Embed Size (px)
Citation preview

Chnical Radtology (1986) 37, 285-286 © 1986 Royal College of Radiologists
0009-9260/86/638285502.00
Pleural Effusion Causing Unmatched Ventilation Defects in Ventilation and Perfusion Scanning PAUL GODDARD, JOHN HENSON and E. RHYS DAVIES
Imaging Research Unit, Departments of Radiodiagnosis, Bristol Royal Infirmary and Bristol University, Bristol
In a survey of patients who had chest radiographs and ventilation and perfusion radionuclide scans, 20 patients had pleural thickening or effusion. Defects of ventilation unmatched with defects of perfusion occurred in 13 of the 20. This usually occurred if the fluid was freely mobile and was a result of the procedure adopted for imaging. Upon injection in the supine position, labelled albumin microspheres were trapped in the areas perfused at that time. Since, in this position, the effusion moved post- eriorly, the bases of the lungs were better perfused than the dependent areas. On imaging in the erect position when the effusion was subpulmonary, the microspheres remained in the base but the ventilation was reduced, resulting in a mismatch in the basal regions. This appearance could be misinterpreted.
Mismatched defects of perfusion have been well described in the literature and are most commonly caused by pulmonary embolism (Hoffer et al., 1982). A variety of other causes have been described (Li et al., 1978; Fraser et al., 1984). Mismatched defects of ventila- tion have been described less commonly but can occur with fibrosing lung diseases and pulmonary infections. The chest radiograph can assist in determining the cause of abnormalities shown on ventilation and perfusion radionuclide scanning and will improve the accuracy of reporting (Henson et al., 1985).
A retrospective survey of chest radiographs and ven- tilation and perfusion scintigrams was undertaken in a series of patients. The radionuclide-scan appearances in patients with pleural thickening or effusion were studied.
PATIENTS AND METHOD
The scintigrams and chest radiographs of 100 consecu- tive patients who had undergone ventilation and perfu- sion scanning were studied and analysed by two experienced radiologists independently.
All of the patients with pleural thickening or effusion demonstrable on the chest radiographs were selected as a different subgroup and careful comparison with the scintigrams was made.
The perfusion scans were performed using micro- spheres of albumin labelled with technetium-99m and injected intravenously with the patient in the supine position. The ventilation scintigrams were obtained using Krypton-81m gas. The scintigraphy of perfusion and ventilation was done simultaneously in the erect position using an IGE 400 T gamma camera.
RESULTS
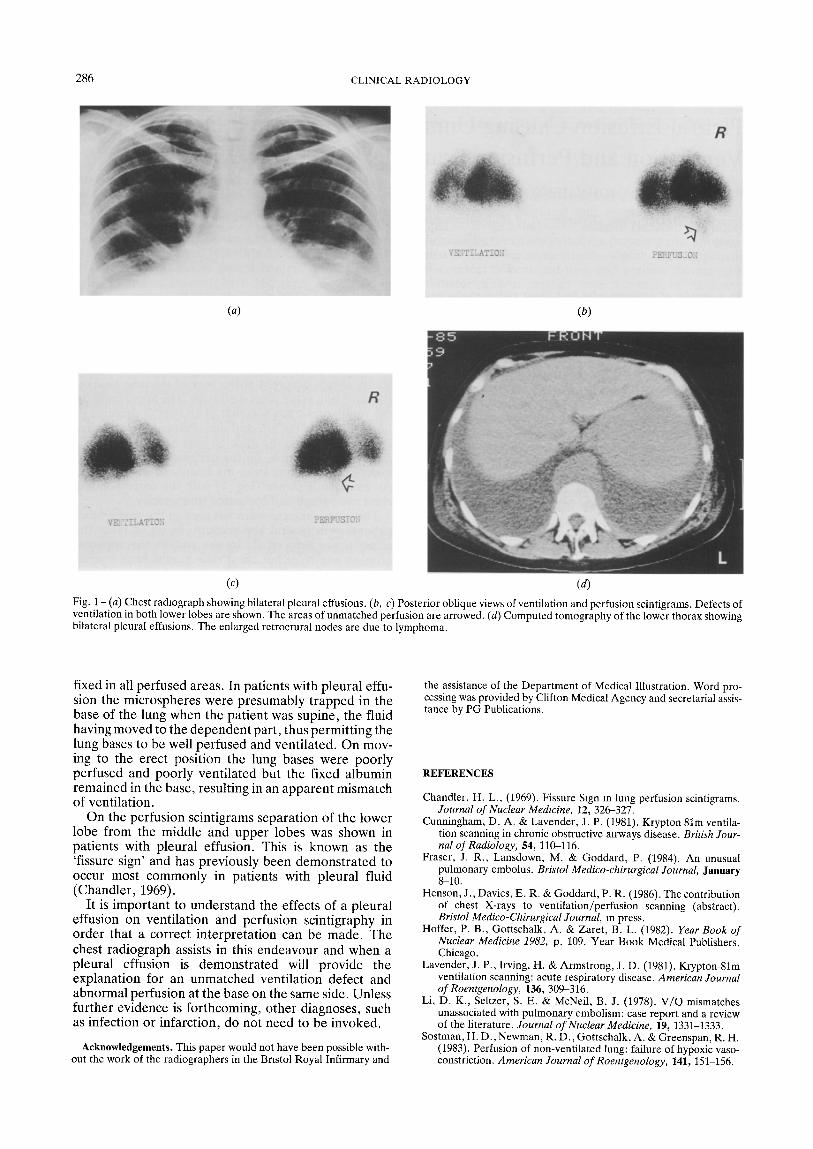
Twenty of the 100 patients had either pleural thicken- ing or pleural effusion shown by chest radiography. Of the 20 patients, 13 had unmatched ventilation defects on ventilation and perfusion scintigraphy. This abnor- mality always occurred at the base of the lung field on the same side as the pleural effusion. The appearance on the ventilation study was that of an overall decrease in lung volume on the affected side. Perfusion was greater than ventilation at the affected base and in some cases there was separation, on the perfusion scintigrams, of lower-lobe segments from the lingula or middle lobe. An example is shown (Fig. 1) with the corresponding chest radiograph and computed tomography.
These appearances were not seen in the seven other patients with pleural abnormality. In six of these the effusion was very small. In one patient the apparent effusion was large but chest radiographs from 6 years previously showed an exactly similar appearance and the pleural abnormality was, therefore, considered to be due to fibrosis and adhesions, rather than effusion.
The basal ventilation mismatch was not seen in any of the 80 patients without pleural abnormality.
DISCUSSION
A number of causes of ventilation defects with preser- vation of perfusion have been reported. These include pneumonia, lobar collapse (Lavender etal., 1981), acute exacerbation of chronic obstructive airways disease (Cunningham and Lavender, 1981; Sostman et al., 1983) and fibrosing alveolitis.
In this series unmatched ventilation defects occurred in association with pleural effusion. In a few cases underlying consolidation could not be excluded, but in the majority of cases further investigation, including decubitus radiographs, ultrasound and computed tomography, demonstrated the freely mobile pleural effusion and showed no evidence of infection. In one patient with bilateral pleural effusions the ventilation and perfusion scans were repeated with the patient erect during both the injection and scintigraphy. In this case unmatched defects had been present bilaterally on the first investigation but only matched basal defects were demonstrated on the second investigation.
The mismatching of the ventilation defect probably results from the method of undertaking the examina- tion. Following the procedure adopted in many centres, the injection of albumin was made with the patients in the supine position but scintigraphy was performed in the erect position. The microspheres of albumin were
286 CLINICAL RADIOLOGY
vv;
VEUTILATiOI$
(a) (b)
PBRFUS_Og
/i'
/7
VETTILATZO.7 -
V
P~RFUSiOE
(c) (d)
Fig. 1 - (a) Chest radiograph showing bilateral pleural effusions. (b, c) Posterior oblique views of ventilation and perfusion scintigrams. Defects of ventilation in both lower lobes are shown. The areas of unmatched perfusion are arrowed. (d) Computed tomography of the lower thorax showing bilateral pleural effusions. The enlarged retroerural nodes are due to lymphoma.
fixed in all perfused areas. In patients with pleural effu- sion the microspheres were presumably trapped in the base of the lung when the patient was supine, the fluid having moved to the dependent part, thus permitting the lung bases to be well perfused and ventilated. On mov- ing to the erect position the lung bases were poorly perfused and poorly ventilated but the fixed albumin remained in the base, resulting in an apparent mismatch of ventilation.
On the perfusion scintigrams separation of the lower lobe from the middle and upper lobes was shown in patients with pleural effusion. This is known as the 'fissure sign' and has previously been demonstrated to occur most commonly in patients with pleural fluid (Chandler, 1969).
It is important to understand the effects of a pleural effusion on ventilation and perfusion scintigraphy in order that a correct interpretation can be made. The chest radiograph assists in this endeavour and when a pleural effusion is demonstrated will provide the explanation for an unmatched ventilation defect and abnormal perfusion at the base on the same side. Unless further evidence is forthcoming, other diagnoses, such as infection or infarct ion, do not need to be invoked.
Acknowledgements. This paper would not have been possible with- out the work of the radiographers in the Bristol Royal Infirmary and
the assistance of the Department of Medical Illustration. Word pro- cessing was provided by Clifton Medical Agency and secretarial assis- tance by PG Publications.
REFERENCES
Chandler, H. L., (1969). Fissure Sign in lung perfusion scintigrams. Journal of Nuclear Medmine, 12, 326-327.
Cunningham, D. A. & Lavender, J. P. (1981). Krypton 81m ventila- tion scanning in chronic obstructive airways disease. British Jour- nal of Radiology, 54, 110-116.
Fraser, J. R., Lansdown, M. & Goddard, P. (1984). An unusual pulmonary embolus. Bristol Medico-chirurgical Journal, January 8-10.
Henson, J., Davies, E. R. & Goddard, P. R. (1986). The contribution of chest X-rays to ventilation/perfusion scanning (abstract). Bristol Medico-Chirurgical Journal, in press.
Hoffer, P. B., Gottschalk, A. & Zaret, B. L. (1982). Year Book of Nuclear Medicine 1982. p. 109. Year Book Medical Publishers, Chicago.
Lavender, J. P., Irving, H. & Armstrong, J. D. (1981). Krypton-81m ventilation scanning: acute respiratory disease. American Journal of Roentgenology, 136, 309-316.
Li, D. K., Seltzer, S. E. & McNeil, B. J. (1978). V /Q mismatches unassociated with pulmonary embolism: case report and a review of the literature. Journal of Nuclear Medicine, 19, 1331-1333.
Sostman, H. D., Newman, R. D., Gottschalk, A. & Greenspan, R. H. (1983). Peffusion of non-ventilated lung: failure of hypoxic vaso- constriction. American Journal of Roentgenology, 141,151-156.