Embed Size (px)
Citation preview
Pooled Analysis of IMS III and MR CLEAN Trials
NIHSS ≥ 20Joseph P. Broderick, Diederik W. Dippel, Yuko Y.
Palesch, Aad van der Lugt, Thomas A. Tomsick, Wimvan Zwam, Andrew M. Demchuk, Robert J van
Oostenbrugge, Pooja Khatri, Charles B. Majoie, Lydia D. Foster, Yvo BWEM Roos, For the IMS III and MR
CLEAN Trial Investigators
IMS III: NINDS U01-NS05220, NS054630. Clinicaltrial.gov ID number : 0359424MR CLEAN: Dutch Heart Foundation. Current Controlled Trials Number: ISRCTN10888758
Financial Disclosures • Study medication for IMS III from Genentech.
EKOS, Concentric, and Codman supplied catheters for first several years of IMS III.
• MR CLEAN: Nominal restricted grants from: AngioCare BV, Covidien/EV3®, MEDAC Gmbh/LAMEPRO, Penumbra Inc.,TopMedical/Concentric
• Research monies from Genentech for PRISMS Trial – Executive Committee – Dr. Broderick
Background
• IMS III Trial was stopped for overall futility but there was evidence of potential benefit in subgroups of patients (NIHSS ≥ 20, major arterial occlusions on pre-treatment CTA, and ICA occlusions).
• Prior to unblinding of MR CLEAN, these subgroups of patients were defined in late spring of 2014 as targets for pooled analyses of IMS III and MR CLEAN.
• MR CLEAN published results in NEJM in December after which the pooled analyses were begun.
Study Design• Pooled analyses included all subjects of both trials treated with
IV t-PA within 3 hours of onset with an NIHSS ≥ 20. • We performed a pooled analysis using all IMS III patients with an
NIHSS ≥ 20 just prior to treatment with IV t-PA• Because MR CLEAN defined NIHSS at time of randomization
(often several hours after start of IV t-PA), we also performed an exploratory pooled analysis using those subjects in IMS III who had an NIHSS ≥ 20 at 40 minutes after start of IV t-PA to better approximate the MR CLEAN study population.
Study Design• Primary analysis: Logistic ordinal regression model with pre-
specified covariates (NIHSS, age, previous stroke, diabetes, atrial fibrillation and carotid terminus occlusion) PLUS the study ID (1= IMS III; 0= MR CLEAN)
• Secondary analysis: Logistic regression as above but on the DICHOTOMIZED (0-2 vs 3-6) mRS at 90 days.
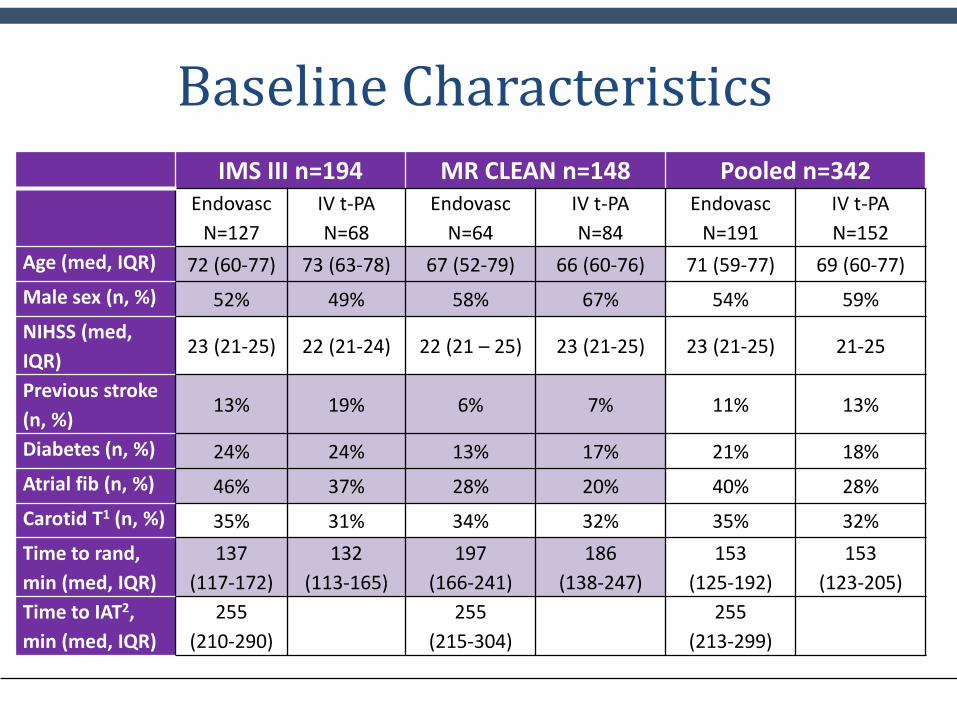
Baseline CharacteristicsIMS III n=194 MR CLEAN n=148 Pooled n=342
EndovascN=127
IV t-PAN=68
EndovascN=64
IV t-PAN=84
EndovascN=191
IV t-PAN=152
Age (med, IQR) 72 (60-77) 73 (63-78) 67 (52-79) 66 (60-76) 71 (59-77) 69 (60-77)Male sex (n, %) 52% 49% 58% 67% 54% 59%NIHSS (med, IQR)
23 (21-25) 22 (21-24) 22 (21 – 25) 23 (21-25) 23 (21-25) 21-25
Previous stroke (n, %)
13% 19% 6% 7% 11% 13%
Diabetes (n, %) 24% 24% 13% 17% 21% 18%Atrial fib (n, %) 46% 37% 28% 20% 40% 28%Carotid T1 (n, %) 35% 31% 34% 32% 35% 32%Time to rand, min (med, IQR)
137 (117-172)
132 (113-165)
197 (166-241)
186 (138-247)
153 (125-192)
153 (123-205)
Time to IAT2, min (med, IQR)
255 (210-290)
255 (215-304)
255 (213-299)
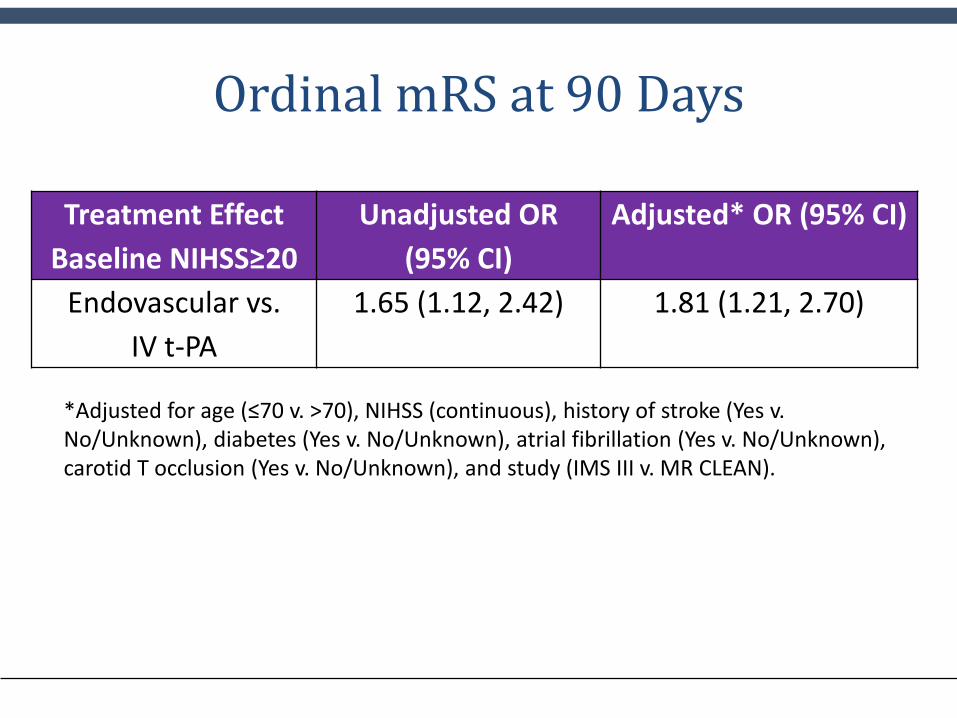
Ordinal mRS at 90 Days
Treatment Effect Baseline NIHSS≥20
Unadjusted OR (95% CI)
Adjusted* OR (95% CI)
Endovascular vs. IV t-PA
1.65 (1.12, 2.42) 1.81 (1.21, 2.70)
*Adjusted for age (≤70 v. >70), NIHSS (continuous), history of stroke (Yes v. No/Unknown), diabetes (Yes v. No/Unknown), atrial fibrillation (Yes v. No/Unknown), carotid T occlusion (Yes v. No/Unknown), and study (IMS III v. MR CLEAN).
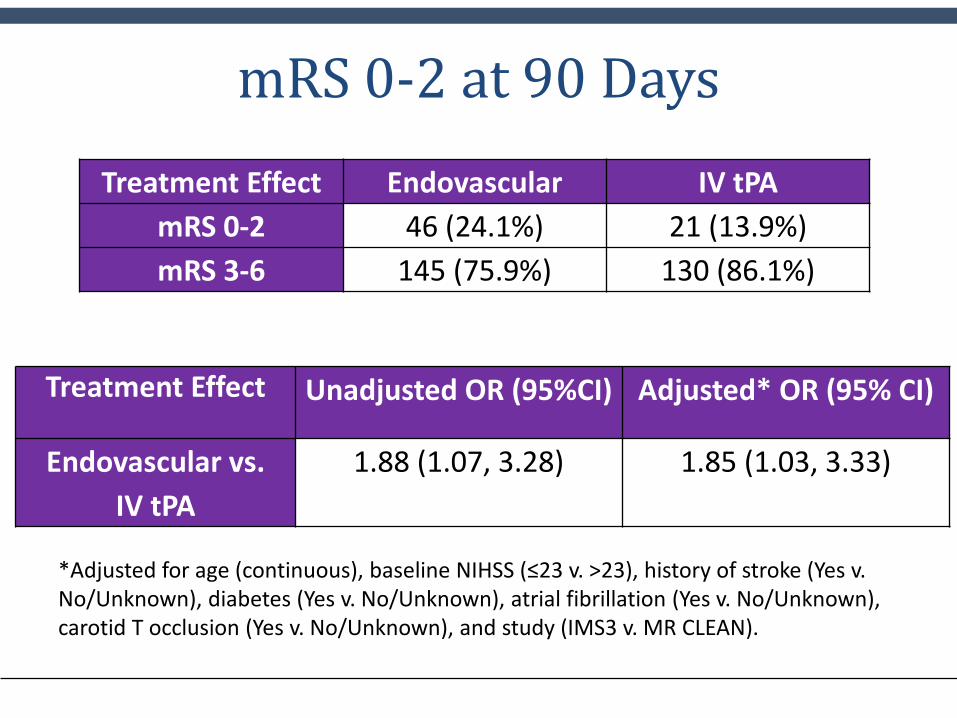
mRS 0-2 at 90 Days
*Adjusted for age (continuous), baseline NIHSS (≤23 v. >23), history of stroke (Yes v. No/Unknown), diabetes (Yes v. No/Unknown), atrial fibrillation (Yes v. No/Unknown), carotid T occlusion (Yes v. No/Unknown), and study (IMS3 v. MR CLEAN).
Treatment Effect Endovascular IV tPAmRS 0-2 46 (24.1%) 21 (13.9%)mRS 3-6 145 (75.9%) 130 (86.1%)
Treatment Effect Unadjusted OR (95%CI) Adjusted* OR (95% CI)
Endovascular vs.IV tPA
1.88 (1.07, 3.28) 1.85 (1.03, 3.33)
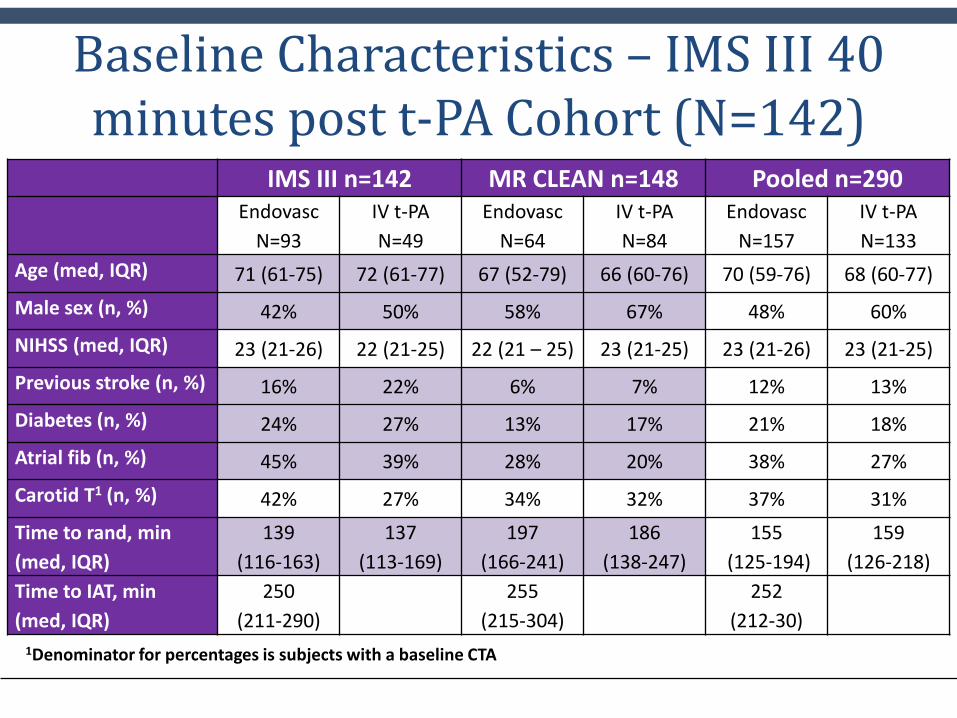
Baseline Characteristics – IMS III 40 minutes post t-PA Cohort (N=142)
IMS III n=142 MR CLEAN n=148 Pooled n=290Endovasc
N=93IV t-PAN=49
EndovascN=64
IV t-PAN=84
EndovascN=157
IV t-PAN=133
Age (med, IQR) 71 (61-75) 72 (61-77) 67 (52-79) 66 (60-76) 70 (59-76) 68 (60-77)Male sex (n, %) 42% 50% 58% 67% 48% 60%NIHSS (med, IQR) 23 (21-26) 22 (21-25) 22 (21 – 25) 23 (21-25) 23 (21-26) 23 (21-25)Previous stroke (n, %) 16% 22% 6% 7% 12% 13%Diabetes (n, %) 24% 27% 13% 17% 21% 18%Atrial fib (n, %) 45% 39% 28% 20% 38% 27%Carotid T1 (n, %) 42% 27% 34% 32% 37% 31%Time to rand, min (med, IQR)
139(116-163)
137 (113-169)
197 (166-241)
186 (138-247)
155(125-194)
159 (126-218)
Time to IAT, min (med, IQR)
250 (211-290)
255 (215-304)
252 (212-30)
1Denominator for percentages is subjects with a baseline CTA
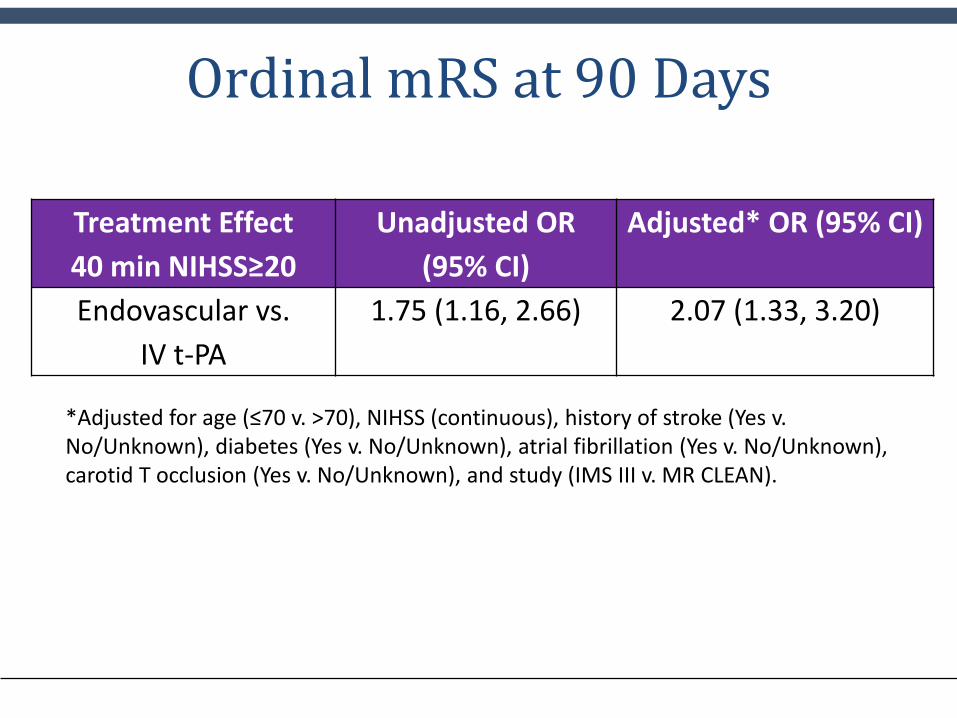
Ordinal mRS at 90 Days
Treatment Effect 40 min NIHSS≥20
Unadjusted OR (95% CI)
Adjusted* OR (95% CI)
Endovascular vs. IV t-PA
1.75 (1.16, 2.66) 2.07 (1.33, 3.20)
*Adjusted for age (≤70 v. >70), NIHSS (continuous), history of stroke (Yes v. No/Unknown), diabetes (Yes v. No/Unknown), atrial fibrillation (Yes v. No/Unknown), carotid T occlusion (Yes v. No/Unknown), and study (IMS III v. MR CLEAN).
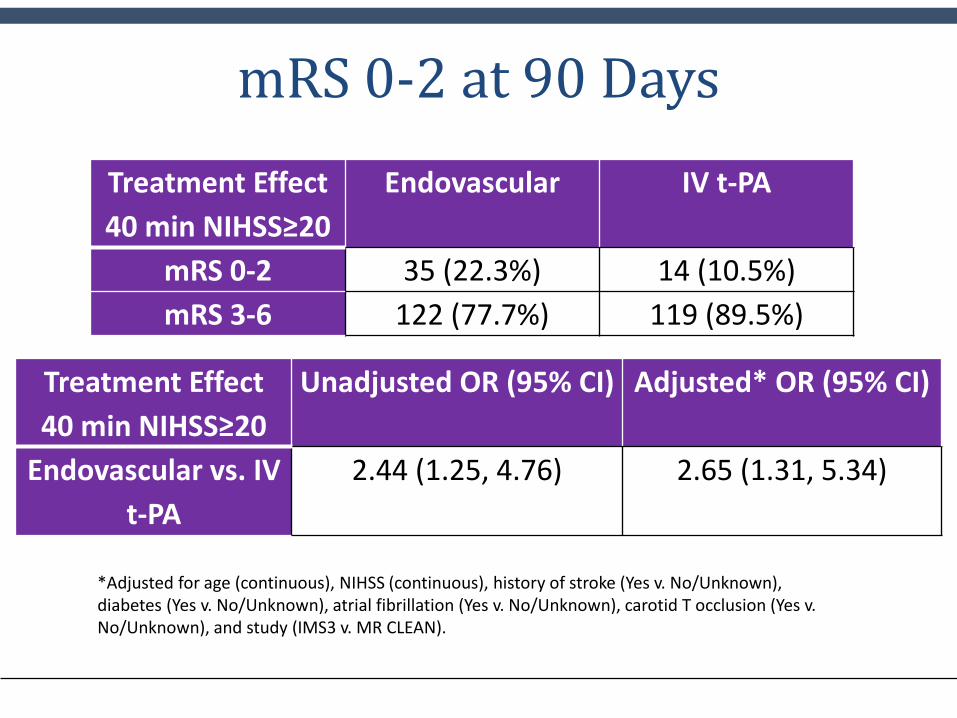
mRS 0-2 at 90 DaysTreatment Effect 40 min NIHSS≥20
Endovascular IV t-PA
mRS 0-2 35 (22.3%) 14 (10.5%)mRS 3-6 122 (77.7%) 119 (89.5%)
Treatment Effect 40 min NIHSS≥20
Unadjusted OR (95% CI) Adjusted* OR (95% CI)
Endovascular vs. IV t-PA
2.44 (1.25, 4.76) 2.65 (1.31, 5.34)
*Adjusted for age (continuous), NIHSS (continuous), history of stroke (Yes v. No/Unknown), diabetes (Yes v. No/Unknown), atrial fibrillation (Yes v. No/Unknown), carotid T occlusion (Yes v. No/Unknown), and study (IMS3 v. MR CLEAN).
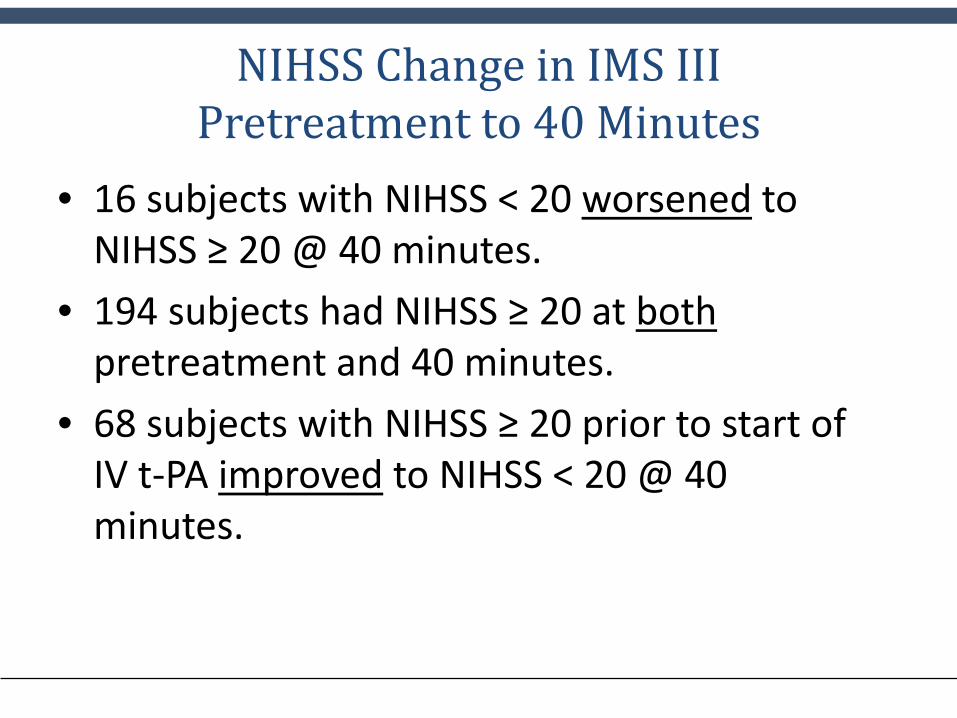
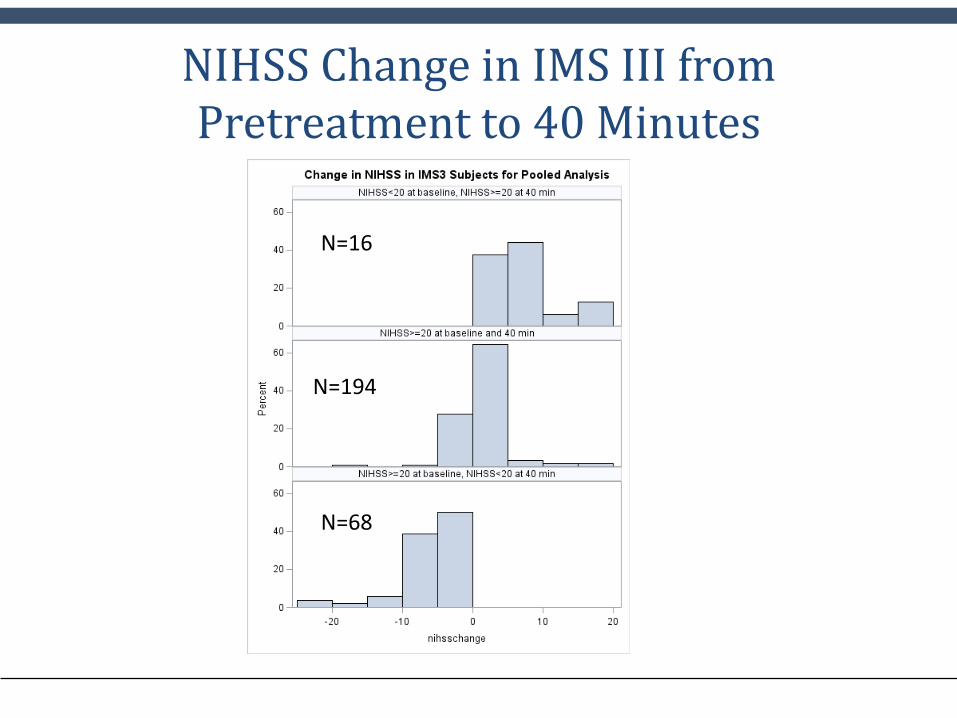
NIHSS Change in IMS IIIPretreatment to 40 Minutes
• 16 subjects with NIHSS < 20 worsened to NIHSS ≥ 20 @ 40 minutes.
• 194 subjects had NIHSS ≥ 20 at bothpretreatment and 40 minutes.
• 68 subjects with NIHSS ≥ 20 prior to start of IV t-PA improved to NIHSS < 20 @ 40 minutes.
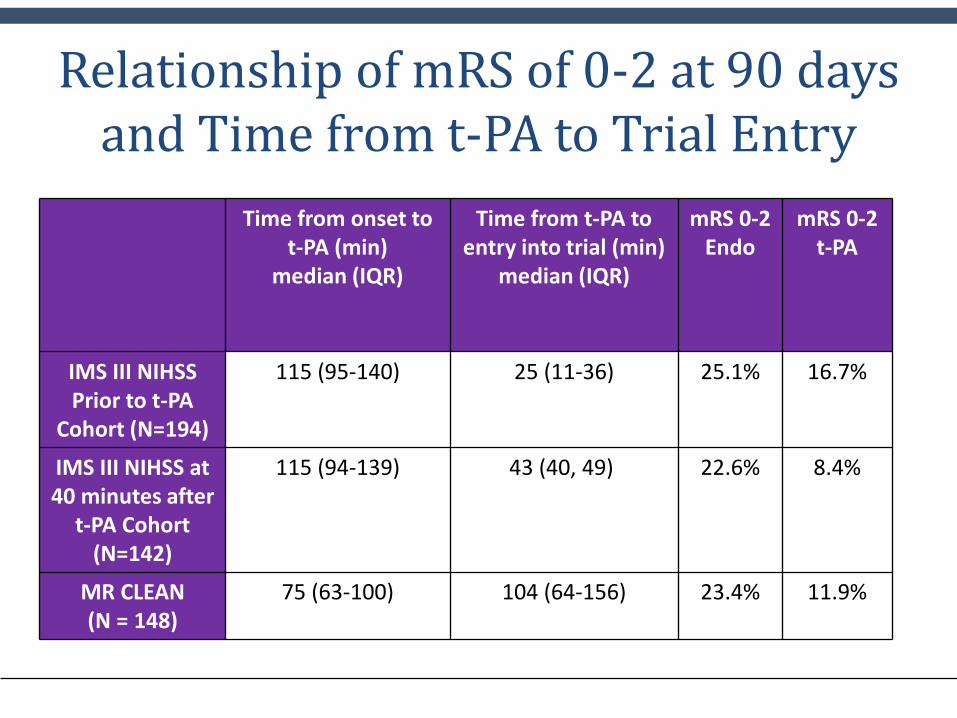
Relationship of mRS of 0-2 at 90 days and Time from t-PA to Trial Entry
Time from onset to t-PA (min)
median (IQR)
Time from t-PA to entry into trial (min)
median (IQR)
mRS 0-2Endo
mRS 0-2t-PA
IMS III NIHSSPrior to t-PA
Cohort (N=194)
115 (95-140) 25 (11-36) 25.1% 16.7%
IMS III NIHSS at 40 minutes after
t-PA Cohort(N=142)
115 (94-139) 43 (40, 49) 22.6% 8.4%
MR CLEAN(N = 148)
75 (63-100) 104 (64-156) 23.4% 11.9%
CONCLUSIONS1) For patients with severe stroke (NIHSS≥20),
endovascular therapy after IV t-PA improves functional outcome at 90 days (about 1 in 4 subjects functionally independent) as compared to IV t-PA alone (about 1 in 10),with no increase in mortality.
2) In the IMS III subgroup with an NIHSS ≥ 20 pretreatment, IV t-PA was associated with improvement in the NIHSS to NIHSS <20 in about 1/3 of patients during the first 40 minutes.
CONCLUSIONS
3) Our pooled data, as well as other reported trials, call for thoughtful consideration of current triage for patients who present with severe stroke and who are candidates for endovascular therapy within a given region.
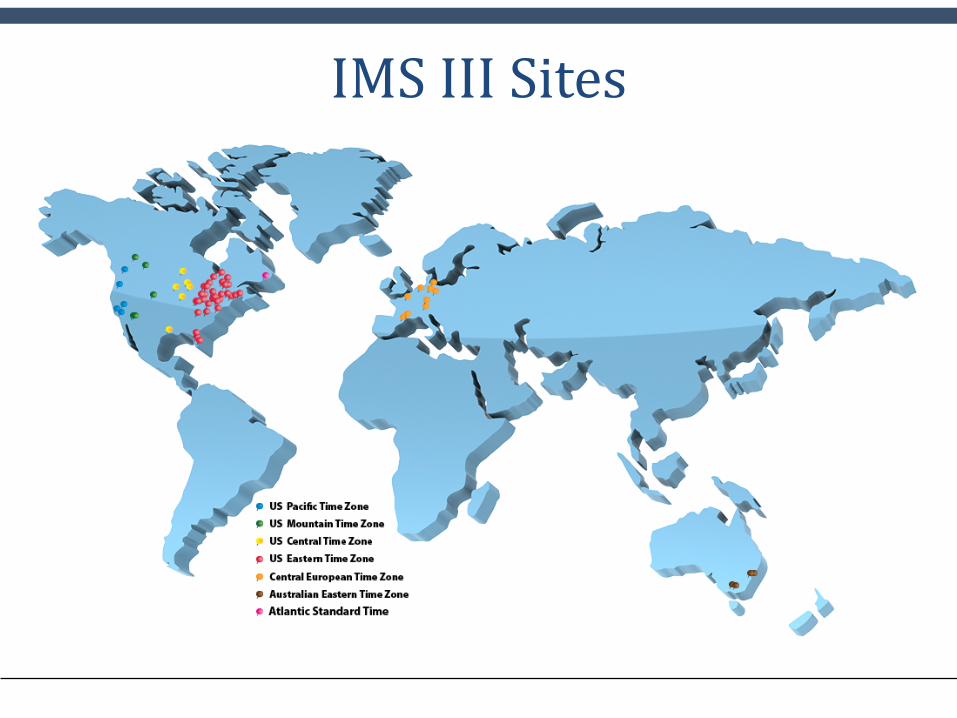
IMS III Sites
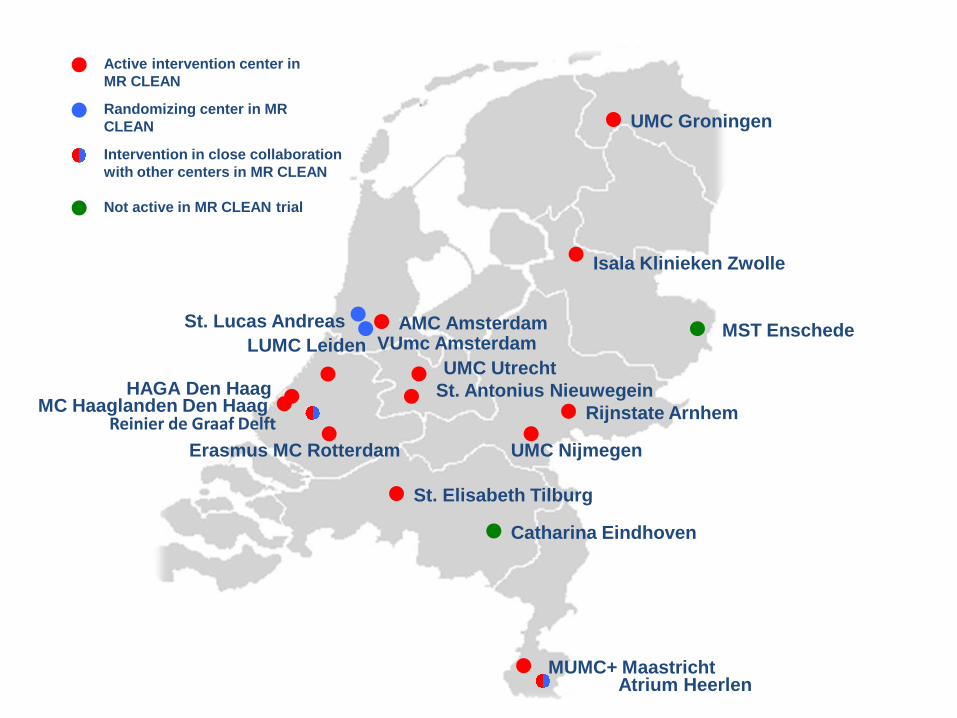
UMC Groningen
Isala Klinieken Zwolle
AMC Amsterdam
UMC UtrechtSt. Antonius Nieuwegein
Rijnstate Arnhem
UMC Nijmegen
LUMC Leiden
HAGA Den HaagMC Haaglanden Den Haag
Erasmus MC Rotterdam
St. Elisabeth Tilburg
Catharina Eindhoven
MUMC+ Maastricht
VUmc Amsterdam
Atrium Heerlen
MST Enschede
Active intervention center in MR CLEAN
Randomizing center in MR CLEAN
Intervention in close collaboration with other centers in MR CLEAN
Not active in MR CLEAN trial
Reinier de Graaf Delft
St. Lucas Andreas

Extra slides
NIHSS Change in IMS III from Pretreatment to 40 Minutes
N=16
N=194
N=68
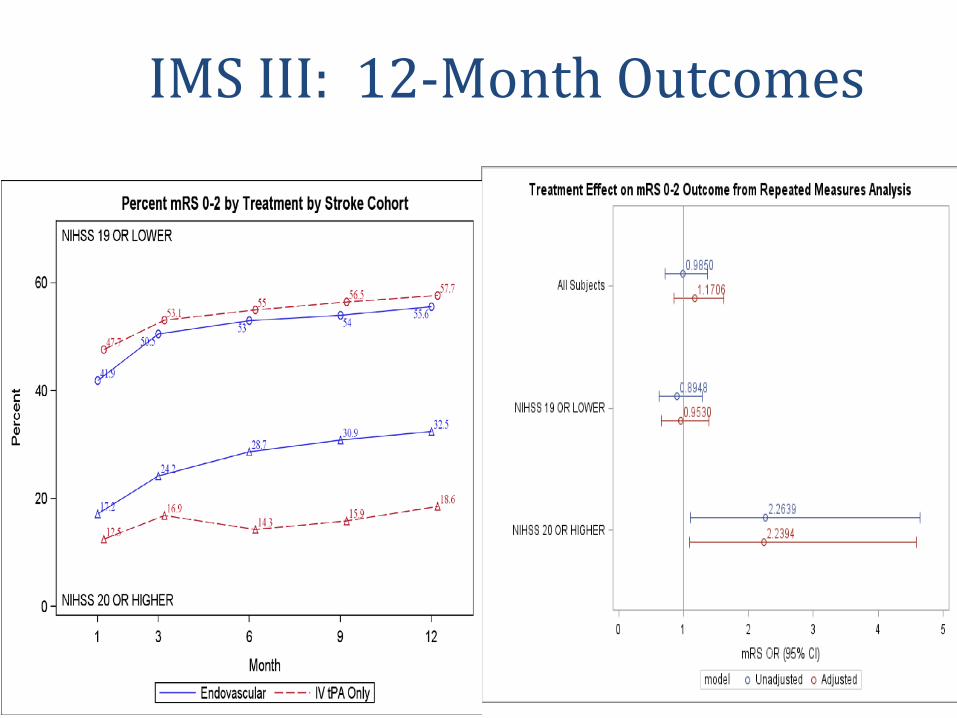
IMS III: 12-Month Outcomes
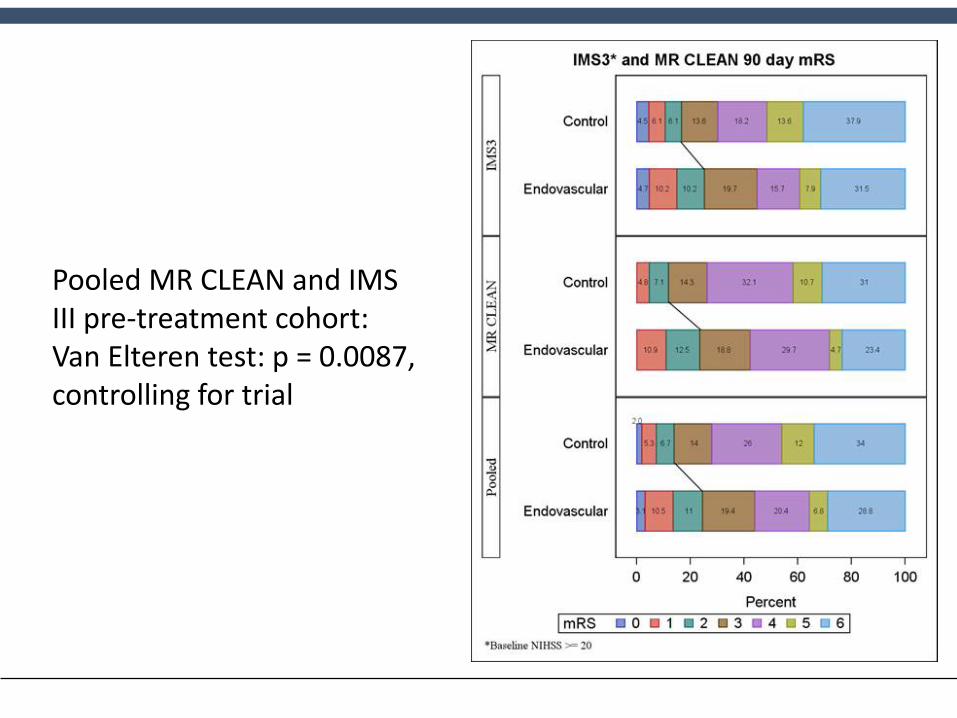
Pooled MR CLEAN and IMS III pre-treatment cohort: Van Elteren test: p = 0.0087, controlling for trial
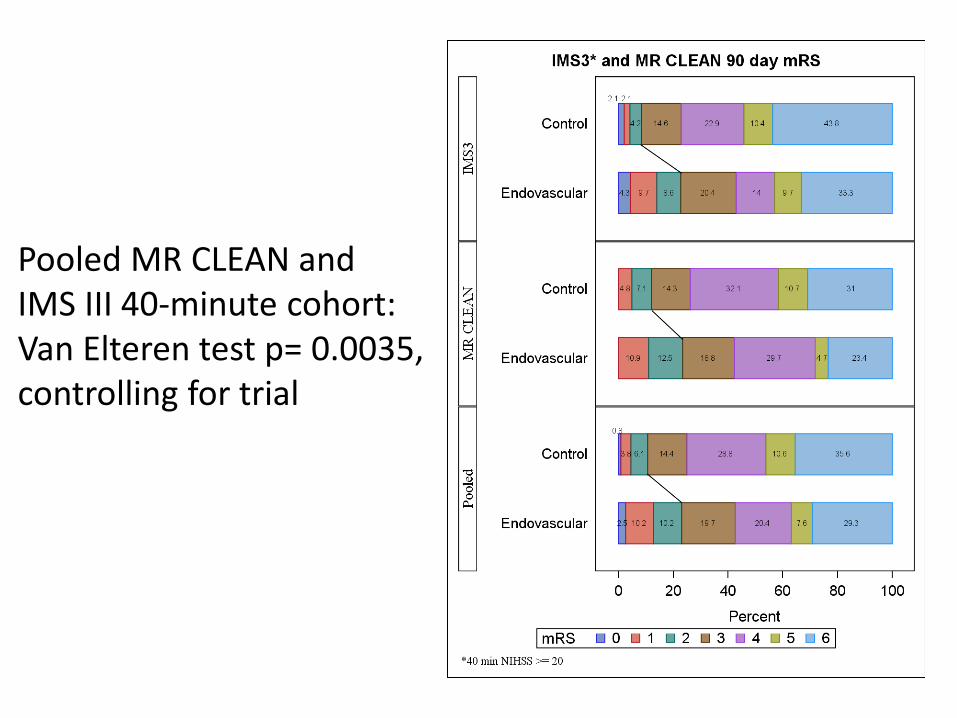
Pooled MR CLEAN and IMS III 40-minute cohort: Van Elteren test p= 0.0035, controlling for trial
IMS III SupportGRANT SUPPORT:
NIH/NINDS Grant Numbers: UC U01NS052220
MUSC U01NS054630 and U01NS077304.
FDA IND: #5785Study Drug: Genentech,Inc.
Microcatheters: EKOS Corp., Concentric Inc., CordisNeurovascular, Inc.
ENROLLING CLINICAL CENTERS:• University of Cincinnati College of Medicine (72 subjects) J. Broderick, T. Tomsick;• University of Pittsburgh Medical Center (46) L Wechsler, T. Jovin;• Calgary Health Region/Foothills Medical Centre (44) A. Demchuk, M. Goyal;• Toronto Western Hospital (29) F. Silver, K. Murphy;• Hospital Vall d'Hebron (28) C. Molina, M. Ribo;• Royal Melbourne Hospital (27) B. Yan, P. Mitchell;• Mayo Clinic Arizona (26) B. Demaerschalk, B. Chong;• Oregon Health Sciences University, Oregon Stroke Center (24 ) W. Clark, S. Barnwell;• Riverside Methodist Hospital (24) R. Budzik;• Alexian Brothers Hospital Network (23) T. Malisch;• Froedtert Hospital/ Medical College of Wisconsin (23) O.Zaidat;• Colorado Neurological Institute/Swedish Medical Center (21) C. Fanale, D. Frei;• Allegheny General Hospital (18) A. Tayal, A. Ku;• Dresden University of Technology (17), U. Bodechtel, R. von Kummer;• Ruan Neurology /Mercy Medical Center, (16) M Jacoby, W. Young;• Lehigh Valley Hospital (15) Y. Isayev, D. Shaff;• UCLA Medical Center (14) S. Starkman, F. Vinuela;• University of Louisville (11) A. Abou-Chebl;• Martin Luther University (10) K. Wartenberg, K. Stock;• Royal Prince Alfred Hospital (10) C. Anderson, G. Parker;• Abington Memorial Hospital (9) Q. Shah;• Vancouver General Hospital (9) A. Woolfenden, G. Redekop;• Henry Ford Hospital (8) C. Lewandowski, W. Sanders;• University of Virginia Health System (8) E. Clarke Haley, A. Evans;• Washington University (8) P. Panagos, C. Derdeyn;• Hoag Memorial Hospital Presbyterian (7) D. Brown, M. Brandt-Zawadzki;• Morton Plant Mease Health Care (7) A. Arora, E. Lopez De Valle;• PENN State M.S. Hershey Medical Center (7) K. Cockroft;
• University of Miami Miller School of Medicine/Jackson Memorial Hospital (7) D. Yavagal; • Lahey Clinic Medical Center (6) In Sup Choi; • Mission Hospitals/Mission Neurology Services (6) A. Schneider, J. Short; • Monash Medical Centre (6)T. Phan, W. Chong; • University of North Carolina (5) D. Huang, S. Solander; • University of Texas Medical School at Houston (5), J. Grotta, P. Chen; • Upstate Medical University (5) Z. El Zammar, E. Deshaies; • Bichat Stroke Centre and Paris Diderot University (4) P. Amarenco, M. Mazighi;,• Medical University of South Carolina (4) E. Jauch, A.Turk; • Ottawa Hospital-Civic Campus (4) G. Stotts, C. Lum; • Park Nicollet Institute (4) S. Hanson, M. Madison; • Trillium Health Care (4) D. Selchen, D. Rosso; • Chattanooga Ctr. for Neurological Res (3) T. Delvin, B. Baxter; • Jewish Hospital Louisville (3) J. Gebel, R. Paulson; • Nevada Neuroscience Institute Research Foundation (3) S. Selco, L. Blake;• St. Antonius Hospital (3) W. Schonewille, JA. Vos; • Stroke Center at Hartford (3) L. Abbott, G. Spiegel; • University of Montreal Notre Dame Hospital (3) A. Poppe, J. Raymond;• Barrow Neurology Clinics at St. Joseph’s Hospital and Med. Ctr. (2), J. Frey, F. Albuquerque; • Cleveland Clinic (2) D. Krieger, T. Masaryk; • Michigan State University Sparrow Hospital (2), S. Hussain; • Sunnybrook Health Sciences Centre (2) R. Swartz, P. Howard; • University Hospitals Case Medical Center (2) R. Tarr; • Rhode Island Hospitals (1) P. Panagos, R. Haas; • Hospital Universitari Germans Trias i Pujol (1) A. Davalos, P. Bermejo;• Johns Hopkins University (1) V. Urrutia, M. Radvany;• Massachusetts General Hospital (1) L. Schwamm, R. Nogueira; • St. Vincent’s Hospital (1) R. Markus, R. Parkinson; • University Medical Center at Brackenridge & Seton Medical Center (1) J. Neal Rutledge; • William Beaumont Hospital (1) C. Kazmierczak.
COORPORATE PARTNERS: • Genentech, Inc., • Codman Neurovascular (a business unit of Codman &
Surtleff, Inc.), • EKOS Corporation, • Concentric Medical Inc. (a wholly owned subsidiary of
Stryker Neurovascular), • Penumbra, Inc, • ev3 Neurovascular (division of Tyco Healthcare Group
d/b/a/ Covidien).
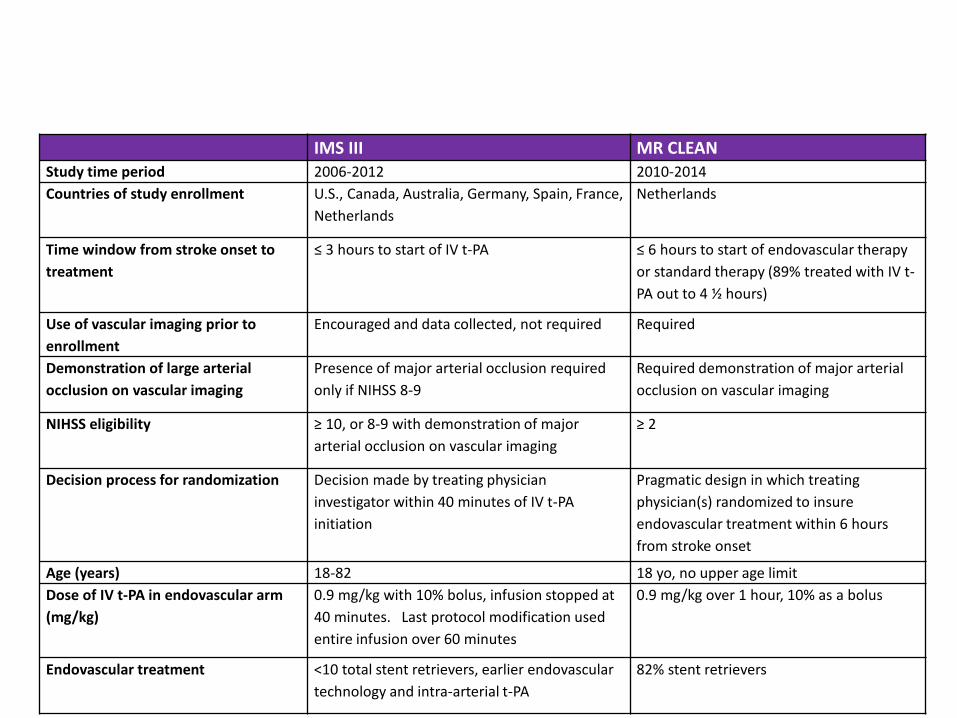
IMS III MR CLEANStudy time period 2006-2012 2010-2014Countries of study enrollment U.S., Canada, Australia, Germany, Spain, France,
NetherlandsNetherlands
Time window from stroke onset to treatment
≤ 3 hours to start of IV t-PA ≤ 6 hours to start of endovascular therapy or standard therapy (89% treated with IV t-PA out to 4 ½ hours)
Use of vascular imaging prior to enrollment
Encouraged and data collected, not required Required
Demonstration of large arterial occlusion on vascular imaging
Presence of major arterial occlusion required only if NIHSS 8-9
Required demonstration of major arterial occlusion on vascular imaging
NIHSS eligibility ≥ 10, or 8-9 with demonstration of major arterial occlusion on vascular imaging
≥ 2
Decision process for randomization Decision made by treating physician investigator within 40 minutes of IV t-PA initiation
Pragmatic design in which treating physician(s) randomized to insure endovascular treatment within 6 hours from stroke onset
Age (years) 18-82 18 yo, no upper age limitDose of IV t-PA in endovascular arm (mg/kg)
0.9 mg/kg with 10% bolus, infusion stopped at 40 minutes. Last protocol modification used entire infusion over 60 minutes
0.9 mg/kg over 1 hour, 10% as a bolus
Endovascular treatment <10 total stent retrievers, earlier endovascular technology and intra-arterial t-PA
82% stent retrievers