Embed Size (px)
Citation preview

Faculdade de Engenharia da Universidade do Porto
Post-Stroke Postural Control: comprehensive analysis towards more competent prediction and rehabilitation
Maria Carolina Fornari
Thesis Plan
Doctoral Program in Biomedical Engineering
Supervisor: Prof. Dr. João Manuel R. S. Tavares (FEUP)
Co-supervisors: Prof. Dr. Andreia P. Sousa (IPP) / Prof. Dr. Marcos Duarte (UFABC)
2017/2018

ii

iii
Abstract
The postural control is the basis to any voluntary or automatic movement. This complex
capability establishes reciprocal actions between sensory and motor systems in order to
ensure postural orientation and balance. The balance assessment provides a clue of the
integrity of the communication between the sensory and motor systems, the neural
mechanisms involved in this process, and how the central nervous system processes,
execute and coordinate postural responses. Quantitative posturography, a useful and
very reliable tool, uses a force platform to evaluate the center of pressure (COP), which
is the result of the forces applied to the ground by the human being. The COP is widely
used in scientific and, increasingly, in the clinical practice, and is competent to make an
accurate diagnosis and to follow rehabilitation of stroke patients with postural control
deficits. Stroke is the main cause of long-term disability and causes impairment in
postural control and gait. Furthermore, the posturography variables applied to predict
functional recovery in stroke may be of interest to rehabilitation professionals in order
to help the prognosis and the planning of the treatment. The main purpose of the PhD
project is to contribute to the improvement and consistency of knowledge of the
postural control system of stroke patients and their relevant functional implications such
as gait and activities of daily living. To address these aims, it is proposed to investigate
posturography variables which are used to evaluate the upright quiet stance of healthy
and stroke individuals and to indicate which ones best characterize these populations,
and among them, which would be more appropriate for scientific and clinical
evaluation. Finally, it is expected to demonstrate which of these variables would be
more predictive of the functional recovery.
Keywords: postural control, balance, center of pressure, stroke, gait, prediction,
rehabilitation.

iv

v
Content
Chapter 1 ............................................................................................................... 1
Introduction ....................................................................................................... 1
1.1 Motivation ........................................................................................... 2
1.2 Research Goals .................................................................................... 4
1.3 Structure of the document ................................................................... 6
Chapter 2 ............................................................................................................... 8
Postural Control ................................................................................................ 8
2.1 Methods of assessment ...................................................................... 10
2.2 Theories ............................................................................................. 11
2.3 Post-stroke ......................................................................................... 13
Chapter 3 ............................................................................................................. 16
State of the Art ................................................................................................ 16
3.1 Variables of the posturography ......................................................... 16
3.2 Variables of the posturography in stroke ........................................... 18
3.2.1 Other implications ....................................................................... 20
3.3 Prediction in stroke recovery ............................................................. 25

vi
Chapter 4 ............................................................................................................. 27
Methods ........................................................................................................... 27
4.1 Work package I .................................................................................. 27
4.2 Work package II ................................................................................ 28
4.3 Work package III ............................................................................... 36
4.4 Work package IV ............................................................................... 37
4.5 Timetable ........................................................................................... 38
Chapter 5 ............................................................................................................. 39
Final Remarks ................................................................................................. 39
References ........................................................................................................... 40

vii
List of figures
Figure 1. World map showing burden of cerebrovascular disease – DALYs
(from [9]). ......................................................................................................................... 3
Figure 2. Location of the 21 reflective markers used to estimate COM and to
investigate the quiet standing kinematics (from Winter el al. [26]). .............................. 32

viii
Abbreviations and symbols
A/D Analogical-digital
AP Anterior-posterior
BBS Berg Functional Balance Scale
BOS Base of support
CNS Central nervous system
COG Center of gravity
COM Center of mass
COP Center of pressure
COPap COP anterior-posterior
COPml COP medial-lateral
CT Computed tomography
DALYs Disability-adjusted life years
EMG Electromyographic
H-reflex Hoffman reflex
ICC Intraclass Correlation Coefficient
ML Medial-lateral
Mmax Maximum M
MRI Magnetic resonance imaging

ix
PCA Principal Component Analysis
PST Postural Stress Test
TUG Timed up and go test

1
Chapter 1
Introduction
The postural control is a complex ability established on the reciprocal action of
the sensory and motor systems [1, 2]. It uses afferent information from visual, vestibular
and somatosensory receptors to detect and control movements and coordinate reflex and
voluntary muscle responses while ensures stability [3, 4], manages postural orientation
and balance [4].
Impairment or damage in any of postural control related system can disturb
balance or motor activities and increase the fall risks. One of these disorders, with
elevated incidence of falls and high personal and social impact, is the stroke.
Stroke is the main cause of long-term disability in the older population [5].
Although its incidence has decreased in recent decades, the absolute number increases
each year [5], including young adult individuals. Consequently, there is a large
influence on activities of daily life, economics, family, psychological, etc. [5].
Studies suggest that posturography is competent to make an accurate diagnosis
and to follow rehabilitation of stroke patients with postural control deficits [6].

2
The posturography uses a force platform to evaluate the center of pressure
(COP), which is the result of the forces applied to the ground by the human being. The
COP is widely used in scientific and, increasingly, in the clinic practice, to evaluate the
postural control of healthy or disabled subjects.
There are many studies in this area, but still, no consensus on which variable
calculated from the COP would best characterize the functioning of the control of
posture and balance [6], especially with alterations caused by stroke.
Studies have shown that patients with stroke have worse stability than healthy
subjects [7], as well as alterations in gait and in the functional activities of daily living.
There is an urgent need to improve the diagnosis, evaluation, and prognosis of
these patients quickly after the stroke, in order to accelerate hospital discharge and the
return to activities of daily living, to avoid the consequences of immobility and hospital
contamination, to reduce expenses and to start soon the rehabilitation process. That is
important to consider that the maximum recovery of these patients occurs within the
first three months after the stroke [8].
1.1 Motivation
The postural control is a relevant scientific and clinical issue because it is an
important requirement for the performance of any voluntary or automatic movement
and functional activities especially gait. However, despite the extensive literature on
biomechanics and neurophysiology of postural control in humans, there is still no
complete understanding.
Extending the study of postural control in individuals with brain lesion and the
comparison with healthy subjects may provide clues to a better comprehension of the

3
biomechanical and neurophysiological mechanisms by which the maintenance of the
posture and balance is operated, contribute to the scientific and clinical assessment and
can help the understanding of functional disabilities that occur with some pathologies
such as stroke, as well as assist the right prognosis and more focused treatment.
A few years ago, per thousand people, more than two had suffered from a stroke,
of which 13% died [5]. Although its incidence has declined in recent decades, the
absolute number increases each year, that is, in 2013 there were almost 11 million
people living with stroke sequelae and approximately 1.5 million deaths [5]. From 1990
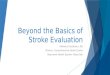
to 2013, there was a 24.4% increase in the disability-adjusted life years (DALYs), what
represents a major impact on personal life, work productivity, and a financial, economic
and social burden [5] (Figure 1).
Figure 1. World map showing burden of cerebrovascular disease – DALYs (from [9]).

4
There were not find many studies in the literature on the quiet upright posture of
stroke patients, principally with a further complete and accurate methodology. Besides,
there is no consensus on which methodology and variables would be most appropriate
in the use of the evaluation of this topic.
The main contribution of this PhD project will be the investigation of
posturography variables never before used in stroke patients (especially COP structural
variables, of which it were found no studies), which will allow further understanding
about the postural control, the mechanisms of neuromotor adaptations caused by
nervous system injury, and the associated functional recovery.
Despite the advances and a large number of studies, the prognosis and
mechanisms of the functional recovery and motor learning after stroke are still not well
established. Additionally, there are few clinical models predictive of motor recovery in
stroke used by rehabilitation professionals.
Accordingly, the posturography variables applied to predict functional recovery
in stroke patients may be of interest to rehabilitation professionals in order to help the
prognosis and the planning of clinical treatment and physical rehabilitation, optimizing
resources, focusing on the real potentials of each patient and appropriate treatment
methods, decreasing anxieties and better instructing the patients, caregivers, and family.
1.2 Research Goals
The main purpose of the PhD project is to contribute to the improvement and
consistency of knowledge of the postural control system of stroke patients and their
relevant functional implications, such as gait and activities of daily living, and
predictive value to motor outcome and recovery.

5
To address these aims, it is proposed to conceive four work packages with the
following objectives:
I - A systematic review of the literature on posturography variables calculated
from the COP raw data, which are used to evaluate the upright quiet stance of healthy
and stroke individuals.
II - A cross-sectional study to evaluate the variables related to the upright quiet
stance used in the literature and selected based on the previous study (systematic
review) in healthy and stroke subjects, with the purpose of establishing which ones best
characterize the populations, and among them, which would be more appropriate for
scientific and clinic evaluation.
A statistical analysis, "Principal Component Analysis" (PCA), will be utilized in
order to eliminate the overlaps and determine the most representative data through
linear combinations of the original variables.
The propose is a more comprehensive methodological approach in order to a
more complex and extensive data interpretation and a better understanding of the
associated events with these nervous system tasks. Therefore, four approaches will be
proposed:
(a) to correlate kinetic to kinematic and electromyographic (EMG) variables;
(b) to compare the COP acquisition of the stroke subjects between one and two
force platforms;
(c) to compare the differences in postural control between right and left
hemisphere lesions;

6
(d) to investigate the Hoffman reflex (H-reflex) in the upright quiet stance of the
stroke subjects (and to correlate with the biomechanics and neurophysiology involved in
postural control).
III – A reliability analysis of the protocol and variables studied in the works
described above, through "Intraclass Correlation Coefficient" (ICC) [10].
The intrarater and test-retest reliability will be tested (subjects will be
reevaluated after 72 hours of the first collection).
IV – A longitudinal study through the follow-up of stroke patients during the
rehabilitation process. Subjects will be reassessed 1, 3, 6 and 12 months after the first
evaluation. It will be demonstrated which of the investigated variables in the cross-
sectional study (item 2) would be more predictive of the functional gait recovery,
through the correlation with Fugl-Meyer Scale and gait parameters, such as speed,
cadence and limb coordination.
It is intended to correlate the posturography with Magnetic resonance imaging
(MRI) data.
Finally, it is expected to develop a model (or a database) that provides a
prediction of gait recovery in order to support the prognosis and rehabilitation planning
(or a more quantitative and reliable method of assessing postural control and balance for
physiotherapists).
1.3 Structure of the document
The current document has four more chapters:

7
Chapter 2, exposes the basic information about the postural control and
assessment methods, particularly in stroke patients.
Chapter 3, relates the state of art of the methodology and variables studied by the
posturography of healthy subjects and with AVE, and clinical predictive models for
motor recovery from stroke patients.
Chapter 4, explains the methodology and procedures that will be used on the
PhD project and related studies. The work packages are comprehensively described and
presented at the timetable.
Chapter 5, presents the final remarks and future expectations.

8
Chapter 2
Postural Control
The central nervous system (CNS) coordinates and integrates vital and physical
functions, processes information and provides responses. It receives inputs from many
types of sensory receptors, integrates them with past experiences and other sources,
plans and executes actions. The nerves of the peripheral nervous system communicate
the CNS – cerebral cortex and spinal cord – with the inputs of the different parts of the
body [11].
The cerebral cortex is the major responsible structure for motor control through
the planning, processing and execution of commands. The spinal cord and brainstem
help coordinate reflex and voluntary movements, with the assistance of other
subcortical structures such as the cerebellum and basal ganglia [11, 12].
An essential motor system topic is the postural control, which is the basis to any
voluntary or automatic movement and a complex capability established on reciprocal
action of sensory and motor systems [1, 2]. The postural control is involved in several
subsystems: nervous, sensory, biomechanical and muscular.

9
The fundamental aims of postural control are postural orientation and balance [4,
13]. The postural orientation requires the biomechanical alignment of the body and its
position in the environment and its relations with gravity, base of support (BOS), visual
field, internal references, memory, etc. [1, 4]. Balance involves the coordination of
movement strategies to maintain the center of mass (COM) within the BOS during
externally provoked and self-initiated postural disturbances [1, 12].
Postural control uses afferent information from visual, vestibular and
somatosensory receptors to detect and control movements and coordinate reflex and
voluntary muscle responses while ensures stability [3, 4, 14]. Afferent signals are sent
to the cortical motor centers in order to the cortex can be able to process the actual
requests for balance and postural control, and to send efferent signals if was required
[15].
The CNS operates two essential mechanisms to control balance: anticipatory or
proactive mechanisms and compensatory or reactive mechanisms [13].
Anticipatory postural adjustments maintain the postural stability in response to a
predictable disturbance, external – adjustment based on past experience [4] – or due to
voluntary movements [16]. This anticipatory mechanism is related to several factors:
expected magnitude and direction of the displacement, voluntary action associated with
the perturbation, current postural condition, past experiences and practice.
On the other hand, compensatory mechanisms are automatic or reflex responses
to unexpected external disturbances [13] or failures of anticipatory adjustments. These
adjustments are usually extremely fast, and the specific strategy used depends on the
characteristics of the external postural displacement, the individual's expectations and
previous experiences [1].

10
This chapter aims to present the postural control theory, associated mechanisms,
and methods of evaluation, its impairments with stroke and the consequences in gait and
functionality.
2.1 Methods of assessment
The balance assessment provides a clue of the integrity of the communication
between the sensory and motor systems because external postural responses quantify
how much the motor system is able to respond to a particular sensory stimulus pattern,
how much the CNS is prepared and adapted for different disturbances, and how well it
is able to learn, execute and coordinate preplanned motor patterns. This evaluation also
allows the inference of the neural mechanisms involved in the process of postural
control, and their coordination to ensure postural orientation and balance.
However, despite the extensive literature on postural control in healthy and
disabled subjects, the assessment of postural adjustments remains difficult to perform
because of the complexity of postural control. Several instruments were developed in
attempt to identify the neural, cortical or subcortical mechanisms underlying this control
[3].
There are simple methods that make predictions of postural stability, as
retropulsion test [17], widely used in clinical practice; the "Postural Stress Test" (PST) –
a more reliable version of the retropulsion test [18, 19]; Berg Functional Balance Scale
(BBS), used to quantify the risk of falls in the elderly [20, 21]; Tinetti test, Mini
Balance Evaluation Systems Test; Timed up and go test (TUG); Unified Balance Scale
and others [1].

11
These methods are accessible to any examiner, but they have some
disadvantages, such as the difficulty of reproducibility and standardization for different
masses and heights of the subjects, and they are not useful for the identification of the
physiology involved in the regulation of posture.
Further, these tests are not useful for assessing the performance of any
population since they distinguish only high balance deficits [22].
Currently, more elaborate methodologies have been developed to identify the
influence of sensory inputs and the efficiency of muscle activity in the postural control.
Quantitative posturography, a useful and very reliable tool, uses high technology
to measure ground reaction forces in the BOS by a force platform, EMG and kinematic
patterns and biomechanical analysis related to various motor tasks or to different types
of disturbances [17, 23].
2.2 Theories
Despite the development of sophisticated methods for assessment of postural
control and intense research in this area, there is still no consensus about the
biomechanical and neural mechanisms underlying the control of posture and balance.
The complexity of human postural control is very high due to the involvement of
several subsystems: neural, sensory, biomechanical and muscular.
The literature suggests that neuronal signals sent by stretching or shortening
muscle length alone are insufficient for controlling upright posture [24], consequently,
only a combination of afferent inputs can provide the information necessary to control
body balance [25].

12
However, Winter et al. [26] argue that static postural control is maintained only
by the stiffness of the musculoskeletal apparatus. But this statement was debated by
several authors [27, 28].
Morasso et al. [29] indicated that the stiffness of ankle muscles is insufficient to
stabilize the body, suggesting an important role of muscle and sensory receptors foot
plant in controlling human posture. They advocate an anticipatory control of posture
without, however, eliminating the contribution of stiffness of the musculoskeletal
system. They therefore believe in a synergy of these mechanisms.
Presumably, the muscle tonus also contributes to the standing posture [30], but
there is no agreement in the literature about the importance of the active or passive
contribution in the tonus generation.
Some studies shows a dominant role of active mechanisms [25], and others a
predominant contribution of passive mechanisms [31].
Although quiet erect posture could be possible only due to the mechanical
rigidity of the muscles, still, it is verified that the vertical balance is a delicate state. Any
movement of the center of gravity (COG), even if it does not shift the balance is
detected by afferent signals and compensated by the contraction of the postural muscles.
Since all forces in a standing individual are transmitted to the foot, postural reflexes
often involve the contraction of many muscles and are more complex than a simple
stretch reflex [12].
The postural control involves both spinal reflexes and longer loops, more
adaptable and recent phylogenetically related to the motor cortex, brainstem and
cerebellum [11, 12, 25].
Studies indicate that higher cortical structures also play an important role in the
regulation of balance in static and dynamic conditions [32]. It is observed that the

13
superior cortical functions related to the posture are linked to the human cognitive
processing. The amount of cognitive processing required for postural control depends
on both the complexity of the postural task and the capacity of the subject's postural
control system [1].
Systems theory suggests that postural control is given by the interaction between
the individual, task and environment, assuming that the ability to control the position of
the body in space comes from the complex interaction between the musculoskeletal and
neural systems [33]. Accordingly with this theory, the maintenance of the quiet upright
posture requires the synergic muscle activation of the two sides of the legs so that the
COM stays within the BOS [34], and there is evidence that this interlimb coordination is
mediated by spinal cord circuits, which are under supraspinal control [35].
The models and theories of postural control have not yet been completely tested
and proven and present many conflicting aspects, so this discussion is still very
vigorous in the scientific community.
2.3 Post-stroke
Studies have shown that patients with stroke have worse stability than healthy
subjects [7], alterations in gait and a greater probability of fall. Several factors may be
associated: biomechanical malalignment, muscle weakness, altered muscle tone and
sensitivity, visual or vestibular deficits, limitations in joint range of motion, emotional
factors as fear of falling, and deficits of attention [5].
In clinical practice, the following changes related to post-stroke postural control
and balance were reported: worse balance stability in the frontal plane, different weight
discharge in the right and left limbs [36], lower efficiency of the postural adjustments,

14
stereotyped muscle synergies to disturbances, inadequate muscular activity of lower
limbs and trunk [17, 37-39], and greater difficulty in compensatory adjustments [40].
Many researchers are interested in finding better ways of approaching diagnosis
and treatment of stroke effects that cause equilibrium deficits [2, 41]. The study and
better understanding of the multiple mechanisms underlying the postural control can
help the evaluation of patients with balance deficits, understanding of functional
compensations and effective rehabilitation of balance to improve mobility and prevent
falls.
The results of this study by Rongies et al. [6] indicate that posturography is
competent to make an accurate diagnosis and even to follow the motor and functional
recovery of stroke patients with postural control deficits.
Concerning the posturography, the literature suggests that the lower the area of
postural oscillation (i.e., the amplitude of the area of oscillation of the COP), the better
the control of postural stability [42].
In patients with stroke, many changes were observed in the parameters
associated with the force platform, such as: deviations of the COP to the non-paretic
limb [43], higher frequency of COP oscillation [40], higher COP velocity [44], greater
COP area and amplitude [45, 46], difference in COP amplitude between right and left
lower limbs [47], differences in COP parameters between patients with left and right
hemisphere lesions [48].
Several studies have compared clinical tests with global posturography
variables. Pyoria et al. [36] found correlations between higher velocities of oscillation
with scores in the Functional Standing Balance Scale that indicates equilibrium deficit.

15
These disorders in the postural and balance control of stroke patients,
concurrently with other complications, contribute to impairment in gait and
performance of functional activities of daily living.
Although the variations of gait patterns of the stroke patients vary with the
location and extent of the injury, as well as the time after stroke and recovery and
rehabilitation process [49], the literature reports: gait asymmetry, reduced walking
speed, inadequate propulsion of the paretic limb, reduced stance phase and prolonged
swing of the paretic limb, alterations of COM trajectory, synergic patterns of muscle
contraction of the paretic limb, rather than individual control of each joint, more co-
contractions during the stance, among other changes [49, 50].

16
Chapter 3
State of the Art
3.1 Variables of the posturography
Many experiments have already been carried out based on the behavior of the
COP and muscular activity in upright static situations [22]. The COP is the point of
application of the resultant of the vertical forces acting on the BOS, and represents a
combined result of the postural control system and the force of gravity. Some authors
consider the COP a response of the CNS to adjust the oscillations of the COM in the
erect posture [38].
It is called posturography or stabilography the measurement and record of the
human postural oscillation.
Static posturography studies the upright quiet posture when the subject tries to
stay without any movements; and the dynamics posturography evaluates the subject's
response when a disturbance is applied [51, 52].
Force platform studies have shown that evoked responses by disturbance provide
excellent examples of the complexity of postural adjustments. Behaviors vary according

17
to the instability of the surface and the force of the disturbance. Thus, postural reactions
caused by equilibrium disturbances through different paradigms have been studied [17].
Some of the variables used to examine the behavior of the forces in upright static
posture are areas of trajectory of the COP, velocity and amplitude of displacement,
standard deviation and normalized root mean square.
However, according to a literature review [22], most studies related to the
evaluation of postural control choose techniques, methods, and quantitative variables,
not taking into account the studied population, the goal of the postural task, and the
conditions of the environment.
Usually, raw data of the COP displacement is only used for visual
representations and construction of statokinesigram and stabilogram. It is necessary to
calculate other variables of the COP to intensify the analysis of the mechanisms
involved in the postural system [22].
Global variables are represented by the magnitude of the resultant or
components anterior-posterior (AP) and medial-lateral (ML) of COP (COPap and
COPml, respectively) in terms of time or frequency. Generally, it is considered that
lower the magnitude or deviation of these variables, better the postural stability [22].
The variable considered more reliable and sensitive in the study of postural control is
the velocity of the COP, which reflects the efficiency of the postural control system
[22], and may have a major role in the feedforward mechanisms during quiet stance.
But these variables are not sensitive to other components of COP that could
provide important data to understand the complexity of the functioning of postural
control. Some studies have developed structural variables, which are decomposition of
the COP oscillation patterns, for example, rambling and trembling [53] and fractal
analysis of the COP [22]. Though, these theoretical considerations are not yet entirely

18
tested and confirmed. It is still necessary to expand the analysis of all the components
related to the postural control system for the real understanding of its function.
3.2 Variables of the posturography in stroke
Usually the studies about stroke postural control evaluate only some of the
global COP variables.
Wei et al. [7] evaluated, with two platforms, only the standard deviation of the
COPap and COPml displacement of the stroke patients. Rongies et al. [6] only studied
the following variables: COG mean, oscillation amplitude, and area.
In the study of Gasq [54], the variables investigated were: mean and standard
deviation of COP velocity, COPap and COPml mean velocity, area of the 90%
confidence ellipse enclosing COP, absolute value of the mean COPml position, in order
to evaluate the weight-bearing asymmetry. All variables presented a good level of
agreement, except the area and COPml. The area presented low reliability, and the
absolute value of mean COP was not reliable in the study.
The study of Nardone et al. [43] evaluated the postural stability of stroke
patients with a single force platform. Only four variables were evaluated: COPap and
COPml mean position; Area; and COP sway. It has been reported that the area and
length of COP displacement were greater in subjects with stroke than controls, and that
COPml drifted further to the side of the non-paretic limb. But an interesting result was
the correlation between COPml asymmetry and lower limb strength (by the Motricity
index scale). As there was no correlation with spasticity, they conclude that spasticity
alone does not explain the altered balance in these patients, which could primarily be

19
explained by alteration of descending cortical signals that control the activation of
motor neurons related to the postural musculature [43].
Gray et al. [44] evaluated the following variables: COP mean velocity, area,
COPap and COPml amplitude. They tested the reliability of the measures with two
force platforms in patients with stroke. The COP mean velocity was the most reliable
variable. They recommend making more than one attempt to improve reliability but
avoid stroke patient fatigue.
Sawacha et al. [55] correlated the following balance tests: Fugl-Meyer, Motricity
Index, Trunk Control Test, Functional Independence Measure, TUG, BBS, and Tinetti
with some COP variables (ellipse, sway area, path and velocity in both directions, AP
and ML). And there were significant differences between healthy and stroke subjects
with open eyes. With closed eyes there was only a difference between parameters
related to COPap and velocity. They argue that CNS post-stroke adapts to maintain the
ML position with eyes closed because of the proprioceptive deficiency, and, therefore,
there was no difference with controls. But in opposition to other studies, they used only
one force platform. They also reported correlations of the tests with a few variables,
showing that clinical tests and posturography evaluate different aspects of the postural
control system [55].
Niam et al. [37], correlated some global variables (COPap and COPml velocity,
RMS velocity, RMS amplitude, COPap and COPml mean frequency) with BBS.
However, only the COPap velocity showed correlation. Their conclusions emphasize
the importance of evaluating the AP and ML directions separately, chose carefully the
parameters, and not use the posturography data alone to make statements [37].
There is, consequently, a requirement of a more comprehensive methodology,
including EMG and kinematic data.

20
The study by Roerdink et al. [56] evaluated variables derived from the
dynamical systems, to verify if they add value to the analysis of the conventional
posturography parameters. Among a lot of results and inferences, they reported a
decrease in local stability in stroke patients, which they interpreted as a deterioration of
the neuromuscular control system, and a reduced ability to compensate for minor
disturbances.
They also suggested that the postural system of healthy subjects is more
concerned with the maintenance of the AP balance (which presents greater oscillation
and greater regularity) and the system of stroke subjects is more concerned with the
oscillation in the ML direction [56].
A more comprehensive interpretation could infer that greater oscillation in the
ML direction is due to a greater contribution of the proximal muscles of legs and the
trunk than distal muscles, which are generally more impaired in stroke.
These results corroborate with the importance of EMG evaluation with the
posturography data.
Besides, there was found no agreement in these studies, and there were no
research about COP structural variables in the stroke population.
3.2.1 Other implications
a. Interlimb coordination
An earliest study of Sherrington [57], initiated investigations into interlimb
coordination and demonstrated reflex interconnections between the cervical and lumbar
cat´s cord, that is, between the front and rear limbs during stance and walking. Many
authors have studied spinal cord quadruped coordination [58]; however, it is known that

21
the regulation of posture and bipedal gait has fundamental differences, requiring
specific neuronal mechanisms to maintain the body in an upright position.
Among the movements, one of the most studied is certainly the human gait [24],
since the cross responses really have great importance in locomotion. However, few
studies have been found in the literature on interlimb coordination during maintenance
of human orthostatic posture.
Dietz studied spinal cord coordination in humans through displacements in the
quiet erect posture [35]. When only one leg was stimulated, EMG responses for
recovery of balance were very symmetrical in both sides. The minimal movement at the
contralateral ankle joint suggests that these crossed responses come from the displaced
leg signals. However, when contralateral leg is not supporting the body, its muscles
were not activated [35], so they are not connected to a postural program [59].
Short-latency responses are not the same under different conditions: muscle
activation patterns are highly specific for different motor tasks [35].
It was also verified that, after bilateral perturbations in opposite directions, linear
subtraction of EMG responses occurred, that is, activation was induced in the agonist
muscle of one leg and contralateral coactivation in the antagonist - mutual reciprocal
inhibition in the respective antagonists of each activated muscle [35]. The greater the
postural destabilization caused by the disturbance, the greater the degree of muscular
activation. Therefore, lower limbs act synergistically, that is, each limb affects the
activation force and the temporospatial behavior of the other limb.
This coordination between the lower limbs must have a spinal cord origin,
mediated by a few interneurons, because the latencies after the stimulus, approximately
75 to 100 ms, are compatible with propagation in afferents associated with type II
endings of the neuromuscular spindles [35]. Schieppati and Nardone [60] performed a

22
series of investigations that point to an important role of type II afferent fibers in the
medium latency component of the human stretching reflex, particularly in the reflex
response of anti-gravity muscles, evoked by disturbances in upright quiet posture.
In addition, no cross excitatory effects from Ia fibers are known in
humans. Disturbances in a single leg do not elicit short latency responses, mediated by
fibers Ia, in the muscles of the undisturbed leg. On the other hand, the medium latency
responses are elicited bilaterally, what is compatible with the hypothesis of the
transmission by type II fibers [60].
Therefore, despite the monosynaptic stretching reflexes do not play an important
role during postural disorders [15], it can be affirmed that afferent feedback and reflexes
have a significant function in the regulation of coordination between members [61].
However, this spinal coordination system, probably mediated by type II afferent
fibers, seems to be under higher influence [35]. The spinal mechanism does not receive
sensory information about body orientation, for instance. Its function is the transmission
of the supraspinal commands about motor patterns of postural corrections. Supraspinal
structures receive information from the vestibular system about orientation of the body
and generate commands for postural corrections [58].
It was reported that, after disturbances of the upright position, patients with
spasticity presented delayed and decreased EMG responses in comparison with healthy
subjects, and the reduction of EMG was correlated with the severity of paresis [62].
There is no evidence that transcortical pathways contribute to the long latency reflexes
observed in lower limbs [15]. Thus, this corroborate with a supraspinal influence on the
spinal reflex pathways. Dietz et al. [15] suggested that the afferent signals are sent to the
cortical motor centers in order to the cortex can be able to process the actual requests
for balance and postural control, and to send efferent signals if was required.

23
The comprehensive analysis of interlimb coordination of the stroke individuals
in association with the investigation of the reflex pathways, through the measurement
and analysis of H-reflex during the maintenance of quiet standing posture, could
provide clues about neurophysiological mechanisms involved in the control of posture
and the dysfunctions occurring in the nervous system with brain injury (approach ‘d’ of
work package II).
Dickstein and Abulaffio [63] evaluated the coordination between hip and leg
oscillation and between the paretic and non-paretic limbs of stroke patients and control
subjects. An asymmetry was found between limbs in the patients, with greater
oscillation in the paretic limb. They also found a synchronization deficit between the
movements of the hips and legs of the same limbs of the patients. It has been reported a
correlation between the oscillation of the hips of both limbs but not of the legs,
suggesting a more pronounced deficit in stabilizing more distal segments in the paretic
leg of these patients, as verified in clinical practice. Nevertheless, they did not correlate
these data with posturography data.
A study by Wei et al. [7] has shown that patients with stroke have poorer
coordination between members in the AP direction. Notably, the coordination between
members improves with the eyes closed perhaps because the system tries to compensate
the absence of an important sensory afferent. They also found greater oscillation in the
non-paretic leg than the paretic, but did not correlate these data with muscle activation.
They suggested that the system attempts to maintain equilibrium by increasing the
adjustments in the non-paretic limb, and therefore, a greater oscillation demonstrates a
greater CNS action [7]. However, this result could be due to a decrease of the muscular
activity by the injury in the cortex motor area.

24
The comparison of COP behavior between one and two force platforms, with
EMG and kinematic data, can provide valuable information for the comprehension of
interlimb coordination in stroke quiet standing (approaches ‘a’ and ‘b’ of work package
II).
b. Differences between lesions in the left and right hemispheres
Another important question is about the sample of evaluated stroke patients,
which is always highly heterogeneous.
Fernandes et al. [48] compared postural control of hemiparetic patients on the
right and left. Although patients exhibited similar scores in clinical tests, patients with
right hemisphere lesions presented bigger changes in posturography data compared to
patients with a left lesion, in accordance with others studies [37, 64]. Since they did not
find a correlation in the sensory system manipulations (without vision and alteration in
proprioception) between healthy subjects and patients, it was suggested that this
alteration would not be explained by a specialization of the right hemisphere in
somatosensory processing, but by a change in the generation of descending responses.
Thus, the right hemisphere would be more specialized in maintaining the quiet posture
(which requires small adjustments of the body to maintain balance).
It has been suggested that these adjustments would be related to muscle intrinsic
stiffness and viscosity [48].
From these data, it will be interesting to evaluate the stiffness in the quiet upright
posture in the stroke population. The stiffness can be calculated from kinematic data,
according to the methodology of Winter et al. [26].
They also argue that there was no difference in muscle activation of the non-
paretic leg of patients compared to healthy subjects, but it was not concluded whether it

25
is a normal activation or CNS recovery process (to compensate for paretic leg deficit)
[48]. The literature suggests that the ipsilateral limb to the lesion would also suffer
deficits through uncrossed neural pathways [49]. This could be tested by comparing
patients with acute and chronic stroke.
Considering that the brain lesions caused by stroke are always very specific and
in different locations, it is necessary a better characterization of these subjects and a
separation between two groups: the patients with right and with left lesion (approach ‘c’
of work package II).
3.3 Prediction in stroke recovery
Predicting motor recovery, despite being better known in medical practice, is
still limited adopted or not well understood by physiotherapists [65, 66].
There are many tools for clinicians described in the literature and used in clinical
practice, however, the quantity and application of instruments that can guide or predict
the prognosis and assist in the planning of an effective and optimized treatment is still
very limited in physiotherapeutic practice.
This study by Eghidemwivbie and Schneeweis [67] has shown that
physiotherapists are able to make predictions about the outcome of walking and daily
living activities, and that this prediction is extremely useful in determining the treatment
plan and orientation to the patients and their relatives. The earlier this prediction is
made, the results tend to be more accurate. However, there is a lack of tools to assist or
guide this process, and it is recommended to use statistical models for appropriate
prognosis and treatment plans [67].

26
The result of a systematic review has suggested that neuroimaging data may be
useful in predicting motor recovery of upper limbs, but there is no strong evidence that
models with such data are better than models with clinical data or that adding
neuroimaging data improves such prediction [68]. Besides, to date, none of the
prediction models for walking have been validated [68].
The meta-analysis of Fahey et al. [39] did not identify any impact assessment
study, as randomized follow-up or cross-sectional, or any of the study assessments of
utility, such as decision curve analysis. However, more than half of the models included
in this review would need studies that focus on additional validation using different
external cohorts, improving the accuracy reported by refinement models, and
significantly evaluating the impact of models in the clinic.
Those who wish to predict the outcome of stroke are advised to build on
previous work, to update and adapt validated models to their specific contexts rather
than to build new models. Although this study identified precise predictive risk factors
for mortality and recovery, its usefulness remains uncertain [39].

27
Chapter 4
Methods
The following will describe in detail the methodologies that will be applied to
achieve the objectives described in chapter 1, namely: a systematic review, cross-
sectional study, reliability study, and longitudinal study.
4.1 Work package I
A systematic review will be divided into two parts:
The first one will review and study the papers about posturography variables
used to evaluate the upright quiet stance in healthy individuals.
A search will be performed on the databases: MedLine, ISI Web of Sciences,
and Scopus. The following keywords will be used:
((postural AND control) OR balance OR posture OR standing) AND ((upright
OR orthostatic) AND quiet) AND (posturography OR stabilography OR (force AND
platform) OR (center AND pressure) OR COP).

28
The second review will be about the variables used to investigate the postural
control of stroke patients. The same databases will be used for searching. To the
keywords will be added "stroke":
stroke AND ((postural AND control) OR balance OR posture OR standing)
AND ((upright OR orthostatic) AND quiet) AND (posturography OR stabilography OR
(force AND platform) OR (center AND pressure) OR COP).
Only articles that evaluate the upright quiet stance, in force platform (and not
other devices) in healthy subjects, without any pathology, will be selected.
The following criteria of inclusion will be established: 1) the study must be
written in English; 2) studies with different main focus will be excluded.
4.2 Work package II
This second study will be the experimental analysis of the COP variables.
Subjects
It will be made a statistic approach, to determine the minimum quantity of the
sample of the acute stroke subjects necessary to reliable results.
The stroke subjects will be divided into two groups: patients with right
hemisphere lesion and patients with left hemisphere lesion (verified by computed
tomography – CT – or MRI).
A group of control subjects with matched age, weight and height will be
evaluated for comparison.

29
For the selection of patients and data collection, some agreements will be made
with institutions, namely Centro de Estudos de Movimento e Actividade Humana da
Escola Superior de Tecnologia da Saúde do Instituto Politécnico do Porto, Centro de
Reabilitação Profissional de Gaia, Hospital São João. Other laboratories and clinical
centers will be considered if necessary.
The inclusion criteria for the group of patients will be: (1) hemiparesis due to a
first ischemic stroke in the territory of the middle cerebral artery visualized by CT or
MRI; (2) have the ability to stand without assistance, but with supervision if necessary.
The exclusion criteria will be: (1) cognitive deficits that prevent understanding
and cooperation in the tests (evaluated by the Mini Mental State Examination); (2)
history of orthopedic or neurological disorders (other than stroke); (3) history of stroke
involving the brainstem or cerebellar areas; and (4) taking medications that may affect
motor performance.
As selection criteria for the control group, it will be necessary that the individual
does not present antecedents or current history of neurological pathologies or articular
deformities.
The project will be submitted to the Ethics Committee of the Instituto
Politécnico do Porto, in accordance with the Declaration of Helsinki. All subjects will
sign an informed consent form to participate in the experiments.
Local
The experiments will be performed in the Centro de Estudos de Movimento e
Actividade Humana da Escola Superior de Tecnologia da Saúde do Instituto
Politécnico do Porto.

30
Materials and equipment
Force Platform
Two force platforms, model FP4060-10 from Bertec Corporation (USA),
connected to a Bertec AM 6300 amplifier, with default gains, and at 1000 Hz sampling
rate, will be used. The amplifier will be connected to a Biopac 16 bit analogical-digital
(A/D) converter from Biopac Systems, Inc. (USA).
EMG
For the EMG activity will be used the model MP 100 Workstation from Biopac
Systems, Inc. (USA), with a sampling rate of 1000 Hz and an amplified band-pass filter
between 10-500 Hz.
Data will be collected using steel electrodes, model TSD150 from Biopac
Systems, Inc. (USA), bipolar configuration, with an 11.4 mm contact area and an inter-
electrode distance of 20 mm, and a ground electrode.
Prior to the placement of the electrodes, the skin will be cleaned with 90%
alcohol and prepared with an abrasive solution. The electrodes will be firmly fixed with
an anti-allergic tape, and an electrolytic gel will be used to contact the skin. The skin
impedance will be measured and should have a maximum of 20 kΩ.
The following convention [69] will be adopted for the positioning of the
electrodes in the muscles (both sides), reported in the literature with an important role in
maintaining the posture:
Tibialis Anterior, 1/3 on the line between the tip of the tibia and the tip of the
medial malleolus;

31
Soleus, 2 cm distal to the lower border of the medial gastrocnemius muscle belly
and 2 cm medial to the posterior midline of the leg;
Medial Gastrocnemius, most prominent bulge of the muscle;
Rectus Femoris, 1/2 on the line from the anterior spina iliaca to the superior
border of the patella;
Vastus Medialis, 4 cm above the patella upper border and 3 cm measured
medially and oriented 55º to a reference line drawn between the right anterior-superior
iliac spine and the patella center;
Biceps Femoris, 1/2 on the line from the ischial tuberosity and the lateral
epicondyle of the tibia;
Rectus Abdominis, 3 cm to the right of the umbilicus;
Erector spinae, 2 finger width lateral from the spinous process of L1.
Video Cameras
The software Qualysis Track Manager will capture video from seven high speed
cameras.
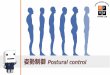
Twenty-one reflective markers will be placed on the legs, thighs, lower arms,
upper arms, pelvis, and trunk, according to Winter et al. [26], because this is the
approach to calculate the stiffness, one variable of interest in this work (Figure 2).

32
Figure 2. Location of the 21 reflective markers used to estimate COM and to investigate the quiet standing
kinematics (from Winter el al. [26]).
Procedures
The stroke patients will be evaluated with the Fugl-Meyer Assessment by a
trained physiotherapist.
Then, in the orthostatic posture, the EMG surface electrodes will be placed on
the subject, and then the reflective markers will be attached at the mentioned anatomical
points above.
First, the subject will stand on one force platform, with the two feet, assuming a
quiet upright stance with the feet positioned as comfortable as possible. The anterior

33
and lateral limits of the feet shall be demarcated with adhesive tape so that the
individual returns to the same position in subsequent trials.
The subject will be asked to remain in the orthostatic position as still as possible
for 60 s. There will be three trials with open eyes and three trials with eyes closed.
Between each trial, there will be a rest period of two minutes. When the subject
stands up, there will be a period of 10 to 15 s in order to stabilize before starting each
acquisition.
Two force platforms
Second, the subject will stand on two force platforms with one foot in each one.
The anterior and lateral limits of the feet shall be demarcated again, and the same
instructions and protocols will be performed.
Gait analysis
Following another rest period, all subjects will be required to walk, with a
preferred speed (self-selected), for 10 m along a force platform located in the middle of
the walkway. The subjects will be barefoot and will look forward, walking as naturally
as possible. There will be a previous practice in order that only one foot at a time have
full contact with the platform, and there will be no extra pressure of any other kind on
the platform [70].
H-reflex
Another group of stroke patients will be selected for the H-reflex approach in
order to avoid fatigue. The subject characteristics and inclusion/exclusion criteria will
be the same described above.

34
The tibial nerve will be stimulated with an electrical stimulator MEB 4200, by a
surface electrode with a cathode of 5 mm diameter, fixed to both legs, in the popliteal
fossa. The anode will be attached on the patella.
The stimulus intensity will be determined for each leg that causes an H-reflex
amplitude equal to about 20% of the corresponding maximum M (Mmax) amplitude
response. All trains of stimuli used in the experiments will be at 1 Hz. The electrical
stimulation will follow the model used to capture the reflex of the soleus described by
Mezzarane & Kohn [71].
The subjects will be positioned in the sitting posture with the lower limbs in
extension supported in a seat (no knee flexion will be allowed during the experiment in
order to avoid displacement of the stimulation electrode). In this position, the Mmax
wave of the soleus muscle will be determined through pulses of 1 ms duration. It will be
selected a current intensity which can evoke an H wave of 20% of the Mmax wave.
As in the above protocol, the subject will stand on two force platforms. The
anterior and lateral limits of the feet will be demarcated.
The subject will be asked to remain in the orthostatic posture as still as possible
for 60 s. Around the 20 s of acquisition, a moment unknown to the subject so that he
does not anticipate any reaction, the experimenter will release an electrical stimulus of
the determined intensity. After the stimulus, the acquisition will be completed with a
total time of 60 s. Then, the subject will be asked to sit in a comfortable armchair for 2
min rest. The amplitude of the H wave will be measured in real time.
The experiment will be replicated as many times as necessary so that three
acquisitions are obtained in which the value of the H-reflex amplitude is equal to that
determined value. Three acquisitions will be recorded with eyes open and three with
eyes closed.

35
Analysis of the results
After the conclusion of the trials, the acquisition of the maximum voluntary
contraction of all muscles bilaterally, for normalization of the EMG signals, will be
performed [72].
Subjects will be encouraged to perform maximum force through verbal stimuli
of the experimenter. Only after the beginning of the activity by the subject, the
experimenter will begin the collection. It will be collected 5 s of EMG and saved in the
DataWave environment. For the estimation of the CVM, a time window will be taken
from the middle of the captured period, since the data are more constant, and therefore,
more reliable in this interval.
The signals will be recorded on the personal computer and converted to a text
file so that they can be evaluated via the Matlab software, which will be used for all
tasks of signals visualization and processing and graphics production.
The EMG signals will be normalized, rectified and filtered so that the
observation of the patterns of the muscular activities is facilitated.
The platform signals will be calibrated and converted into units of force
(Newton) and moments of force (Newton x meter). The COP on the foot surface will be
calculated from them, although in this research it will also be included in the analysis
the basic variables provided by the platform (forces and moments), which may help for
a better understanding of the mechanisms involved.
The images of the cameras will be paired with the EMG and the force platform
signals.
The gait data will be used in work package IV.

36
Firstly, the various captured and processed signals will be evaluated individually
for each subject and their mean and standard error will serve to characterize the
individual and its intrinsic variability. In the set of individuals, an analysis of inter-
subject variability will be made.
Comparisons will be made between the three groups (right stroke, left stroke,
and control), between the data from one and two force platforms, and between the
paretic and non-paretic leg of the stroke subjects. Correlations between the kinetic,
EMG and kinematic data will be performed.
A statistical procedure, PCA, will be performed to eliminate the overlaps and
determine the most representative data through linear combinations of the original
variables of the groups.
The statistical analysis will be performed in the Minitab environment with a
significance level of 0.05.
4.3 Work package III
The evaluated variables in the work package II will be tested for reliability.
For this, the subjects will be assessed 72 hours after the first evaluation, with the
same protocol.
A statistical treatment of concordance analysis will be done through the ICC
procedure.
The statistical analysis will be performed in the Minitab environment with a
significance level of 0.05.

37
4.4 Work package IV
The procedure of the work package II will be replicated in stroke group after 1,
3, 6 and 12 months.
It will be verified which variables would be predictive of motor recovery
through:
- the collected posturographic data will be correlated with the Fugl-Meyer score.
- correlation between the gait parameters, such as (speed, cadence and limb
coordination) and posturography.
An attempt will be made to create a model or program that will assist in
evaluation, prognosis, and treatment plan of the stroke patients.

38
4.5 Timetable
Work package I Work package II Work package III Work package IV Thesis
Systematic review Cross-sectional study Reliability analysis Longitudinal study
2018 2019 2019 2020 2020
JUL AGO SET OUT NOV DEZ JAN FEV MAR ABR MAI JUN JUL AGO SET OUT NOV DEZ JAN FEV MAR ABR MAI JUN JUL AGO SET OUT NOV DEZ
Literature review
Reading Writing
Variable analysis
Writing
Variable analysis
Writing
Variable analysis
Writing
Thesis writing
Ethics Committee
First data collection
Data processing
Ethics Committee
First data collection
Data processing
X
Data collection Data
processing

39
Chapter 5
Final Remarks
In this PhD project, it is intended to settle a posturographic protocol that could
be used in the evaluation of the postural control in both healthy or disabled individuals,
highlighting which the variables calculated from raw COP data would best characterize
and discriminate different populations or tasks in an upright postural, such as quiet
standing.
The second expectation is to create a tool, from the posturography data, for
evaluation and prediction of the motor recovery of patients with stroke, which, in the
future, could be extended to other pathologies or contexts.

40
References
[1] F. B. Horak, "Postural orientation and equilibrium: what do we need to know
about neural control of balance to prevent falls?," Age Ageing, vol. 35 Suppl 2,
pp. ii7-ii11, Sep 2006.
[2] D. A. Winter, A.B.C. (Anatomy, Biomechanics, and Control) of Balance during
Standing and Walking. Waterloo, Ontario: Waterloo Biomechanics, 1995.
[3] F. B. Horak, "Clinical measurement of postural control in adults," Physical
Therapy, vol. 67, pp. 1881-5, 1987.
[4] A. Shumway-Cook and M. H. Woollacott, Motor control : theory and practical
applications. Philadelphia Lippincott Williams & Wilkins, 2001.
[5] R. V. Krishnamurthi, A. E. Moran, V. L. Feigin, S. Barker-Collo, B. Norrving,
G. A. Mensah, et al., "Stroke Prevalence, Mortality and Disability-Adjusted Life
Years in Adults Aged 20-64 Years in 1990-2013: Data from the Global Burden
of Disease 2013 Study," Neuroepidemiology, vol. 45, pp. 190-202, 2015.
[6] W. Rongies, B. Slomka, A. Duczek, and W. Dolecki, "The Role of
Posturography in Assessing the Process of Rehabilitation in Poststroke Patients-
A Case Study," J Stroke Cerebrovasc Dis, vol. 26, pp. e34-e37, Feb 2017.
[7] W. Wei, L. Ke, W. Na, Y. Cuiping, and Y. Shouwei, "Evaluation of postural
instability in stroke patient during quiet standing," Conf Proc IEEE Eng Med
Biol Soc, vol. 2017, pp. 2522-2525, Jul 2017.
[8] C. M. Stinear and W. D. Byblow, "Predicting and accelerating motor recovery
after stroke," Curr Opin Neurol, vol. 27, pp. 624-30, Dec 2014.
[9] S. Mendis, P. Puska, and B. Norrving, Eds., Global Atlas on Cardiovascular
Disease Prevention and Control. Geneva World Health Organization, 2011.
[10] T. K. Koo and M. Y. Li, "A Guideline of Selecting and Reporting Intraclass
Correlation Coefficients for Reliability Research," J Chiropr Med, vol. 15, pp.
155-63, Jun 2016.

41
[11] C. Hendry, A. Farley, E. McLafferty, and C. Johnstone, "Nervous system: part
2," Nurs Stand, vol. 28, pp. 45-9, Apr 15 2014.
[12] J. Rothwell, Control of Human Voluntary Movement. London: Chapman and
Hall, 1994.
[13] M. J. Pavol and Y. C. Pai, "Feedforward adaptations are used to compensate for
a potential loss of balance," Experimental Brain Research, vol. 145, pp. 528-
538, Aug 2002.
[14] V. Krishnamoorthy, S. Goodman, V. Zatsiorsky, and M. L. Latash, "Muscle
synergies during shifts of the center of pressure by standing persons:
identification of muscle modes," Biological Cybernetics, vol. 89, pp. 152-161,
Aug 2003.
[15] V. Dietz, G. A. Horstmann, and W. Berger, "Perturbations of human posture:
influence of impulse modality on EMG responses and cerebral evoked
potentials," J Mot Behav, vol. 21, pp. 357-72, Dec 1989.
[16] W. A. Lee, C. F. Michaels, C. Y. Pai, and A. M. Russo, "The function and
organization of postural adjustments during voluntary pulls made by standing
humans," IEEE Eng Med Biol Mag, vol. 11, p. 93, 1992.
[17] F. B. Horak, "Clinical assessment of balance disorders," Gait & Posture, vol. 6,
pp. 76-84, Aug 1997.
[18] L. I. Wolfson, R. Whipple, P. Amerman, and A. Kleinberg, "Stressing the
postural response. A quantitative method for testing balance," J Am Geriatr Soc,
vol. 34, pp. 845-50, Dec 1986.
[19] M. E. Piemonte, E. S. Takata, M. C. Moura, T. T. Capato, M. C. Fornari, and E.
R. Barbosa, "Rapid improvement in balance of patients with Parkinson's disease
through training based on movements guided by rhythmic cues," Movement
Disorders, vol. 19, pp. S210-S210, 2004.
[20] K. O. Berg, S. L. Wood-Dauphinee, J. I. Williams, and B. Maki, "Measuring
balance in the elderly: validation of an instrument," Can J Public Health, vol. 83
Suppl 2, pp. S7-11, Jul-Aug 1992.
[21] K. O. Berg, B. E. Maki, J. I. Williams, P. J. Holliday, and S. L. Wood-
Dauphinee, "Clinical and laboratory measures of postural balance in an elderly
population," Arch Phys Med Rehabil, vol. 73, pp. 1073-80, Nov 1992.
[22] T. Paillard and F. Noe, "Techniques and Methods for Testing the Postural
Function in Healthy and Pathological Subjects," Biomed Research International,
2015.
[23] F. Benvenuti, R. Mecacci, I. Gineprari, S. Bandinelli, E. Benvenuti, L. Ferrucci,
et al., "Kinematic characteristics of standing desequilibrium: reliability and
validity of a posturographic protocol.," Archives in Physical and Medical
Rehabilitation, vol. 80, pp. 278-287, 1999.

42
[24] L. M. Nashner, "Adapting reflexes controlling the human posture,"
Experimental Brain Research, vol. 26, pp. 59-72, 1976.
[25] R. J. Peterka, "Sensorimotor integration in human postural control," Journal of
Neurophysiology, vol. 88, pp. 1097-118, Sep 2002.
[26] D. A. Winter, A. E. Patla, F. Prince, M. Ishac, and K. Gielo-Perczak, "Stiffness
control of balance in quiet standing," J Neurophysiol, vol. 80, pp. 1211-21, Sep
1998.
[27] P. Gatev, S. Thomas, T. Kepple, and M. Hallett, "Feedforward ankle strategy of
balance during quiet stance in adults," J Physiol, vol. 514 ( Pt 3), pp. 915-28,
Feb 1 1999.
[28] A. Bottaro, M. Casadio, P. G. Morasso, and V. Sanguineti, "Body sway during
quiet standing: is it the residual chattering of an intermittent stabilization
process?," Hum Mov Sci, vol. 24, pp. 588-615, Aug 2005.
[29] P. G. Morasso and V. Sanguineti, "Ankle muscle stiffness alone cannot stabilize
balance during quiet standing," J Neurophysiol, vol. 88, pp. 2157-62, Oct 2002.
[30] A. M. Bronstein, T. Brandt, and M. H. Woollacott, Eds., Clinical Disorders of
Balance, Posture and Gait. London: Arnold, 1996.
[31] I. D. Loram, C. N. Maganaris, and M. Lakie, "Human postural sway results from
frequent, ballistic bias impulses by soleus and gastrocnemius," J Physiol, vol.
564, pp. 295-311, Apr 2005.
[32] S. Slobounov, M. Hallett, S. Stanhope, and H. Shibasaki, "Role of cerebral
cortex in human postural control: an EEG study," Clin Neurophysiol, vol. 116,
pp. 315-23, Feb 2005.
[33] A. Shumway-Cook and M. H. Woollacott, Controle motor: teoria e aplicações
práticas. São Paulo: Manole, 2003.
[34] G. Mochizuki, J. G. Semmler, T. D. Ivanova, and S. J. Garland, "Low-frequency
common modulation of soleus motor unit discharge is enhanced during postural
control in humans," Exp Brain Res, Jun 17 2006.
[35] V. Dietz and W. Berger, "Spinal coordination of bilateral leg muscle activity
during balancing," Exp Brain Res, vol. 47, pp. 172-6, 1982.
[36] O. Pyoria, P. Era, and U. Talvitie, "Relationships between standing balance and
symmetry measurements in patients following recent strokes (<= 3 weeks) or
older strokes (>= 6 months)," Physical Therapy, vol. 84, pp. 128-136, Feb 2004.
[37] S. Niam, W. Cheung, P. E. Sullivan, S. Kent, and X. Gu, "Balance and physical
impairments after stroke," Arch Phys Med Rehabil, vol. 80, pp. 1227-33, Oct
1999.
[38] D. A. Winter, "Human balance and posture control during standing and walking
" Gait&Posture, vol. 3, pp. 193-214, December 1995.

43
[39] M. Fahey, E. Crayton, C. Wolfe, and A. Douiri, "Clinical prediction models for
mortality and functional outcome following ischemic stroke: A systematic
review and meta-analysis," PLoS One, vol. 13, p. e0185402, 2018.
[40] A. Schinkel-Ivy, J. C. Singer, E. L. Inness, and A. Mansfield, "Do quiet standing
centre of pressure measures within specific frequencies differ based on ability to
recover balance in individuals with stroke?," Clinical Neurophysiology, vol.
127, pp. 2463-2471, Jun 2016.
[41] P. Madeleine, H. Prietzel, H. Svarrer, and L. Arendt-Nielsen, "Quantitative
posturography in altered sensory conditions: a way to assess balance instability
in patients with chronic whiplash injury," Arch Phys Med Rehabil, vol. 85, pp.
432-8, Mar 2004.
[42] L. Pizzigalli, M. Micheletti Cremasco, A. Mulasso, and A. Rainoldi, "The
contribution of postural balance analysis in older adult fallers: A narrative
review," J Bodyw Mov Ther, vol. 20, pp. 409-17, Apr 2016.
[43] A. Nardone, M. Godi, M. Grasso, S. Guglielmetti, and M. Schieppati,
"Stabilometry is a predictor of gait performance in chronic hemiparetic stroke
patients," Gait & Posture, vol. 30, pp. 5-10, Jul 2009.
[44] V. L. Gray, T. D. Ivanova, and S. J. Garland, "Reliability of center of pressure
measures within and between sessions in individuals post-stroke and healthy
controls," Gait & Posture, vol. 40, pp. 198-203, May 2014.
[45] H. Corriveau, R. Hebert, M. Raiche, and F. Prince, "Evaluation of postural
stability in the elderly with stroke," Archives of Physical Medicine and
Rehabilitation, vol. 85, pp. 1095-1101, Jul 2004.
[46] M. Roerdink, A. C. H. Geurts, M. de Haart, and P. J. Beek, "On the Relative
Contribution of the Paretic Leg to the Control of Posture After Stroke,"
Neurorehabilitation and Neural Repair, vol. 23, pp. 267-274, Mar 2009.
[47] L. Y. Wang, G. Pare, and T. Rundek, "DNA methylation predicts stroke
outcome better The epigenetic clock is ticking," Neurology, vol. 89, pp. 758-
759, Aug 22 2017.
[48] C. A. Fernandes, D. B. Coelho, A. R. Martinelli, and L. A. Teixeira, "Right
cerebral hemisphere specialization for quiet and perturbed body balance control:
Evidence from unilateral stroke," Hum Mov Sci, vol. 57, pp. 374-387, Feb 2018.
[49] A. S. P. Sousa, A. Silva, R. Santos, F. Sousa, and J. M. R. S. Tavares, "Interlimb
Coordination During the Stance Phase of Gait in Subjects With Stroke,"
Archives of Physical Medicine and Rehabilitation, vol. 94, pp. 2515-2522, Dec
2013.
[50] R. Verma, K. N. Arya, P. Sharma, and R. K. Garg, "Understanding gait control
in post-stroke: implications for management," J Bodyw Mov Ther, vol. 16, pp.
14-21, Jan 2012.

44
[51] M. Duarte, "Análise estabilográfica da postura ereta humana quasi-estática,"
Livre Docência, Escola de Educação Física e Esporte, Universidade de São
Paulo, São Paulo, 2000.
[52] M. C. Fornari and A. F. Kohn, "High frequency tendon reflexes in the human
soleus muscle," Neurosci Lett, vol. 440, pp. 193-6, Aug 1 2008.
[53] V. M. Zatsiorsky and M. Duarte, "Instant equilibrium point and its migration in
standing tasks: rambling and trembling components of the stabilogram," Motor
Control, vol. 3, pp. 28-38, Jan 1999.
[54] D. Gasq, M. Labrunee, D. Amarantini, P. Dupui, R. Montoya, and P. Marque,
"Between-day reliability of centre of pressure measures for balance assessment
in hemiplegic stroke patients," J Neuroeng Rehabil, vol. 11, p. 39, Mar 21 2014.
[55] Z. Sawacha, E. Carraro, P. Contessa, A. Guiotto, S. Masiero, and C. Cobelli,
"Relationship between clinical and instrumental balance assessments in chronic
post-stroke hemiparesis subjects," Journal of Neuroengineering and
Rehabilitation, vol. 10, Aug 13 2013.
[56] M. Roerdink, M. De Haart, A. Daffertshofer, S. F. Donker, A. C. H. Geurts, and
P. J. Beek, "Dynamical structure of center-of-pressure trajectories in patients
recovering from stroke," Experimental Brain Research, vol. 174, pp. 256-269,
Sep 2006.
[57] C. S. Sherrington and E. E. Laslett, "Observations on some spinal reflexes and
the interconnection of spinal segments," J Physiol, vol. 29, pp. 58-96, Feb 23
1903.
[58] T. G. Deliagina, I. N. Beloozerova, P. V. Zelenin, and G. N. Orlovsky, "Spinal
and supraspinal postural networks," Brain Res Rev, Jul 27 2007.
[59] F. B. Horak and L. M. Nashner, "Central programming of postural movements:
adaptation to altered support-surface configurations," J Neurophysiol, vol. 55,
pp. 1369-81, Jun 1986.
[60] M. Schieppati and A. Nardone, "Group II spindle afferent fibers in humans: their
possible role in the reflex control of stance," Prog Brain Res, vol. 123, pp. 461-
72, 1999.
[61] S. P. Swinnen and J. Duysens, "Understanding coordination: a coalescence of
constraints at multiple levels," in Neuro-behavioral determinants of interlimb
coordination: a multidisciplinary approach, J. Duysens and S. P. Swinnen, Eds.,
ed: Kluwer Academic Publishers, 2004.
[62] V. Dietz and W. Berger, "Interlimb coordination of posture in patients with
spastic paresis. Impaired function of spinal reflexes," Brain, vol. 107 ( Pt 3), pp.
965-78, Sep 1984.
[63] R. Dickstein and N. Abulaffio, "Postural sway of the affected and nonaffected
pelvis and leg in stance of hemiparetic patients," Archives of Physical Medicine
and Rehabilitation, vol. 81, pp. 364-367, Mar 2000.

45
[64] B. Manor, K. Hu, P. Zhao, M. Selim, D. Alsop, P. Novak, et al., "Altered
control of postural sway following cerebral infarction: a cross-sectional
analysis," Neurology, vol. 74, pp. 458-64, Feb 9 2010.
[65] P. Beattie and R. Nelson, "Clinical prediction rules: what are they and what do
they tell us?," Aust J Physiother, vol. 52, pp. 157-63, 2006.
[66] G. M. Knox, S. J. Snodgrass, and D. A. Rivett, "Physiotherapy clinical
educators' perceptions and experiences of clinical prediction rules,"
Physiotherapy, vol. 101, pp. 364-72, Dec 2015.
[67] N. T. Eghidemwivbie and V. A. Schneeweis, "Early prediction of functional
outcome by physiotherapists in post stroke patients. A prospective cohort study,"
presented at the European School of Physiotherapy, Amsterdam, 2010.
[68] L. K. Kwah and R. D. Herbert, "Prediction of Walking and Arm Recovery after
Stroke: A Critical Review," Brain Sci, vol. 6, Nov 2 2016.
[69] A. S. Sousa, A. Silva, and J. M. Tavares, "Interlimb relation during the double
support phase of gait: an electromyographic, mechanical and energy-based
analysis," Proc Inst Mech Eng H, vol. 227, pp. 327-33, Mar 2013.
[70] A. S. Sousa and J. M. Tavares, "Effect of gait speed on muscle activity patterns
and magnitude during stance," Motor Control, vol. 16, pp. 480-92, Oct 2012.
[71] R. A. Mezzarane and A. F. Kohn, "Bilateral soleus H-reflexes in humans elicited
by simultaneous trains of stimuli: symmetry, variability, and covariance," J
Neurophysiol, vol. 87, pp. 2074-83, Apr 2002.
[72] A. S. Sousa and J. M. Tavares, "Surface electromyographic amplitude
normalization methods: a review," in Electromyography: New Developments,
Procedures and Applications., ed: Neuroscience Research Progress, Nova
Science Publishers, Inc., 2012.