Embed Size (px)
DESCRIPTION
PMTCT and health systems in resource-limited settings: mutual strengthening and lessons learnt . Rene Ekpini E , MD, MPH. Senior Adviser UNICEF, New York. Access to and uptake of PMTCT and Paediatric HIV care and treatment services has significantly increased . - PowerPoint PPT Presentation
Citation preview

PMTCT and health systems in resource-limited settings: mutual strengthening and lessons learnt
Rene Ekpini E, MD, MPHSenior Adviser
UNICEF, New York

Access to and uptake of PMTCT and Paediatric HIV care and treatment
services has significantly increased

Virtual elimination of PMTCT: implications for health systems
C •Geographic coverage: bringing services to all women and children in need
Q•Quality/efficacy of interventions:
providing the most efficacious/quality interventions
U •Access to and utilization of services Wor
king
wit
h co
mm
unit
ies
for
com
mun
itie
s
Health Systems Strengthening

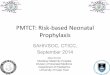
Percent of ANC facilities that provide HIV testing and counselling, and ARVs
for PMTCT
0
20
40
60
80
100 >95>95 9587 86
7664
58 58 55 53 5144
19 16 148 8 3
Source: WHO, UNICEF and UNAIDS, Towards Uni-versal Access: Scaling up priority HIV/AIDS interven-tions in the health sector, Geneva, 2009.
Percent

Where geographic coverage does not mean access to and utilization of
services

Where high coverage can be misleading:
ARV regimens provided to pregnant women living with HIV in 2008

Closing the funding gap to scale up programmes for virtual elimination
of MTCT • Maximizing Global Health Initiatives (IHP+;
H4; H8; USG GHI, etc...) -HIV/PMTCT-Health systems synergies in reaching the goal of virtual elimination of MTCT
High level advocacy Political leadership at all level Planning and implementation
• Leveraging existing resources (GFATM , PEPFAR, ...) to strengthen the MNCH platform and laboratory infrastructure for rapid scale up of PMTCT

Inducing good governance and enabling policies
• Strong political leadership and commitment to ensure that health system goals of access, equity, efficiency and improvement in outcomes are achieved
• Promotion of innovative policies on: - Provider initiated HIV testing and counselling- access to treatment for women and children - Abolition of user fees for antenatal and
delivery care
• Induction of changes in resource allocation including innovative approaches such as performance-based financing

Bringing services closer to women, their children and families through
decentralisation and devolution • Decentralisation and devolution to sub-national
levels with a focus on:– strengthening sub-national management
structures– Integrated management processes (integrated
micro plans, integrated supervision, etc )– Promoting innovative financing mechanisms to
support implementation
• Expansion of services through evidence-based planning that take into account the epidemiology and actual needs
• Strengthening PSM systems

Improving the quality of MNCH services including HIV interventions
• Training of service providers (including CHW) on PMTCT and MNCH with mentoring and supervision. Task shifting and sharing
• Building capacity to scale up 2009 WHO
recommendations:– Improved antenatal and delivery care– Building the capacity within MNCH services for
immunological assessment (CD4) – Improving follow up care (IF and nutritional
counselling and support; CTX, EID) and linkages to ART
• Strengthening the evidence base including national M&E systems, supporting operational research including impact assessment

Improving postnatal care in the context of PMTCT, Swaziland
% of observed providers who counselled on danger signs for mother during postnatal care
% of observed providers who counselled on danger signs for infant during postnatal care

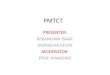
Current Scenario Scenario under policy shift If all women are reached with HAART
0
100
200
300
400
500
600
Transmission rate Number of children infected
3.7% 2.8%.9%
490
366
119
Is elimination of MTCT possible without improving the performance of existing
systems?● 94% of PWLWH receiving: AZT >38 wks - AZT 28-32 wks or HAART
● 6% have no intervention
● 94% of PWLWH receiving
universal HAART ● 6% have no
intervention
100% of PWLWH receiving universal
HAART
Improving the performance of the
system

Increasing access to and utilisation of services
• Bridging programme areas and components (primary prevention, SRH)
• Leveraging resources to improve infrastructure and equipment, optimize working conditions, and improve efficient delivery of services
• Scaling up innovation to service delivery to improve the continuum of MNCH care (e.g. Mother-Baby-Packs ; Point of care machines ; Mobile phone technology)
• Addressing socio-cultural and economic barriers, and ensuring equity (high cost of antenatal and delivery care, stigma, transportation, unfriendly environment)

Utilisation of family planning services by HIV Infected women and their partners, Rwanda National PMTCT Program, 2005-
2009

Partnering with individuals, families and communities
• Engaging civil society, lay counsellors, people living with HIV more systematically as a scale up strategy (planning, demand creation, provision of services)
• Engaging male spouses as partners
• Strengthening community structures using an integrated approach (same community workers to provide integrated package of services)
• Community-based delivery of MNCH services including (antenatal, syphilis, immunization, newborn care, PMTCT)

Proportion of women who reported exclusive breastfeeding last 24 hours
following community based-interventions, Kenya
Susan Kaai, Carolyn Baek et al. : Community-based Approaches to Prevention of Mother-to-Child Transmission of HIV: Findings from a Low-income Community in Kenya

Two Worlds, Two Realities, One Hope: addressing inequity for social justice