Embed Size (px)
Citation preview

Post Neoadjuvant therapy: issues in
interpretation

Disclosure:

Overview D
Prognostic features in assessment of post treatment specimens:
Tumor size
Cellularity
Grade
Receptors
LN

Neoadjuvant chemotherapy: receiving chemotherapy before surgery
Adjuvant: Chemotherapy after surgery

Who are the candidates
Offered to LABC patients to reduce the size
Improves the surgical options
NACT achieve the same survival results as adjuvant

Advantages of NACT
In vivo assessment of tumor response to different systemic interventions
Pathologically detected residual disease predicts prognosis
Increased eligibility for breast conservation

Tumor bed visible
the periphery residual tumor nodules may or may not be visible
Measure: TB, residual nodules and distance to margins
post-ttt
How to approach a specimen post NACT

Tumor bed is not visible:
Radiology report (residual calcs, response, location)
Clip inserted at the time of the biopsy
Send specimen to imaging
post-ttt

If the specimen is small, tumor bed not clearly
image the specimen, could submit sections guided by location of clip
If the tumor bed is large > 5 cm (variability in guidelines)
Start with 1-2 blocks/1cm, if no residual tumour is found submit in toto
How many sections are enough?

What is pCR 1.No residual invasive tumor in the breast and lymph node
2.No residual invasive or in situ carcinoma in the breast and lymph node
3.No residual invasive carcinoma in the breast
4.No residual invasive carcinoma in the lymph node

pCR
Powerful predictor of long-term outcome(OS and DFS)pCR
pCR: as absence of residual invasive disease in the breast and ipsilateral lymph nodes after NACT
(ypT0/isypN0)

pCR related to several factors
Higher tumor grade
Proliferative fraction
Hormone receptor status (TN and HER2 +ve)

Sorlie et al, Proc Natl Acad Sci U S A. 2003 Jul 8;100(14):8418-23.
ve usually achieve pCR while luminal A tumours are least likely,
Luminal B intermediate respond) (Rouzier et al 2005)

Triple Negative
Core bx ER PR
HER2 Tumor bed LN

HER2 positive
Core bx � ER� PR�
HER2� Tumor bed � LN �

Luminal B HER2 positive
Core bx ER PR
HER2 Post ttt LN

Luminal B
Core bx ER PR
HER2 Post ttt LN

Reporting post Neoadjuvant Chemotherapy
Residual invasive carcinoma (size - cellularity)
Tumor bed
Grade
Margins
Receptors
LN

How can we identify the tumor bed ?
pCR or near pCR
If carcinoma is not palpable

Tumor bed Loosely vascularized fibrotic area
with absence of normal glands
Fibromyxoid stroma
Mucin pools (if no epithelial cells present should not be considered residual tumour)
hemosiderin deposition and absence of normal mammary glandular elements

Residual tumor Residual tumor: most
show decrease in cellularity.
Single cells, cords or
stroma, multiple residual foci or a mass that has shrunk in size circumferentially
Cytologic features: Hyper eosinophilic cytoplasm, nuclear enlargement and vesicular chromatin
Pre-ttt Post-ttt
Post-ttt Post-ttt
Post-ttt Post-ttt

Tumor size
If response is minimal, tumour is
If response is marked, multiple small foci dispersed over a large tumour bed
The size of the largest continuous focus and the number of residual foci should be reported

Tumor cellularity Carcinomas are often less
cellular post NACT
Loss of cellularity is not always
which can lead to clinical overestimation
Cellularity is determined with accuracy only if pretreatment specimen is available for comparison
Loss of cellularity is associated with better prognosis and clinical outcome
(Ogston et al, 2003)

Chen A at MD Anderson found that a residual tumor > 2.0 cm is associated with higher LRR
Multifocal disease is associated with higher LRR
5 year LRR-free survival for multifocal residual, solitary residual and no residual was 82%, 93% and 95%.
(Chen A M et al , 2004)

Reporting post Neoadjuvant Chemotherapy
Residual invasive carcinoma (size - cellularity)
Tumor bed
Grade
Margins
Receptors
LN

Histologic grade correlation with Outcomes
Elston & Ellis (1991) Histopathology 19:403
Score Tubule formation Nuclear pleomorphism
Mitotic counts *
1 >75 % similar to normal 0-9
2 10-75% Larger than normal, nucleoli
10-19
3 <10% Marked, large and bizarre
>20
* Mitotic counts depend on field diameter

Nottingham grade Usually the same
NACT causes increased pleomorphism of residual cells
Mitotic activity is reduced in addition to reduction in tumor cellularity which can
mitotic count Pre-ttt Post-ttt

The pretreatment assessment of histological grade remains an independent prognostic factor for DFS and OS
Post NACT grade important ? retains its prognostic value with lower tumour grades associated with better survival
(Pierga et al 2003)

Hormone receptors and HER2

In untreated tumors, minimal discordance between core needle and excisional biopsy has been reported
ER (discordance 1.8%)
PR (discordance 15%)
HER2 (discordance 1.2%)
(Ardenos M et al, 2009)

Hormone receptors can change after treatment
A change in HR status has been reported in 8 - 33% of patients.
For ER, half the discordance was from negative to positive
For PgR, changes from a positive to a negative result was commonly seen
(Van de Ven S etal, 2011)

Tumor heterogeneity
Limited amount present either before or after treatment
Selection: if multiple tumors or heterogenous expression some foci respond to therapy more than others
Technical factors has to be considered as well

HER2
Changes in HER2 after untargeted therapy are uncommon
Some studies reported decrease in expression of HER2 on IHC but in situ hibridization is not changed due to stable HER2 gene

Reporting after Neoadjuvant chemotherapy
Residual invasive carcinoma (size - cellularity)
Tumor bed
Grade
Margins
Receptors
LN

Lymph nodes
Number of involved lymph nodes
Size of the deposits
EXtranodal extension
Lymph nodes showing treatment effects

Lymphoid depletion
Fibrous scarring with little or no residual tumour
LN metasases with CR are often
aggregates of macrophages
Should not be considered
LN

LMWK �

Micrometastases/ITC
Post NACT micrometastases/ITC are mostly considered macro metastases that partially responded to therapy
(Newman LA et al, 2003)

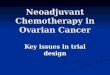
Post NACT lymph node status is the most important prognostic factor.
LN response after chemotherapy is a better prognostic factor than response of the primary tumor to primary chemotherapy
(Rouzier R et al JCO, 2002).

Fig 2.
Rouzier R et al. JCO 2002;20:1304-1310
©2002 by American Society of Clinical Oncology
Distant disease-free survival according to the axillary nodal status after primary chemotherapy. —, No residual nodal disease; ---, residual nodal disease.�

Number of involved nodes: The increased number of LN with residual positive lymph nodes is associated with worse DFS
Size of the deposit: The larger the size of the metastatic deposit the worse the DFS

Systems for evaluating response to treatment
American Joint Committee on Cancer system: adds the
Relies mainly on tumor size post treatment and lymph node status in the post treatment specimen
Tumor size : based on the size of largest continuos
added.
The categories are the same as those used for the pre-ttt
Disadvantage: cellularity is not included in the overall assessment

The Miller-Payne System: divided into 5 grades based on pre and post treatment cellularity and was correlated with OS and DFS
Disadvantage: Doesn’t include response in the lymph node
(Ogston K et al, 2003)

Residual cancer burden:
Residual invasive carcinoma cellularity
Number of lymph nodes with metastases
Size of the largest metastatic deposit
Combined to provide a continuos parameter of response (RCB index) divided into four categories

Reporting after neo-adjuvant chemotherapy
Tumor bed
Size of the largest continuous focus or number of foci over the tumor bed
Grade
Margins
LN (number and size of met)