Embed Size (px)
Citation preview

180 THE NATIONAL MEDICAL JOURNAL OF INDIA VOL. I, NO.4
•Portal haemodynamics in non-cirrhotic portal fibrosisS. K. SARIN, A. K. SINGAL
ABSTRACTNon-cirrhotic portal fibrosis (NCPF) is a common causeof portal hypertension in India. Haemodynamic studiesindicate that intrasplenic pressure (ISP) and portal veinpressure (PVP) are markedly elevated in patients withportal hypertension. While intravariceal pressure (IVP)truly reflects PVP, intrahepatic pressure (IHP) andwedged hepatic vein pressure (WHVP) underestimate theportal pressure because of the existence of twohaemodynamic gradients, one between ISP and IHP dueto presinusoidal block and the other between IHP andWHVP due to perisinusoidal block. WHVP may be normalor elevated in NCPF, depending on the extent of theperisinusoidal fibrosis. The estimated hepatic blood flow(EHBF) has been shown to be normal or increased, mainlybecause of increased splenic arterial flow. This, however,does not explain the disproportionate splenomegaly seenin NCPF. Both extrahepatic and intrahepatic shunts areseen in NCPF, though intrahepatic shunts are less com-mon in patients with cirrhosis. Further studies arerequired in patients with NCPF to identify primaryhaemodynamic events leading to splenomegaly and thedevelopment of portal hypertension.
BACKGROUNDIn 1889, Banti described patients with splenomegaly andanaemia not caused by a blood disease.' He consideredthe spleen to be the primary seat of the disease, which hecalled 'fibroadenia' of the spleen. Later, Dock and Warthinsuggested that splenomegaly was caused by circulatorychanges, and provided evidence that there was thrombo-phlebitis of the portal vein.i-' In 1962, Ramalingaswamiet al." clearly identified a group of patients with spleno-megaly with non-cirrhotic liver disease. The term 'non-cirrhotic portal fibrosis' (NCPF) was introduced in 1969in a workshop organized by the Indian Council of MedicalResearch.f At the same time, Boyer et at.6in Calcutta andMikkelsen? in Los Angeles coined the terms 'Idiopathicportal hypertension' (IPH) and 'Hepatoportal sclerosis',both describing patients with portal hypertension withoutevidence of cirrhosis.
A disease very similar to NCPF has been reported frommany countries, especially Japan and India. It is found in25% to 30% of all patients with portal hypertensionundergoing surgery or sclerotherapy in India.f-? In the
G.B. Pant Hospital, New Delhi 110002, IndiaS. K. SARIN, A. K. SINGAL Department of Gastroenterology
Correspondence to S. K. SARIN
© The National Medical Journal of India, 1988
West, it constitutes about 3% to 5% of all cases with portalhypertension.IO-12 Initially, NCPF was a diagnosis of ex-clusion but is now accepted to be a separate entity withdistinct clinical, haemodynamic and radiological features.
HAEMODYNAMIC EVALUATION OF PORTALHYPERTENSIONAfter the early work of Thompson et al.13 in 1937, mea-surement of ISP and PVP remained the most importantprocedures for the evaluation of a patient with portalhypertension. Later, a number of other techniques weredeveloped (Fig. 1) to provide additional information onthe aetiology of portal hypertension (Table I).Haemodynamic evaluation of a patient with portal hyper-tension includes: (i) Measurement of pressure in thesplanchnic circulation, (ii) Estimation of splanchnic andcollateral blood flow, (iii) Calculation of haemodynamicgradients.
While the first two measurements indicate the status ofportal hypertension, calculation of haemodynamic gra-dients helps to identify the site and estimate the extent ofvascular resistance to blood flow. On the basis of suchhaemodynamic data, portal hypertension has been classi-fied into the presinusoidal, sinusoidal and postsinusoidaltypes, though the term postsinusoidal is now usedinfrequently.
HAEMODYNAMIC CHANGES IN NCPFThough Okuda et al. have tried to establish a similaritybetween IPH of Japan and NCPF of India, 14,15a numberof epidemiological differences, especially in the age and sexof patients, exist between the two countries. It seems thatthe disease can result from a number of different aetiolo-gical factors. NCPF and IPH may be a heterogeneousgroup of disorders, and this may explain the discrepanciesin its characteristics seen in patients from different partsof the world. Differences in haemodynamic data generatedby different researchers can also be explained by the dif-ferences in patient population and investigativetechniques. We will discuss the various haemodynamicchanges observed in NCPF patients against thebackground of these facts.
Splanchnic Pressures and Haemodynamic GradientsIt is well established that intrasplenic pressure and portalvein pressure are markedly elevated in patients withNCPF and IPH.6,16,17No correlation has been found bet-ween the splenic size and these pressures. 7

SARIN, SINGAL: PORTAL HAEMODYNAMICS IN NCPF
TABLE1. Techniques for measurement of portal pressure
181
Technique•
Remarks
1 Peroperative2 Percutaneous transhepatic catheterization3 Umbilico-portal catheterization4 Transvenous portal catheterization5 Wedged hepatic vein pressure (WHVP)
6 Intrahepatic pressure (IHP)7 Intravariceal pressure (IVP)
(a) Direct puncture of varix
(b) Indirect measurement by pneumatic pressure sensor
Reliable; effects of anaesthetic drugs cannot be excludedReliable, but highly invasiveReliable, invasive and riskyReliable, technically difficult and invasiveReliable in alcoholic cirrhosis not presinusoidal portal hypertension; hepatic blood
flow can be simultaneously measuredSimple, less invasive, less reliable
Simple, reliable, non-invasive, can be performed with routine endoscopy; repeatstudies not possible
Simple, less reliable, repeat studies possible
3
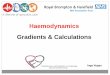
FIG. 1 Various techniques employed for the measurement ofsplanchnic pressure: (1) Intrasplenic pressure, (2) catheteri-zation through umbilical vein or mesenteric vein,(3) percutaneous transhepatic puncture, (4) intrahepaticpressure through Chiba needle, (5) trans-juglar portal veincatheterization, (6) wedged hepatic venous pressure,(7) intra variceal pressure through direct variceal puncture.
One of the main controversies. in the haemodynamicevaluation of NCPF concerns WHVP measurements.WHVP has been reported to be normap·18.19 or mildly ormoderately increased.8.16.20-22 The mean WHVP valuesreported in some larger studies are given in Table II.
TABLEII. Mean (±SO) splanchnic pressures in NCPF patients
Investigator ISP(mmHg) WHVP(mmHg)
Boyer et al. 6
Williams et al.23
Sarna et al. 16
Datta et a/.22Habibullah et at.21
Sarin et al. 20
23.3± 6.222.5± 7.020.2± 6.216.8±13.824.7± 6.024.5± 4.2
13.5±5.513.8±3.1l2.7±6.211.0±3.211.2±4.19.1±3.7
Williams et al. reported raised WHVP in more than half(52%) of their patients.P Sarna et al. found increasedWHVP in 40 of their 44 patients (91 %).16 In a recentstudy, we found that WHVP was 8 mm or less in nearlyhalf of the patients.POn the other hand, in patients withIPH, WHVP has been shown to be almost always higherthan that in controls. In the large Japanese National Studycomprising 469 patients, a mean WHVP of 204 mm H20(approximately 15.2 mm Hg) was recorded.> The differ-ences found in these studies could be caused by variationsin the extent and site of fibrosis in the patients.
In cirrhosis, particularly alcoholic cirrhosis, the PVPcorrelates closely with WHVP; but in NCPF, the WHVPis significantly lower than PVP and ISP.16.20This may bebecause WHVP measures the hepatic sinusoidal pressureand not the PVP. Therefore, if the resistance to portalblood flow exists prior to the formation of the hepaticsinusoids (presinusoidal), the portal pressure will not betruly reflected in the sinusoidal circulation. In fact, a cleargradient, called the portohepatic gradient is seen betweenISP and WHVP.16.17.20,23
Till recently, the exact site of resistance to portal flowin NCPF resulting in the portohepatic gradient was notknown. It could have been presinusoidal or perisinusoidal.IHP measurement has now been used to investigate thisissue.P IHP, which can be recorded by a thin Chiba needle,gives an indication of the hepatic sinusoidal pressure.> Itmeasures the pressure exerted by the liver interstitiumagainst a static column of tissue and fluid. A close correla-tion between IHP and WHVP has been reported in patientswith cirrhosis.P especially alcoholic cirrhosis. In patientswith NCPF, the IHP was found to be significantly lowerthan ISP but higher than WHVP, 20These findings suggest

182
MEAN (!SD)GRADIENT
8.89!6.48
MEAN (! SO)GRADIENT
15.1!5.86
40 401&1
1&1 IXIX :J:J 30 30 enen enen 1&11&1
'"IX a>
CI: Q, :I:Q, :I:"" 20 20 u
U E Z EZ E 1&1 EI&J oJoJ Q,Q, 10 10 enen -e~ CI:CI:l- I-
!: z0 0
IHP WHVP(mmHg) (mmHgl
FiG. 2. Intrasplenic, intrahepatic (IHP) and wedged hepaticvenous pressure (WHVP) in patients with non-cirrhotic por-tal fibrosis along with two haemodynamic gradients. (FromSarin et al. Gut 1987; 28:260-6; reproduced with permission.)
the existence of two independent pressure gradients inNCPF patients, the first between ISP and IHP and the sec-ond between IHP and WHVP (Fig. 2). While the formerhaemodynamic gradient indicates the presence of a presi-nusoidal block, the existence of the latter gradientsuggests a perisinusoidal resistance to the flow of portalblood.
The sites of origin of the two haemodynamic gradientscan be explained on the basis of the anatomical lesionsseen in NCPF. The two specific pathological lesionsobserved in NCPF are: (1) focal occlusive changes in theintrahepatic portal vein radicles known as obliterativeportovenopathy.P and (2) diffuse collagenization in thespace of Disse." While occlusive pyelephlebitic changesin the portal vein can explain the presinusoidal resistance,the rise in WHVP seems to result from collagenization ofthe space of Disse, secondary to diminished portal venous
L
FIG.3. Tracing of intra variceal pressure.
THE NATIONAL MEDICAL JOURNAL OF INDIA VOL. I, NO.4
.CIRRHOSISo NCPF
40o
Ia.Ia:!:)en 30enIa.Ia:Q. '"
~ ~ 20Ia.I e~ ea:~ 10-ea:I-~
o 10 20 30 40INTRASPLENIC PRESSURE
(mm/Hg)
FIG. 4. Intrasplenic and intravariceal pressures in patients withcirrhosis and non-cirrhotic portal fibrosis.
flow and compensated increased hepatic arterial flow. 20.29
Variation in collagen deposition in the space of Disse inindividual patients may explain the wide variations inWHVP measurements observed in NCPF.
Both WHVP and IHP underestimate the ISP in patientswith NCPF. Recently, interest has been generated in themeasurement of IVP by indirect'? or direct techniques.?"Direct IVP measurement is a simple technique which canbe performed before routine intravariceal sclerotherapyby puncturing the varix with the injector needle. IVP hasbeen shown to closely correlate (p<O.OOl) with the ISP,both in patients with cirrhosis and those with NCPpo(Figs. 3 and 4).
Splanchnic Blood FlowBy definition, PVP is increased in patients ofNCPF. Pres-sure depends upon the amount of blood flow and the resis-tance to this flow, i.e.
p= Q xR
where P is portal venous pressure, Q blood flow across theportal venous bed, and R resistance to portal venousblood flow.
One of the key issues in the pathophysiology of NCPFis the disproportionate splenomegaly seen in thesepatients. It is not clear whether splenomegaly is a result ofcongestion due to portal hypertension or because thesplenic involvement and the increased splenic blood floware the primary events.
A number of techniques have been used to study thehepatic blood flow in patients with portal hypertension(Table III). Total estimated hepatic blood flow (EHBF)may be either norma16,8,I6,18 or increased23,24,31,32 inpatients with NCPF. It has been suggested that splenicvenous inflow is increased in NCPF and contributes to the

SARIN, SINGAL: PORTAL HAEMODYNAMICS IN NCPF
TABLEIII. Techniques for measuring hepatic and portal blood flow
183
Technique Remarks
Reflects total (portal venous and hepatic arterial) estimated hepatic blood flow (EHBF).Reliable only if hepatic extraction exceeds 12% and remains constant. Does not measure
intrahepatically shunted blood.. Reliable, reflects EHSF, gives higher values than dye dilution. Technically difficult.
Non-invasive (intravenous route), sophisticated, can provide portal venous fraction of totalhepatic blood flow.
Direction of blood flow, rate of flow and collateral flow can be measured. Less reliable.Used for estimation of azygos venous blood flow. Reliable but technically difficult.Non-invasive, gives portal venous flow, errors up to 20-30% in estimation, collateral and
variceal flow can also be measured.
Dye dilution (SSP, ICG)
Multiple indicator dilution (SICr, 12sl-albumin)Computerized radionuclide angiography
(133Xe, 99Tc pertechnate)ScintiphotosplenoportographyThermodilutionEcho Doppler flowmetry
TABLEIV. lntra- and extraphepatic shunt indices in IPH
Investigator No. of Intrahepatic No. of Extrahepaticcases shunt index cases shunt index
Okuda erc/.>' 8 10% I 0%Nakamura et al.ss 14 21% 6 42%Ohnishi et al. 32 17 2.8-17.3%
(mean about 5.5%)
increased EHBF. It has also been suggested that bloodflow per 100 g of splenic tissue remains constant or isdecreased in NCPF and the absolute increase in splenicvenous inflow is a result of splenomegaly." A reductionin splenic blood flow related to the weight of the spleenmay result in splenic infarcts and is seen in about 30%cases of lPH. A significant correlation was found betweenthe splenic artery diameter and total splenic blood flowwhich suggests that the enlargement of the splenic arterymay be responsible for increased splenic blood flow inthese patients." Hepatic arterial diameter and arterialblood flow have been shown to remain normal ordecreased in TPH.
It has been shown that portal perfusion pressure (PVPminus free hepatic vein pressure) increases in somepatients with NCPF. In response to increased flow, thevascular resistance should decrease to normalize the pres-sure. However, because of pyelephlebitic changes, thecompliance of the portal venous system is reduced. Theincrease in blood flow causes a rise in PVP.
Portosystemic shunting in portal hypertension mayoccur at two places, outside or inside the liver. The extentof this shunting has been studied by injecting 99mTcmacro-aggregated albumin at the splenic hilum and !31J-macro-aggregated albumin into the portal trunk followed bydifferential counting over the lungs and the liver.P Quan-titative evaluation of portosystemic shunting has beenevaluated only in Japanese patients.'? It has been shownby Nakamura= and Okuda " that the extrahepatic shunt-ing is markedly increased in IPH. Intrahepatic shunting isless-common than in cirrhosis (Table IV).
Portal Vascular ResistanceThe other factor besides increased blood flow, which maycontribute to portal hypertension, is an increased portal
vascular resistance. This may be estimated by the follow-ing formulae.F
(i) Portal vascular resistance (Rpv)
PVP-FHVP
PVFIlOO cm ' LV
(ii) Presinusoidal portal vascular resistance (Rpre)
PVP-WHVP
PVFI100 cm ' LV
(iii) Postsinusoidal portal vascular resistance (Rpost)
WHVP-FHVPR =-----post EHBF/IOO cm ' LV
(where PVP is portal venous pressure, FHVP free hepaticvenous pressure, PVF portal venous flow, EHBF esti-mated hepatic blood flow, and LV liver volume).
In the absence of sufficient data, Rpv has been observedto be raised in the majority of patients with IPH. Rpre ismuch more in patients with normal PVF than in those withincreased flow.P
Congestion Index of the Portal VeinIn patients with portal hypertension, the cross-sectionalarea of the portal vein is increased while the total bloodflow is maintained or increased. The blood flow velocitymay in fact be reduced. The ratio of the portal vein cross-sectional area and the portal blood flow velocity is knownas the congestion index (CI) of the portal vein. It has beenshown that the CI in patients with IPH and cirrhosis is 2.5

184
times higher than that in normal subjects. This indi-cates that the main portal vein remains pliable in NCPFand changes its shape depending on the blood flow."
ADVANTAGES OF HAEMODYNAMICSTUDIES IN NCPFThe haemodynamic studies can be used for:
Differentiating NCPF from early cirrhosis of the liver-WHVP may be normal or mildly elevated in the former,while markedly elevated in the latter condition.Differentiating NCPF from the tropical splenomegalysyndrome (TSS). Besides the absence of varices,WHVP and IHP are normal in TSS patients, and ISP ismuch lower than that in NCPF patients.Understanding the natural history of NCPF. It isbelieved that NCPF does not ever progress to cirrhosis. 17
However, many NCPF patients do have nodular andshrunken livers. Whether such features represent a latestage of the disease with haemodynamic changes akinto cirrhosis is not known.Resolving the mystery of disproportionate splenome-galy in NCPF. Development of an animal model ofNCPF may be of great help in this direction.Evaluating the effect of pharmacological agents on portalpressure and flow. It is not known whether NCPFpatients behave in a way similar to cirrhotic patients inresponse to different drugs.Though haemodynamic investigations have helped
improve our understanding of the pathophysiology ofNCPF, they have failed to provide an insight into thecause of portal hypertension and the initial events leadingto increased blood flow, splenomegaly and pre- andperisinusoidal resistance to portal blood flow. More suchfundamental work is required.
REFERENCESBanti G. Splenomegalie mit leberzirrhose. Beitr Pathol Anat1889;24:21-33.
2 Dock G, Warthin AS. A clinical and pathological study of two casesof splenic anaemia with early and late stages of cirrhosis. Am J MedSciI904;127:24-55.
3 Warthin AS. The relationship of thrombophlebitis of portal andsplenic veins to splenic anaemia and Banti's disease. Int Clin1910;4:189-98.
4 Ramalingaswami V, Wig KL, Sama SK. Cirrhosis of the liver inNorthern India. Arch Intern Med 1962;110:350-8.
5 Proceedings of the workshop on non-cirrhotic portal fibrosis. IndianCouncil of Medical Research, 1969.
6 Boyer Jl., Sengupta KP, Biswas SK, et al. Idiopathic portal hyper-tension. Comparison with the portal hypertension of cirrhosis andextrahepatic portal vein obstruction. Ann Intern Med 1967;66:41-68.
7 Mikkelsen WP, Edmondson HA, Peters RL, Redeker AG,Reynolds TB. Extra- and intrahepatic portal hypertension withoutcirrhosis (hepatoportal sclerosis). Ann Surg 1965;162:602-20.
8 Basu AK, Guharay BN. Non-cirrhotic portal fibrosis with portalhypertension. Academic Publications, Calcutta, 1978.
9 Sarin SK, Sachdev G, Nanda R. Follow-up of patients after varicealeradication. A comparison of patients with cirrhosis, noncirrhoticportal fibrosis, and extrahepatic obstruction. Ann Surg1986;204:78-82.
10 Eckhauser FE, Appleman HD, KnollA, Strodel WE, Coran AG,Turcotte lG. Noncirrhotic portal hypertension: Differing patternsof disease in children and adults. Surgery 19R3;94:721-8.
THE NATIONAL MEDICAL JOURNAL OF INDIA VOL. I, NO.4
11 Kingham JGC, Levison DA, Stansfeld AG, Dawson AM. Noncir-rhotic intrahepatic portal hypertension: A long term follow-upstudy. Q J Med 1981;50:259-{i8. .
12 Villeneuve lP, Huet PM,loly JG, et al. Idiopathic portal hyperten-sion. Am J Med 1976;61:459-{i4.
13 Thompson WP, Caughey L, Wipple AL, Rousselot LM. Splenicvein pressure in congestive splenomegaly (Banti's syndrome). J ClinInvest 1937;16:571-2. .
14 Okuda K, Nakashima T, Okudaira M, et al. Liver pathology ofidiopathic portal hypertension. Comparison with non-cirrhoticportal fibrosis of India. Liver 1982;2:176-92. .
15 Okuda K, Omata M (eds). Idiopathic portal hypertension. Univer-sity of Tokyo Press, Tokyo, 1983.
16 Sama SK, Bhargava S, Gopinath N, et al. Noncirrhotic portal fib-rosis. Am J Med 1971;51:160-9.
17 Okuda K, Kono K, Ohnishi K, et al. Clinical study of eighty-sixcases of idiopathic portal hypertension and comparison with cir-rhosis with splenomegaly. Gastroenterology 1984;86:600--10.
18 Imanaga H,Yamamoto S, Kuroyanagi Y. Surgical treatment of por-tal hypertension according to state of intrahepatic circulation. AnnSurg 1962;155:43-50.
19 Koshy A. Haemodynamic diagnosis of NCPF. In: Okuda K, OmataM (eds). Idiopathic portal hypertension. University of Tokyo Press,Tokyo, 1983;357-62.
20 Sarin SK, Sethi KK, Nanda R. Measurement and correlation ofwedged hepatic, intrahepatic, intrasplenic and intravariceal pressuresin patients with cirrhosis of liver and non-cirrhotic portal fibrosis.Gut 1987;28:26Q-{i.
21 Habibullah CM, Rao GN, Murthy DK, et al. Non-cirrhotic portalfibrosis in Andhra Pradesh. ] Assoc Physicians India 1978;26:379-82.
22 Datta DV, Mitra SK, Chuttani PN, Chakravarti RN. Chronic oralarsenic intoxication as a possible aetiological factor in .idiopathicportal hypertension (non-cirrhotic portal fibrosis) in India. Gut1979;20:378-84.
23 Williams R, Parsonson A, Somers K, Hamilton JPS. Portal hyper-tension in idiopathic tropical splenomegaly. Lancet 1966;i:329-33.
24 Kameda H, Yamazaki K, Imai F. Clinical and epidemiological sur-vey of idiopathic portal hypertension. Interim report. In: Ministryof Health and Welfare Research Committee for the Study ofIdiopathic portal hypertension. Chairman Kunio Okuda. AnnualReport 1980;164-8.
25 Vermes lA. Transhepatic pressure measurements. Ann NY AcadSci 1970;170:193-200.
26 Orrego H, Amenabar E, Lara G, et al. Measurement of intrahepaticpressure as index of portal pressure. Am] Med Sci 1964;247:278-82.
27 Nayak NC, Ramalingaswami V. Obliterative portovenopathy of theliver associated with so-called idiopathic portal hypertension intropical splenomegaly. Arch PathoI1969;87:359-69.
28 Tandon BN, Lakshminarayanan R, Bhargava S, Nayak NC, Sam aSK. Ultrastructure of the liver in non-cirrhotic port·al fibrosis withportal hypertension. Gut 1970;11:905-10.
29 Iber FL. The cause of portal hypertension. Am J Med Sci1968;255:217-20.
30 Mosimann R. Non-aggressive assessment of portal hypertensionusing endoscopic measurement of variceal pressure. Am ] Surg1982;143:212-14.
31 Ueda H, Kitani K, Kameda HM, et al. Splenic blood flow inidiopathic portal hypertension in Japan measured by 85Kr clearancemethod. Acta Hepato-Splenologica 1971;18:28-40.
32 Ohnishi K, Saito M, Saito S, et al. Portal haemodynamics inidiopathic portal hypertension (Banti's syndrome) comparison withchronic persistent hepatitis and normal subjects. Gastroenterology1987;92:751-8.
33 Nakamura S, Kera K, Sasaki K, et al. Hepatic haemodynamics inidiopathic presinusoidal portal hypertension in Japan. Angiology1972;23:7-16.
34 Okuda K, Suzuki K, Musha H, et al. Percutaneous transhepaticcatheterization of the portal vein for the study of portalhaemodynamics and shunts. Gastroenterology 1977;73:279-84.
35 Moriyasu F, Nishida 0, Ban N, et al. 'Congestion index' of the por-tal vein. A]R 1986;146:735-9.