Embed Size (px)
Citation preview
Policy andStandards
to support the provision of AntenatalScreening in
Wales
December 2005
Policy and Standards to supportthe provision of AntenatalScreening in Wales
December 2005
2
Public consultation on these standards was held fromOctober 2004 to February 2005.
Antenatal Screening Wales are extremely grateful to thosewho took the time to respond to the consultation. Allconsultation responses have been reviewed by the AllWales Multi Professional Management Group (AWMMG)and changes recommended by the AWMMG have beenincorporated in this document.
Copies of this document are available from the AntenatalScreening Wales office:
Antenatal Screening Wales18, Cathedral Road CardiffCF11 9LJ02920 787837

3
1.0 Introduction 4
2.0 Wales Antenatal Screening Policy 6
3.0 Antenatal Screening for rubella susceptibility 8
4.0 Antenatal Screening for syphilis 10
5.0 Antenatal Screening for hepatitis B 12
6.0 Antenatal Screening for HIV 14
7.0 Ultrasound: Early pregnancy ultrasound dating scan 16
8.0 Ultrasound: fetal anomaly scan 18
9.0 Antenatal Screening for blood group and antibodies 20
10.0 Antenatal Screening for sickle cell and thalassaemia 22
11.0 Antenatal Screening for Down’s syndrome 24
12.0 References 26
13.0 Explanatory notes 27
Contents

4
1.0 Introduction
1.1 The need for improvements in antenatal screening and recommendations for the managementof antenatal screening were consulted on by the Antenatal Screening Project in 2001 in its report ‘Choices’ - Recommendations for the Provision and Management of Antenatal Screening in Wales (available on www.antenatalscreening.org).
In April 2003 the Minister for Health and Social Services agreed that a Managed Clinical Networkfor antenatal screening should be established in Wales, based on the principles described in theAntenatal Screening Project Report ‘Choices’. The network is known as Antenatal ScreeningWales (ASW) and is hosted by Velindre NHS Trust Screening Services.
ASW has developed, printed and provided to Trusts written information for women on antenatalscreening tests. The information is also available on the ASW web site.
ASW has been asked by the Welsh Assembly Government to establish policies, standards and aperformance management framework for antenatal screening. It is intended that theimplementation of the standards and protocols will support demonstrable improvements in thequality of antenatal screening offered to women. The implementation of the standards will bemonitored by the ASW all Wales Performance Management Framework and BalancedScorecard.
The liability for antenatal screening provision continues to rest with the provider Trust/PowysLHB. Similarly the responsibility for implementing antenatal screening protocols to meet theproposed standards rests with NHS Trusts/ Powys LHB.
There are a number of important United Kingdom (UK) documents which support antenatalscreening and the work of the UK National Screening committee (NSC) is ongoing. Theseminimum standards have been drawn from the many recommendations of the NationalInstitute for Clinical Excellence (NICE), NSC, specific laboratory national standards, the advice ofRoyal Colleges and good practice models. These standards should be implemented with dueregard to the recommendations contained in supporting literature e.g. guidance of ProfessionalBodies, Royal Colleges and Welsh Risk Pool Standards.
A review of antenatal screening services by questionnaire and site visits was undertaken inOctober to December 2004. Information gained from this comprehensive review combinedwith advice from the three Local Multiprofessional Management Groups (LMMG) and a publicconsultation (‘Making Decisions’ available on www.antenatalscreening.org) have been used toset minimum service standards.
1.2 Purpose of the Antenatal Screening Programme in Wales
The Antenatal Screening Project proposed, and consulted on the following as the definition ofthe purpose of antenatal screening;
Antenatal screening is undertaken to detect defined serious conditions present in eitherthe mother or baby that are likely to have an adverse effect on the health of either, andfor which an effective intervention is available and warranted.
For some conditions, preventive treatment is available during the antenatal period orafter delivery to improve the baby’s health.
For others, the condition can be identified during the antenatal period but nopreventive treatment is available. With high quality counselling women can make aninformed choice about whether they wish to continue the pregnancy and appropriatesupport, depending on their ultimate choice, can be arranged.
5
1.3 Principles for the provision of antenatal screening tests
• Verbal, written and information in other media must be provided by health professionals in atimely and non directive manner to the pregnant woman to support informed decisionmaking.
• All women must give informed verbal consent before having any antenatal screening test anda record of her verbal consent made in the maternity notes.
• All women should be informed of their antenatal screening test results in a timely andappropriate way.
Adequate records of all antenatal screening activity must be maintained in the woman’smaternity notes.
1.4 Programme management
The UK National Screening Committee has made recommendations to improve the organisationand management of screening programmes and to maximise the benefits of the screening testand reduce the risks of harm to individuals.
As agreed by the Welsh Assembly Government and building on the recommendations andprinciples set out in ‘Choices’, the management of the antenatal screening programme inWales is coordinated by a Managed Clinical Network called Antenatal Screening Wales. The network operates at three levels i.e.
• Nationally by the All Wales Multiprofessional Management Group
• Regionally by the Local Multiprofessional Management Group
• Locally, coordinated by a named screening midwife/local coordinator in each NHS Trust whois responsible for managing and coordinating the local antenatal screening programme.
1.5 Health professional education
Appropriate multiprofessional education must be planned and provided for all healthprofessionals involved in antenatal screening by the Trust/Powys LHB. It is recommended thatthis education programme is coordinated by the screening midwife/local coordinator, who isalso responsible for preparing an annual Antenatal Screening Education Report. The screeningmidwife/ local coordinator should make appropriate links with the local generic trainingcoordinator and other practice development staff when developing the programme.
6
2.0 Wales Antenatal Screening Policy
Antenatal screening services must be provided to meet the requirements of the all Walesantenatal screening policy i.e.
Antenatal screening should be offered for;
• Rubella susceptibility a
• Syphilisa a
• Hepatitis B a,b
• HIV (human immunodeficiency virus) a,c,d
• Rhesus antibodies a
• Down’s syndrome which provides a minimum of a 60% detection rate for a 5% falsepositive rate and is supported by early pregnancy ultrasound scanning a,e
• Sickle cell and thalassaemia for all pregnant women at an increased risk of having a childaffected by a sickle cell disorder or thalassaemia major. e,f
All women should also be offered the following ultrasound scans;
• Early pregnancy ultrasound scan (10 to 13+6 weeks of pregnancy) a, e
• Fetal anomaly ultrasound scan (18 to 20 weeks of pregnancy) a, g
Antenatal screening for the following conditions is not currently supported by NICE for theirefficacy and/or cost effectiveness and therefore are not included in this framework and shouldnot be offered as part of the antenatal screening programme;
Asymptomatic bacterial vaginosisChlamydia trachomatisCytomegalovirusHepatitis C virusStreptococcus Group BToxoplasmosisVitamin D screening.
2.1 Minimum standards for screening tests
Minimum standards for each element of the antenatal screening programme, mainly based onexisting national standards, have been selected to establish an agreed and coordinatedframework specifically for all antenatal screening services to ensure an equitable and consistentapproach. These minimum standards are set out by each test included in the programme insections 3 to 10.
a National Institute of Clinical Excellence (NICE 2003) CG6 Antenatal Care – routine care for the healthy pregnant woman.www.nice.org.uk.
b Welsh Office (1998) Screening of pregnant women for hepatitis B and immunisation of babies at risk.WHC(98)36.
c National Assembly for Wales (2000) Antenatal screening to reduce mother to baby transmission of HIV. Cardiff: National Assembly forWales.
d WHC (2002) 06 Service and Financial Planning Framework (2003).
e WHC (2003) 127 Annual Priorities and Planning Guidance for Services and Financial Planning Framework (2004);1.6.
f For the purpose of antenatal screening, these women are defined as • women, or women with partners who have a family history of sickle cell or thalassaemia• women who have unexplained anaemia• women or women with partners who’s family, no matter how many generations back, came from anywhere in the world apart from
the United Kingdom and the Republic of Ireland• women who do not know their family history – for example, they were adopted.
g Royal College of Obstetricians and Gynaecologists Routine. (2000) Routine ultrasound screening in pregnancy, protocols, standardsand training. Supplement to ultrasound screening for fetal abnormalities. Report of the RCOG working party. London: RCOG Press.

7
Antenatal screening tests are provided by radiology, pathology, genetics and haematologyservices as a small part of that departments services. Each specialty also has its own specificstandards to quality assure its services to the public.
Laboratories performing screening tests must use contemporaneous and relevant guidelines,such bodies such as DoH, RCPath etc, to direct their practice. Departures from such guidelinesmay be necessary when ‘best practice’ has moved on or the availability of tests has changed;however any such departurtes must be justified.
2.2 Clinical pathways for antenatal screening
Locally appropriate clinical pathways for antenatal screening are required. It is proposed thateach clinical pathway has, as a minimum, the following clearly defined elements:
• local arrangements for giving pre test information and offering the test
• local arrangements for provision of the test
• record keeping arrangements
• arrangements ensuring agreed timescales are met
• results handling process
• provision of counselling and support if required
• arrangements for necessary antenatal and immediate postnatal care and follow-up
• arrangements for referral to other agencies if required.
Documentation of locally agreed clinical pathways is in progress within Trusts/ Powys LBH.

8
3.0 Antenatal screening for rubella susceptibility
3.1 Policy:
All women resident in Wales should be offered antenatal screening for rubella susceptibility(NICE 2003).
3.2 Rationale:
To identify rubella susceptibility (i.e. antibodies less than 10 IU/ml) in pregnant women. Ifidentified by screening, these women can be given appropriate advice regarding immunisationwith Measles, Mumps and Rubella vaccine (MMR) following completion of the pregnancy. Theaim of the MMR immunisation is to reduce the risk of congenital rubella syndrome insubsequent pregnancies.
Screening to assess antenatal rubella susceptibility does not identify or prevent congenitalrubella syndrome in the current pregnancy.
3.3 Standards for antenatal screening for rubella susceptibility
S 3.1 The woman must be given verbal and written pre test information1 and a record of theinformation provided made in the maternity notes.
S 3.2 The woman’s informed verbal consent is required for this test and a record of herconsent must be made in the maternity notes.
S 3.3 Rubella susceptibility screening should be offered and the sample taken in earlypregnancy.
S 3.4 The laboratory request form must require a signature and the identification of thesample as ‘antenatal screening’. If a single request form is used for multiple screeningtests, the form must require a clear indication of the screening tests to which thewoman has given consent and those that are declined. 2
S 3.5 A record of the sample being taken must be made in the maternity notes.
S 3.6 The test should be undertaken by a laboratory that is either accredited by CPA (UK)Ltd.3 or has enrolled in the process of obtaining this standard.
S 3.7 The sample should normally be received by the local/forwarding laboratory4 within 24 hours of the sample being taken.
Developmental Minimum standard to be achieved by September 2006;90% of antenatal screening samples should be received by the local/ forwardinglaboratory4 within 24 hours of the sample being taken.
S 3.8 The testing laboratory must provide the test result to the maternity service within 7 working days of the sample being received by the testing laboratory.
Developmental Minimum standard to be achieved by September 2006;75% of antenatal screening test results should be provided to the maternity servicewithin 7 working days of the sample being received by the testing laboratory.

9
S 3.9 Women should be informed of the result by the maternity service within 15 workingdays of the sample being taken.
Developmental Minimum standard to be achieved by September 2006;90% of women should be informed of the result by the maternity service within 20 working days of the sample being taken.
S 3.10 A record of the test result should be made in the maternity notes.
S 3.11 If the woman is rubella susceptible (less than 10 IU/ml), immunisation with MMR mustbe offered and provided by the maternity service when the pregnancy is completed.

4.3 Standards for antenatal screening for syphilis
S 4.1 The woman must be given verbal and written pre test information1 and a record of theinformation provided made in the maternity notes.
S 4.2 The woman’s informed verbal consent is required for this test and a record of herconsent must be made in the maternity notes.
S 4.3 Whenever possible screening should be offered and the sample taken before 13 weeksof pregnancy to enable maternal treatment of women with syphilis to start promptlyand to reduce the risk of fetal damage.
S 4.4 A record of the sample being taken must be made in the maternity notes.
S 4.5 The laboratory request form must require a signature and the identification of thesample as ‘antenatal screening’. If a single request form is used for multiple screeningtests, the form must require a clear indication of the screening tests to which thewoman has given consent and those that are declined.2
S 4.6 The test should be undertaken by a laboratory that is either accredited by CPA (UK)Ltd.3 or has enrolled in the process of obtaining this standard.
S 4.7 The sample should normally be received by the local/forwarding laboratory4 within 24 hours of the sample being taken.
Developmental Minimum Standard to be achieved by September 2006; 90% of antenatal screening samples should be received by the local/ forwardinglaboratory4 within 24 hours of the sample being taken.
S 4.8 The testing laboratory must provide the test result to the maternity services within 7 working days of the sample being received by the testing laboratory.
Developmental Minimum Standard to be achieved by September 2006;75% of antenatal screening test results should be provided to the maternity service within 7 working days of the sample being received by the testing laboratory.
S 4.9 Women should be informed of the result by the maternity service within 15 working days of the sample being taken.
Developmental Minimum Standard to be achieved by September 2006;90% of women should be informed of the result by the maternity service within 20 working days of the sample being taken.
10
4.0 Antenatal screening for syphilis
4.1 Policy:
All women resident in Wales should be offered antenatal screening for syphilis(NICE 2003).
4.2 Rationale:
To identify and treat in early pregnancy women who have syphilis. Appropriate treatment ofwomen infected with syphilis in early pregnancy will reduce the risks of the fetus contractingcongenital syphilis. The identification and treatment of this communicable disease also hasconsiderable health benefits for the mother.

S 4.10 Confirmed syphilis positive test results indicating current infection should betelephoned to the consultant obstetrician, screening midwife or named deputy. Urgentarrangements (within 3 working days) should be made for the woman to return to theantenatal clinic for the result.
The result should not be electronically transferred from the laboratory to the maternityor other services unless appropriate security arrangements are in place to ensure theresult can only be accessed by locally agreed named individuals.
S 4.11 Syphilis is a rare condition in the UK; only locally agreed named health professionalswith suitable skills and knowledge should give the result to the woman. All womenwith a confirmed syphilis positive result should be referred to a specialist inGenitourinary Medicine for assessment, counselling and possible treatment.
S 4.12 A record of the test result should normally be made be in the maternity notes but awoman’s suspected or confirmed syphilis positive status should;
• only be recorded on the maternity information system with the woman’s informed consent
• only be written in an appropriate way in the hospital maternity notes
• not be written on blood request forms or other request forms if hospital staff unconnected to the woman’s care will have unnecessary access to this information.
11
12
5.3 Antenatal screening for hepatitis B
S 5.1 The woman must be given verbal and written pre test information1 and a record of theinformation provided made in the maternity notes.
S 5.2 The woman’s informed verbal consent is required for this test and a record of herconsent must be made in the maternity notes.
S 5.3 The laboratory request form must require a signature and the identification of thesample as ‘antenatal screening’. If a single request form is used for multiple screeningtests, the form must require a clear indication of the screening tests to which thewoman has given consent and those that are declined.2
S 5.4 A record of the sample being taken must be made in the maternity notes.
S 5.5 The test should be undertaken by a laboratory that is either accredited by CPA (UK)Ltd. 3 or has enrolled in the process of obtaining this standard.
S 5.6 The sample should normally be received by the local/forwarding laboratory4 within 24 hours of the sample being taken.
Developmental Minimum Standard to be achieved by September 2006;90% of antenatal screening samples should be received by the local/ forwardinglaboratory4 within 24 hours of the sample being taken.
S 5.7 The testing laboratory should provide the test result to the maternity service within 7 working days of the sample being received by the testing laboratory.
Developmental Minimum Standard to be achieved by September 2006;75% of antenatal screening test results should be provided to the maternity servicewithin 7 working days of the sample being received by the testing laboratory.
S 5.8 Women should be informed of the result by the maternity service within 15 workingdays of the sample being taken.
Developmental Minimum Standard to be achieved by September 2006;90% of women should be informed of the result by the maternity service within 20 working days of the sample being taken.
S 5.9 Confirmed hepatitis B positive test results should be reported to the consultantobstetrician, screening midwife or named deputy so arrangements can be made forthe woman to return to clinic for the result.
The result should not be electronically transferred from the laboratory to the maternity or other services unless appropriate security arrangements are in place to ensure theresult can only be accessed by locally agreed named individuals.
5.0 Antenatal screening for hepatitis B
5.1 Policy:
All women resident in Wales should be offered antenatal screening for hepatitis B (Welsh Office 1998, NICE 2003).
5.2 Rationale:
To enable the identification of chronic hepatitis B carriers whose infants will be at significant riskof contracting hepatitis B. These babies can then be offered a programme of immunisation,which usually successfully protects the neonate against hepatitis B infection.

13
S 5.10 If the woman is hepatitis B positive, only locally agreed named health professionalswith suitable skills and knowledge should give the result to the woman.
S 5.11 Arrangements should be made in the antenatal period for infants of women who arehepatitis B positive to receive appropriate immunisation as soon as possible after birth.
S 5.12 A record of the test result should normally be made in the maternity notes but awoman’s hepatitis B positive status should:
• only be recorded on the maternity information system with the woman’s informed consent
• only be written in an appropriate way in the hospital maternity notes
• not be written on blood request forms or other request forms if hospital staff unconnected to the woman’s care will have unnecessary access to this information.
Additional InformationArrangements should be in place for the baby to receive the accelerated hepatitis Bimmunisation programme and for family members of women who are hepatitis B positiveto be offered screening and immunisation as recommended in the WHC (98) 36.

14
6.3 Standards for antenatal HIV screening
S 6.1 The woman must be given verbal and written pre test information1 and a record of theinformation provided made in the maternity notes.
S 6.2 The woman’s informed verbal consent is required for this test and a record of herconsent must be made in the maternity notes.
S 6.3 Whenever possible, screening should be offered and the sample taken before 13 weeksof pregnancy to enable treatment of women who are HIV positive to start and reducethe risk of mother to child transmission.
S 6.4 The laboratory request form must require the identification of the sample as ‘antenatalscreening’. If a single request form is used for multiple screening tests, the form mustrequire a clear indication of the screening tests to which the woman has given consentand those that are declined.2
S 6.5 A record of the sample being taken must be made in the maternity notes.
S 6.6 The test should be undertaken by a laboratory that is either accredited by CPA (UK) Ltd.3
or has enrolled in the process of obtaining this standard.
S 6.7 The sample should normally be received by the local/forwarding laboratory4 within 24 hours of the sample being taken.
Developmental Minimum Standard to be achieved by September 2006;90% of antenatal screening samples should be received by the local/ forwardinglaboratory4 within 24 hours of the sample being taken.
S 6.8 The testing laboratory must provide the test result to the maternity service within 7 working days of the sample being received by the testing laboratory.
Developmental Minimum Standard to be achieved by September 2006;75% of antenatal screening test results should be provided to the maternity servicewithin 7 working days of the sample being received by the testing laboratory.
S 6.9 Women should be informed of the result by the maternity service within 15 workingdays of the sample being taken.
Developmental Minimum Standard to be achieved by September 2006;90% of women should be informed of the result by the maternity service within 20 working days of the sample being taken.
S 6.10 Local arrangements must be established to ensure that HIV positive results are given towomen appropriately by locally agreed named health professionals with suitable skillsand knowledge and that confidentiality regarding this result is maintained.
6.0 Antenatal screening for HIV
6.1 Policy:
All women resident in Wales should be offered antenatal screening for HIV (National Assembly for Wales 2000, NICE 2003).
6.2 Rationale:
To identify women who have HIV so that treatment and care can be offered to reduce the riskof mother to baby transmission of the virus. The identification and treatment of HIV also hasconsiderable health benefits for the woman.

15
S 6.11 HIV positive results must not be electronically transferred from the laboratory to thematernity or other services unless appropriate security arrangements are in place toensure the result can only be accessed by locally agreed named individuals.
S 6.12 A record of the test result should normally be made in the maternity notes but thewoman’s HIV positive status should:
• only be recorded on the maternity information system with the woman’s informed consent
• only be written in an appropriate way in the hospital maternity notes
• not be written on blood request forms or other request forms if hospital staff unconnected to the woman’s care will have unnecessary access to this information.
Additional InformationWomen who have not been offered an HIV screening test in the antenatal period shouldbe offered the test in the immediate postnatal period (National Assembly for Wales 2000).
16
7.3 Standards for an early pregnancy ultrasound dating scan
S 7.1 The woman must be given verbal and written pre test information1 and a record of theinformation provided made in the maternity notes.
S 7.2 The woman’s informed verbal consent is required for this test and a record of herconsent must be made in the maternity notes.
S 7.3 Early pregnancy ultrasound dating scans should be requested on an appropriate locallydetermined request form and require the signature of a health professional.
(By signing the request form the requesting health professional is confirming thatwritten and/or verbal information about the purpose of the scan has been given to thewoman and that informed consent has been given for the test.)
S 7.4 Accurate demographic and relevant clinical information must be included on theultrasound request form. Relevant obstetric, medical and social issues which can affectfetal well being should be provided on the ultrasound request form includinginformation about;
• maternal diabetes
• epilepsy (and medication if taken)
• prescribed and non prescribed drugs and
• excess alcohol intake.
S 7.5 Only an appropriately trained sonographer should perform ultrasound scans.5
S 7.6 The equipment must be of an appropriate standard as outlined in RCOG (2000) andNICE (2003).
S 7.7 The gestation should be calculated using the CRL measurement up to 12+6 weeksgestation (i.e. 66mm or less) and BPD after 13 weeks (i.e. if the CRL is greater than66mm).
S 7.8 The woman should be given verbal information on the findings of the scan by thesonographer.
If an abnormality is not identified, the woman should be provided with a writteninformation leaflet1 by the sonographer to explain the scan result.
7.0 Ultrasound: Early pregnancy ultrasound dating scan
7.1 Policy:
All women resident in Wales should be offered an early pregnancy ultrasound dating scan (NICE 2003).
7.2 Rationale:The early pregnancy ultrasound dating scan is offered to determine viability, the gestational ageand to detect multiple pregnancies. This will improve the performance of the Down’s syndromescreening serum test and reduce the need for post term induction of labour (NICE 2003).

17
S 7.9 If the pregnancy is ongoing and a problem is identified, an appropriately trainedmidwife or obstetrician should see the woman within 24 hours.
Developmental Minimum Standard to be achieved by September 2006;90% of women should be seen within 24 hours by an appropriately trained midwife or obstetrician if the pregnancy is ongoing and a problem is identified.
S 7.10 A record that the ultrasound scan has been performed and the result should be madein the maternity notes.
S 7.11 A full record of the findings must be made in the ultrasound department records asdetermined locally.
S 7.12 As a minimum standard, the sonographer should report;
• presence or absence of a fetus;
• viability (i.e. presence of heart pulsation and fetal movement);
• CRL (up to 66mm) or BPD as appropriate;
• fetal number and in multiple pregnancies the chorionicity and amnionicity;
• any gross fetal abnormality which is seen.
S 7.13 If indicated, following an abnormal ultrasound scan, women should be offered anappointment and seen in a fetal medicine department.
Developmental Minimum Standard to be achieved by September 2006;90% of women should be seen within 3 working days in a fetal medicine department.
S 7.14 If nuchal translucency screening is provided by the Trust, it must meet the NSCstandards and guidance6 and be part of the locally agreed, funded and monitoredscreening programme of the Trust.
NB: Currently Neath Port Talbot Maternity Unit is the only NHS service in Wales providing thecombined test. This is part of a feasibility project in cooperation with Antenatal ScreeningWales. Further discussion on whether this screening method should be recommended forintroduction in other Trusts in Wales is planned.

18
8.3 Standards for a fetal anomaly scan
S 8.1 The woman must be given verbal and written pre test information1 and a record of theinformation provided made in the maternity notes.
S 8.2 The woman’s informed verbal consent is required for this test and a record of herconsent must be made in the maternity notes.
S 8.3 Fetal anomaly ultrasound scans should be requested on an appropriate locallydetermined form and require the signature of a health professional.
(By signing the request form the requesting health professional is confirming thatwritten and/or verbal information about the purpose of the scan has been given to thewoman and that informed consent has been given for the test).
S 8.4 Accurate demographic and relevant clinical information must be included on theultrasound request form. Relevant obstetric, medical and social issues which can affectfetal well being should be provided on the ultrasound request form includinginformation about; • maternal diabetes• epilepsy (and medication if taken) • prescribed and non prescribed drugs and • excess alcohol intake.
S 8.5 Only an appropriately trained sonographer should perform ultrasound scans.5
S 8.6 The equipment must be of an appropriate standard as outlined in RCOG (2000) andNICE (2003).
S 8.7 A record that the ultrasound scan has been performed and the result should be madein the maternity notes.
S 8.8 A full record of the findings must be made in the ultrasound department records asdetermined locally.
S 8.9 The minimum standard for the 18 to 20 week fetal anomaly ultrasound scan, as setout by NICE (2003) and the RCOG (2000), should be achieved if possible. 7, 8
8.0 Ultrasound: fetal anomaly scan
8.1 Policy:
All women resident in Wales should be offered a fetal anomaly ultrasound scan at 18 to 20 weeks of pregnancy (NICE 2003, RCOG 2000).
8.2 Rationale:To detect major structural fetal anomalies that are likely to have an adverse effect on the healthof the mother or baby, and for which an effective intervention is available and warranted. Forsome conditions, preventive treatment is available during the antenatal period or after deliveryto improve the baby’s health. For others, the condition can be identified by ultrasound scanningbut no preventive treatment is available. Women can make an informed decision aboutwhether they wish to continue the pregnancy.

19
S 8.10 In Trusts/ Powys LHB where there is resource and capacity, the following additionalfindings should be reported;• cardiac outflow tracts • face and lips.
Developmental Minimum Standard to be achieved by September 2006;All Trusts/Powys LHB where scanning for cardiac outflow tracts, face and lips is notcurrently offered should develop a training plan for sonographers.
S 8.11 The woman should be given verbal information on the findings of the scan by thesonographer.
If an abnormality is not identified, the woman should also be provided with a writteninformation leaflet1 by the sonographer to explain the scan result.
S 8.12 If an abnormality is suspected on the fetal anomaly scan, the woman should be seenwithin 24 hours by an appropriately trained midwife or obstetrician.
Developmental Minimum Standard to be achieved by September 2006;90% of women should be seen within 24 hours by an appropriately trained midwife or obstetrician if an abnormality is suspected on the fetal anomaly scan.
S 8.13 If indicated, following an abnormal ultrasound scan, women should be offered anappointment and seen in a fetal medicine department.
Developmental Minimum Standard to be achieved by September 2006;90% of women should be seen within 3 working days in a fetal medicine department.
S 8.14 If indicated, following a confirmed abnormal fetal anomaly ultrasound scan, thewoman should be seen within 7 working days by a fetal cardiologist.
Developmental Minimum Standard to be achieved by September 2006;If indicated, following a confirmed abnormal fetal anomaly ultrasound scan, 50% ofwomen should be seen within 7 working days by a fetal cardiologist.
Additional InformationSeparate guidance has been published by ASW regarding the reporting of specificultrasound findings.
20
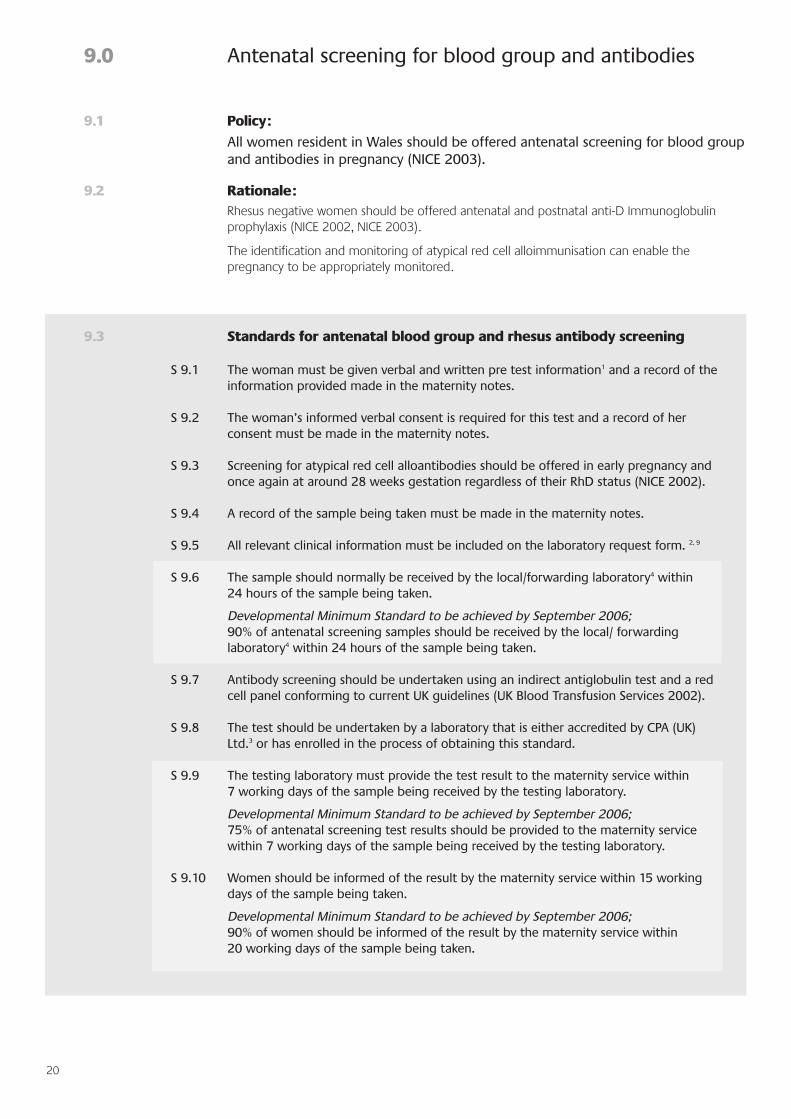
9.3 Standards for antenatal blood group and rhesus antibody screening
S 9.1 The woman must be given verbal and written pre test information1 and a record of theinformation provided made in the maternity notes.
S 9.2 The woman’s informed verbal consent is required for this test and a record of herconsent must be made in the maternity notes.
S 9.3 Screening for atypical red cell alloantibodies should be offered in early pregnancy andonce again at around 28 weeks gestation regardless of their RhD status (NICE 2002).
S 9.4 A record of the sample being taken must be made in the maternity notes.
S 9.5 All relevant clinical information must be included on the laboratory request form. 2, 9
S 9.6 The sample should normally be received by the local/forwarding laboratory4 within 24 hours of the sample being taken.
Developmental Minimum Standard to be achieved by September 2006; 90% of antenatal screening samples should be received by the local/ forwardinglaboratory4 within 24 hours of the sample being taken.
S 9.7 Antibody screening should be undertaken using an indirect antiglobulin test and a redcell panel conforming to current UK guidelines (UK Blood Transfusion Services 2002).
S 9.8 The test should be undertaken by a laboratory that is either accredited by CPA (UK)Ltd.3 or has enrolled in the process of obtaining this standard.
S 9.9 The testing laboratory must provide the test result to the maternity service within 7 working days of the sample being received by the testing laboratory.
Developmental Minimum Standard to be achieved by September 2006;75% of antenatal screening test results should be provided to the maternity servicewithin 7 working days of the sample being received by the testing laboratory.
S 9.10 Women should be informed of the result by the maternity service within 15 workingdays of the sample being taken.
Developmental Minimum Standard to be achieved by September 2006;90% of women should be informed of the result by the maternity service within 20 working days of the sample being taken.
9.0 Antenatal screening for blood group and antibodies
9.1 Policy:
All women resident in Wales should be offered antenatal screening for blood groupand antibodies in pregnancy (NICE 2003).
9.2 Rationale:Rhesus negative women should be offered antenatal and postnatal anti-D Immunoglobulinprophylaxis (NICE 2002, NICE 2003).
The identification and monitoring of atypical red cell alloimmunisation can enable thepregnancy to be appropriately monitored.

21
S 9.11 If antibodies are detected they should be identified and if necessary quantified by thelaboratory to assess the likelihood of haemolytic disease of the newborn.
S 9.12 All RhD negative women should receive verbal and written information aboutantenatal and post natal anti-D Immunoglobulin prophylaxis and have the opportunityto discuss this treatment with a midwife in the antenatal period.
S 9.13 A record of the test result should be made in the maternity notes.
S 9.14 If the baby is Rhesus positive, non sensitised women who are RhD negative should beoffered postnatal anti-D Immunoglobulin within 72 hours of delivery (RCOG 2002).
S 9.15 A maternal sample is required post delivery (within 2 hours) from all RhD negativewomen (and from women where the maternal Rhesus group is for any reason notknown) accompanied by a cord blood sample. This is to assess feto-maternalhaemorrhage in Rh D negative women who have delivered a Rh D positive infant toestablish whether the woman requires additional anti-D Immunoglobulin .
22
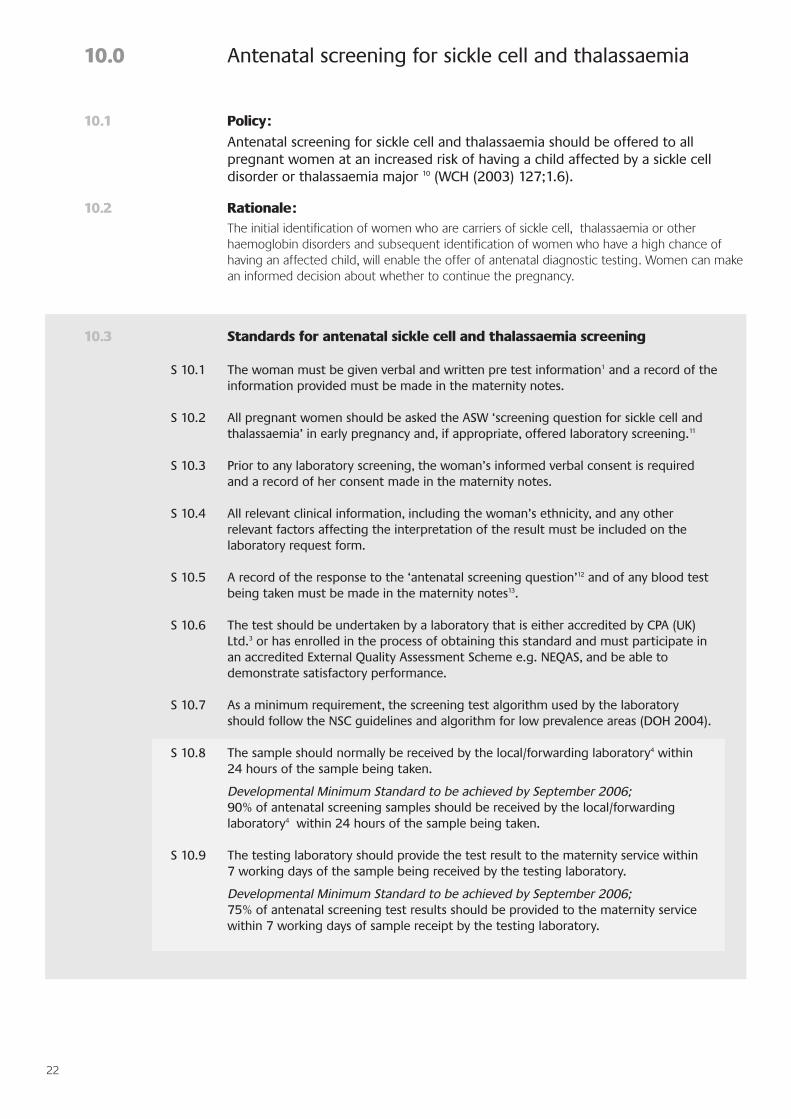
10.3 Standards for antenatal sickle cell and thalassaemia screening
S 10.1 The woman must be given verbal and written pre test information1 and a record of theinformation provided must be made in the maternity notes.
S 10.2 All pregnant women should be asked the ASW ‘screening question for sickle cell andthalassaemia’ in early pregnancy and, if appropriate, offered laboratory screening.11
S 10.3 Prior to any laboratory screening, the woman’s informed verbal consent is requiredand a record of her consent made in the maternity notes.
S 10.4 All relevant clinical information, including the woman’s ethnicity, and any otherrelevant factors affecting the interpretation of the result must be included on thelaboratory request form.
S 10.5 A record of the response to the ‘antenatal screening question’12 and of any blood testbeing taken must be made in the maternity notes13.
S 10.6 The test should be undertaken by a laboratory that is either accredited by CPA (UK)Ltd.3 or has enrolled in the process of obtaining this standard and must participate inan accredited External Quality Assessment Scheme e.g. NEQAS, and be able todemonstrate satisfactory performance.
S 10.7 As a minimum requirement, the screening test algorithm used by the laboratoryshould follow the NSC guidelines and algorithm for low prevalence areas (DOH 2004).
S 10.8 The sample should normally be received by the local/forwarding laboratory4 within 24 hours of the sample being taken.
Developmental Minimum Standard to be achieved by September 2006; 90% of antenatal screening samples should be received by the local/forwardinglaboratory4 within 24 hours of the sample being taken.
S 10.9 The testing laboratory should provide the test result to the maternity service within 7 working days of the sample being received by the testing laboratory.
Developmental Minimum Standard to be achieved by September 2006;75% of antenatal screening test results should be provided to the maternity servicewithin 7 working days of sample receipt by the testing laboratory.
10.0 Antenatal screening for sickle cell and thalassaemia
10.1 Policy:
Antenatal screening for sickle cell and thalassaemia should be offered to all pregnant women at an increased risk of having a child affected by a sickle cell disorder or thalassaemia major 10 (WCH (2003) 127;1.6).
10.2 Rationale:The initial identification of women who are carriers of sickle cell, thalassaemia or otherhaemoglobin disorders and subsequent identification of women who have a high chance ofhaving an affected child, will enable the offer of antenatal diagnostic testing. Women can makean informed decision about whether to continue the pregnancy.

23
S 10.10 Women should be informed of the result by the maternity service within 15 workingdays of the sample being taken.
Developmental Minimum Standard to be achieved by September 2006;90% of women should be informed of the result by the maternity service within 20working days of the sample being taken.
S 10.11 A record of the test result should be made in the maternity notes.
S 10.12 If the woman is a confirmed carrier of sickle cell or thalassaemia, or has a haemoglobindisorder, with the woman’s consent, the maternity services should offer the father ofthe fetus sickle cell and thalassaemia screening as soon as possible.
S 10.13 Neonatal screening for sickle cell should be offered if the baby has a high chance ofinheriting a sickle cell disorder.
Developmental Minimum Standard to be achieved by September 2006;All Trusts should have a policy regarding which babies are offered neonatal screeningfor sickle cell by September 2006.

24
11.3 Standards for antenatal Down’s syndrome screening
S 11.1 The woman must be given verbal and written pre test information1 and a record of theinformation provided made in the maternity notes.
S 11.2 The woman’s informed verbal consent is required for this test and a record of herconsent must be made in the maternity notes.
S 11.3 The detection rate and false positive rate of the Down’s syndrome screeningprogramme must be monitored and achieve a minimum standard of a 60% detectionrate for a 5% false positive rate (WCH (2003) 127; 6.1).
S 11.4 Down’s syndrome serum screening must be supported by measurements for gestationobtained from an early pregnancy ultrasound dating scan.
Serum screening for Down’s syndrome:
S 11.5 All the clinical and demographic information fields must be completed on thelaboratory request form. 14
S 11.6 The health professional requesting the test must complete and sign the request form.
(By signing the request form the requesting health professional is confirming thatwritten and/or verbal information about the purpose of the test has been given to thewoman and that informed consent has been given for the test).
S 11.7 A record of the sample being taken must be made in the maternity notes.
S 11.8 The sample should normally be received by the local/forwarding laboratory4 within 24hours of the sample being taken.
Developmental Minimum Standard to be achieved by September 2006; 90% of antenatal screening samples should be received by the local/forwardinglaboratory4 within 24 hours of the sample being taken.
11.0 Antenatal screening for Down’s syndrome
11.1 Policy:
Antenatal screening for Down’s syndrome should be offered to all pregnant women (NICE 2003).
11.2 Rationale:Identification of women who have a higher chance of having a baby with Down’s syndrome willenable the offer of antenatal diagnostic testing. If the fetus is affected by Down’s syndrome,the woman can make an informed decision about whether to continue with the pregnancy. Ifthe pregnancy is continuing appropriate identification of additional structural problems e.g.cardiac problems should be made and suitable care advised.
Down’s syndrome screening gives the woman more accurate information about the chance ofthe pregnancy being affected than by using her age alone. There are a number of screeningtests for Down’s syndrome and the limits of the gestation when the test can be offered willdepend on the screening test and the laboratory specification.
25
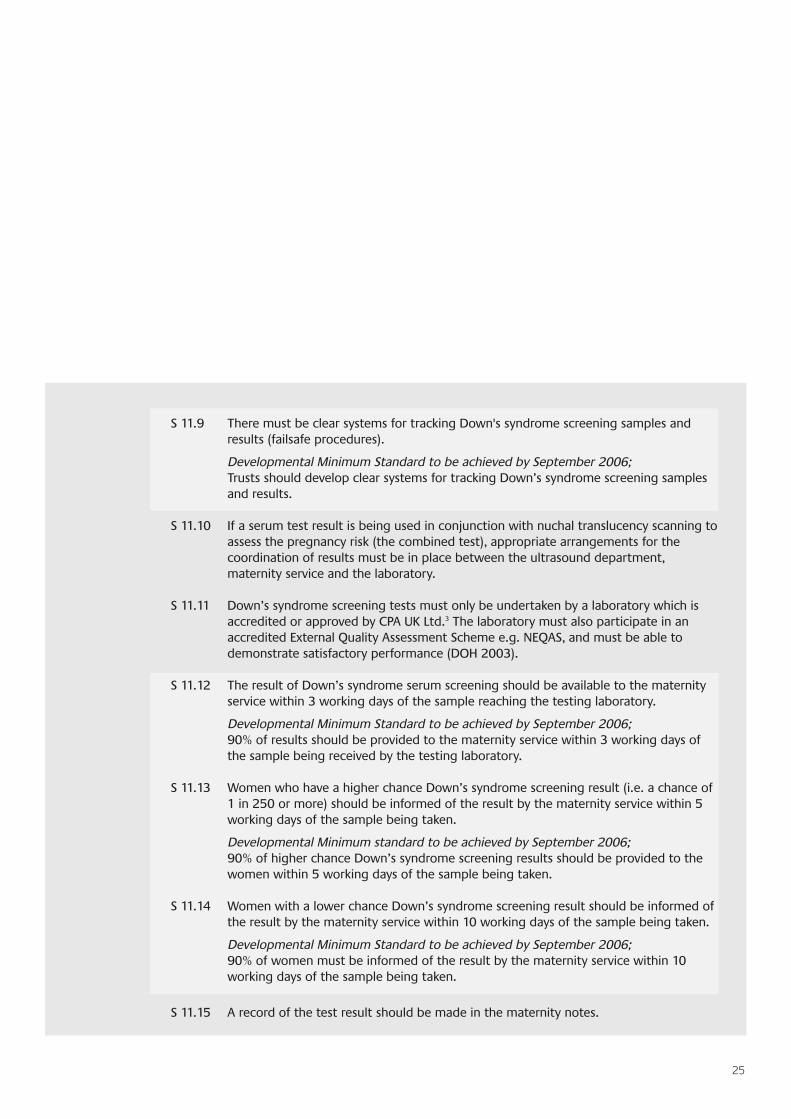
S 11.9 There must be clear systems for tracking Down's syndrome screening samples andresults (failsafe procedures).
Developmental Minimum Standard to be achieved by September 2006;Trusts should develop clear systems for tracking Down’s syndrome screening samplesand results.
S 11.10 If a serum test result is being used in conjunction with nuchal translucency scanning toassess the pregnancy risk (the combined test), appropriate arrangements for thecoordination of results must be in place between the ultrasound department,maternity service and the laboratory.
S 11.11 Down’s syndrome screening tests must only be undertaken by a laboratory which isaccredited or approved by CPA UK Ltd.3 The laboratory must also participate in anaccredited External Quality Assessment Scheme e.g. NEQAS, and must be able todemonstrate satisfactory performance (DOH 2003).
S 11.12 The result of Down’s syndrome serum screening should be available to the maternityservice within 3 working days of the sample reaching the testing laboratory.
Developmental Minimum Standard to be achieved by September 2006;90% of results should be provided to the maternity service within 3 working days ofthe sample being received by the testing laboratory.
S 11.13 Women who have a higher chance Down’s syndrome screening result (i.e. a chance of1 in 250 or more) should be informed of the result by the maternity service within 5working days of the sample being taken.
Developmental Minimum standard to be achieved by September 2006;90% of higher chance Down’s syndrome screening results should be provided to thewomen within 5 working days of the sample being taken.
S 11.14 Women with a lower chance Down’s syndrome screening result should be informed ofthe result by the maternity service within 10 working days of the sample being taken.
Developmental Minimum Standard to be achieved by September 2006;90% of women must be informed of the result by the maternity service within 10working days of the sample being taken.
S 11.15 A record of the test result should be made in the maternity notes.

26
12.0 References
Department of Health (2003) Antenatal Screening - working standards incorporating those forthe National Down's Syndrome Screening programme for England.http://www.nelh.nhs.uk/screening/http://www.nsc.nhs.uk
Department of Health (2004) Sickle cell and thalassaemia programme.http://www.kcl-phs.org.uk/haemscreening
National Assembly for Wales (2000) Antenatal screening to reduce mother to baby transmissionof HIV. Cardiff: National Assembly for Wales.
National Institute of Clinical Excellence (2002) Guidance on the use of routine antenatal anti-Dprophylaxis for Rh D negative women. London: NICE.
National Institute of Clinical Excellence (2003) Antenatal Care – routine care for the healthypregnant woman. London: NICE.
Royal College of Obstetricians and Gynaecologists. (2000) Routine ultrasound screening inpregnancy, protocols, standards and training. Supplement to ultrasound screening for fetalabnormalities. Report of the RCOG working party. London: RCOG Press.
Royal College of Obstetrics and Gynaecology (2002) Use of Anti-D Immunoglobulin for RhProphylaxis. Green top guidelines.
WHC (2003) 127 Annual Priorities and Planning Guidance for Services and Financial PlanningFramework (2004).
UK Blood Transfusion Services (2002) Guidelines for the Blood Transfusion Service. 6th ed.London; TSO; [www.transfusionguidelines.org.uk/uk_guidelines/ukbts6_$01.html] Accessed 20August 2003.
Welsh Office (1998) Screening of pregnant women for hepatitis B and immunisation of babiesat risk. WHC (98)36.
27
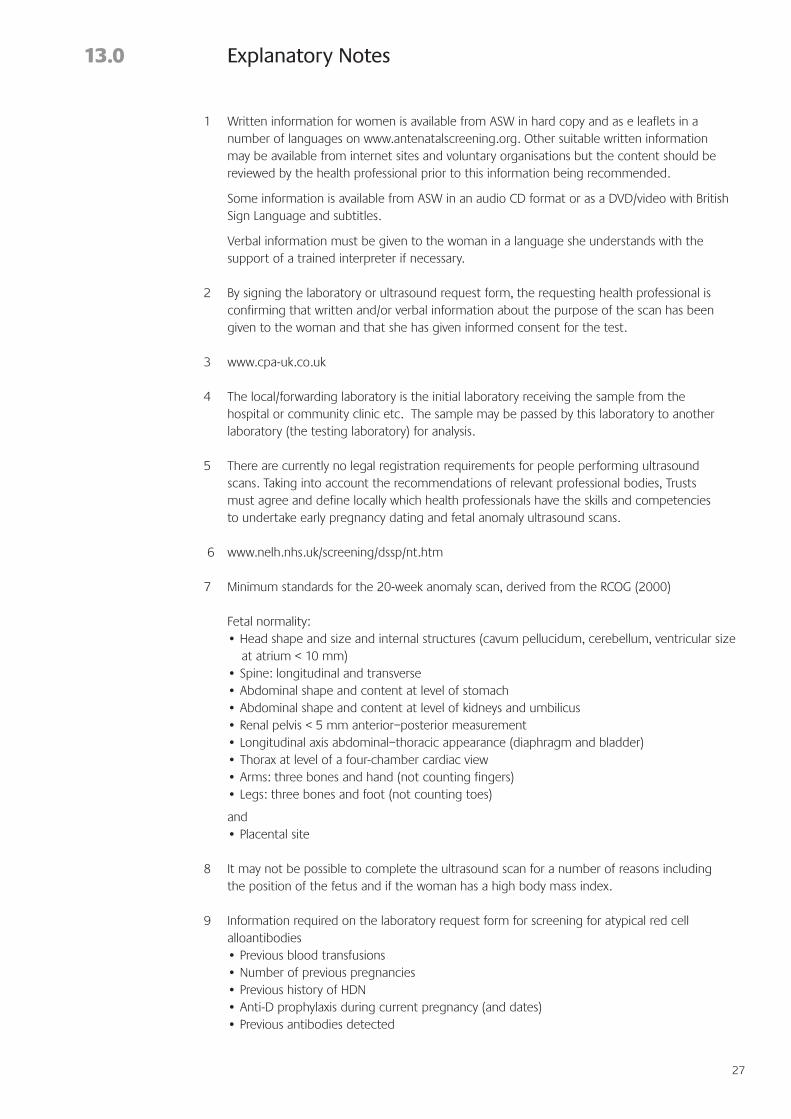
13.0 Explanatory Notes
1 Written information for women is available from ASW in hard copy and as e leaflets in anumber of languages on www.antenatalscreening.org. Other suitable written informationmay be available from internet sites and voluntary organisations but the content should bereviewed by the health professional prior to this information being recommended.
Some information is available from ASW in an audio CD format or as a DVD/video with BritishSign Language and subtitles.
Verbal information must be given to the woman in a language she understands with thesupport of a trained interpreter if necessary.
2 By signing the laboratory or ultrasound request form, the requesting health professional isconfirming that written and/or verbal information about the purpose of the scan has beengiven to the woman and that she has given informed consent for the test.
3 www.cpa-uk.co.uk
4 The local/forwarding laboratory is the initial laboratory receiving the sample from thehospital or community clinic etc. The sample may be passed by this laboratory to anotherlaboratory (the testing laboratory) for analysis.
5 There are currently no legal registration requirements for people performing ultrasoundscans. Taking into account the recommendations of relevant professional bodies, Trustsmust agree and define locally which health professionals have the skills and competenciesto undertake early pregnancy dating and fetal anomaly ultrasound scans.
6 www.nelh.nhs.uk/screening/dssp/nt.htm
7 Minimum standards for the 20-week anomaly scan, derived from the RCOG (2000)
Fetal normality:• Head shape and size and internal structures (cavum pellucidum, cerebellum, ventricular size
at atrium < 10 mm)• Spine: longitudinal and transverse• Abdominal shape and content at level of stomach• Abdominal shape and content at level of kidneys and umbilicus• Renal pelvis < 5 mm anterior–posterior measurement• Longitudinal axis abdominal–thoracic appearance (diaphragm and bladder)• Thorax at level of a four-chamber cardiac view• Arms: three bones and hand (not counting fingers)• Legs: three bones and foot (not counting toes)
and• Placental site
8 It may not be possible to complete the ultrasound scan for a number of reasons includingthe position of the fetus and if the woman has a high body mass index.
9 Information required on the laboratory request form for screening for atypical red cellalloantibodies• Previous blood transfusions• Number of previous pregnancies • Previous history of HDN• Anti-D prophylaxis during current pregnancy (and dates)• Previous antibodies detected

28
• Date of sample (some antibodies deteriorate on storage. Samples greater than 7 days old cannot be tested).
10 For the purpose of antenatal screening, these women are defined as:• women, or women with partners who have a family history of sickle cell or thalassaemia• women who have unexplained anaemia• women or women with partners who’s family, no matter how many generations back, came
from anywhere in the world apart from the United Kingdom and the Republic of Ireland• women who do not know their family history – for example, they were adopted.
11 The purpose of this question is to identify pregnant women with an increased chance ofhaving a child affected by a sickle cell disorder or thalassaemia major. Women identified asbeing at higher chance should be offered laboratory screening (WHC (2003)127;1.6).
12 ASW screening question for sickle cell and thalassaemia
You should think about having the test if:• you or your partner have a family history of sickle cell or thalassaemia;• you have unexplained anaemia;• you, your partner, anyone in your family, or anyone in your partner's family, no matter
how many generations back, came from anywhere in the world apart from the United Kingdom and the Republic of Ireland; or
• you do not know your family history – for example, you were adopted.
13 If the woman declines to answer the screening question for sickle cell and thalassaemia,‘declined to answer screening question’ should be recorded in the maternity notes.
14 Specific guidance for health professionals on completing the request form is available fromASW.