Embed Size (px)
Citation preview
Possible role of differential growth in airway wallremodeling in asthma
D.E. Moulton∗
OCCAM,Institute of Mathematics,
University of Oxford,Oxford, UK
A. GorielyOCCAM,
Institute of Mathematics,University of Oxford,
Oxford, [email protected]
January 14, 2011
Abstract
Airway remodeling in patients with chronic asthma is characterized by a thick-ening of the airway walls. It has been demonstrated in previous theoretical modelsthat this change in thickness can have an important mechanical effect on the prop-erties of the wall, in particular on the phenomenon of mucosal folding induced bysmooth muscle contraction. In this paper, we present a model for mucosal fold-ing of the airway in the context of growth. The airway is modeled as a bi-layeredcylindrical tube, with both geometric and material nonlinearities accounted for viathe theory of finite elasticity. Growth is incorporated into the model through thetheory of morphoelasticity. We explore a range of growth possibilities, allowingfor anisotropic growth as well as different growth rates in each layer. Such nonuni-form growth, referred to as differential growth, can change the properties of thematerial beyond geometrical changes through the generation of residual stresses.We demonstrate that differential growth can have a dramatic impact on mucosalfolding, in particular on the critical pressure needed to induce folding, the buck-ling pattern, as well as airway narrowing. We conclude that growth may be animportant component in airway remodeling.keywords: mucosal folding, chronic asthma, growth, elasticity, instability
∗Corresponding author
1

1 IntroductionAsthma is a disease characterized by a narrowing of the airway and reduced lung func-tion. Chronic asthma is often accompanied by irreversible structural changes to theairway wall, collectively referred to as airway remodeling [43]. Airway remodelingis a complex process occurring at multiple time and length scales and involving manydifferent chemical, biochemical, and physical stimuli. Despite a wealth of research itis still not clear how each of the different structural changes individually affects airwayfunction [51], nor is it known whether these different changes are beneficial or detri-mental to asthmatic patients [32]. A well documented key feature of airway remodelingis an increase in airway wall thickness, detected at all levels of the bronchial tree andall layers of the airway wall [19, 22, 24, 36].
In this theoretical paper, we focus on the mechanics of airway wall thickeningand the mechanism of mucosal folding at a macroscopic level by building a modelbased on the most sophisticated constitutive theory for elastic tissue available in thebio-engineering literature. In response to certain stimuli, the smooth muscle surround-ing the airway wall contracts, and the luminal boundary folds or buckles - this is thephenomenon of mucosal folding. In “normal patients,” such an event is marked byonly modest narrowing of the airway [34]. In asthmatic patients, however, this airwaynarrowing tends to occur for lower stimuli, and also leads to exaggerated narrowing[23].
Mucosal folding is also observed in the esophagus [28, 57], blood vessels [27], andgastrointestinal tract [30]. On a mechanical level, this folding indicates an instability ofthe inner mucosal edge in response to an external pressure provided by the contractionof smooth muscle. A number of models have looked at mechanical and geometricalaspects of mucosal folding. Some of the key issues from a modeling perspective are:determining the critical buckling pressure, critical buckling mode (i.e. the number offolds in the buckled state), and the degree of airway narrowing; finding relationshipsbetween these quantities; and determining the impact of airway wall thickness. Lam-bert [25] modeled the basement membrane as a single layer elastic tube and showed thatthe buckling mode can have a dramatic impact on airway narrowing; in particular thatan airway with fewer folds will have a greater degree of occlusion if the folds extenduntil epithelial cells come into contact. This basic model was expanded upon in [26],in which a geometric constraint was included as a mechanism for selecting the numberof folds, and was further expanded to include a thin layer of fluid on the inner edgeof the airway allowing for possible surface tension effects [15]. Other geometry basedmodels have been proposed, including [47], in which inextensibility of the basementmembrane was taken as a geometrical constraint, and the number of folds was directlyconnected to tethers between the airway and smooth muscle; and [6], which studiedeffective airway radius given fixed folding geometry. Wiggs et al. put the problem on amore mechanical level in [54], in which the airway was modeled as a bilayered elastictube. Solving the buckling problem in a finite element analysis, they found wall thick-ness to have a significant effect on the buckling mode and degree of narrowing. Similarmodels, also solved with finite elements, were presented a few years later, also incor-porating inertial effects of the basement membrane [3] and a comparison with bucklingexperiments with rubber tubes [18].
2

There are two potential drawbacks to previous models which should be elucidated.First, it is important to note that none of these models allowed for nonlinear materialresponses to large deformations, which are common in airway narrowing [37]. Overthe past decade, it has become increasingly clear in studying the mechanical propertiesof biological tissues that nonlinear tissue response, inhomogeneity, and remodelingare important, if not crucial, features [8]. The importance of nonlinear elasticity inbiological systems is well documented and appreciated in the case of arteries [48, 9,13, 17, 40], heart [29], muscles [49], brain tissue [55], and many other plants [50, 12]and biological systems [48]. It is clear that in order to understand both the mechanicalresponse and remodeling processes in airways, a constitutive theory based on nonlinearelasticity is required.
Secondly, a potentially important assumption in previous mechanical models is thatthe mechanical properties of the airway wall do not vary during remodeling, despiteevidence that these properties might be altered [21]. That is, airway wall thickness isexplored by varying reference dimensions, without any account for how the dimensionsmight have changed and whether mechanical properties might have varied in the pro-cess. This is a key distinction, and underlies the primary question we seek to answer inthis paper: could growth significantly impact the mechanical response of the airway tosmooth muscle contraction beyond the change in geometry, and thus be an importantfactor in airway remodeling?
The structural changes involved in airway remodeling fall into the large category ofprocesses known in the bio-engineering literature as growth and remodeling of elastictissues. Growth in biological systems can be the result of many different processes.Continuum mechanics and the theory of elasticity have long been used to study growthprocesses and the mechanical properties of growing tissues. It is now understood thatbiological materials commonly exhibit differential growth, that is the tissue does notgrow equally in all directions and/or different parts of the tissue grow at different rates.Differential growth can profoundly alter the geometry and mechanical properties of amaterial. Local changes of mass induce not only a change in the geometry but alsoelastic stresses which cannot be eliminated geometrically, and thus generate so-calledresidual stresses, which persist in the absence of external loads on the material. Resid-ual stress is a hallmark of biological tissues, and plays a key role in the regulation ofmany biological systems, including arteries [20, 13, 16], blood vessels [7], the humanaorta [17], and plant stems [50].
In this paper we model the airway as a two-layer cylindrical structure, and take intoaccount both geometrical and material nonlinearities by utilizing the theory of finiteelasticity [39]. The growth of the airway is described via the theory of morphoelas-ticity, and the buckling of the airway is computed using an incremental deformationstability analysis [2]. As mentioned, the model presented here combines both the non-linear response of the tissues in large deformation and the effect of growth, featureswhich are absent from previous modeling attempts. (Note Yang et al. recently pre-sented an interesting analysis using the same machinery of finite elasticity for a modelof the esophagus [57], but did not consider growth.) Using this model, we demon-strate that differential growth, in particular anisotropic growth, can have a dramaticimpact on the critical pressure exerted by smooth muscles needed to trigger buckling,the number of folds, the buckling pattern, and the degree of airway narrowing. Growth
3

can also alter stability properties and lead to seemingly counterintuitive results, for ex-ample an airway wall may become thicker while losing stability. Our results highlightthe importance of mechanical effects due to growth and suggest a need for further ex-perimental research along these lines. Indeed, our hypotheses may be tested by directmeasurement of residual stress as noted in [31].
2 Model and MethodsWe model an airway segment as a bilayer cylindrical structure, considering only tissueinterior to the smooth muscle. Following the model given by Wiggs et al. [54], astiff and thin inner layer corresponds to the mucosal region, consisting of the basementmembrane, the lamina propria, and the epithelium [1]. Surrounding this is a portion ofthe submucosa region, consisting of loose connective tissue. The inner layer is muchthinner and stiffer than the outer layer.
The airway smooth muscle (ASM) surrounds the outer layer, with ASM contractionproviding a force that deforms and eventually buckles the tube. ASM contraction is afairly complex process, and several models have been formulated to couple the under-lying chemical processes to mechanics [5, 42, 53]. The net mechanical effect of ASMcontraction is a normal force applied at the airway wall - smooth muscle interface [42].Since our purpose here is to focus on growth and buckling, ASM contraction is takeninto account as an applied normal pressure boundary condition at the outer edge. Also,since mucosal folding occurs at the mucosal region while the smooth muscle remainsroughly circular [26], we impose the boundary condition that the outer edge remaincircular in the deformed, buckled state.
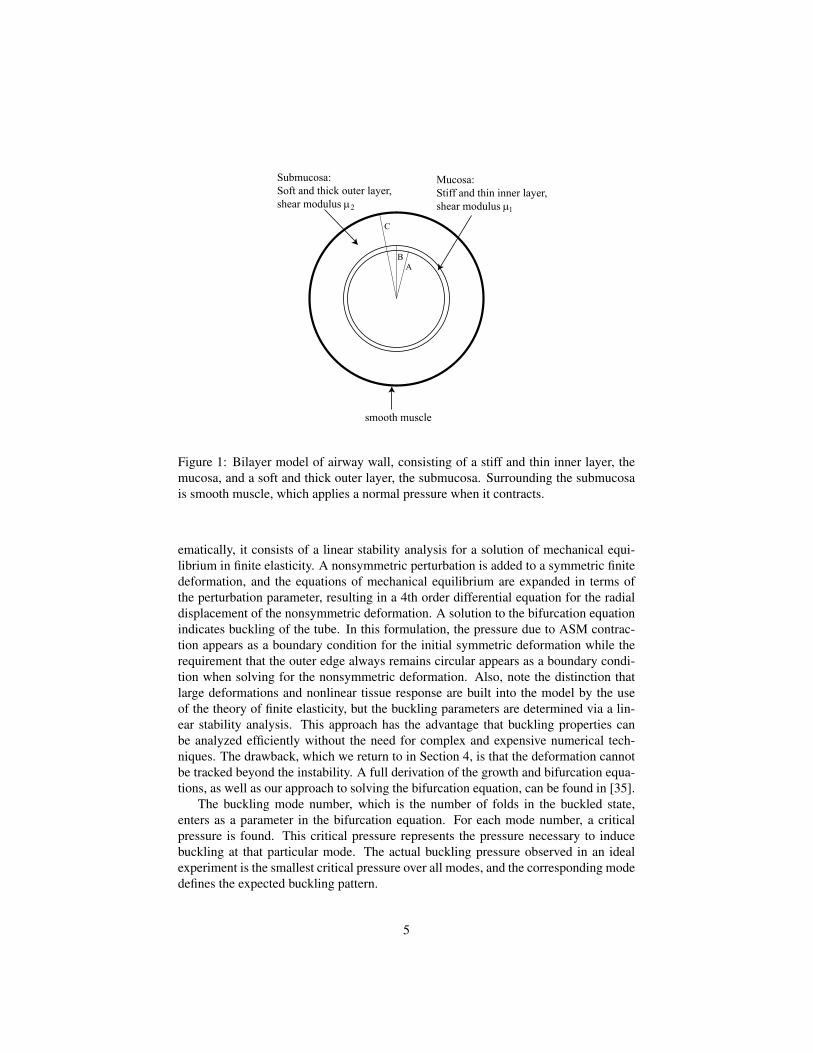
The setup is depicted in Figure 1. Material dimensions for the undeformed, ref-erence airway are the inner radius A, the thickness of the inner layer, B−A, and thethickness of the outer layer C−B. We assume an isotropic, incompressible hypere-lastic material [4]. To characterize the difference in stiffness between the two layers,the value of the shear modulus is assumed different in each layer, thus we have theparameters µ1 and µ2.
The model is three dimensional but assumes only plane strain deformation, so thatthe deformation is uniform along the tube axis. The basic idea behind the analysis isthat as the smooth muscle contracts, it creates a pressure normal to the circular crosssection and the tube deforms in a symmetric fashion, maintaining its circular shape,until a bifurcation point is reached at a critical pressure, at which point the cylinder“buckles” to an asymmetric state. The typical output of our mathematical model willbe the value of the critical pressure. Physiologically, this can be linked to the magni-tude of contractile force of the ASM necessary to induce buckling of the airway. Whilethe precise relationship between normal pressure and contractile force is nontrivial andwould require knowing material properties of the smooth muscle, it is a monotonicrelationship. Thus, an increase in critical pressure corresponds to a greater contractileforce for buckling. In terms of airway hyper-reponsiveness, buckling pressure (or con-tractile force of ASM for buckling) provides a good measure of the “strength” of anairway. This issue is discussed more fully in Section 4.
The buckling analysis follows the incremental theory, as described in [52]. Math-
4
AB
C
Submucosa:Soft and thick outer layer,shear modulus µ2
Mucosa:Stiff and thin inner layer,shear modulus µ1
smooth muscle
Figure 1: Bilayer model of airway wall, consisting of a stiff and thin inner layer, themucosa, and a soft and thick outer layer, the submucosa. Surrounding the submucosais smooth muscle, which applies a normal pressure when it contracts.
ematically, it consists of a linear stability analysis for a solution of mechanical equi-librium in finite elasticity. A nonsymmetric perturbation is added to a symmetric finitedeformation, and the equations of mechanical equilibrium are expanded in terms ofthe perturbation parameter, resulting in a 4th order differential equation for the radialdisplacement of the nonsymmetric deformation. A solution to the bifurcation equationindicates buckling of the tube. In this formulation, the pressure due to ASM contrac-tion appears as a boundary condition for the initial symmetric deformation while therequirement that the outer edge always remains circular appears as a boundary condi-tion when solving for the nonsymmetric deformation. Also, note the distinction thatlarge deformations and nonlinear tissue response are built into the model by the useof the theory of finite elasticity, but the buckling parameters are determined via a lin-ear stability analysis. This approach has the advantage that buckling properties canbe analyzed efficiently without the need for complex and expensive numerical tech-niques. The drawback, which we return to in Section 4, is that the deformation cannotbe tracked beyond the instability. A full derivation of the growth and bifurcation equa-tions, as well as our approach to solving the bifurcation equation, can be found in [35].
The buckling mode number, which is the number of folds in the buckled state,enters as a parameter in the bifurcation equation. For each mode number, a criticalpressure is found. This critical pressure represents the pressure necessary to inducebuckling at that particular mode. The actual buckling pressure observed in an idealexperiment is the smallest critical pressure over all modes, and the corresponding modedefines the expected buckling pattern.
5

Growth is included in the analysis via the theory of morphoelasticity and multi-plicative decomposition of the deformation tensor [46, 11]. The basic concept is thatthe deformation of the body is due to a local change of mass and to an elastic defor-mation. Since the change of mass is expressed locally, neighboring “cells” can growdifferentially. In the absence of elastic deformation, this can induce incompatibilitiessuch as overlapping cells or separation of tissue. The elastic deformation then bringsthe material back to a compatible configuration; this step can be seen as an elasticresponse to growth, and can induce residual stress in the material.
The effect of symmetric growth in each layer is captured by two parameters perlayer, instructing the gain or loss of mass in the radial and circumferential directions.We denote these growth parameters γ
(i)r , γ
(i)θ
, γ(o)r , γ
(o)θ
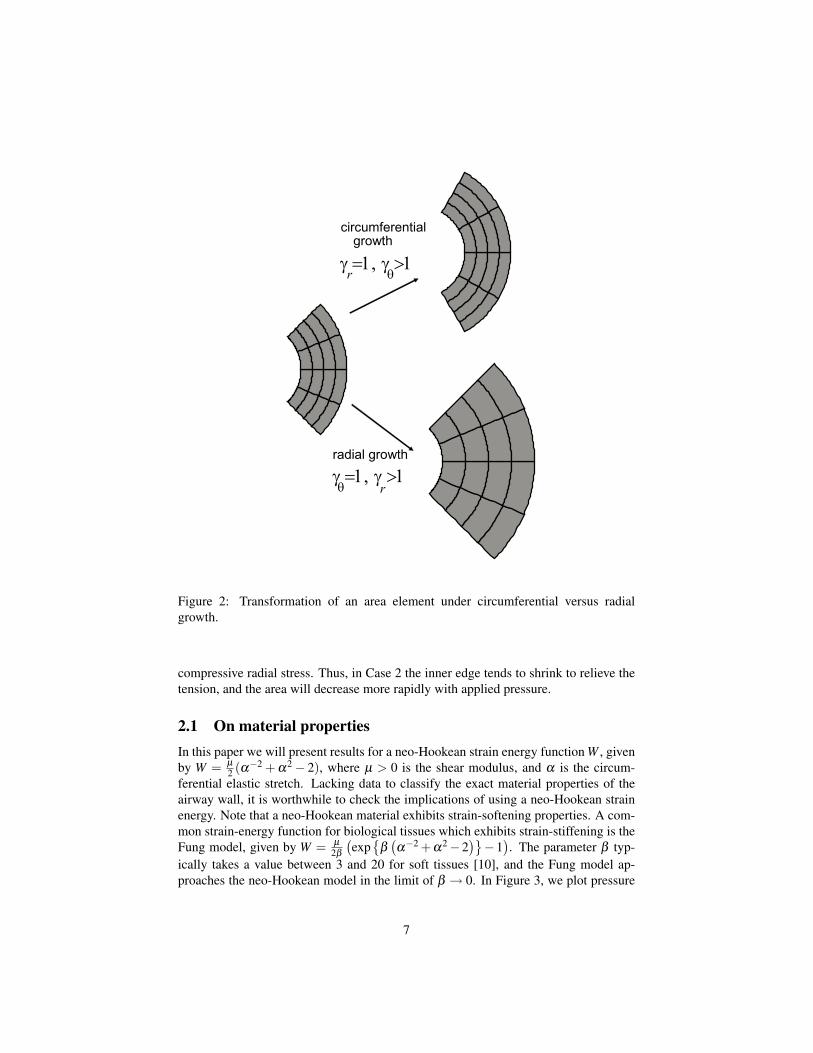
. Here γr corresponds to radialgrowth, with a gain or loss of mass in the radial direction if γr is greater than or lessthan 1. The addition or loss of mass in the circumferential direction is captured byγθ , where γθ > 1 corresponds to circumferential growth and γθ < 1 to circumferentialresorption. Figure 2 gives a schematic of radial versus circumferential growth. Thesuperscript differentiates the inner and outer layers. In general, these parameters canbe functions of radius, which would signal the case of different “rings” of the airwaygrowing at different rates. Here we consider anisotropic but homogeneous growth ineach layer, thus the γ’s are constant but not equal.
As our results are largely focused on varying these parameters, it is instructive tofurther clarify their meaning via a simple example. Consider a single layer tube withradii A = 1, B = 2, with no applied pressure and three different forms of growth:
1. γr = 2, γθ = 2. The parameter values imply that there is a doubling of mass inboth the radial and circumferential directions. Since growth is isotropic and noother forces are applied to the system, the deformed grown tube has radii a = 2,b = 4, highlighting a doubling of all radial and circumferential lines. In this case,no residual stress is generated.
2. γr = 1, γθ = 2. In this case, there is growth only in the circumferential direction.To account for the anisotropic growth, the tube expands to a larger total radius,while keeping nearly the same length of radial lines. A numerical computationgives that the tube after growth has radii a = 2.48, b = 3.49. The growth inducesa slight tensile radial stress. There will also be circumferential stress, namely theinner edge will be in tension and the outer edge in compression.
3. γr = 2, γθ = 1. Here, growth occurs only in the radial direction. A numericalcomputation gives the radii after growth as a = 0.69, b = 2.54; in this case radiallines want to double in length but are constrained, thus the anisotropic growthinduces a compressive radial stress.
To further understand the effect of growth, if we were to plot pressure-area curves(pre-buckling), the area would decrease more rapidly with increased external pressurein Case 2 than in Case 3. This can be understood in terms of the stress induced by thegrowth. In Case 2, the inner edge is in tension, i.e. there is a positive circumferen-tial stress, whereas the inner edge is in compression in Case 3, corresponding to the
6
circumferentialgrowth
γ =1, γ >1r θ
radial growth
γ =1, γ >1rθ
Figure 2: Transformation of an area element under circumferential versus radialgrowth.
compressive radial stress. Thus, in Case 2 the inner edge tends to shrink to relieve thetension, and the area will decrease more rapidly with applied pressure.
2.1 On material propertiesIn this paper we will present results for a neo-Hookean strain energy function W , givenby W = µ
2 (α−2 + α2− 2), where µ > 0 is the shear modulus, and α is the circum-ferential elastic stretch. Lacking data to classify the exact material properties of theairway wall, it is worthwhile to check the implications of using a neo-Hookean strainenergy. Note that a neo-Hookean material exhibits strain-softening properties. A com-mon strain-energy function for biological tissues which exhibits strain-stiffening is theFung model, given by W = µ
2β
(exp
{β
(α−2 +α2−2
)}−1
). The parameter β typ-
ically takes a value between 3 and 20 for soft tissues [10], and the Fung model ap-proaches the neo-Hookean model in the limit of β → 0. In Figure 3, we plot pressure
7
Pressure (kPa)
Are
a (m
m )
Fung, β=20
Fung, β=3
neo-Hookean
Linear
0.4 2.8 3.61.2 2.0
2
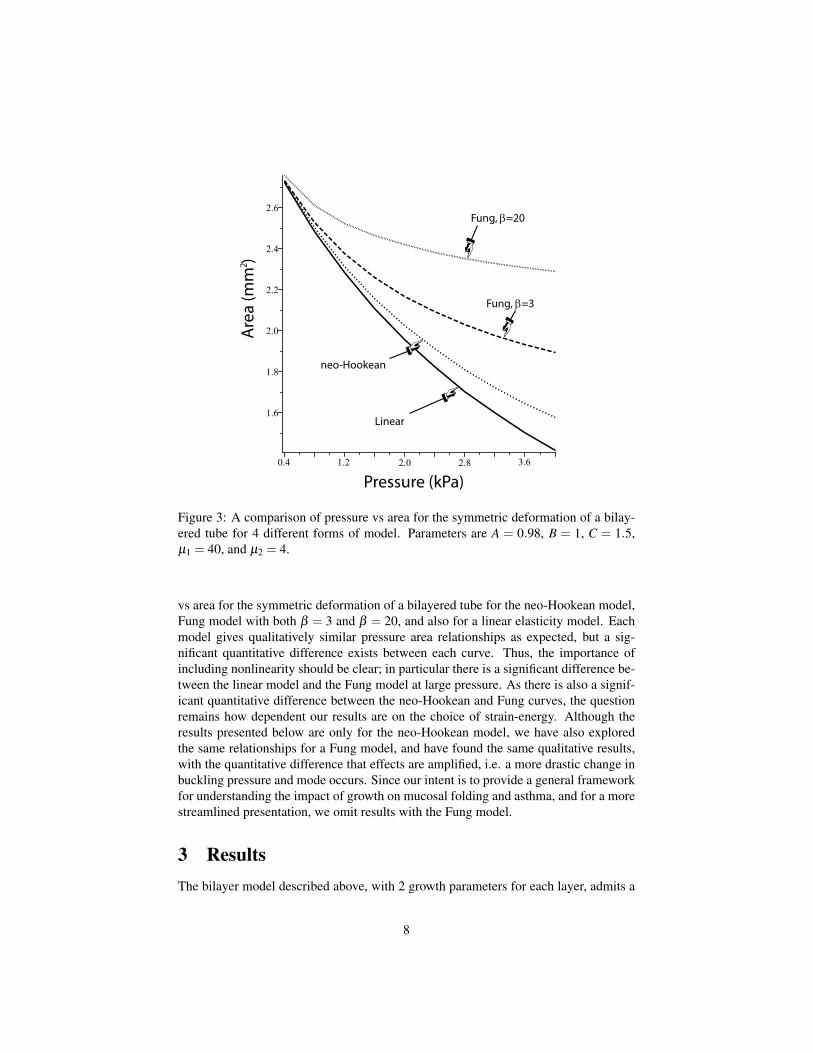
Figure 3: A comparison of pressure vs area for the symmetric deformation of a bilay-ered tube for 4 different forms of model. Parameters are A = 0.98, B = 1, C = 1.5,µ1 = 40, and µ2 = 4.
vs area for the symmetric deformation of a bilayered tube for the neo-Hookean model,Fung model with both β = 3 and β = 20, and also for a linear elasticity model. Eachmodel gives qualitatively similar pressure area relationships as expected, but a sig-nificant quantitative difference exists between each curve. Thus, the importance ofincluding nonlinearity should be clear; in particular there is a significant difference be-tween the linear model and the Fung model at large pressure. As there is also a signif-icant quantitative difference between the neo-Hookean and Fung curves, the questionremains how dependent our results are on the choice of strain-energy. Although theresults presented below are only for the neo-Hookean model, we have also exploredthe same relationships for a Fung model, and have found the same qualitative results,with the quantitative difference that effects are amplified, i.e. a more drastic change inbuckling pressure and mode occurs. Since our intent is to provide a general frameworkfor understanding the impact of growth on mucosal folding and asthma, and for a morestreamlined presentation, we omit results with the Fung model.
3 ResultsThe bilayer model described above, with 2 growth parameters for each layer, admits a
8

large parameter space. As our goal is to investigate the effect of growth on the bucklingof a normal versus a remodeled airway, we will primarily keep reference dimensionsof the airway fixed, and change the thickness of the airway by varying the growthparameters. In this way the growth defines a deformation from the normal airway to theremodeled airway. In prior studies, thicker airways have been studied by changing thereference dimensions themselves, without any particular mechanism to account for thechange. By keeping the reference dimensions fixed and altering the growth parameters,we can explore the effect of thickness on the buckling, but we are able to account forthe change of thickness as well as the changes in material properties resulting fromadditional residual stresses. We use as reference “normal airway” dimensions the basevalues A = 0.98, B = 1, C = 1.5, µ1 = 40, and µ2 = 4, giving a stiffness ratio µ1/µ2 =10. Here the radius values are in units of mm, and the shear moduli in units of kPA.The critical pressures appearing in this paper are also measured in kPa. These valuesare motivated by physiological measurements [22, 38] and would correspond roughlyto a medium sized cartilaginous airway with inner perimeter approximately 6.16 mmand Youngs modulus of the inner layer of 120 kPa; this choice of base values has alsobeen used in previous airway models [54, 18]. It should be noted that obtaining precisevalues for thickness and stiffness ratios is a challenging task and varies over generationsof the bronchial tree. Thus, we also explore the effect of changing reference dimensionsin Section 3.5.
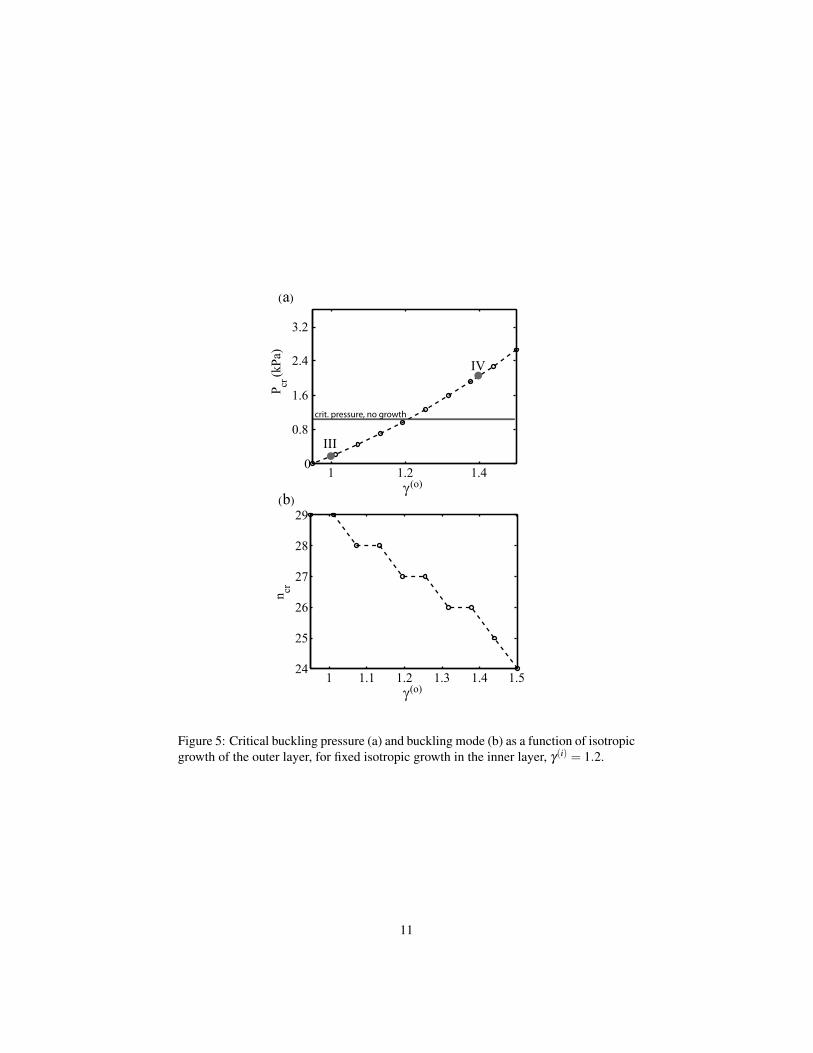
3.1 Isotropic growthThe first effect we consider is isotropic growth, but with different growth rates in eachlayer. That is, we assume γr = γθ in each region but that γ(i) 6= γ(o). As an example, welet γ(o) = 1.2 and vary γ(i) > 1. We plot in Figure 4 the critical pressure (a) and criticalbuckling mode (b) as a function of γ(i) ranging from 0.9 to 1.4. In Figure 5 the sameplots are shown with γ(i) = 1.2 fixed and γ(o) ranging from 0.95 to 1.5. It should benoted that the critical buckling pressure only depends on the ratio γ(i)/γ(o). Differentvalues with the same ratio are equivalent up to an isotropic and equal growth multiple ineach layer, so that the critical pressure does not differ (note that the airway dimensionswill vary by the same scalar multiple). Thus, the critical pressure for γ(i) = 1.2 inFigure 4, and for γ(o) = 1.2 in Figure 5, corresponds exactly to the critical pressurein the absence of growth (as shown by the horizontal line on the figures). Comparingthe critical pressure to this reference case, it is interesting to note that when the ratioγ(i)/γ(o) > 1, the airway is less stable, i.e. it buckles at a lower pressure. On the otherhand, a greater pressure is required when this ratio is less than one. In other words, theairway is weaker with respect to buckling when the inner layer grows at greater ratethan the outer layer, and likewise stronger when the outer layer grows faster. Observethat this effect is significant as the change in critical pressure increases by a factor ofabout 8 as γ(o) changes from 1 to 1.5.
As stated, the linear stability analysis enables us to find critical buckling parame-ters, but once buckling occurs we have no direct information on the magnitude of thedeformation. Thus, we cannot comment directly on the exact amount of narrowing ofthe airway after buckling occurs. Nevertheless, we can make relative comparisons ofthe size of the non-symmetric deformation for different parameters. In this way, we can
9

1 1.2 1.40
0.8
1.6
2.4
3.2
γ(i)
P (
kPa)
cr
1 1.2 1.422
24
26
28
30
(i)
n cr
γ
(a)
(b)
crit. pressure, no growth
I
II
Figure 4: Critical buckling pressure (a) and buckling mode (b) as a function of isotropicgrowth of the inner layer, for fixed isotropic growth in the outer layer, γ(o) = 1.2.
10
1 1.1 1.2 1.3 1.4 1.524
25
26
27
28
29
(o)
n cr
1 1.2 1.40
(o)γ
γ
crit. pressure, no growth
(a)
(b)
III
IV
0.8
1.6
2.4
3.2
P (
kPa)
cr
Figure 5: Critical buckling pressure (a) and buckling mode (b) as a function of isotropicgrowth of the outer layer, for fixed isotropic growth in the inner layer, γ(i) = 1.2.
11

0.5
1
1.5
2
0.5
1
1.5
2
0.5
1
1.5
2
0.5
1
1.5
2
III IV
I II
Figure 6: Buckling patterns, or tube deformation, after bifurcation for the pointsmarked I-IV in Figures 4(a) and 5(a).
determine whether buckling at one set of parameters should result in more or less nar-rowing (initially) than buckling at another set of parameter values. Buckling patternsfor the points marked I-IV in Figures 4(a) and 5(a) are shown in Figure 6. Comparing Iand II, in the case of γ(o) = 1.2 fixed, each type of growth can be argued to have advan-tageous and disadvantageous features. At the lower value of γ(i), the buckling pressureis much higher but the airway narrows significantly more. If an airway were to growwith the growth rates at point I, it would have a greater resistance to ASM contractionbut would have exaggerated narrowing when buckling occurs. At the higher value, itis the opposite: the airway narrowing is reduced but the buckling pressure is muchlower. There is essentially a trade off between the two growth rates. This trade off doesnot occur in the case of fixed γ(i) (Figure 5). The larger value of γ(o) (point IV) hasa higher resistance to buckling and comparable narrowing to the smaller value of γ(o)
(point III). Note that the growth ratio is nearly equal at points I and IV, but both valuesof γ are higher at IV, and the increased growth leads to a larger airway area. Betweenthe destabilizing growths, III is more detrimental to airway function as it has greaterairway narrowing.
Referring to Figures 4 - 5, it seems counterintuitive that more growth in the outerlayer is required to strengthen the airway wall, since the inner layer is stiffer. In fact,a primary result of Wiggs et al. [54] was that increasing the thickness in the inner
12
1 1.5 20.8
1.2
1.6
γr(i)
P
(kPa
)cr
n=25
n=14
0.5
1
1.5
0.5
1
1.5
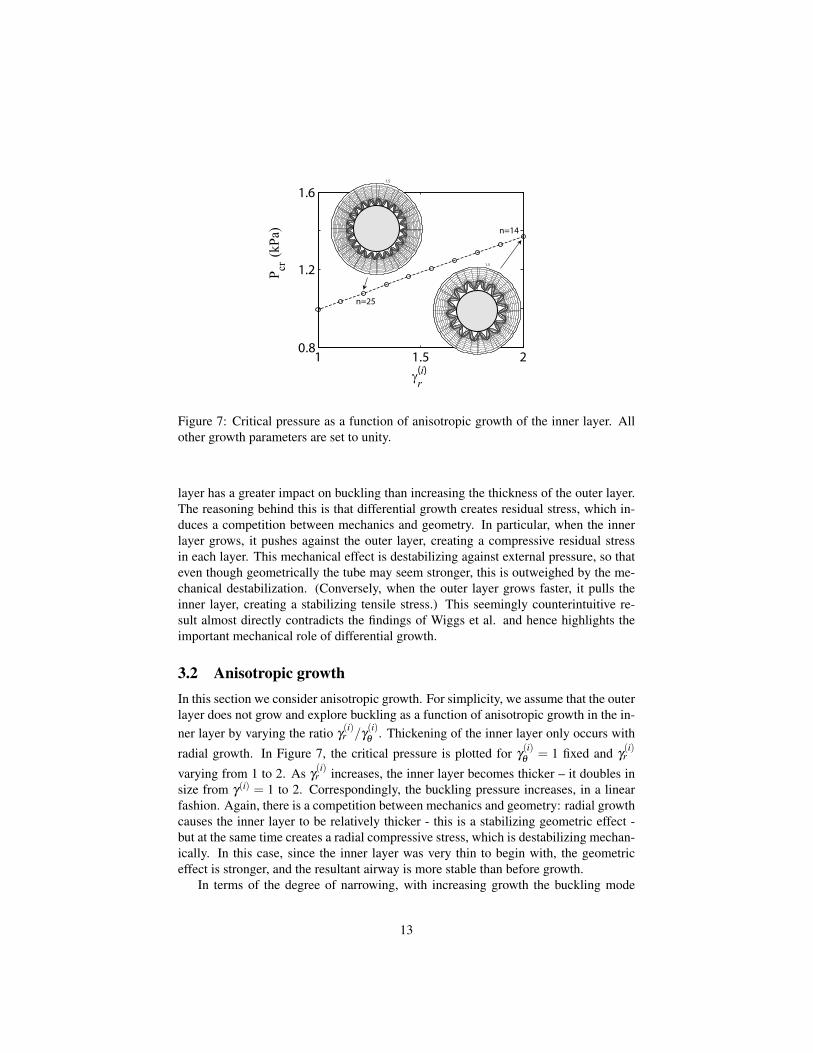
Figure 7: Critical pressure as a function of anisotropic growth of the inner layer. Allother growth parameters are set to unity.
layer has a greater impact on buckling than increasing the thickness of the outer layer.The reasoning behind this is that differential growth creates residual stress, which in-duces a competition between mechanics and geometry. In particular, when the innerlayer grows, it pushes against the outer layer, creating a compressive residual stressin each layer. This mechanical effect is destabilizing against external pressure, so thateven though geometrically the tube may seem stronger, this is outweighed by the me-chanical destabilization. (Conversely, when the outer layer grows faster, it pulls theinner layer, creating a stabilizing tensile stress.) This seemingly counterintuitive re-sult almost directly contradicts the findings of Wiggs et al. and hence highlights theimportant mechanical role of differential growth.
3.2 Anisotropic growthIn this section we consider anisotropic growth. For simplicity, we assume that the outerlayer does not grow and explore buckling as a function of anisotropic growth in the in-ner layer by varying the ratio γ
(i)r /γ
(i)θ
. Thickening of the inner layer only occurs with
radial growth. In Figure 7, the critical pressure is plotted for γ(i)θ
= 1 fixed and γ(i)r
varying from 1 to 2. As γ(i)r increases, the inner layer becomes thicker – it doubles in
size from γ(i) = 1 to 2. Correspondingly, the buckling pressure increases, in a linearfashion. Again, there is a competition between mechanics and geometry: radial growthcauses the inner layer to be relatively thicker - this is a stabilizing geometric effect -but at the same time creates a radial compressive stress, which is destabilizing mechan-ically. In this case, since the inner layer was very thin to begin with, the geometriceffect is stronger, and the resultant airway is more stable than before growth.
In terms of the degree of narrowing, with increasing growth the buckling mode
13

decreases monotonically and significantly, from n = 27 at γ(i)r = 1 to n = 14 at γ
(i)r = 2.
Included in Figure 7 are the form of the deformation at the values γ(i)r equals 1.2 and
2. Here the effect of buckling mode is apparent. In both cases, the inner radius atthe point of bifurcation is about 0.87, and both plots are produced using the same sizedperturbation in the incremental deformation, but the airway narrowing is exaggerated atthe point with the lower mode, γ
(i)r = 2. Defining the effective lumen as the area inside
the innermost point of the folds (the shaded gray circles), we compute that this area is18% greater in the case γ
(i)r = 1.2. Interestingly, if the anisotropic growth of the inner
layer is accompanied by an isotropic swelling of the outer layer, the critical pressure isalmost doubled, while the lumen area stays roughly the same (plot not shown).
3.3 Fixed outer radiusThe model as we have presented it does not restrict outward growth. For instance inCase IV of Figure 6, notice that the outer edge is well beyond the location of the smoothmuscle cells boundary before deformation (the outer radius of the reference state, equalto 1.5). This may not be realistic. It is likely that ASM, even before contracting, placesa geometric constriction on the growth of the outer layer, so that the airway is restrictedto grow radially outward, and must otherwise grow radially inward. The exact formof this constraint is complicated by the fact that the smooth muscle also grows duringremodeling [23] and would require a detailed understanding of the growth relationshipsbetween the various layers of the airway. Nevertheless, some insight on the effect ofa geometric constraint can be obtained if we fix the size of the outer radius duringdeformation. Mathematically, this changes the structure of the problem through theboundary condition since growth and pressure become inter-dependent. Fixing growthparameters automatically sets the pressure – a given growth creates pressure at the outerwall since the outer edge pushes against the smooth muscle. In this case, pressure isnot a control parameter but is slaved to the growth parameters.
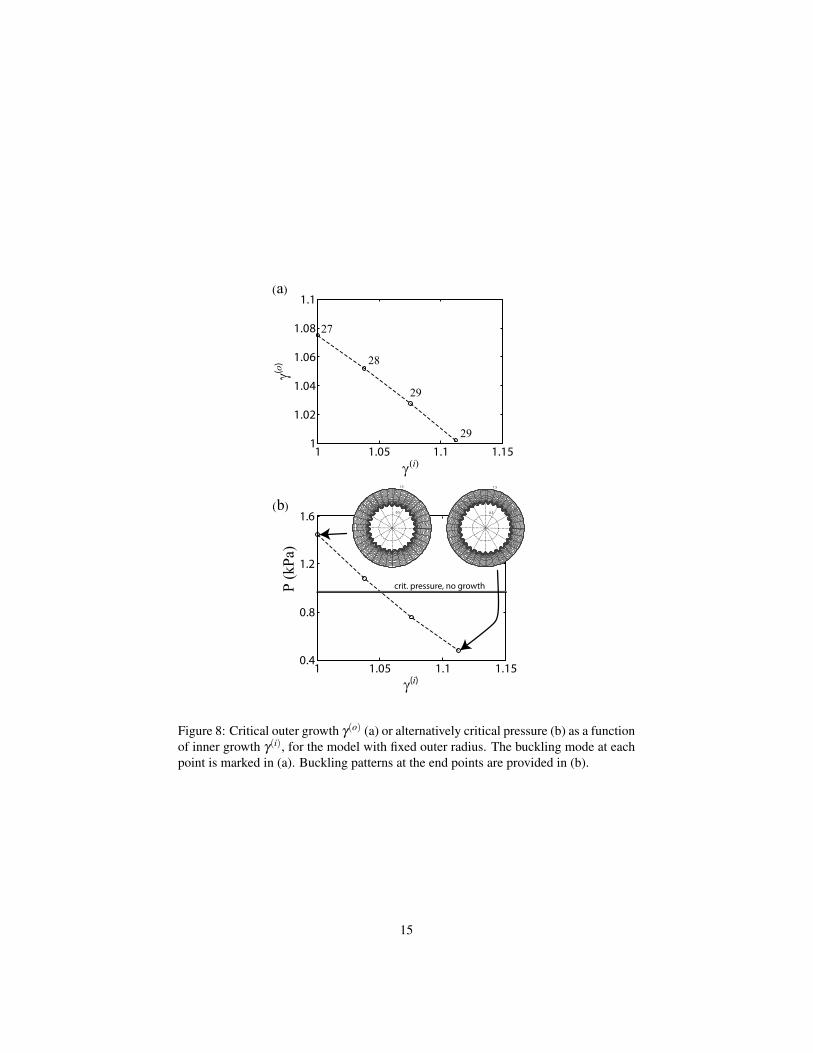
In Figure 8(a), we plot the bifurcation relationship between γ(o) and γ(i) for fixedouter radius. A given value of γ(i) and the corresponding γ(o) represent a form ofgrowth which induces buckling. For each growth pair, the corresponding pressure isplotted in Figure 8(b).
There are different ways to view these plots and this version of the model. If weassume that the ASM interface is rigid and does not allow any outward growth, thenFigure 8(a) shows the critical growth which induces buckling and Figure 8(b) is thepressure induced at the ASM interface due to the growth. In this sense growth itself isinducing buckling without any required contraction of the ASM. Alternatively, if theASM layer is compliant, then some outward growth can occur, and when the ASMcontracts the fixed outer radius requirement pushes the outer edge back to its originalposition. The biggest effect of the fixed outer radius condition is that the amount ofgrowth is greatly restricted. Only the lower-left triangular region in Figure 8(a) con-stitutes valid growth. Viewing Figure 8(b), growth can be stabilizing or destabilizing.Buckling patterns are included at the select points, indicating again a trade off wherebythe stronger airway is also narrower.
14
1 1.05 1.1 1.151
1.02
1.04
1.06
1.08
1.1
γ(i)
γ(o)
1 1.05 1.1 1.150.4
0.8
1.2
1.6
γ(i)
P (k
Pa)
27
29
29
28
crit. pressure, no growth
(a)
(b) 0.5
1
1.5
0.5
1
1.5
Figure 8: Critical outer growth γ(o) (a) or alternatively critical pressure (b) as a functionof inner growth γ(i), for the model with fixed outer radius. The buckling mode at eachpoint is marked in (a). Buckling patterns at the end points are provided in (b).
15

3.4 Inverse problemIt is clearly very difficult to determine experimentally the growth rates in the differentlayers. However, some geometric parameters, such as the thicknesses of normal airwayand asthmatic airways are accessible. This raises the question: if we knew exactlyhow much thicker each layer of the airway wall became during remodeling and thepressure applied by the smooth muscle, could we determine the growth parametersand the amount of differential growth which occurred? We refer to this as the inverseproblem: given the details of the deformation and the buckling, can we determine thetype of growth which induced the deformation? Surprisingly, this can be done. Adetailed analysis of this idea is given in a companion paper [35]. Mathematically, theargument can roughly be made by counting equations - there are 4 equations involvedin determining the bifurcation of a bilayered cylinder. Since there are also 4 growthparameters, the inverse problem is well formulated, and a solution can in principle befound. A mathematical proof of this is lacking, but in all of the simulations we haveattempted, a solution has been found.
We demonstrate here with a suggestive example. We start with a reference systemin the absence of growth where the critical pressure is P∗ = 0.2492, the buckling modeis n = 27, and the radii at the point of buckling are a = 0.8750, b = 0.8974, and c =1.4336. We now ask whether a growth could occur such that each layer is twice thethickness at the point of buckling and the buckling pressure is halved. We keep thesame value of b and double the relative thickness of each layer by taking a = 0.8526and c = 1.9698. Then setting P = P∗/2 = 0.1246, we find that the inverse problem hasthe solution γ
(i)r = 1.92, γ
(i)θ
= 1.03, γ(o)r = 2.35, and γ
(o)θ
= 1.05. Notice that the ratioγr/γθ is greater than one in each layer. The interpretation is that if growth is faster inthe radial direction in each layer at these particular values, the walls would grow suchthat the thickness at the point of buckling is doubled while at the same time bucklingoccurs at half the critical pressure as compared to the case with no growth. (Conversely,a solution could also be found with half the thickness and double the pressure.)
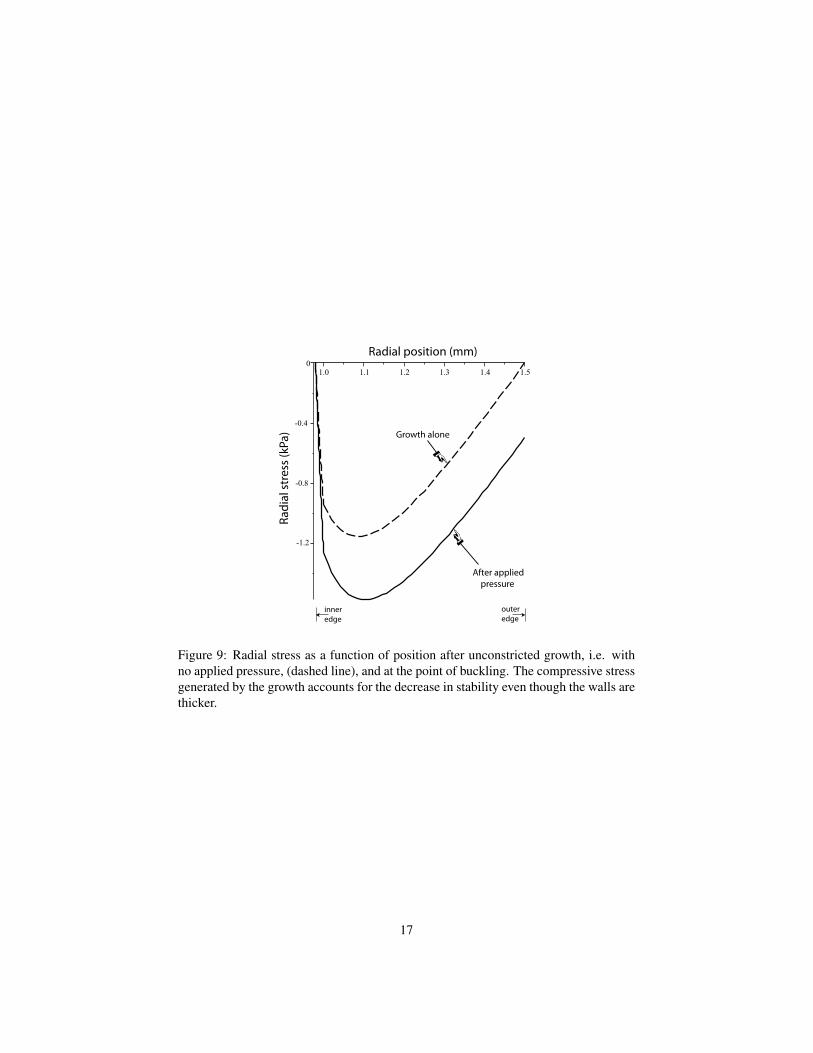
Again, the rationale for the existence of these solutions relates to the competingeffects of residual stress and geometric effects. Given the large range of possibilitieswith anisotropic growth in two layers, there is sufficient flexibility in the growth vari-ables that residual stress effects can be made dominant. For the example given, thegrowth causes a large compressive radial stress which dominates the geometric effectof the thicker inner layer. To further illustrate this effect, in Figure 9 we plot the radialstress profile in the tube. The dashed line is the stress due to growth alone, i.e. with nopressure applied, and the solid line is the stress at the point of bifurcation. We see thatgrowth creates a strong compressive stress, so that only a small amount of additionalpressure is required to induce buckling.
The point of this example is not to suggest that this exact value of growth maybe occurring in airways, but rather to demonstrate the very significant impact that dif-ferential growth can have. If residual stress is generated, simply measuring airwaydimensions and changes in dimensions could potentially be misleading as far as under-standing mechanical stability.
16
Growth alone
After applied pressure
Radi
al s
tres
s (k
Pa)
Radial position (mm)
inneredge
outeredge
-0.4
-0.8
-1.2
Figure 9: Radial stress as a function of position after unconstricted growth, i.e. withno applied pressure, (dashed line), and at the point of buckling. The compressive stressgenerated by the growth accounts for the decrease in stability even though the walls arethicker.
17

3.5 Airway sizeIn order to focus on the effect of growth, we have thus far kept fixed the reference di-mensions and stiffness ratio. Our choice of reference parameters was motivated by thegeneral observation that the mucosa is significantly stiffer and thinner than the submu-cosa. However, one set of parameters certainly does not characterize all generations ofthe bronchial tree [22], and is also dependent on where you define the submucosa layeras ending. In this section, we briefly explore the impact of varying those parameters.
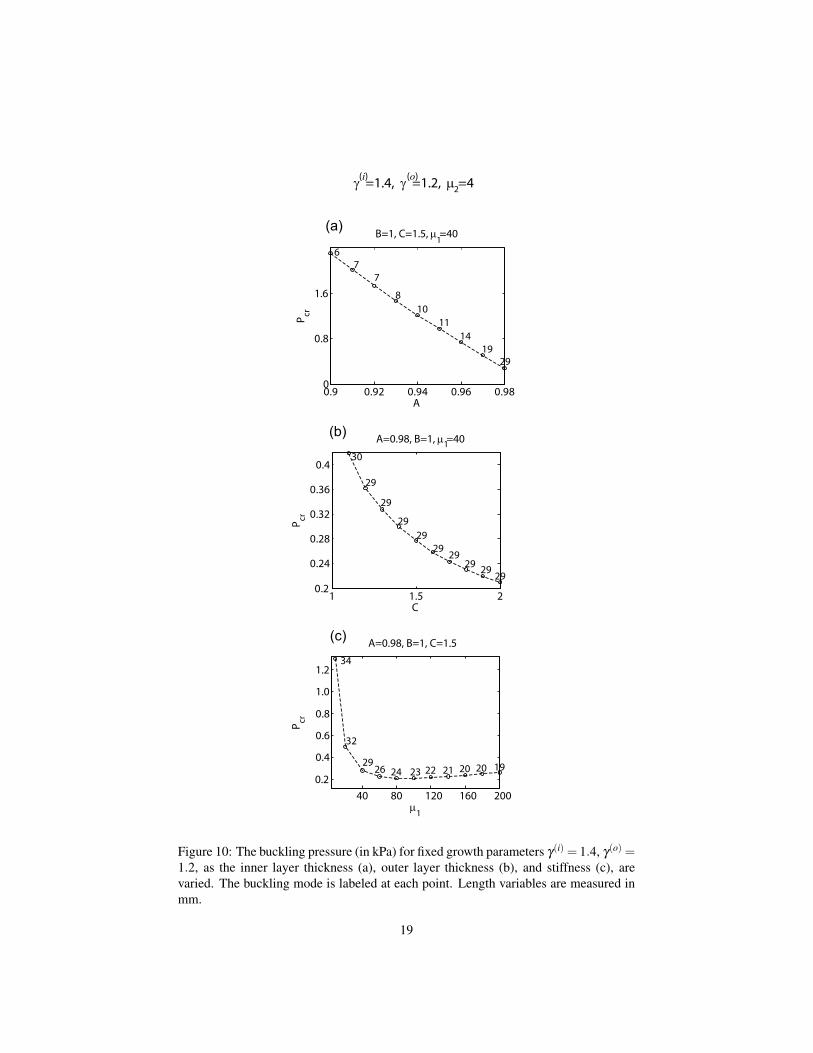
To do this, we fix the growth parameters at γ(i) = 1.4, γ(o) = 1.2, and vary the in-ner layer thickness, outer layer thickness, and stiffness ratio. The result is plotted inFigure 10. As the inner layer thickness is increased (Figure 10(a)), the critical pres-sure increases and the buckling mode decreases. Observe that both critical pressureand buckling mode vary quite significantly; for instance starting from the base valueA = 0.98, if the thickness of the inner layer is doubled to A = 0.96, the critical pres-sure increases by more than a factor of 2, while the critical mode decreases from 29to 14. There is a key distinction between this result and those of Section 3.1: here wehave increased the inner layer thickness in the reference dimensions, which is mechan-ically stabilizing, whereas in 3.1 it was shown that increasing the inner layer thicknessthrough differential growth can have the opposite effect and be destabilizing. Interest-ingly, an increase in thickness of the outer layer (Figure 10(b)) leads to a decrease inthe critical pressure. The explanation for this is that, as explained in Section 3.1, thegiven growth parameters are destabilizing because the inner layer pushes against theouter layer and creates a destabilizing compressive stress. Increasing the outer layerthickness results in a harder body for the inner layer to push against, and thus leadsto further destabilization. Nevertheless, we observe that the change in magnitude incritical pressure is quite small, and the buckling mode is essentially unaffected. Thissuggests that buckling behavior is not strongly dependent on small changes of submu-cosa thickness. Finally, as seen in Figure 10(c), varying the relative stiffness of thelayers does not have a dramatic impact either, except in the limit when the stiffnessratio approaches unity.
4 DiscussionSimilar to previous modeling attempts, in this paper we have studied the mechanicaleffect of airway wall thickness on mucosal folding and airway narrowing. The majoraddition in the present work which has not been included in any prior studies is thatairway thickening occurs as a consequence of differential growth. Doing so, we havebeen able to study changes in material properties, in particular stability properties, dueto the generation of residual stress.
Generally speaking, we have shown that differential growth can have a significanteffect on airway buckling and therefore may be an important contributing factor in un-derstanding the mechanical behavior of airways which have undergone airway remod-eling. Note that only differential growth was considered, because it is the competitionbetween geometry and mechanics that occurs as a result of the locally incompatible na-ture of differential growth that leads to interesting and counterintuitive behavior. Still,
18
0.9 0.92 0.94 0.96 0.980
0.8
1.6
A
P cr
67
7
810
1114
1929
1 1.5 20.2
0.24
0.28
0.32
0.36
0.4
C
P cr
29
29
2929
2929
29 2929
30
40 80 120 160 2000.2
0.4
0.6
0.8
1.0
1.2
µ 1
P cr
34
32
2926 24 23 22 21 20 20 19
γ =1.4, γ =1.2, µ =4(i) (o)
B=1, C=1.5, µ =40
A=0.98, B=1, µ =40
A=0.98, B=1, C=1.5
1
2
1(a)
(b)
(c)
Figure 10: The buckling pressure (in kPa) for fixed growth parameters γ(i) = 1.4, γ(o) =1.2, as the inner layer thickness (a), outer layer thickness (b), and stiffness (c), arevaried. The buckling mode is labeled at each point. Length variables are measured inmm.
19

there are many ways in which differential growth could occur, and we have exploredonly a few possibilities here. Isotropic growth with differing rates in each layer ledto the somewhat surprising conclusion that if the stiff mucosa grows at a faster ratethan the soft submucosa, the airway actually becomes less stable. Anisotropic growthof the inner layer led to a strengthened airway but significantly decreased the bucklingmode. Fixing the outer radius so as to account for the growth constriction of the smoothmuscle greatly limited the amount of growth.
Our analysis provides a general framework to understand the mechanical effect ofgrowth and remodeling, and our approach gives the ability to test hypotheses regardinggrowth and changes in airway stability. However, many open questions remain be-fore anything definitive may be said. Differential growth provides a mechanism to ex-plain otherwise contradictory structural changes, for instance an airway wall becomingthicker and at the same time less stable. But airway remodeling involves more complexchanges than just an increase of the mucosal and submucosal layers. The ASM layeralso gains mass, and there is uncertainty as to whether the contractile potential changes[41]. Thus, whether the airways are actually less stable after remodeling is not yetestablished.
An obvious question is whether any direct evidence exists of differential growth inairway remodeling. We contend that more information is needed to conclude whetherindividual airway layers grow anisotropically, although anisotropic growth is known tooccur in arteries [20, 33]. On the other hand, it seems quite likely that different layersof the airway grow at different rates, since the material composition varies drastically,and there is good evidence to suggest that this form of differential growth is presentin airway remodeling [44]. It should be noted, however, that in actuality growth iscomplex and cannot be fully captured by constant parameters γi as utilized here, sincethe mass that is added may be of a different density or type than the normally presentmaterial [45].
If airway walls grow differentially and induce residual stress, as we have postulatedhere, this can be detected by opening-angle experiments, in which a ring of airway wallis cut radially. Any residual stress is relieved by the cut and the ring opens up. Suchexperiments are difficult, and have been carried out in only one study [31], wherethey reached the conclusion that human airways are essentially free of residual stress.However, it is important to note that none of the human lungs in that experimental studycame from humans with asthma. This is a critical distinction, because our hypothesisis that normal airways are in a zero stress state, and that stress might be introducedthrough airway remodeling, in which case only asthmatic lungs would show an openingangle. Hence, opening angle experiments would need to be carried out on normal andasthmatic airways to confirm or deny the possibility of differential growth.
We now turn to the shortcomings of an idealized model. The airway is a complexstructure, composed of multiple layers, which we have modeled as a bilayer cylindricaltube. This is certainly a simplification, although the purpose is to provide insight intothe effect of growth in mucosal folding and an idealized model is sufficient to investi-gate these generic effects. The two dimensional nature of the model and the plane strainassumption are supported by the fact that folds in airways are observed as longitudinalridges [56]. The linear stability analysis has the drawback that it only provides infor-mation on the deformation up to the point of the buckling. Nevertheless, knowledge
20

of the buckling pressure is a good measure of the “strength” of an airway, and previ-ous studies have shown that a tube becomes much more compliant after buckling [54],suggesting that narrowing occurs more rapidly after buckling. This is also apparent byan increased negative slope in pressure-area curves after buckling [54]. Thus, giventwo airways with different buckling pressures and all other characteristics equal, theairway with lower buckling pressure would be prone to greater hyper-responsiveness.Buckling pressure would hence seem to be a valid measure for investigating the me-chanical impact of growth on airway narrowing. Moreover, the conclusion from priormodels that buckling mode may be a significant indicator of airway narrowing seemsto be supported by our analysis as well. Still, a proper analysis of occlusion and thechange in cross sectional area would necessitate continuing the deformation beyondthe point of buckling, which would require a much more computationally heavy nu-merical approach such as finite elements. Such an analysis coupled with growth wouldbe an interesting direction for future modeling attempts. One should also keep in mindthat while our focus has been on stability in terms of buckling pressure, physiologi-cally this pressure is generated by smooth muscle contraction, thus any conclusionsregarding growth and changes in airway response must take into account the exact re-lationship between ASM contraction and induced pressure at the airway wall as wellas any possible changes in contractile potential of the ASM.
The study we have presented is a preliminary examination of growth and mechanicsin airways, and is largely qualitative. While we have attempted to use physiologicallyreasonable parameter values, exact values, in particular of the growth parameters, areunknown to us. Regarding the buckling pressure, which relates the normal force in-duced at the interface due to smooth muscle contraction, experiments have found thatcanine airways can generate pressures around 3 kPA [14]. This seems to be in linewith our findings, as the critical pressure in our simulations ranged from about 0.7kPa to 3.2 kPa. Note that these values corresponded to a neo-Hookean material; thestrain-stiffening Fung model leads to an increase in the critical stress.
Finally, the results presented here might also suggest a future direction of research.The structural changes associated with airway remodeling are generally considereduncontrollable and detrimental. However, if airways can be stimulated to grow in aparticular way, growth can potentially both strengthen the airways against narrowingand reduce the degree of narrowing. In this sense, an analysis such as the one presentedhere could serve as a guideline for the type of growth necessary to achieve this.
Acknowledgments: This publication is based on work supported by Award No. KUK-C1-013-04 , made by King Abdullah University of Science and Technology (KAUST),and based in part upon work supported by the National Science Foundation under grantDMS-0907773 (AG). AG is a Wolfson/Royal Society Merit Award holder.
Figure Legends
Figure 1: Bilayer model of airway wall, consisting of a stiff and thin inner layer, themucosa, and a soft and thick outer layer, the submucosa. Surrounding the submucosais smooth muscle, which applies a normal pressure when it contracts.
21
Figure 2: Transformation of an area element under circumferential versus radial growth.
Figure 3: A comparison of pressure vs area for the symmetric deformation of a bi-layered tube for 4 different forms of model. Parameters are A = 0.98, B = 1, C = 1.5,µ1 = 40, and µ2 = 4.
Figure 4: Critical buckling pressure (a) and buckling mode (b) as a function of isotropicgrowth of the inner layer, for fixed isotropic growth in the outer layer, γ(o) = 1.2.
Figure 5: Critical buckling pressure (a) and buckling mode (b) as a function of isotropicgrowth of the outer layer, for fixed isotropic growth in the inner layer, γ(i) = 1.2.
Figure 6: Buckling patterns, or tube deformation, after bifurcation for the points markedI-IV in Figures 4(a) and 5(a).
Figure 7: Critical pressure as a function of anisotropic growth of the inner layer. Allother growth parameters are set to unity.
Figure 8: Critical outer growth γ(o) (a) or alternatively critical pressure (b) as a functionof inner growth γ(i), for the model with fixed outer radius. The buckling mode at eachpoint is marked in (a). Buckling patterns at the end points are provided in (b).
Figure 9: Radial stress as a function of position after unconstricted growth, i.e. withno applied pressure, (dashed line), and at the point of buckling. The compressive stressgenerated by the growth accounts for the decrease in stability even though the walls arethicker.
Figure 10: The buckling pressure for fixed growth parameters γ(i) = 1.4, γ(o) = 1.2,as the inner layer thickness (a), outer layer thickness (b), and stiffness (c), are varied.The buckling mode is labelled at each point. Length variables are measured in mm.
References[1] Bai A., D. H. Eidelman, J. C. Hogg, A. L. James, R. K. Lambert, M. S. Ludwig,
J. Martin, D. M. McDonald, W. A. Mitzner, M. Okazawa, and al. et. Proposednomenclature for quantifying subdivisions of the bronchial wall. J. Appl. Physiol.,77:1011–1014, 1994.
[2] Ben Amar M. and A. Goriely. Growth and instability in elastic tissues. J. Mech.Phys. Solids, 53:2284–2319, 2005.
[3] Bando K., D. Yamashita, and K. Ohba. Numerical Simulation for Mechanism ofAirway Narrowing in Asthma. JSME International Journal Series C, 45(4):1020–1027, 2002.
22
[4] Boyce M. C. and E. M. Arruda. Constitutive models for rubber elasticity: areview. Rubber Chem. Technol., 73, 2000.
[5] Brook B. S., S. E. Peel, I. P. Hall, AZ Politi, J. Sneyd, Y. Bai, MJ Sanderson,and OE Jensen. A biomechanical model of agonist-initiated contraction in theasthmatic airway. Respiratory physiology & neurobiology, 170(1):44–58, 2010.
[6] Donovan G.M. and M.H. Tawhai. A simplified model of airway narrowing due tobronchial mucosal folding. Respiratory physiology & neurobiology, 171(2):144–150, 2010.
[7] Fung Y. C. What are the residual stresses doing in our blood vessels? AnnalsBiomed. Eng., 19:237–249, 1991.
[8] Fung Y. C. Biomechanics: Material Properties of Living Tissues. Springer, NewYork, 1993.
[9] Gleason R. L. and J. D. Humphrey. A mixture model of arterial growth andremodeling in hypertension: altered muscle tone and tissue turnover. J. Vasc.Research, 41:352–363, 2004.
[10] Goriely A., M. Destrade, and M. Ben Amar. Instabilities in elastomers and insoft tissues. The Quarterly Journal of Mechanics and Applied Mathematics,59(4):615, 2006.
[11] Goriely A., and D. E. Moulton. Morphoelasticity - a theory of elastic growth.In M. Mueller M. Ben Amar, A. Goriely, editor, New Trends in the Physics andMechanics of Biological Systems. Oxford University Press, 2010.
[12] Goriely A., D. E. Moulton, and R. Vandiver. Elastic cavitation, tube hollowing,and differential growth in plants and biological tissues. EPL (Europhysics Let-ters), 91:18001, 2010.
[13] Goriely A. and R. Vandiver. On the mechanical stability of growing arteries. IMAJ. Appl. Math., Accepted:1–22, 2010.
[14] Gunst S. J. and J. Q. Stropp. Pressure-volume and length-stress relationships incanine bronchi in vitro. Journal of Applied Physiology, 64(6):2522, 1988.
[15] Hill M.J.,T.A. Wilson, and R.K. Lambert. Effects of surface tension and intra-luminal fluid on mechanics of small airways. Journal of Applied Physiology,82(1):233, 1997.
[16] Holzapfel G. A. , T. C. Gasser, and R. W. Ogden. Comparison of a multi-layerstructural model for arterial walls with a Fung-type model, and issues of materialstability. J. Biomech. Engineering, 126:264, 2004.
[17] Holzapfel G. A. and R.W. Ogden. Modelling the layer-specific three-dimensionalresidual stresses in arteries, with an application to the human aorta. Journal ofthe Royal Society Interface, 7(787-799), 2010.
23
[18] Hrousis C. A., B. R. Wiggs, J. M. Drazen, D. M. Parks, and R. D. Kamm. Mucosalfolding in biologic vessels. J. Biomech. Eng., 124(4):334–341, 2002.
[19] Huber H. L. and K. K. Koessler. The pathology of bronchial asthma. Arch. Intern.Med., 30, 1922.
[20] Humphrey J. D. . Continuum biomechanics of soft biological tissues. Proc. Roy.Soc. Lond. A, 459:3–46, 2003.
[21] James A. Airway remodeling in asthma. Curr. Opin. Pulm. Med., 11:1–6, 2004.
[22] James A. L., P. D. Pare, and J. C. Hogg. The mechanics of airway narrowing inasthma. Am. Rev. Respir. Dis., 139(1):242–246, 1989.
[23] King G. G., P. D. Pare, and C. Y. Seow. The mechanics of exaggerated airwaynarrowing in asthma: the role of smooth muscle. Resp. Physiol., 118:1–13, 1999.
[24] Kuwano K., C. H. Bosken, P. D. Pare, T. R. Bai, B. R. Wiggs, and J. C. Hogg.Small airways dimensions in asthma and in chronic obstructive pulmonary dis-ease. Am. Rev. Respir. Dis., 148(5):1220–1225, 1993.
[25] Lambert R. K. Role of bronchial basement membrane in airway collapse. J. Appl.Physiol., 71:666–673, 1991.
[26] Lambert R. K., S. L. Codd, M. R. Alley, and R. J. Pack. Physical determinants ofbronchial mucosal folding. J. Appl. Physiol., 77:1206–1216, 1994.
[27] Lee M. M. L. and S. Chien. Morphologic effects of pressure changes on caninecarotid artery endothelium as observed by scanning electron microscopy. TheAnatom. Rec., 194:1–14, 1978.
[28] Liao D., J. Zhao, J. Yang, and H. Gregersen. The oesophageal zero-stress state andmucosal folding from a giome perspective. World J. Gastroenterol, 13(9):1347–1351, 2007.
[29] Lin L. E. and L. Taber. A model for stress-induced growth in the developing heart.J. Biomech. Engineering, 117:343–349, 1995.
[30] Lu X., J. Zhao, and H. Gregersen. Small intestinal morphometric and biomechan-ical changes during physiological growth in rats. J. Biomech., 38, 2005.
[31] McKay K. O., B. R. Wiggs, P. D. Pare, and R. D. Kamm. Zero-stress state ofintra- and extraparenchymal airways from human, pig, rabbit, and sheep lung. J.Appl. Physiol., 92:1261–1266, 2002.
[32] McParland B. E., P. T. Macklem, and P. D. Pare. Airway hyperresponsiveness:From molecules to bedside. J. Appl. Physiol., 95:426–434, 2003.
[33] Menzel A. Modelling of anisotropic growth in biological tissues. Biomechanicsand modeling in mechanobiology, 3(3):147–171, 2005.
24
[34] Moore B. J., C. C. Hilliam, L. M. Verburgt, B. R. Wiggs, S. Vedal, and P. D. Pare.Shape and position of the complete dose-response curve for inhaled methacholinein normal subjects. Am. J. Respir. Crit. Care. Med., 154, 1996.
[35] Moulton D. E. and A. Goriely. Circumferential buckling instability of a growingcylindrical tube. J. Mech. Phys. Solids, doi 10.1016/j.jmps.2011.01.005, 2011.
[36] Niimi A., H. Matsumoto, R. Amitani, Y. Nakano, M. Mishima, M. Minakuchi,K. Nishimura, H. Itoh, and T. Izumi. Airway wall thickness in asthma assessedby computed tomography. Am. J. Respir. Crit. Care Med., 162:1518–1523, 2000.
[37] Noble P. B., A. Sharma, P. K. McFawn, and H. W. Mitchell. Airway narrowingin porcine bronchi with and without lung parenchyma. European RespiratoryJournal, 26(5):804, 2005.
[38] Ogawa Y. Study on the strength of human lower air-passages. J. Kyoto PrefectUniv. Med, 66:781–800, 1959.
[39] Ogden R. W. Non-linear elastic deformation. Dover, New york, 1984.
[40] Ogden R. W. and C. A. J. Schulze-Bauer. Phenomenological and structural as-pects of the mechanical response of arteries. ASME Applied Mech., 242:125–140,2000.
[41] Pare P. D., B. E. McParland, and C. Y. Seow. Structural basis for exaggeratedairway narrowing. Can. J. Physiol. Pharmacol., 85(7):635–638, 2007.
[42] Politi A. Z., G. M. Donovan, M. H. Tawhai, M. J. Sanderson, A. M. Lauzon, J.H. T. Bates, and J. Sneyd. A multiscale, spatially distributed model of asthmaticairway hyper-responsiveness. Journal of Theoretical Biology, 2010.
[43] Redington A. E. and P. H. Howarth. Airway wall remodelling in asthma. Thorax,52:310–312, 1997.
[44] Roberts C. R. Is asthma a fibrotic disease? Chest, 107:111S–117S, 1995.
[45] Roche W.R., J. H. Williams, R. Beasley, and S. T. Holgate. Subepithelial fibrosisin the bronchi of asthmatics. The Lancet, 333(8637):520–524, 1989.
[46] Rodriguez E. K., A. Hoger, and A. McCulloch. Stress-dependent finite growth insoft elastic tissues. J. Biomech, 27:455–467, 1994.
[47] Seow C. Y., L. Wang, and P. D. Pare. Airway narrowing and internal structuralconstraints. Journal of Applied Physiology, 88(2):527, 2000.
[48] Taber L. A. Biomechanics of growth, remodeling and morphogenesis. Appl.Mech. Rev., 48:487–545, 1995.
[49] Taber L. A. Biomechanical growth laws for muscle tissues. J. Theor. Biol.,193:201–213, 1998.
25
[50] Vandiver R. and A. Goriely. Tissue tension and axial growth of cylindrical struc-tures in plants and elastic tissues. Europhys. Lett., 84:58004, 2008.
[51] Vignola A. M., F. Mirabella, G. Costanzo, R. Di Giorgi, M. Gjomarkaj, V. Bellia,and G. Bonsignore. Airway remodeling in asthma. Chest, 123(3):417S–422S,2003.
[52] Wang A. S. D. and A. Ertepinar. Stability and vibrations of elastic thick-walledcylindrical and spherical shells subjected to pressure. Int. J Non-Linear Mech.,7:539–555, 1972.
[53] Wang I., A. Z. Politi, N. Tania, Y. Bai, M. J. Sanderson, and J. Sneyd. A math-ematical model of airway and pulmonary arteriole smooth muscle. Biophysicaljournal, 94(6):2053–2064, 2008.
[54] Wiggs B. R., C. A. Hrousis, J. M. Drazen, and R. D. Kamm. On the mechanismof mucosal folding in normal and asthmatic airways. J. Appl. Physiol, 83:1814–1821, 1997.
[55] Xu G., P. V. Bayly, and L. A. Taber. Residual stress in the adult mouse brain.Biomechanics and modeling in mechanobiology, 8(4):253–262, 2009.
[56] Yager D., T. Cloutier, H. Feldman, J. Bastacky, J. M. Drazen, and R. D. Kamm.Airway surface liquid thickness as a function of lung volume in small airways ofthe guinea pig. J. Appl. Physiol., 77(5):2333–2340, 1994.
[57] Yang W., T. C. Fung, K. S. Chian, and C. K. Chong. Instability of the two-layered thick-walled esophageal model under the external pressure and circularouter boundary condition. J. Biomech., 40, 2007.
26