Embed Size (px)
Citation preview

PROGRESSIVE GAITWAYS LLC. • 305 Society Drive, Suite C-3 • Telluride, CO USA 81435-8935 (888) 410-8062 • (866) 886-7736 fax • www.gaitways.com • [email protected]
Popliteal Angle? An In-Depth Critique of a Reliability Study
8 July 2016 ten Berge SR, Halbertsma JPK, Maathuis PGM, et al. Reliability of popliteal angle measurement: a study in cerebral palsy patients and healthy controls. J Pediatr Orthop. 2007; 27(6): 648-652. I once reported to an orthopedic surgeon that I found -34 o R1 in testing hamstring muscle length (with the femur vertical) in a child with diplegic CP whom I had seen on a consultation. In my experience, this finding is close to normal for anyone after age 4 years. The surgeon proceeded to lengthen those hamstrings. I was stunned. Later, at a national conference, the same surgeon remarked to me that this same child was not doing as well as he’d hoped post-operatively. I was both saddened and not at all surprised by this news.
I’ve learned that replicable tests of hamstring muscle length can operate like a report card, showing the influences on lower limb muscle and soft tissue extensibility of the child’s balance and motor skills and of implementing management strategies designed to build core postural control in children with pyramidal types of cerebral palsy.
If you know me, then you know that when I find a research project like the one by ten Berge et al (see citation above), I’m excited to see what other clinicians are doing to help us to gain proficiency in the use of assessments of lower limb musculoskeletal status in children with and without CP. Well, this article was disappointing on several counts including the use of inaccurate nomenclature and the rejection by the researchers and their journal editors of the standards of scientific method that demand that a study be published in enough detail that readers could replicate the procedures, challenging and, perhaps, confirming the results and conclusions of the original researchers. In the past 20 years, this scientific reporting standard has disappeared in most of the literature that features clinical assessments and related research. In the study that is the target of this article, we readers are denied a single illustration of the “popliteal angle” procedure that the researchers are evaluating.
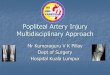
On the use of errant nomenclature, the original popliteal angle test was designed to help neonatologists to determine the gestational age of premature infants, and begins by flexing the test hip until the ipsilateral thigh contacts the abdomen (Fig. 1). Then examiner then lifts the leg to extend the knee to unforced end range and measures the angle formed by the thigh and leg.i
Several researchers have adopted the same name (popliteal angle test) for a different test of hamstring muscle length that features a vertical femur rather than a fully flexed hip.ii, iii In so doing, these clinicians have polluted the literature and the general understanding of this aspect of clinical practice for those of us who work with children. The test performed with the femur vertical was described by Holt in 1965.iv
Fig. 1. The popliteal angle test
The authors assessed 15 nondisabled adults, ages 20 to 29 years (mean age 23.1 years), and 15 children with cerebral palsy (CP), ages 2 to 17 years (mean age 9 years). The group with CP showed GMCS levels spanning II through V – six of them at Levels IV and V. Three of the children had hemiplegia.
Here – in blue – is the authors’ description of their test procedure (p. 649). My comments are inserted in red:
“The patients were in a supine position with a normal resting lordosis. Both hips were fully extended. Full hip extension is probable in the control group, but in this population of children with CP I think it’s improbable that they all showed both a normal lordosis and full hip extension. When the pelvis is tilted anteriorly, the proximal attachment for the hamstrings muscles is displaced posteriorly, adding stretch to the muscles to be tested. I would have set the pelvis with the sacrum flat on the table, flexing the hips as needed to assure comfort in this position.

Popliteal Angle? An In-Depth Critique of a Reliability Study Page 2 © 2016 Progressive GaitWays, LLC
The ipsilateral hip was flexed at 90 degrees. This femoral position is NOT used in the original popliteal angle test. What are the landmarks used in setting this position? How was it measured? Was it maintained through the measurement?
The knee was extended until the next end point of resistance was felt. The “next” end point? Next after what end point? It appears that the three testers made no attempt to standardize their limb handling technique with regard to the speed and force applied to the leg as they raise it. These factors require training as they impact test reliability. If the rate was high and the force was light – merely taking out the slack in the tested soft tissues – then they would have found an R 1 end range, which in my considerable experience, when performed correctly, is very reliable, even when repeated, as no stretch is applied to the tissues.
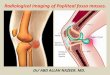
To eliminate possible initial muscle stiffness, Eliminate it? If this “initial stiffness” is R1 end range, this phenomenon is readily detectable in the hamstrings in typically developing children and adults, beginning at age 4 years, v and is more relevant to function and use history than is maximum end range. In fact, this “first catch” in normal lower limb muscles - used for body stabilization and acceleration - is also referred to as “functional” length, vi, vii, viii as it is related to peak isometric contractile force generation on the active length-tension relationship (L1 on Fig. 2).
…the extension of the ipsilateral knee was performed 3 times before taking measurements. ix
Again, how fast and how forcefully? Gajdosik (2001) x explains on page 89: “As the velocity of stretch is increased the viscous behaviors of muscles contribute to increased passive resistance and increased passive elastic stiffness. This rate-dependent response has been demonstrated in animal musclesxi and in human muscles in the absence of stretch induced muscle activations.” xii,xiii
The authors claim, without reporting the test velocity, that repeated tests reduced the measured angle of knee flexion obtained by the third tester. So it seems that they stretched the tissues beyond slack removal, tapping the elastic capacity of soft tissues to gain length under repeated stretches.xiv
When the contralateral hip flexed as a result of the knee extension in the ipsilateral leg, The magnitide of resistance to stretch in the tested tissues should be the focus of attention, rather than the behavior of the contralateral limb, in my opinion. I have found that elevation of the contralateral leg occurs inconsistently across children with CP, and is more likely to occur in those with severe involvement, who show more massed boy responses to specific stimuli, and in those who are lying with the pelvis anteverted. The anteverted pelvis applies more stretch to the hamstring muscles by displacing the ischial tuberosities posteriorly and reducing the reliability of the findings.
I take all tension off of shortened hip flexors by putting a pillow under the thighs, allowing the spine to flatten and the pelvis to rest on the surface. This repositioning also reduces tension on the proximal hamstrings, and standardizes this level of tension across tests and across clients.
If the contralateral thigh still rises with the test, I request that a helper simply keep the contralateral thigh from elevating beyond the supported resting position vs. to push it down to the table surface, which would antevert the pelvis again.
the popliteal angle was visually estimated by the 3 observers (JH, PM, and KM) independently. It seems reasonable to me that all evaluating clinicians cannot be expected to possess the same aptitude for visual estimation of joint angles. Even considering this factor in a reliability study is absurd. Assessment findings are used as clinical evidence of existing soft tissue status and of change after intervention.
Afterwards, with the knee still in the same position, How long had the tester been holding it? Long enough to add length to the test tissues? How did he or she know that the femur was still vertical and that the tension on the hamstrings and surrounding tissues did not change?

Popliteal Angle? An In-Depth Critique of a Reliability Study Page 3 © 2016 Progressive GaitWays, LLC
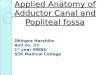
…a blinded goniometer was placed over the joint… The axis hinge of the goniometer was placed on the lateral femoral epicondyle. The legs of the goniometer pointed to the trochanter major and the lateral malleolus.” Who placed the goniometer? The tester? A different person? The goniometer legs “pointed to” the trochanter and malleolus? To where on the trochanter and malleolus were they pointed? The anterior or posterior border? The bisection? I found a photograph of a different researcher using a goniometer for this test (Figure 3) that illustrates the problems with precision in setting the femur vertical and with having to sight the distance between the goniometer end and the landmark. (And the child in Figure 3 has the contralateral hip and knee fully flexed, which might retrovert the pelvis a few more degrees, reducing tension on the hamstring muscles, but which has no functional relevance.)
Fig. 3. Shortfalls of
goniometer use.
ten Berge’s study included 6 of 15 children - >33% - in GMFCS Levels IV and V. They state on p. 651: “Because of their severe handicap, these patients were not able to cooperate very well with the examination (some patients were crying and protesting at the moment of testing, making it difficult to position them on the examination table). To enhance reliability of range-of-motion measurement, correct positioning of patients is essential…Therefore, it is possible that reliability of
popliteal angle measurement will be higher when the patients are more cooperative. ”
I rarely try to measure hamstrings length – or any aspect of ROM - in children who are severely involved when there are stumbling blocks to replicability, such as asymmetrical torso or limb postures, significant hip muscle contractures, known hip subluxation, and/or bony deformities. For these children, I find that filing photographs of the tests is a more useful method of documenting status than obtaining measurements. Since the majority of children with CP fall into GMFCS levels I, II, and III, I would exclude the severely involved children – especially those that could not comply - from participating in a reliability study of a clinical assessment procedure on the bases of common sense and practicality.
Holt et al (2000) xv measured passive resistance to hamstring muscle stretch in six severely involved, nonambulatory children with CP who reportedly accepted stretching of the hamstring muscles. The researchers cited Magnusson et al (1996)xvi as the source for their assessment procedure. They used a Kin-com isokinetic dynamometer with a modified thigh pad to mechanically execute the stretch test at a rate of 5o/second, and to arrive at a predetermined knee angle that seems to me to have occurred at the subject’s maximum tolerated knee extension. They did not assess R1 end range.
I don’t find Holt’s procedural description clear enough to replicate. And once again, there’s not one illustration of the test set-up or of the test position that they measured. While these researchers were able to determine that the extensibility and stiffness of the tested tissues did not change over a period of six weeks, their method is not one that the average pediatric physician or physical therapist clinician can use at this time.
I propose that the failure of ten Berge and others to demonstrate even good interrater reliability for their (misnamed) hamstring length test lies in their repeated inattention to detail and standardization, including:
• Describing the test position as one of normal lumbar lordosis with both hips fully extended (p. 649). (Really? Could this be true of the six children at Levels IV & V?)
• Failing to position the children with the pelvis and lumbar spine flat on the surface to standardize the proximal tension on the hamstring muscles. If this required that the hips be supported in residual flexion, then so be it. This is not a test of hip extension range of motion. Replicable pelvic alignment is key.
• Failing to first train each other in test execution aspects such as rate and force
• Relying on contralateral limb lifting rather than ipsilateral tissue resistance to arrive at the test position
• Failing to landmark the bones in both thigh and leg segments
• Using a goniometer that is too short to reach the landmarks – they might have adapted the lengths of the “legs” on it by taping rulers or telescoping pointers to them.
• Using a goniometer that requires that someone else do the measuring, or that requires one tester to manipulate one-handed while holding the test limb in test position.

Popliteal Angle? An In-Depth Critique of a Reliability Study Page 4 © 2016 Progressive GaitWays, LLC
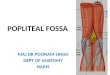
I’d like to suggest a more replicable and clinically relevant way to test the resting or functional length of the hamstring muscle and soft tissues (Figures 4 and 5). I refer to this procedure as the Hamstring Length Test (HLT), and recommend using a small angle finder (AF) with an extendable stick as a measuring tool, holding the stick in the short groove in the AF, such that the AF dial reads zero (0°) at the top when the stick is vertical.
Figures 4a and 4b.
1. With the femur vertical, palpate and mark the center of the greater trochanter
2. Elevate the leg to R1 end range. Palpate and mark the center of the femoral epicondyle the bisections of the fibular head and malleolus.
3. Lower the leg, flexing the knee. 4. With the femur vertical, quickly lift the leg
to R1 end range without force, taking the slack out of the tissues. Hold the leg at R1 end range.
5. Set the AF and stick on the femoral landmarks (shown right) and align the femur at vertical (0°).
Fig. 4a 4b .
Figures 5a and 5b.
Keeping the femur at 0° and the hamstrings at R1 end range, quickly move the AF & stick onto the fibular landmarks.
Read and record the angle formed by the leg and the tangent of the vertical femur (shown right).
As Reimer’s suggests, and I agree, the apparent - as yet unsubstantiated - ideal R1 HLT finding is -30° from age 4 years into adulthood. xvii Fig. 5a. 5b.
We need to gain confidence in our assessment procedures and findings so that we can rely upon them as evidence of management effectiveness (or ineffectiveness), and use them to acquire and publish meaningful normative data, particularly regarding R1 end ranges.
I will gladly train any clinicians – practicing or undergraduate - who are serious about undertaking a reliability study of the R1 the Hamstring Length Test as it is both described here and as I demonstrate it in the instructional DVD: Legs & Feet: A Review of Musculoskeletal Assessments (2015). xviii
Please contact me at [email protected] when you have a proposal for a research project drafted and an advisor on board. I’m no statistician, but I’ll help with collecting references, too.
Let’s all raise the bar!
References i Amiel-Tison C.1968. Neurological evaluation of the maturity of newborn infants. Arch Disease Childhood. 43(227):
89-93. ii Katz K, Rosenthal A, Yosipovitch Z. (1992) Normal ranges of popliteal angle in children. J Pediatr Orthop. 12(2):
229-231. [Another failure to clearly describe the test, so the data acquired is unclear too. These authors evidently stretched past R1 end range, too.]
iii Reade E, Hom L, Hallum A, Lapopolo R. 1984. Changes in popliteal angle measurement in infants up to 1 year of age. Devel Med Child Neurol. 26: 774-780.

Popliteal Angle? An In-Depth Critique of a Reliability Study Page 5 © 2016 Progressive GaitWays, LLC
iv Holt KS. 1965. Assessment of Cerebral Palsy. I. Muscle Function, Locomotion and Hand Function. London: Lloyd-Luke
Medical Books. Cited by Reimers J, 1974. v Maitland GD. 1977. Peripheral Manipulation, second edition, pp.346-347. Boston, MA: Butterworths Company. vi Lieber RL. 2010. Skeletal Muscle Structure, Function, and Plasticity: The Physiological Basis of Rehabilitaiton , 3rd
edition. Philadelphia PA: Wolters Kluwer – Lippincott Williams & Wilkins. vii Reimers J. 1974. Contracture of the hamstrings in spastic cerebral palsy: A study of three methods of operative
correction. Bone Jt J. 56(1): 102-109. viii Lin JP, Brown JK, Walsh EG. 1997. Soleus muscle length, stretch reflex excitability, and the contractile properties of
muscle in children and adults: a study of the functional joint angle. Dev Med Child Neurol 39: 469-480. ix Lissauer T, Clayden G. 1997. Illustrated Textbook of Paediatrics. London, PA: Mosby, Times International Publishers
Limited. Cited by ten Berge SR et al, 2007. x Gajdosik RL. 2001. Passive extensibility of skeletal muscle: review of the literature with clinical implications. Clin
Biomech (Bristol, Avon). 16(2): 87-101. Review. xi Taylor DC, Dayton JD, Seaber AV, Garrett WE. 1990. Viscoelastic properties of muscle-tendon units. The
biomechanical effects of stretching. Am J Sports Med. 18(3): 300-308. Cited by Gajdosik RL. 2001. xii Gajdosik RL. 1997. Influence of age on calf muscle length and passive stiffness variables at different stretch
velocities. Isokinetics Exerc Sci 1997;6:163-174. Cited by Gajdosik RL, 2001. xiii Lamontagne A, Malouin F, Richards CL. 1997. Viscoelastic behavior of plantar flexor muscle-tendon unit at rest. J
Orthop Sports Phys Ther. 26(5): 244-252. xiv Herbert R. 1988. Passive mechanical properties of muscle and their adaptations to altered patterns of use. Austral J
Physiother. 4(3):141-149. xv Holt S, Baagoe S, Lillelund F, Magnusson SP. 2000. Passive resistance of hamstring muscles in children with severe
multiple disabilities? Devel Med Child Neurol. 42(8): 541-544. xvi Magnusson SP, Simonsen EB, Aagaard P, Kjaer M. 1996. Biomechanical responses to repeated stretches in human
hamstring muscle in vivo. Am J Sports Med 24(5): 622-628. Cited by Holt S, 2000. xvii Reimers J. 1992. Clinically based decision making for surgery. In M.D. Sussman (Ed.): The Diplegic Child - Evaluation
and Management 151-161. Rosemont, IL: American Academy of Orthopedic Surgeons. xviii Cusick B. 2015. Legs & Feet: A Review of Musculoskeletal Assessments. www.gaitways.com