Embed Size (px)
Citation preview

CRVASA-205; No. of Pages 6
Case report
Potentially misleading manifestation of a ventricularpre-excitation§
Jirina Hurychova a,*, Ludek Haman b
aDepartment of Cardiology, Prince Philip Hospital Llanelli, Hywel Dda University Health Board, United KingdombDepartment of Cardiovascular Medicine, University Hospital Hradec Kralove, Charles University in Prague,Faculty of Medicine in Hradec Kralove, Czech Republic
c o r e t v a s a x x x ( 2 0 1 4 ) e 1 – e 6
a r t i c l e i n f o
Article history:
Received 19 January 2014
Received in revised form
16 March 2014
Accepted 18 March 2014
Keywords:
Broad complex tachycardia
Accessory pathway
AVRT
Pre-excited atrial fibrillation
Sudden cardiac death
a b s t r a c t
We present the case report of a 56-year-old man with an unusual manifestation of an
accessory pathway. Failure to detect, or incorrect diagnosis, of this anomaly could have put
the patient at high risk of sudden cardiac death. The accessory pathway described in this
case report was located at the left posteroseptal area and presented initially with a broad
QRS complex tachycardia. Despite being pre-excited atrial fibrillation, it could have been
misinterpreted as ventricular tachycardia. Once the rhythm had changed to sinus, a Q-wave
in the inferior ECG leads became apparent. This finding could have been misdiagnosed as an
old myocardial infarction and treated as such, including prescription of betablockers which
might, in theory, increase the risk of sudden cardiac death. The treatment of choice for the
patient was radio frequency ablation of the accessory pathway.
Crown Copyright # 2014 Published by Elsevier Urban & Partner Sp. z o.o. on behalf of the
Czech Society of Cardiology. All rights reserved.
Available online at www.sciencedirect.com
ScienceDirect
journal homepage: http://www.elsevier.com/locate/crvasa
Introduction
Accessory atrioventricular (AV) pathways represent a pres-ence of abnormal conductive tissue between atria andventricles. They can be clinically completely asymptomatic,but on the other hand the abnormal accessory AV conductivitymay result in narrow or broad complex tachycardia. In thelatter case the diagnosis may be less obvious and theelectrocardiogram (ECG) can be misinterpreted. We presentthe case report of one of these manifestations to stress out theneed for carefully set diagnosis.
§ Supported by the programme PRVOUK P37/03.* Corresponding author. Tel.: +420 737710321.E-mail addresses: [email protected], [email protected]
Please cite this article in press as: J. Hurychova, L. Haman, Potentially m(2014), http://dx.doi.org/10.1016/j.crvasa.2014.03.002
http://dx.doi.org/10.1016/j.crvasa.2014.03.0020010-8650/Crown Copyright # 2014 Published by Elsevier Urban & Partnreserved.
Case description
A 56-year-old man was admitted to the cardiology depart-ment with a 2-day history of exertional shortness of breath,weakness and fatigue. He also developed central chestdiscomfort (pressure) and presented to the accident andemergency (A&E) department 2 hours later. He denied havingany palpitations or collapse. He was an ex-smoker whostopped smoking 5 years ago and his past medical historycomprised of arterial hypertension and chronic allergicalveolitis. His medications included losartan 50 mg/D,
(J. Hurychova).
isleading manifestation of a ventricular pre-excitation, Cor et Vasa
er Sp. z o.o. on behalf of the Czech Society of Cardiology. All rights

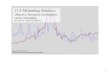
Fig. 1 – ECG on admission. Irregular broad complex tachycardia, positive concordancy + LAH morphology: pre-excited atrialfibrillation with rapid ventricular response, shortest pre-excited RR interval 200 ms.
c o r e t v a s a x x x ( 2 0 1 4 ) e 1 – e 6e2
CRVASA-205; No. of Pages 6
prednisolon 20 mg/D and salicylic acid 100 mg/D. He was on alow fat diet due to hypercholesterolaemia. He had a positivefamily history of a premature ischaemic heart disease (hisfather died from myocardial infarction at 60). On admission,he was haemodynamically stable with no signs of heartfailure, BP was 120/70 mmHg and heart sounds were irregular230 beats per minute with the peripheral pulse deficit. Thepressure chest pain eased off completely with sublingualnitrate. ECG on admission (Fig. 1) showed irregular broad-complex tachycardia (BCT) with positive concordancy inprecordial leads, left axis deviation (LAH) and a ventricularrate of approximately 250 beats/min. The tachycardia wasinitially slowed down by i.v. amiodarone 300 mg but, as heremained tachycardic he was cardioverted to sinus bysynchronized electrical cardioversion. The subsequent ECG(Fig. 2) showed sinus rhythm with varying QRS width and Qwave pattern in leads III and aVF. No previous ECG wasavailable for comparison. Blood results were unremarkablewith no electrolytes abnormalities, normal thyroid functiontest and normal creatine kinase (including MB fraction).Troponin T was slightly elevated. Transthoracic echocardi-ography was carried out and revealed well maintained leftventricular systolic function with mild multifocal regionalwall motion abnormalities and moderate mitral regurgita-tion.
What is the diagnosis?
On detail ECG analysis we can see a broad complex tachycardiawhich could be misinterpreted as ventricular tachycardia (VT),
Please cite this article in press as: J. Hurychova, L. Haman, Potentially m(2014), http://dx.doi.org/10.1016/j.crvasa.2014.03.002
but the obvious irregular rhythm indicates that the correctdiagnosis is pre-excitated atrial fibrillation with an antegra-dely conducting accessory pathway (Fig. 1). Shortest pre-excited RR interval 200 ms indicates high-risk accessorypathway (very fast antegrade conduction via accessorypathway with risk of degeneration to ventricular fibrillation).The varying QRS width on ECG after electrical cardioversion iscaused by pre-excitation including Q wave pattern in theinferior leads which is in fact a negative delta wave. Pre-excitation is more expressed with atrial premature beats(Fig. 2).
This patient underwent an electrophysiology study whichconfirmed the presence of the atrioventricular accessorypathway in the left posteroseptal region (antegrade conduc-tion – atrial effective refractory period/ERP/240 ms, accessorypathway ERP < 260 ms, AV re-entry tachycardia non-induc-ible). The pathway was successfully ablated (Fig. 3) with nofurther ECG evidence of pre-excitation (Fig. 4).
Start of the radio frequency energy application during atrialstimulation with marked pre-excitation (first three beats,positive delta waves in aVL, V1, V4, V5, negative delta waves inII, III, aVF). Fourth and fifth stimulus is not conducted viaaccessory pathway (successful ablation), fifth stimulus isconducted to ventricle via AV node with no marks of pre-excitation – note narrow QRS complex, His bundle potential onHBE 2-3 (in first three beats hidden in pre-excited ventricularpotential), prolongation of atrioventricular interval on coro-nary sinus electrograms.
II, III, aVL, aVF, V1, V4, V5 – surface lead ECG, HRA – highright atrium, HBE 2-3 – electrogram from His bundle region, CS9-10 – coronary sinus ostium electrogram, CS 1-2 – distal
isleading manifestation of a ventricular pre-excitation, Cor et Vasa

Fig. 2 – ECG after electrical cardioversion. Sinus rhythm and pre-excitation (negative delta wave in III, aVF, positive delta wavein V2–V6), two atrial premature beats (second and fourth beat) with marked pre-excitation.
Fig. 3 – Catheter ablation of accessory pathway.
c o r e t v a s a x x x ( 2 0 1 4 ) e 1 – e 6 e3
CRVASA-205; No. of Pages 6
Please cite this article in press as: J. Hurychova, L. Haman, Potentially misleading manifestation of a ventricular pre-excitation, Cor et Vasa(2014), http://dx.doi.org/10.1016/j.crvasa.2014.03.002

Fig. 4 – ECG after catheter ablation. Sinus rhythm with no signs of pre-excitation.
c o r e t v a s a x x x ( 2 0 1 4 ) e 1 – e 6e4
CRVASA-205; No. of Pages 6
coronary sinus electrogram, RF bip – electrogram from ablationcatheter. Paper speed was 100 mm/s.
Discussion
Accessory atrioventricular pathways are congenital abnor-malities involving the presence of abnormal conduction tissuebetween the atria and the ventricles which can cause earlydepolarisation of the ventricular myocardium: pre-excitation.
The first suggestion of the existence of these pathways wasmentioned by Holzmann and Scherf in 1932 [1]. Until 1932 thepresence of a broad QRS complex associated with paroxysmaltachycardia was categorized as a bundle-branch block phe-nomenon [2,3]. First histological evidence of accessorypathway was proved in 1942 by Wood et al. [4]. David Scherfis thought to be the first person who described our currentunderstanding of the pathogenesis of the Wolff–Parkinson–White (WPW) syndrome in terms of a re-entrant circuitinvolving both the AV node – His axis and the accessorypathway. This hypothesis was not universally accepted untilthe 1970s when Durrer and others applied invasive electricalstimulation to the heart to confirm the pathophysiologicalprocesses [5–9]. Morady and Scheinman were the first tosuccessfully ablate an accessory pathway (posteroseptal)using high-energy direct-current shocks. Subsequently Jack-man, Kuck, Morady, and a number of groups proved theremarkable safety and efficiency of catheter ablation forpathways in all locations using radio frequency energy [10].
Accessory atrioventricular pathways arise during embry-onic evolution when atria and ventricles are not adequatelydivided. These may be either isolated or multifocal with septalor posterior location [11]. The electrical impulse can pass
Please cite this article in press as: J. Hurychova, L. Haman, Potentially m(2014), http://dx.doi.org/10.1016/j.crvasa.2014.03.002
through the pathway either antegrade, towards to ventricle,retrograde, away from the ventricle or in both directions. Themajority of pathways allow conduction in both direction, withretrograde only conduction occurring in 17–37% of cases(known as a concealed accessory pathway) and antegrade onlyconduction rarely seen [12,13]. The electrical activation of themyocardium starts from sinoatrial node and reaches theventricles through both the accessory pathway and atrioven-tricular (AV) node. As the accessory pathway conducts theimpulse faster than the AV node, the ventricular depolarisa-tion starts from the accessory pathway region and is followedby depolarisation via the AV node-His conduction system. Thisresults in a short PR interval and slurred upstroke of the QRScomplex known as the delta wave.
The patients with pre-excitation ECG pattern are oftenasymptomatic. The antegrade conductivity can spontaneouslyresolve in about 30% of all cases. Symptomatic patients mayexperience palpitations, dizziness, shortness of breath orsyncope. Of note the first presentation of pre-excitation maybe a sudden cardiac death. Fortunately this happens veryrarely (0.15–0.4%) [14,15].
Symptoms are caused by atrioventricular re-entry tachy-cardia (AVRT) which can be either orthodromic or antidromic.The terminology depends on the direction of the electricalimpulse going through AV node. The ventricular myocardiumis activated through either the normal conduction systemresulting in a narrow complex tachycardia (orthodromicAVRT) or through the accessory pathway (antidromic AVRT)with a broad complex tachycardia.
A complex of symptoms due to supraventricular tachycar-dia with evidence of pre-excitation on ECG is called WPWsyndrome [16]. The presence of an accessory pathways isdangerous in patients with atrial fibrillation [17–19]. The AV
isleading manifestation of a ventricular pre-excitation, Cor et Vasa

c o r e t v a s a x x x ( 2 0 1 4 ) e 1 – e 6 e5
CRVASA-205; No. of Pages 6
node provides protection against a fast ventricular response toatrial tachycardia. In the presence of a rapidly conductingaccessory pathway fast atrial electrical impulses conductedvia the pathway may lead to an extremely rapid ventricularresponse with degeneration to ventricular fibrillation.
The first line of treatment for symptomatic patients is radiofrequency ablation of the accessory pathway with success rateof 90–95% depending of its location [20–22]. There is no clearindication for this treatment in asymptomatic patients but itshould be considered with respect to the patient's profession(e.g. pilot), age (higher prevalence of atrial fibrillation withincreasing age) and electrophysiological parameters of acces-sory pathways. Medical management includes either class Iantiarrhythmic drugs (propafenone) or class III (sotalol,amiodarone) which slow down pathway conduction. Theuse of AV node conduction blocking/slowing drugs (particu-larly verapamil) may be harmful allowing rapid unopposedconduction down the accessory pathway with the potential ofthe above-mentioned consequences [23–25].
Summary
A careful ECG analysis is vital for obtaining a correct diagnosisof pre-excited atrial fibrillation. This is necessary for furthermanagement with respect to the symptoms and prognosis,particularly the risk of sudden cardiac death. The widerdifferential diagnosis like ventricular tachycardia caused byacute coronary syndrome based on history, ECG and laboratoryresults could have been considered in brainstorming process,but eliminated as a false route.
We also aimed to show a less common ECG presentationof an accessory atrioventricular pathway due to negativedelta wave in inferior leads. This could be potentiallymisleading for less experienced physician who could be leadto believe that they were dealing with consequences chestpain/acute myocardial ischaemia – ventricular tachycardiaand treat the patient accordingly with potentially harmfulmedication.
We have to keep pre-excitation syndrome in mindespecially in young patients with history of palpitations butit may occur at any age, irrespective of the presence ofcomorbidities or risk factors.
Conflicts of interest
No known conflicts of interest associated with this publica-tion.
Funding
No financial support received for this work.
Ethical statement
We hereby declare we have not breached any ethical standardsby writing this article.
Please cite this article in press as: J. Hurychova, L. Haman, Potentially m(2014), http://dx.doi.org/10.1016/j.crvasa.2014.03.002
r e f e r e n c e s
[1] M. Holzmann, D. Scherf, Uber Elektrokardiogramme mitverkurzter Vorhof-Kammerdiztanz und positiven P-Zacken,Zeitschrift fur Klinische Medizin 121 (1932) 404–423.
[2] A.E. Cohn, F.R. Fraser, Paroxysmal tachycardia and theeffect of stimulation of the vagus nerve by pressure, Heart 5(1913–1914) 93–105.
[3] L. Wolff, J. Parkinson, P.D. White, Bundle-branch block withshort P-R interval in healthy young people prone toparoxysmal tachycardia, American Heart Journal 5 (1930)685–704.
[4] F.C. Wood, C.C. Wolferth, G.D. Geckeler, Histologicdemonstration of accessory muscular connections betweenauricle and ventricle in a case of short P-R interval andprolonged QRS complex, American Heart Journal 25 (1943)454–462.
[5] D. Durrer, J.P. Roos, Epicardial excitation of the ventricles ina patient with the Wolff–Parkinson–White Syndrome (typeB), Circulation 35 (1967) 15–21.
[6] D. Durrer, R.M. Schuilenburg, H.J.J. Wellens, Pre-excitationrevisited, American Journal of Cardiology 25 (1970) 690–697.
[7] H.B. Burchell, R.L. Frye, M.W. Anderson, et al.,Atrioventricular and ventriculo-atrial excitation in Wolff–Parkinson–White syndrome (type B): temporary ablation atsurgery, Circulation 36 (1967) 663–672.
[8] F.R. Cobb, S.D. Blumenschein, W.C. Sealy, et al., Successfulsurgical interruption of the bundle of Kent in a patient withWolff–Parkinson–White syndrome type A, Circulation 38(1968) 1018–1029.
[9] A. Castellanos Jr., A.S. Agha, C.S. Castillo, et al.,Ventricular activation in the presence of Wolff–Parkinson–White syndrome, in: L.S. Dreifus, Likoff (Eds.),Cardiac Arrhythmias, Grune & Stratton, New York, 1973,pp. 457–474.
[10] M.M. Scheinman, F. Morady, D.S. Hess, et al., Catheter-induced ablation of the atrioventricular junction to controlrefractory supraventricular arrhythmias, Journal ofAmerican Medical Association 248 (1982) 851–855.
[11] B.D. Lindsay, K.J. Crossen, M.E. Cain, Concordance ofdistinguishing electrocardiographic features during sinusrhythm with the location of accessory pathways in theWolff–Parkinson–White syndrome, American Journal ofCardiology 59 (1987) 1093.
[12] M.E. Cain, R.A. Luke, B.D. Lindsay, Diagnosis andlocalization of accessory pathways, Pacing and ClinicalElectrophysiology 15 (1992) 801.
[13] J.M. Miller, Therapy of Wolff–Parkinson–White syndromeand concealed bypass tracts: Part I, Journal ofCardiovascular Electrophysiology 7 (1996) 85.
[14] D.M. Todd, G.J. Klein, A.D. Krahn, et al., AsymptomaticWolff–Parkinson–White syndrome: is it time to revisitguidelines? Journal of the American College of Cardiology41 (2003) 245.
[15] J.W. Leitch, G.J. Klein, R. Yee, Prognostic value ofelectrophysiologic testing in asymptomatic patients withWolff–Parkinson–White pattern, Circulation 82 (1990) 1718.
[16] Definition of terms related to cardiac rhythm, Am Heart J95 (1978) 796.
[17] P.J. Fitzsimmons, P.D. McWhirter, D.W. Peterson, W.B.Kruyer, The natural history of Wolff–Parkinson–Whitesyndrome in 228 military aviators: a long term follow-up of22 years, American Heart Journal 142 (2001) 530.
[18] R. Yee, G.J. Klein, A.D. Sharma, et al., Tachycardiaassociated with accessory atrioventricular pathways, in: D.P. Zipes, J. Jalife (Eds.), Cardiac Electrophysiology, WBSaunders, Philadelphia, 1990, p. 463.
isleading manifestation of a ventricular pre-excitation, Cor et Vasa

c o r e t v a s a x x x ( 2 0 1 4 ) e 1 – e 6e6
CRVASA-205; No. of Pages 6
[19] C. Timmermans, J.L. Smeets, L.M. Rodriguez, Abortedsudden death in the Wolff–Parkinson–White syndrome,American Journal of Cardiology 76 (1995) 492.
[20] S.A. Chen, C.T. Tai, Ablation of atrioventricular accessorypathways: current technique-state of the art, Pacing andClinical Electrophysiology 24 (2001) 1795.
[21] H. Calkins, J. Langberg, J. Sousa, Radiofrequency catheterablation of accessory atrioventricular connection in 250patients. Abbreviated therapeutic approach to Wolff–Parkinson–White syndrome, Circulation 85 (1992) 1337.
[22] M.M. Scheinman, S. Huang, The 1998 NASPE prospectivecatheter ablation registry, Pacing and ClinicalElectrophysiology 23 (2000) 1020.
[23] Doporučené postupy pro diagnostiku a léčbusupraventrikulárních tachyarytmií, Supplementum CorVasa 47 (9) (2005) 18–39.
[24] C. Blomstrom-Lundqvist, M.M. Scheinman, E.M. Aliot, et al.,ACC/AHA/ESC guidelines for the management of patients
Please cite this article in press as: J. Hurychova, L. Haman, Potentially m(2014), http://dx.doi.org/10.1016/j.crvasa.2014.03.002
with supraventricular arrhythmias – executive summary: areport of the American College of Cardiology/AmericanHeart Association Task Force on Practice Guidelines andthe European Society of Cardiology Committee for PracticeGuidelines (Writing Committee to Develop Guidelines forthe Management of Patients With SupraventricularArrhythmias), Circulation 108 (2003) 1871.
[25] D.P. Zipes, A.J. Camm, M. Borggrefe, et al., ACC/AHA/ESC2006 guidelines for management of patients withventricular arrhythmias and the prevention of suddencardiac death: a report of the American College ofCardiology/American Heart Association Task Force andthe European Society of Cardiology Committee forPractice Guidelines (Writing Committee to DevelopGuidelines for Management of Patients With VentricularArrhythmias and the Prevention of Sudden CardiacDeath), Journal of the American College of Cardiology 48(2006) e247.
isleading manifestation of a ventricular pre-excitation, Cor et Vasa