Embed Size (px)
Citation preview

389
often used as such in the preparation of tissues for electron
microscopy. Thus rather than helping to destroy or removeadherent tissue it may well preserve the tissue and cause it to stick tothe metal of the forceps. We have exposed tissue to disinfectantsolutions of 2% glutaraldehyde and fmd that the tissues are virtuallyindistinguishable from those fixed directly in formalin. There maybe some blurring of the nuclear chromatin pattern but this is aninconsistent and subtle feature and is unlikely to be noticed by thehistopathologist. We therefore strongly recommend that all theatresand endoscopy clinics are equipped with sufficient biopsy forceps topermit ultrasonification of the instruments after every case. Thisshould be done before immersion in glutaraldehyde.
Northampton General Hospital,Northampton NN1 5BD
S. B. COGHILLC. H. MASON
J. G. N. STUDLEY
1 Anon. Cleaning and disinfection of equipment for gastrointestinal flexible endoscopy:interim recommendations of a working party of the British Society of
Gastroenterology Gut 1988; 29: 1134-51.2. Hanson PJV, Jeffries DJ, Batten JC, Collins JV Infection control revisited: dilemma
facing today’s bronchoscopists. Br Med J 1988; 297: 185-87.
EPILEPTIC SEIZURES AND SMOTHER-PROOFPILLOWS
SiR,—Eighteen years ago H. J. A. Longmore and I reportedthree patients with grand mal epilepsy who suffocated during sleepA further seven cases have since become known to me.2--4 Weadvocated the use of a smother-proof pillow by all sufferers of grandmal epilepsy, a suggestion taken up by the Epileptic Assocation.
I retired from general practice three years ago, so judge myastonishment when a distraught mother telephoned to inform methat her daughter, a 14-year-old with epilepsy, had died ofsuffocation during a seizure in the night. The daughter had been apupil in a large residential school for epileptic children. Sodistressed was the mother that she had searched the literature andtracked me down. She was especially upset because she had used asafety pillow at home and had assumed the school would do thesame-the school had not, although it does now.The death of yet another epileptic patient poses the question:
what more can be done to publicise this danger? Some doctors mayrequire further proof of the benefit of smother-proof pillows, eventhough no epileptic patient using such a pillow has been reported tosuffocate during a seizure. Recently the manufacturer has ensuredconformity to government fire regulations.The Whins,Kinnel Banks,Lochmaben,Lockerbie DG11 1TD J. B. WILSON
1 Longmore HJA, Wilson JB. Epileptic death due to suffocation during sleep Lancet1970, ii: 782
2 Wilson JB Suffocation in epilepsy Br Med J 1973; iv. 173.3 Wilson JB Hazards of epilepsy. Br Med J 1978; ii: 200.4 Wilson JB. Epilepsy. Br Med J 1979; i. 1218.
HISTIOCYTIC MEDULLARY RETICULOSIS:A LETHAL FORM OF PRIMARY EBV INFECTION IN
YOUNG CHILDREN IN TAIWAN
SiR,-Histiocytic medullary reticulosis (HMR) remainscontroversial in respect of aetiology and the nature of the atypical"histiocytes". The clinical features and geographical distribution ofHMR have led to the suggestion that it is a fatal form of infectiousmononucleosis.12We have observed a high frequency of HMR in Taiwan, as
reported from mainland China and Uganda.Z3 The disease affectedpreviously healthy young children who presented with fever,jaundice, hepatosplenomegaly, and pancytopenia; the illness lasted2-3 weeks. The seasonal clustering of cases in Taiwan in July,August, and September made us question whether NMR is aneoplastic disease. We have studied fresh lymphoid tissue from ayoung patient with HMR looking for Epstein-Barr virus (EBV) bySouthern blot and in situ DNA hybridisation and investigated the
lineage of these atypical large cells. We found a high copy number ofEBV genomes (more than 100 per cell) in the extracted tissue DNA.In situ hybridisation demonstrated that the EBV-positive granuleswere present in the cytoplasm of the atypical histiocytes.Immunohistochemical study revealed that these atypical histiocytesrepresented polyclonal B-immunoblastic lymphoproliferation. Wereviewed our necropsy material and found that these childhoodcases of HMR shared the following features: lymphoid organs,liver, spleen, lungs, and bone marrow showed diffuse sinusoidinfiltration with variable numbers of large atypical cells,plasmacytoid cells, lymphocytes, and mature histiocytes with activehaemophagocytosis.
Since the age prevalence of primary EBV infection in Taiwancorrelates quite well with the age distribution of our HMR patients,’we hypothesise that cases of HMR in young children in Taiwanmay be a consequence of primary EBV infection or a fatal form ofinfectious mononucleosis.A fatal form of EBV-induced lymphoproliferative disorder, with
clinical and haematological features of HMR, has been reported inpatients with acquired immunodeficiency and in organ transplantrecipients.5-8 We do not know whether our young patients had anunderlying immunodeficiency, however, they had been well beforethe onset of disease. We are now studying the immune status andEBV serology of HMR patients to clarify this point.
Departments of Pathologyand Paediatrics,
College of Medicine,National Taiwan University Hospital,Taipei, Taiwan, Republic of China
IH-JEN SUHONG-JONG HSIEHCHIN-YING LEE
1. Mallick NP, Davson J. Is histiocytic medullary reticulosis a fatal form of infectiousmononucleosis? Lancet 1981; ii: 43.
2. Martelli MF, Tabilio A, Aversa F, Falini B, Rocchi G. Is histiocytic medullaryreticulosis an infectious disease? Lancet 1982; ii: 446-47.
3. Amsel S, Bijlsma F. Histiocytic medullary reticulosis: clinical and pathological studiesin Uganda. Trop Geogr Med 1974; 26: 31-38.
4 Lm KH, Chiang CH, Yang CS. Age distribution and Epstem-Barr virus,cytomegalovirus, and rubella virus antibodies. J Formosan Med Assoc 1987; 86:1316-19.
5. Mroczek EC, Weisenburger DD, Grierson HL, Markm R, Purtilo DT. Fatalinfectious mononucleosis and virus-associated hemophagocytic syndrome. ArchPathol Lab Med 1987; 111: 530-35.
6. Beissner RS, Rappaport ES, Diaz JA Fatal case of Epstein-Barr virus-inducedlymphoproliferative disorder associated with a human immunodeficiency virusinfection. Arch Pathol Lab Med 1987; 111: 250-53
7. Zutter MM, Martin PJ, Sale GE, et al. Epstein-Barr virus lymphoproliferation afterbone marrow transplantation. Blood 1988; 72: 520-29.
8. Nalesnik MA, Jaffe R, Starzl TE, et al. The pathology of post-transplantlymphoproliferative disorders occurring in the setting of cyclosporineA-prednisone immunosuppression. Am J Pathol 1988; 133: 173-92.
POSTICTAL SPET IN EPILEPSY
SiR,—Your Jan 21 editorial discusses the value of metabolic
imaging with positron emission tomography (PET) and singlephoton emission tomography (SPET) in the localisation of theepileptic focus. Accurate localisation is essential in the surgicaltreatment of intractable temporal lobe epilepsy (TLE), a valuableand underused procedure.’ As you say, interictal PET is useful forthis purpose but is not widely used because of its very high cost.SPET is widely available and preliminary reports, which youreview, suggest that peri-ictal studies may be especially valuable.Over the past eighteen months we have done postictal SPET with99n’-technetium hexamethylpropyleneamine oxime (99IDTc-HMPAO) in 45 patients with unilateral temporal lobe epilepsydiagnosed by ictal electroencephalogram (EEG) recordings.z°3 Thisstudy confirmed the value of postictal SPET and revealed hithertounknown features of postictal cerebral blood flow.
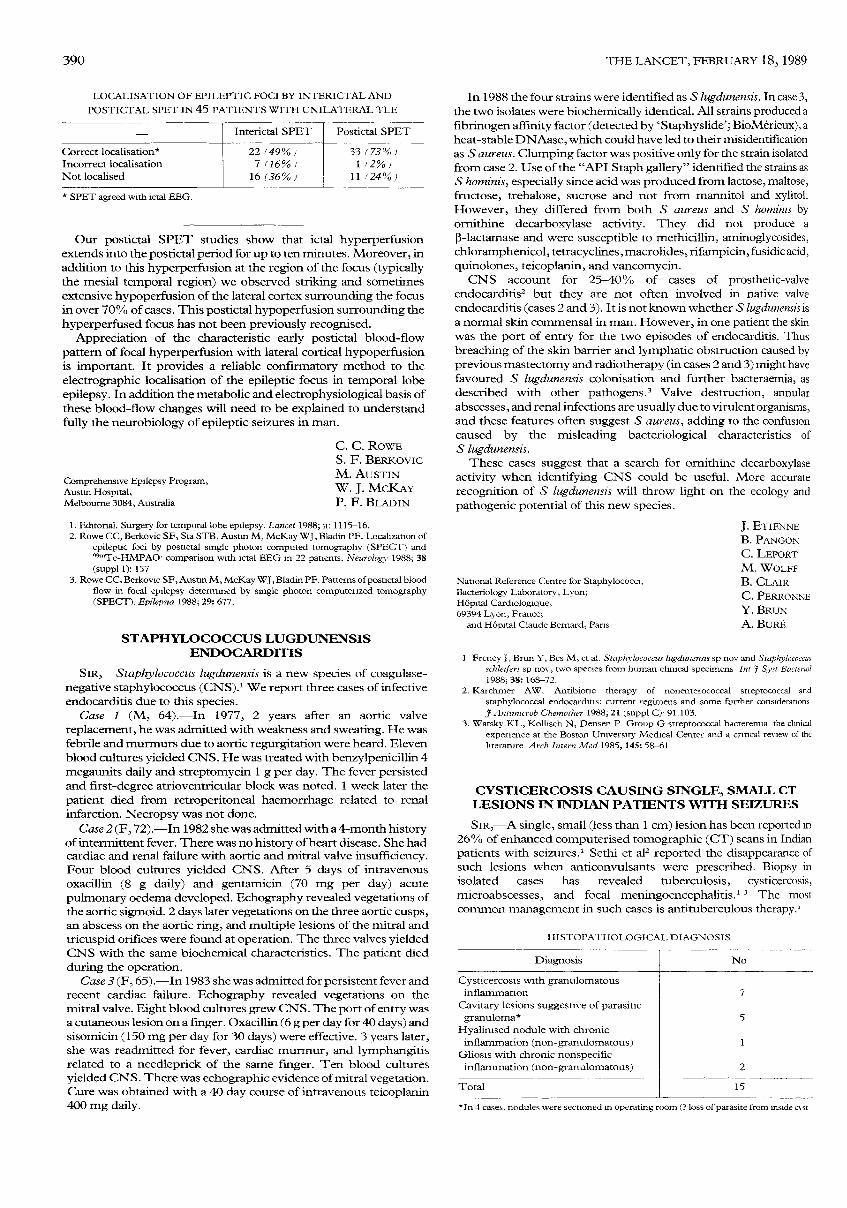
Whilst interictal SPET with lz3l_iodoamphetamines or 99IDTc-HMPAO shows hypoperfusion in a significant proportion ofpatients with temporal lobe epilepsy, our data with HMPAOdemonstrate that interictal abnormalities are not sufficiently specificto localise the epileptic focus confidently (table). In contrast,characteristic patterns of postictal perfusion2 gave correct
localisation in 33 of 45 cases (73%) and incorrect localisation in only1 patient. Our preliminary quantitative SPET analyses agree withthe quantitative interpretation.
390
LOCALISATION OF EPILEPTIC FOCI BY INTERICTAL AND
POSTICTAL SPET IN 45 PATIENTS WITH UNILATERAL TLE
* SPET agreed with ictal EEG.
Our postictal SPET studies show that ictal hyperperfusionextends into the postictal period for up to ten minutes. Moreover, inaddition to this hyperperfusion at the region of the focus (typicallythe mesial temporal region) we observed striking and sometimesextensive hypoperfusion of the lateral cortex surrounding the focusin over 70% of cases. This postictal hypoperfusion surrounding thehyperperfused focus has not been previously recognised.
Appreciation of the characteristic early postictal blood-flowpattern of focal hyperperfusion with lateral cortical hypoperfusionis important. It provides a reliable confirmatory method to theelectrographic localisation of the epileptic focus in temporal lobeepilepsy. In addition the metabolic and electrophysiological basis ofthese blood-flow changes will need to be explained to understandfully the neurobiology of epileptic seizures in man.
Comprehensive Epilepsy Program,Austin Hospital,Melbourne 3084, Australia
C. C. ROWES. F. BERKOVICM. AUSTINW. J. MCKAYP. F. BLADIN
1. Editorial. Surgery for temporal lobe epilepsy. Lancet 1988; ii: 1115-16.2. Rowe CC, Berkovic SF, Sia STB, Austin M, McKay WJ, Bladin PF. Localization of
epileptic foci by postictal single photon computed tomography (SPECT) and99mTc-HMPAO comparison with ictal EEG in 22 patients. Neurology 1988; 38(suppl 1): 157
3. Rowe CC, Berkovic SF, Austin M, McKay WJ, Bladin PF. Patterns of postictal bloodflow in focal epilepsy determined by single photon computerized tomography(SPECT). Epilepsia 1988; 29: 677.
STAPHYLOCOCCUS LUGDUNENSISENDOCARDITIS
SrR,-Staphylococcus lugdunensis is a new species of coagulase-negative staphylococcus (CNS).1 We report three cases of infectiveendocarditis due to this species.
Case 1 (M, 64).-In 1977, 2 years after an aortic valve
replacement, he was admitted with weakness and sweating. He wasfebrile and murmurs due to aortic regurgitation were heard. Elevenblood cultures yielded CNS. He was treated with benzylpenicillin 4megaunits daily and streptomycin 1 g per day. The fever persistedand first-degree atrioventricular block was noted. 1 week later thepatient died from retroperitoneal haemorrhage related to renalinfarction. Necropsy was not done.
Case 2 (F, 72).-In 1982 she was admitted with a 4-month historyof intermittent fever. There was no history of heart disease. She hadcardiac and renal failure with aortic and mitral valve insufficiency.Four blood cultures yielded CNS. After 5 days of intravenousoxacillin (8 g daily) and gentamicin (70 mg per day) acute
pulmonary oedema developed. Echography revealed vegetations ofthe aortic sigmoid. 2 days later vegetations on the three aortic cusps,an abscess on the aortic ring, and multiple lesions of the mitral andtricuspid orifices were found at operation. The three valves yieldedCNS with the same biochemical characteristics. The patient diedduring the operation.
Case 3 (F, 65).-In 1983 she was admitted for persistent fever andrecent cardiac failure. Echography revealed vegetations on themitral valve. Eight blood cultures grew CNS. The port of entry wasa cutaneous lesion on a finger. Oxacillin (6 g per day for 40 days) andsisomicin (150 mg per day for 30 days) were effective. 3 years later,she was readmitted for fever, cardiac murmur, and lymphangitisrelated to a needleprick of the same finger. Ten blood culturesyielded CNS. There was echographic evidence of mitral vegetation.Cure was obtained with a 40 day course of intravenous teicoplanin400 mg daily.
In 1988 the four strains were identified as S lugdunensis. In case 3,the two isolates were biochemically identical. All strains produced afibrinogen affinity factor (detected by ’Staphyslide’; BioMerieux), aheat-stable DNAase, which could have led to their misidentificationas S aureus. Clumping factor was positive only for the strain isolatedfrom case 2. Use of the "API Staph gallery" identified the strains asS hominis, especially since acid was produced from lactose, maltose,fructose, trehalose, sucrose and not from mannitol and xylitol.However, they differed from both S aureus and S hotniiiis byornithine decarboxylase activity. They did not produce a
p-lactamase and were susceptible to methicillin, aminoglycosides,chloramphenicol, tetracyclines, macrolides, rifampicin, fusidic acid,quinolones, teicoplanin, and vancomycin.CNS account for 25-40% of cases of prosthetic-valve
endocarditis2 but they are not often involved in native valveendocarditis (cases 2 and 3). It is not known whether S lugdunensis isa normal skin commensal in man. However, in one patient the skinwas the port of entry for the two episodes of endocarditis. Thusbreaching of the skin barrier and lymphatic obstruction caused byprevious mastectomy and radiotherapy (in cases 2 and 3) might havefavoured S lugdunensis colonisation and further bacteraemia, asdescribed with other pathogens.3 Valve destruction, annular
abscesses, and renal infections are usually due to virulent organisms,and these features often suggest S aureus, adding to the confusioncaused by the misleading bacteriological characteristics ofS lugdunensis.These cases suggest that a search for ornithine decarboxylase
activity when identifying CNS could be useful. More accuraterecognition of S lugdunensis will throw light on the ecology andpathogenic potential of this new species.
National Reference Centre for Staphylococci,Bacteriology Laboratory, Lyon;Hôpital Cardiologique,69394 Lyon, France;
and Hôpital Claude Bernard, Pans
J. ETIENNEB. PANGON
C. LEPORTM. WOLFFB. CLAIRC. PERRONNEY. BRUNA. BURÉ
1 Freney J, Brun Y, Bes M, et al. Staphylococcus lugdunensis sp nov and Staphylococcusschleiferi sp nov, two species from human clinical specimens Int J Syst Bacteriol1988; 38: 168-72.
2. Karchmer AW. Antibiotic therapy of nonenterococcal streptococcal and
staphylococcal endocarditis: current regimens and some further considerationsJ Antimicrob Chemother 1988; 21 (suppl C) 91.103.
3. Watsky KL, Kollisch N, Densen P Group G streptococcal bacteremia the clinicalexperience at the Boston University Medical Center and a critical review of theliterature Arch Intern Med 1985, 145: 58-61
CYSTICERCOSIS CAUSING SINGLE, SMALL CTLESIONS IN INDIAN PATIENTS WITH SEIZURES
SIR,-A single, small (less than 1 cm) lesion has been reported m26% of enhanced computerised tomographic (CT) scans in Indianpatients with seizures.’ Sethi et ap reported the disappearance ofsuch lesions when anticonvulsants were prescribed. Biopsy in
isolated cases has revealed tuberculosis, cysticercosis,microabscesses, and focal meningoencephalitis.’ The most
common management in such cases is antituberculous therapy.’
HISTOPATHOLOGICAL DIAGNOSIS
*In 4 cases, nodules were sectioned m operating room(? loss of parasite from mstde 0st

















![Anni, spet ornk akcija! [back2school 2011]](https://img.pdfslide.net/doc/110x75/568c0e361a28ab955a8fa986/anni-spet-ornk-akcija-back2school-2011.jpg)