Embed Size (px)
Citation preview
POLICY STATEMENT
Levels of Neonatal Care
abstractProvision of risk-appropriate care for newborn infants and motherswas first proposed in 1976. This updated policy statement providesa review of data supporting evidence for a tiered provision of careand reaffirms the need for uniform, nationally applicable definitionsand consistent standards of service for public health to improve neo-natal outcomes. Facilities that provide hospital care for newborninfants should be classified on the basis of functional capabilities,and these facilities should be organized within a regionalized systemof perinatal care. Pediatrics 2012;130:587–597
OBJECTIVE
This revised policy statement reviews the current status of the des-ignation of levels of newborn care definitions in the United States,which were delineated in a 2004 policy statement by the AmericanAcademy of Pediatrics (AAP).1 Since publication of the 2004 policystatement, new data, both nationally and internationally, have rein-forced the importance of well-defined regionalized systems of perinatalcare, population-based assessment of outcomes, and appropriate epi-demiologic methods to adjust for risk. This revised statement updatesthe designations to provide (1) a basis for comparison of health out-comes, resource use, and health care costs, (2) standardized nomen-clature for public health, (3) uniform definitions for pediatricians andother health care professionals providing neonatal care, and (4)a foundation for consistent standards of service by institutions; statehealth departments; and state, regional, and national organizationsfocused on the improvement of perinatal care.
BACKGROUND
The availability of neonatal intensive care has improved the outcomesof high-risk infants born either preterm or with serious medical orsurgical conditions.2–4 Many of these improvements can be attributedto the concept and implementation of regionalized systems of peri-natal care, broadly articulated in the 1976 March of Dimes report“Toward Improving the Outcome of Pregnancy” (TIOP I).5 The TIOP Ireport included criteria that stratified maternal and neonatal careinto 3 levels of complexity and recommended referral of high-riskpatients to higher-level centers with the appropriate resources andpersonnel to address the required increased complexity of care.However, since the initial TIOP I report was published more than 3decades ago, there have been signs of deregionalization, including (1)
COMMITTEE ON FETUS AND NEWBORN
KEY WORDSneonatal intensive care, high-risk infant, regionalization,maternal and child health, health policy, very low birth weightinfant, hospital newborn care services, nurseries
ABBREVIATIONSAAP—American Academy of PediatricsaOR—adjusted odds ratioCI—confidence intervalCON—certificate of needELBW—extremely low birth weightTIOP—“Toward Improving the Outcome of Pregnancy”VLBW—very low birth weight
This document is copyrighted and is property of the AmericanAcademy of Pediatrics and its Board of Directors. All authorshave filed conflict of interest statements with the AmericanAcademy of Pediatrics. Any conflicts have been resolved througha process approved by the Board of Directors. The AmericanAcademy of Pediatrics has neither solicited nor accepted anycommercial involvement in the development of the content ofthis publication.
Authors with federal affiliations do not necessarily represent theofficial position of their agencies.
All policy statements from the American Academy of Pediatricsautomatically expire 5 years after publication unless reaffirmed,revised, or retired at or before that time.
www.pediatrics.org/cgi/doi/10.1542/peds.2012-1999
doi:10.1542/peds.2012-1999
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2012 by the American Academy of Pediatrics
PEDIATRICS Volume 130, Number 3, September 2012 587
FROM THE AMERICAN ACADEMY OF PEDIATRICS
Organizational Principles to Guide and Define the ChildHealth Care System and/or Improve the Health of all Children
by guest on May 26, 2018http://pediatrics.aappublications.org/Downloaded from

an increase in the number of NICUsand neonatologists, without a consis-tent relationship to the percentage ofhigh-risk infants, (2) a proliferation ofsmall NICUs in the same regions aslarge NICUs,6–11 and (3) failure ofstates to reach the Healthy People2010 goal that 90% of deliveries ofvery low birth weight (VLBW; <1500 g)infants occur at level III facilities.12,13
In the environment of deregionaliza-tion, preterm birth rates have in-creased 13% overall from 1990 to 2010(10.6%–12.0%) as a result of a varietyof factors, including increases in elec-tive early cesarean deliveries, multiplebirths, advanced maternal age, andcomplications of pregnancy.14–20 Themajority of the increase in the pretermbirth rate (>70%) is attributable tolate preterm births.21 Infants born latepreterm can experience significantmorbidity that may result in the needfor specialized care and advancedneonatal services.22,23 An increase inthe supply of specialty staff24,25 andavailability of new neonatal therapies(eg, bubble continuous positive airwaypressure), have expanded the scope ofcare in level II facilities.26 Some haveexpressed concern that level II hospi-tals have expanded their scope of carewithout sufficient evidence of favorableoutcome. Because most infant deathsin the United States occur among themost immature infants in the first fewdays after birth,27,28 improvements inregionalized systems may reduce mor-tality among the most preterm new-born infants.
REVIEW OF THE LITERATURE ONNEONATAL LEVELS OF CARE SINCETHE 2004 AAP POLICY STATEMENT
In 2004, the AAP defined neonatal levelsof care, including 3 distinct levels withsubdivisions in 2 of the levels.1 Level Icenters provided basic care; level IIcenters provided specialty care, withfurther subdivisions of IIA and IIB
centers; and level III centers providedsubspecialty care for critically ill new-born infants with subdivisions of levelIIIA, IIIB, and IIIC facilities. Data pub-lished since the 2004 statement haveinformed the development of the levelsof care in this new policy statement.
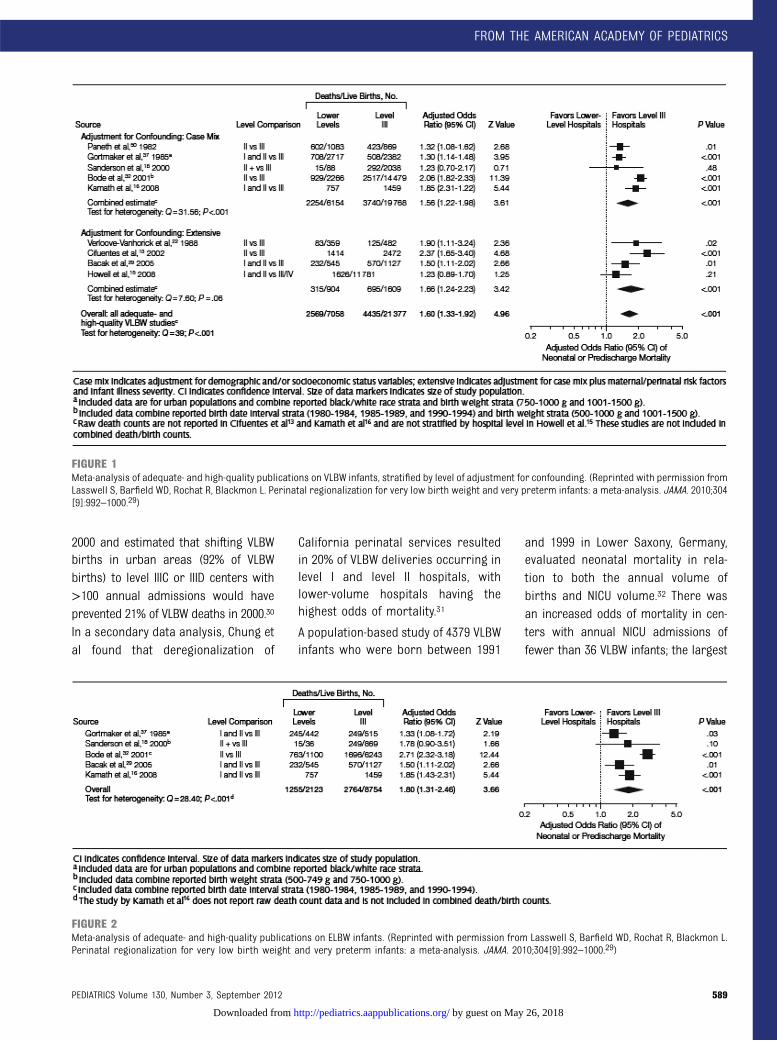
A meta-analysis of the published liter-ature from 1978 to 2010 clearly dem-onstrates improved outcomes for VLBWinfants and infants <32 weeks’ gesta-tional age born in level III centers.Lasswell et al reviewed 41 English-language US and international stud-ies, which included >113 000 VLBWinfants and found that VLBW infantsborn at non–level III hospitals had a62% increase in odds of neonatal orpredischarge mortality compared withthose born at level III hospitals (ad-justed odds ratio [aOR], 1.62; 95%confidence interval [CI], 1.44–1.83).Subset comparisons of studies identi-fying infants <32 weeks’ gestation andextremely low birth weight (ELBW)infants (<1000 g) demonstrated simi-lar effects (aOR, 1.55; 95% CI, 1.21–1.98;aOR, 1.64; 95% CI, 1.14–2.36, respec-tively). When only higher-quality stud-ies were included, the findings wereconsistent (VLBW aOR, 1.60; 95% CI,1.33–1.92; <32 weeks’ gestation aOR,1.42; 95% CI, 1.06–1.88; ELBW aOR, 1.80;95% CI, 1.31–2.36). The effect of level ofcare on VLBW mortality did not vary bydecade of publication29; hence, the riskof death for VLBW infants born in level Ior II facilities remained higher thanthose born within a level III facility.Figures 1, 2, and 3 summarize thefindings of these studies.
As Lasswell and colleagues found, partof the difficulty in collecting evidenceto provide accurate assessments ofVLBW outcomes has been in obtain-ing appropriate standardized mea-sures. Heterogeneity among studies onneonatal levels of care suggests theneed for a quality standard for com-parison which includes the following
elements: (1) population-based studieswithin well-defined geographic regions,(2) clear definitions of the “intervention”or hospital level of care, and (3) ap-propriate adjustment for confoundingfactors to include maternal social anddemographic risk factors, pregnancyand perinatal risks, and severity of ill-ness at delivery.
Current Controversies in Levels ofCare Designation
Although little debate exists on theneed for advanced neonatal servicesfor the most immature and surgicallycomplex neonates, ongoing contro-versies exist regarding which facili-ties are qualified to provide theseservices and what is the most ap-propriate measure for such qualifi-cation. These issues are, in general,based on the need for comparison offacility experience (measured by pa-tient volume or census), location(inborn/outborn deliveries, regionalperinatal center, or children’s hospi-tal), or case mix (including stillbirths,delivery room deaths, and complexcongenital anomalies).
Several studies have explored the topicof center experience as measured byvolume or census of VLBW infants.30–35
Phibbs et al conducted a population-based retrospective cohort study of48 237 California VLBW infants to ex-amine differences in neonatal mortalityamong NICUs with various levels ofcare and patient volumes. When com-pared with high-volume, high-levelcenters, the odds ratio of death was1.19 (range, 1.04–1.37) for level IIIB, IIIC,or IIID centers with <100 annualadmissions, 1.78 (range, 1.35–2.34) forlevel IIIA centers with 26 to 50 annualadmissions, and 2.72 (range, 2.37–3.12)for level I centers with <10 annualadmissions. The authors also foundthat the percentage of VLBW infantsdelivered in level IIIB, IIIC, or IIID centersdecreased from 36% in 1991 to 22% in
588 FROM THE AMERICAN ACADEMY OF PEDIATRICS
by guest on May 26, 2018http://pediatrics.aappublications.org/Downloaded from
2000 and estimated that shifting VLBWbirths in urban areas (92% of VLBWbirths) to level IIIC or IIID centers with>100 annual admissions would haveprevented 21% of VLBW deaths in 2000.30
In a secondary data analysis, Chung etal found that deregionalization of
California perinatal services resultedin 20% of VLBW deliveries occurring inlevel I and level II hospitals, withlower-volume hospitals having thehighest odds of mortality.31
A population-based study of 4379 VLBWinfants who were born between 1991
and 1999 in Lower Saxony, Germany,evaluated neonatal mortality in rela-tion to both the annual volume ofbirths and NICU volume.32 There wasan increased odds of mortality in cen-ters with annual NICU admissions offewer than 36 VLBW infants; the largest
FIGURE 1Meta-analysis of adequate- and high-quality publications on VLBW infants, stratified by level of adjustment for confounding. (Reprinted with permission fromLasswell S, Barfield WD, Rochat R, Blackmon L. Perinatal regionalization for very low birth weight and very preterm infants: a meta-analysis. JAMA. 2010;304[9]:992–1000.29)
FIGURE 2Meta-analysis of adequate- and high-quality publications on ELBW infants. (Reprinted with permission from Lasswell S, Barfield WD, Rochat R, Blackmon L.Perinatal regionalization for very low birth weight and very preterm infants: a meta-analysis. JAMA. 2010;304[9]:992–1000.29)
PEDIATRICS Volume 130, Number 3, September 2012 589
FROM THE AMERICAN ACADEMY OF PEDIATRICS
by guest on May 26, 2018http://pediatrics.aappublications.org/Downloaded from

effect on mortality was for infants bornat less than 29 weeks’ gestation.
Other studies assessing NICU volumesuggest caution in using this mea-sure as an effective indicator of qualityof care. Rogowski and colleaguesassessed the potential usefulness ofNICU volume as a quality indicatoramong 94 110 VLBW infants enteredinto the Vermont Oxford Network da-tabase between 1995 and 2000 andcompared NICU volume with otherindicators based on hospital charac-teristics and patient outcomes.33 Theyfound that although annual volumeexplained 9% of the variation in hos-pital mortality rates, other hospitalcharacteristics explained another 7%.They suggested that direct measuresbased on patient outcomes are moreuseful quality indicators than volumefor the purpose of selective referral.
Several studies assessed the effects oflevel of care, patient volume, and racialdisparities on mortality of VLBW in-fants based on births in minority-serving hospitals. Morales34 and Howell35
evaluated mortality of VLBW infantsborn in minority-serving hospitals. Inboth studies, neonatal level of careand patient volume were each inde-pendently associated with mortality,suggesting that delivery of all VLBWinfants at high-volume hospitals would
reduce black-white disparities in VLBWmortality rates. Rogowski and col-leagues further suggest that thequality of care in poor-outcome hos-pitals could be improved through col-laborative quality improvement, andevidence-based selective referral.36
Several studies have compared theshort-term outcome of VLBW infantsborn in centers with level III units (in-born) compared with those born atlower level centers and soon transferredto a higher level (level III or children’shospital; outborn). Many of these stud-ies are retrospective and may be sub-ject to selection bias because infantswho were transferred most likelyhad the highest chance of survivaland thus gave the impression of lowermortality.24 In a secondary analysis ofa randomized placebo-controlled studyof preemptive morphine analgesia onneonatal outcomes, Palmer et al com-pared neonatal mortality as related toplace of birth for 894 infants whowere born at 23 to 32 weeks’ gesta-tion. Outborn babies were more likelyto have severe intraventricular hem-orrhage (P = .0005), and this increasedrisk persisted after controlling for se-verity of illness. However, when ad-justed for antenatal steroids, the effectof birth center was no longer signifi-cant.37
Evaluating and controlling for con-founding variables and “case-mix”presents another set of challenges be-cause these factors vary by popula-tion. For example, race and insurancestatus may have more of an effecton birth outcomes in the UnitedStates34–36,38 than in countries witha more homogenous population anduniversal national health care.39 Thereare also potential confounding factorsfor which measurement is frequentlylacking, such as parental wishes re-garding aggressive resuscitation of aninfant. Arad et al noted that parentalwishes varied by religious affilia-tion in their 2-hospital study. Becausereligious affiliation was unequallydistributed between the 2 hospitals,fewer attempts at resuscitation mayhave been made at the level III hos-pital, with a result of improved sur-vival at the level II facility.40 Morecomprehensive studies controlling forconfounding factors are needed.
Measured outcomes other than VLBWmortality (notably, fetal mortality,postdischarge mortality, and long-termphysical and neurodevelopmental out-comes) may offer important infor-mation in assessing the evidence fornewborn levels of care and perinatalregionalization. Studies measuring theeffect of hospital level of birth on fetal
FIGURE 3Meta-analysis of adequate- and high-quality publications on very preterm infants (<32 weeks’ gestation). (Reprinted with permission from Lasswell S,Barfield WD, Rochat R, Blackmon L. Perinatal regionalization for very low birth weight and very preterm infants: a meta-analysis. JAMA. 2010;304[9]:992–1000.29)
590 FROM THE AMERICAN ACADEMY OF PEDIATRICS
by guest on May 26, 2018http://pediatrics.aappublications.org/Downloaded from

and neonatal outcomes stratified bygestational age, as well as by birthweight, are also helpful, because ges-tational age is a better gauge of fe-tal maturity.41–44 Although some studiesinclude stillbirths and intrapartum fetaldeaths, measurement and surveillanceof fetal death varies widely.3 Congenitalanomalies are often excluded fromstudies of perinatal regionalization butshould be considered in the provisionof risk appropriate care.45
Additional studies are also needed toassess the effectiveness and potentialcost savings of centralizing expensivetechnologies and provider expertise forrelatively rare conditions at a few loca-tions and to assess the effectiveness,including costs, of antenatal transport.
IMPORTANCE OF NEONATAL LEVELSOF CARE
Provision of StandardizedNomenclature for Public Health
Since 2004, efforts have been made toimprove the comparison of health out-comes by hospital facility through theuse of standardized nomenclature onthe US birth certificate. The NationalCenter for Health Statistics at the Cen-ters for Disease Control and Preventionhas worked with states to use the newlyrevised US Standard Certificate ofBirth.46 This 2003 revised certificatedefines a NICU as a “hospital facility orunit staffed and equipped to providecontinuous mechanical ventilatory sup-port for a newborn infant.” It alsoincludes information on the use of an-tenatal therapies and postpartum sur-factant, which may be useful inmonitoring population-based utilizationof technologies at birth.47 In an analysisof 16 states using the revised certificateof birth, Barfield et al found that overall,77.3% of VLBW infants were admitted toNICUs; this estimate varied by state andranged from 63.7% in California to93.4% in North Dakota. Among VLBWinfants of Hispanic mothers, 71.8% were
admitted to NICUs, compared with79.5% of VLBW infants of non-Hispanicblack mothers and 80.5% of VLBWinfants of non-Hispanic white mothers.In multivariable analysis, preterm de-livery, multiple gestation, and cesareandelivery were associated with higherprevalence of NICU admission amongVLBW infants.13 State variations in thereceipt of intensive care for VLBWinfants may explain, in part, variation inVLBW outcomes across the country.
Use of Uniform Definitions of Levelsof Care for Pediatricians and OtherHealth Care Professionals
Variation in definition, criteria, andstate enforcement still occurs despitethe TIOP I guidelines. Blackmon et alconducted an extensive review of all50 states and the District of Columbiagovernmental Web sites to assess statedefinitions and levels terminology, func-tional and utilization criteria, regulatorycompliance and funding measures, andcitation of AAP documents on levelsof neonatal care. The authors foundthat state definitions, criteria, compli-ance, and regulatory mechanisms forthe specific type of care neonatal cen-ters provide varied considerably, andthey suggested a consistent nationalapproach.48 Lorch et al assessed all 50states and the District of Columbia toidentify state certificate of need (CON)legislation, a mechanism that regulatesthe expansion of NICU facilities andNICU beds. Thirty states regulatedthe construction of NICUs through CONprograms, and non-CON program stateswere associated with more NICU facili-ties and more NICU beds (relative risk,2.06; 95% CI, 1.74–2.45; and relative risk,1.96; 95% CI, 1.89–2.03, respectively).In large metropolitan areas, non-CONstates had higher infant mortality forall birth weight groups.49
The Maternal and Child Health Bureau ofthe Health Resources and Services Ad-ministration has worked with state Title
V agencies to document the percentageof VLBW infants delivered in level IIIhospitals or subspecialty perinatalclinics. In 2009, only 5 states met thegoal of at least 90% of VLBW infantsdelivered at high-risk facilities.12 Yet,the interpretation and reporting ofthese facilities may be inconsistent assome states had unclear facility defi-nitions or included level II facilities intheir reporting. Recently, several states,in partnership with national organiza-tions, have taken more definitive actionin defining and regulating organizationof perinatal care.50
Development of ConsistentStandards of Service
Efforts by quality-improvement collabo-ratives, health services researchers, andpublic health officials will continue toimprove the standards by which tomeasure quality of care.51,52 Quality-improvement activities have begun toflourish at all levels to improve maternaland perinatal health and ideally preventpreterm births; this includes provider-level quality-improvement activities,hospital-level performance measures,and regional, state, and national per-formance measures.53 Organizationssuch as the March of Dimes have pro-moted standard definitions of levels ofcare since the introduction of perinatalregionalization in the 1970s, reaffirmedits importance in 1993 (TIOP II),54 andincluded the concept of quality care forthe prevention of preterm birth witha new TIOP (TIOP III) in 2010.53
DEFINITIONS OF LEVELS OFNEONATAL CARE
The updated classification consists ofbasic care (level I), specialty care (levelII), and subspecialty intensive care (levelIII, level IV; Table 1). These definitionsreflect the overall evidence for risk-appropriate care through the availabil-ity of appropriate personnel, physicalspace, equipment, technology, and
PEDIATRICS Volume 130, Number 3, September 2012 591
FROM THE AMERICAN ACADEMY OF PEDIATRICS
by guest on May 26, 2018http://pediatrics.aappublications.org/Downloaded from
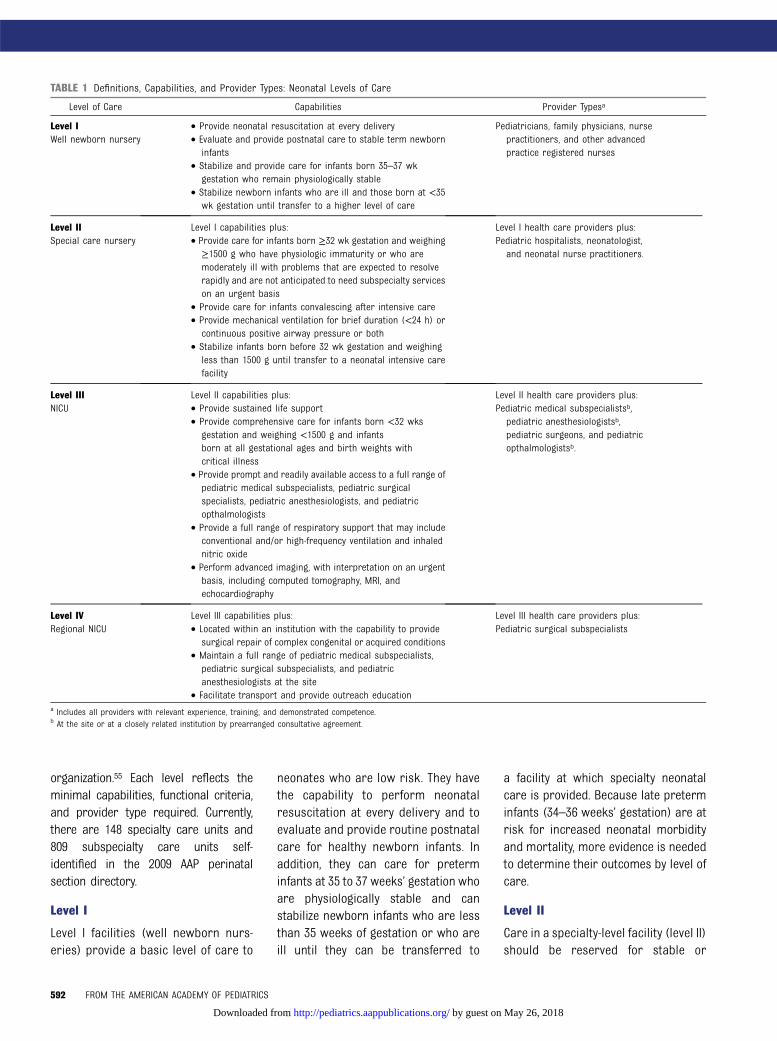
organization.55 Each level reflects theminimal capabilities, functional criteria,and provider type required. Currently,there are 148 specialty care units and809 subspecialty care units self-identified in the 2009 AAP perinatalsection directory.
Level I
Level I facilities (well newborn nurs-eries) provide a basic level of care to
neonates who are low risk. They havethe capability to perform neonatalresuscitation at every delivery and toevaluate and provide routine postnatalcare for healthy newborn infants. Inaddition, they can care for preterminfants at 35 to 37 weeks’ gestation whoare physiologically stable and canstabilize newborn infants who are lessthan 35 weeks of gestation or who areill until they can be transferred to
a facility at which specialty neonatalcare is provided. Because late preterminfants (34–36 weeks’ gestation) are atrisk for increased neonatal morbidityand mortality, more evidence is neededto determine their outcomes by level ofcare.
Level II
Care in a specialty-level facility (level II)should be reserved for stable or
TABLE 1 Definitions, Capabilities, and Provider Types: Neonatal Levels of Care
Level of Care Capabilities Provider Typesa
Level I • Provide neonatal resuscitation at every delivery Pediatricians, family physicians, nursepractitioners, and other advancedpractice registered nurses
Well newborn nursery • Evaluate and provide postnatal care to stable term newborninfants
• Stabilize and provide care for infants born 35–37 wkgestation who remain physiologically stable
• Stabilize newborn infants who are ill and those born at <35wk gestation until transfer to a higher level of care
Level II Level I capabilities plus: Level I health care providers plus:Special care nursery • Provide care for infants born ≥32 wk gestation and weighing
≥1500 g who have physiologic immaturity or who aremoderately ill with problems that are expected to resolverapidly and are not anticipated to need subspecialty serviceson an urgent basis
Pediatric hospitalists, neonatologist,and neonatal nurse practitioners.
• Provide care for infants convalescing after intensive care• Provide mechanical ventilation for brief duration (<24 h) or
continuous positive airway pressure or both• Stabilize infants born before 32 wk gestation and weighing
less than 1500 g until transfer to a neonatal intensive carefacility
Level III Level II capabilities plus: Level II health care providers plus:NICU • Provide sustained life support Pediatric medical subspecialistsb,
pediatric anesthesiologistsb,pediatric surgeons, and pediatricopthalmologistsb.
• Provide comprehensive care for infants born <32 wksgestation and weighing <1500 g and infantsborn at all gestational ages and birth weights withcritical illness
• Provide prompt and readily available access to a full range ofpediatric medical subspecialists, pediatric surgicalspecialists, pediatric anesthesiologists, and pediatricopthalmologists
• Provide a full range of respiratory support that may includeconventional and/or high-frequency ventilation and inhalednitric oxide
• Perform advanced imaging, with interpretation on an urgentbasis, including computed tomography, MRI, andechocardiography
Level IV Level III capabilities plus: Level III health care providers plus:Regional NICU • Located within an institution with the capability to provide
surgical repair of complex congenital or acquired conditionsPediatric surgical subspecialists
• Maintain a full range of pediatric medical subspecialists,pediatric surgical subspecialists, and pediatricanesthesiologists at the site
• Facilitate transport and provide outreach educationa Includes all providers with relevant experience, training, and demonstrated competence.b At the site or at a closely related institution by prearranged consultative agreement.
592 FROM THE AMERICAN ACADEMY OF PEDIATRICS
by guest on May 26, 2018http://pediatrics.aappublications.org/Downloaded from

moderately ill newborn infants whoare born at ≥32 weeks’ gestation orwho weigh ≥1500 g at birth withproblems that are expected to re-solve rapidly and who would not beanticipated to need subspecialty-levelservices on an urgent basis. Thesesituations usually occur as a result ofrelatively uncomplicated preterm laboror preterm rupture of membranes.There is limited evidence to supportthe specific subdivision of level II care,in part because of the lack of studieswith well-defined subdivisions. Level IIfacilities should take into consider-ation geographic constraints andpopulation size when assessing thestaffing resources needed to careappropriately for moderately ill new-born infants.
Level II nurseries may provide assistedventilation on an interim basis until theinfant’s condition either soon improvesor the infant can be transferred toa higher-level facility. Delivery of con-tinuous positive airway pressureshould be readily available by experi-enced personnel, and mechanicalventilation can be provided for a briefduration (less than 24 hours). Level IInurseries must have equipment (eg,portable x-ray machine, blood gasanalyzer) and personnel (eg, physi-cians, specialized nurses, respiratorytherapists, radiology technicians, lab-oratory technicians) continuouslyavailable to provide ongoing care aswell as to address emergencies. Re-ferral to a higher level of care shouldoccur for all infants when needed forpediatric surgical or medical sub-specialty intervention.
Level III
Evidence suggests that infants who areborn at <32 weeks’ gestation, weigh<1500 g at birth, or have medical orsurgical conditions, regardless of ges-tational age, should be cared for ata level III facility. Designation of level III
care should be based on clinical ex-perience, as demonstrated by largepatient volume, increasing complexityof care, and availability of pediatricmedical subspecialists and pediatricsurgical specialists. Subspecialty careservices should include expertise inneonatology and also ideally maternal-fetal medicine, if mothers are referredfor the management of potential pre-term birth. Level III NICUs are definedby having continuously availablepersonnel (neonatologists, neonatalnurses, respiratory therapists) andequipment to provide life supportfor as long as necessary. Facilitiesshould have advanced respiratorysupport and physiologic monitoringequipment, laboratory and imagingfacilities, nutrition and pharmacysupport with pediatric expertise,social services, and pastoral care.
Level III facilities should be able toprovide ongoing assisted ventilationfor 24 hours or more, which may in-clude conventional ventilation, high-frequency ventilation, and inhalednitric oxide. Level III facility capabilitiesshould also be based on a region’s con-sideration of geographic constraints,population size, and personnel re-sources. If geographic constraints forland transportation exist, the level IIIfacility should ensure availability of ro-tor and fixed-wing transport servicesto quickly and safely transfer infantsrequiring subspecialty intervention.56
Potential transfer to higher-level facili-ties or children’s hospitals, as well asback-transport of recovering infantsto lower-level facilities, should be con-sidered as clinically indicated.
A broad range of pediatric medicalsubspecialists and pediatric surgicalspecialists should be readily accessibleon site or by prearranged consultativeagreements. Prearranged consultativeagreements can be performed byusing telemedicine technology and/ortelephone consultation, for example,
from a distant location.50 Pediatricophthalmology services and an orga-nized program for the monitoring,treatment, and follow-up of retinopathyof prematurity should be readilyavailable in level III facilities.57 Level IIIunits should have the capability toperform major surgery on site or at aclosely related institution, ideally inclose geographic proximity. Becausethe outcomes of less complex surgi-cal procedures in children, suchas appendectomy or pyloromyotomy,are better when performed bypediatric surgeons compared withgeneral surgeons, it is recommendedthat pediatric surgical specialists (in-cluding anesthesiologists with pedi-atric expertise) perform all proceduresin newborn infants.58
Level III facilities should have the ca-pability to perform advanced imagingwith interpretation on an urgent basis,including CT, MRI, and echocardiogra-phy. Level III facilities should collect datato assess outcomes within their facilityand to compare with other levels.
Level IV
Level IV units include the capabilities oflevel III with additional capabilities andconsiderable experience in the care ofthe most complex and critically illnewborn infants and should have pe-diatric medical and pediatric surgi-cal specialty consultants continuouslyavailable 24 hours a day. Level IV fa-cilities would also include the capa-bility for surgical repair of complexconditions (eg, congenital cardiacmalformations that require cardiopul-monary bypass with or without ex-tracorporeal membrane oxygenation).More evidence is needed to assess therisk of morbidity and mortality by levelof care for newborn infants with com-plex congenital cardiac malformations.A recent study by Burstein et al59 wasnot able to note a difference in post-operative morbidity or mortality
PEDIATRICS Volume 130, Number 3, September 2012 593
FROM THE AMERICAN ACADEMY OF PEDIATRICS
by guest on May 26, 2018http://pediatrics.aappublications.org/Downloaded from

associated with dedicated pediatriccardiac ICUs versus NICUs and PICUsbut did not separately assess thenewborn and postneonatal periods.Although specific supporting dataare not currently available, it isthought that concentrating the careof such infants at designated level IVcenters will allow these centers todevelop the expertise needed toachieve optimal outcomes.
Not all level IV hospitals need to act asregional centers; however, regionalorganization of perinatal health careservices requires that there be co-ordination in the development ofspecialized services, professionalcontinuing education to maintaincompetency, facilitation of opportu-nities for transport and back-trans-port,60 and collection of data on long-term outcomes to evaluate both theeffectiveness of delivery of perinatalhealth care services and the safetyand efficacy of new therapies. Thesefunctions usually are best achievedwhen responsibility is concentratedin a single regional center with bothperinatal and neonatal subspecialtyservices. In some cases, regionalcoordination may be provided ade-quately by the collaboration of achildren’s hospital with a sub-specialty perinatal facility that is inclose geographic proximity.61
STANDARDS OF SERVICE FORHOSPITALS PROVIDING NEONATALCARE
Current evidence indicates that familyand cultural considerations are im-portant for care of sick neonates.62–65
These considerations include family-and patient-centered care, culturallyeffective care, family-based educa-tion, and opportunities for back-transport to level II facilities ortransfer to the family’s local com-munity facility when medically andsocially indicated.64–67
SUMMARY ANDRECOMMENDATIONS
1. Regionalized systems of perinatalcare are recommended to ensurethat each newborn infant is deliveredand cared for in a facility mostappropriate for his or her healthcare needs, when possible, and tofacilitate the achievement of opti-mal health outcomes.
� Because VLBW and/or very pre-term infants are at increasedrisk of predischarge mortalitywhen born outside of a level IIIcenter, they should be deliv-ered at a level III facility unlessthis is precluded by the moth-er’s medical condition or geo-graphic constraints.
2. The functional capabilities of facili-ties that provide inpatient care fornewborn infants should be classi-fied uniformly on the basis of geo-graphic and population parametersin collaboration with state healthdepartments, as follows:
� Level I: a hospital nursery or-ganized with the personnel andequipment to perform neonatalresuscitation, evaluate and pro-vide postnatal care of healthynewborn infants, provide carefor infants born at 35 to 37weeks’ gestation who remainphysiologically stable, and sta-bilize ill newborn infants orinfants born at less than 35weeks’ gestational age untiltransfer to a facility that canprovide the appropriate levelof neonatal care.
� Level II: a hospital special carenursery organized with thepersonnel and equipment toprovide care to infants bornat 32 weeks’ gestation or moreand weighing 1500 g or moreat birth who have physiologicimmaturity, such as apnea ofprematurity, inability to maintain
body temperature, or inabilityto take oral feedings; whoare moderately ill with problemsthat are expected to resolve rap-idly and are not anticipated toneed subspecialty services onan urgent basis; or who areconvalescing from a higher levelof intensive care. A level II cen-ter has the capability to providecontinuous positive airway pres-sure and may provide me-chanical ventilation for briefdurations (less than 24 hours).
� Level III: a hospital NICU orga-nized with personnel and equip-ment to provide continuous lifesupport and comprehensivecare for extremely high-risknewborn infants and those withcritical illness. This includesinfants born weighing <1500 gor at <32 weeks’ gestation. LevelIII units have the capability toprovide critical medical and sur-gical care. Level III units routinelyprovide ongoing assisted ventila-tion; have ready access to a fullrange of pediatric medical sub-specialists; have advanced imag-ing with interpretation on anurgent basis, including CT, MRI,and echocardiography; have ac-cess to pediatric ophthalmologicservices with an organizedprogram for the monitoring,treatment, and follow-up of reti-nopathy of prematurity; andhave pediatric surgical special-ists and pediatric anesthesiolo-gists on site or at a closelyrelated institution to performmajor surgery. Level III unitscan facilitate transfer tohigher-level facilities or child-ren’s hospitals, as well as back-transport recovering infants tolower-level facilities, as clinicallyindicated.
� Level IV units have the capa-bilities of a level III NICU and
594 FROM THE AMERICAN ACADEMY OF PEDIATRICS
by guest on May 26, 2018http://pediatrics.aappublications.org/Downloaded from

are located within institutionsthat can provide on-site surgi-cal repair of serious congenitalor acquired malformations. LevelIV units can facilitate transportsystems and provide outreacheducation within their catchmentarea.
3. The functional capabilities of facilitiesthat provide inpatient care for new-born infants should be classified uni-formly and with clear definitions thatinclude requirements for equipment,personnel, facilities, ancillary serv-ices, training, and the organizationof services (including transport) forthe capabilities of each level of care.
4. Population-based data on patientoutcomes, including mortality, mor-bidity, and long-term outcomes,should be obtained to providelevel-specific standards for patientsrequiring various categories ofspecialized care, including surgery.
LEAD AUTHORCAPT Wanda Denise Barfield, MD, MPH
COMMITTEE ON FETUS ANDNEWBORN, 2011–2012Lu-Ann Papile, MD, ChairpersonJill E. Baley, MDWilliam Benitz, MDJames Cummings, MDWaldemar A. Carlo, MD
Praveen Kumar, MDRichard A. Polin, MDRosemarie C. Tan, MD, PhDKristi L. Watterberg, MD
LIAISONSCAPT Wanda Denise Barfield, MD, MPH – Centersfor Disease Control and PreventionGeorge Macones, MD – American College ofObstetricians and GynecologistsAnn L. Jefferies, MD – Canadian Pediatric So-cietyRosalie O. Mainous, PhD, RNC, NNP – NationalAssociation of Neonatal NursesTonse N. K. Raju, MD, DCH – National Institutes ofHealthKasper S. Wang, MD – Section on Surgery
STAFFJim Couto, MA
REFERENCES
1. Stark AR; American Academy of PediatricsCommittee on Fetus and Newborn. Levels ofneonatal care. Pediatrics. 2004;114(5):1341–1347
2. Bode MM, O’shea TM, Metzguer KR, StilesAD. Perinatal regionalization and neonatalmortality in North Carolina, 1968–1994. AmJ Obstet Gynecol. 2001;184(6):1302–1307
3. MacDorman MF, Kirmeyer S. Fetal andperinatal mortality, United States, 2005.Natl Vital Stat Rep. 2009;57(8):1–19
4. Clement MS. Perinatal care in Arizona1950–2002: a study of the positive impactof technology, regionalization and the Ari-zona perinatal trust. J Perinatol. 2005;25(8):503–508
5. March of Dimes, Committee on PerinatalHealth. Toward Improving the Outcomeof Pregnancy: Recommendations for theRegional Development of Maternal andPerinatal Health Services. White Plains,NY: March of Dimes National Foundation;1976
6. Richardson DK, Reed K, Cutler JC, et al.Perinatal regionalization versus hospitalcompetition: the Hartford example. Pediat-rics. 1995;96(3 pt 1):417–423
7. Yeast JD, Poskin M, Stockbauer JW, ShafferS. Changing patterns in regionalization ofperinatal care and the impact on neonatalmortality. Am J Obstet Gynecol. 1998;178(1pt 1):131–135
8. Goodman DC, Fisher ES, Little GA, Stukel TA,Chang CH. Are neonatal intensive careresources located according to need?
Regional variation in neonatologists, beds,and low birth weight newborns. Pediatrics.2001;108(2):426–431
9. Howell EM, Richardson D, Ginsburg P, FootB. Deregionalization of neonatal intensivecare in urban areas. Am J Public Health.2002;92(1):119–124
10. Haberland CA, Phibbs CS, Baker LC. Effect ofopening midlevel neonatal intensive careunits on the location of low birth weightbirths in California. Pediatrics. 2006;118(6).Available at: www.pediatrics.org/cgi/con-tent/full/118/6/e1667
11. Dobrez D, Gerber S, Budetti P. Trends inperinatal regionalization and the role ofmanaged care. Obstet Gynecol. 2006;108(4):839–845
12. US Department of Health and HumanServices, Health Resources and Ser-vice Administration, Maternal and ChildHealth Bureau. National PerformanceMeasure # 17. Available at: https://perfdata.hrsa.gov/mchb/TVISReports/. Accessed July12, 2012
13. Centers for Disease Control and Prevention(CDC). Neonatal intensive-care unit admis-sion of infants with very low birth weight—19 States, 2006. MMWR Morb Mortal WklyRep. 2010;59(44):1444–1447
14. Martin JA, Hamilton BE, Ventura SJ, et al.Births: final data for 2009. Natl Vital StatRep. 2011;60(1):1–70
15. Yoder BA, Gordon MC, Barth WH Jr. Late-preterm birth: does the changing obstet-ric paradigm alter the epidemiology of
respiratory complications? Obstet Gynecol.2008;111(4):814–822
16. Schieve LA, Ferre C, Peterson HB, MacalusoM, Reynolds MA, Wright VC. Perinatal out-come among singleton infants conceivedthrough assisted reproductive technologyin the United States. Obstet Gynecol. 2004;103(6):1144–1153
17. Joseph KS, Marcoux S, Ohlsson A, et al;Fetal and Infant Heath Study Group of theCanadian Perinatal Surveillance System.Changes in stillbirth and infant mortality as-sociated with increases in preterm birthamong twins. Pediatrics. 2001;108(5):1055–1061
18. Kaaja RJ, Greer IA. Manifestations ofchronic disease during pregnancy. JAMA.2005;294(21):2751–2757
19. Shapiro-Mendoza CK, Tomashek KM, Kotel-chuck M, et al. Effect of late-preterm birthand maternal medical conditions on new-born morbidity risk. Pediatrics. 2008;121(2). Available at: www.pediatrics.org/cgi/content/full/121/2/e223
20. Yang Q, Greenland S, Flanders WD. Associ-ations of maternal age- and parity-relatedfactors with trends in low-birthweightrates: United States, 1980 through 2000.Am J Public Health. 2006;96(5):856–861
21. Davidoff MJ, Dias T, Damus K, et al. Changesin the gestational age distribution amongU.S. singleton births: impact on rates oflate preterm birth, 1992 to 2002. SeminPerinatol. 2006;30(1):8–15
22. Engle WA, Tomashek KM, Wallman C; Com-mittee on Fetus and Newborn, American
PEDIATRICS Volume 130, Number 3, September 2012 595
FROM THE AMERICAN ACADEMY OF PEDIATRICS
by guest on May 26, 2018http://pediatrics.aappublications.org/Downloaded from

Academy of Pediatrics. “Late-preterm”infants: a population at risk. Pediatrics.2007;120(6):1390–1401
23. Ramachandrappa A, Rosenberg ES, WagonerS, Jain L. Morbidity and mortality in late pre-term infants with severe hypoxic respiratoryfailure on extra-corporeal membrane oxy-genation. J Pediatr. 2011;159(2):192–198, e3
24. Philip AG. The evolution of neonatology.Pediatr Res. 2005;58(4):799–815
25. Thompson LA, Goodman DC, Little GA. Ismore neonatal intensive care always bet-ter? Insights from a cross-national com-parison of reproductive care. Pediatrics.2002;109(6):1036–1043
26. Gould JB, Marks AR, Chavez G. Expansion ofcommunity-based perinatal care in Cal-ifornia. J Perinatol. 2002;22(8):630–640
27. Stoll BJ, Hansen NI, Bell EF, et al; EuniceKennedy Shriver National Institute of ChildHealth and Human Development NeonatalResearch Network. Neonatal outcomes ofextremely preterm infants from the NICHDNeonatal Research Network. Pediatrics.2010;126(3):443–456
28. Heron M, Sutton PD, Xu J, Ventura SJ,Strobino DM, Guyer B. Annual summary ofvital statistics: 2007. Pediatrics. 2010;125(1):4–15
29. Lasswell SM, Barfield WD, Rochat RW,Blackmon L. Perinatal regionalization forvery low-birth-weight and very preterminfants: a meta-analysis. JAMA. 2010;304(9):992–1000
30. Phibbs CS, Baker LC, Caughey AB, DanielsenB, Schmitt SK, Phibbs RH. Level and volumeof neonatal intensive care and mortality invery-low-birth-weight infants. N Engl J Med.2007;356(21):2165–2175
31. Chung JH, Phibbs CS, Boscardin WJ,Kominski GF, Ortega AN, Needleman J. Theeffect of neonatal intensive care level andhospital volume on mortality of very lowbirth weight infants. Med Care. 2010;48(7):635–644
32. Bartels DB, Wypij D, Wenzlaff P, Dammann O,Poets CF. Hospital volume and neonatalmortality among very low birth weightinfants. Pediatrics. 2006;117(6):2206–2214
33. Rogowski JA, Horbar JD, Staiger DO, KennyM, Carpenter J, Geppert J. Indirect vs directhospital quality indicators for very low-birth-weight infants. JAMA. 2004;291(2):202–209
34. Morales LS, Staiger D, Horbar JD, et al.Mortality among very low-birthweightinfants in hospitals serving minority pop-ulations. Am J Public Health. 2005;95(12):2206–2212
35. Howell EA, Hebert P, Chatterjee S, KleinmanLC, Chassin MR. Black/white differences in
very low birth weight neonatal mortalityrates among New York City hospitals. Pe-diatrics. 2008;121(3). Available at: www.pe-diatrics.org/cgi/content/full/121/3/e407
36. Rogowski JA, Staiger DO, Horbar JD. Var-iations in the quality of care for very-low-birthweight infants: implications for policy.Health Aff (Millwood). 2004;23(5):88–97
37. Palmer KG, Kronsberg SS, Barton BA, HobbsCA, Hall RW, Anand KJ. Effect of inbornversus outborn delivery on clinical out-comes in ventilated preterm neonates:secondary results from the NEOPAIN trial.J Perinatol. 2005;25(4):270–275
38. Wall SN, Handler AS, Park CG. Hospitalfactors and nontransfer of small babies:a marker of deregionalized perinatal care?J Perinatol. 2004;24(6):351–359
39. Zeitlin J, Gwanfogbe CD, Delmas D, et al.Risk factors for not delivering in a level IIIunit before 32 weeks of gestation: resultsfrom a population-based study in Paris andsurrounding districts in 2003. PaediatrPerinat Epidemiol. 2008;22(2):126–135
40. Arad I, Baras M, Bar-Oz B, Gofin R. Neonataltransport of very low birth weight infantsin Jerusalem, revisited. Isr Med Assoc J.2006;8(7):477–482
41. Institute of Medicine. Preterm Birth: Cau-ses, Consequences, and Prevention. Wash-ington, DC: National Academies Press; 2007
42. Rautava L, Lehtonen L, Peltola M, et al;PERFECT Preterm Infant Study Group.The effect of birth in secondary- ortertiary-level hospitals in Finland onmortality in very preterm infants: a birth-register study. Pediatrics. 2007;119(1).Available at: www.pediatrics.org/cgi/con-tent/full/119/1/e257
43. Johansson S, Montgomery SM, Ekbom A,et al. Preterm delivery, level of care, andinfant death in sweden: a population-basedstudy. Pediatrics. 2004;113(5):1230–1235
44. Vieux R, Fresson J, Hascoet JM, et al; EPI-PAGE Study Group. Improving perinatalregionalization by predicting neonatal in-tensive care requirements of preterminfants: an EPIPAGE-based cohort study.Pediatrics. 2006;118(1):84–90
45. Audibert F. Regionalization of perinatalcare: did we forget congenital anomalies?Ultrasound Obstet Gynecol. 2007;29(3):247–248
46. Martin JA, Menacker F. Expanded healthdata from the new birth certificate, 2004.Natl Vital Stat Rep. 2007;55(12):1–22
47. Menacker F, Martin JA. Expanded healthdata from the new birth certificate, 2005.Natl Vital Stat Rep. 2008;56(13):1–24
48. Blackmon LR, Barfield WD, Stark AR. Hos-pital neonatal services in the United States:
variation in definitions, criteria, and regu-latory status, 2008. J Perinatol. 2009;29(12):788–794
49. Lorch SA, Maheshwari P, Even-Shoshan O.The impact of certificate of need programson neonatal intensive care units. J Peri-natol. 2012;32(1):39–44
50. Nowakowski L, Barfield WD, KroelingerCD, et al. Assessment of state measuresof risk-appropriate care for very lowbirth weight infants and recom-mendations for enhancing regionalizedstate systems. Matern Child Health J.2012;16(1):217–227
51. Acolet D, Elbourne D, McIntosh N, et al;Confidential Enquiry Into Maternal andChild Health. Project 27/28: inquiry intoquality of neonatal care and its effect onthe survival of infants who were born at 27and 28 weeks in England, Wales, andNorthern Ireland. Pediatrics. 2005;116(6):1457–1465
52. Ohlinger J, Kantak A, Lavin JP Jr;et al.Evaluation and development of potentiallybetter practices for perinatal and neonatalcommunication and collaboration. Pediat-rics. 2006;118(suppl 2):S147–S152
53. March of Dimes. Toward Improving theOutcome of Pregnancy III: Enhancing Peri-natal Health Through Quality, Safety,and Performance Initiatives (TIOP3). WhitePlains, NY: March of Dimes Foundation;2010
54. Committee on Perinatal Health. TowardImproving the Outcome of Pregnancy: The90s and Beyond. White Plains, NY: March ofDimes Foundation; 1993
55. American Academy of Pediatrics, AmericanCollege of Obstetrics and Gynecology.Guidelines for Perinatal Care. 6th ed. ElkGrove Village, IL: American Academy of Pe-diatrics; 2007
56. American Academy of Pediatrics. Sectionon Transport Medicine. Guidelines for Airand Ground Transport of Neonatal andPediatric Patients. 3rd ed. Elk Grove Vil-lage, IL: American Academy of Pediatrics;2012
57. Fierson WM; Section on OphthalmologyAmerican Academy of Pediatrics; Ameri-can Academy of Ophthalmology; AmericanAssociation for Pediatric Ophthalmologyand Strabismus. Screening examinationof premature infants for retinopathy ofprematurity. Pediatrics. 2006;117(2):572–576
58. Kosloske A; American Academy of Pediat-rics, Surgical Advisory Panel. Guidelines forreferral to pediatric surgical specialists.Pediatrics. 2002;110(1 pt 1):187–191; reaf-firmed in Pediatrics. 2007;119(5):1031
596 FROM THE AMERICAN ACADEMY OF PEDIATRICS
by guest on May 26, 2018http://pediatrics.aappublications.org/Downloaded from

59. Burstein DS, Jacobs JP, Li JS, et al. Caremodels and associated outcomes in con-genital heart surgery. Pediatrics. 2011;127(6). Available at: www.pediatrics.org/cgi/content/full/127/6/e1482
60. Attar MA, Lang SW, Gates MR, Iatrow AM,Bratton SL. Back transport of neonates:effect on hospital length of stay. J Perinatol.2005;25(11):731–736
61. Berry MA, Shah PS, Brouillette RT, HellmannJ. Predictors of mortality and length of stayfor neonates admitted to children’s hospitalneonatal intensive care units. J Perinatol.2008;28(4):297–302
62. American College of Obstetricians andGynecologists. Cultural sensitivity andawareness in the delivery of health care.Committee Opinion No. 493. Obstet Gynecol.2011;117(5):1258–1261
63. American College of Obstetricians andGynecologists. Effective patient-physiciancommunication. Committee Opinion No. 492.Obstet Gynecol. 2011;117(5):1254–1257
64. Tucker CM. US Department of Health andHuman Services Advisory Committee on Mi-nority Health. Reducing Health Disparities byPromoting Patient-Centered Culturally andLinguistically Sensitive/Competent Health
Care. Rockville, MD: US Public Health Service;2009
65. Britton CV; American Academy of PediatricsCommittee on Pediatric Workforce. Ensur-ing culturally effective pediatric care:implications for education and health pol-icy. Pediatrics. 2004;114(6):1677–1685
66. Eichner JM, Johnson BH; Committee on Hos-pital Care. American Academy of Pediatrics.Family-centered care and the pediatrician’srole. Pediatrics. 2003;112(3 pt 1):691–697
67. Kattwinkel J, Cook LJ, Nowacek G, et al.Regionalized perinatal education. SeminNeonatol. 2004;9(2):155–165
PEDIATRICS Volume 130, Number 3, September 2012 597
FROM THE AMERICAN ACADEMY OF PEDIATRICS
by guest on May 26, 2018http://pediatrics.aappublications.org/Downloaded from

DOI: 10.1542/peds.2012-1999 originally published online August 27, 2012; 2012;130;587Pediatrics
COMMITTEE ON FETUS AND NEWBORNLevels of Neonatal Care
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/130/3/587including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/130/3/587.full#ref-list-1This article cites 58 articles, 21 of which you can access for free at:
Subspecialty Collections
orn_infant_subhttp://classic.pediatrics.aappublications.org/cgi/collection/fetus:newbFetus/Newborn Infant_on_fetus__newbornhttp://classic.pediatrics.aappublications.org/cgi/collection/committeeCommittee on Fetus & Newbornlicyhttp://classic.pediatrics.aappublications.org/cgi/collection/current_poCurrent Policyfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
https://shop.aap.org/licensing-permissions/in its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://classic.pediatrics.aappublications.org/content/reprintsInformation about ordering reprints can be found online:
ISSN: . 60007. Copyright © 2012 by the American Academy of Pediatrics. All rights reserved. Print American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since . Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on May 26, 2018http://pediatrics.aappublications.org/Downloaded from
DOI: 10.1542/peds.2012-1999 originally published online August 27, 2012; 2012;130;587Pediatrics
COMMITTEE ON FETUS AND NEWBORNLevels of Neonatal Care
http://pediatrics.aappublications.org/content/130/3/587located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: . 60007. Copyright © 2012 by the American Academy of Pediatrics. All rights reserved. Print American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since . Pediatrics is owned, published, and trademarked by the Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on May 26, 2018http://pediatrics.aappublications.org/Downloaded from