Embed Size (px)
Citation preview
Point-Of-Care Testing in
Primary Care Kent Lewandrowski MD
Associate Chief Pathology
Director of Clinical Laboratories and Molecular Medicine)
Massachusetts General Hospital
Professor
Harvard Medical School

Laboratory Testing
On Airline Flights

Conventional Wisdom
POCT is:
• More expensive than central laboratory testing
• Is difficult to manage quality and documentation
• Is difficult to comply with regulatory requirements
For these reasons POCT should only be
performed if there is a demonstrable benefit
(e.g. outcomes)
Objectives
• Describe the classification of outcomes including
medical, financial and outcomes relating to
hospital operations
• Analyze different models for performing
laboratory testing in primary care
• Evaluate different tests that have been shown to
improve outcomes and practice efficiency in
primary care

5
Types Of Outcomes
• Medical outcomes: Live longer, better
– Very difficult to document
• Financial outcomes: Save money, more cost effective
– Complex and difficult to document
• Operations outcomes: Improve length of stay, improve efficiency, streamline processes
– Easier to document
Options for Obtaining Laboratory
Testing in Primary Care 1. Sending the patient to a central laboratory after the
office visit: Inconvenient for the patient.
Patient may never show up at the laboratory.
Prevents test results from being reviewed with the patient at the time of the office visit.
Follow-up letters and phone calls and follow-up office visits may be required.
2. Sending the patient to a central laboratory several days before the office visit:
Assumes the required tests can be anticipated in advance.
Patient may never show up at the laboratory.
Allows test results to be reviewed with the patient during the office visit.
Requires an extra trip to the laboratory which may be inconvenient and may incur costs including travel, parking and potentially lost wages.
Options for Obtaining Laboratory
Testing in Primary Care
3. Performing testing in the physician’s office
at the time of the patients visit using rapid POCT
devices:
Individual tests do not need to be anticipated in advance
Results can be reviewed directly with the patient.
Follow-up letters and phone calls may be reduced and revisits for abnormal
test results potentially eliminated.
Which choice would you prefer?
A Relative of Mine
• Saw physician for a chronic complaint
• Tests ordered and the patient was told to
go to a phlebotomy site 15 miles away
• Round trip would require several hours
away from work
• Due to inconvenience the patient never
went
Sample Acquisition: A Key Issue With Point-
of-Care Testing
• Most practices do not have on-site
phlebotomy
• Finger-stick tests therefore highly
desirable
• Alternate sample types useful in some
cases (e.g. salivary samples, urine)
• New technologies coming on the horizon
One New Technology
Place device on skin
Collects 20 uL of blood essentially without
pain
Future devices planned to collect a larger
sample
Key Factors Impacting POCT in
Primary Care
• Accuracy of the test
• Cost of testing supplies
• Labor cost
• Space
• Ease of use
• Need for finger stick or phlebotomy on-site
• Billing revenues
• Clinical impact of the test on patient care
• Clinical impact of the test on the practice
The All Important CLIA Waiver
Status In Primary Care
Office practice using only CLIA waived tests
• Requires certificate of waiver
• No routine inspections by regulators
• No proficiency testing required
Office practice using moderately complex tests
• Requires certificate of compliance
• Routine inspections by regulators
• Proficiency testing required
What Type of Practice is it?
• Private practice
Basically functions as a small business
Very sensitive to cost and revenue
• Hospital affiliated practice
Functions as a business unit in the larger organization
Very sensitive to annual budget
• Salaried staff physician
Functions as an employee of the organization
Sensitive to the overall organizational cost
Selected Traditional POCT Tests in
Primary Care Rapid Strep A
Influenza
Sexually transmitted diseases
Rapid HIV
Dipstick urinalysis
Pregnancy testing
HbA1c
Glucose
Fecal occult blood
PT-INR
Lipid panel
Examples of Missing Tests and Potentially
Emerging Tests
• CBC: No viable current options. A major missing piece in POCT
• Chemistry panels (CMP/BMP): Some options available but all require phlebotomy
• Thyroid screen: A common rule out for many patient presentations
• BNP/NT proBNP: Manage patients with heart failure: Some options available but all require phlebotomy
• Salivary DOA: Eliminates observation of urine sample collection
• Lyme serology: CDC estimates 300,000 cases annually
Case Example: HIV Testing
Over 1 million people in US infected with HIV
Over 250,000 unaware of their infection
CDC Guidelines
• Screen all people 13-64 years old
• Identify HIV infected patients and connect them
to early care
• Educate patients of risk factors
• Three quarters will modify at-risk behaviors
when they know their HIV status
The Problem
• Many at-risk patients have poor access to the health care system and are easily lost to follow-up
• Many never return to learn their results
• Kassler et al. AIDS 1997;11:1045-1051
Compared rapid testing to central laboratory testing
Rapid testing resulted in a 210% increase in patients learning their HIV status for uninfected and a 23% increase for infected patients
• Rapid in-office HIV tests result in more patients being tested and connected to follow-up care and education
Case Example: HbA1c for Diabetes Care
Clinical Utility of HbA1c
Traditional use:
Monitoring diabetic therapy
Requires reproducible assay
New uses (utilize fixed cut-points thus
assays must be accurate, reproducible
and free from bias)
Screening for diabetes
Diagnosis of diabetes
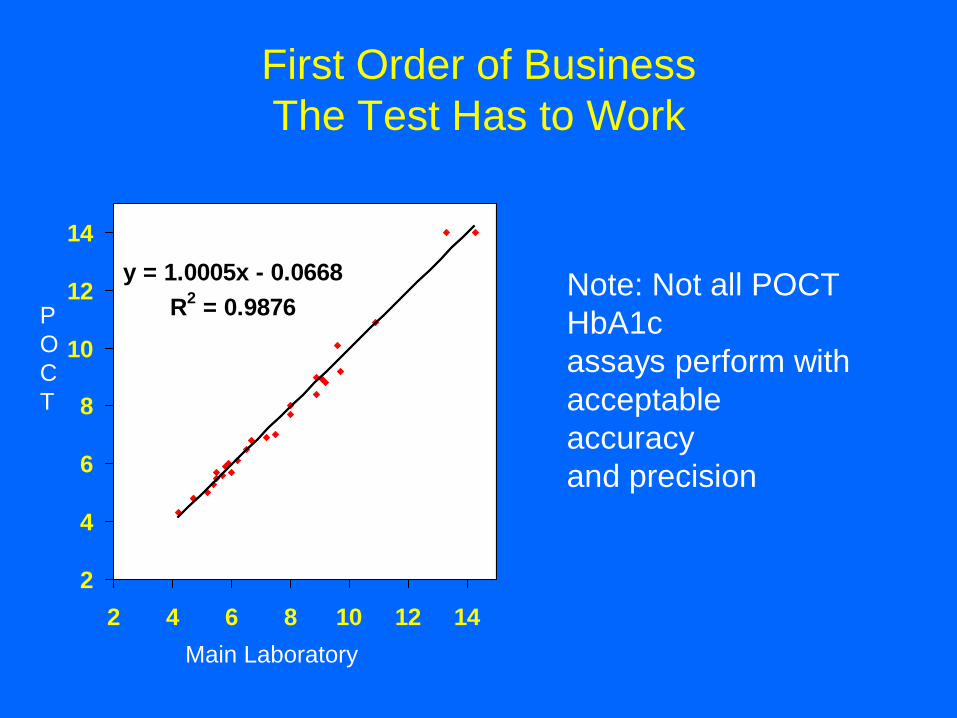
First Order of Business
The Test Has to Work
y = 1.0005x - 0.0668
R2 = 0.9876
2
4
6
8
10
12
14
2 4 6 8 10 12 14
Main Laboratory
P
O
C
T
Note: Not all POCT
HbA1c
assays perform with
acceptable
accuracy
and precision
A Word Of Caution On Some POCT Devices
Clin Chem 2010 Jan;56(1):44-52. Six of eight
hemoglobin A1c point-of-care instruments do not meet
the general accepted analytical performance criteria.
Lenters E and Slingerland
HbA1c devices should conform to standards of the
National Glycohemoglobin Standardization Program
Only 2 of eight POCT devices for HbA1c passed NGSP
criteria
POCT Outcomes: Glycemic Control
Some (but not all) studies of POCT for HbA1c
have shown an improvement in glycemic control
Cagliero et al, Diabetes Care 1999;22:1785-1789
Randomized controlled trial in 201 diabetic
patients
• HbA1c levels decreased over 6 and 12 months
with POCT by 0.57% and 0.40%
• No change in HbA1c in controls
Case Example: Rapid testing For
Strep A
Culture requires 18-24 hours: This delay leads to
over diagnosis and unnecessary preemptive
antibiotic usage
Clinical diagnosis is unreliable
One study: 48% of patients with pharyngitis
received antibiotics
Only 28% were positive by culture
Rapid strep A tests are highly specific but will
miss some cases of Strep A pharyngitis
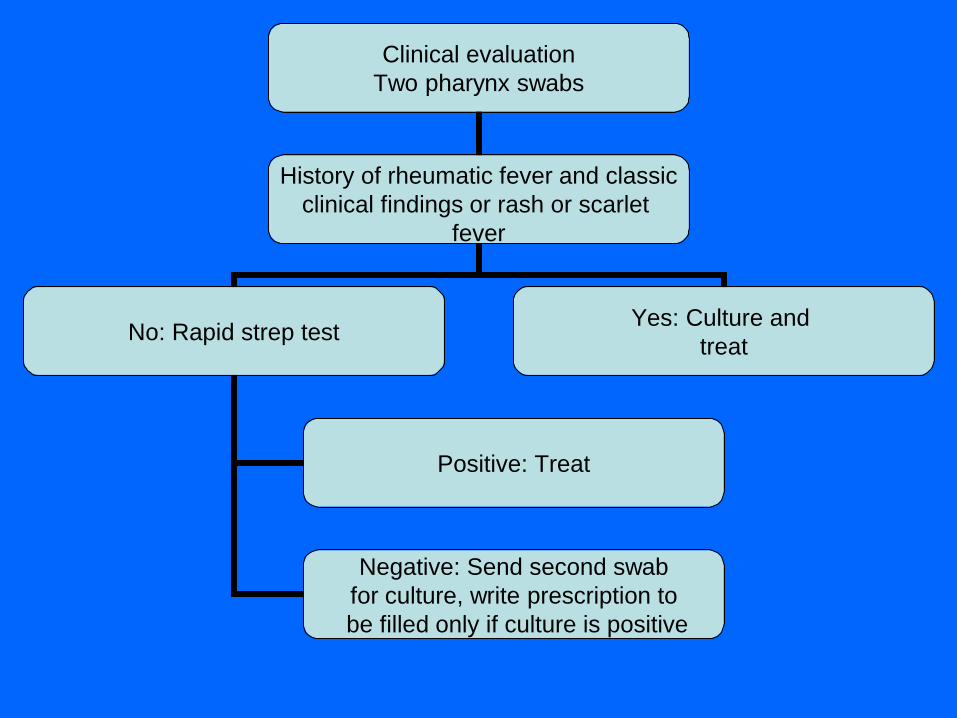
Clinical evaluation
Two pharynx swabs
History of rheumatic fever and classic
clinical findings or rash or scarlet
fever
No: Rapid strep test Yes: Culture and
treat
Positive: Treat
Negative: Send second swab
for culture, write prescription to
be filled only if culture is positive
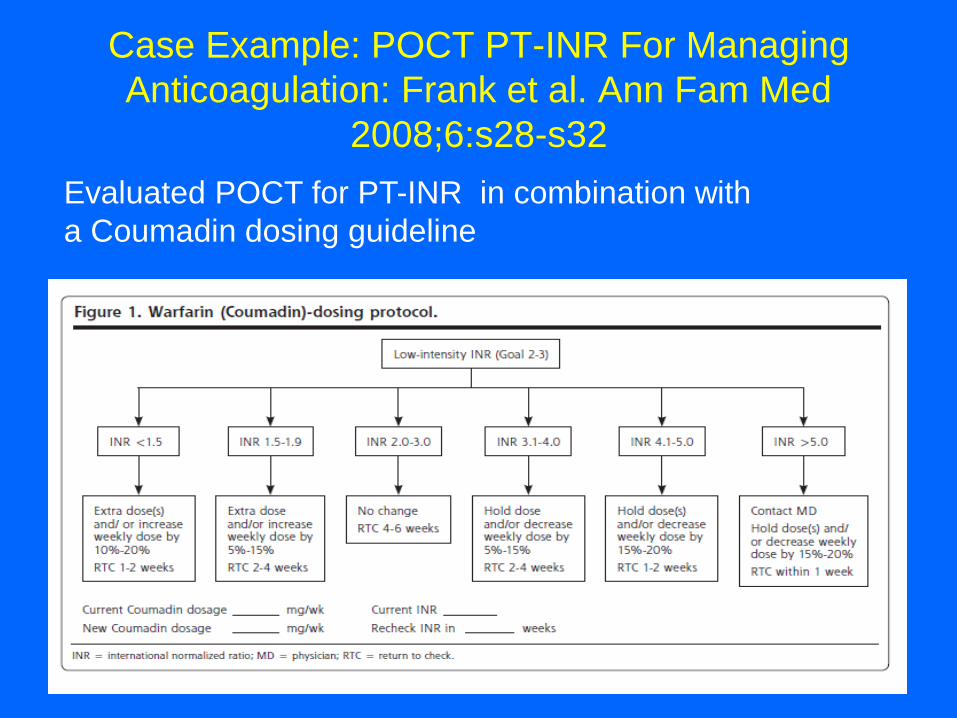
Case Example: POCT PT-INR For Managing
Anticoagulation: Frank et al. Ann Fam Med
2008;6:s28-s32
Evaluated POCT for PT-INR in combination with
a Coumadin dosing guideline
Results
Baseline control
32.1 % of patients within the INR goal
With POCT-INR
45.9 % of patients within INR goal
Reimbursement Models
• Traditional fee for service
• Global reimbursement or capitation
• Risk sharing reimbursement model
Each reimbursement model creates its own incentives and disincentives with regards to: – Practice costs
– Revenues
– Practice efficiency metrics
– System wide costs
Traditional Fee-For-Service
• Practice gets paid for each billable unit of
service it produces
• Outpatient labs often profitable
• Favors POCT assuming there are easy to
use devices that don’t require phlebotomy
Global Reimbursement or
Capitation
• Practice gets paid a fixed amount to provide all needed services
• Many carve-outs can create perverse incentives (e.g. lab carve-out)
• Strongly discourages POCT unless there is a carve-out
• Accountable Care Organizations (ACO’s) will introduce a global fee for all services to a healthcare organization (not an isolated practice)
The Basic Accountable Care Model
Doctors
Hospitals
Ancillary Services
Pharmacy
Other stakeholders
Risk Sharing Reimbursement
Contracts: Pay for Performance
The physician is typically subject to a
payment withhold pending performance of:
• Quality metrics
• Utilization metrics
• Financial metrics
Risk Sharing Reimbursement Contracts: An
Example for Patients With Diabetes
For Diabetes Care to be paid the withhold the
practice must perform
1. HbA1c twice a year
2. Annual urinary microalbumin
3. Annual lipid profile
4. Annual eye examination
Note 3 of 4 are laboratory tests
How often does the patient not go to the lab to get
the tests (especially less reliable patients)
A Key Element for the Future of POCT
in Primary Care
Reimbursement will progressively move towards global payments to the healthcare system including elements of:
• Capitation
• Risk sharing
• Pay for performance
The future of POCT in this new world will depend on:
• Reimbursement (or lack thereof)
• Demonstration of cost saving outcomes
• Dollars at risk in pay for performance contracts
MGH Study Patient Satisfaction With POCT
in Primary Care: Clin Chem Acta
2013;424:8-11
150 patients who received POCT were given an anonymous patient satisfaction survey at the end of their clinic visit.
Satisfaction scores were rated 1 to 4 (4 being the most satisfied). The surveys identified the tests that were performed and asked for additional comments.
Completed surveys were deposited in an anonymous collection
Patient Satisfaction Study Questionnaire
Compared with your past experiences of physician
office visits that did not have on-site testing please
rank your overall level of satisfaction with today’s
office visit:
Circle one:
1= poor (today was less satisfactory)
2= acceptable (today was about the same)
3= good (today was generally better
4= excellent (today was a much better experience)
Other comments:
Patient Satisfaction Survey At An
MGH Primary Care Practice
Results
Overall the mean satisfaction score on a scale of 1 (poor) to 4 (excellent) was 3.96.
Selected comments:
• Wonderful to have the results and directions for medications while I was here. It made the plan clear. Also a true time saver- not only a lab visit but follow-up phone calls
• It is so much easier to do it at the office while I am here.
• It was great to be able to consult immediately with the doctor having the results in front of us.
• I thinks it good to get the results while still talking to the doctor.

POCT may offer some advantages over centralized laboratory
testing including
• Reducing follow-up visits
• Eliminating letters and phone calls to patients regarding test
results
• Improved patient management by having the test results
available at the time of the office visit.
However, POCT must be financially viable to cover the
cost of the testing supplies and labor in the practice.
MGH Outcomes Study on POCT Cost and
Practice Efficiency Metrics
Implemented POCT for hemoglobin A1c (Siemens
Diagnostics), lipid panel and comprehensive metabolic panel
(Abaxis)
The cost of performing the testing was calculated using:
Cost of the reagents
Consumables (including phlebotomy)
Labor required for practice assistants to perform the testing.
Potential revenues were estimated using Medicare fee
schedules including a phlebotomy charge of $3.00.
Cost Analysis for POCT in Primary
Care
The average cost for testing was $25.25 per patient.
Estimated revenues were $31.87.
The per patient margin $6.62.
The revenues actually collected would depend on the payer
mix of the practice.
Using a margin of $6.62 per patient it would take
approximately 2266 patients to cover the cost of the capital
equipment.
Financial Analysis
Financial Analysis
Other cost reductions in the practice would add to the potential financial benefits of the POCT program including:
1. Costs incurred for writing and processing letters:
– A simple letter detailing normal findings costs $ 7.03 to the practice,
– A letter with minor abnormal findings costs $ 15.52
– A letter with major abnormal findings costs $ 29.67.
2. The cost of a typical phone call was estimated to be
$ 28.30
3. Costs incurred for follow-up visits are approximately $ 3.24 per minute including physician and office support staff labor.
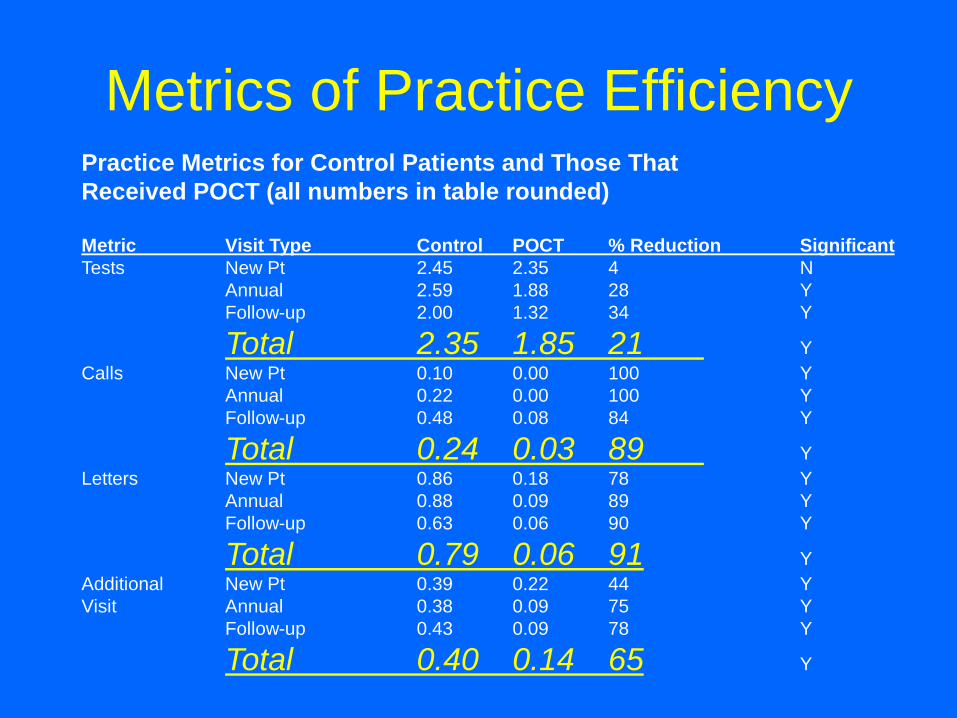
Practice Metrics for Control Patients and Those That
Received POCT (all numbers in table rounded)
Metric Visit Type Control POCT % Reduction Significant
Tests New Pt 2.45 2.35 4 N
Annual 2.59 1.88 28 Y
Follow-up 2.00 1.32 34 Y
Total 2.35 1.85 21 Y
Calls New Pt 0.10 0.00 100 Y
Annual 0.22 0.00 100 Y
Follow-up 0.48 0.08 84 Y
Total 0.24 0.03 89 Y
Letters New Pt 0.86 0.18 78 Y
Annual 0.88 0.09 89 Y
Follow-up 0.63 0.06 90 Y
Total 0.79 0.06 91 Y
Additional New Pt 0.39 0.22 44 Y
Visit Annual 0.38 0.09 75 Y
Follow-up 0.43 0.09 78 Y
Total 0.40 0.14 65 Y
Metrics of Practice Efficiency
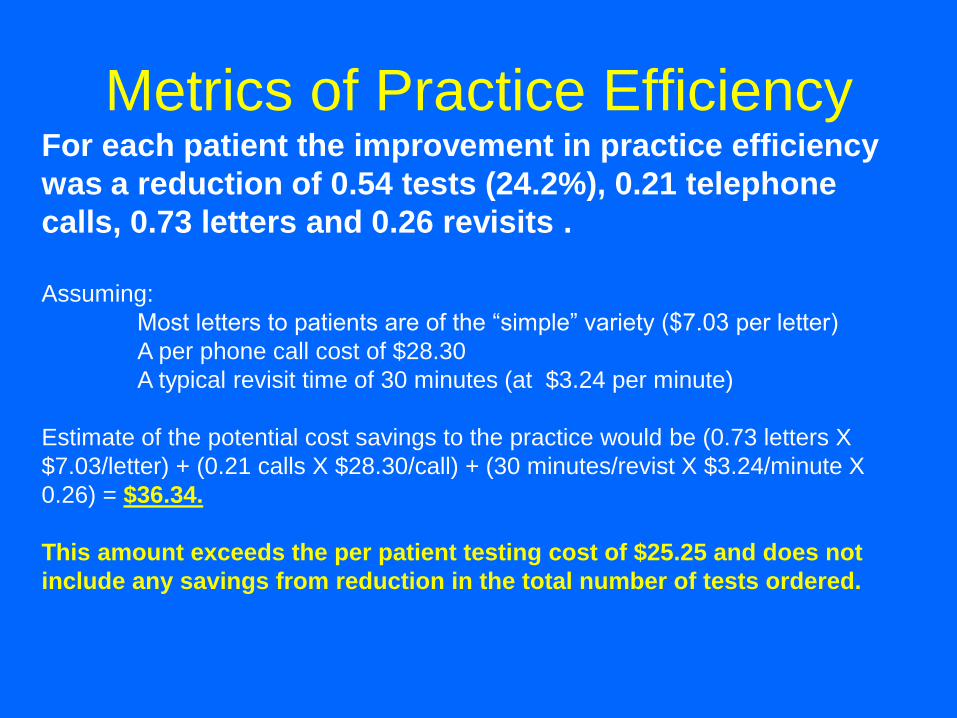
For each patient the improvement in practice efficiency
was a reduction of 0.54 tests (24.2%), 0.21 telephone
calls, 0.73 letters and 0.26 revisits .
Assuming:
Most letters to patients are of the “simple” variety ($7.03 per letter)
A per phone call cost of $28.30
A typical revisit time of 30 minutes (at $3.24 per minute)
Estimate of the potential cost savings to the practice would be (0.73 letters X
$7.03/letter) + (0.21 calls X $28.30/call) + (30 minutes/revist X $3.24/minute X
0.26) = $36.34.
This amount exceeds the per patient testing cost of $25.25 and does not
include any savings from reduction in the total number of tests ordered.
Metrics of Practice Efficiency
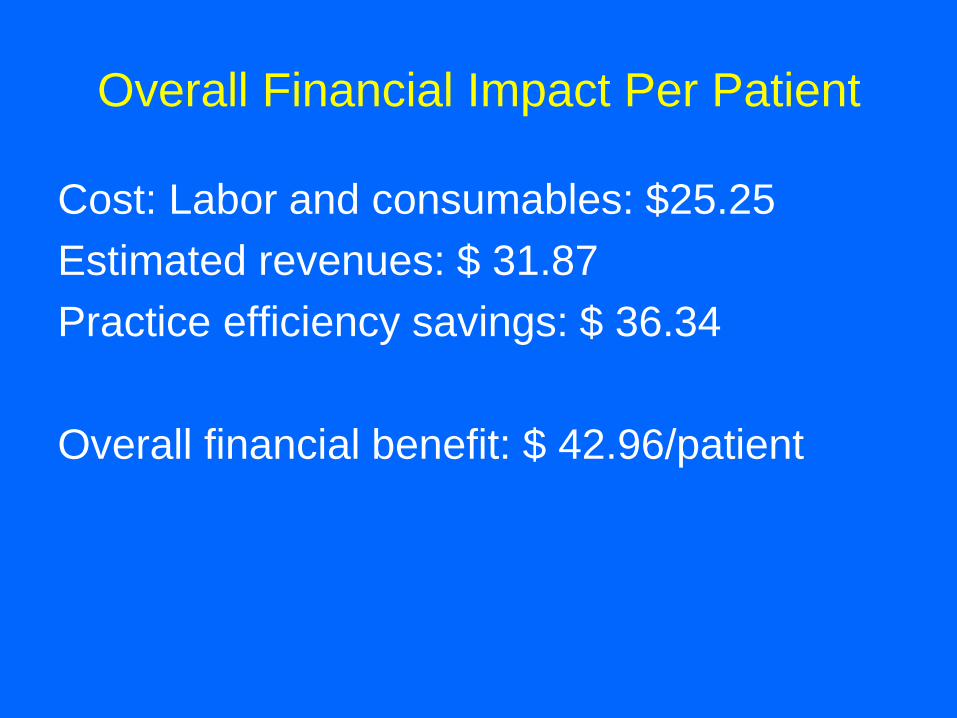
Overall Financial Impact Per Patient
Cost: Labor and consumables: $25.25
Estimated revenues: $ 31.87
Practice efficiency savings: $ 36.34
Overall financial benefit: $ 42.96/patient
Home Testing
(Analogous to over the counter medications)
• Blood Glucose
• Pregnancy
• Ovulation Testing
• Cholesterol
• Drugs of abuse
• HIV
• Coagulation (PT-INR)
• Occult blood
• Many Others
Includes at home test kits and specimen “mail in” testing
Who Wins With Home Testing
• Insurance carrier: Patient pays for all tests
and treatment (if any)
• Capitated physician practices
• The patient: Assuming they can afford the
tests and didn’t make a mistake
Remember When…..
• Motrin required a prescription
• The were no OTC drugs for yeast vaginitis
• OTC pregnancy tests did not exist
An example of the future trend: Recent FDA approval of an OTC salivary HIV test
As new products become available patients will take more of their care into their own hands
Conclusions: POCT in Primary
Care Can
• Improve patient satisfaction
• Improve practice efficiency
• May in selected cases improve outcomes
Conclusions: But…….
• More and improved technologies will be
required (e.g. CBC)
• More studies will be needed to
demonstrate improved outcomes
(financial, medical, or operations)
• Reimbursement models cannot create
disincentives
49