Embed Size (px)
Citation preview

REVIEW
Polio Eradication in India
T. N. Dhole • Vikas Mishra
Received: 18 October 2011 / Accepted: 14 November 2011 / Published online: 1 March 2012
� The National Academy of Sciences, India 2012
Abstract The Global Polio Eradication Initiative gained
a great success in India in the last one year, especially on
the epidemiology of type 1 wild poliovirus (WPV), by the
intensive use of monovalent oral polio vaccine (OPV) type
1. However, failure to completely interrupt the transmis-
sion of type 1 and persistence of type 3 WPV in western
Uttar Pradesh and Bihar are still causes of concern. The
year 2010 was very crucial for polio eradication in India; as
good control over transmission of type 1 wild polio virus
was achieved. While mOPV1 is a sharper tool against
WPV1, bOPV seems to be adequate against WPV3; hence
there may not be any more need for mOPV3. Thus, the key
to success lies in intelligent and imaginative use of the
three OPVs, i.e. mOPV1, bOPV and tOPV, against WPV
types 1 and 3, and circulating vaccine derived polio virus
types 1, 2 and 3. Serious consideration should be given to a
contingency plan to the use of inactivated polio vaccine or
non OPV in endemic areas.
Keywords Epidemiology � Inactivated polio vaccine �Oral polio vaccine � Vaccine derived polio virus �Wild poliovirus
Introduction
Global eradication of polio is not possible without taking care
of circulation of wild polio virus in India, Pakistan, Afghan-
istan and Africa. India’s original goal was to eliminate polio
by the year 2000—the gift of a polio free world to the children
of the 21st century. That goal was missed for wild polioviruses
(WPV’s) type 1 and type 3 and these two serotypes are still in
circulation. The Government of India then revised the goal in
2005 and extended to 2015 [1]. By the year 2010, a good
decline in the number of polio cases has been observed in Uttar
Pradesh and Bihar [2].
In 2003 the formal view of the officers of the Health
Ministry and National Polio Surveillance Project (NPSP)
which was the reason for lack of success was ‘‘failure to
vaccinate’’ an adequate proportion of children [3–5]. Both
efficacy and protection of trivalent vaccine (tOPV) in children
of temperate climate was questioned [6–8]. The mucosal
response to tOPV was doubted and felt that there was need of
inactivated polio vaccine IPV [7]. In 2005 the failure of vac-
cine was officially acknowledged and monovalent vaccine
OPV (mOPV) types 1 and 3 were licensed for the first time in
India. It has been shown long back by Indian scientists that the
vaccine efficacy (VE) of trivalent oral polio vaccine (tOPV)
was very low against WPV types 1 and 3 and that it was 2–3
times higher in mOPV 1 and 3, respectively [9–11]. In India
the trial for monovalent vaccine was carried out in 2003 and
2004 in Ahmedabad, Indore and Bhopal. The conclusion of
trial was drawn on basis of the minimum excretion of the
vaccine virus inversely proportion to large amount of the
intestinal antibody present in the fecal sample by plaque
counting assay.
Epidemiology
The disease of poliomyelitis has a long history. The first
example may even have been more than 3000 years ago. An
Egyptian stele dating from the 18th Egyptian dynasty
(1580–1350 BCE) shows a priest with a deformity of his leg
characteristic of the flaccid paralysis typical of poliomyelitis.
T. N. Dhole (&) � V. Mishra
Department of Microbiology, Sanjay Gandhi Post Graduate
Institute of Medical Sciences, Lucknow, Uttar Pradesh, India
e-mail: [email protected]
123
Proc. Natl. Acad. Sci. Sect B. Biol. Sci. (January–March 2012) 82(1):123–133
DOI 10.1007/s40011-011-0010-0

The first known clinical description of poliomyelitis is
attributed to Michael Underwood, a British physician, who in
1789 reported observing an illness which appeared to target
primarily children and left those afflicted with residual
debility of the lower extremities. Initial outbreaks in Europe
were documented in the early 19th century and outbreaks in
the United States were first reported in 1843. However, it was
not until the early 20th century that the number of paralytic
poliomyelitis cases reached epidemic proportions [12]. The
polio is in circulation in India since ages especially in Uttar
Pradesh and Bihar because of poor sanitation and high pop-
ulation density. If one looks at the picture of different villages
of Uttar Pradesh and Bihar, old paralytic cases of acute flaccid
paralysis (AFP) can easily be found. This indicates that the
polio virus has survived and circulated in these areas for years.
This circulating virus has made victim of polio cases time to
time depending upon the immunity in general population.
Molecular Epidemiology of Wild Poliovirus
Circulation in India
The role of molecular surveillance in eradication initiatives
of poliomyelitis has proven to be an extremely powerful
tool for assessing the transmission pathways, monitoring
quality of the national immunization program, assessing
vaccine coverage and monitoring the success of eradication
strategies. The polio virus has three serotypes; PV1, PV2
and PV3 (Figs. 1, 2), sufficient genetic clusters [11] have
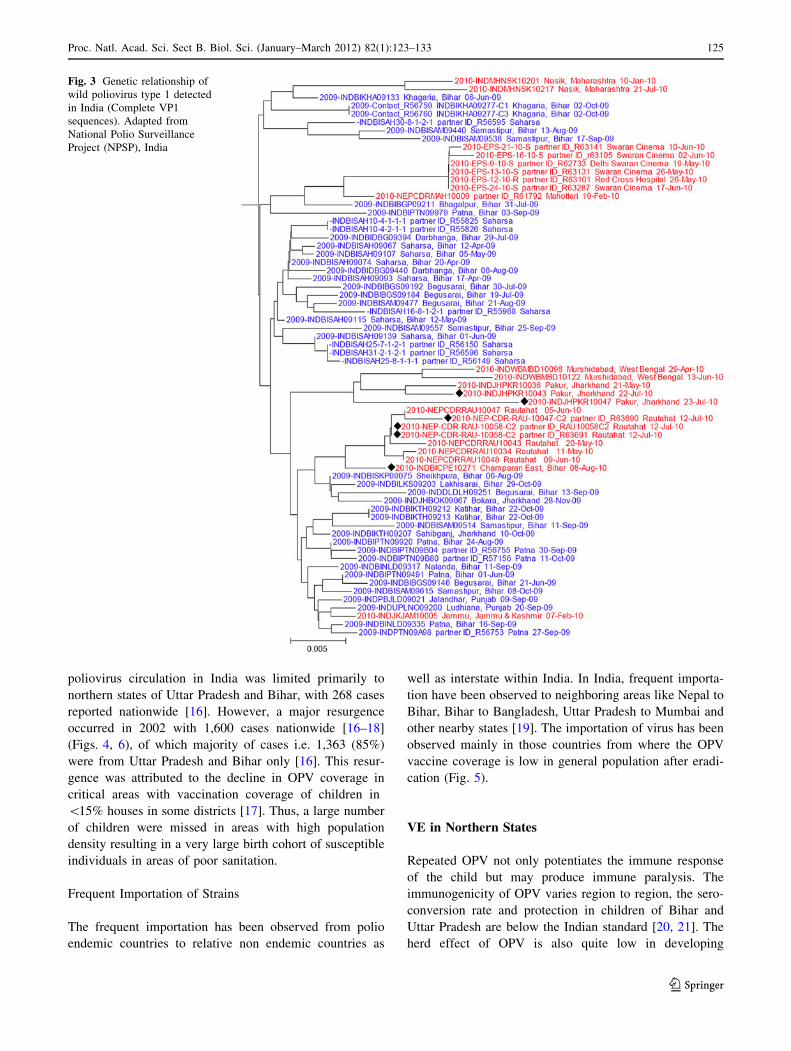
been observed in each serotype (Fig. 3). The genotype and
cluster, lineage and sublineage are the operational taxo-
nomic units for molecular surveillance. For all practical
purposes, VP1-906 nt has been sequenced and compared
[13]. It is essential to know the indigenous baseline geno-
type/cluster/lineage circulating in different states of India
and to monitor the changes with accelerated efforts for
elimination of these lineages.
Currently the Polio virus wild type 1 has three clusters
with multiple lineages circulating in different parts of India
while wild type 3 has four clusters with few lineages. P2
wild polio virus has already been eradicated from India
[14]. Surveillance for poliomyelitis is a dynamic process
and continuous monitoring of appearance and disappear-
ance of different lineages in any given region is imperative.
The most effective and useful strategy of strain surveil-
lance is crossing over from endemic to relatively non-
endemic area. Depending upon the effective and optimal
immunization coverage, circulation of indigenous lineage
may persist or disappear. The close similarity of sequences
within each lineage indicates good quality of surveillance.
Some of the wild poliovirus strains may disappear without
surfacing for more than 2 years (silent transmission) or
may appear as importation from other countries. It is a
barometer of current status of polio eradication which helps
in refining the strategies to achieve the goal in shortest
possible time.
An Update on Epidemiology
In May 1988, during the World Health Assembly, Minister
of health of all member states of the World Health Orga-
nization (WHO) voted to launch global goal to eradicate
polio. As a result of this global polio eradication initiative
started and estimated global incidence of polio decreased
by more than 99% with three WHO regions (Americas,
Western Pacific and Europe) being certified polio-free [15].
Intensive polio eradication program in the South–East
Asia Region (SEAR), with the use of tOPV, led to the
substantial decrease in the number of polio cases. By 2001,
Fig. 1 Poliovirus serotypes. Three immunologically distinct types of
PV, PV-1, PV-2 and PV-3 have been recognized. Strains which cause
severe paralysis are known as wild poliovirus (PV1-wild, PV2-wild
and PV3-wild). Sabin PV1, PV2 and PV3 strains are used as efficient
vaccine known as Vaccine derived poliovirus. Adapted from www.
http://wenliang.myweb.uga.edu
Fig. 2 Structure of poliovirus. Poliovirus genome consists of a single
molecule of single stranded RNA, *7,500 nucleotides long. It acts
like mRNA in infected cell and is translated into a single large
polypeptide. This polypeptide is cleaved by virus coded enzymes into
capsid proteins (VP1, VP2, VP3 and VP4) and non-structural proteins
which include proteases and RNA-dependent RNA polymerase.
Partially adapted from ‘‘Poliovirus proves IRES-istible in vivo’’ [60]
124 Proc. Natl. Acad. Sci. Sect B. Biol. Sci. (January–March 2012) 82(1):123–133
123
poliovirus circulation in India was limited primarily to
northern states of Uttar Pradesh and Bihar, with 268 cases
reported nationwide [16]. However, a major resurgence
occurred in 2002 with 1,600 cases nationwide [16–18]
(Figs. 4, 6), of which majority of cases i.e. 1,363 (85%)
were from Uttar Pradesh and Bihar only [16]. This resur-
gence was attributed to the decline in OPV coverage in
critical areas with vaccination coverage of children in
\15% houses in some districts [17]. Thus, a large number
of children were missed in areas with high population
density resulting in a very large birth cohort of susceptible
individuals in areas of poor sanitation.
Frequent Importation of Strains
The frequent importation has been observed from polio
endemic countries to relative non endemic countries as
well as interstate within India. In India, frequent importa-
tion have been observed to neighboring areas like Nepal to
Bihar, Bihar to Bangladesh, Uttar Pradesh to Mumbai and
other nearby states [19]. The importation of virus has been
observed mainly in those countries from where the OPV
vaccine coverage is low in general population after eradi-
cation (Fig. 5).
VE in Northern States
Repeated OPV not only potentiates the immune response
of the child but may produce immune paralysis. The
immunogenicity of OPV varies region to region, the sero-
conversion rate and protection in children of Bihar and
Uttar Pradesh are below the Indian standard [20, 21]. The
herd effect of OPV is also quite low in developing
Fig. 3 Genetic relationship of
wild poliovirus type 1 detected
in India (Complete VP1
sequences). Adapted from
National Polio Surveillance
Project (NPSP), India
Proc. Natl. Acad. Sci. Sect B. Biol. Sci. (January–March 2012) 82(1):123–133 125
123

countries like India [21]. Vaccine viruses are less infectious
than their wild counterparts and spread to non-immune
children (contact immunization) is another reason. Both of
these factors are weak in children of Uttar Pradesh and
Bihar. Therefore, virtually every child must be vaccinated
with repeated doses of OPV to ensure personal protection
but it is difficult to achieve where primary immunization is
weak. If the immunization rates fall after achieving high
level of immunity in the polio-free community, risk of
large outbreaks increase rapidly among the growing
cohorts of non-immune children. The routine immunization
with OPV will no longer outweigh the burden of diseases
Fig. 4 Monthly incidence of
wild poliovirus cases in India
with national, sub-national and
large scale immunization.
Adapted from National Polio
Surveillance Project (NPSP),
India
• Wild virus type 1• Wild virus type 3• Wild virus type 1 and 3
Endemic countries Case or outbreak following importation (last 6 months)Case or outbreak following importation (6-12 months)
Fig. 5 Tracing virus transmission pathways. Adapted from National Polio Surveillance Project (NPSP), India
126 Proc. Natl. Acad. Sci. Sect B. Biol. Sci. (January–March 2012) 82(1):123–133
123

either due to paralysis caused by OPV (vaccine associated
paralytic polio), or outbreak caused by circulating vaccine-
derived poliomyelitis (cVDPV) [22].
The mucosal immunity induced by OPV in India varies
by location, serotype, and vaccine formulation [10]. The
present discrepancies in tOPV versus IPV is debatable
based on scientific merit and demerit, advantage versus
disadvantage of their use in two highly populated states of
the country [23]. The tOPV/Monovalent OPV (mOPV) has
reduced the circulation of wild poliovirus from major part
of the country without making significant impact in their
circulation in 107 sub-districts of Uttar Pradesh and Bihar.
Therefore the success of tOPV cannot be ignored, but its
small amount inherent problem of the vaccine needs to be
addressed. It is difficult to maintain the high level of
immunity in the community with tOPV because of sero-
conversion, GI immunity and sustaining the high level of
antibody for protection. The polio eradication stands for,
eradication of wild as well as vaccine strain from the
community. Therefore prolonged use of tOPV will invite
innumerable problems like frequent importation of wild
strains, occurrence of circulating cVDPV’s and vaccine-
associated paralytic poliomyelitis (VAPP), circulation of
Sabin strains in the community [24–26].
Recent studies have shown that the VE of IPV is very
high and it is completely safe to use [27, 28]. Where VE of
OPV is problematic, IPV provides predictably high VE.
However, the areas which are of concern with IPV devel-
opment and implementation are the choice of appropriate
adjuvant to be used in IPV [29–31], population immunity
[27], assessment of risks of paralytic diseases due to
poliomyelitis in the post eradication era [32]. The above
needs methodical evaluation for policy making and rec-
ommendation of IPV.
Risk Associated With OPV Vaccine Use
Seroconversion Studies in Children Given OPV
A number of studies have shown that seroconversion fre-
quency is less than expected after giving tOPV [26, 33, 34].
WHO has tried to overcome serious problem with subop-
timal efficacy of OPV by dividing tOPV into monovalent
vaccines. Since 2005, two vaccines, mOPV1 and mOPV3,
were used to immunize children. The selection of vaccine
type was in accordance with the prevailing wild virus type
circulation in the different parts of Uttar Pradesh and Bihar.
The epidemiological data generated with this strategy
seems very promising as there is drastic reduction in cir-
culation of P1 wild while still the detection rate of P3 wild
strain remains static [35].
The above diminishing of one strain while static detection
rate of other strain depicts a possible pattern. Prioritization of
eradication of P1 type wild strain tend to minimize the
attention on eradication of other variants, which subsequently
lead to the emergence of P3 wild, P2 cVDPV and P1 cVDPV
isolates (Fig. 6). Thus in policy making further changes has
been incorporated, which states maintenance of the equal
pressure on the eradication of all three strains of wild polio
viruses, while trying to eradicate at least one.
Recent studies of WHO has shown the servoconversion
rate of mOPV-1 and mOPV-3 is 99 and 95%, respectively.
The study advocates, that there is no need to opt for IPV as
IPV is no way better than OPV as far as seroconversion is
concerned. The question remains to be answered that,
whether 99% seroconversion is cumulative effect of repe-
ated vaccination or 99% were above the protection level
and sustaining the same level for period of at least 3 years.
The seroconversion is easy to achieve but difficult to sus-
tain above the protection level, especially in settings where
children are malnourished, school dropout rate is high and
there is least or no education [21, 36, 37]. Frequent waxing
waning would result snacking of virus in the community
from highly immunized population to relatively under
immunized population after prolonged gap.
Emergence of Vaccine Derived Polio viruses (VDPVs)
Rare cases of paralytic polio occur due to the Sabin strain,
called as vaccine derived poliovirus (VDPV). VDPVs can
cause paralytic polio in humans and have the potential for
sustained circulation. VDPVs resemble WPVs biologically
and differ from the majority of vaccine related poliovirus
(VRPV) isolates by having genetic properties consistent
with prolonged replication or transmission. Because
poliovirus genomes evolve at a rate of approximately 1%
per year, VRPVs that differ from the corresponding OPV
strain by [1% of nucleotide positions (VP1 genomic
region) are presumed to have replicated for at least 1 year
in one or more persons after administration of an OPV
dose. This is substantially longer than the normal period of
vaccine virus replication of 4–6 weeks in an OPV reci-
pient. Poliovirus isolates are grouped into three categories,
based on the extent of divergence of the VP1 nucleotide
region compared with the corresponding OPV strain:
(a) VRPVs (\1% divergent [types 1 and 3] or \0.6%
divergent [type 2]);
(b) VDPVs (VRPVs that are[1% divergent [types 1 and
3] or [0.6% divergent [type 2] from the correspond-
ing OPV strain).
(c) WPVs (no genetic evidence of derivation from any
vaccine strain).
There are three types of VDPV
(A) Circulating vaccine-derived poliovirus (cVDPV).
Proc. Natl. Acad. Sci. Sect B. Biol. Sci. (January–March 2012) 82(1):123–133 127
123

(B) Immunodeficiency-related vaccine-derived poliovi-
rus (iVDPV).
(C) Ambiguous vaccine-derived poliovirus (aVDPV).
Circulating vaccine-derived poliovirus (cVDPV) On very
rare occasions, if a population is seriously under-immu-
nized, there are enough susceptible children for the
excreted vaccine-derived polioviruses to begin circulating
in the community. These viruses are called cVDPV which
has 1–15 nucleotide (nt) substitution of RNA at VP1 region
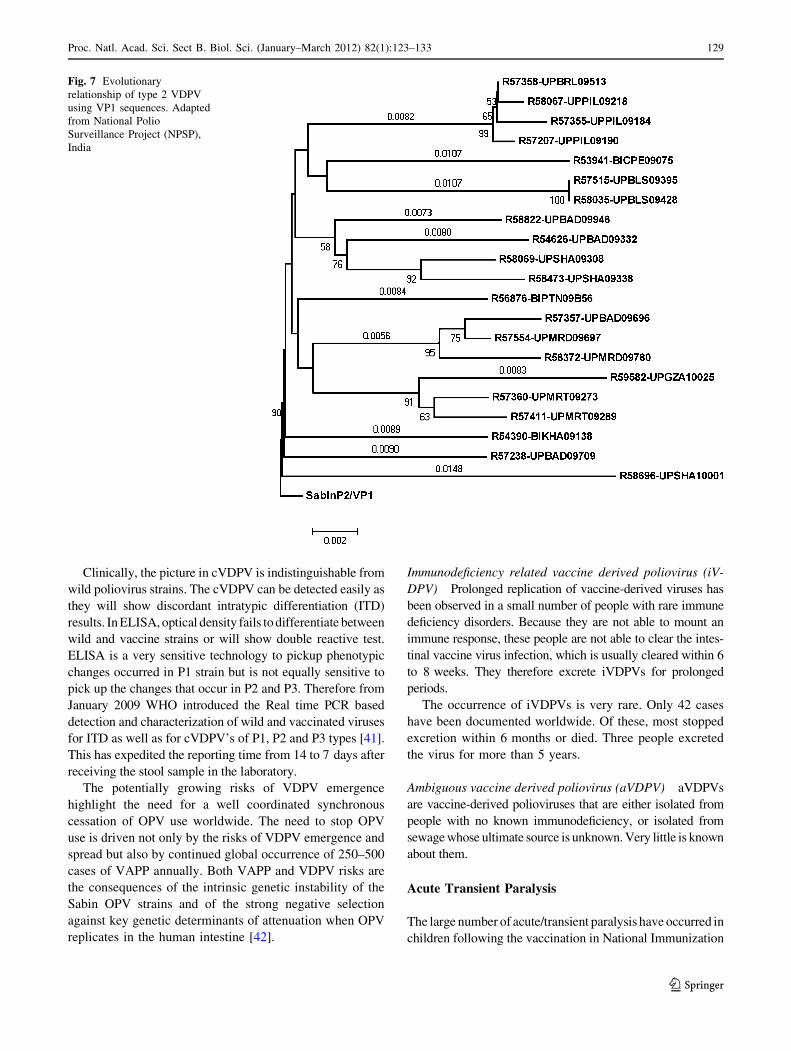
from other enteroviruses [38, 39] (Figs. 2, 7). The lower
the population immunity, the longer these viruses survive.
The longer they survive, the more they replicate, change,
and exchange genetic material with other enteroviruses as
they spread through a community. If a population is fully
immunized against polio, it will be protected against the
spread of both wild and vaccine strains of poliovirus.
Episodes of cVDPV are rare. Between 2000 and 2009—a
period in which nearly 10 billion doses of oral polio vaccine
were given worldwide—14 cVDPV outbreaks occurred,
resulting in 428 polio cases (Fig. 8). In the same period, wild
poliovirus paralyzed nearly 14,000 children [40].
Fig. 6 Geographical distribution of wild polio virus cases in India (1998–2011). Adapted from National Polio Surveillance Project (NPSP),
India
128 Proc. Natl. Acad. Sci. Sect B. Biol. Sci. (January–March 2012) 82(1):123–133
123
Clinically, the picture in cVDPV is indistinguishable from
wild poliovirus strains. The cVDPV can be detected easily as
they will show discordant intratypic differentiation (ITD)
results. In ELISA, optical density fails to differentiate between
wild and vaccine strains or will show double reactive test.
ELISA is a very sensitive technology to pickup phenotypic
changes occurred in P1 strain but is not equally sensitive to
pick up the changes that occur in P2 and P3. Therefore from
January 2009 WHO introduced the Real time PCR based
detection and characterization of wild and vaccinated viruses
for ITD as well as for cVDPV’s of P1, P2 and P3 types [41].
This has expedited the reporting time from 14 to 7 days after
receiving the stool sample in the laboratory.
The potentially growing risks of VDPV emergence
highlight the need for a well coordinated synchronous
cessation of OPV use worldwide. The need to stop OPV
use is driven not only by the risks of VDPV emergence and
spread but also by continued global occurrence of 250–500
cases of VAPP annually. Both VAPP and VDPV risks are
the consequences of the intrinsic genetic instability of the
Sabin OPV strains and of the strong negative selection
against key genetic determinants of attenuation when OPV
replicates in the human intestine [42].
Immunodeficiency related vaccine derived poliovirus (iV-
DPV) Prolonged replication of vaccine-derived viruses has
been observed in a small number of people with rare immune
deficiency disorders. Because they are not able to mount an
immune response, these people are not able to clear the intes-
tinal vaccine virus infection, which is usually cleared within 6
to 8 weeks. They therefore excrete iVDPVs for prolonged
periods.
The occurrence of iVDPVs is very rare. Only 42 cases
have been documented worldwide. Of these, most stopped
excretion within 6 months or died. Three people excreted
the virus for more than 5 years.
Ambiguous vaccine derived poliovirus (aVDPV) aVDPVs
are vaccine-derived polioviruses that are either isolated from
people with no known immunodeficiency, or isolated from
sewage whose ultimate source is unknown. Very little is known
about them.
Acute Transient Paralysis
The large number of acute/transient paralysis have occurred in
children following the vaccination in National Immunization
Fig. 7 Evolutionary
relationship of type 2 VDPV
using VP1 sequences. Adapted
from National Polio
Surveillance Project (NPSP),
India
Proc. Natl. Acad. Sci. Sect B. Biol. Sci. (January–March 2012) 82(1):123–133 129
123

Day’s (NID’s) and Sub-National Immunization Day’s
(SNID’s) and mopping up within first 3 days of vaccine
delivery [43, 44] (Fig. 4). A large number of stool samples
from these AFP cases were routinely sent for laboratory
investigations; where isolation of vaccine viruses has con-
firmed the role of OPV in AFP after vaccination. Although the
vaccine viruses are enough attenuated as evident by their
genetic analysis [45, 46], the hotspots in vaccine viruses
should be investigated to find out the possibilities of any
change/mutation following immunization.
Vaccine Delivery
The vaccine delivery needs a perfect organization and syn-
chronization between the deliverer and the recipient. Most of
the village heads are illiterate and do not have any docu-
mentation about the recent births and deaths. In the absence of
such epidemiological data, there are virtually no pre-prepa-
ration for implementation and delivery of vaccines and thus
entire program become highly disorganized. Missing of
children in every drive becomes very high following door to
door campaign and further it is very difficult to have a match
between first and second immunization drive. Most vaccina-
tors are not well trained, illiterate and do not have the ability to
motivate the parents for the benefits associated with vacci-
nation [47]. Thus whole purpose behind the safe delivery of
vaccine has been defeated.
Injectable Polio Vaccine (IPV)
The first vaccine against polio virus was developed by
Jonas Salk (1952), consisting of inactivated whole virions
of polioviruses, without any adjuvant [48, 49]. Today IPV
is prepared by growing the wild strains of polioviruses in
tissue culture medium in continuous culture flasks to have a
40-, 8- and 32-D antigen units for the three PV1, PV2 and
PV3 virus types, respectively [50, 51]. The viruses are
grown in MRC-5 cells (diploid cell origin), a line of normal
human diploid cell by micro-carrier technique in serum
free medium of M-199. After clarification and filtration,
viral suspension has been concentrated by ultra-filtration
and purified. After intradermal injection, the IPV is sup-
posed to raise the IgG neutralizing antibodies in the blood
and will also infiltrate the IgG’s and secretary IgA’s in the
intestinal lumen [52]. The neutralizing antibody will not
only inactivate the vaccine viruses as well as wild viruses,
thus it will confer total protection against circulating vac-
cine and wild strains. The IPV has been advised to be given
in two doses, 2 months apart, with alternate oral polio
vaccine [53]. It has been advised to be given in primary
immunization along with DPT [9].
The modern IPV is highly immunogenic, but how much
systemic antibodies will infiltrate at gut level is not known.
We still do not know whether the gut immunity in IPV will
be able to prevent the colonization of Sabin strains in initial
period of eradication while switching over from OPV to
Fig. 8 Geographical distribution of vaccine-derived polioviruses. Adapted from ‘‘update on vaccine-derived polioviruses-worldwide, July 2009–
March 2011
130 Proc. Natl. Acad. Sci. Sect B. Biol. Sci. (January–March 2012) 82(1):123–133
123

IPV in a phased manner. However, its immunogenicity is
dampened by the presence of maternal antibodies in the
young infants, especially up to 8 weeks. Two doses
(0.5 ml) of IPV have been given, preferably by subcuta-
neous injection and at an interval of 8 or more weeks to
induce antibody response in virtually 100% children [54].
The booster doses will be given at the age of 4–6 years
[55]. However, OPV would be needed to control any future
outbreak of wild polio viruses.
The main shortcoming for the use of IPV in developing
countries involves the trained vaccinator for injecting
(subcutaneous, intramuscular or intradermal). The disad-
vantage of using needles for injecting vaccines involves
pain at the site of administration, logistical difficulties,
safety and disposal concerns.
New Trials for IPV
Countries like Cuba and Oman are testing the viability of
fractional doses and evaluating serologic response to 1/5th of a
standard dose with intradermal jet injector, which uses no
sharps and can be reset manually without use of batteries [56–
58]. If these studies prove successful, they would confer non-
inferior serologic and mucosal immunity at 1/5th of the cost of
the current IPV dose and could be administered by the vol-
unteers with an innovative and painless tool.
Future Strategies
This is the crucial time to discuss and plan for the future
vaccination strategy rather than waiting till WPV elimi-
nation is achieved. Phased introduction of IPV is required
in the RI (Routine Immunization) programs of southern
states where WPV transmission has already halted years
ago, followed gradually by universal use in RI all over the
country (when Uttar Pradesh and Bihar are also polio-free)
[59]. OPV used thereafter should be confined to three-
annual pulses through NIDs, until confirmed cessation of
the WPV transmission. There is urgent requirement to
chalk out a clear strategy on how to deal with the issues
like OPV cessation plans, global synchronization versus
regional/national synchronization, duration of AFP sur-
veillance, tackling of future outbreaks of both wild and
vaccine viruses, role of IPV in controlling future outbreaks
of cVDPVs, development of safe and affordable IPV etc.
Conclusions
Tremendous progress has been made in the global fight
against polio virus since 1988. A number of initiatives have
been implemented in India to intensify efforts to interrupt
transmission of WPV. Advocacy efforts have been
strengthened; mOPV1 to bOPV has been introduced in
January 2010 and they were used in campaigns in high-risk
areas. New strategies are being developed for switching
over for IPV from OPV with greater focus on 107 sub
districts of Northern India. The Polio eradication from
India is now mainly dependent on states of Uttar Pradesh
and Bihar as how quickly the transmission chains of WPV
is interrupted from these areas.
The areas which are of concern with IPV development and
implementation are the choice of appropriate adjuvant to be
used in IPV, VE, population immunity, assessment of risks of
paralytic diseases due to poliomyelitis in the post eradication
era. The above needs methodical evaluation for policy
making and recommendation of IPV. Although it is one of
the toughest tasks ever but polio eradication from India is
showing light of hope in near future. As per the new direc-
tives received from WHO, Indian manufacturers are
encouraged to prepare the IPV from Sabin polio virus strains
instead of their counterpart wild strains. Since the protein
yield of Sabin strain in tissue culture is low, therefore we
have to look for suitable adjuvant to enhance the antibody
response. At present we do not have any manufacturer in
India, except Panacea Biotech, who has some experience in
manufacturing IPV. Importing IPV vaccine from outside
India will be very expensive as we might need billion doses
to eradicate polio. Till date no indigenous manufacturer is
available for bulk and safe production of IPV. The intra-
dermal (non oral) polio vaccine which might be used in
future for polio eradication would have enumerable advan-
tage over wild as well as cVDPV.
References
1. Taylor S, Shimp L (2010) Using data to guide action in polio
health communications: experience from the polio eradication
initiative (PEI). J Health Commun 15(S1):48–65
2. Arora NK, Chaturvedi S, Dasgupta R (2010) Global lessons from
India’s poliomyelitis elimination campaign. Bull World Health
Organ 88(3):232–234
3. Pallansch MA, Sandhu HS (2006) The eradication of polio—
progress and challenges. N Engl J Med 355(24):2508–2511
4. Shah NK, John TJ, Thacker N et al (2006) Polio eradication
strategies in India: recommendations under IAP action plan 2006.
Indian Pediatr 43(12):1057–1063
5. Paul Y (2005) Polio eradication programme: some ethical issues.
Indian J Med Ethics 2(4):115–116
6. Patriarca PA, Wright PF, John TJ (1991) Factors affecting the
immunogenicity of oral poliovirus vaccine in developing coun-
tries: review. Rev Infect Dis 13(5):926–939
7. Skern T (2010) 100 years poliovirus: from discovery to eradi-
cation. A meeting report. Arch Virol 155(9):1371–1381
8. Chaturvedi G (2008) The vital drop: communication for polio
eradication in India. Sage Publications Pvt Ltd, New Delhi
Proc. Natl. Acad. Sci. Sect B. Biol. Sci. (January–March 2012) 82(1):123–133 131
123
9. Yotsu RR (2008) Global priorities and local realities: exploring
what happens to children identified with acute flaccid. University
of Liverpool
10. Grassly NC, Jafari H, Bahl S et al (2009) Mucosal immunity after
vaccination with monovalent and trivalent oral poliovirus vaccine
in India. J Infect Dis 200(5):794–801
11. John T, Jain H, Ravishankar K, et al (2011) Monovalent type 1 oral
poliovirus vaccine among infants in India: Report of two ran-
domized double-blind controlled clinical trials. Vaccine 5(29/34):
5793–5801
12. De Jesus NH (2007) Epidemics to eradication: the modern history
of poliomyelitis. Virol J 4:70. doi:10.1186/1743-422X-4-70
13. Martin J (2011) Detection and characterization of polioviruses.
Methods Mol Biol (Clifton) 665:233
14. Barrett S (2009) Polio eradication: strengthening the weakest
links. Health Aff (Millwood) 28(4):1079–1090
15. Sutter RW, Tangermann RH, Aylward RB et al (2001) Polio-
myelitis eradication: progress, challenges for the end game, and
preparation for the post-eradication era. Infect Dis Clin North Am
15(1):41–64
16. Faraj AA (2006) Poliomyelitis: orthopaedic management. Curr
Orthop 20(1):41–46
17. Mukherji WCS, Jindal LCAK, Singh BZ et al (2005) Polio
eradication in India: myth or reality. Med J Arm Forces Ind 61(4):
364–366
18. Sathyamala C, Mittal O, Dasgupta R et al (2005) Polio eradica-
tion initiative in India: deconstructing the GPEI. Int J Health Serv
35(2):361–383
19. Andrus JK, Thapa AB, Withana N et al (2001) A new paradigm
for international disease control: lessons learned from polio
eradication in Southeast Asia. Am J Public Health 91(1):146–150
20. Vashishtha VM (2009) Polio eradication in India: need for cau-
tion. Indian J Pediatr 76(7):757
21. Paul Y (2007) Role of genetic factors in polio eradication: new
challenge for policy makers. Vaccine 25(50):8365–8371
22. Heymann DL, Sutter RW, Aylward RB (2006) A vision of a world
without polio: the OPV cessation strategy. Biologicals 34(2):
75–79
23. Blume SS (2005) Lock in, the state and vaccine development:
lessons from the history of the polio vaccines. Res Policy
34(2):159–173
24. Modlin JF (2010) The bumpy road to polio eradication. N Engl J
Med 362(25):2346–2349
25. Heymann DL, Sutter RW, Aylward RB (2006) Polio eradication:
interrupting transmission, towards a polio-free world. Future
Virol 1(2):181–188
26. Estıvariz CF, Molnar Z, Venczel L et al (2011) Paralytic polio-
myelitis associated with sabin monovalent and bivalent oral polio
vaccines in Hungary. Am J Epidemiol 174(3):316–325
27. Ehrenfeld E, Modlin J, Chumakov K (2009) Future of polio
vaccines. Expert Rev Vaccines 8(7):899–905
28. Vashishtha VM, Kalra A, Jacob John T et al (2010) Recom-
mendations of national consultative meeting on polio eradication,
2010; polio eradication committee, Indian academy of pediatrics
(IAP). Indian Pediatr 47(9):749–751
29. Baldwin SL, Fox CB, Pallansch MA et al (2010) Increased
potency of an inactivated trivalent polio vaccine with oil-in-water
emulsions. Vaccine 29(4):644–649
30. Henriksen M (2011) Formulation and development of cationic
liposomes as adjuvants for subunit protein vaccinese. PhD Thesis,
Aston University
31. Bramwell VW, Perrie Y (2005) The rational design of vaccines.
Drug Discov Today 10(22):1527–1534
32. Chumakov K, Ehrenfeld E, Plotkin S (2008) New generation of
inactivated poliovirus vaccines for universal immunization after
eradication of poliomyelitis. Clin Infect Dis 47(12):1587–1592
33. Paul Y (2009) Oral polio vaccines and their role in polio eradi-
cation in India. Exp Rev Vaccines 8(1):35–41
34. Paul Y (2008) OPV cannot eradicate polio from India: do we
need any further evidence? Vaccine 26(17):2058–2061
35. Kidd S (2009) Progress toward poliomyelitis eradication—India,
January 2007-May 2009. Morb Mortal Wkly Rep 58(26):719–723
36. Chandra R (1975) Reduced secretory antibody response to live
attenuated measles and poliovirus vaccines in malnourished
children. Br Med J 2(5971):583–585
37. Paul Y (2009) Why polio has not been eradicated in India despite
many remedial interventions? Vaccine 27(28):3700–3703
38. Savolainen Kopra C, Blomqvist S (2010) Mechanisms of genetic
variation in polioviruses. Rev Med Virol 20(6):358–371
39. Yakovenko ML, Korotkova EA, Ivanova OE et al (2009) Evo-
lution of the Sabin vaccine into pathogenic derivatives without
appreciable changes in antigenic properties: need for improve-
ment of current poliovirus surveillance. J Virol 83(7):3402
40. Thomas ES (2010) Investigating the impact of polio vaccines and
vaccine-derived polioviruses (VDPVs) on the global effort to
eradicate polio. Washington College
41. WHO (2011) Tracking progress toward global polio eradication—
worldwide, 2009–2010. J Am Med Assoc 305(21):2165–2167
42. Kew O (2006) What role for inactivated poliovirus vaccine in the
eradication endgame? J Infect Dis 193(10):1341–1343
43. Doshi SJ, Sandhu HS, Venczel LV et al (2011) Poliomyelitis-
related case-fatality ratio in India, 2002–2006. Clin Infect Dis
53(1):13–19
44. Zhou W, Pool V, Iskander JK et al (2003) Surveillance for safety
after immunization: vaccine adverse event reporting system
(VAERS)—United States, 1991–2001. MMWR Surveill Summ
52(1):1–24
45. Chezzi C, Dommann C, Blackburn N et al (1998) Genetic sta-
bility of oral polio vaccine prepared on primary monkey kidney
cells or Vero cells—effects of passage in cell culture and the
human gastrointestinal tract. Vaccine 16(20):2031–2038
46. Horie H, Miyazawa M, Ota Y et al (2001) Analysis of the
accumulation of mutants in Sabin attenuated polio vaccine viru-
ses passaged in Vero cells. Vaccine 19(11–12):1456–1459
47. Asia UNS (2003) A critical leap to polio eradication in India.
Kathmandu: United Nations Children’s Fund Regional Office for
South Asia. 1–84
48. Furesz J (2006) Developments in the production and quality
control of poliovirus vaccines—historical perspectives. Biologi-
cals 34(2):87–90
49. Salk J (1979) Immunization against poliomyelitis: risk/benefit/
cost in a changing context. Dev Biol Stand 43:151–157
50. Lewis JA (2011) Production of polio virus at high titers for
vaccine production. WO Patent WO/2011/006,823
51. Prevots D, Burr R, Sutter R, Murphy T (2000) Advisory committee
on immunization practices. Poliomyelitis prevention in the United
States. Updated recommendations of the Advisory Committee on
Immunization Practices (ACIP). MMWR Recomm Rep 49:1–22
52. Neutra MR, Kozlowski PA (2006) Mucosal vaccines: the promise
and the challenge. Nat Rev Immunol 6(2):148–158
53. Finn A, Bell F (1998) Polio vaccine: is it time for a change? Arch
Dis Child 78(6):571–574
54. Dayan GH, Thorley M, Yamamura Y et al (2007) Serologic
response to inactivated poliovirus vaccine: a randomized clinical
trial comparing 2 vaccination schedules in Puerto Rico. J Infect
Dis 195(1):12–20
55. Modlin JF, Halsey NA, Thoms ML et al (1997) Humoral and
mucosal immunity in infants induced by three sequential inacti-
vated poliovirus vaccine-live attenuated oral poliovirus vaccine
immunization schedules. J Infect Dis 175(1):S228–S2234
56. Resik S, Tejeda A, Mas Lago P et al (2010) Randomized con-
trolled clinical trial of fractional doses of inactivated poliovirus
132 Proc. Natl. Acad. Sci. Sect B. Biol. Sci. (January–March 2012) 82(1):123–133
123

vaccine administered intradermally by needle-free device in
Cuba. J Infect Dis 201(9):1344–1352
57. Mohammed AJ, AlAwaidy S, Bawikar S et al (2010) Fractional
doses of inactivated poliovirus vaccine in Oman. N Engl J Med
362(25):2351–2359
58. Hickling J, Jones K, Friede M et al (2011) Intradermal delivery of
vaccines: potential benefits and current challenges. Bull World
Health Organ 89(3):221–226
59. Vashishtha VM, Kalra A, John TJ et al (2010) Recommendations
of national consultative meeting on polio eradication, 2010; polio
eradication committee, Indian academy of pediatrics (IAP).
Indian Pediatr 47:749–751
60. Semler BL (2004) Poliovirus proves IRES-istible in vivo. J Clin
Invest 113(12):1678–1680
Proc. Natl. Acad. Sci. Sect B. Biol. Sci. (January–March 2012) 82(1):123–133 133
123