Embed Size (px)
Citation preview
J Clin Pathol 1984;37:1282-1288
Postmortem radiographic, histological andbacteriological studies of terminal respiratoryinfections and other pulmonary lesions in hospital andnon-hospital necropsiesPAAVO PAAKKO,* TERTTU SARKIOJA,t JORMA HIRVONEN,t TAPIO NURMI,JREIJO LAHTI,§ SEPPO SUTINEN*
From the Departments ofPathology, * Forensic Medicine, t Medical Microbiology, t and DiagnosticRadiology, § University of Oulu, Finland
SUMMARY One lung from 109 unselected hospital and 43 unselected non-hospital necropsies wasstudied using postmortem radiography with histological verification. Signs of acute bacterialinfection, including bronchiolitis or bronchopneumonia, were present in 42-2% of the hospitalnecropsies and infection was the immediate cause of death in 8-3%. There was only one case ofincipient bronchopneumonia among the non-hospital necropsies. Emphysema was the mostcommon other pulmonary lesion in both groups.
Gram negative bacteria were found significantly more often in the bronchial mucus of lungswith any pulmonary lesion, particularly those with signs of bacterial infection, than in the bron-chial mucus of morphologically normal lungs in both groups of patients. In addition, the fre-quency of infections was associated with length of stay in hospital. This may reflect the prevalenceof Gram negative infections in hospitals.
Bacterial pneumonia is common in postmortem mat-erial,'-4 and is found in about half of the cases seenat necropsy. There are no studies of the simultane-ous prevalence of other lesions in the lungs at nec-ropsy, which moreover, might predispose to infec-tion. The pathological verification of pneumonia haslargely been based on macroscopic observations. Inour experience, however, even considerablepneumonic foci may go undetected macroscopically,whereas radiography of excised and air inflatedlungs5 has proved reliable in detecting even minutepneumonic changes.6
Colonisation of the respiratory tract by Gramnegative bacilli has been shown in patients in hospi-tal.'-9 We have also found a significant associationbetween length of stay in hospital and the occur-rence of Gram negative bacteria both in the bron-chial mucus and heart blood at necropsy (Paakkoet al, unpublished observations) but correlationsbetween postmortem bacteriology and morphologi-cal pulmonary lesions studied systematically havenot yet been presented.
Accepted for publication 13 June 1984
In this study we have used postmortem radiogra-phy of excised lungs with histological verification todetermine how often pulmonary lesions, especiallyterminal bacterial infections, occur in hospital andnon-hospital necropsies and how often infection isthe immediate cause of death.
Material and methods
The material consisted of 152 unselected adult nec-ropsies: 109 represented deaths in hospital and 43deaths outside hospital. The hospital series com-prised 67 men and 42 women (aged 22 to 89 years;mean 66 years); the non-hospital series consisted of36 men and 7 women (aged 15 to 80 years; mean 53years). Necropsies of the former series were per-formed one to eight days after death (average 3.9)and those of the latter one to 11 days after death(average 4.4). Almost all bodies were placed in arefrigerator within 4 h of death and preserved at 4°Cuntil necropsy. In 12 forensic cases the bodies hadbeen left at room temperature for from 5 h to 7 days(mean 41 hours) before being placed in arefrigerator. Of the hospital necropsies, 69 right and
1282
copyright. on 16 June 2019 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.37.11.1282 on 1 Novem
ber 1984. Dow
nloaded from
Postmortem studies of terminal respiratory infections
Table 1 Causes ofdeath in hospital and non-hospitalpatients
Cause ofdeath Type ofpatient
Hospital Non-hospital
Cardiovascular diseases 68 18Ischaemic heart diseases 38 16Cerebrovascular disease 19Others 11 2
Malignant neoplasms 22Respiratory organs 4Others 18
Respiratory diseases 9Emphysema 4Asthma 2Others 3
Other natural deaths 10 2Violent deaths
(suicides, accidents, etc) 23Total 109 43
40 left lungs were studied; of the non-hospital nec-
ropsies 37 right and 6 left lungs were studied. Table1 gives the main causes of death in hospital andnon-hospital patients.An aspirate of bronchial mucus for culture was
obtained with a sterile disposable syringe from thelower lobe bronchus as deep as possible immediatelyafter the severance of the main bronchus. Afteraspiration, a sterile needle with a rubber stopper wasattached to the syringe. A heart blood sample wasaspirated from the left ventricle before dissectingthe lungs and heart and immediately injected intoblood culture bottles at room temperature(Hemobact A and B, Orion Diagnostica, Finland).All microbiological specimens were taken to thebacteriology laboratory as soon as possible, whereGram staining, cultures of aerobic and anaerobicbacteria and fungi, and isolation of chlamydia were
performed within about 1 h of the collection of thespecimens. The mucus and blood specimens werecultured on blood, chocolate, and lactose agar andincubated for 96 h under both aerobic andanaerobic conditions before being discarded asnegative. Positive cultures were immediately subcul-tured on appropriate solid agar media for isolationof colonies. Final species identification was madeusing differential media and tests.'" Sabour andmedia for the recovery of fungi were used. The isola-tion of chlamydia was performed using culturedMcCoy cells."For the recognition of pulmonary lesions one lung
of each patient was excised and radiographed aftertying the blood vessels during continuous airinflation, fixed intrabronchially with a formalin,polyethylene glycol, and alcohol solution, dried byair insufflation, and sliced sagittally.5 For histologi-cal examination, five 5 x 5 cm tissue blocks werecollected systematically. In addition, a large number
1283
of tissue blocks were taken from interesting areasseen in the radiographs. Sections (15 ,um) mountedon photographic glass slides were first examined byprojecting them on to a screen, and the lesions thusseen were further studied microscopically at higherpower on corresponding 6 ,um sections.
In this study the following lesions were recordedseparately: inflammatory changes, emphysema,chronic congestion, alveolar haemorrhage, infarc-tion, scars, non-specific interstitial fibrosis, bron-chiectasis, bronchogenic cysts, and neoplasms.Alveolar and interstitial (lobular) oedema were notincluded here but were regarded as a sign of themechanism of death.
INFLAMMATORY CHANGESNo case of acute lobar pneumonia was found ineither series. Acute bronchiolitis and lobularpneumonia were regarded as signs of acute bacterialinfection in the lung tissue. Acute bronchiolitismanifested itself as an inflammatory exudate in thelumen and mucosa of the bronchioli.2 Intra-alveolarpolymorphonuclear leucocytic exudate without con-comitant interstitial inflammatory infiltration wasdiagnosed as lobular or bronchopneumonia. If theinflammatory focus was not visible in the radiographor was otherwise small, solitary, and limited, weclassified the lesion as incipient. Other types ofinflammation of the lung tissue such as usual intersti-tial pneumonia,'2 tuberculous pneumonia, chroniclobar pneumonia with granulomatous necroticinflammation, carnification pneumonia,2 andgranulomatous inflammation were also recordedseparately.
OTHER PULMONARY LESIONSThe severity of emphysema was evaluated on thebasis of the radiographs of excised lungs'3 and grossspecimens using a set of photographs of standardgrades.'4 Grades 10-20 represented mild, grades30-50 moderate, and grade 60 or more severe em-physema.'5 Emphysema was classified as centrilobu-lar, panlobular, or paracicatricial.5Abundant alveolar macrophage collections
("heart failure cells") were regarded as a sign ofchronic congestion. Necrosis of tissue with haemor-rhage was required for the diagnosis of fresh infarc-tion.'6 Scars included parenchymal and pleural scars,as well as foci of tuberculosis. Non-specific intersti-tial fibrosis included local alveolar wall fibrosis,fibrosis of the lobular septa, and honeycombing ofthe lung.'2 Neoplastic lesions included primary neo-plasms and pulmonary metastases.
Information about length of stay in hospital wasobtained from the hospital records. The significanceof associations was determined using the X2 test or
copyright. on 16 June 2019 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.37.11.1282 on 1 Novem
ber 1984. Dow
nloaded from
1284
Table 2 Macroscopic, radiographic andlor histologicalfindings in lungs from hospital and non-hospital
*necropsies
Macroscopic, radiographic Hospital Non-hospitalandlor histological finding necropsies necropsies
No (%) No (%)o
Normal lung 10 (9.2) 10 (23.3)Inflammatory changest 53 (48.6) 3 (7.0)Emphysema (all grades) 54 (49.5 19 (44-2)Chronic congestion 37 (33-9 10 (23.3)Alveolar haemorrhage 18 (16-5 5 (11.6)Infarction 8 (7.3 4 (9-3)Scars 40 (36-7 13 (302)Non-specific interstitial fibrosis 9 (8-3) -Bronchiectasis 1 (0.9 -Bronchogenic cyst 1 (0. -Neoplasm 4 (3.7) -Total 109 43
*Some lungs showed more than one lesion.tSignificant difference between the two groups (p < 0-003).
Student's t test or by calculating the standard errorof the difference between two proportions.'7
Results
PULMONARY LESIONSMacroscopic and radiographic and/or histologicalfindings in the lungs from the hospital and non-hospital necropsies are shown in Table 2. Most ofthe lungs showed more than one lesion, and theproportion of completely normal lungs was low inboth groups (9.2% and 23-3%, respectively).
Poaakko, Sarkioja, Hirvonen, Nurmi, Lahti, Sutinen
Table 3 Morphological signs ofinfiammalion in lungsfrom hospital and non-hospital necropsies
Morphological finding Hospital Non-hospitalnecropsies necropsies
No (to) No (%o)
No inflammatory changes 56 (51-4) 40 (93-0)Signs of acute bacterial infection 46 (42.2)* 1 (2 3)
Bronchiolitis 3Incipient bronchopneumonia 16 1Bronchopneumonia 27
Other types of inflammation 7 (6-4) 2 (4-7)Interstitial pneumonia 2Tuberculous pneumonia 2 1Chronic lobar pneumonia withgranulomatous necrotic foci 1Chronic pneumonia withcarnification 1Granulomatous inflammation(Sarcoidosis) 1 1
Total 109 (100-0) 43 (100-0)
*Significant difference between two groups (p < 0-003).
INFLAMMATORY LESIONSMorphological signs of inflammation found in thelungs from the hospital and non-hospital necropsiesare shown in Table 3. The hospital series containedsignificantly more cases with acute inflammationthan the non-hospital series. In nine of the hospitalseries (8.3%) bronchopneumonia was considered tobe the immediate cause of death. In addition, someother type of inflammation was seen in seven lungs(6.4%). Two of these represented interstitialpneumonia, and five chronic or granulomatousinflammation. Two of the latter were confirmed as
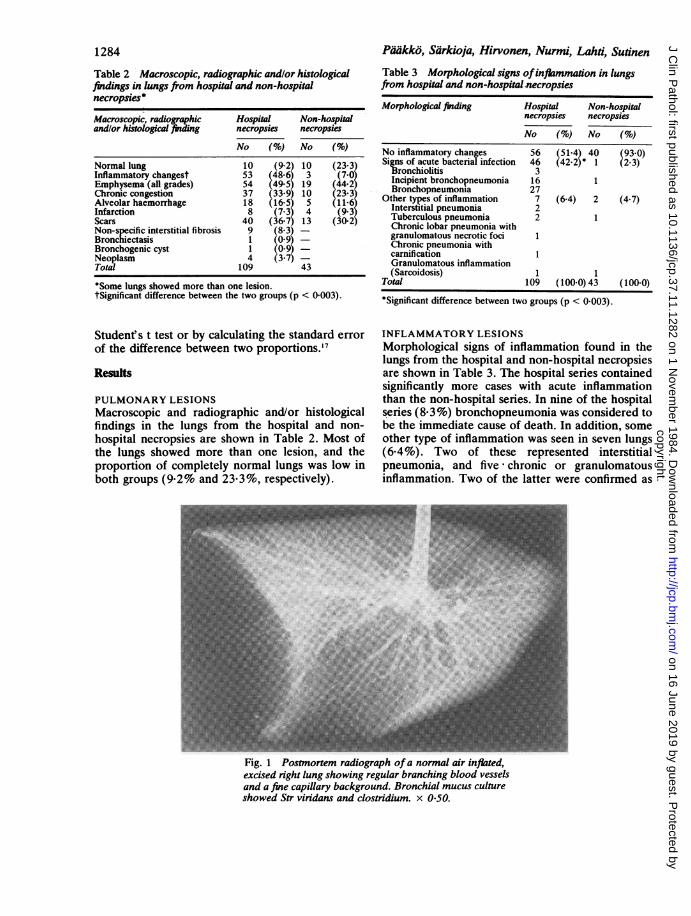
Fig. 1 Postmortem radiograph of a normal air inflated,excised right lung showing regular branching blood vesselsand a fine capillary background. Bronchial mucus cultureshowed Str viridans and clostridium. x 0-50.
copyright. on 16 June 2019 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.37.11.1282 on 1 Novem
ber 1984. Dow
nloaded from
Postmortem studies of terminal respiratory infections
Table 4 Hospital necropsies: number ofoccasionsdifferent species were isolated from bronchial mucusspecimens correlated with macroscopic radiographic andlorhistological findings ofany pulmonary lesion
Species isolated from No of occasions species isolatedbronchial mucus
Macroscopic and radiographicandlor histological funding in lung
Normal Abnormal Total
Gram positive cocci* 22 151 173Gram negative bacteriat 3 87 90Otherst 9 44 53Negative cultures - 5Insufficient specimen - 1Total number of occasions
different species isolated 34 282 316Total number of cases 10 99 109Average number of species perspecimen§ 3-4 2-9 3-1
XI = 8-00, p < 0 025 (negative cultures and insufficient specimenexcluded).*Str viridans, Str non-haemolyticus, Str faecalis, Staph aureus, Str8-haemolyticus, Staph epidermidis, Diplococcus pneumoniae,sarcina, unspecified.tE coli, klebsiella, proteus, enterobacter, pseudomonas,bacteroides, serratia, citrobacter, haemophilus, acinetobacter,unspecified.tGram negative cocci: neisseria, veillonella, unspecified.Gram positive rods: difteroid, bacillus, clostridium,corynebacterium.Fungi: candida, Torulopsis glabrata, Geotrichum candidum,aspergillus.Minibacterium: chlamydia.§Difference between groups not significant.
1285
Table 5 Non-hospital necropsies: number ofoccasionsdifferent species were isolated from bronchial mucusspecimens correlated with macroscopic, radiographic andlor histological findings ofany pulmonary lesion
Species isolated from No of occasions species isolatedbronchial mucus
Macroscopic and radiographicandlor histological findingNormal Abnormal Total
* Gram positive cocci* 18 56 74Gram negative bacteriat 1 23 24Otherst 5 14 19Negative culture 1Total number of occasions
different species isolated 24 93 117Total number of cases 10 33 43Average number of species per
specimen§ 2-4 2-8 2-8
X2= 495, p < 0-05 (negative culture excluded, gram positive cocciand others combined).*Str viridans, Str non-haemolyticus, Staph aureus, Diplococcuspneumoniae, Str ,B-haemolyticus, Staph epidermidis.tE coli, Haemophilus influenzae, Klebsiella, bacteroides,enterobacter, proteus, pseudomonas.tGram negative cocci: neissena.Gram positive rods: difteroid, clostridium, corynebacterium,unspecified.Fungi: candida.§Difference between groups not significant.
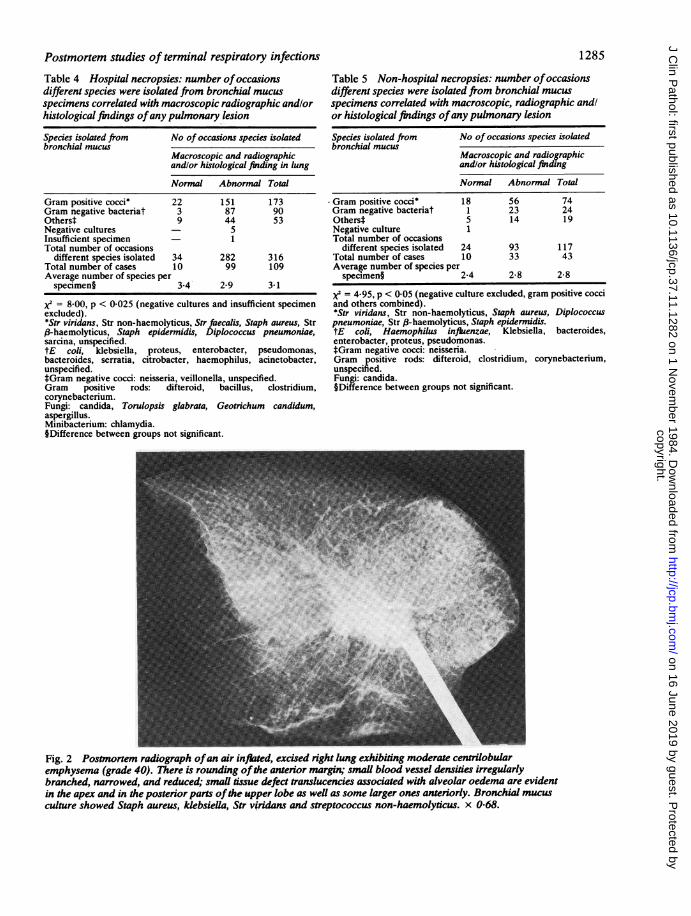
Fig. 2 Postmortem radiograph ofan air inflated, excised right lung exhibiting moderate centrilobularemphysema (grade 40). There is rounding ofthe anterior margin; smaUl blood vessel densities irregularlybranched, narrowed, and reduced, small tssue defect translucencies associated with alveolar oedema are evidentin the apex and in the posterior parts ofthe upper lobe as well as some larger ones anteriorly. Bronchial mucusculture showed Staph aureus, kdebsieUla, Str vfridans and streptococcus non-haemolyticus. x 0-68.
copyright. on 16 June 2019 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.37.11.1282 on 1 Novem
ber 1984. Dow
nloaded from
1286Padkko, Sarkioja, Hirvonen, Nurmi, Lahti, Sufinen
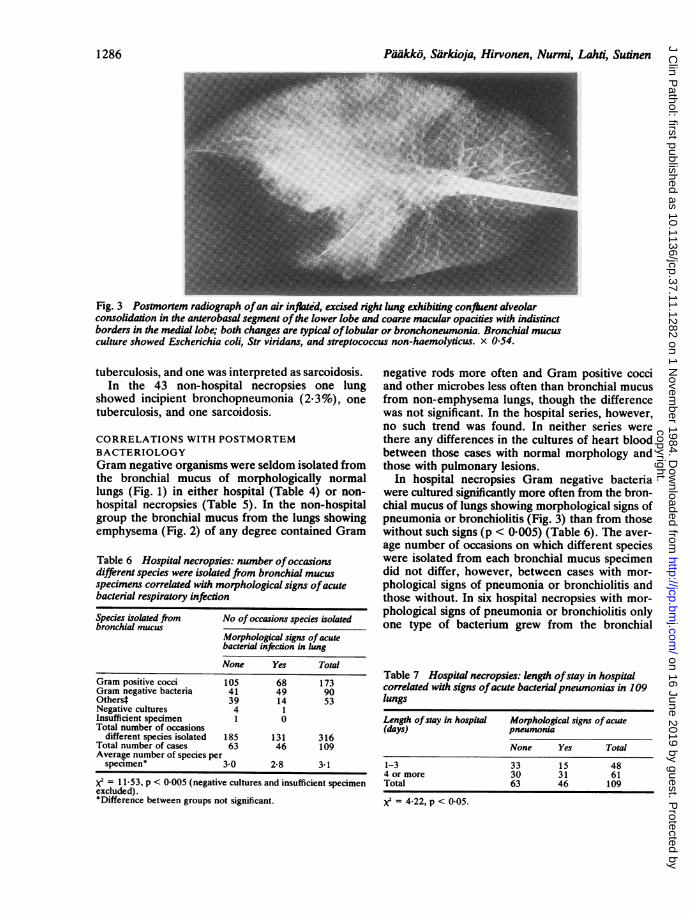
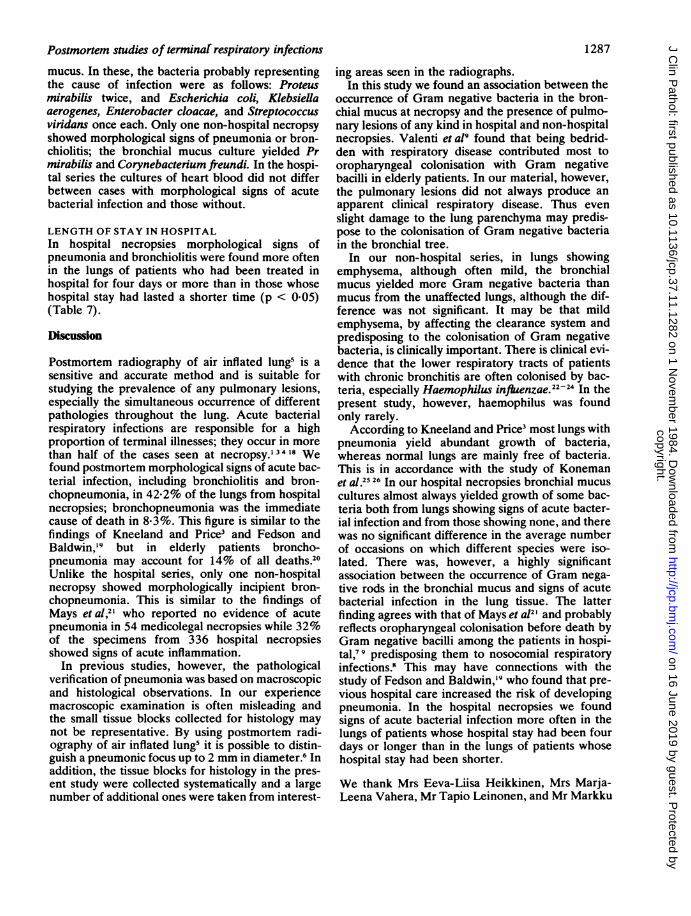
Fig. 3 Postmortem radiograph ofan air inflated, excised right lung exhibiting confluent alveolarconsolidation in the anterobasal segment ofthe lower lobe and coarse macular opacities with indisdnctborders in the medial lobe; both changes are typical oflobular or bronchoneumonia. Bronchial mucusculture showed Escherichia coli, Str viridans, and streptococcus non-haemolydcus. x 054.
tuberculosis, and one was interpreted as sarcoidosis.In the 43 non-hospital necropsies one lung
showed incipient bronchopneumonia (2.3%), onetuberculosis, and one sarcoidosis.
CORRELATIONS WITH POSTMORTEMBACTERIOLOGYGram negative organisms were seldom isolated fromthe bronchial mucus of morphologically normallungs (Fig. 1) in either hospital (Table 4) or non-hospital necropsies (Table 5). In the non-hospitalgroup the bronchial mucus from the lungs showingemphysema (Fig. 2) of any degree contained Gram
Table 6 Hospital necropsies: number ofoccasionsdifferent species were isolated from bronchial mucusspecimens correlated with morphological signs ofacutebacterial respiratory infection
Species isolated from No of occasions species isolatedbronchial mucus
Morphological signs of acutebacterial infection in lung
None Yes Total
Gram positive cocci 105 68 173Gram negative bacteria 41 49 90Others* 39 14 53Negative cultures 4 1Insufficient specimen 1 0Total number of occasions
different species isolated 185 131 316Total number of cases 63 46 109Average number of species perspeclmen* 3-0 2-8 3-1
X2 = 11-53, p < 0-005 (negative cultures and insufficient specimenexcluded).*Difference between groups not significant.
negative rods more often and Gram positive cocciand other microbes less often than bronchial mucusfrom non-emphysema lungs, though the differencewas not significant. In the hospital series, however,no such trend was found. In neither series werethere any differences in the cultures of heart bloodbetween those cases with normal morphology andthose with pulmonary lesions.
In hospital necropsies Gram negative bacteriawere cultured significantly more often from the bron-chial mucus of lungs showing morphological signs ofpneumonia or bronchiolitis (Fig. 3) than from thosewithout such signs (p < 0.005) (Table 6). The aver-age number of occasions on which different specieswere isolated from each bronchial mucus specimendid not differ, however, between cases with mor-phological signs of pneumonia or bronchiolitis andthose without. In six hospital necropsies with mor-phological signs of pneumonia or bronchiolitis onlyone type of bacterium grew from the bronchial
Table 7 Hospital necropsies: length ofstay in hospitalcorrelated with signs ofacute bacterial pneumonias in 109lungs
Length ofstay in hospital Morphological signs of acute(days) pneumonia
None Yes Total
1-3 33 1 5 484 or more 30 31 61Total 63 46 109
X= 4-22, p < 005.
1286
copyright. on 16 June 2019 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.37.11.1282 on 1 Novem
ber 1984. Dow
nloaded from
Postmortem studies of terminaf respiratory infections
mucus. In these, the bacteria probably representingthe cause of infection were as follows: Proteusmirabilis twice, and Escherichia coli, Klebsiellaaerogenes, Enterobacter cloacae, and Streptococcusviridans once each. Only one non-hospital necropsyshowed morphological signs of pneumonia or bron-chiolitis; the bronchial mucus culture yielded Prmirabilis and Corynebacterium freundi. In the hospi-tal series the cultures of heart blood did not differbetween cases with morphological signs of acutebacterial infection and those without.
LENGTH OF STAY IN HOSPITALIn hospital necropsies morphological signs ofpneumonia and bronchiolitis were found more oftenin the lungs of patients who had been treated inhospital for four days or more than in those whosehospital stay had lasted a shorter time (p < 0.05)(Table 7).
Discussion
Postmortem radiography of air inflated lung5 is asensitive and accurate method and is suitable forstudying the prevalence of any pulmonary lesions,especially the simultaneous occurrence of differentpathologies throughout the lung. Acute bacterialrespiratory infections are responsible for a highproportion of terminal illnesses; they occur in morethan half of the cases seen at necropsy.' 34 18 Wefound postmortem morphological signs of acute bac-terial infection, including bronchiolitis and bron-chopneumonia, in 42-2% of the lungs from hospitalnecropsies; bronchopneumonia was the immediatecause of death in 8-3%. This figure is similar to thefindings of Kneeland and Price3 and Fedson andBaldwin,'9 but in elderly patients broncho-pneumonia may account for 14% of all deaths.20Unlike the hospital series, only one non-hospitalnecropsy showed morphologically incipient bron-chopneumonia. This is similar to the findings ofMays etal,2' who reported no evidence of acutepneumonia in 54 medicolegal necropsies while 32%of the specimens from 336 hospital necropsiesshowed signs of acute inflammation.
In previous studies, however, the pathologicalverification of pneumonia was based on macroscopicand histological observations. In our experiencemacroscopic examination is often misleading andthe small tissue blocks collected for histology maynot be representative. By using postmortem radi-ography of air inflated lung5 it is possible to distin-guish a pneumonic focus up to 2 mm in diameter.6 Inaddition, the tissue blocks for histology in the pres-ent study were collected systematically and a largenumber of additional ones were taken from interest-
1287
ing areas seen in the radiographs.In this study we found an association between the
occurrence of Gram negative bacteria in the bron-chial mucus at necropsy and the presence of pulmo-nary lesions of any kind in hospital and non-hospitalnecropsies. Valenti et a!9 found that being bedrid-den with respiratory disease contributed most tooropharyngeal colonisation with Gram negativebacilli in elderly patients. In our material, however,the pulmonary lesions did not always produce anapparent clinical respiratory disease. Thus evenslight damage to the lung parenchyma may predis-pose to the colonisation of Gram negative bacteriain the bronchial tree.
In our non-hospital series, in lungs showingemphysema, although often mild, the bronchialmucus yielded more Gram negative bacteria thanmucus from the unaffected lungs, although the dif-ference was not significant. It may be that mildemphysema, by affecting the clearance system andpredisposing to the colonisation of Gram negativebacteria, is clinically important. There is clinical evi-dence that the lower respiratory tracts of patientswith chronic bronchitis are often colonised by bac-teria, especially Haemophilus infLenzae.2224 In thepresent study, however, haemophilus was foundonly rarely.According to Kneeland and Price3 most lungs with
pneumonia yield abundant growth of bacteria,whereas normal lungs are mainly free of bacteria.This is in accordance with the study of Konemanet al.2526 In our hospital necropsies bronchial mucuscultures almost always yielded growth of some bac-teria both from lungs showing signs of acute bacter-ial infection and from those showing none, and therewas no significant difference in the average numberof occasions on which different species were iso-lated. There was, however, a highly significantassociation between the occurrence of Gram nega-tive rods in the bronchial mucus and signs of acutebacterial infection in the lung tissue. The latterfinding agrees with that of Mays et a12' and probablyreflects oropharyngeal colonisation before death byGram negative bacilli among the patients in hospi-tal,' 9 predisposing them to nosocomial respiratoryinfections.8 This may have connections with thestudy of Fedson and Baldwin,'9 who found that pre-vious hospital care increased the risk of developingpneumonia. In the hospital necropsies we foundsigns of acute bacterial infection more often in thelungs of patients whose hospital stay had been fourdays or longer than in the lungs of patients whosehospital stay had been shorter.
We thank Mrs Eeva-Liisa Heikkinen, Mrs Marja-Leena Vahera, Mr Tapio Leinonen, and Mr Markku
copyright. on 16 June 2019 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.37.11.1282 on 1 Novem
ber 1984. Dow
nloaded from

1288
Koskela for technical assistance. This study wassupported by grants for the Sigrid Juselius Founda-tion and the Finnish Anti-Tuberculosis Association,Helsinki, Finland.
References
Smillie WG, Duerschner DR. The epidemiology of terminalbronchopneumonia. II The selectivity of nasopharyngeal bac-teria in invasion of the lungs. Am J Hyg 1947;45: 13-8.
2 Spencer H. Pathology of the lung. 3rd ed. Vol 1. Oxford: Perga-mon Press, 1977.
Kneeland Y, Price KM. Antibiotics and terminal pneumonia. AmJ Med 1960;29:967-79.
4Polednak AP. Postmortem bacteriology and pneumonia in amentally retarded population. Am J Clin Pathol 1977;67:190-5.
Sutinen S, Paakko P, Lahti R. Post-mortem inflation, radiogra-phy, and fixation of human lungs: A method for radiologicaland pathological correlations and morphometric studies.Scand J Respir Dis 1979;60:29-35.
6 Paakko P, Sutinen S, Lahti R. Pattern recognition in radiographsof excised air-inflated human lungs: II Acute inflammation innon-emphysematous lungs. Eur J Respir Dis 1981;62:33-45.
'Johanson WG, Pierce AK, Sanford JP. Changing pharyngealbacterial flora of hospitalized patients. Emergence of Gram-negative bacilli. N Engl J Med 1969;281:1137-40.
Johanson WG, Pierce AK, Sanford JP, Thomas GD. Nosocomialrespiratory infections with gram-negative bacilli. Ann InternMed 1972;77:200-3.
Valenti WM, Trudell RG, Bentley DW. Factors predisposing tooropharyngeal colonization with gram-negative bacilli in theaged. N Engl J Med 1978;298:1108-11.
10 Buchanan RE, Gibbons NE. Bergey's manual of determinativebacteriology. 8th ed. Baltimore: Williams and Wilkins Com-pany, 1974.
Gordon FB, Quan AI. Isolation of the trachoma agent in cellculture. Proc Soc Exp Biol Med 1965;118:354-9.
2 Liebow AA. Definition and classification of interstitialpneumonias in human pathology. Prog Resp Res 1975; 8:1-33.
3 Sutinen S, Paakko P, Lohela P, Lahti R. Pattern recognition inradiographs of excised air-inflated human lungs: IV
Paakko, Sarkioja, Hirvonen, Nurmi, Lahti, Sutinen
Emphysema alone and with other common lesions. Eur JRespir Dis 1981;62:297-314.
4 Thurlbeck WM, Dunnill MS, Hartung W, Heard BE, HepplestonAG, Ryder RC. A comparison of three methods of measuringemphysema. Hum Pathol 1970; 1:215-26.
Sutinen S, Vaajalahti P, Paakko P. Prevalence, severity, andtypes of pulmonary emphysema in a population of deaths in aFinnish city: Correlation with age, sex and smoking. Scand JRespir Dis 1978;59:101-5.
16 Spencer H. Pathology ofthe lung. 3rd ed. Vol 2. Oxford: Perga-mon Press, 1977.
7 Hill AB. Principles ofmedical staistiscs. 7th ed. Edinburgh: R andR Clark Ltd, 1961.
18 Zanem-Lim OG, Zanen HC. Postmortem bacteriology of thelung by printculture of frozen tissue: A technique for in situculture of microorganisms in whole frozen organs. J ClinPathol 1980;33:474-80.
91 Fedson DS, Baldwin JA. Previous hospital care as a risk factorfor pneumonia. JAMA 1982; 248:1989-95.
20 Gerber IE. Terminal pneumonia in the aged. Mt Sinai J Med1980;47:166-7.
21 Mays BB, Thomas GD, Leonard JS, Southern PM, Pierce AK,Sanford JP. Gram-negative bacillary necrotizing pneumonia:A bacteriologic and histopathologic correlation. J Infect Dis1969; 120:687-97.
22 Brumfitt W, Willoughby MLN, Bromley LL. An evaluation ofsputum examination in chronic bronchitis. Lancet 1957;ii: 1306-9.
23 Lees AW, McNaught W. Bacteriology of lower-respiratory-tractsecretions, sputum, and upper-respiratory-tract secretions in"normals" and chronic bronchitics. Lancet 1959;ii: 1112-5.
24Laurenzi GA, Potter RT, Kass EH. Bacteriologic flora of thelower respiratory tract. N Engl J Med 1961;265: 1273-8.
25 Koneman EW, Minckler TM, Shires DB, deJongh DS. Postmor-tem bacteriology: II Selection of cases for culture. Am J ClinPathol 1971;55:17-23.
26 Koneman EW, Davis MA. Postmortem bacteriology. III Clinicalsignificance of microorganisms recovered at autopsy. Am JClin Pathol 1974;61:28-40.
Requests for reprints to: Dr Paavo P-aakko, Department ofPathology, University of Oulu, Kajaanintie 52 D, SF-90220 Oulu 22, Finland.
copyright. on 16 June 2019 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.37.11.1282 on 1 Novem
ber 1984. Dow
nloaded from