuged at 4°C, and theplasma fraction stored at -20°C within 30minutes of sampling. Plasma prolactin concen-trations were measured on 1340 duplicate 20 iilsamples by radioimmunoassay (CIS France).The percentage cross reactions obtained by theassay were: prolactin 100%, human growth hor-mone 0-24%, and human placental lactogen,luteinising hormone, follicle stimulating hor-mone, human chorionic gonadotrophin, andthyroid stimulating hormonex 10-4%. Mini-mum assay sensitivity was 26 mU/l (0-85 [tg/l).
25000-
+2SD
100000
/ ~~~~~~Mean5000-
E 2500- -2SD
1000-
500-
250-
100-25 26 27 28 29 30 31 32 33 34
Gestation (weeks)
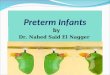
Figure IPlasma prolactin (plotted on a logarithmic scale)in preterm neonates during thefirst 48 hours at gestationsfrom 25 to 34 weeks. Data have been smoothed and representthe geometric mean±2SD. To convert mUll to pgll divideby 30 4.
Statistical analyses were performed usingStudent's t test and x2 tests; multiple and logis-tic regression was used to explore the associa-tion between plasma prolactin concentrationsand a range of perinatal and neonatal factors.For these analyses, plasma prolactin has beentreated either as a dichotomous variable (a valueabove or below a given threshold) or as a con-tinuous one. In the latter case, as data werepostively skewed, they were analysed after logtransformation. For presentation, data havebeen antilogged, providing geometric meanswith 95% confidence intervals.
ResultsREFERENCE VALUES FOR PLASMA PROLACTIN INPRETERM INFANTSPlasma prolactin concentrations in the first 48hours after birth were strongly related to gesta-tion (fig 1 shows a smoothed reference chart).At 25-26 weeks plasma prolactin was 950 mU/l(31-3 pg/l) (95% of values lying between 340(112) and 2660 (87 5)) rising to 5420 (178-3)(2120 (69 7), 13840 (455-3)) mU/l (pg/l) at33-34 weeks (p<0 001).
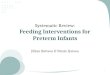
Table 1 shows smoothed reference values forplasma prolactin in the first seven weeks accord-ing to gestation. Early values, up to 14 days, arefor both sexes combined, because as shownbelow, consistent sex differences do not emergeuntil later in the neonatal period. In each gesta-tional age group plasma prolactin concentra-tions fell postnatally to a nadir at a mean ofseven to 10 days followed by a rise. The overalltrend in plasma prolactin over the first sevenweeks depended on gestation (table 1 and fig2A). In infants under 28 weeks, after an initialfall (p<0001), values rose progressively overthe next six weeks (p<0001). In contrast (fig2A) infants of 32-36 weeks' gestation showedoverall a major fall in plasma prolactin frombirth to week 7 (p<0*001).
Figure 2B shows sex differences in plasmaprolactin for the whole cohort. In the first 48hours, values were lower in boys 2440 (80 3)
Table I Plasma prolactin concentrations in mU/l* in pretertn infants in the first seven weeks according to gestational age andsex. For the period 1-14 days and in infants under 28 weeks' gestation both sexes are combined. Data were originally logtransformned to derive means and SDs; the data here have been antilogged to provide a geometric mean plus or minus 2 SD
Postnatal 25-27 Weeks' gestation (n=36) 28-31 Weeks' gestation (n= 152) 32-36 Weeks' gestation (n= 92)age
-2SD Mean +2SD -2SD Mean +2SD -2SD Mean +2SD
Day:t1-2 350 1620 7590 870 3020 10470 2240 5370 128803-4 270 910 3090 680 2400 8510 1150 2820 69205-6 190 630 2140 590 2040 7080 810 2140 56207-8 180 580 1860 540 1820 6170 710 2000 56209-10 200 630 2000 510 1700 5620 720 2140 631011-12 300 830 2290 650 1910 5620 790 2340 692013-14 360 980 2690 910 2400 6310 910 2690 7940
28-36 Weeks' gestation combinedtBays (n= 120) Girls (n= 124)
Week:3 410 1180 3390 760 1910 4790 680 2340 81304 510 1480 4270 660 1700 4370 710 2290 74105 530 1510 4570 590 1510 3890 780 2340 70806 520 1620 5010 490 1320 3550 810 2340 67607 550 1700 5250 430 1180 3240 870 2340 6310
*To convert mU/I to ILg/l divide by 30 4.tAs subjects provided one sample/week, data for days 1-14 are based only on those subjects who were sampled in each two day timeperiod (about one third of subjects sampled/two day period).tFrom week 3, infants of 28-31 and 32-36 weeks' gestation have been combined as there were no significant differences between thesegroups after this age.
978
on Septem
ber 5, 2021 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.9.977 on 1 Septem
ber 1990. Dow
nloaded from

Plasma prolactin and clinical outcome in preterm infants
5000"
4000'
> 31 weeks
< 28 weeks
I I
1 2 3 4Postnatal age (weeks)
3000'"EC-M
0
a- 2000-
1000
4000-
3000
:DE
C
Q 2000-0
5 6 7 ffE
0c
rI
1 2 3 4Postnatal age (weeks)
1000]0 ; 2 3 4 5 6 7
Postnatal age (weeks)
Figure 2 Plasma prolactin inpreterm infants during thefirst two months: (A) infants under 28 weeks compared with those above 31 weeks' gestation;(B) boys compared with girls; and (C) infants whose mothers hadpregnancy related hypertension compared with those with normotensive mothers. Data are
geometric mean (SE) * * *p<O0OOI; **p<OO1; *p<005. To convert mUll to pg/l divide by 30 4.
(620 (20 4) to 9600 (315-8)) mU/l ([ig/l) than ingirls 3600 (120-4) (1100 (36 2) to 12180 (400'7))mU/, (R.g/1) (p<05). This difference did notreach significance again until week 3, afterwhich there was a major and progressive diver-gence in values between the sexes.
FACTORS RELATING TO PLASMA PROLACTINCONCENTRATIONSIn addition to gestation and sex, a range of otherfactors were explored for their association withplasma prolactin.
Effect of dietFigure 3A shows plasma prolactin in infants intrials 1 and 2. While those fed on breast milkshowed no change in prolactin values from thesecond to seventh week, values in the group fedpreterm formula declined progressively and
were significantly lower beyond weeks 3. Asimilar trend was seen in trials 3 and 4 withlower values on preterm formula. The differ-ences (not depicted) did not reach significancein this much smaller comparison. In fig 3B,however, all four trials have been combined tocompare infants fed 'unfortified' diets: bankedmilk or term formula compared with those fed a
'fortified' preterm formula. As this is a balancedaddition of trials, the comparison is a ran-
domised one. In infants fed preterm formula,plasma prolactin concentrations declinedlinearly (p<001) with values progressivelydiverging from those seen on banked milk or
standard formula.As high prolactin concentrations are found in
early milk,28 we considered that these mightcontribute to high plasma concentrations innewborn infants. A comparison of infants fed90% or more of their own mothers early pretermmilk with infants fed on mature donor breast
6000
5000-1
4000 1
3000-
E 2000r-
CL
E
1000
5
0 06
5 6 7
r.. a I. I
979
--
on Septem
ber 5, 2021 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.9.977 on 1 Septem
ber 1990. Dow
nloaded from

Lucas, Baker, Cole
3000-
2500'
2000-
E
E
2000
oa
E
X 1500-
1000-
3000-
2500-
E
X 50
10001
Figure 3prolactin imonths. (4pretermfoand (B) stcomparedmatemal
milk, h(neonata]ference.-and 0-7
Other factors(c Using regression modelling, a range of factors
T - have been examined for their independent re-(60) 156) lationship with prolactin concentration, calcu-
r5j i5 lated as the mean of all values for each subject in, \ E - ---1 ' r the first month (dependent variable). Indepen-
dent variables included the infant's sex, ges-tation (above or below 28 weeks), birth weight,diet (banked milk or standard formula com-
149) pared with preterm formula), and fetal growthretardation (birth weight above or below 10thcentile). Also included were pregnancy related
(38) () hypertension (diastolic blood pressure 90 mmPreterm formula Hg or over; or systolic blood pressure 140 mm
Hg or over), days of mechanical ventilation (logtransformed; plus 1, to avoid log 0), Apgar
19) score at five minutes (below 5 compared with 5and above), mode of delivery (caesarean com-pared with vaginal), necrotising enterocolitis,number of days to attain full enteral feeds(defined as 150 ml/kg per day or more), and
0 1 2 3 4 5 6 7 days of dopamine treatment (only eight cases).Four factors were independently associated
with plasma prolactin: sex (higher in girls,Standard formula p<0-001), gestation (higher above 28 weeks;
(84) or banked milk p<0001), pregnancy related hypertensionT1 ~182) (42)(32) (associated with higher values, p<002), and
182)1)T diet (lower on preterm formula, p<002). Raw"'X I 1L-.---^ 't---(54) vdata on the association between these four fac-
(75) "'T54 tors and plasma prolactin (against postnatal age)>'are shown in table and figs 1, 2, and 3.
Interaction terms were also introduced into(78) > the models to explore any interactions between
\71) gestation, sex, diet, and hypertension. The onlyone identified was between gestation and hyper-
(5-6) 1 + tension, demonstrating that a significant rise inplasma prolactin in hypertensive subjects was
Preterm formula 128) greatest in infants of low gestation. As babies ofhypertensive subjects had a slightly higher
119)mean gestation than those of those who werenormotensive (31-7 compared with 30 5 weeks),the data depicted in fig 2C represent an under-estimate of the difference that would have been
° 7 ^ 3 i 5 seen if the two groups had had the same meanPostnatal age (weeks) gestation.
Effect ofdiet, randomly assigned, on plasma In order to explore the possibility that theconcentranon tn preterm infants during thefirst twoA)Banked donor breast milk compared with dietary effect (above) related to sodium status,
nnula, as sole diets or supplements to maternal milk mean plasma sodium concentration (in week 1
tandardformula or banked milk ('unfortified diets') or month 1) was added to the models. No asso-
'with pretermformula as sole diets or supplements to ciation between plasma sodium and plasma pro-milk. **p<O.O1, *p<0.O5.
lactin emerged, and the dietary effect was
unchanged.)wever, failed to show any difference in It should be noted that in all the longitudinalI plasma prolactin (t values for the dif- data described above, sample size diminishedat ages 1-3 days and 4-7 days were 0-02 when the larger babies were discharged from'1). hospital. Thus after the first month the popula-
Table 2 Raw data on association between the minimum (lowest) plasma prolactin concentration in the neonatal period andrespiratory disease, prolonged establishment of enteral feeds, and neonatal linear growth rate
Minimum plasma prolactin concentration (mU/l)*<1000 1000-1999 2000-2999 ¢3000
No (%) infants with respiratory distress syndrome(needing ventilation) 50/67 (75)** 65/128 (51) 26/50 (52) 16/35 (46)
No (%) of infants ventilated >7 days 29/67 (43)*** 15/128 (12) 4/50 (8) 2/35 (6)No (%) infants taking >14 days to full enteral feeds 16/59 (27)* 14/120 (12) 6/49 (12) 4/33 (12)Mean (SE) length gain (mm/day) 1109 (0 07) 1-33 (0-06) 1-33 (0-08) 1-33 (0-09)
*To convert mU/I to pg/l divide by 30 4.tNineteen of 280 subjects died before attaining full feeds.***p<O-O01, **p<O-Ol, *p<0 025 for comparison of infants whose minimum plasma prolactin was below 1000 mU/I and all infantswhose minimum plasma prolactin was 1000 mU/I and above (last three columns in the table combined).
980
on Septem
ber 5, 2021 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.9.977 on 1 Septem
ber 1990. Dow
nloaded from

Plasma prolactin and clinical outcome inprerm infants
tion remaining in the study was predominantlyinfants below 32 weeks' gestation.
ASSOCIATION BETWEEN PLASMA PROLACTIN ANDCLINICAL OUTCOMEIn a series of regression models, plasma prolac-tin has been treated as an independent variableto explore its association with the followingclinical outcome responses (dependent vari-ables): duration of respiratory disease (days ofventilation), necrotising enterocolitis, days tofull enteral feeds (over 150 ml/kg per day),weight gain (g/kg per day), length gain (mm!day), and head circumference gain (mm/day)(the growth rates were assessed from the day ofregaining birth weight to discharge from thestudy). Logistic regression was used for thedichotomous dependent variable, necrotisingenterocolitis. Further independent variableswere the same as those in the models describedin the previous section.No association was found between mean or
the peak (highest) plasma prolactin concentra-tion and any of the outcome responses. Afteradjusting for confounding factors (above),however, the minimum plasma prolactin con-centration, usually occurring between days 5and 12, was found to be significantly related toduration of ventilation (p<0005), linear growth(length gain) in the neonatal period (p<002),and the number of days of full enteral feeds(p<0 03) (minimum prolactin concentrationwas log transformed in these models to achievethe best fit).From inspection of the raw data in table 2, it
is apparent that when the minimum plasma pro-lactin concentration fell below 1000 mU/l (32-9gg/l) there was a sharp rise in the duration ofventilatory assistance and days to full feeds anda sharp fall in linear growth. Using regressionanalysis to adjust for confounding factors, avalue of 1000 mU/l (32-9 [ig/l) again proved tobe the best modelled cut off for predicting theseadverse outcomes. Plasma prolactin valuesunder 1000 mU/l (32-9 ttg/l) in the first weekwere independently associated with an increasein the number of days of ventilation (p<0 001),the proportion of subjects ventilated for overseven days (p<0001), neonatal length gain(p=0 018), and the number of days to attain fullenteral feeds (p=0 027) (fig 4).The raw data (table 2) show that the inci-
dence of respiratory disease as well as the dura-tion was related to low plasma prolactin; after
Table 3 Association between low plasma prolactin (<1000mUll) and duration of severe respiratory disease, days toestablish full enteralfeeds, and linear growth, after adjustingfor potentially confounding factors (see text) by multipleregression
Dependent variable Plasma 95% Conftdence p Valueprolactin interval<1000 mU/M
Days of ventilationt Increased 1-4:1 to 3-6:1 <0-001by 2-2:1
Days to attain full Increased 1-0:1 to 1-4:1 0-027enteral feeds by 1-2:1
Length gain (mm) Decreased -0-08 to -0 74 0-018by 0-33
*To convert mU/I to tg/l divide by 30 4.tLog transformed for statistical analyses.
adjusting for confounders (table 3), only theduration was significantly related. Interestingly,despite previous reports that low plasma prolac-tin at birth relates to the incidence of respiratorydistress,6 7 12 we found no association betweenplasma prolactin in the first 48 hours and theincidence or duration of respiratory disease.Low plasma prolactin was unrelated to weightgain, head circumference gain, or necrotisingenterocolitis.
DiscussionIn a large cohort of preterm infants monitoredduring the early months we have defined thecomplex pattern of longitudinal changes inplasma prolactin concentration and providednew reference standards. A major effect of dieton plasma prolactin concentration emerged, andafter adjusting for other factors the infant's sexand gestation and pregnancy related hyperten-sion in the mother were strongly related to thepattern of prolactin release. Most important,low plasma prolactin in the neonatal period wassignificantly related to prolonged respiratorydisease, an increase in the length of time takento establish enteral feeds, and reduced lineargrowth performance, even after adjusting for awide range of potentially confounding factors.
Several studies describe hyperprolactinaemiain preterm and term infants,"' but the com-plexity of the postnatal changes and theirrelation to gestation and sex had not beenadequately defined. Cord plasma values havebeen shown to rise with gestation.21 Our datashow a sixfold increase in plasma prolactinbetween 25 and 30 weeks' gestation, from a con-centration little above the normal adult refer-ence range. High fetal values, which arebelieved to derive from the fetal pituitary andnot the mother, may be induced by maternaloestrogens.5 This could explain high plasmaprolactin we and others have observed in theearly days after birth.9 We showed that regard-less of gestation and in all subgroups studiedplasma concentrations fell rapidly to reach anadir at seven to 10 days, followed by a signifi-cant rise by the 12th day and possibly a secondsmaller fall.
Breast milk contains very high prolactin con-centrations in the first three days.28 Our datadid not suggest that this contributed to highneonatal plasma prolactin, however, as valueswere the same whether infants were fed earlymaternal milk or mature donor breast milk.
It has been argued that hyperprolactinaemia,which even occurs in anencephalic neonates,5 29implies a failure of prolactin inhibition, by pro-lactin inhibitory factor, rather than a stimula-tion of release. Maturation of the ability torelease prolactin inhibitory factor5 11 couldaccount in part for the progressive decline inplasma prolactin during the early monthsobserved here and described previously.However, our data suggest a more complexexplanation. Firstly, in the most immatureinfants, below 28 weeks' gestation, plasmavalues rose considerably over a period of weeksfrom the nadir at seven to eight days; such a riseis difficult to reconcile with the explanation of
981
on Septem
ber 5, 2021 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.9.977 on 1 Septem
ber 1990. Dow
nloaded from

Lucas, Baker, Cole
hyperprolactinaemia above. Furthermore, boysshowed a much more rapid decline in valuesduring the first two months than that seen ingirls.The sex difference in plasma prolactin in pre-
term infants, found also after adjustment forpotentially confounding factors, was of interest.In adolescence and adulthood, females havehigher prolactin values than males, principallyearly in the menstrual cycle when plasma oes-trogen is high.'0 This sex difference has notbeen described during infancy or childhood.Indeed, in a much smaller sample it was pre-term boys who transiently had higher plasmaprolactin concentrations during the first week. 10We found girls had transiently higher valuesafter birth (consistent with a previousobservation'5 based on cord blood analyses),and beyond 2 weeks of age when a major andprogressive divergence in plasma prolactinbetween boys and girls was found. It requiresexploration whether this difference could con-tribute to the well described poorer prognosis inboy preterm neonates.30 31
Maternal hypertension has been associatedwith an increase in plasma prolactin in cordblood.2' It might be supposed that maternalpre-eclampsia had exerted a transient influenceon the metabolic milieu of the fetus. However,our data show, surprisingly, that the associationbetween high plasma prolactin and pregnancyrelated hypertension persists and increases inmagnitude during the first two months (evenafter adjustment for confounding factors). Thepossibility is raised therefore that pregnancyrelated hypertensive disease might induce longterm changes in the infant's endocrine state.
Diet was a major factor influencing plasmaprolactin. In a strictly randomised comparisoninfants fed preterm formula developed lowerplasma prolactin concentrations than those feddonor breast milk or standard formula (whenthese diets were used alone or as supplements tomothers' milk). The preterm formula wasenriched in protein, energy, sodium, and otherminerals. Ertl et al showed a significant post-natal decline in plasma prolactin,32 as seen herein infants fed the preterm formula with sodiumchloride supplementation. We found thatplasma sodium and plasma prolactin were unre-lated. While this does not exclude the possibil-ity that our dietary effect was solely due todifferences in salt intake, effects of other nut-rients on prolactin release need to be excluded.
Prolactin has been identified as a possibletrigger for surfactant synthesis.2-l'7 Fetal pro-lactin secretion rises before surfactant produc-tion and there are prolactin receptors in thelung,'6 and after experimental administration ofprolactin to fetal rabbits pulmonary lecithincontent increases rapidly.'3 Some investigatorsfind that a low plasma prolactin concentrationin cord blood relates to the development ofrespiratory distress6 7 12; others do not20 22 andclaim low plasma prolactin is simply a markerfor low gestation.20 Such reports have relied onsimple correlative analyses, however, with littleadjustment for potentially confounding factors.Moreover, these investigations have relatedvaluies at birth to the incidence of respiratory
distress and have not examined the associationbetween the subsequent development of lowplasma prolactin and the persistence of respira-tory disease. Our raw data showed a strong asso-ciation between the incidence of respiratorydisease and minimum plasma prolactin, with asharp rise in incidence as prolactin values fellbelow 1000 mU/l (32-9 [tg/l). After adjusting forconfounding factors, this association was notsustained, casting doubt on some previousobservations. Nevertheless, the subsequentdevelopment of low plasma prolactin wasstrongly and independently related to the dur-ation of severe respiratory disease. This rela-tionship held when minimum plasma prolactinwas treated as a continuous variable, but datamodelling showed that for prognostic purposes,a minimum value below 1000 mU/l (32-9 [tg/l)was associated with a major increase in durationof mechanical ventilation. Infants whose plasmaprolactin concentration fell below 1000 mU/l(32-9 tg/l) had a more than twofold increase inthe number of days of ventilation that theyrequired and were over twice as likely to be ven-tilated for more than seven days, even afteradjusting for birth weight, gestation, fetalgrowth retardation, sex, pre-eclampsia, lowApgar scores, and other major factors.
After adjusting for the same factors, infantswhose plasma prolactin fell below 1000 mU/l(32-9 [ig/l) took 20% longer (median three dayslonger) to attain full enteral feeds and, moreimportant, had a linear growth rate 30% lowerthan in infants in whom values remained abovethis concentration. Possibly, these outcomesrelated in part to slower gut maturation in thosewith low plasma prolactin.2326 It is unlikelythat delayed establishment of enteral feeds andreduced linear growth in those with low plasmaprolactin simply reflected increased respiratorydisease in this group, as adjustment for the pres-ence and duration of severe lung disease didnot abolish these associations. Interestingly, lowprolactin values only related to reduced lineargrowth and not reduced weight gain or headgrowth. Low plasma prolactin might have had aselective effect on nutrient absorption, withreduction in intestinal transport of bone mineralsubstrate.
This speculation accords with Mainoya'sexperimental findings in rats that prolactinenhanced jejunal absorption of calcium (andother ions).26 Furthermore, prolactin has beenimplicated in regulation of 1-25 hydroxyvita-min D production,33 and this might also influ-ence bone growth. Indeed in humans withhypopituitarism prolactin treatment promotesskeletal growth.3
Preterm birth may disrupt normal endocrinedevelopment. Previously we have identified (inthe same cohort) low plasma concentrations oftwo other hormones that may have an importantbearing on clinical outcome: low neonataltriiodothyronine concentrations were associatedwith later reduced developmental scores34 andlow testosterone values in boys with failure oftesticular descent.35 In this study we have pre-sented a further example of an early endocrinedisturbance that relates to an adverse outcome:preterm infants, born before the normal rise in
982
on Septem
ber 5, 2021 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.9.977 on 1 Septem
ber 1990. Dow
nloaded from

Plasma prolactin and clinical outcome in preterm infants 983
fetal prolactin in the third trimester, may havelow plasma prolactin concentrations and theseare strongly related to prolonged respiratorydisease, delay in establishment of full enteralfeeds, and reduced linear growth performance.Collectively, these data are relevant to theimportant question, requiring further scientificconsideration, of whether infants of low gesta-tion require multiple endocrine replacementtreatment.
1 Ganong WF. Prolactin: a general overview. In: MacLeodRM, Scapagnini U, eds. Central and peripheral regulation ofprolactin function. New York: Raven Press; 1980:1-10.
2 Ensor DM. Comparative endocrinology of prolactin. London:Chapman and Hall, 1978.
3 Root AW. Growth hormone and prolactin in the fetus. In:New MI, Fiser R, eds. Diabetes and other endocrine disordersduing pregnancy and in the newborn. Vol 10. New York:Liss; 1976:170-26.
4 Lorenzo AV, Winston KR, Welch K, Adler JR, GranholmL. Evidence of prolactin receptors in the choroid plexusand a possible role in water balance in neonatal brain.Z Kinderchir 1983;38(suppl 2):68-70.
5 Aubert ML, Grumbach MM, Kaplan SL. The ontogenesis ofbuman fetal hormones: 3. prolactin. J Clin Invest 1975;56:155-4.
6 Gluckman PD, Ballard PL, Kaplan SL, Liggins GC,Grumbach MM. Prolactin in umbilical cord blood and therespiratory distress syndrome. J Pediatr 1978;93:1011-4.
7 Hauth JC, Parker CR, Macdonald PC, Porter JC, JohnstonJM. A role of fetal prolactin in lung maturation. ObstetGynecol 1978;51:81-8.
8 Friesen HG. Human prolactin in clinical endocrinology: theimpact ofradioimmunoassay. Metabolism 1973;22:1039-45.
9 Sack J, Fisher DA, Wang CC. Serum thyrotropin, prolactin,and growth hormone levels during the early neonatal periodin the human infant. Pediatics 1976;89:298-300.
10 Guyda HJ, Friesen HG. Serum prolactin levels in humansfrom birth to adult life. Pediatr Res 1973;7:534-40.
11 Perlman M, Schenker J, Glassman M, Ben-David M.Prolonged hyperprolactinemia in preterm infants. J ClinEndocrinol Metab 1978;47:894-7.
12 Smith YF, Mullon DK, Hamosh M, Scanlon JW, Hamosh P.Serum prolactin and respiratory distress syndrome in thenewborn. Pediatr Res 1979;14:93-5.
13 Hamosh M, Hamosh P. The effect of prolactin on the lecithincontent of fetal rabbit lung. J Clin Invest 1977;59:1002-5.
14 Smith YF, Mullon DK, Hamosh M, Scanlon JW, Hamosh P.Prolactin and human lung maturation. PediatrRes 1978;12:569.
15 Dhanireddy R, Smith YF, Hamosh M, Mullon DK, ScanlonJW, Hamosh P. Respiratory distress syndrome in the new-born: relationship to serum prolactin, thyroxine, and sex.Biol Neonate 1983;43:9-15.
16 Cox MA, Torday JS. Relative increase in saturated lecithin in
prolactin-treated fetal lung cultures. Pediatr Res 1978;12:559.
17 Josimovich JB, Merisko K, Boccella L, et al. Binding of pro-lactin by fetal rhesus cell membrane fractions. Endocrino-logy 1977;100:557-63.
18 Ballard PL. Hormones and lung maturation. MonogrEndocri-nol 1986;28:1-354.
19 Blumenthal NJ, Van der Walt LA, Gordon E, Langer 0.Prolactin, cortisol and thyroxine levels and the prematureinfant. S Afr Med J 1983;63:605-6.
20 Schober E, Simbruner G, Saizer H, Husslein P, Sponer J.The relationship of prolactin in cord blood, gestational ageand respiratory compliance after birth in newborn infants.J Perinat Med 1982;10:23-6.
21 Grosso DS, Macdonald CP, Thomasson JE, Christian CD.Relationship of newborn serum prolactin levels to therespiratory distress syndrome and maternal hypertension.Am J Obstet Gynecol 1980;137:569-74.
22 Luerti M, Spagnolo D, Zavattini G, Bianchi C, Barbera AG,Corbella E. Cord blood prolactin and thyroid hormonelevels after antenatal administration of betamethasone orambroxol for prevention of respiratory distress syndrome(RDS). Biol Res in Pregnancy 1984;5:124-9.
23 Theintz GE, Nussle D, Cox J, Carmignac D, Duhamel D,Sizonenko PC. Prolactin and the gut: a controversy. jPediatr Gastroenterol Nutr 1984;3:523-8.
24 Varkonyi A, Falkay G. Hyperprolactinemia in children withcoeliac disease. Monatsschr Kinderheilkd 1984;132:547-9.
25 Stern M, Harmatz PR, Kleinman RE, Walker WA. Foodproteins and gut mucosal barrier. III. The influence of lac-tation and prolactin on the in vitro binding and uptake ofbovine serum albumin and ovalbumin in the rat jejunum.Pediatr Res 1985;19:320-4.
26 Mainoya JR. Further studies on the action of prolactin onfluid and ion absorption by the rat jejunum. Endocrinology1975;96:1 158-64.
27 Lucas A, Gore SM, Cole TJ, et al. Multicentre trial on feed-ing low birthweight infants: effects on diet on early growth.Arch Dis Child 1984;59:722-30.
28 Healy DL, Rattigan S, Hartman PE, Herrington AC, BurgerHG. Prolactin in human milk: correlation with lactose,total protein, and a-lactalbumin levels. AmJ Physiol 1980;238:E83-6.
29 Hayek A, Driscoll SG, Warshaw JB. Endocrine studies inanencephaly. J Clin Invest 1973;52:1636-41.
30 Miller HC, Futrakul P. Birth weight, gestational age and sexas determining factors in the incidence of respiratory dis-tress syndrome ofprematurely born infants. J Pediatr 1968;72:628-35.
31 Naeye RL, Bunt LS, Wright DL, et al. Neonatal mortality,the male disadvantage. Pediatrics 1971;48:902-6.
32 Ertd T, Sulyok E, Varga L, Csaba IF. Postnatal developmentof plasma prolactin level in premature infants with andwithout NaCl supplementation. Biol Neonate 1983;44:219-23.
33 Spanos E, Colston KW, Evans IMS, Galante S, McCauly SJ,Maclntyre I. Effect of prolactin on vitamin D metabolism.Mol Cell Endocrinol 1976;5:163-7.
34 Lucas A, Rennie J, Baker BA, Morley R. Low plasmatriiodothyronine concentrations and outcome in preterminfants. Arch Dis Child 1988;63:1201-6.
35 Baker BA, Morley R, Lucas A. Plasma testosterone in pre-term infants with cryptorchidism. Arch Dis Child 1988;63:1198-200.
on Septem
ber 5, 2021 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.65.9.977 on 1 Septem
ber 1990. Dow
nloaded from