Embed Size (px)
Citation preview

www.elsevier.com/locate/yebeh
Epilepsy & Behavior 6 (2005) 102–110
Case Report
Postictal mania associated with frontal lobe epilepsy
Takuji Nishida*, Tatsuya Kudo, Fumihiro Nakamura, Masaki Yoshimura,Kazumi Matsuda, Kazuichi Yagi
National Epilepsy Center, Shizuoka Institute of Epilepsy and Neurological Disorders, 886 Urushiyama, Shizuoka, 420-8688, Japan
Received 1 August 2004; revised 28 October 2004; accepted 1 November 2004Available online 23 December 2004
Abstract
A 38-year-old man, possibly with frontal lobe epilepsy, developed postictal mania. The changes in psychiatric symptoms andlaboratory examinations over time were investigated in two episodes of postictal mania, using long-term electroencephalographywith closed circuit television (EEG/CCTV) monitoring, magnetoencephalography (MEG), and single-photon emission computedtomography (SPECT) to elucidate the underlying mechanism of postictal mania. According to the clinical symptoms, the postictalmanic episodes of this case had four phases: a lucid interval, manic phase, hypomanic phase, and recovery phase. EEG showedforced normalization during the florid manic phase. The serial findings of EEG, MEG, and SPECT during the postictal manic epi-sodes suggest that functional changes in bilateral frontal lobes, especially the right frontal lobe, right temporal lobe, and right para-limbic area, are crucial in the development of postictal mania, and that these functional changes are dynamic.� 2004 Elsevier Inc. All rights reserved.
Keywords: Epilepsy; Postictal mania; Frontal lobe; Temporal lobe; Paralimbic area; Forced normalization; Electroencephalography;Magnetoencephalography; Single-photon emission computed tomography
1. Introduction
Mood disturbances are common in patients withchronic epilepsy [1–3]. Blumer et al. reported that briefeuphoric moods are observed commonly in patients withinterictal dysphoric disorder [1]. Longstanding manicepisodes, however, are rarely reported, and a search ofthe literature identified a small number of cases of manicand hypomanic state observed in the interictal period[4,5], ictal period [6–8] and postictal period [4,5,9–16].
Kudo et al. [5] reported patients with interictal manicepisodes that fulfilled the DSM-IV [17] criteria for manicepisode, and showed that their clinical features were lesssevere and more rapidly cycling compared with those ofpatients with bipolar I disorder. However, very few casesof epilepsy with manic episodes that fulfilled diagnostic
1525-5050/$ - see front matter � 2004 Elsevier Inc. All rights reserved.
doi:10.1016/j.yebeh.2004.11.009
* Corresponding author. Fax: +81 54 247 9781.E-mail address: [email protected] (T. Nishida).
criteria such as those of DSM-IV and ICD-10 [18] havebeen reported.
Postictal psychosis is well known to be a psychiatricdisturbance observed in the postictal period, and thesymptoms are pleomorphic, including various kinds ofdelusions, auditory hallucinations, mental diplopia, dis-inhibited sexual behavior, and mood disturbances[13,19]. Kanemoto et al. [19] reported that one of thestriking features of postictal psychosis was the relativelyfrequent occurrence of religious and grandiose delusionin the setting of elated moods. Therefore, it is possiblethat the psychiatric disturbance called ‘‘postictal psy-chosis’’ includes heterogeneous and distinguishablepsychopathologies.
Although some cases of manic and hypomanic stateobserved in the postictal period have been reported[4,5,9–16], whether these states represent a distinct psy-chiatric disturbance and whether clinical features are re-lated to the localization and hemispheric laterality of theepileptogenic zone remain unknown.

Case Report / Epilepsy & Behavior 6 (2005) 102–110 103
We documented two episodes of manic state observedin the postictal period in a patient, possibly with leftfrontal lobe epilepsy, and investigated the changes inpsychiatric symptoms and laboratory examinations overtime, using long-term electroencephalography withclosed circuit television (EEG/CCTV) monitoring, mag-netoencephalography (MEG), and single-photon emis-sion computed tomography (SPECT).
2. Patient
A 38-year-old right-handed man was admitted to ourhospital because of intractable seizures and postictalpsychiatric symptoms.
The patient had suffered from generalized convul-sions since age 15 and postictal psychiatric symptomssince age 28. There were no convulsive and mental dis-orders in his family history, except bipolar mood disor-der in a paternal relative. The patient had no history ofserious illness before age 15. His habitual seizure is ageneralized convulsion with an initial cry, occurringmainly during sleep and sometimes accompanied by uri-nary incontinence. The first generalized convulsion oc-curred at age 15, and since then he has had seizuresonce every 2 or 3 months despite antiepileptic drug med-ication. The seizure frequency increased to once or twiceevery month between ages 26 and 28. At age 28, hedeveloped psychiatric symptoms for the first time, whichlasted several days following a lucid interval of about 1day after generalized convulsions, and he was admittedto a hospital. The psychiatric symptoms in this postictalepisode were similar to those we confirmed later. Sincethen, psychiatric episodes did not recur until age 37,although seizures had continued once every 2 or 3months. At age 37, postictal paresis on the right sidewas confirmed by a neurologist after generalized convul-sions. Between the ages of 37 and 38, postictal psychiat-ric episodes recurred six times.
On the first admission to our hospital, neurologicalexamination revealed no definite deficit. Interictal scalpEEG showed sporadic spike and waves, sharp waves,and high-voltage slow waves at Fp1, Fp2, F3, and F4.Computed tomography (CT) and magnetic resonanceimaging (MRI) showed moderately diffuse cerebral atro-phy, particularly in the left frontal and temporal lobes. Bythe Wechsler Adult Intelligence Scale—Revised (WAIS-R), his full-scale intelligence quotient (IQ) was 88, verbalIQ was 95, and performance IQ was 81. He was allowed ashort stay at home because he had had no seizure formorethan 1 month after admission. While at home, he had onegeneralized convulsion. Following a lucid interval ofabout 1 day, he began to manifest psychiatric symptoms.When he returned to the hospital with his family, he al-ready manifested the psychiatric symptoms described in4. Results. The psychiatric symptoms lasted about 2
weeks. In addition to carbamazepine 800 mg, which hehad been taking, phenytoin 200 mg was started from thefirst postictal day and levomepromazine 25 mg wasadministered on the first and sixth postictal days for hispsychiatric symptoms (Episode 1, see Fig. 1).
Several months after he was discharged from the hos-pital, he had three generalized convulsions within112hours and came to our hospital the next day. Follow-
ing a lucid interval of about 2 days, he began to manifestthe same psychiatric symptoms as in Episode 1. The psy-chiatric symptoms lasted about 3 weeks. Phenytoin225 mg and carbamazepine 800 mg were continued andlevomepromazine 25 mg was administered on the secondand third postictal days and from the 14th to 22nd post-ictal day and chlorpromazine 12.5 mg was administeredon the second postictal day (Episode 2, see Fig. 1).
He tended to have seizures when he led an intemper-ate life and failed to take his medication. Even when heregained his usual mental state, he tended to behave self-ishly, and quarreled with other patients over trivialthings in the hospital. His mother said that althoughhe was doing well at school, he became inconsiderateand led an intemperate life, wasting money withoutthinking as he grew up.
3. Methods
Both Episodes 1 and 2 were divided into four phasesaccording to the psychiatric symptoms of this patient.The first phase was the lucid interval lasting 1 or 2 daysafter seizures, during which the patient had no definitepsychiatric symptoms. The second phase was the manicphase, during which he had manic symptoms describedin Results. The third phase was the hypomanic phase,during which the manic symptoms were improving buthad not subsided completely. The fourth phase wasthe recovery phase, in which he regained his mental statebefore the seizures. On the basis of this division, theserial EEG, MEG, and SPECT findings in Episodes 1and 2 were related to the psychopathological state ofthis patient.
All long-term EEG/CCTV monitoring and routineEEGs were performed with scalp electrodes placedaccording to the international 10–20 system.
All SPECT scans were recorded with a ring-shapedSPECT scanner (Headtome-SET070; Shimazu, Kyoto,Japan). Tc-ECD 740 MBq was injected into a peripheralvein and data acquisition was initiated 5 minutes afterthe injection. SPECT analysis was performed by thesubtraction of ictal and interictal SPECT coregisteredto MRI (SISCOM) [20]. The images obtained duringevery phase of the postictal episodes were comparedwith one image obtained during the recovery phase,using SISCOM. The areas showing significant increase(above 2 SD) of radioisotope uptake were in color.

Fig. 1. Schematic representation of psychiatric state, laboratory examinations, and medications in Episodes 1 and 2. Black dots show examinations ordrug administrationduring thepostictal episodes.Blackbars represent long-termEEGmonitoringor continueddrugadministrationduring thepostictalepisodes. Figures are shown later. Details are described in 2. Patients and 3. Methods. EEG, electroencephalography; SPECT, single-photon emissioncomputed tomography; MEG, magnetoencephalography; PHT, phenytoin; CBZ, carbamazepine; LP, levomepromazine; CP, chlorpromazine.
104 Case Report / Epilepsy & Behavior 6 (2005) 102–110
All magnetoencephalograms were recorded with twosets of a 37-channel superconducting quantum interfer-ence device (SQUID) (Magnes II magnetometer; Bio-magnetic Technologies, San Diego, CA, USA).
InEpisode 1, long-term24-hourEEG/CCTVmonitor-ing was performed from the second to sixth postictal day,and routine EEG was performed on the 9th, 13th, 19th,27th, and 54th postictal days. SPECT was performed onthe 2nd, 6th, 34th, and 70th postictal days.MEGwas per-formed on the 9th, 30th, and 86th postictal days (Fig. 1).
In Episode 2, long-term 24-hour EEG/CCTV moni-toring was performed from the 1st to 13th postictalday and routine EEG was performed on the 25th and37th postictal days. SPECT was performed on the 1stand 7th postictal days (Fig. 1).
4. Results
4.1. Episode 1
After a generalized convulsion, the lucid intervallasted about 1 day (Fig. 1). During this phase, the pa-tient had no definite psychiatric symptoms but the de-tails are not known because he was not in the hospital.
Following the lucid interval, the manic phase lastedabout 3 days. During this phase, the patient exhibitedeuphoria, hyperthymia, distractibility, pressured speech,monologue, logorrhea, flight of ideas, incoherence, and
grandiose delusion. He was in ecstasy and talked to him-self loudly. When asked how he was feeling, he replied,‘‘I feel wonderful!’’ He was proud and claimed that thesimultaneous terrorist attacks in the United States mim-icked a computer game software he had programmed.The content of his speech changed rapidly. Althoughhe usually read books written in Japanese, he tried toread a book written in English but could not concen-trate. He also became suddenly irritated about trivialthings and shouted at the nursing staff. During themanic phase, EEG showed no definite epileptiform dis-charges in both waking and sleep stages (Fig. 2A).SPECT showed hyperperfusion in the right medial pre-frontal area, frontal pole, cingulate cortex, and a partof the superior frontal gyrus (Fig. 3A).
Following the manic phase, the hypomanic phaselasted about 10 days. In this phase, he continued to bein a euphoric mood with an arrogant and irritable atti-tude. He boastfully talked to others who were nearhim. During the hypomanic phase, EEG showed almostcontinuous spike and waves, sharp waves, and high-voltage slow waves at Fp1, Fp2, F3, and F4 in the wak-ing stage and sleep stages 1 and 2 (Fig. 2B). SPECTshowed hyperperfusion in the right lateral prefrontalarea and frontal operculum (Fig. 3B). MEG showed awide distribution of equivalent-current dipoles in bilat-eral frontal lobes (Fig. 4A).
During the recovery phase, EEG showed the grad-ual disappearance of spike and waves, sharp waves,

Fig. 2. Serial EEG findings in Episode 1. (A) Manic phase: No definite epileptiform discharges are observed in waking and sleep stages. (B)Hypomanic phase: Almost continuous spike and waves, sharp waves, and high-voltage slow waves are detected at Fp1, Fp2, F3, and F4 in wakingand sleep stages. (C) Recovery phase: The epileptiform discharges and high-voltage slow waves have subsided.
Case Report / Epilepsy & Behavior 6 (2005) 102–110 105

Fig. 3. SPECT findings in Episode 1. Colored spots are areas with a significant increase (above 2 SD) in radioisotope uptake compared with theimage obtained during recovery phase. (A) Manic phase: Hyperperfusion is shown in the right medial prefrontal area, frontal pole, and cingulatecortex. (B) Hypomanic phase: Hyperperfusion is shown in the right lateral prefrontal area and frontal operculum.
Fig. 4. MEG findings in Episode 1. (A) Hypomanic phase: a wide distribution of equivalent-current dipoles is observed in bilateral frontal lobes. (B,C) Recovery phase: Equivalent-current dipoles are localized near the cingulate cortex.
106 Case Report / Epilepsy & Behavior 6 (2005) 102–110
and high-voltage slow waves at Fp1, Fp2, F3, andF4 (Fig. 2C). SPECT showed the disappearance ofhyperperfusion (data not shown). MEG showed adistribution of equivalent-current dipoles in bilateral
medial frontal areas on the 30th postictal day (Fig.4B) and localization of equivalent-current dipolesnear the left cingulate cortex on the 86th postictalday (Fig. 4C).

Case Report / Epilepsy & Behavior 6 (2005) 102–110 107
He was alert and oriented during the entire Episode 1and later could recall his experience during this episode.
4.2. Episode 2
After three generalized convulsions, the lucid intervallasted about 2 days (Fig. 1). During this phase, he hadno definite psychiatric symptoms except slight cloudingof consciousness and slower speech than usual. Duringthe lucid interval, EEG showed sporadic spike andwaves, sharp waves, and high-voltage slow waves atFp1, Fp2, F3, and F4 in the waking stage and sleep
Fig. 5. EEG findings in Episode 2. Sporadic spike and waves, sharp waves,waking and sleep stages during lucid interval.
Fig. 6. SPECT findings in Episode 2. (A) Lucid interval: Hyperperfusion icingulate cortices. (B) Latter half of manic phase: Hyperperfusion is observe
stages 1 and 2 (Fig. 5). SPECT showed hyperperfusionin bilateral medial prefrontal areas and orbitofrontaland cingulate cortices (Fig. 6A).
Following the lucid interval, the manic phase lastedabout 10 days. The psychiatric symptoms in the manicphase were the same as in Episode 1. During the firsthalf of the manic phase, EEG showed the disappearanceof spike and waves, sharp waves, and high-voltage slowwaves in both waking and sleep stages (data not shown),as in Episode 1. During the latter half of the manicphase, spike and waves, sharp waves, and high-voltageslow waves reappeared almost continuously at Fp1,
and high-voltage slow waves are detected at Fp1, Fp2, F3, and F4 in
s observed in bilateral medial prefrontal areas and orbitofrontal andd in the right superior temporal gyrus and frontal operculum.

108 Case Report / Epilepsy & Behavior 6 (2005) 102–110
Fp2, F3, and F4 in the waking stage and sleep stages 1and 2 (data not shown), identical to the hypomanicphase in Episode 1. SPECT showed hyperperfusion inthe right superior temporal gyrus and frontal operculumduring the latter half of the manic phase (Fig. 6B).
Following the manic phase, the hypomanic phaselasted about 10 days. During the hypomanic phase,EEG showed continuous spike and waves, sharp waves,and high-voltage slow waves at Fp1, Fp2, F3, and F4 inthe waking stage and sleep stages 1 and 2 (data notshown), as in Episode 1.
During the recovery phase, EEG showed gradual dis-appearance of spike and waves, sharp waves, and high-voltage slow waves (data not shown), as in Episode 1.
5. Discussion
The psychiatric symptoms in this patient began witheuphoria and hyperthymia, which were the cardinalsymptoms throughout all postictal episodes. He couldnot concentrate on anything and his speech was pres-sured. The grandiose delusion was congruent with hismood and never systematic. No hallucinations andpersecutory delusion were observed. This psychiatric dis-turbance observed in the postictal period fulfilled theDSM-IV criteria for manic episode and we diagnosedthis disturbance as ‘‘postictal mania.’’ Kanemoto et al.have already shown that elated moods are observed com-monly in patients with postictal psychosis [19]. The psy-chiatric disturbance called ‘‘postictal psychosis’’ may beheterogeneous. We consider that the unique manic statelike our case, which fulfilled DSM-IV criteria for a manicepisode, has a special position in the heterogeneous psy-chiatric disturbance, and can be distinguished from thepsychotic state characterized chiefly by delusions andhallucinations observed in the postictal period.
It remains unknown whether the clinical features ofpostictal mania are related to the localization and hemi-spheric laterality of the epileptogenic zone. Regarding
Table 1Summary of changes in psychiatric states and serial findings of laboratory e
Lucid interval Manic phase
EEG Sporadic sp-w.sharp, and HVS inbilateral frontal areas
Disappearance ofsp-w, sharp,and HVS
Continuous sfrontal areas
MEG
SPECT Hyperperfusion inbilateral medialprefrontal areasand orbitofrontaland cingulate cortices
Hyperperfusion in theright medial prefrontalarea, frontal pole,cingulate cortex, andsuperior frontal gyrus
Hyperperfusioin the right sutemporal gyrufrontal opercu
a sp-w, spike and slow waves; sharp, sharp waves; HVS, high-voltage slo
the localization of the epileptogenic zone in reportedcases of manic state in the postictal period, the focuswas in the temporal lobe in eight patients [4,5,12–15],multifoci or an unknown focus was reported in sevenpatients [10,11], and idiopathic generalized epilepsywas diagnosed in two patients [9,13]. The epileptogeniczone of our case was suspected to be in the left frontallobe based on the findings of generalized convulsionswith Todd�s paresis on his right side, interictal epilepti-form discharges in the frontal polar and frontal regionson EEG, and equivalent-current dipoles localized in theleft medial frontal lobe on interictal MEG.
The hemispheric laterality of the epileptogenic zonealso remains controversial. Flor-Henry [21] and Hurwitzet al. [15] suggested that the manic or hypomanic statewas related to the nondominant hemisphere. However,some studies have reported on patients who enter themanic state in the postictal period who have an epilepto-genic zone on the left side [4,5]. In our case, the epilep-togenic zone was suspected to be on the left side.However, the patient showed functional changes inbilateral frontal lobes, especially in the right frontallobe, right temporal lobe, and right paralimbic areasduring the manic episodes. This suggests that even ifthe epileptogenic zone is on the left side of the cerebralcortex, functional changes on the contralateral side orbilateral sides may contribute to the development ofpostictal mania.
The postictal manic episodes of our case followed aclinical course of lucid interval, manic phase, hypomanicphase, and recovery phase as summarized in Table 1.The EEG findings changed almost in line with these clin-ical phases: sporadic spike and waves, sharp waves, andhigh-voltage slow waves in bilateral frontal areas duringthe lucid interval; disappearance of epileptiform dis-charges and high-voltage slow waves during the floridmanic phase; continuous spike and waves, sharp waves,and high-voltage slow waves in bilateral frontal areasduring the latter half of the manic phase and hypomanicphase; and disappearance of the epileptiform discharges
xaminations (EEG, MEG, and SPECT)a
Hypomanic phase Recovery phase
p-w. sharp, and HVS in bilateral Disappearance of sp-w.sharp, and HVS
Equivalent-current dipolesin bilateral frontal lobes
Equivalent-current dipolesnear the left cingulate cortex
nperiors andlum
Hyperperfusion in the rightlateral prefrontal area andfrontal operculum
Disappearance ofhyperperfusion
w waves.

Case Report / Epilepsy & Behavior 6 (2005) 102–110 109
and high-voltage slow waves during the recovery phase.Thus, the postictal manic episodes comprised almostfour phases clinicoelectrically.
MEG showed a wide distribution of equivalent-cur-rent dipoles in bilateral frontal lobes during the hypo-manic phase, consistent with the EEG findings, andlocalization of equivalent-current dipoles near the leftcingulate cortex during the recovery phase. MEG dem-onstrated residual functional change in the paralimbicarea (cingulate cortex) during the recovery phase, whichwas not depicted on EEG.
SPECT showed hyperperfusion in bilateral medialprefrontal areas and paralimbic areas (orbitofrontaland cingulate cortices) during the lucid interval; hyper-perfusion in the right medial prefrontal area, right para-limbic area (cingulate cortex), and right superior frontalgyrus during the manic phase; hyperperfusion in theright superior temporal gyrus and right frontal opercu-lum during the latter half of the manic phase; and hyp-erperfusion in the right lateral prefrontal area and rightfrontal operculum during the hypomanic phase. Thus,SPECT showed distinct functional changes in the rightprefrontal lobe, right temporal lobe, and right paralim-bic areas, and it is possible that these functional changesin cerebral cortex reflect the underlying cause of the clin-icoelectrical changes during the postictal manic episodesin this patient.
The clinicoelectrical finding observed during the flor-id manic phase was equivalent to ‘‘forced normaliza-tion,’’ a phenomenon in which epileptiform dischargesin patients with epilepsy normalize during psychosis[22]. In our case, this phenomenon proved to be duenot merely to an elevated arousal level but to an intrinsicmechanism that normalizes epileptic activities, becauseepileptiform discharges disappeared not only in the wak-ing stage but also in the sleep stage. The forced normal-ization observed during the florid manic phase in thiscase is a phenomenon forming a part of the functionalchanges during the whole course of postictal mania,and may be based on the pathogenesis of postictalmania.
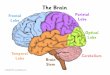
Our investigation suggests that functional changes inbilateral frontal lobes, especially in the right frontallobe, right temporal lobe, and right paralimbic area,are crucial in the development of postictal mania. Theparalimbic area is supposed to be closely connected tothe limbic area, temporal lobe, and frontal lobe. Thelimbic area and temporal lobe have a faculty associatedwith emotion, and the frontal lobe has integrative andinhibitory faculties of mental activity [23]. This supportsour hypothesis that postictal mania, with cardinal symp-toms of mood disturbance and disinhibition, is relatedto these cerebral structures. No report has describedthe relation between psychiatric symptoms and labora-tory examinations in the manic state observed in thepostictal period. Our hypothesis is, however, supported
by a report that suggests that the frontal lobe and tem-poral lobe are associated with the interictal manic epi-sodes in patients with epilepsy [5]. In some reports ofmanic patients with bipolar mood disorder, SPECT de-picted hyperperfusion in the temporal lobe and basalganglia and hypoperfusion in the prefrontal area [24],hypoperfusion in selective frontal and temporal lobes[25], and hyperperfusion in the right anterior temporallobes [26]. These findings also support the idea thatthe manic state is related to functional changes in frontaland temporal lobes.
Our investigation demonstrates that the clinicalsymptoms and functional changes in bilateral frontallobes, especially in the right frontal lobe, right temporallobe, and right paralimbic area, are dynamic duringpostictal manic episodes. Further detailed studies are re-quired to understand the underlying mechanism of post-ictal mania.
Finally, we discuss the interictal behavioral trait ofthis patient. This patient became inconsiderate and ledan intemperate life, wasting money without thinking.Laboratory examinations showed disturbance of frontallobe function even in the interictal period. The interictalbehavioral trait of this patient is considered to be relatedto dysfunction of the frontal lobe and may be equivalentto the so-called frontal syndrome [23].
References
[1] Blumer D, Montouris G, Hermann BP. Psychiatric morbidity inseizure patients on a neurodiagnostic monitoring unit. J Neuro-psychiatry Clin Neurosci 1995;7:445–56.
[2] Lambert MV, Robertson MM. Depression in epilepsy: etiology,phenomenology, and treatment. Epilepsia 1999;40:S21–47.
[3] Hermann BP, Seidenberg M, Bell B. Psychiatric comorbidity inchronic epilepsy: identification, consequences, and treatment ofmajor depression. Epilepsia 2000;41:S31–41.
[4] Wolf P. Manic episodes in epilepsy. In: Akimoto H, KazamatsuriH, Seino M, Ward A, editors. Advances in epileptology: XIIIthEpilepsy International Symposium. New York: Raven Press;1982. p. 237–40.
[5] Kudo T, Ishida S, Kubota H, Yagi K. Manic episode in epilepsyand bipolar I disorder: a comparative analysis of 13 patients.Epilepsia 2001;42:1036–42.
[6] Gillig P, Sackellares JC, Greenberg HS. Right hemisphere partialcomplex seizures: mania, hallucination, and speech disturbancesduring ictal events. Epilepsia 1988;29:26–9.
[7] Guillem E, Plas J, Musa C, Notides C, Lepine JP. Ictal mania: acase report. Can J Psychiatry 2000;45:493–4.
[8] Thomas P, Zifkin B, Migneco O, Lebrun C, Darcourt J,Andermann F. Nonconvulsive status epilepticus of frontal origin.Neurology 1999;52:1174–83.
[9] Chakrabarti S, Aga VM, Singh R. Postictal mania followingprimary generalized seizures. Neurol India 1999;47:332–3.
[10] Kanner AM, Stagno S, Kotagal P, Morris HH. Postictalpsychiatric events during prolonged video-electroencephalo-graphic monitoring studies. Arch Neurol 1996;53:258–63.
[11] Savard G, Andermann F, Olivier A, Remillard GM. Postictalpsychosis after partial complex seizures: a multiple case study.Epilepsia 1991;32:225–31.

110 Case Report / Epilepsy & Behavior 6 (2005) 102–110
[12] Byrne A. Hypomania following increased epileptic activity. Br JPsychiatry 1988;153:573–4.
[13] Logsdail SJ, Toone BK. Post-ictal psychoses: a clinical andphenomenological description. Br J Psychiatry 1988;152:246–52.
[14] Barczak P, Edmunds E, Betts T. Hypomania following complexpartial seizures: a report of three cases. Br J Psychiatry1988;152:137–9.
[15] Hurwitz TA, Wada JA, Kosaka BA, Strauss EH. Cerebralorganization of affect suggested by temporal lobe seizures.Neurology 1985;35:1335–7.
[16] Wolf P. Status epilepticus and psychosis. In: Akimoto H,Kazamatsuri H, Seino M, Ward A, editors. Advances inepileptology: XIIIth Epilepsy International Symposium. NewYork: Raven Press; 1982. p. 211–7.
[17] Diagnostic and statistical manual of mental disorders. 4th ed.Washington DC: American Psychiatric Association; 1994.
[18] The ICD-10 classification of mental and behavioural disorders:clinical descriptions and diagnostic guidelines. Geneva: WorldHealth Organization; 1992.
[19] Kanemoto K, Kawasaki J, Kawai I. Postictal psychosis: acomparison with acute interictal and chronic psychoses. Epilepsia1996;37:551–6.
[20] O�Brien TJ, So EL, Mullan BP, et al. Subtraction ictalSPECT co-registered to MRI improves clinical usefulness of
SPECT in localizing the surgical seizure focus. Neurology1998;50:445–54.
[21] Flor-Henry P. Psychosis and temporal lobe epilepsy: a controlledinvestigation. Epilepsia 1969;10:363–95.
[22] Landolt H. Serial electroencephalographic investigations duringpsychotic episodes in epileptic patients and during schizophrenicattacks. In: Lorenz de Haas AM, editor. Lectures on epi-lepsy. Amsterdam: Elsevier; 1958. p. 91–133.
[23] Mesulam MM. Behavioral neuroanatomy: large-scale networks,association cortex, frontal syndromes, the limbic system,and hemispheric specializations. 2nd ed. In: Mesulam MM,editor. Principles of behavioral and cognitive neurology. NewYork: Oxford Univ. Press; 2000. p. 1–120.
[24] O�Connell RA, Van Heertum RL, Luck D, et al. Single-photonemission computed tomography of the brain in acute mania andschizophrenia. J Neuroimag 1995;5:101–4.
[25] Rubin E, Sackeim HA, Prohovnik I, Moeller JR, Schnur DB,Mukherjee S. Regional cerebral blood flow in mood disorders: IV.Comparison of mania and depression. Psychiatry Res1995;61:1–10.
[26] Gyulai L, Alavi A, Broich K, Reilley J, Ball WB, Whybrow PC. I-123 iofetamine single-photon computed emission tomography inrapid cycling bipolar disorders: a clinical study. Biol Psychiatry1997;41:152–61.