Embed Size (px)
Citation preview

CASE REPORT drug abuse, pneumothorax; IJV; pneumothorax, drug abuse
Pneumothorax in Drug Abusers: A Complication of Internal Jugular Venous Injections
We report the cases of six patients who suffered pneumothorax following admitted drug injection into the internal jugular vein area. One was treated in the hospital with observation and serial roentgenograms, two were treated w~th chest tube thoracostomy, and three left the emergency depart- ment against medical advice and were lost to follow up. As increasing num- bers of parenteral addicts turn to central venous injection sites, this com- plication is likely to become more common. ]Bell C, Borak J, Loeffler JR: Pneumothorax in drug abusers: A complication of internal jugular venous injections. Ann Emerg Med 12:167-170, March 1983.]
INTRODUCTION Complications of parenteral drug abuse pose problems often treated in
emergency departments. Among the most common are injuries and infec- tions that result from contact with the penetrating needle, including celluli- tis, localized abscess, thrombophlebitis, and obliterative venous sclerosis. 1 Recently we recognized a growing number of veteran drag abusers using cen- tral veins, particularly the jugular veins, as preferred sites for venipuncture. These individuals are subject to complications that are not normally associ- ated with parenteral drug abuse and that are currently ignored in standard textbooks. ~-4
To bring attention to this new aspect of the drug abuse problem, we report the cases of six patients suffering pneumothorax as a complication of drug injection into the internal jugular vein (IW).
Charlotte Bell, MD Jonathan Borak, MD John R. Loeffler, MD New Haven, Connecticut
From the Section of Emergency Medicine, The Hospital of St Raphael; and the Departments of Internal Medicine and Surgery, Yale University School of Medicine, New Haven, Connecticut.
Address for reprints: Charlotte Bell, MD, Section of Emergency Medicine, The Hospital of St Raphael, 1450 Chapel Street, New Haven, Connecticut 06511.
CASE REPORTS Case Number One
A 33-year-old woman presented to the emergency department of The Hos- pital of St Raphael complaining of left pleuritic pain of six hours duration. The onset of pain immediately followed an injection of drugs into the left side of the patient's neck by another person. The patient admitted to a long history of parenteral drug abuse, and used the central venous injection route primarily because her longstanding habit had resulted in the obliteration of her more accessible peripheral veins. She had recently been hospitalized for treatment of chronic ulcerations resulting from injection of her leg veins.
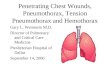
Physical examination revealed a blood pressure of 120/70 m m Hg; pulse, 100/min; respirations, 24/min; and temperature, 37 C. There was splinting of the left hemithorax, but breath sounds were not decreased. A systolic mur- mur was noted along the left sternal border. Multiple injection sites were present on the neck bilaterally (Figure 1A), well above the medial head of the clavicle. Needle scars were present on both arms, and multiple chronic ulcers and significant pretibial edema were found on both legs (Figure 1B to 1D}. Chest films demonstrated a 30% left pneumothorax (Figure 2}. The pa- tient refused further treatment and left against medical advice. No follow-up information is available.
Case Number Two A 28-year-old woman presented to the emergency department of Yale-New
12:3 March 1983 Annals of Emergency Medicine 167/85

PNEUMOTHORAX IN DRUG ABUSERS Bell, Borak & Loeffler
Fig. IA. Needle tracks and puncture sites on neck of patient in Case Num- ber One. The examiner's fingertip in- dicates the suprasternal notch. B-D. Chronic ulcerations on the legs of this patient.
Haven Hospital complaining of in- tense pain in the right shoulder. She admitted a long history of parenteral heroin abuse, but denied a history of chest disease. Forty-eight hours prior to presentation she had self-injected her right IJV, her usual injection site, but experienced unusual difficulty withdrawing blood during venipunc- ture. Following injection she apparent- ly lost consciousness. Upon reviving, she began to suffer shortness of breath and pleuritic pain radiating to the right shoulder.
Physical examination revealed a well-developed woman with a BP of 140/70 mm Hg; pulse, 96/min; res- pirations, 20/rain; and temperature, 36.67 C. Her respirations were not la- bored. Needle track marks were noted on both sides of her neck well above
the clavicle, indicative of IJV injec- tion. Decreased breath sounds were noted over the right lung. Her right shoulder was normal. A 30% right pneumothorax was noted on chest film.
The patient was treated successfully by chest tube thoracostomy and was discharged after four days of hospital- ization.
Case Number Three A 23-year-old woman presented to
the emergency department of The Hospital of St Raphael complaining of shortness of breath and pleuritic right chest pain. The patient was known to have a long history of parenteral drug abuse, and she had undergone multi- ple hospitalizations for treatment of associated complications. Three days prior to presentation she had been dis- charged from the hospital following treatment for bilateral cellulitis of the hands. Immediately prior to presenta- tion, she had engaged the services of a professional "hit-man" to inject her- oin into her IJV. Insertion of the nee- dle into the right side of her neck pro-
yoked acute pleuritic pain and dysp- nea prior to the actual venipuncture and injection.
Examination revealed a BP of 100/ 70 mm Hg; pulse, 72/rain; resPira- tions, 18/min; and temperature, 36.33 C. Needle track marks were noted on her neck well above the clavicle. Both hands showed resolving cellulitis. Her chest examination was normal. A 20% right pneumothorax was found on chest film.
The patient was successfully treated by observation, serial roentgenograms that showed gradual resolution of the pneumothorax, and nasal oxygen. No chest tube was inserted. She was dis- charged after five days of hospitaliza- tion. Follow-up clinic examinations revealed complete resolution without recurrences of pneumothorax.
Case Number Four A 26-year-old woman presented to
the emergency department of Yale- New Haven Hospital with a com- plaint of pleuritic left chest pain. She had an eight-year history of parenteral heroin abuse. Several hours earlier she
86/168 Annals of Emergency Medicine 12:3 March 1983

Fig. 2. PA chest film demonstrating a 30% lef t p n e u m o t h o r a x in Case Number One.
had self-injected her left IJV, ex- periencing the immediate onset of pleuritic pain. She did not complain of dyspnea.
Physical examination revealed a blood pressure of 144/72 rnm Hg; pulse, ll6/min; respirations, 20/rain; and temperature, 38.1 C. She had fresh needle puncture marks on the left side of her neck, well above the clavicle. Examination of the chest re- vealed a loud friction rub over the lateral chest. On chest film, a 15% left apical pneumothorax was seen.
The patient refused treatment and left the hospital against medical ad- vice. No follow-up information is available.
Case Number Five A 22-year-old woman presented to
the emergency department at The Hospital of St Raphael complaining of pleuritic left chest pain. The patient admitted to a history of heroin abuse. Three weeks before she had been assisted by an associate in injecting her left IJV. She had immediately felt
shortness of breath and pleuritic pain, but did not seek medical attention. Several days later, pneumothorax was discovered during a screening chest film required for entry into a metha- done program. Referred to the emer- gency department of Yale-New Haven Hospital, she refused admission and left without treatment. Because of the persistence of her left chest pain, she finally sought treatment.
Her physical examination revealed a BP of 92/70 mm Hg; pulse, 80/rain; respirations, 20/min; and temperature, 37.3 C. Her breathing was not labored. Auscultation of the chest indicated decreased breath sounds over the left lung. Needle track marks were noted along both sides of her neck well above the clavicle. A 30% left pneu- mothorax was found on chest film.
The patient was successfully treated with chest tube thoracostomy and was discharged after five days of hos- pitalization.
Case Number Six A 23-year-old woman presented to
the emergency department of The Hospital of St Raphael complaining of substemal chest pain without associ- ated shortness of breath. She admitted to a long history of intravenous heroin and cocaine abuse that had resulted in the sclerosis of her peripheral veins, making them unsuitable for venipunc- ture. During the preceding 18 months she had regularly self-injected both in- ternal jugular veins. On the day of admission, she had attempted veni- puncture of the right internal jugular with return of mixed "light and dark" blood. She nevertheless injected co- caine and heroin and immediately ex- perienced substernal chest pain but no drug "high." She then apparently in- jected successfully into the left inter- nal jugular, obtaining a "high" but no pain relief. She then sought medical attention.
On physical examination, the pa- tient had a tachycardia of 100, blood pressure of 110/70 mm Hg, and mild tachypnea with a rate of 24. Needle scars were noted on the neck bilateral- ly in the area of the supraclavicular notch. Breath sounds were decreased over the right apex. No cardiac mur- mur was present. Chest film revealed a 20% right pneumothorax.
The patient refused to permit phle- botomy for laboratory testing and re- fused admission to the hospital. She left against medical advice, and no fol- low-up information is available.
DISCUSSION These six patients developed pneu-
mothorax as a traumatic complication of parenteral drug abuse. All had be- gun using the IJV site because years of self-injection had caused obliteration of t h e more accessible peripheral veins. Remarkably most of these pa- tients, and others we have seen, are regularly sticcessful in self-injecting the IJV, a process requiring both a steady hand and a knowledge of anat- omy. Most frequently they approach the IJV by inserting the needle at the inferolateral border of the stemomas- toid muscle and aiming toward the suprastemal notch.
Pneumothorax previously has been considered a relatively rare complica- tion of IJV injection and cannulation. Although listed among the possible side effects of IJV cannulation, iat-
12:3 March 1983 Annals of Emergency Medicine 169/87

PNEUMOTHORAX IN DRUG ABUSERS Bell, Borak & Loeffler
r o g e n i c p n e u m o t h o r a x has been documented in just a handful of pa- t ients, s7 Still more rare, pneumo- thorax caused by IJV injection of illicit drugs has been reported only once. s The possibility that our patients repre- sent a newly emerging complication of parenteral drug abuse is enhanced by the fact that during the five years prior to the presentation of our first patient, in mid 1980, no similar cases had been diagnosed at either The Hos- pital of St Raphael or Yale-New Haven Hospital.
The clinical complaints presented by these patients, particularly short- ness of breath and pleur i t ic chest pain, 24 were typical for vict ims of pneumothorax. Nevertheless, confu- sion and delay in reaching this diagno- sis may result from the tendency to attribute dyspnea among drug abusers to the pulmonary effects of heroin. 9 The reported occurrence of potentially
lethal tension pneumothorax in this s e t t i n g 8 h i g h l i g h t s t he n e e d for p rompt recogni t ion and t reatment . Failure to consider the site of injection as well as the type of drug used may resul t in m i s m a n a g e m e n t of drug abuse patients.
The authors acknowledge the secretarial excellence of Mrs Ida Apicella, and the bib- liographic assistance of Ms Patricia Wales, MSLS.
REFERENCES 1. Gellhoed GW, Joseph WL: Surgical se- quelae of drug abuse. Surg Gynecol Obstet 139:749-755, 1974.
2. Schwartz GR, Safar P, Stone JH, et al (eds): Principles and Practice of Emergency Medicine. Philadelphia, WB Saunders, 1978.
3. Wilkins EW, Dineen JJ, Moncure AC: MGH Textbook of Emergency Medicine. Baltimore, Williams and Wilkins, 1978.
4. Fraser RG, Pare JAP: Diagnosis of Dis- eases of the Chest. Philadelphia, WB Saun- ders, 1979.
5. English ICW, Frew RM, Pigott JF, et al: Percutaneous catheterization of the inter- nal jugular vein. Anaesthesia 24:521-531, 1969.
6. Cook TL, Dueker CW: Tension pneu- mothorax following internal jugular calmu- lation and general anesthesia. Anesthesiol- ogy 45:554-555, 1976.
7. McGoon MD, Benedetto PW, Green BM: Complications of percutaneous central venous catheterization: A report of two cases and review of the literature. Johns Hopkins Med J 145:1-6, 1979.
8. Lewis JW, Groux N, Elliott JP, et al: Complications of attempted central venous injections performed by drug abusers. Chest 78:613-617, 1980.
9. Becker CE: Medical complications of drug abuse, in Stollerman GH (ed): Ad- vances in Internal Medicine. Chicago, Year Book Publishers, 1979, vol 24, p 183-202.
88/170 Annals of Emergency Medicine 12:3 March 1983