Embed Size (px)
Citation preview

Polypharmacy and Polymorbid
Patients: Practical Tips and Tricks
November 2, 2013

Faculty/Presenter Disclosure
Faculty: Chris Fan-Lun, BScPhm, ACPR, CGP Pharmacist - Geriatric Medicine
Clinical Practice Leader - Dept. of Pharmacy Services,Mount Sinai Hospital
Relationships with commercial interests: I have NO actual or potential conflicts of interest in relation to this
program

Objectives
• Highlight common polypharmacy issues in
patients with multimorbidity
• Review the physiologic changes of aging and
pharmacological basis for these concerns
• Provide practical tips to address polypharmacy
in polymorbid patients

Polypharmacy in the Elderly
Polypharmacy means
"many drugs“ • 5 or more drugs
The use of more
medication than is
clinically indicated
or warranted

Barnett K et al. Lancet 2012; 380 (9836):37 – 43.


Polypharmacy Consequences
Adverse Drug Reactions
Nonadherence
Drug costs
Poor quality of life, outcomes
Magaziner J et al. J Aging Health. 1989;1:470-484.
Espino DV et al. J Gerontol A Biol Sci Med Sci. 2006;61:170-175.

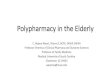
Percentage of seniors with polypharmacy, by number of chronic
conditions and age group
Reason B et al. Fam Pract 2012;29(4):427-432.

Percentage of seniors who experienced a side effect requiring medical
attention within the past 12 months, by number of prescription
medications
Reason B et al. Fam Pract 2012;29(4):427-432.

Canadian Impact
• Seniors with three or more reported chronic conditions accounted
for 40% of reported health care use among seniors, even though
they comprised only 24% of all seniors
• Seniors who reported ≥3chronic conditions were taking an average
of 6 Rx meds, twice as many medications as seniors with only 1
chronic condition
• Seniors taking a high number of prescription medications were at a
greater risk of experiencing side effects requiring medical
attention, yet fewer than half of seniors with chronic conditions
reported having medication reviews
Seniors and the Health Care System: What Is the Impact of Multiple
Chronic Conditions?. CIHI 2011

Adverse Drug Effects &
Prescribing Cascade
Drug 1
ADE interpreted as new
medical condition
Drug 2
ADE interpreted as new
medical condition
Drug 3
Rochon PA, Gurwitz JH. BMJ 1997;315:1097.

Case: Ms Dale
84 yo woman
• widowed, living alone
• severe knee pain
limiting mobility
• 3 falls in last 6
months
• “memory problems”
PMHx
A Fib
HTN
OA

Case: Ms Dale
• EC ASA 81 mg daily
• Ibuprofen 400 mg bid
• GRAVOL 50 mg qhs
• Zopiclone 3.75 mg qhs
• Warfarin as directed
• Amlodipine 10 mg daily
• Perindopril 4 mg daily
• Furosemide 40 mg bid
• Metoprolol 50mg bid
• Slow-K 16 mEq daily
• Atorvastatin 40 mg daily
• Dextromethophan syrup
• Pantoprazole 40 mg daily
• Solifenacin 5 mg daily
• Vitamin B12 1 mg daily
• Glucosamine 1 cap tid

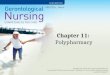
Ms Dale’s Prescribing Cascades
ibuprofen
amlodipine
perindopril
ASA
dimenhydrinate
pantoprazole
furosemide potassium
dextromethorphan
solifenacin
zopiclone
Vitamin B12
Prescribing Web Allegory
Barb Farrell, Pharmacist, Bruyere Geriatric Day Hospital

Prescribing Web Allegory
Barb Farrell, Pharmacist, Bruyere Geriatric Day Hospital
• Dx Afib- metoprolol & warfarin
• Widowed- zopiclone 10 yrs ago
•Knee pain - ibuprofen
•HTN - perindopril
•Cough - DM
•HTN - Amlodipine
•ASA – neighbour said she should take it
5 yrs ago
•Ankle swelling - furosemide
•Hypokalemia - potassium
•Nausea - dimenhydrinate; pantoprazole
•Low Vit B12 - Vit B12 supplement
•Nocturia - solifenacin
1 yr ago

Polypharmacy Risk Factors
• Age
• Multimorbidity
• Acute hospitalization
• Health care visits
• Multiple providers
Hajjar ER, Am J Geriatr Pharmacother. 2007;5(4):345-51 Betteridge TM, et al. Int Med J 2012;42(2):208-11.
Jorgensen T et al. Ann Pharmacother. 2001;35:1004-1009.

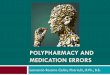
Contributing Factors:
Age-Related Physiological Changes
YOUNG ELDERLY
Drug
absorption Faster
Slower/
decreased
Metabolism Faster Slower
Excretion Faster Slower
Fat : lean body
mass
Total body
water

Contributing Factors:CPGs
• Guidelines = standardise, reduce
unacceptable variation to improve quality
of care
• Treating diseases in isolation
– burdensome and potentially inappropriate
treatment
Barnett K et al. Lancet 2012; 380 (9836):37 – 43.

Contributing Factors:CPGs
• A hypothetical case – elderly woman with COPD, DM II, OP, HTN, and OA
• If all CPGs are followed… – 12 medications, costing $406 (US)/month
– Undesirable effects, drug-disease and drug-drug interactions
• Limited applicability to elderly with multimorbidity and medications
• May have sections for special populations
• Frail elderly and >80yo underrepresented in CPGs and clinical trials
Boyd CM et al. JAMA. 2005;294(6):716-24.
Cox L. CFP 2011;57(7):e263 –e269.
Lugtenberg M et al. PLoS One 2011;6:e25987

CPGs and the elderly
Age + Polymorbidity + CPGs
= Lots of medications


Screening and Assessment Tools


START & STOPP
STOPP – Screening Tool of Older Person’s Prescriptions
• inappropriate combinations of medicines and disease
START – Screening Tool to Alert doctors to Right Treatment
• a set of recommended treatments for given conditions
Gallagher P, O'Mahony D. Age and Ageing 2008;37:673-9.
Barry PJ, Gallagher P, Ryan C, O'Mahony D. Age and Ageing 2007;36:632-8.

Avoiding Polypharmacy Pitfalls
1. Obtain accurate history
2. Link medications to disease state
3. Identify prescribing cascade
4. Initiate interventions to ensure adherence
5. Reconcile medications upon discharge from
acute care or rehabilitation facility
6. Medication review

Reducing Drug-Related
Iatrogenesis in the Elderly
• Start low, go slow
• Limit medication changes
• Avoid “high risk” meds
• Understand the pharmacokinetics and pharmacodynamics of drugs prescribed
– renal/hepatic dosing as needed
• Early recognition of problems as med side effect

Stopping Medications
Medication streamlining
Deprescribing
Pharmaceutical debridement
Drugectomy
Rocking the Boat

How to Stop?
Reduce or stop one medication at a time
Start with medications where there is:
• Risk of harm with no known benefit
• Little chance drug withdrawal
• Unclear or no indication
• Indication but unknown or minimal benefit
• Benefit but side effect or safety issues

Deprescribing: Monitoring
Hardy JE, Hilmer SN. J Pharm Pract Res 2011;41:146-51

Summary
Decreasing medication use in elderly can:
– Adverse events (eg falls, hospitalization)
– Pill burden and costs
– Adherence with remaining medications
– QOL
Team approach
Take one step at a time
– Review medications regularly
– Develop a plan for rationale
prescribing/deprescribing


Question 1
Which of the following age-related
changes has implications on drug
distribution and duration of action? a) Increased hepatic drug metabolism
b) Increased percentage of body fat
c) Increased amount of total body water
d) All of the above

Question 2
An 84 yo woman began showing symptoms of memory problems and
was referred to a neurologist. She was diagnosed w/ Alzheimer’s
disease and initiated on donepezil. Six weeks later, the patient made
an appointment with her primary physician to ask for an “overactive
bladder” medicine that she saw advertised on TV. She was then
prescribed darifenacin. This may be a case of:
a) Drug interaction
b) Adverse drug event
c) Prescribing cascade
d) Geriatric syndrome

Question 3
Which of the following drugs can
be stopped without tapering
a) Citalopram
b) Docusate
c) Bisoprolol
d) Lorazepam