Embed Size (px)
Citation preview
Platelet
Thrombocytes
Platelets (Thrombocytes)
• 2- 4 micromillimeters in diameter• 250,000 – 400,000 per microliter (too few
thrombocytopenia – too many thrombocytosis)
• Lifespan on average 6 – 10 days• 1/3 trapped in spleen (for reserve)• No significant marrow reserve• 5 –days for new production
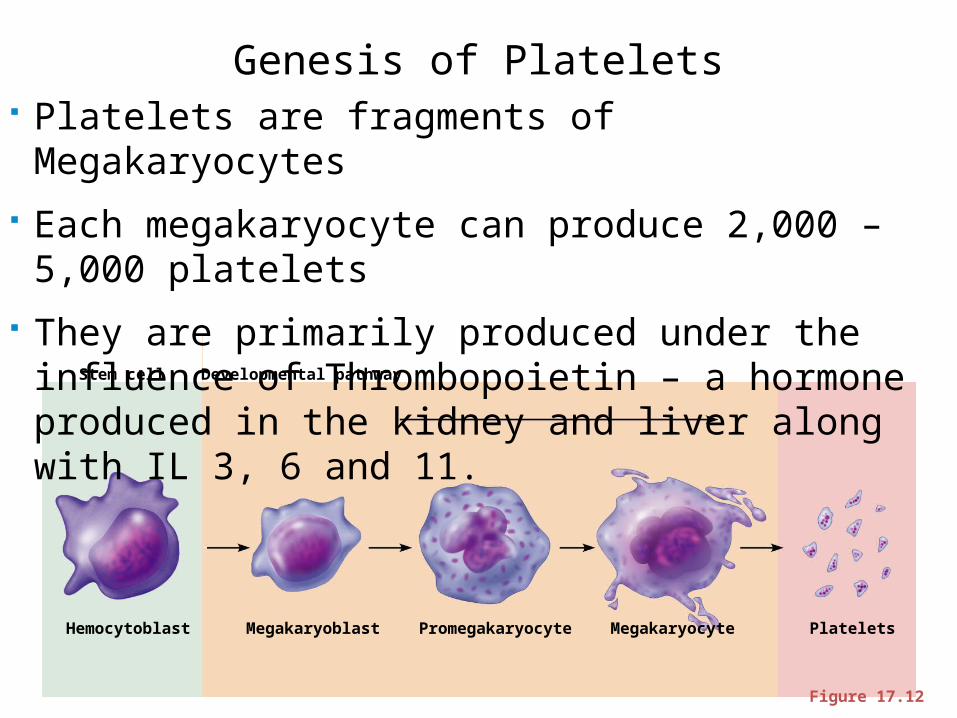
Stem cell Developmental pathway
Hemocytoblast Megakaryoblast Promegakaryocyte Megakaryocyte Platelets
Figure 17.12
Genesis of Platelets Platelets are fragments of Megakaryocytes Each megakaryocyte can produce 2,000 – 5,000 platelets They are primarily produced under the influence of
Thrombopoietin – a hormone produced in the kidney and liver along with IL 3, 6 and 11.
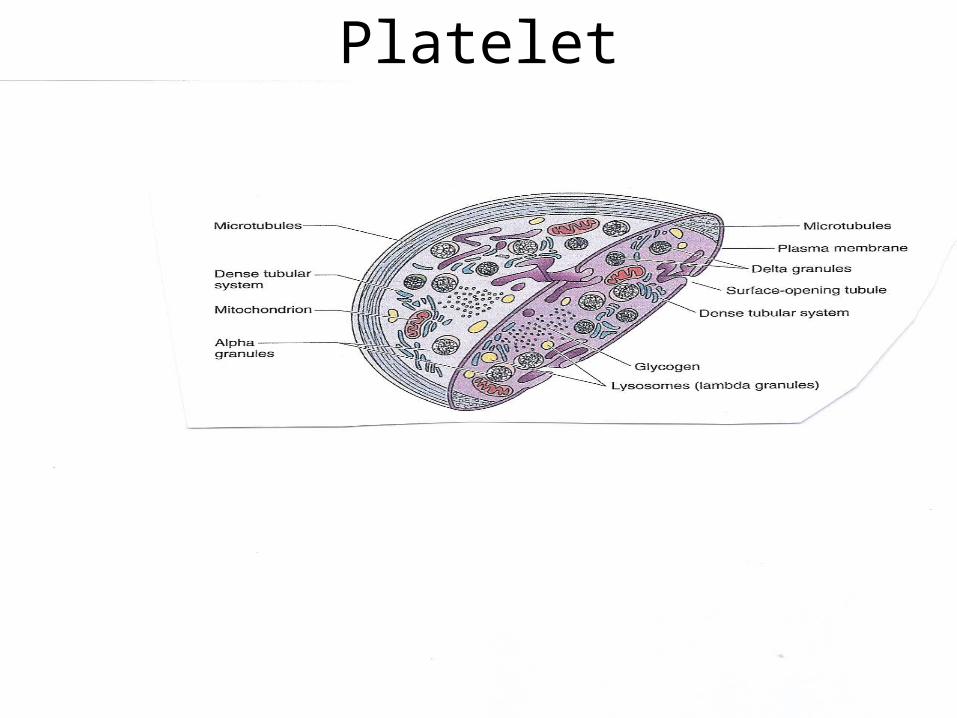
• Platelets are non-nucleated fragments of megakaryocytes with a blue-staining outer region (Hyalomere and a purple granular center (Granulomere)
• The Hyalomere is where the surface opening tubular system is found and the Dense Tubular system
• Open tubular system is site for rapid release and uptake of chemicals associated with granules (stained vesicles)
• Dense tubular system sequesters calcium so as to prevent platelet stickiness
Platelets
• Their granules are termed alpha, beta and lambda contain serotonin, Ca2+, enzymes, ADP, and platelet-derived growth factor (PDGF)
• Platelets function in the clotting mechanism by forming a temporary plug that helps seal breaks in blood vessels
• Platelets not involved in clotting are kept inactive by NO and prostacyclin
Granulomere (region that contains granules)
• Alpha Granules contain Fibrinogen, Platelet Derived Growth Factor, Thrombospondin and certain coagulation factors (Von Willebrand Factor) and Factor V
• Dense Granules contain Calcium, ADP, ATP, serotonin, histamine, pyrophosphatase
• Lambda Granules are lysosomes
Platelet’s other organelles
• Mitochondria• Cytoskeleton – microtubules and other
proteins for example Actin and Myosin
Platelet
Platelet Activation (Formation of Platelet Plug)
Injured blood vessels release Von Willebrand Factor and Tissue Factor and exposure of Collagen
1. Shape Change (Cytoskeleton)2. Platelet Aggregation –(surface ADP and Thrombospondin) 3. Degranulation
Result: Platelet Plug Formation
1. Normally the intact endothelium produces prostacyclin and Nitric Oxide, which inhibit platelet aggregation. It also blocks coagulation by the presence of thrombomodulin and heparin-like molecule on its surface membrane. These two membrane-associated molecules inactivate specific coagulation factors.
2. Injured endothelial cells release Von Willebrand factor and tissue thromboplastin and cease the production and expression of inhibitors of coagulation and platelet aggregation. They also release endothelin, a powerful vasoconstrictor.
3. Platelets (1) avidly adhere to subendothelial collage especially in the presence of Von Willebrand factor, (2) release the contents of their granules, and (3) adhere to one another. These three events collectively are termed platelet activation.
4. The release of some of their granular contents especially *adenosine diphosphate (ADP), and thrombospondin, makes platelets “sticky” causing circulating platelets to adhere to collagen-bound platelets and to degranulate.
* Note Plavix Action-
5. Arachidonic acid formed in the platelet membrane is converted to thromboxane A2, and potent vasoconstrictor and platelet activator.
6. The aggregated platelets act as a plug, blocking bleeding. In addition they express platelet factor 3 on their cell membrane, providing the necessary phospholipid surface for the proper assembly of the coagulation factors (especially thrombin).
7. As part of the complex cascade of reactions involving the various coagulation factors, tissue thromboplastin and platelet thromboplastin both act on circulating prothrombin, converting it into thrombin. Thrombin is an enzyme that facilitates platelet aggregation. In the presence of calcium (Ca+2), it also converts fibrinogen to fibrin.
8. The fibrin monomers thus produced polymerize and form a reticulum of a clot, entangling additional platelets, RBCs and WBCs in a stable, gelatinous blood clot (thrombus). The RBCs facilitate platelet activation, whereas neutrophils, and endothelial cells limit both platelet activation and thrombus size.
9. Approximately 1 hour after clot formation, actin and myosin monomers form thick and thin filaments, which interact by utilizing ATP as their energy source. As a result the clot retracts to about ½ its previous size, pulling the edges of the vessel closer together, and minimizing blood loss.
10.When the vessel is repaired, the endothelial cells release plasminogen activators, which convert plasminogen to plasmin, the enzyme that initiates lysis of the thrombus. The lysosome enzymes in the platelets assist in this action.
Plavix
• Plavix (clopidogrel bisulfate) is an inhibitor of ADP-induced platelet aggregation acting by direct inhibition of adenosine diphosphate (ADP) binding to its receptor and of the subsequent ADP-mediated activation of the glycoprotein GPIIb/IIIa complex. Chemically it is methyl (+)-(S)-α(2-chlorophenyl)-6,7-dihydrothieno[3,2-c]pyridine-5(4H)-acetate sulfate (1:1). The empirical formula of clopidogrel bisulfate is C16H16ClNO2S•H2SO4 and its molecular weight is 419.9.
Aspirin
• Aspirin also has an antiplatelet effect by by blocking COX 1 – thus inhibiting the production of thromboxane, which under normal circumstances binds platelet molecules together to create a patch over damage of the walls within blood vessels.
Thrombocytopenia
• Pseudothrombocytopenia – in vitro due to antibodies created in test tube due to the use of EDTA.
• Infection induced – many viral and bacterial infections cause this in particular HIV
• Drug induced – several drugs cause thrombocytopenia especially heparin therapy
• Immune (Idiopathic)Thrombocytopenia• Thrombotic Thrombocytopenia
Idiopathic Thrombocytopenia Purpura
a condition of having a low platelet count (thrombocytopenia) of no known cause (idiopathic). As most causes appear to be related to antibodies against platelets, ITP is also known as immune thrombocytopenic purpura or immune-mediated thrombocytopenic purpura.
ITP Signs and symptomsSigns include the development of bruises (purpura) and petechiae, especially on the extremities, bleeding from the nostrils and bleeding at the gums, any of which may
occur if the platelet count is below 20,000 per mm3.
A very low count (<10,000 per mm3) may result in the formation of hematomas in the mouth or on other
mucous membranes.Serious and possibly fatal complications due to an
extremely low count (<5,000 per mm3) may include subarachnoid or intracerebral hemorrhage, lower
gastrointestinal bleeding or other internal bleeding.

Thrombotic Thrombocytopenia Purpura (TTP)
a rare disorder of the blood-coagulation system, causing extensive microscopic thromboses to form in small blood vessels throughout the body (thrombotic microangiopathy). Most cases of TTP arise from inhibition of the enzyme ADAMTS13, a metalloprotease responsible for cleaving large multimers of von Willebrand factor (vWF) into smaller units. A rarer form of TTP, called Upshaw-Schülman syndrome, is genetically inherited as a dysfunction of ADAMTS13. If large vWF multimers persist there is tendency for increased coagulation
Thrombocytosis
Thrombocytosis is almost always due to (1) iron deficiency (2) inflammation, cancer or Infection (reactive thrombocytosis); or (3) an underlying myeloproliferative disorder.





























