Embed Size (px)
Citation preview

Introduction and Objectives
Post-operative Infection after Surgery of Brain Tumors: a Five-year Review of Common Pathogens, Presentation and other Associated Factors
Tannaz Asadi1, Adarsh Bhimraj2, Carlos Isada2, Alireza M. Mohammadi3, L. Tricia Bravo2
Departments of Internal Medicine (1) at Fairview Hospital, Infectious Diseases (2), and Neurosurgery (3) at Cleveland Clinic
Mailing address: 18101, Lorain Avenue, suit 757, Fairview hospital, Cleveland, Ohio, 44111 Email: [email protected] Phone: (216)476-7369 Fax: (216)476-2944
Background • Post-op infection happens after 2-4%
intracranial surgeries for brain tumors • Limited data is available regarding
common pathogens and associated risk factors
• We present a descriptive study of patients with these neurosurgical infections during a 5 year period
Methods • Patients who had an infection after brain tumor surgery at our institution from 2010-2014 were retrospectively reviewed after IRB approval • Patients with primary surgery outside the Cleveland clinic or shunt surgery after index tumor surgery and subsequent shunt infection were excluded from study • Total of 75 patients were reviewed including infections after craniotomy (67 patients), after burr hole procedures (5 patients), and after trans-nasal operations (3 patients) • Demographic information, type of intracranial tumor and factors associated with surgery, characteristics of the infection and also re-admission within a year after discharge and mortality were evaluated
Results • Age average was 51 years and 41% were females • Median interval between tumor surgery and diagnosis of infection was 1 month • 72% had post-op wound issues such as wound dehiscence, drainage and pseudo-meningocele • In 10 patients both gram stain and culture were negative and treatment was performed based upon clinical findings • 26 of 75 patients (35%) had re-admissions for recurrent/resistance infection • Out of 20 patients with titanium mesh placement, 10 were readmitted for recurrent/ resistant infection - (50%) • 2 patients (3%) died with 90 days of diagnosis of infection
Conclusions • Staphylococcal infections (MSSA and CONS) are the most common pathogens in post-op infections of brain tumors • The infection recurrence and readmission rate among these patients is relatively high at 35%, and is even greater (50%) in the presence of titanium mesh • With aggressive and appropriate treatment (antibiotics ± wound washout) mortality within 90 days remains relatively low (3%)
Factor No. of patients
Percent
Primary pathology Glioma 31 41% Meningioma 12 16% Metastases 8 11%
Surgery for recurrent tumor 29 39% History of brain radiation before surgery 26 35% Active radiation after index surgery 25 33% Active chemotherapy after index surgery 23 31% Presenting symptoms (alone or in combination)
Wound drainage 28 37% Fever 22 29% Headache 20 27% Neurological deficit 18 24%
LP for diagnosis of infection 37 49% Washout surgery for infection 53 57%
With titanium mesh placement 20 27%
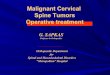
Culture results
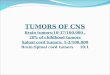
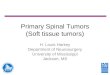
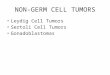
58 year old lady with a history of redo surgery for parasagittal meningioma a few months ago followed by radiation therapy admitted because of minimal drainage from surgical wound. MRI showed a huge epidural abscess (right image). She had washout surgery (culture: P. acnes) with removal of the bone flap and placement of titanium mesh (left image). She was on antibiotics for 6 weeks and successfully treated.
Titanium mesh
Type of infection
Gram stain results
Poster No: 976