Embed Size (px)
Citation preview

Posterior Capsule Tightness
• Common problem of throwers and racket sport players
• Especially seen in pitchers• Prevented with posterior capsule stretches• Results in reduced medial rotation range of
motion• Can increase anterior capsule stress

Progression of Strength Exercises
• Isometrics• Concentrics, eccentrics in single plane• Diagonal, multiplane motions• Begin at less than 60° • Advance to midrange and then to higher
elevations with strength and control
(continued)

Progression of Strength Exercises (continued)
• Isometrics– Performed when use of arm motion or activity is
restricted– Performed in pain-free positions– Contraction: gradually built to maximum, held at
max, decreased gradually– Held for 5-10 s, repeated 10 times
• Isolated-plane isotonic exercises

Figure 19.59a

Figure 19.59b

Figure 19.60

Figure 19.61
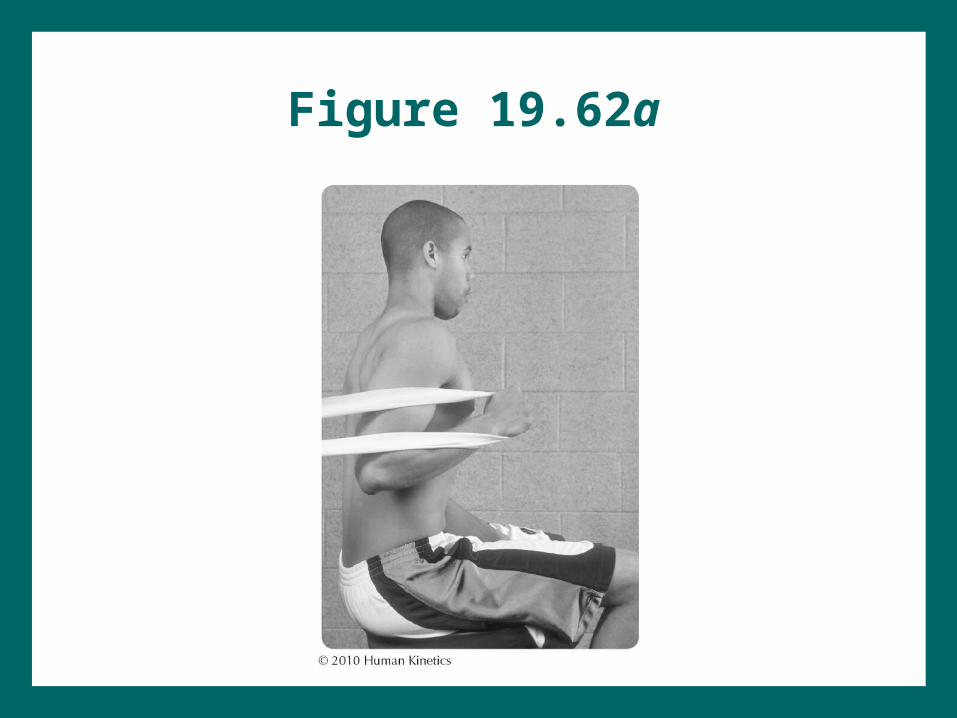
Figure 19.62a

Figure 19.62b

Figure 19.63

Figure 19.64a

Figure 19.64b

Figure 19.65a

Figure 19.65b

Figure 19.65c

Figure 19.66a

Figure 19.66b

Figure 19.66c

Figure 19.66d

Figure 19.67

Figure 19.68

Figure 19.69c

Figure 19.69d

Figure 19.69e
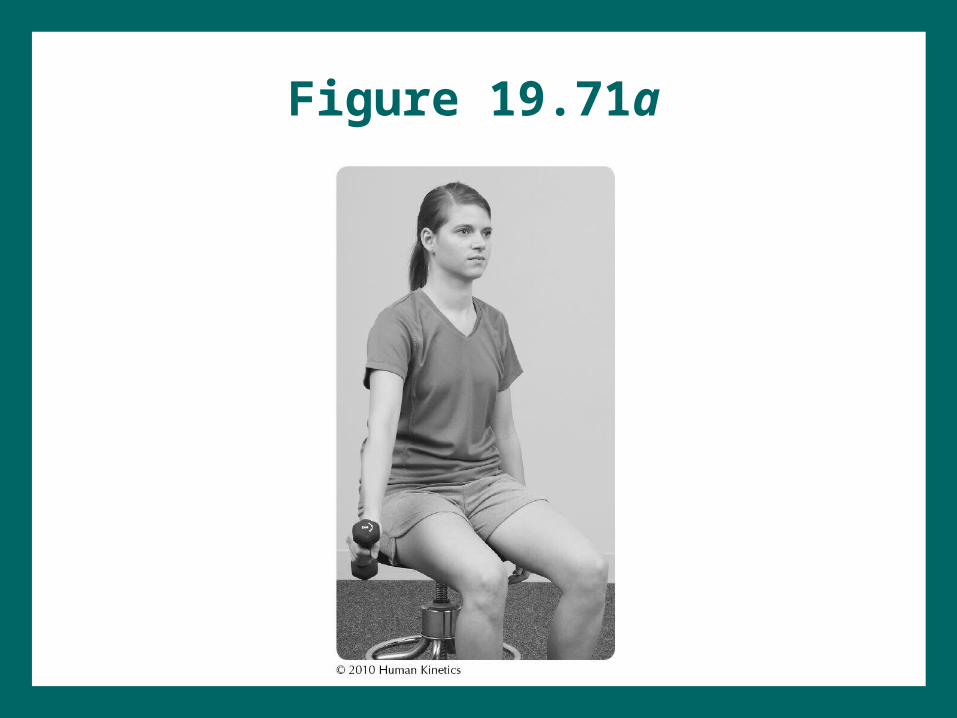
Figure 19.71a

Figure 19.71b

Stabilization Exercises
• Important in aiding strength development and facilitating neuromuscular reeducation
• Some are open kinetic chain; most are closed kinetic chain
• Closed kinetic chain: facilitates cocontraction, permits stabilization with less shear, facilitates proprioception for stabilization
• What is important to improve early in the rehabilitation program? (based on your understanding, provide an answer)

Figure 19.72a

Figure 19.72b

Figure 19.73a

Figure 19.73b

Figure 19.73c

Figure 19.73d

Figure 19.73e

Figure 19.73f

Figure 19.73g

Figure 19.73h

Figure 19.74a

Figure 19.74b

Figure 19.74c

Figure 19.75

Figure 19.76

Figure 19.77

Figure 19.78a

Figure 19.78b

Figure 19.78c

Figure 19.78d
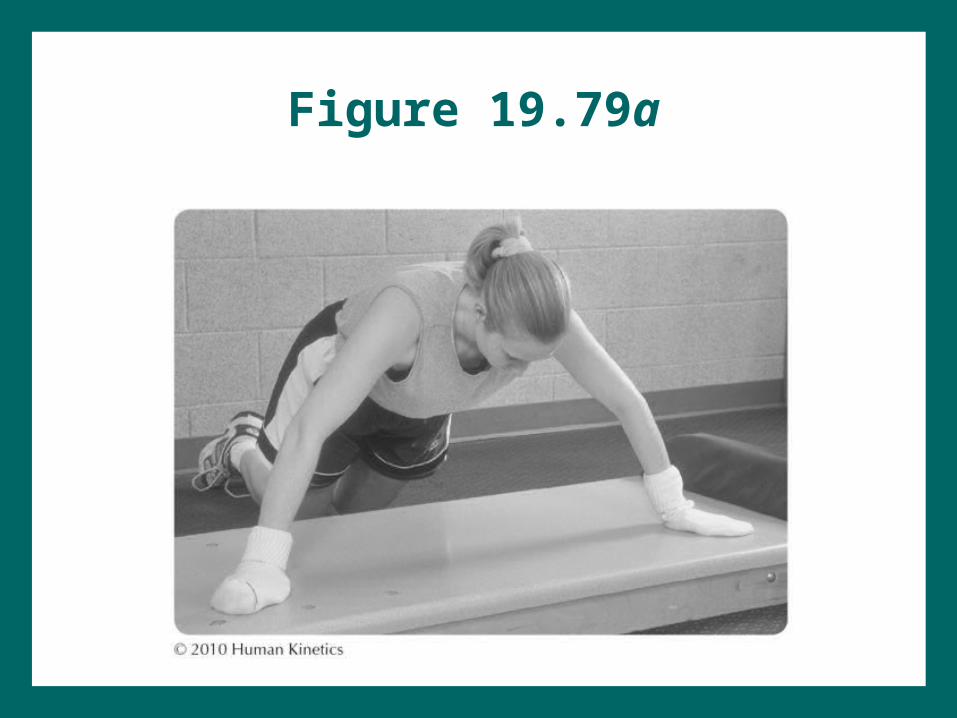
Figure 19.79a

Figure 19.79b

Figure 19.79c

Advanced Exercises
• Plyometrics– Push-up– Resisted movement in weight bearing– Medicine-ball exercises
• Functional activities– Progress in time, resistance, distance– If overhead, from lower to higher
• Activity-specific activities: progression depends on sport, position, or work requirements
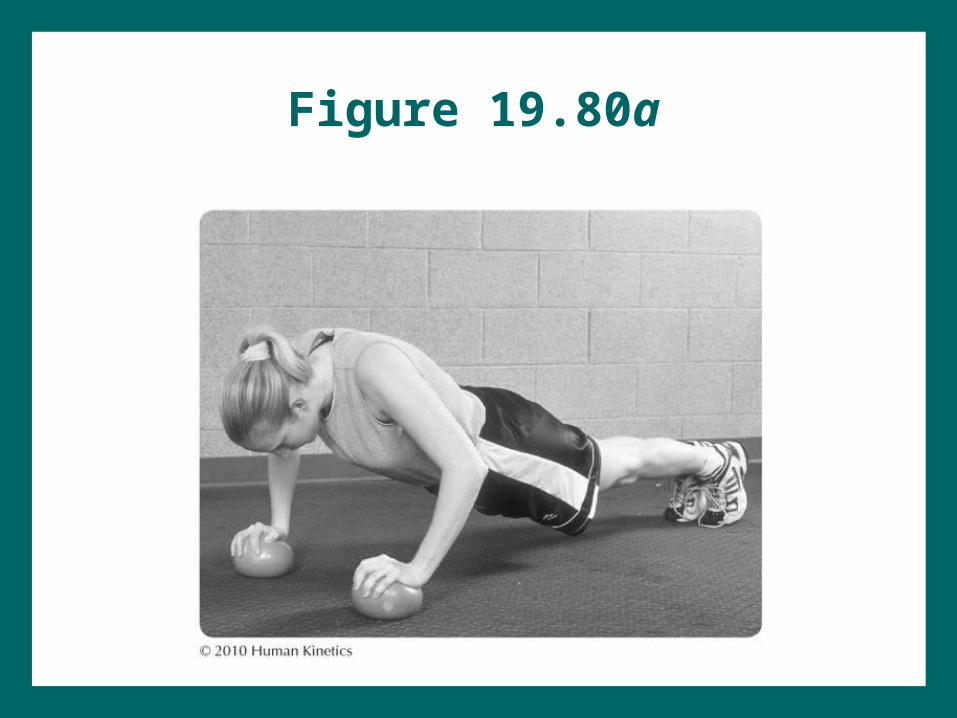
Figure 19.80a
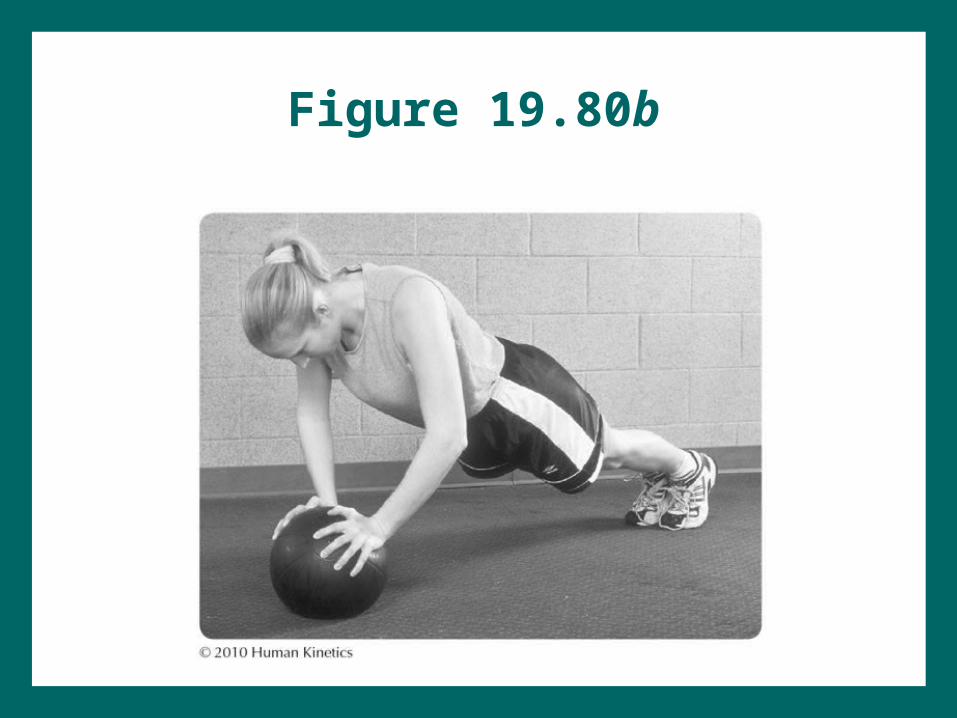
Figure 19.80b

Figure 19.80c
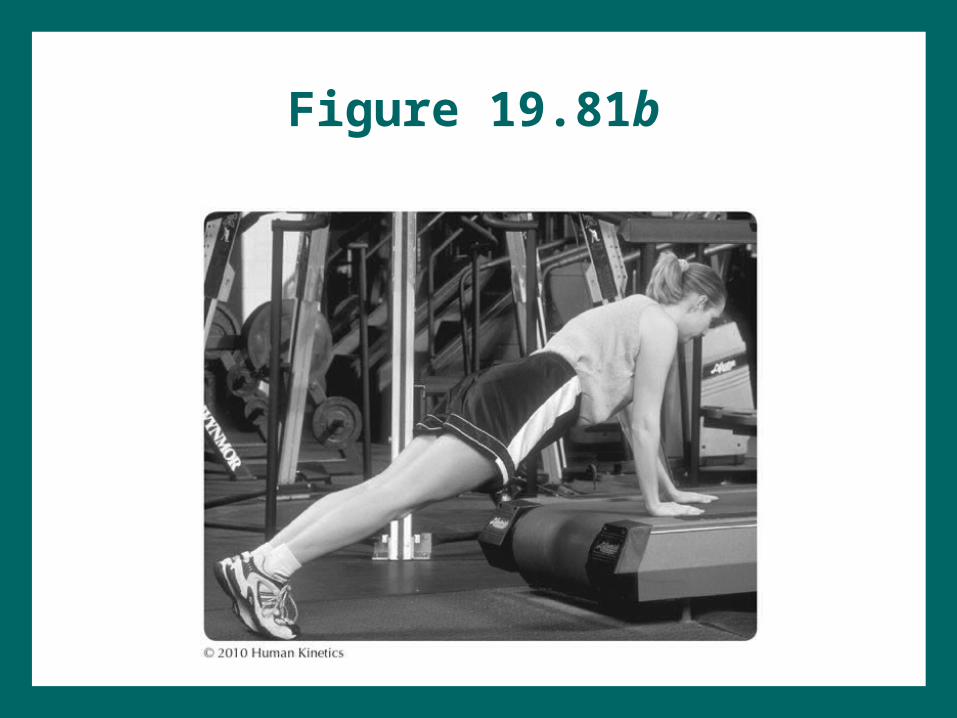
Figure 19.81b

Figure 19.82a

Figure 19.82b
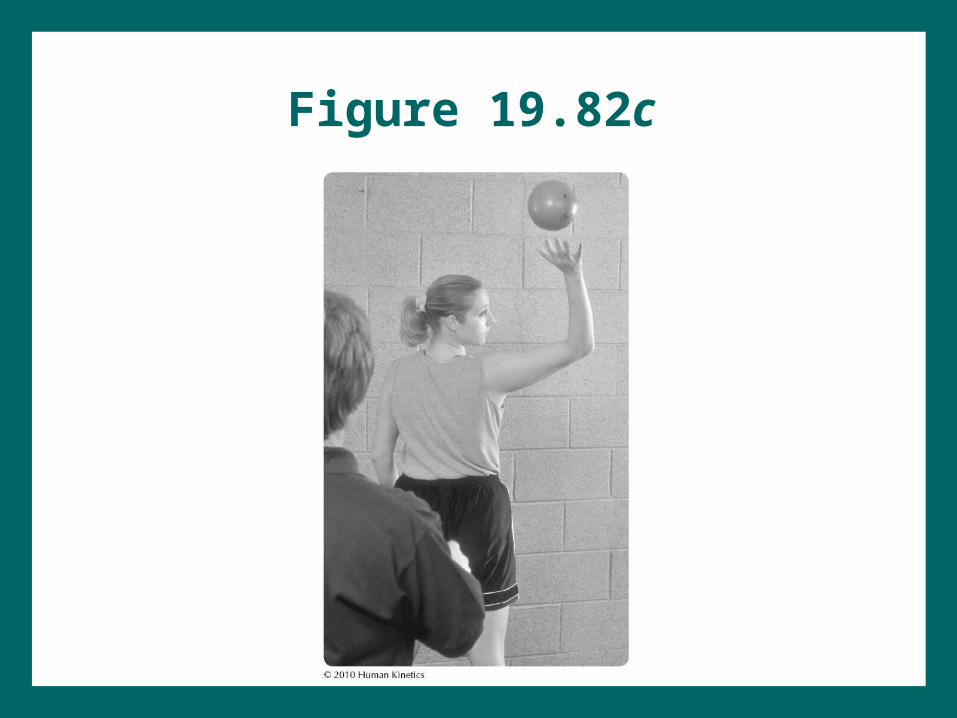
Figure 19.82c

Figure 19.83a

Figure 19.83b

Figure 19.83c

Figure 19.84

GH Instability
• Injury to either static or dynamic restraints instability
• Anterior instability most common• TUBS: Traumatic, Unilateral, Bankart lesion,
Surgery required
• AMBRI: Atraumatic, Multidirectional, Bilateral, Rehabilitation ineffective, Inferior capsule shift required
• What are the concerns for rehabilitation?

Subacromial Impingement
• Primary impingement: result of structures present in narrow subacromial space
• Secondary impingement– Subacromial space narrowed by alterations in
shoulder function – May be caused by or result in instability

Increased Rotation With FlexionGlenoid Positioning
Function Glenoid moves to
give rotator cuff a mechanical advantage + maintain relative spacing
Deficiency Anterior scapular
tilt + reduced rotation upward impingement

Scapula on Thoracic WallSerratus Anterior
Function Serratus anterior
holds scapula on wall
Deficiency Winging
reduced subacromial space

Scapular RetractionRetractor Importance
Function Rhomboids and
middle trapezius prevent round shoulders
Deficiency Protracted scapula
narrows subacromial space

Rotator CuffGH Stabilization
Function Depresses
humeral head into lower glenoid fossa
Deficiency Elevation of
humeral head into upper glenoid fossa

Treating Subacromial Impingement
• What is the rehabilitation emphasis?• What areas should be assessed?• What methods would you use to relieve each
problem?

Rotator Cuff Pathologies
• Pathologies include:– Acute rotator cuff strain– Partial tear– Complete tear– Postsurgical conditions
• Most tears occur after some degeneration of the rotator cuff tendon has occurred.
• Fewer tears occur from sudden traumatic events.

Rx of Rotator Cuff Conditions
• Conservative management versus post-op rehabilitation: Time is 1° difference between them. Rehab procedure is the same but time of progression is slower for surgical management.
• Rehabilitation considerations?? (identify what these are)
Arthroscopic Decompression
• Rehabilitation can begin immediately post-op.
• Rehabilitation takes 3-5 months.
• What are the rehabilitation considerations?

Glenoid Labrum Tears
• SLAP lesion: Superior Labrum tear Anterior and Posterior in location
• 2 to throwing deceleration forces • Difficult to diagnose• Either arthroscopic debridement and repair or
open repair• What are the rehabilitation considerations?

Adhesive Capsulitis
• Capsular motion loss most apparent with ER, followed by abduction, then flexion
• What are the rehabilitation considerations? What are precautions must you take?

Electrothermally Assisted Capsular Shift
• Long-term effects unknown• Immobilization followed by active motion• What are the rehabilitation considerations?
What should you be aware of with these patients?

Acromioclavicular Sprains
• Most such sprains are not surgically repaired or immobilized for more than symptomatic relief.
• Deformity may be present but does not impede performance unless heavy forces or exertion are required of shoulder.
• What are the rehabilitation considerations for the nonsurgical program? What are precautions should be taken? What is the healing time? What motions should the patient avoid?

Biceps Tendon Injuries
• Tendinopathy is more common than ruptures.• Ruptures are often associated with rotator cuff
pathology or impingement.• Ruptures are more often seen in middle-aged
adults nonsurgical. • Surgery may be necessary for younger patients
with long head (LH) ruptures, especially if very active
• What are the rehabilitation considerations?














![Sulforaphane promotes ER stress, autophagy, and cell death: … · 2017-08-25 · drain on healthcare providers [3, 4]. Posterior capsule opacification(PCO) isthemostcommoncomplication](https://img.pdfslide.net/doc/110x75/5e5b933fdabba4232e4e223b/sulforaphane-promotes-er-stress-autophagy-and-cell-death-2017-08-25-drain-on.jpg)













