Embed Size (px)
Citation preview

REHABILITATION IN PRACTICE
‘Posture for Learning’: meeting the postural care needs of children withphysical disabilities in mainstream primary schools in England –a research into practice exploratory study
EVE HUTTON1 & KIRSTIE COXON2
1Department of Allied Health Professions, Canterbury Christ Church University, Canterbury CT1 1QU, UK and 2Department
of Public Health & Primary Care Research, King’s College, Capital House, London, UK
Accepted November 2010
AbstractPurpose. To explore teachers and teaching assistants’ (TAs) views of how to manage the postural care needs of children withphysical disabilities (PD) in mainstream primary schools, with the aim of developing strategies to support teachers andassistants in this role.Method. Qualitative data were gathered from a purposive sample of four primary schools in one county in the UK.Individual and focus group interviews with 36 teachers and TAs were carried out and used to generate an explanatoryframework around their experiences of managing the postural care needs of children with PD.Findings. Teachers and TAs in schools were found to have limited understanding of postural management. Very few hadpersonal experience of the benefits of postural care – instead, most appeared to think in terms of ‘doing’ rather than‘knowing’ about postural care. When implementing therapy programmes, teaching staff followed therapists’ instructionscarefully, but did not understand the purpose of their actions. Participants described the emotional impact of caring for achild with PD and expressed anxieties about causing discomfort when using equipment such as specialist seating andstanding frames. Equipment was viewed as bulky, uncomfortable and restrictive and not suited to the school environment.When asked which kinds of support would be valuable, participants identified practical solutions such as additional space orresources. Based on these findings, therapists, specialist teachers and parents developed an ‘A–Z of postural care’. Thisinformation resource aimed to address the gaps in knowledge and understanding highlighted by teachers and TAs in theinterviews and to acknowledge their anxieties when teaching and caring for children with PD. Stakeholder involvement in allaspects of the project from setting the research question to the development of the A–Z resource has assisted in thedissemination of the resource and its integration into the mainstream school system within the county.
Keywords: Posture, children, physical disabilities, schools
Introduction
It is widely acknowledged that children with complex
physical disabilities (PD) are at risk of long-term
health problems including in some cases severe
spinal deformities that can compromise their func-
tion in adult life [1]. Early preventive measures
including the active management of posture, using a
24 h approach, at home and school are believed to
limit long-term problems such as scoliosis and hip
migration, and may prevent the need for more
invasive measures at a later stage [2–4]. While there
is continuing debate about these issues [5], the
benefits of postural management in promoting the
functional and communication abilities of children
through positioning are recognised by therapists.
Children who are well supported are better able to
communicate and interact with others; there may be
improvements in their ability to carry out cognitive
tasks and the execution of fine motor tasks that
require good trunk stability [6–8]. Conversely, failing
to provide adequate postural support for children at
school may have negative consequences on a child’s
school performance.
A consensus statement [9] defined postural
management as: ‘A planned approach encompassing
all activities and interventions which impact on an
individual’s posture and function. Programmes are
Correspondence: Dr. Eve Hutton, Department of Allied Health Professions, Canterbury Christ Church University, North Holmes Road, Canterbury CT1
1QU, UK. E-mail: [email protected]
Disability and Rehabilitation, 2011; 33(19–20): 1912–1924
ISSN 0963-8288 print/ISSN 1464-5165 online ª 2011 Informa UK, Ltd.
DOI: 10.3109/09638288.2010.544837
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/28/
14Fo
r pe
rson
al u
se o
nly.

tailored specifically for each child and may include
special seating, night-time support, standing sup-
ports, active exercise, orthotics, surgical interven-
tions, and individual therapy sessions’.
Occupational therapists and physiotherapists are
involved in prescribing equipment, designing therapy
programmes and supporting families and the school
team in maintaining the programmes. Both Education
and National Health Service personnel need to work
in close collaboration if they are to meet the complex
needs of these children [10]. A series of studies carried
out by the Social Policy Research Unit based at the
University of York identified gaps in NHS services to
children in mainstream schools in the North East of
England and suggested that communication with
teachers, necessary for understanding the child’s
health needs, requires improvement [11,12].
Delivering a consistent and integrated 24 h pro-
gramme necessitates every environment in which the
child spends time being ‘enabled’ to provide postural
management [13]. Part of this process depends on
the provision of equipment but equally important is
skill and understanding of those responsible for using
equipment and delivering the therapy programmes
on a day-to-day basis. Teaching assistants (TAs) in
UK schools currently assume the greatest responsi-
bility for this work, although they have no specialist
health knowledge and must deliver programmes
within the busy school environment where other
priorities dominate [14–16].
Educational inclusion policy in England has
resulted in more children with PD being educated
in the mainstream school of the families’ choice
[17,18]. This is a welcomed trend but one that
presents challenges for schools unfamiliar with meet-
ing the needs of children with disabilities [19,20]. To
date, there has been little research which has
explored how to achieve good outcomes of postural
management, and a specific aim of this study was to
understand teachers’ and TAs’ views and experiences
of what happens currently within mainstream schools
in order to devise strategies to support them in this
important role. In this article, we first describe the
study we undertook to address this aim (part 1), and
then we outline the development of the ‘A–Z of
postural care’, an information resource which arose
in response to the study findings (part 2).
Part 1: Posture for learning – a research into
practice exploratory study
Methodology: engaging parents and other key
stakeholders
This study arose from concerns expressed by local
therapists working within mainstream primary
schools, who felt that teachers and TAs were finding
it difficult to follow therapy programmes and
integrate postural care into the school routine. This
was the case even where the school had additional
resources for children with PD, meaning that it was a
school where there was a level of experience amongst
the staff team and specialist support. Postural care
programmes seemed at risk of becoming ineffective,
but the problems this might cause for the child may
not be quickly apparent, and could be very difficult
to reverse. The PI (EH) instigated an informal
meeting with parents of children with PD, where
parents were invited to share their experiences and
contribute to the development of a research proposal.
This meeting was seminal in forming the research
study described here. The views of parents provided
further insight into the difficulties of maintaining
consistent ‘postural care’ across sites and settings.
Parents were enthusiastic about the idea of research,
but also vociferous in their belief that the study
should have practical benefit to families and schools,
and not just be of academic interest.
A research steering group was formed and two
parents came forward to work alongside the re-
searchers, practitioners and educationalists [21].
In addition to the parents, the committee included
local therapy leads and teachers from the specialist
teaching service, with academic input from two
universities. The lead researcher (EH), also a
paediatric occupational therapist, chaired the com-
mittee. The co-researcher (KC), an experienced
health services researcher, conducted some of the
interviews and focus groups, assisted with initial
thematic analysis and attended all analysis work-
shops. The committee met regularly throughout the
study and approximately monthly during the analysis
phase.
At the start of the study, the researchers consulted
‘Involve’ guidelines for public involvement and these
contributed to the format and conduct of the steering
committee [22]. Meetings were informal, to encou-
rage a collaborative rather than a ‘business meeting’
atmosphere. ‘Involve’ recommend ‘equal representa-
tion’ of public and researchers, and this was achieved
in the sense that there were two parents and two
researchers, although the full committee was of
course broader than this. However, we were careful
to ‘foreground’ the views and comments of parents,
and encouraged them to give their responses and
experiences throughout the discussions.
Finally, again in line with the ‘Involve’ guidance,
we discussed payment with the parents. At that stage,
we were not in a position to reimburse them for their
time, but they were willing to attend on a voluntary
basis, on the understanding that their involvement
would help improve services for other children and
families. Their altruism had a positive effect on the
Posture for learning 1913
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/28/
14Fo
r pe
rson
al u
se o
nly.

research, and we often reflected that this kept us
focused on continuing and completing the study,
and on finding a way to implement the findings into
practice.
The next stage was to consider what questions
should be addressed and the best way of doing this.
The issues raised by parents and therapists were not
so much about the best interventions to use as how to
provide the best care across multiple sites and
settings, and include families, children and school
staff in ‘seamless’ care. We set out to understand
better the knowledge and understanding of school
staff, and to determine what barriers and facilitators
exist in the school environments in relation to
delivering postural management programmes in
mainstream primary schools, and how these might
be addressed to maximise the child’s potential for
educational progress [21].
Study design
The exploratory nature of the study suggested that a
qualitative research design was most consistent with
the overall research aims [23]. We elected to conduct
interviews and focus groups within four schools, and
to conduct the analysis with the support of the
steering group.
The study design was informed by the principles of
public involvement as outlined by the UK Department
of Health, National Institute for Health Research [22].
Because the PI was already accustomed to working
closely with children and families, it was a natural
extension to include families in the research ideas
under discussion. We also felt it was essential to
collaborate with colleagues in allied health professions
and with representatives of the educational department
who were responsible for supporting schools to include
pupils with PD. These individuals became core
members of the steering committee and contributed
to the analysis. We suggest that this represents an
additional form of stakeholder involvement, in the
sense that the adoption of recommendations into
practice relied on the ownership of the study to be
authentically felt across the range of professions
involved. The policy orientation of the study meant
that the ‘framework’ approach described by Ritchie
and Spencer [24], was appropriate, and the stages of
framework analysis described by these authors formed
the basis of the analytic work we undertook with the
steering committee.
Based on the consultation described above, we
formulated the following research questions:
1. What knowledge and understanding do tea-
chers and TAs have of postural management
for children with PD?
2. What barriers and facilitators exist when using
postural management programmes in the
mainstream primary school environment?
3. What types of information and support would
teachers and TAs value when using postural
management programmes with children with
PD in mainstream primary schools?
Ethical approval
The study was submitted for ethical approval to the
host university’s Research Ethics Committee and to
the Local Education Authority’s Research Govern-
ance Committee, and both panels granted approval
in November 2007. The study was funded by a small
grant from the Posture and Mobility Group (a
registered charity) following a successful application
by the PI (EH). Empirical work was undertaken in
early 2008.
Sample
The sampling strategy for the study was designed to
include mainstream primary schools attended by
children with PD. We wanted to include a selection
of schools, as different settings might encounter a
range of challenges, or display individual strategies
for managing these. Whilst we recognised that there
are additional considerations in the transfer to
secondary education, we decided that given the
importance of the primary school years in develop-
mental terms, we would focus on the primary sector
for this project. The sample was also purposive,
because we wanted to select schools that were all
attended by children with PD, but also to include
different sized schools with various experiences and
levels of resource.
The lead occupational therapist, physiotherapist
and specialist teaching service advisors assisted in
identifying a sample of four primary schools (see
Table 1). One of the ‘designated’ schools was
purpose built with disabled facilities and access, the
other schools were housed in older buildings that had
been adapted and extended to accommodate dis-
abled facilities.
Invitation letters to head teachers providing
information about the proposed research study were
initially sent to five schools. One school declined as a
new head-teacher had only recently been appointed
and the school was undergoing a radical redesign
which left four school sites. The lead researcher
visited the four remaining schools to speak to the
Special Educational Needs Co-ordinator (SENCO).
At this meeting, dates and times for interviews and
focus groups with teachers and TAs were negotiated
1914 E. Hutton & K. Coxon
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/28/
14Fo
r pe
rson
al u
se o
nly.

to fit in with the school timetable, and information
sheets were provided to staff. Between 4 and 16
members of staff were interviewed per school, but
this disparity reflected the relative sizes of the
schools, rather than the willingness of staff to
participate. In School site 4, the two TAs were
interviewed separately (as opposed to taking part in a
small focus group together) because they worked at
different times during the school day and did not
overlap. Further details of sample and methods are
provided in Table 2.
Data gathering
Most participants included in the study took part in
focus groups, each of which was facilitated jointly by
EH and an academic colleague. By using both
individual interviews and focus groups, we aimed
to gain an understanding of individual experiences,
and also an insight into the kinds of attitudes or
processes that might be operating within the school
[23]. The focus groups were most similar to Coreil’s
description of a ‘natural group’ that already work
together [25], rather than a group brought together
from different settings for the purposes of research.
Instead of providing a diverse view, natural groups
are well placed to describe ‘how things are done
here’, which was appropriate to address our research
questions. In this context, it seemed reasonable to do
focus group interviews with small numbers, because
we were not seeking to establish consensus, but
rather to explore local understanding within that
particular school.
Individual interviews were conducted with SEN-
COs, some of whom were head teachers, because we
understood that it might be difficult for staff to talk
openly if their SENCO (often the head teacher) was
in the focus groups. However, we also recognised
that differences in power and status between TAs
and teachers could inhibit open discussion, and for
these reasons, ‘mixed’ groups were avoided, either
through conducting separate focus groups or indivi-
dual interviews. All interviews were tape recorded
and transcribed. Field notes were taken during focus
groups by the facilitator, and they recorded informa-
tion about the group dynamics and the observations
of the co-facilitator. During the interviews with head
teachers and SENCO’s, relevant background infor-
mation was gathered.
The interview schedule was developed with
assistance from the steering committee, and the
same schedule was used for both focus groups and
interviews. Participants were first asked to describe a
typical day in their work with children with a
disability, and to highlight examples of when they
felt that things went well and when things had gone
less well. We then asked what respondents under-
stood by the term ‘postural care’, where they looked
for information or support, whether they had
received any training in postural care and the use
of equipment, and if so who had provided this. We
invited them to share with us their feelings about
being responsible for the child’s postural care needs
at school and how much support, if any, they felt they
received. Finally, we asked how they would like to be
supported in the future and what they felt would
assist them most.
Data analysis
Detailed transcripts of interviews and focus groups
were analysed using the principles of framework
Table I. Features of primary schools included in study.
School Status*
No of children
on school roll
No of children with
postural care needs Types of disability
School 1 Designated 248 9 Cerebral palsy, hyper mobility, neuromuscular, neurodevelopmental
School 2 Mainstream 376 4 Cerebral palsy neuromuscular neurodevelopmental
School 3 Designated 500 3 Cerebral palsy, neuromuscular
School 4 Mainstream 221 2 Cerebral palsy, neurodevelopmental
*Designated¼additional provision for PD. Mainstream¼no additional resources at that school.
Table II. Breakdown of sample and methods used.
Site Teaching assistants Teachers SENCO* Number included at each site (n¼36)
School 1 9 (2 focus groups) 6 (1 focus group) 1 (Interview) 16
School 2 4 (2 focus groups) 3 (1 focus group) 1 (Interview) 8
School 3 5 (1 focus group) 2 (1 focus group) 1 (Interview) 8
School 4 2 (interviews) 1 (interview) 1 (interview) 4
*Special educational needs co-ordinator.
Posture for learning 1915
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/28/
14Fo
r pe
rson
al u
se o
nly.

analysis. This approach was developed to assist with
analysis of data in applied policy research by the
National Centre for Social Research. Ritchie and
Spencer [24], outline five key stages of framework
analysis (see Box 1.) Below, we describe how we
adapted this process to our study.
Stages 1 and 2: Familiarisation with data and
embarking on thematic analysis
The PI (EH) read all transcripts and listened to tapes
during the familiarisation stage, and started to
develop the initial thematic analysis based in part
on the a priori hypotheses, also identifying new and
unanticipated themes within the data. The co-
researcher (KC) read the transcripts independently
and we then discussed our impressions of the data
and to share ideas about emerging themes. We
compared interview transcripts between school sites
and across different groups. Together these formed
the basis of a thematic framework, a section of which
is included in Figure 1 to demonstrate how the a
priori themes were broadened and linked to new,
inductive themes arising from the data.
Stages 3 and 4: Development of themes using charting,
indexing and mapping
We then convened workshops where we presented the
data to the steering committee, and used flipcharts
during workshop discussions. Recording the iterative
development of themes through workshops meant that
the pathway from data to conclusions can be demon-
strated, and these written accounts have also proved
valuable in helping us write up the study. As Ritchie and
Spencer [24] suggest, the ‘stages’ of framework analysis
do not necessarily follow the ‘order’ suggested in Box 1,
and our experience was that indexing, charting and
mapping were all part of developing the thematic
framework, particularly for the ‘new’, inductive themes.
The process described here developed from our
attempts to work closely with the parents and
colleagues on the steering group. We would argue
that the process of framework analysis also supported
the interpretative rigour of the study, and here we use
Liamputtong and Ezzy’s [26, p.39] description of
rigour, meaning that our findings ‘accurately represent
the understandings . . . and worldview of the people
engaged in them’. We used direct quotations and
interrogated our assumptions about these, searching
for possible alternative explanations.
Findings
The findings are presented below. The data from
interviews and focus groups is presented in a way
that addresses the research questions, along with a
summary of the steering group responses. These
issues then informed the development of the ‘A–Z of
postural care’, described in part 2.
What knowledge and understanding did teachers and
TAs have of postural management?
When asked what they understood by the term postural
management it was apparent from the responses from
teachers and TAs that this is not a term widely used or
understood by teachers and TAs in schools.
‘‘I wouldn’t use this term, it’s how you sit, how you
walk – I never use it’’ (TA, designated school)
‘‘No I don’t use these – posture I mean it’s how one sits how
one carry’s one around’’ (Teacher, mainstream school)
‘‘We just say physical disability I don’t think I’ve ever
heard about it’’ (TA, designated school)
One TA said it was about ‘keeping children
comfortable’ (TA, designated school)
Box 1.
1. Familiarisation with the data
2. Identifying a thematic analysis
3. Indexing
4. Charting
5. Mapping and interpretation
Stages of Framework Analysis, Ritchie and
Spencer [24]
Figure 1. Section of thematic framework illustrating the link
between a priori and inductive themes.
1916 E. Hutton & K. Coxon
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/28/
14Fo
r pe
rson
al u
se o
nly.

Teachers and TA’s in their descriptive observation
of children demonstrate that they understand some
principles of good positioning. They knew what to
do, when implementing therapy programmes and
followed therapists’ instructions carefully, but did
not understand the purpose of their actions. They
appeared to lack a conceptual framework that would
assist them in reasoning about and making sense of
their observations of children’s posture and experi-
ences of managing children’s postural needs.
‘‘X won’t sit because he doesn’t feel stable, a normal
chair is too low, his feet are never flat on the floor’’
(Teacher, designated school)
‘‘The child has to be watched because he tends to fall over
in his chair and he can’t right himself, you often find him
slouched in his chair’’ (Teacher, mainstream school)
‘‘Over time his legs have turned inwards, I’ve noticed
that he stands on the side of his feet now . . . now he is
walking his legs have got worse’’ (TA, mainstream
school)
Information and advice about managing the
postural needs of the child are gathered by teachers
and TAs from various sources including: therapists,
parents, children, peers and written information
found in the child’s individual education plans.
Information about the child’s needs, including
postural management is shared during transition
into school or when a child changes class.
‘‘Most of it [information] comes from the physios ..they
will give us a programme of exercises of things we need
to do’’ (TA, designated school)
‘‘They [therapists] are the experts, they say what needs
to happen, we don’t make decisions because we are not
qualified to do this, we take their advice’’ (Teacher,
designated school)
‘‘I have talked with mum, I have a good relationship with
her and would ask any questions, I asked her about the
exercises and what she thought – should he do them or
not’’ (Teacher, mainstream school)
‘‘I just ask the child themselves, ‘are you comfortable?’
she can tell you how she feels, if she’s comfortable, and
she would!’’ (TA, designated school)
‘‘When the child starts school we have their files and
things and find out medical bits and bobs and there is a
hand over from the teachers’’ (Teacher, designated
school)
Teachers suggested that they would like more
information about physical disability, they felt that as
teachers they ‘should’ know this and were often
embarrassed to ask therapists or parents for more
information about a child’s condition. They felt that
initial teacher training did not prepare them for
working with disability. There appears to be little
training available for teachers or TAs focusing
specifically on the postural care needs of the child
in a mainstream school, but where training had been
offered teachers had valued this.
‘‘They don’t train you to look at SEN ..you are not even
clued up on what difficulties the children have – you
could do a whole degree on that’’ (Teacher, designated
school)
‘‘No amount of training would have helped – I actually
had to do it [handle the child] myself’’ (Teacher,
mainstream school)
Issues raised by the steering group. We shared these
comments with the steering committee and a
discussion developed about whether therapists’
use of health terminology (postural management)
was helpful, or whether this was too technical a
term and ‘professional jargon’ for teachers and
TAs. Parents had already suggested it was difficult
to separate out the postural needs of the child from
other health, education and the social aspects of
caring for a child. ‘Good’ posture, it was felt, was a
whole school issue, as relevant to children without
a disability as those with. A ‘whole school’
approach may provide a solution for helping
teachers to understand and address the particular
needs of children with a disability in an inclusive
way.
Greater understanding by teachers and TAs would
mean schools could be more flexible in how they
implemented programmes, rather than adhering to
rigid routines based on time spent in a particular type
of equipment. One group member suggested, how-
ever, that TAs were not there to question, adapt or
interpret programmes of therapy and felt concerned
that this may result in programmes being implemen-
ted incorrectly.
Teachers and TAs needed to appreciate that
postural management is about positioning a child
so they can engage in school activities, whereas the
data suggested that currently teachers and TAs
perceive positioning and postural management as a
subject distinct from the child’s learning. The group
agreed that training for schools was important and
should be made a high priority and discussed the
merits of generic training and bespoke training. One
member felt very strongly that parents should be able
to contribute to the training of the school team.
Another wondered how useful or appropriate any
Posture for learning 1917
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/28/
14Fo
r pe
rson
al u
se o
nly.
generic training could be, because each child was
individual.
What were the barriers and facilitators to the delivery of
effective postural management in mainstream schools?
Teachers and TAs described in their accounts
the emotional impact of caring for a child with
PD at school and expressed anxiety about
potentially hurting the child or ‘doing the wrong
thing’
‘‘I didn’t want to use the equipment improperly and
hurt him, I was afraid of letting him down’’ (Teacher,
mainstream school)
‘‘It’s not a nice experience for them, they have to do
things, to manipulate their bodies and stretches and stuff
like that, it’s not nice’’ (Teacher, designated school)
‘‘I don’t want to start doing something and do it wrong’’
(Teacher, designated school)
Respondents expressed largely negative attitudes
about equipment in their descriptive accounts, e.g.
describing it as ‘too bulky’, ‘separating the child from
others in the class’, ‘uncomfortable’ and ‘restrictive’.
‘‘It elevates the children and puts them at different
levels, and from year 5 they start to recognise that they
are different’’ (Teacher, designated school)
‘‘He always had a bigger chair than everyone else, but that
was a different scenario, now he’s standing up you can see
he is completely different to the other children and that is
singling him out’’ (TA, mainstream school)
‘‘X has a new stander and he can’t go into the stander in
the class so he’s having to be separated, some of the
things I am doing are actually taking away the whole
ethos of inclusion’’ (TA, mainstream school)
‘‘He’s just stood up and strapped into this contraption, it
reminds me a bit of the film Frankenstein, with the
monster strapped to the table and then they tilt it up’’
(TA, mainstream school)
‘‘I wish the classroom had a bit more room, there are
lots of trip hazards, there is not enough room, there is
always something that she could hit herself on’’ (TA,
designated school)
‘‘We’ve got children moving around and different
activities going on, we can’t always move the chair
around’’ (Teacher, mainstream school)
Children with postural needs had been ‘missing
out’ on break times and playtimes and some parts of
the curriculum. Therapy visits were described as
rushed or inconvenient and staff did not feel they had
time to ask questions or gain advice. Therapists often
met only with the TA and did not involve teachers in
their visits.
‘‘They do miss out on things, we try to miss out on PE
or Art’’ (TA, designated school)
‘‘I used to get very frustrated – he would just have got his
coat on and then they [therapists] would turn up and he
would hate this because he likes to go out at break time’’
(Teacher, mainstream school)
‘‘It would be nice if they [therapists] came in on a
regular basis, their timing seems all wrong, it’s so quick,
it’s info, info and then they are gone and you don’t see
them for weeks and then you have forgotten’’ (Teacher,
designated school)
‘‘As teachers we don’t really know much about the
programmes they are following – the physios come in
and it’s usually the TAs they talk to’’ (Teacher,
designated school)
There were several examples of where teachers and
TAs had helped children get the most out of their
therapy programmes and equipment. Some teachers
and TAs had found ways of integrating the pro-
grammes into the school routine so that they were
fun and caused less disruption to the child’s school
routine. Therapy visits in some instances were
planned and good relationships between therapy
services and school had been established.
‘‘She was reluctant to use her stander and now she is OK
and we fit this in every other day if we can – she used to
get quite tearful and stuff and now she is OK’’ (TA,
designated school)
‘‘He was really anti using it (standing frame) at first
because he said it hurt his legs, and I used to hate
putting him in it, but now he’s OK’ (Teacher, main-
stream school)
‘‘If we know we can incorporate into the whole class, he
didn’t like doing his exercises on his own but as soon as
we did this as a warm up he would do it because all the
children were involved’’ (Teacher, designated school)
‘‘I included a warm up and stretch session in PE and he
said to the TA that he loves that now – he used to hate
PE’’ (Teacher, mainstream school)
‘‘I just fit it [therapy] around so that the child doesn’t
miss out, they all go out to play’’ (TA, mainstream
school)
‘‘Therapy staff visit regularly and have built up a good
relationship with staff’’ (Teacher, designated school).
1918 E. Hutton & K. Coxon
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/28/
14Fo
r pe
rson
al u
se o
nly.

It became clear to the steering group that the
emotional burden on teachers and TAs was a major
and unexpected finding, overlooked both by health
and education. It was apparent that there was no
formal supervision or support available to help
individuals cope with the strong and often distressing
emotions associated with being responsible for a
child with a physical disability. A discussion ensued
about whether school was the appropriate place to
carry out some aspects of therapy that might be
uncomfortable for the child. The group concluded
that a child’s annual school review needed to include
an open and honest discussion around how to
respond to a child’s anxiety. Teachers and TAs
may need an identified person that they can talk to,
to ‘off load’ their feelings but also to raise appropriate
concerns about a child’s expression of pain or
discomfort.
The steering group challenged the largely negative
views of equipment expressed in the interviews and
focus groups. One member suggested that the child
actually ‘sees equipment differently because it helps
them feel more like their able-bodied peers’, enabling
them to do things other children can do. The group
acknowledged that as parents, teachers or therapists
they were familiar with equipment and had under-
estimated the perceptions of those less familiar with
specialist devices. Many comments from teachers
and TAs had focused on being uncomfortable with
the idea of ‘restraining’ a child with the use of straps,
and how this limited the child’s autonomy in the
classroom.
There was real concern that in some
instances equipment was acting as a barrier to
inclusion and that children were regularly missing
out on lesson or play time. Incidents of good
practice where schools had integrated the use of
equipment and the child’s therapy programmes
into the school routine successfully needed to be
shared, with illustrations of how this could be
achieved acting as an incentive for others to use
similar strategies.
What types of support and information did teachers and
TA identify as helpful?
Most participants identified practical solutions when
asked about the type of support they wanted.
Additional resources, more space, a quiet room
and additional staff were mentioned. Few identified
training although some wanted advice from thera-
pists and closer working relationships between health
and education.
‘‘Facilities should fit the children not the children having
to fit the facilities’’ (TA, designated school)
‘‘Storage is a huge issue for things in constant use’’
(TA, mainstream school)
‘‘More included, not taken away from the others’’
(TA, mainstream school).
‘‘. . . .somewhere quiet and safe’’ (TA, mainstream
school)
‘‘. . . times other than taught times [such as playtime and
PE and school trips]’’ (TA, mainstream)
‘‘Better sharing of information between health &
education because schools don’t get sufficient informa-
tion’’ (Teacher, designated school)
‘‘Hospital letters have no meaning for us, full of gumpf’’
(Teacher, designated school)
‘‘..Communication with the therapists so that we are
part of things’’ (Teacher, designated school).
The steering group explored these findings and felt
that it was interesting that teachers and TAs had not
identified training when asked what help and support
they would value, and wondered whether they think
in terms of ‘doing’ rather than ‘knowing’. For TAs,
the practical issues that faced them every day were
those that brought them into contact with inadequate
resources and lack of storage for equipment. Yet
having these aspects as a priority did not exclude the
need for training or information – sometimes
individuals ‘didn’t always know what they didn’t
know’.
Summary
Postural management is not a term widely under-
stood or used by Teachers and TAs, who lack a
conceptual framework that could assist them in
making sense of what they observe of children’s
posture, and inform everyday decisions about the
inclusion of children with PD. The negative attitudes
of teachers and TAs towards postural equipment in
the classroom, and the unacknowledged emotional
burden on teachers and TAs of working with
children with PD were identified as potential barriers
to the integration of postural management in school.
Facilitators included teaching staff’s use of humour
with children and the involvement of other children
in therapy programmes. Teachers and TAs focused
on a perceived need for practical resources to assist
them in their role: e.g. more space and additional
TAs, but did not identify the need for information or
training about the approach. They did, however,
want to establish closer working relations with
therapists and would have appreciated a coordinated
Posture for learning 1919
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/28/
14Fo
r pe
rson
al u
se o
nly.

approach to therapy visits, enabling them time to ask
questions. Discussions about the needs identified
during the research led to a number of ideas, and key
to this was finding a way to meet gaps in knowledge
and understanding of postural care in a manner that
was acceptable to parents and teaching staff alike.
Part 2: Developing the content and format of
the ‘A–Z of postural care’
‘The A–Z of postural care’ was developed by
therapists, researchers, parents and educators using
a ‘whole school’ approach to raise awareness within
schools about the importance of good posture and its
impact on children’s learning . Additional funding
was received from the LEA to support the develop-
ment of an information resource, with the intention
was that this would be freely available to all schools
within the county [27]. The steering committee for
the project reconvened and worked closely with a
graphic designer to produce an evidence-based,
accessible and attractive resource. The resulting
‘A–Z of Postural Care’ booklet and accompanying
poster are now available to all schools, to support
awareness of postural care.
The intention of the committee was to find a
means of creating an awareness-raising tool for
schools that would emphasise the importance of
good posture for all children and highlight its positive
impact on learning. Responding to the comments
about health service ‘gumpf’’, the steering group
wanted the information to be easy to understand and
relevant to learning. This is reflected in the title page
and the inclusion of the ‘posture for learning’ logo.
Access to the rich data informed the style and
content of the resource. The positive use of humour
by some teachers and TAs was a source of inspira-
tion, and the juxtaposition of cartoons enlivened an
otherwise ‘dry’ subject.
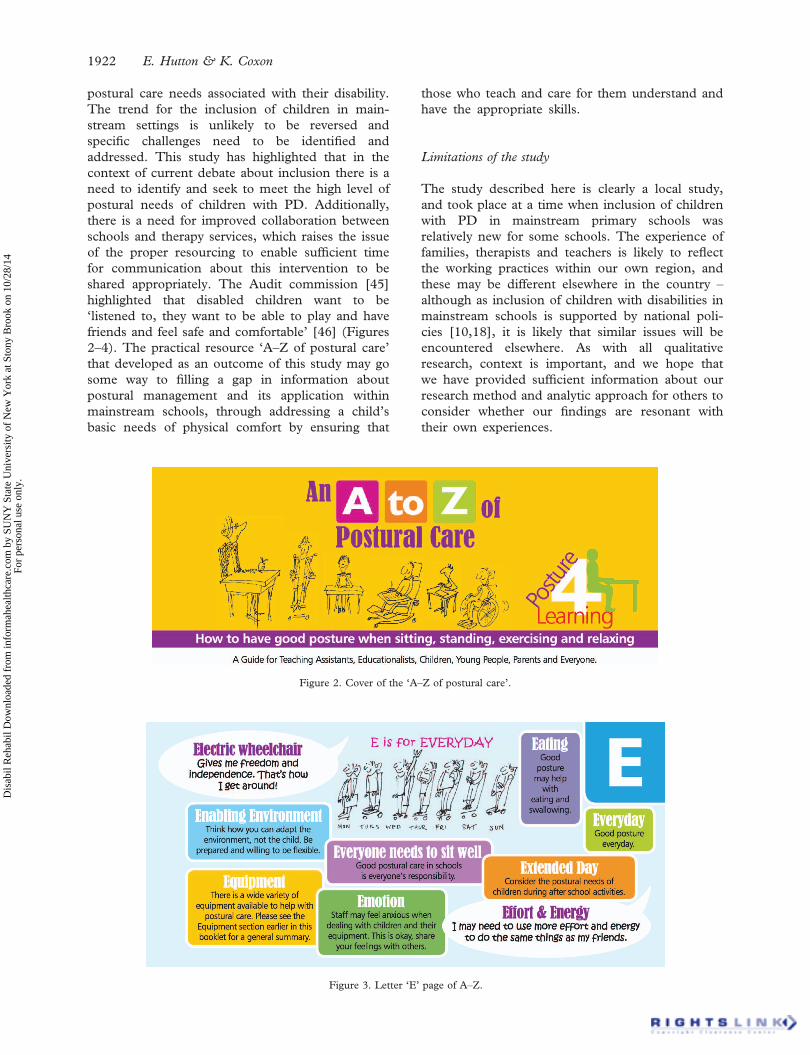
The A–Z approach organised many small
‘chunks’ of information into a limited format.
The booklet was designed with bright colours and
produced in ‘cheque book’ size so that it could sit
on the staff room coffee table and increase the
likelihood that school staff would pick it up and
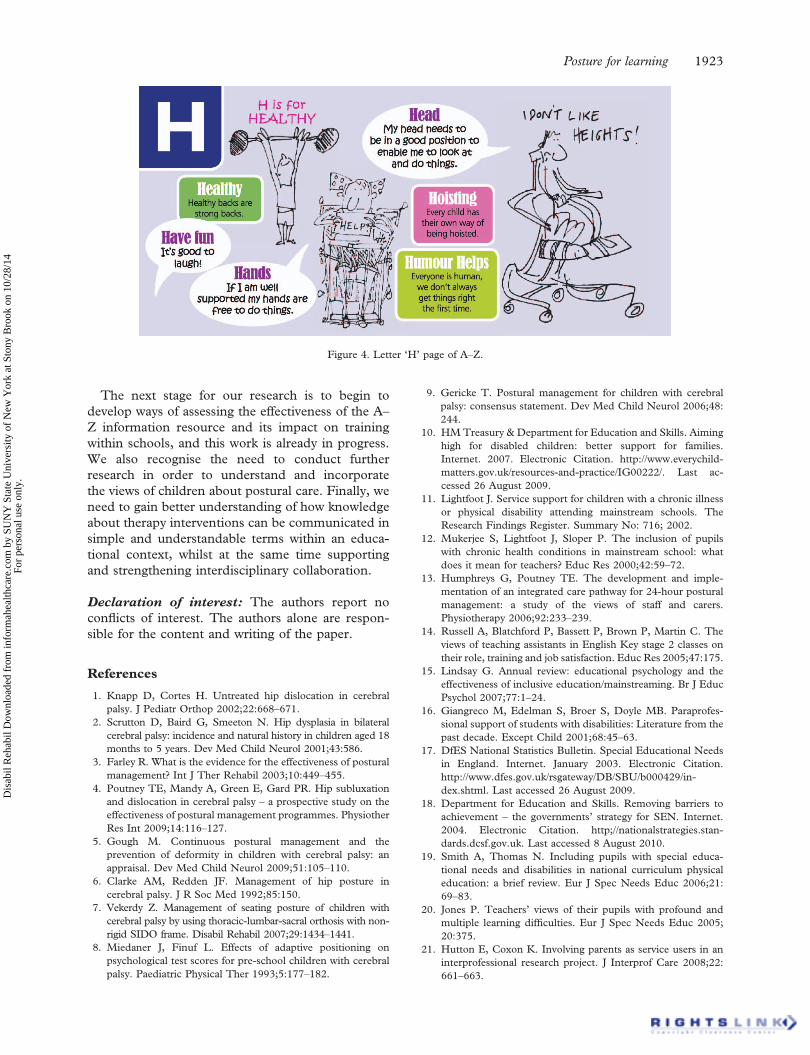
read it. Each letter of the alphabet had a single
message accompanied by a memorable image. For
example ‘E is for everyday’, ‘A is for good posture
for ALL’, ‘T is for teamwork’, all accompanied by
messages about inclusion, emotion, equipment and
function.
The published ‘A–Z of Postural Care’ booklet
and an accompanying poster is currently being
used to support workshops offered to schools to
support their learning and awareness of postural
management.
Discussion
The findings from this small exploratory study
provide an insight into the everyday issues facing
teachers and TAs in mainstream primary schools that
manage the postural care needs of children with a
physical disability. Some issues are relevant to the
development of policy, research and practice and are
discussed within the context of the educational
inclusion of children with special educational needs
in mainstream schools in England.
The most recent guidance on educational inclu-
sion is summarised in the introduction to the strategy
paper, ‘Removing barriers to achievement’ [18, p. 5]:
‘‘All children have the right to a good education and the
opportunity to fulfil their potential. All teachers should expect
to teach children with special educational needs (SEN) and
all schools should play their part in educating children from
their local community, whatever their background or ability.
We must reflect this in the way we train our teachers, in the
way we fund our schools, and in the way we judge their
achievements.’’
Building on earlier legislation [28], this document
outlined the then government’s position on inclusive
education, which reflects wider international trends
towards the educational inclusion of children with
special educational needs in mainstream schools.
Inclusion is believed to be a basic human right, but
educational inclusion is not without its critics; there
is ongoing academic and lay debate about the
appropriateness of what has been interpreted by
some as a ‘one-size fits all’ approach to the education
of children with a diverse range of special needs, and
in some instances; open hostility towards the policy
[29]. It is accepted that despite the rhetoric there is
wide variation in how the policy is implemented in
practice [30].
Those critical of inclusion cite the challenges of
including children with emotional and behavioural
difficulties in mainstream schools. It has been
suggested that the inclusion of children with physical
needs is more easily met [31]. The findings from this
study suggest this is too simplistic, being based on an
assumption that children with PD may not be as
obviously disruptive in the classroom as those with
emotional or behavioural difficulties. To suggest that
inclusion for children with PD occurs easily or
seamlessly is misleading; in common with other
research, this study has highlighted the intensive
work carried out by the children and the adults who
support them, to manage the physical and emotional
challenges that arise everyday [12,27,32,34].
Our study explored a single, but arguably highly
significant aspect of a child’s ‘physical’ needs.
Posture affects both health and educational
1920 E. Hutton & K. Coxon
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/28/
14Fo
r pe
rson
al u
se o
nly.

outcomes – a child’s comfort and positioning
influences not only their functional activity and
engagement in the curriculum but also their longer-
term health and well-being [30]. The interviews
identified that postural management as a concept
was not understood or appropriately applied on a
day-to-day basis by those teachers and TAs we talked
to. It also tended to be the physical and resourcing
barriers to inclusion that were openly acknowledged
by teachers and TAs, and that the underlying
uncertainties about what they were doing and
whether they were helping rather than harming the
child went unacknowledged and unaddressed.
Although the teacher training agency and HE
institutions intend to provide a good grounding in
core knowledge and skills, including access to
specialist skills required to manage children with
PD, gaps in knowledge and understanding exist and
can be attributed to the lack of appropriate training
in specialist skills available in mainstream schools for
both teachers and TAs [15,33,35]. What appeared to
be missing was a grounding in core knowledge about
postural management amongst teachers and TAs,
and this was compounded by variable specialist
support from therapists.
We identified that therapists are an important
source of information and support for teachers and
TAs about this topic; but they are not always in a
position to deliver information in a way that is
meaningful. Parry [36] argues that communication
with those involved in therapy treatment – what is
proposed and the reasons why – is a central part of
successful intervention. Her research into phy-
siotherapists’ accounts of their treatments identified
that they were often constrained by practical issues,
such as lack of time. Parry suggests that commu-
nication can persuade and motivate patients, provide
education, discourage resistance, and communicate
sensitively and informatively about difficult and
demanding activities and topics.
TAs had described therapists’ visits in some
instances as quick and unplanned. Had therapists
allowed sufficient time to respond to teachers’ and
TAs’ need to ‘ask questions’, it is possible that they
could more adequately address the rationale for
treatment interventions and that incidents where
children missed out on activities, due to misunder-
standing of how to apply the principles of postural
management, could have been avoided.
The literature on inclusion suggests that many
professionals believe the system is unworkable [31].
This was not the case in the schools we visited;
without exception all of the schools were working
hard to support the children with PD attending the
school, and several comments from those we
interviewed indicated that teachers and TAs advo-
cated strongly for the children’s inclusion. However,
many of those we spoke to viewed equipment the
children needed as a barrier to inclusion, viewing it
as ‘monstrous’ in some instances, leading to con-
cerns that these negative attitudes may be commu-
nicated to the children.
TAs described many practical difficulties asso-
ciated with storage of equipment. Although design
and manufacture of disability equipment has
developed and advanced, it may be that manufac-
turers need to think more carefully about the
environments where equipment is used and the
general public’s perception of disability equipment
[37]. Incidents where equipment had been recom-
mended by therapists without careful consideration
of where or how it would be used suggest that
therapists also need to think carefully about the
environment before prescribing [38]. The emo-
tional burden on teachers and TAs that the study
encountered echoes the experiences of parents and
other carers of children with a physical disability
[39]. Teachers and TAs may feel similarly un-
supported and overwhelmed when faced with the
associated additional responsibilities particularly
when coping with the child’s pain and discomfort
[40]. This finding in relation to primary school
inclusion rose inductively from the data, meaning
that it was not anticipated. It is of concern that the
individuals who are most intimately involved in
supporting primary aged disabled children are left
feeling unsupported and compromised, and that
the ‘emotional work’ [41], they undertake is
obscured, despite their role having a key impact
on a child’s school experience.
Co-ordination between agencies involved with
children with disabilities has been described by
families as one of the ‘biggest problems’ that face
them, and the evidence from this study suggests that
this remains a challenge [11,12]. The tensions of
inter-agency working are well documented in related
fields [42,43], and similar issues emerged with
regard to collaboration and multiagency working
between education and health. Therapists were
criticised by some teachers for rushed or unplanned
visits. Therapists also targeted their visits at the TA,
bypassing the needs of the teacher. The delegation of
support for children with disabilities to TAs is an
area of concern [16]. Criticism has been levelled at
schools where not only care – but too often the
education of children with special needs is delegated
to the TA [44]. By excluding teachers from their
visits, opportunities for therapists to provide infor-
mation about the application of postural manage-
ment, affecting the inclusion of the child and
necessary adaptations to the curriculum were possi-
bly missed.
Mainstream primary schools present a particular
set of challenges to the inclusion for children with
Posture for learning 1921
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/28/
14Fo
r pe
rson
al u
se o
nly.
postural care needs associated with their disability.
The trend for the inclusion of children in main-
stream settings is unlikely to be reversed and
specific challenges need to be identified and
addressed. This study has highlighted that in the
context of current debate about inclusion there is a
need to identify and seek to meet the high level of
postural needs of children with PD. Additionally,
there is a need for improved collaboration between
schools and therapy services, which raises the issue
of the proper resourcing to enable sufficient time
for communication about this intervention to be
shared appropriately. The Audit commission [45]
highlighted that disabled children want to be
‘listened to, they want to be able to play and have
friends and feel safe and comfortable’ [46] (Figures
2–4). The practical resource ‘A–Z of postural care’
that developed as an outcome of this study may go
some way to filling a gap in information about
postural management and its application within
mainstream schools, through addressing a child’s
basic needs of physical comfort by ensuring that
those who teach and care for them understand and
have the appropriate skills.
Limitations of the study
The study described here is clearly a local study,
and took place at a time when inclusion of children
with PD in mainstream primary schools was
relatively new for some schools. The experience of
families, therapists and teachers is likely to reflect
the working practices within our own region, and
these may be different elsewhere in the country –
although as inclusion of children with disabilities in
mainstream schools is supported by national poli-
cies [10,18], it is likely that similar issues will be
encountered elsewhere. As with all qualitative
research, context is important, and we hope that
we have provided sufficient information about our
research method and analytic approach for others to
consider whether our findings are resonant with
their own experiences.
Figure 2. Cover of the ‘A–Z of postural care’.
Figure 3. Letter ‘E’ page of A–Z.
1922 E. Hutton & K. Coxon
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/28/
14Fo
r pe
rson
al u
se o
nly.
The next stage for our research is to begin to
develop ways of assessing the effectiveness of the A–
Z information resource and its impact on training
within schools, and this work is already in progress.
We also recognise the need to conduct further
research in order to understand and incorporate
the views of children about postural care. Finally, we
need to gain better understanding of how knowledge
about therapy interventions can be communicated in
simple and understandable terms within an educa-
tional context, whilst at the same time supporting
and strengthening interdisciplinary collaboration.
Declaration of interest: The authors report no
conflicts of interest. The authors alone are respon-
sible for the content and writing of the paper.
References
1. Knapp D, Cortes H. Untreated hip dislocation in cerebral
palsy. J Pediatr Orthop 2002;22:668–671.
2. Scrutton D, Baird G, Smeeton N. Hip dysplasia in bilateral
cerebral palsy: incidence and natural history in children aged 18
months to 5 years. Dev Med Child Neurol 2001;43:586.
3. Farley R. What is the evidence for the effectiveness of postural
management? Int J Ther Rehabil 2003;10:449–455.
4. Poutney TE, Mandy A, Green E, Gard PR. Hip subluxation
and dislocation in cerebral palsy – a prospective study on the
effectiveness of postural management programmes. Physiother
Res Int 2009;14:116–127.
5. Gough M. Continuous postural management and the
prevention of deformity in children with cerebral palsy: an
appraisal. Dev Med Child Neurol 2009;51:105–110.
6. Clarke AM, Redden JF. Management of hip posture in
cerebral palsy. J R Soc Med 1992;85:150.
7. Vekerdy Z. Management of seating posture of children with
cerebral palsy by using thoracic-lumbar-sacral orthosis with non-
rigid SIDO frame. Disabil Rehabil 2007;29:1434–1441.
8. Miedaner J, Finuf L. Effects of adaptive positioning on
psychological test scores for pre-school children with cerebral
palsy. Paediatric Physical Ther 1993;5:177–182.
9. Gericke T. Postural management for children with cerebral
palsy: consensus statement. Dev Med Child Neurol 2006;48:
244.
10. HM Treasury & Department for Education and Skills. Aiming
high for disabled children: better support for families.
Internet. 2007. Electronic Citation. http://www.everychild-
matters.gov.uk/resources-and-practice/IG00222/. Last ac-
cessed 26 August 2009.
11. Lightfoot J. Service support for children with a chronic illness
or physical disability attending mainstream schools. The
Research Findings Register. Summary No: 716; 2002.
12. Mukerjee S, Lightfoot J, Sloper P. The inclusion of pupils
with chronic health conditions in mainstream school: what
does it mean for teachers? Educ Res 2000;42:59–72.
13. Humphreys G, Poutney TE. The development and imple-
mentation of an integrated care pathway for 24-hour postural
management: a study of the views of staff and carers.
Physiotherapy 2006;92:233–239.
14. Russell A, Blatchford P, Bassett P, Brown P, Martin C. The
views of teaching assistants in English Key stage 2 classes on
their role, training and job satisfaction. Educ Res 2005;47:175.
15. Lindsay G. Annual review: educational psychology and the
effectiveness of inclusive education/mainstreaming. Br J Educ
Psychol 2007;77:1–24.
16. Giangreco M, Edelman S, Broer S, Doyle MB. Paraprofes-
sional support of students with disabilities: Literature from the
past decade. Except Child 2001;68:45–63.
17. DfES National Statistics Bulletin. Special Educational Needs
in England. Internet. January 2003. Electronic Citation.
http://www.dfes.gov.uk/rsgateway/DB/SBU/b000429/in-
dex.shtml. Last accessed 26 August 2009.
18. Department for Education and Skills. Removing barriers to
achievement – the governments’ strategy for SEN. Internet.
2004. Electronic Citation. http;//nationalstrategies.stan-
dards.dcsf.gov.uk. Last accessed 8 August 2010.
19. Smith A, Thomas N. Including pupils with special educa-
tional needs and disabilities in national curriculum physical
education: a brief review. Eur J Spec Needs Educ 2006;21:
69–83.
20. Jones P. Teachers’ views of their pupils with profound and
multiple learning difficulties. Eur J Spec Needs Educ 2005;
20:375.
21. Hutton E, Coxon K. Involving parents as service users in an
interprofessional research project. J Interprof Care 2008;22:
661–663.
Figure 4. Letter ‘H’ page of A–Z.
Posture for learning 1923
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/28/
14Fo
r pe
rson
al u
se o
nly.

22. INVOLVE guidelines. 2004. Electronic Citation. http://www.in-
vo.org.uk/) Last accessed 31 December 2010.
23. Green J, Thorogood N. Qualitative methods for health
research. London: Sage; 2004.
24. Ritchie J, Spencer L. Qualitative data analysis for applied
policy research. In Bryman A, Burgess RG, editors.
Analysing qualitative data. London, New York: Routledge;
1994. pp 172–194.
25. Coreil J. Group interview methods in community health
research. Med Anthropol 1995;16:193–210.
26. Liamputtong P, Ezzy D. Qualitative research methods. 2nd
ed. Oxford: Oxford University Press; 2005.
27. Carlin J. Including me: managing complex health needs
in schools and early years settings. Internet. 2005. Electronic
Citation. http://nationalstrategies.standards.dcsf.gov.uk/node/
84492. Last accessed 8 August 2010.
28. Special Educational Needs and Disability Act 2001. Internet.
2001. Electronic Citation. http://www.opsi.gov.uk/acts/acts
2001/ukpga_20010010_en_1. Last accessed 8 August 2010.
29. Runswick-Cole K. Between a rock and a hard place: parents’
attitudes to the inclusion of children with special educational
needs in mainstream and special schools. Br J Spec Educ
2008;35:173–180.
30. Curtin M, Clarke G. Listening to young people with physical
disabilities’ experiences of education. Int J Disabil Dev Educ
2005;52:195–214.
31. Baker R. Turning point for special needs? Internet. 2005.
Electronic Citation. http://news.bbc.co.uk/1/hi/education/
4082350.stm. Last accessed 9 August 2010.
32. Mahon J, Cusack T. Physiotherapists’ role in integration
of children with cerebral palsy in mainstream schools.
Physiotherapy 2000;88:595–604.
33. Avramidis E, Bayliss P, Burden R. A survey into mainstream
teachers’ attitudes towards the inclusion of children with
special educational needs in the ordinary school in one local
education authority. Educ Psychol 2000;20:207.
34. Croll P, Moses D. Special needs in the primary school: one in
five? London: Cassell; 2004.
35. Hodkinson A. Pre-service teacher training and special
educational needs in England 1970–2008: is government
learning the lessons from the past or is it experiencing
groundhog day? Eur J Spec Needs Educ 2009;24:277–289.
36. Parry R. Are interventions to enhance communication
performance in allied health professionals effective, and how
should they be delivered? Direct and indirect evidence.
Patient Educ Counsel 2008;73:186–195.
37. Lawlor K, Mihaylov S, Welsh B, Jarvis S, Colver A.
A qualitative study of the physical, social and
attitudinal environments influencing the participation of
children with cerebral palsy. Pediatric Rehabil 2006;9:219–
228.
38. Hemmingson H, Borell L. Environmental barriers in
mainstream schools. Child Care Health Dev 2002;28:
57–63.
39. Contact a family. ‘No time for us’ relationships between
parents who have a disabled child: a survey of over 2,000
parents in the UK. Internet. 2003. Electronic Citation.
www.cafamily.org.uk/pdfs/no_time_for_us_report.pdf. Last
accessed 9 August 2010.
40. Swiggum M. Pain in children with cerebral palsy: implications
for pediatric physical therapy. Pediatric Physiother 2010;22:
86–92.
41. Hochshild AR. Emotion work, feeling rules and social
structure. Am J Sociol 1979;85:551–575.
42. Hudson B. Interprofessionality in health and social care:
the Achilles’ heel of partnership? J Interprof Care 2002;16:
7–17.
43. Johnson P, Wistow G, Schultz R, Hardy B. Interagency and
interprofessional collaboration in community care: the inter-
dependence of structures and values. J Interprof Care 2003;
17:69–83.
44. Groom B, Richard R. Supporting the inclusion of pupils with
social, emotional and behavioural difficulties in primary
schools: the role of teaching assistants. J Res Spec Educ Needs
2005;5:20.
45. Audit commission. Services for disabled children. Internet.
2003. Electronic Citation. http://www.audit-commission.gov.uk/
localgov/nationalstudies/Disabledchildren/Pages/default_copy.
aspx. Last accessed 9 August 2010.
46. Hutton E, Poole C, Townsend I, Mortimore J, Godden S,
Jensen J, Ariss T. A-Z of postural care. Internet. 2009.
Electronic Citation. http://www.ekhuft.nhs.uk/home-page/pa-
tients-and-public/a-z-of-patient-information/a-c/. Last ac-
cessed 8 August 2010.
1924 E. Hutton & K. Coxon
Dis
abil
Reh
abil
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/28/
14Fo
r pe
rson
al u
se o
nly.





























