Embed Size (px)
Citation preview

Postpartum Maternal HealthThe Fourth Trimester & Beyond
Lauren H. Theilen, MD, MSCIFebruary 13th, 2019
No financial disclosures
Objectives! Understand why many are calling for changes to our
traditional model of postpartum medical care
! Review suggestions for shifting the postpartum care paradigm
! Review the literature supporting an association between pregnancy complications and adverse long-term health outcomes
! Present current recommendations for long-term care of women who have had pregnancy complications
Postpartum
! Literal definition! “Following childbirth”
! Clinical definition! The period of time in a woman’s life beginning at childbirth and
continuing for 6-12 weeks thereafter
Our traditional postpartum care model
! 1-4 days of inpatient care following delivery! Clinic visit at 6 weeks postpartum! B’s: baby, breast/bottle, bottom, blues, bedroom, birth control! Handoff to primary care provider?
! +/- incision check at 2 weeks post-op

The modern postpartum woman

Why change?
! Address postpartum needs among our contemporary population of new mothers! Improve immediate maternal and newborn health! Improve longitudinal maternal and child health

“To optimize the health of women and infants, postpartum care should become an ongoing process, rather than a
single encounter, with services and support tailored to each woman’s individual needs.”
Optimizing postpartum care
! Provide anticipatory guidance during pregnancy! Transition from pregnancy to parenthood ! Transition from prenatal care to well-woman preventive care! Family planning and contraceptive choices
ACOG Committee Opinion #736, May 2018.
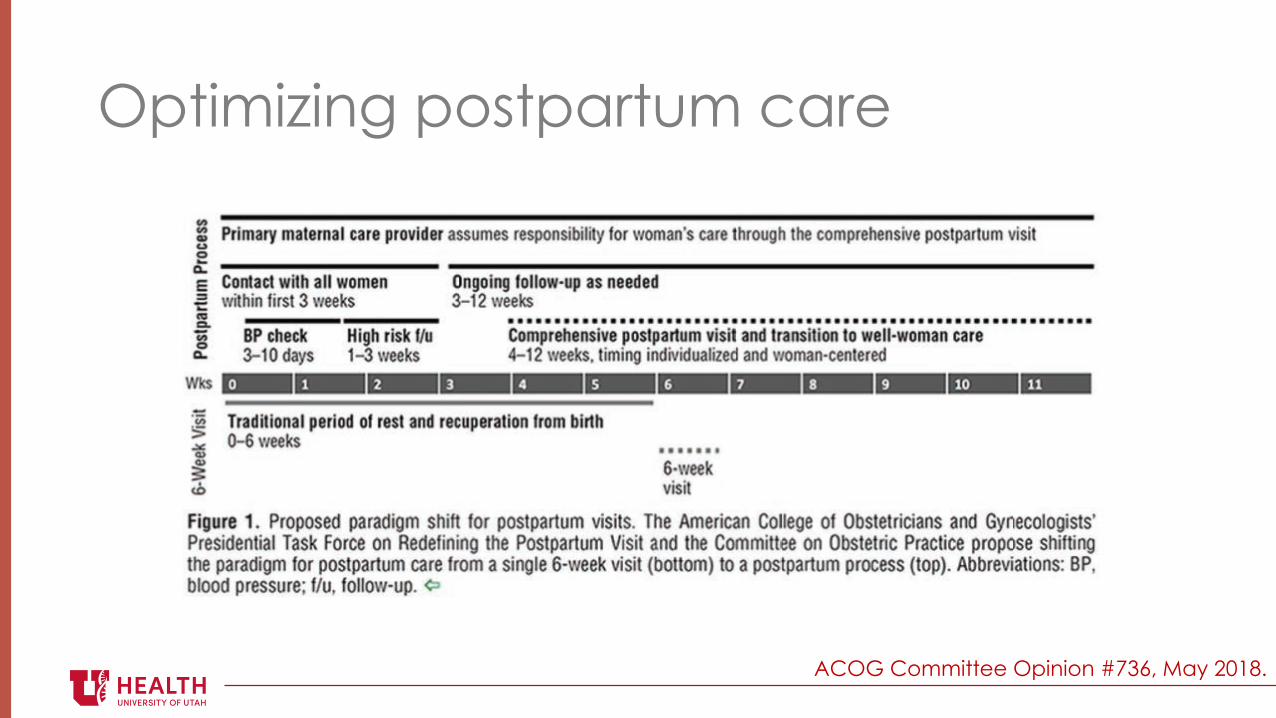
Optimizing postpartum care
ACOG Committee Opinion #736, May 2018.
Postpartum considerations for special populations
! Certain pregnancy complications! Make a plan for management of increased cardiometabolic risk
! Chronic medical conditions! Make a plan for ongoing management (who and when?)
ACOG Committee Opinion #736, May 2018.

Postpartum considerations for special populations
! Miscarriage, stillbirth, or neonatal death! Emotional support! Bereavement counseling! Referral to counselors and support groups as needed! Review of lab/pathology studies related to loss! Counseling regarding recurrence risk! Future pregnancy planning
ACOG Committee Opinion #736, May 2018.
Increasing engagement
! Discuss importance and role of postpartum care during prenatal visits! Use peer counselors, intrapartum support staff, postpartum
nurses, and discharge planners to encourage follow-up! Schedule postpartum visits during prenatal care or before
hospital discharge! Use technology to send automated reminders! Policy change to increase access to paid leave
ACOG Committee Opinion #736, May 2018.

Reimbursement for fourth trimester care
! Policy change to support postpartum care as an ongoing process rather than a single clinic encounter! Coding guidelines! Problem visits can be coded during the postpartum period! Use appropriate CPT E/M code appended with modifier 24! Link to ICD-10-CM code providing medical necessity for service
! Transition to well-woman care! Can schedule well-woman visit at 3 months postpartum (at least one
calendar year from the last annual well-woman service performed/billed)
https://www.acog.org/About-ACOG/ACOG-Departments/Coding/Coding-for-Postpartum-Services-The-4th-Trimester
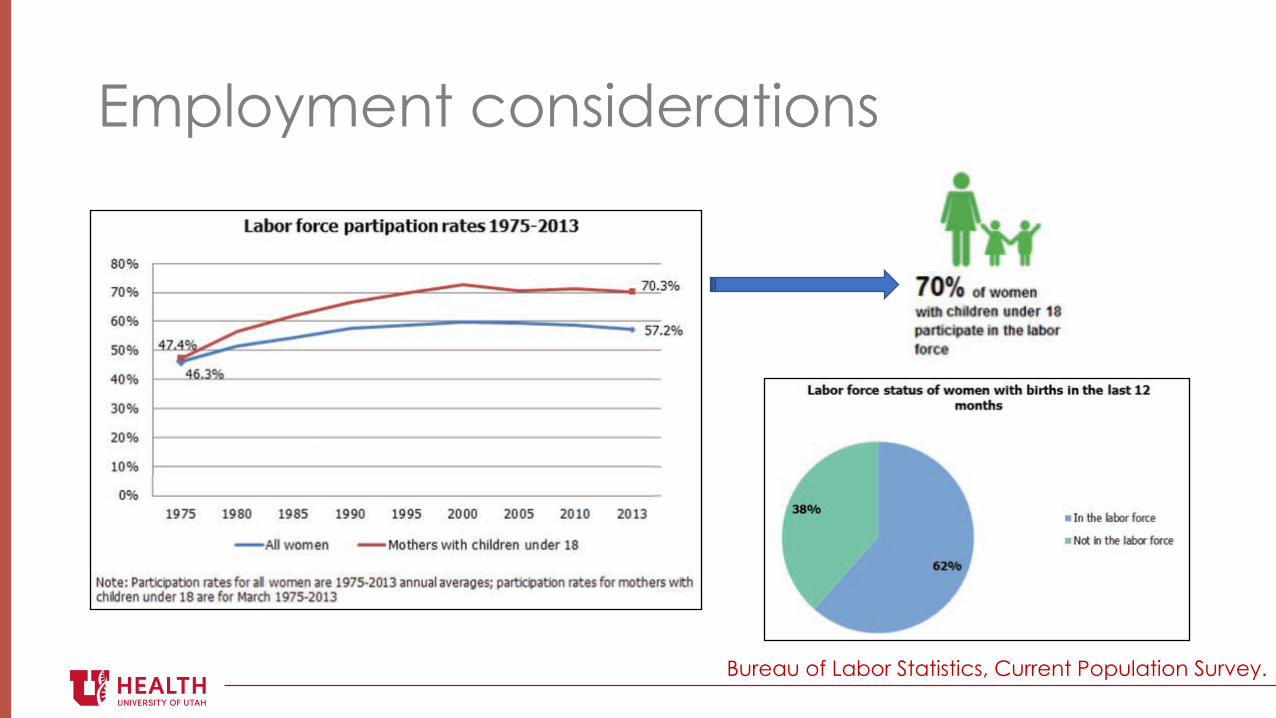
Employment considerations
Bureau of Labor Statistics, Current Population Survey.
Returning to work
The U.S. is the only developed country lacking a national paid maternity or
parental leave program

How can prenatal care providers help?
ACOG Committee Opinion #733, April 2018.
How can prenatal care providers help?
! Help pregnant women continue to work when it is safe for them to do so! Know how to request work accommodations! Bedrest! Number/frequency of prenatal visits! Only perform antenatal testing when indicated
Pregnancy as a window to future health
! Certain pregnancy complications are associated with cardiometabolic disease later in life! Identifying women at risk for early-onset cardiometabolic
disease may allow for timely preventive care to reduce long-term adverse outcomes among mothers
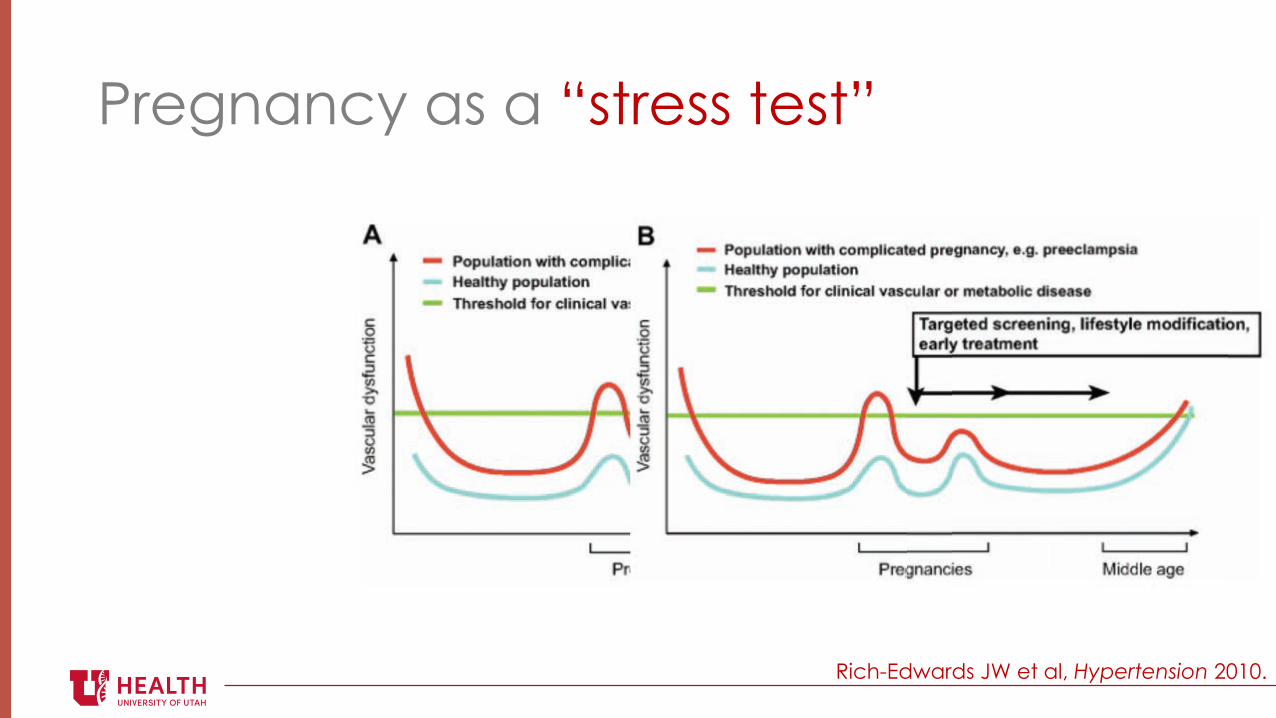
Pregnancy as a “stress test”
Rich-Edwards JW et al, Hypertension 2010.
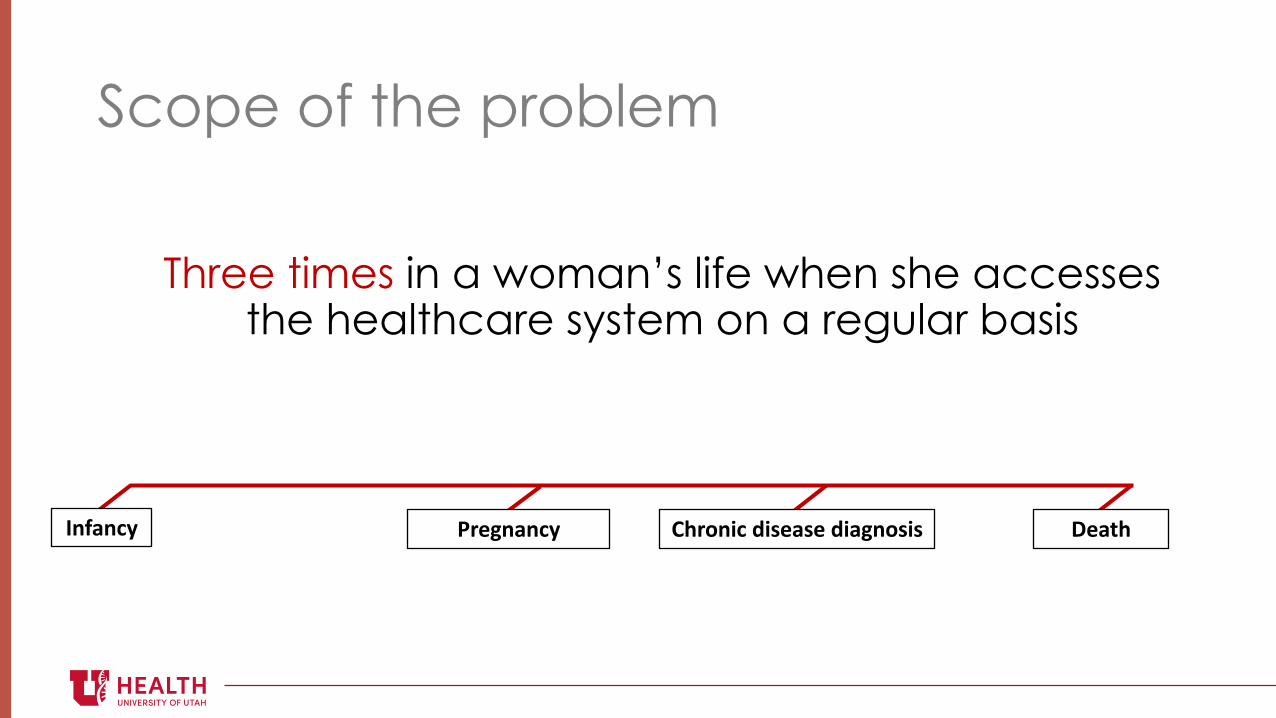
Scope of the problem
Three times in a woman’s life when she accesses the healthcare system on a regular basis
!"#$"%& '()*"$"%& +,(-".%/0.1)$1)/0.$*"-1.1 2)$3,
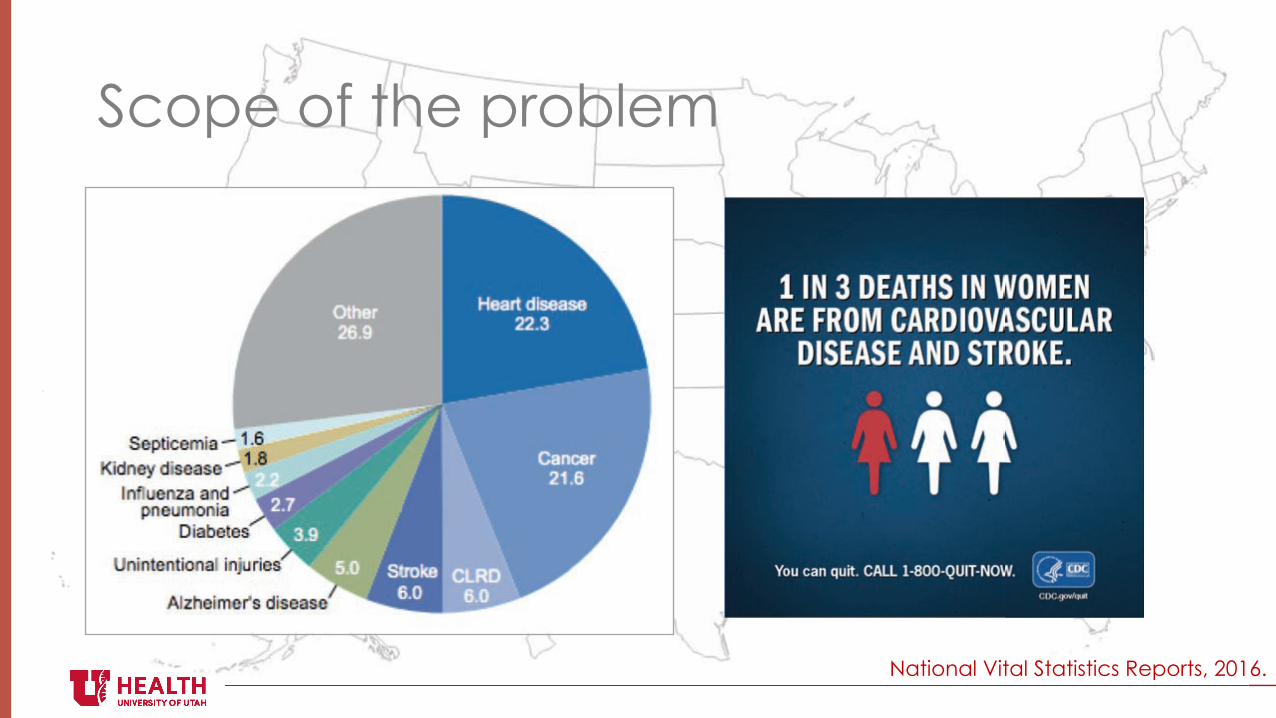
Scope of the problem
National Vital Statistics Reports, 2016.
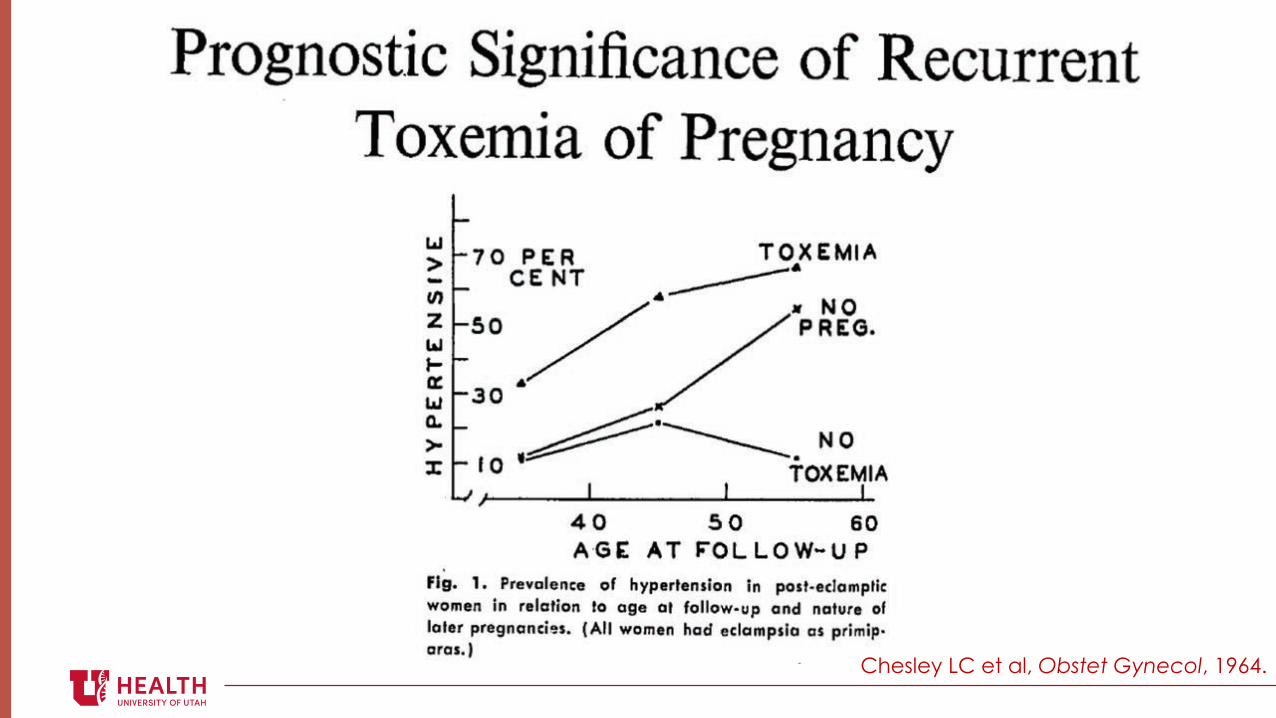
Chesley LC et al, Obstet Gynecol, 1964.
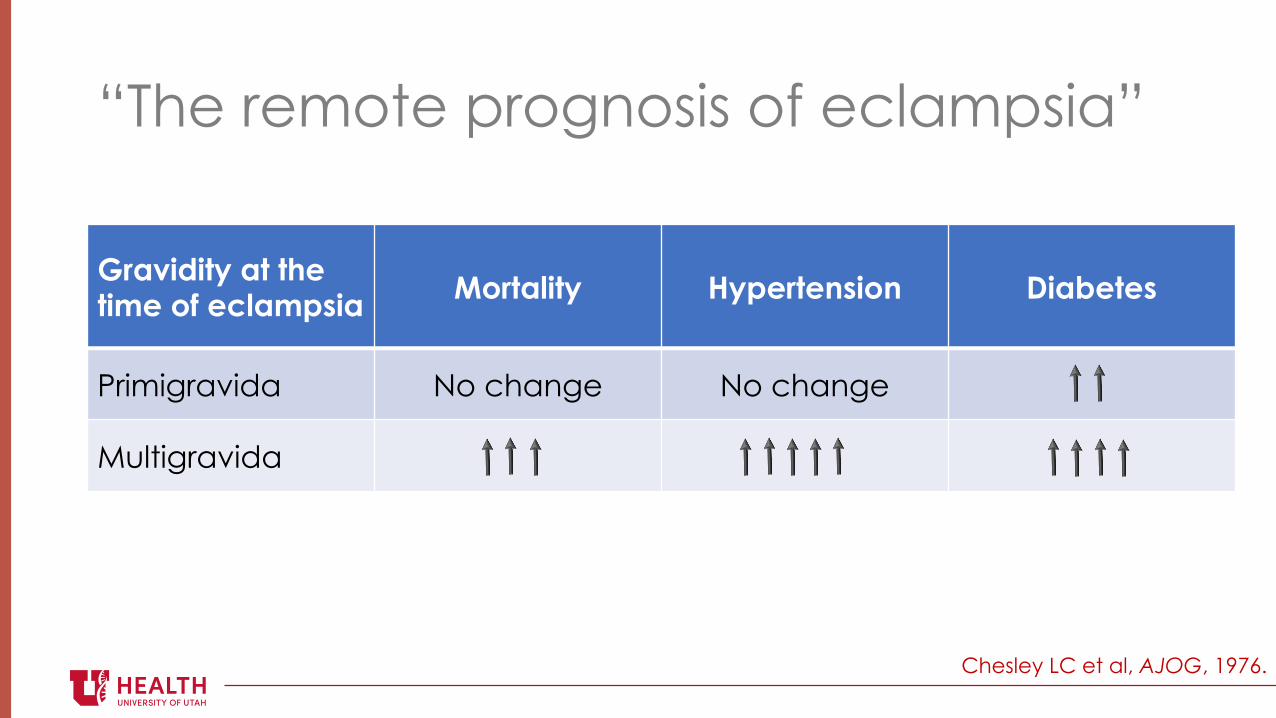
“The remote prognosis of eclampsia”
Chesley LC et al, AJOG, 1976.
Gravidity at the time of eclampsia Mortality Hypertension Diabetes
Primigravida No change No change
Multigravida
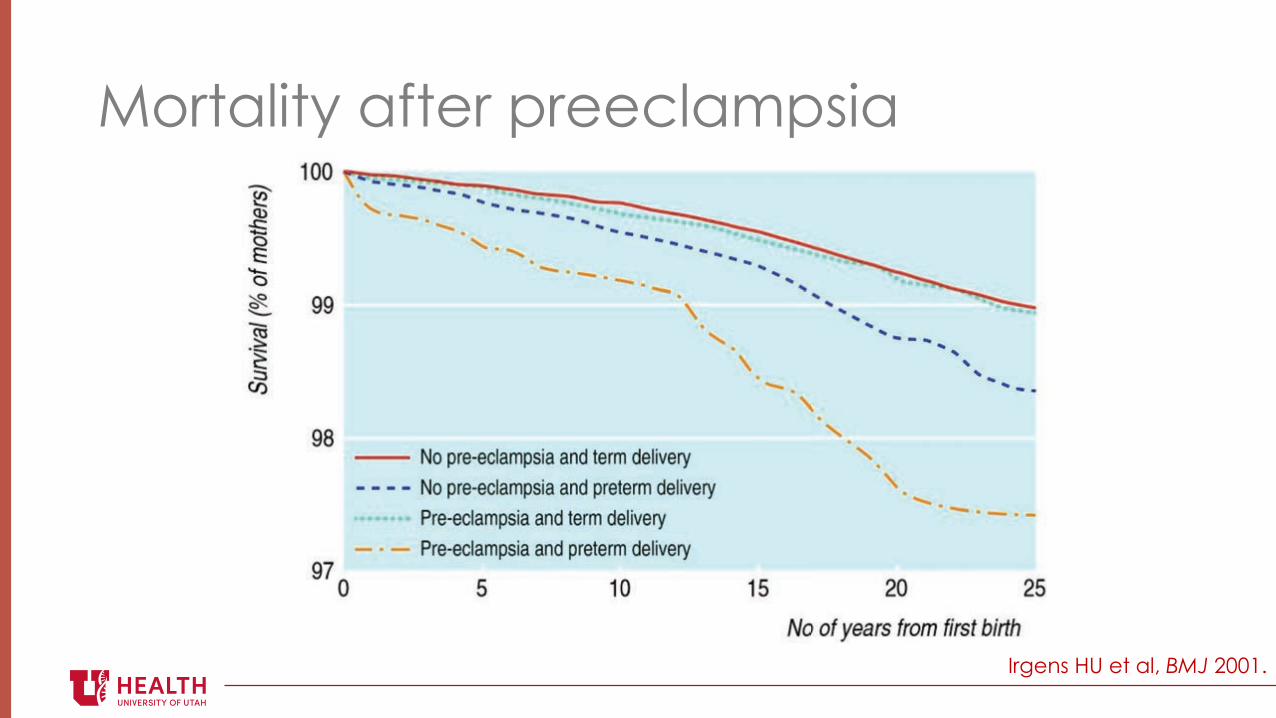
Mortality after preeclampsia
Irgens HU et al, BMJ 2001.
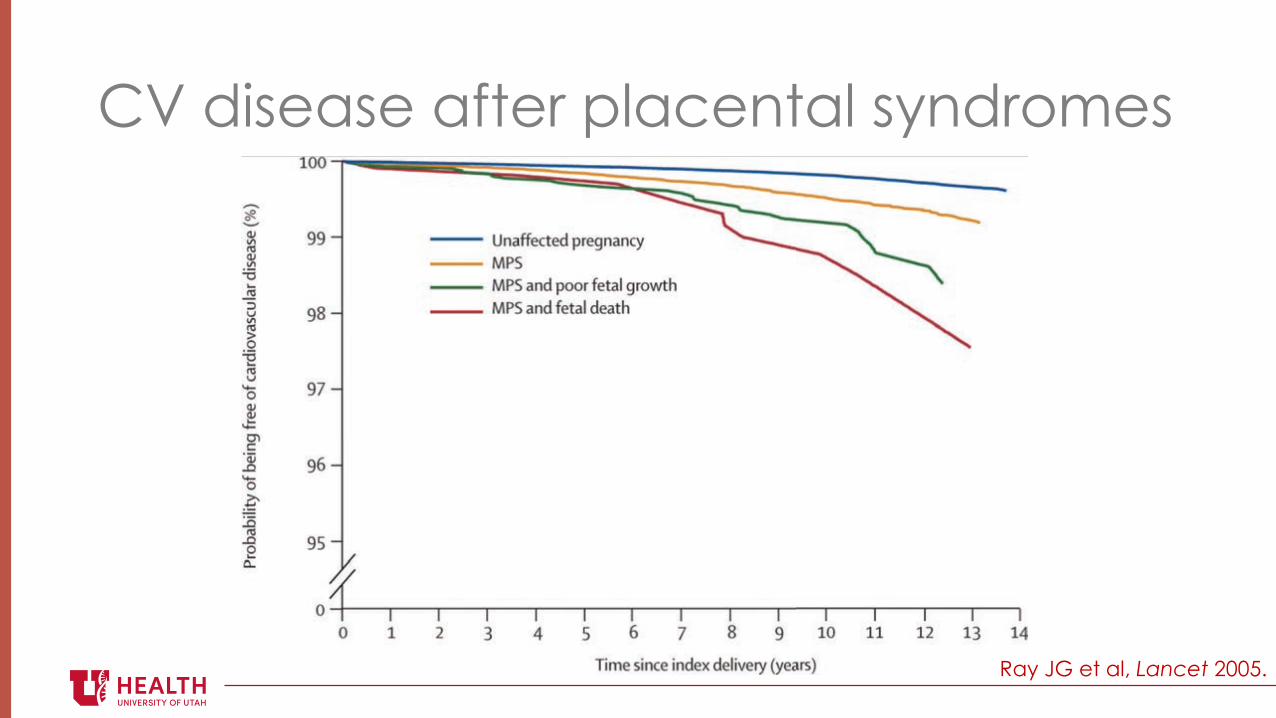
CV disease after placental syndromes
Ray JG et al, Lancet 2005.
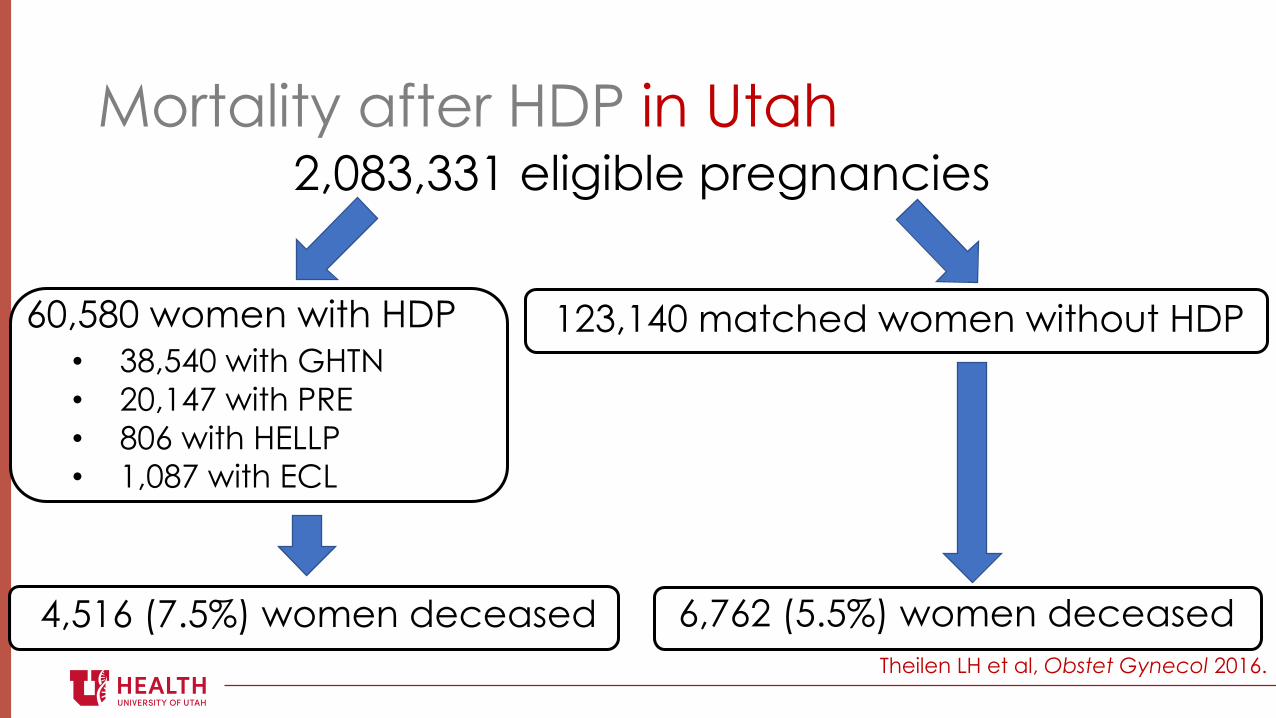
Mortality after HDP in Utah2,083,331 eligible pregnancies
60,580 women with HDP! 38,540 with GHTN! 20,147 with PRE! 806 with HELLP! 1,087 with ECL
123,140 matched women without HDP
6,762 (5.5%) women deceased4,516 (7.5%) women deceasedTheilen LH et al, Obstet Gynecol 2016.
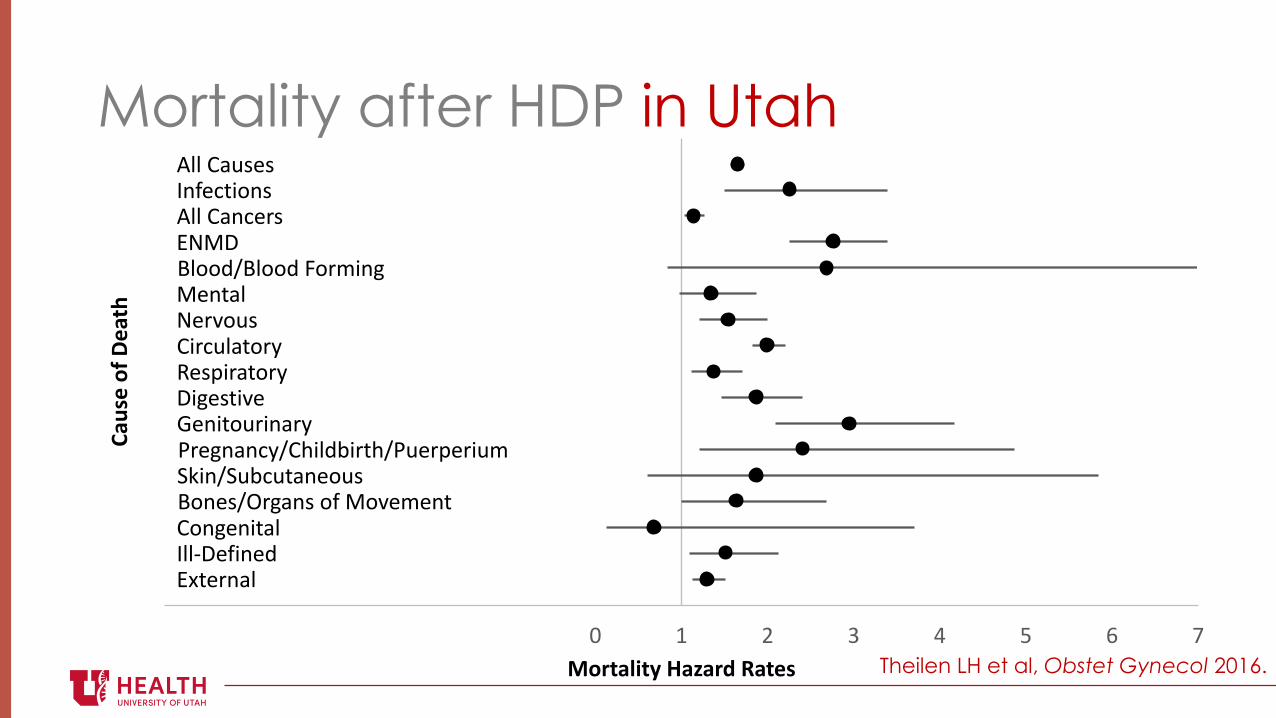
Mortality after HDP in Utah
Theilen LH et al, Obstet Gynecol 2016.
!""#$%&'(')*+(,-./*'!""#$%*,(0'12345"//675"//6#8/09.*:3(*-%"2(0;/&'$.0,&"%-/0<=('>.0%-/0<4.:('-.;(?(*.-/&0.*%0<@0(:*%*,<7$A."6B.0-A7@&(0>(0.&9CD.*7C&B,&-%*(/&'5/*('7E0:%*'#/+#3/;(9(*-$/*:(*.-%")""F4(+.*(61G-(0*%"
FH FI FJ FK FL M L K J I H N O
!"#$%&'(&)%"*+
,'-*"./*0&1"2"-3&4"*%$
Mortality after HDP in Utah!""#$%&'('
)*+,!"#$%&%'
*(-./&'#01'2(3
$4-5&"%2/-1#01'2(3()!
*&+,-%
./01%"2%+3'4!"'%#'%
56 57 58 59 : 9 8 7 6 ; < =
$%&'('#/6#,
(%27
+/-2%"421#8%9%-:#;%2('
>%'&#&",?#/4)@A%+&%?'",?
B+%%C/#2A'"#
DC/#2A'"#
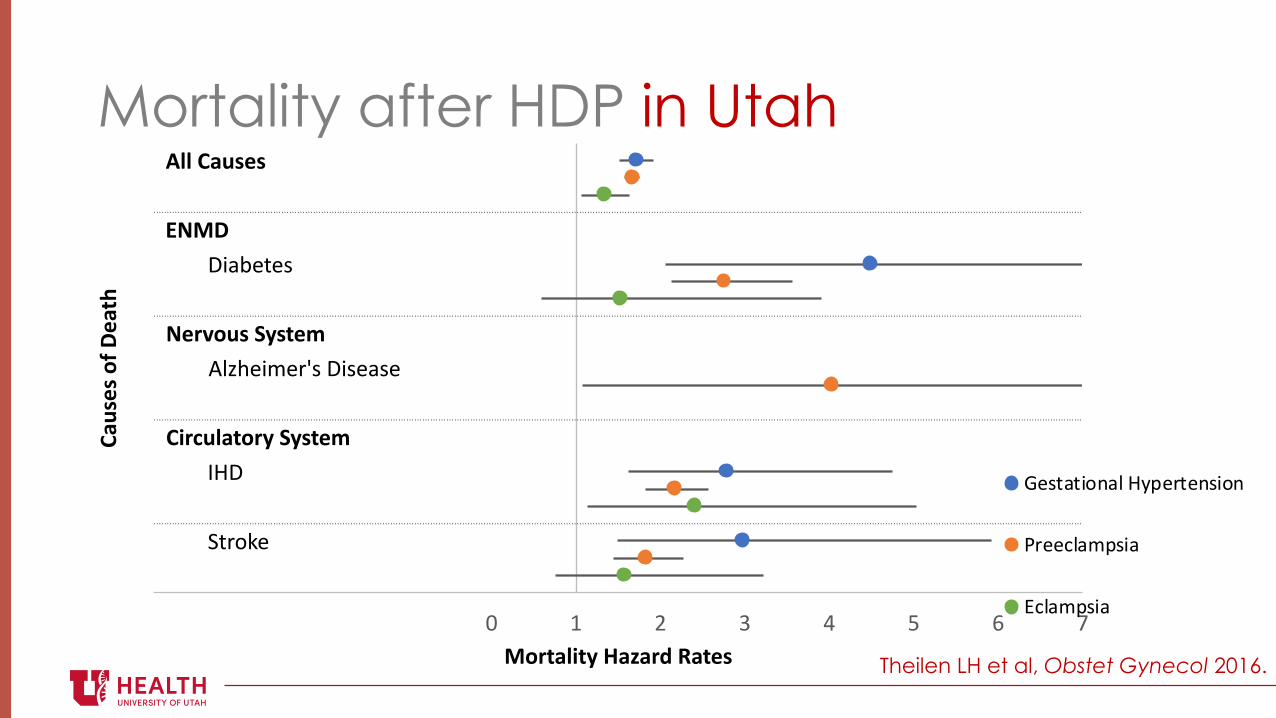
Theilen LH et al, Obstet Gynecol 2016.
Mortality after HDP in Utah
!
!"#
!"$
!"%
!"&
'
! #! $! %! &!
!"#$%$&'()#*+&
+%'%,-
./�(!%12/(314/5(67%'4(8%#,7
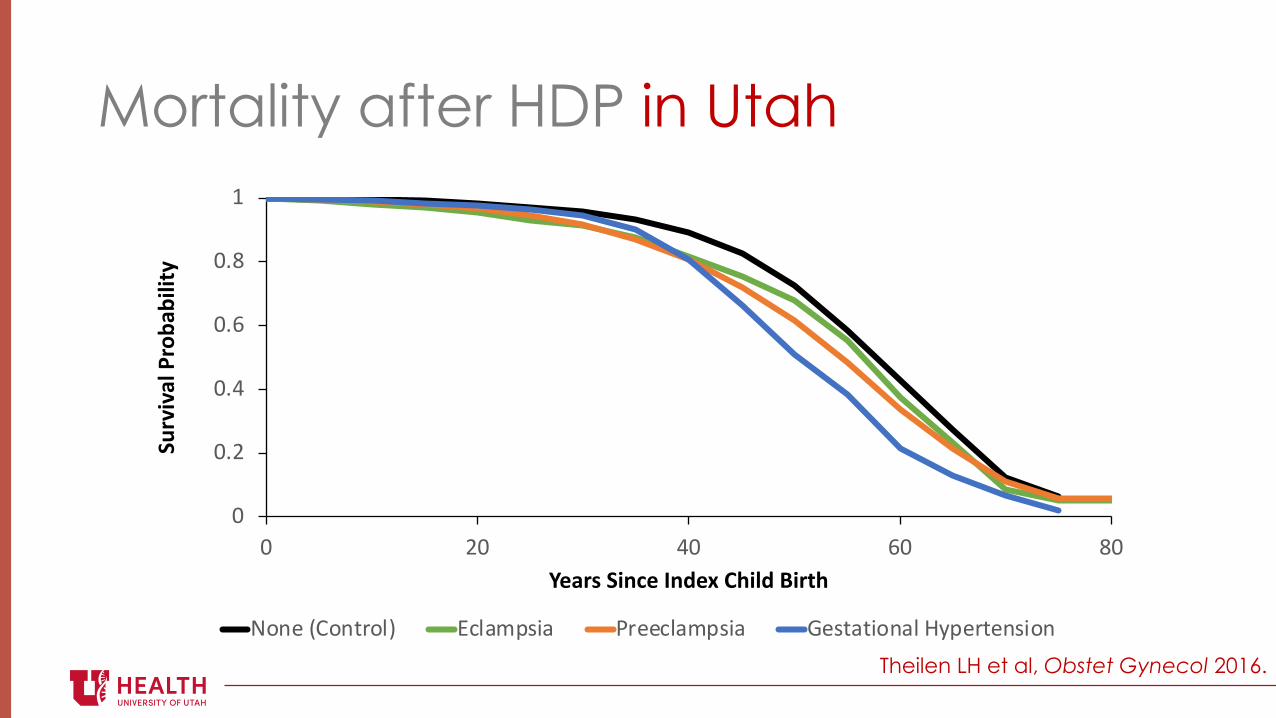
()*+,-.)*/0)12 341567895 :0++41567895 ;+8/5/9)*51,<=7+0/+*89)*Theilen LH et al, Obstet Gynecol 2016.
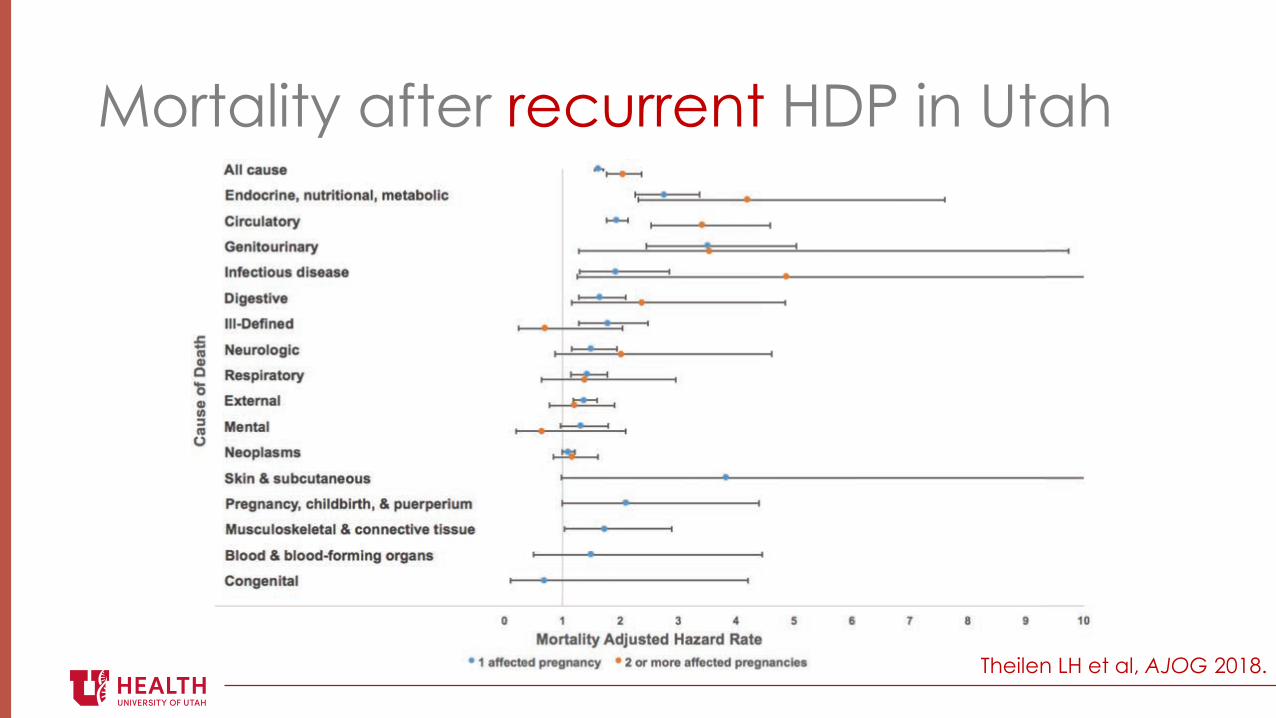
Mortality after recurrent HDP in Utah
Theilen LH et al, AJOG 2018.
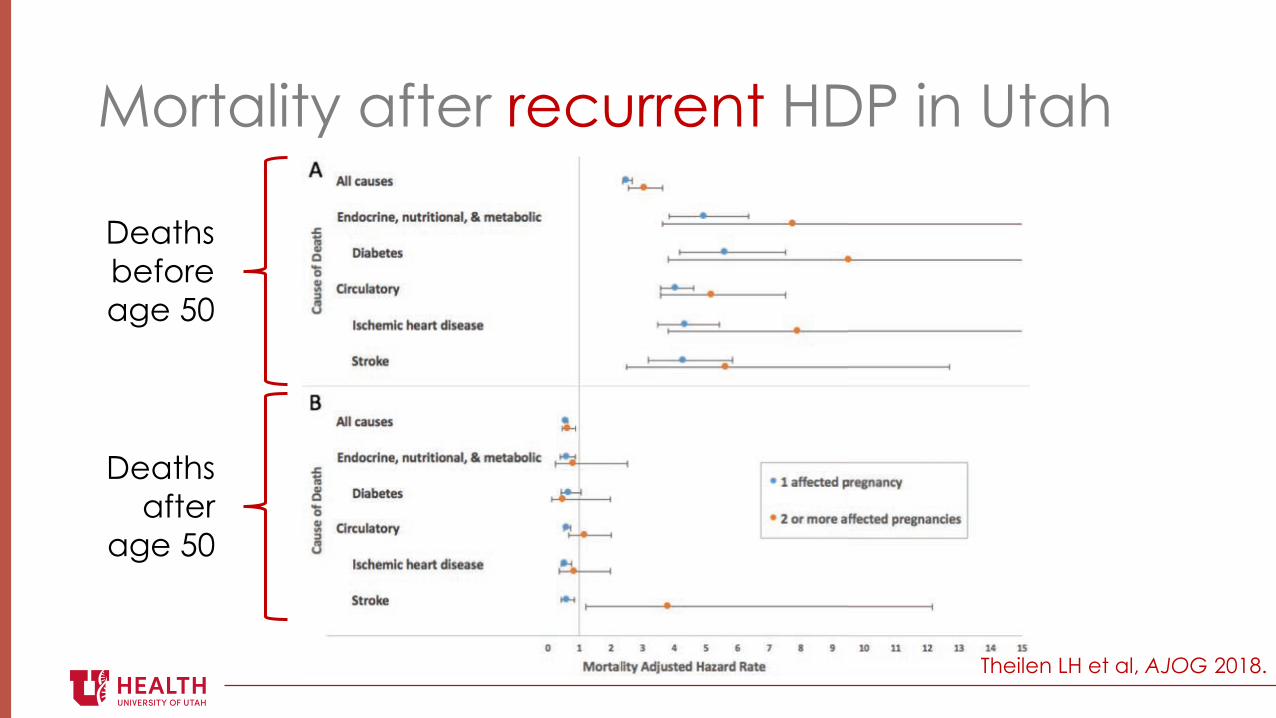
Mortality after recurrent HDP in Utah
Theilen LH et al, AJOG 2018.
Deaths before age 50
Deaths after
age 50
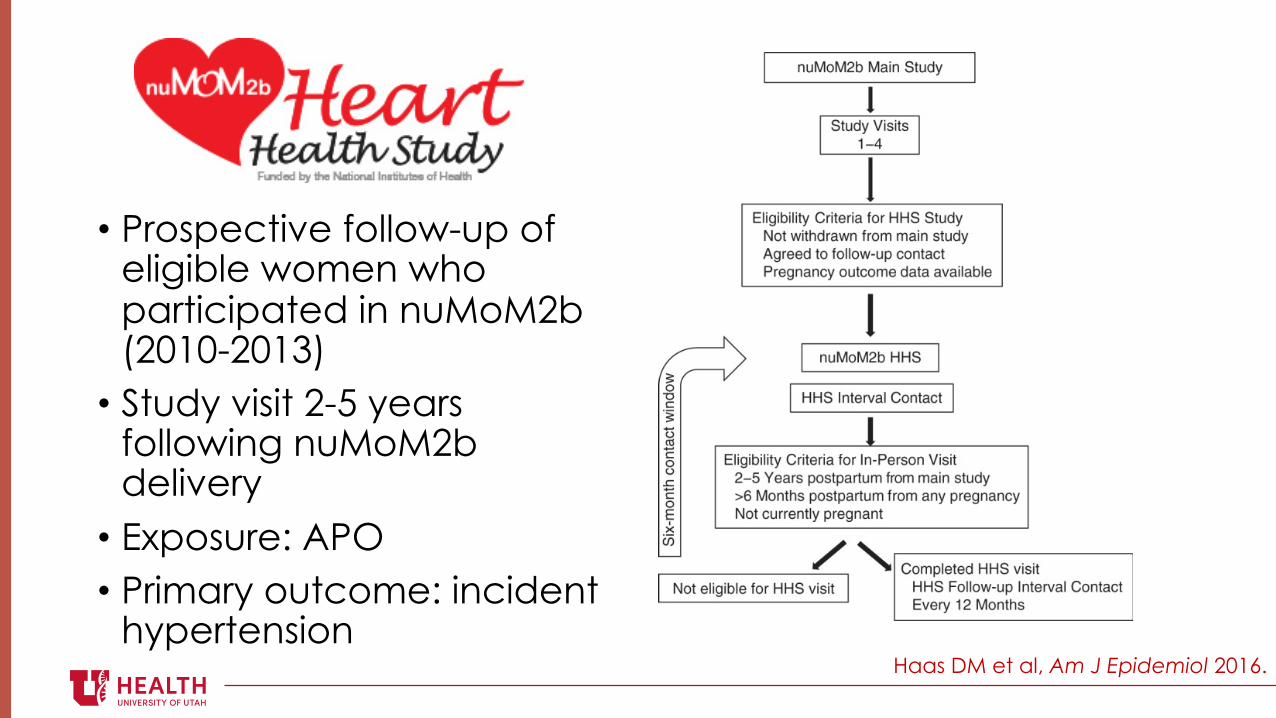
! Prospective follow-up of eligible women who participated in nuMoM2b (2010-2013)! Study visit 2-5 years
following nuMoM2b delivery! Exposure: APO! Primary outcome: incident
hypertensionHaas DM et al, Am J Epidemiol 2016.

Which women are at risk?
! HDP (any category)! Higher risk if preterm! Higher risk if recurrent
! Preterm birth! Growth restriction! Placental abruption! Gestational diabetes
What is the burden?
! Prevalence of cardiovascular death among U.S. women! Prevalence of risk factors! HDP alone complicates 3-5% of pregnancies in the U.S. (200,000
pregnancies per year!)! No data regarding value of early screening
Guidelines for clinical care
!ADA: Diabetes screening recommendations for women with a history of GDM! 4-12 weeks postpartum with a 75-g OGTT! Every 1-3 years thereafter with any of the
recommended screening tests (A1c, fasting plasma glucose, or 75-g OGTT)
ADA, Diabetes Care 2018.
Acknowledged preeclampsia, gestational diabetes, and pregnancy-induced hypertension
as major risk factors for CV disease, but didn’t make recommendations for how or when to
screen these women
Guidelines for clinical care
AHA, Circulation 2011.
Guidelines for clinical care
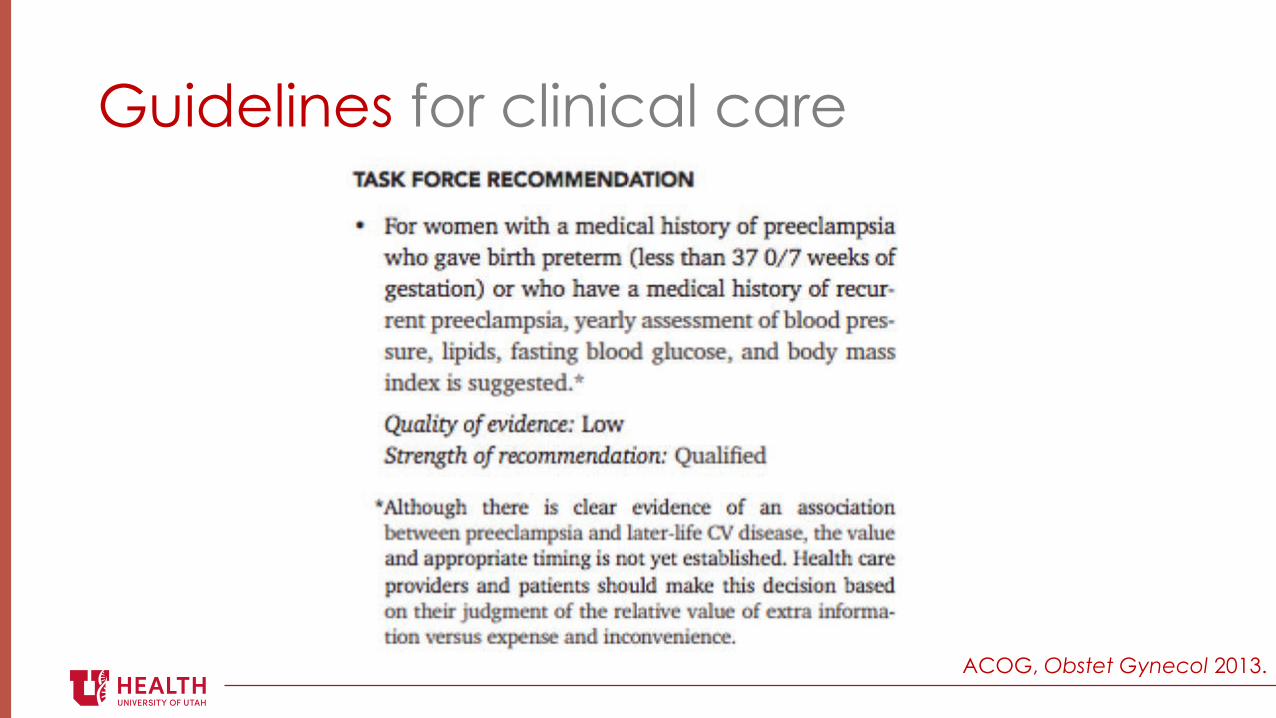
ACOG, Obstet Gynecol 2013.
Guidelines for clinical care
ACOG, Obstet Gynecol 2013.
Guidelines for clinical care
ACOG, Obstet Gynecol 2013.
Guidelines for clinical care
! Preeclampsia associated with 2 to 5-fold increase in odds for:! HTN! MI! CHF! CVA! PAD! CV mortality
! Highest risk! Severity of preeclampsia! Recurrence of preeclampsia! Preeclampsia requiring preterm delivery
Guidelines for clinical care
ACOG Practice Bulletin #202, January 2019.

“Preventive strategies to be considered by patients and health care providers may warrant closer long-term follow-up and lifestyle modifications to better manage risk factors for cardiovascular disease (eg, achieving healthful weight, exercise, diet, smoking
cessation), for which women and their primary care providers may maintain ongoing care and vigilance.”
Guidelines for clinical care
ACOG Practice Bulletin #202, January 2019.

Calls to action
D’Alton M and Tolani S, Obstet Gynecol 2018.
Calls to action
Brown HL et al, Circulation 2018.

Bridging the gaps
Three times in a woman’s life when she accesses the healthcare system on a regular basis
!"#$"%& '()*"$"%& +,(-".%/0.1)$1)/0.$*"-1.1 2)$3,
Summary
! It’s time to restructure the way we care for women after childbirth
! Although support via policy change is needed, we can shift the postpartum care paradigm in our practices now
! Abundant data support an association between certain pregnancy complications and adverse long-term maternal health outcomes
! Expanding postpartum care to include more than a single clinic visit and thoughtful transitions to long-term primary/preventive care may improve long-term health outcomes among mothers

Questions?





























