Embed Size (px)
Citation preview
12/13/2015
1
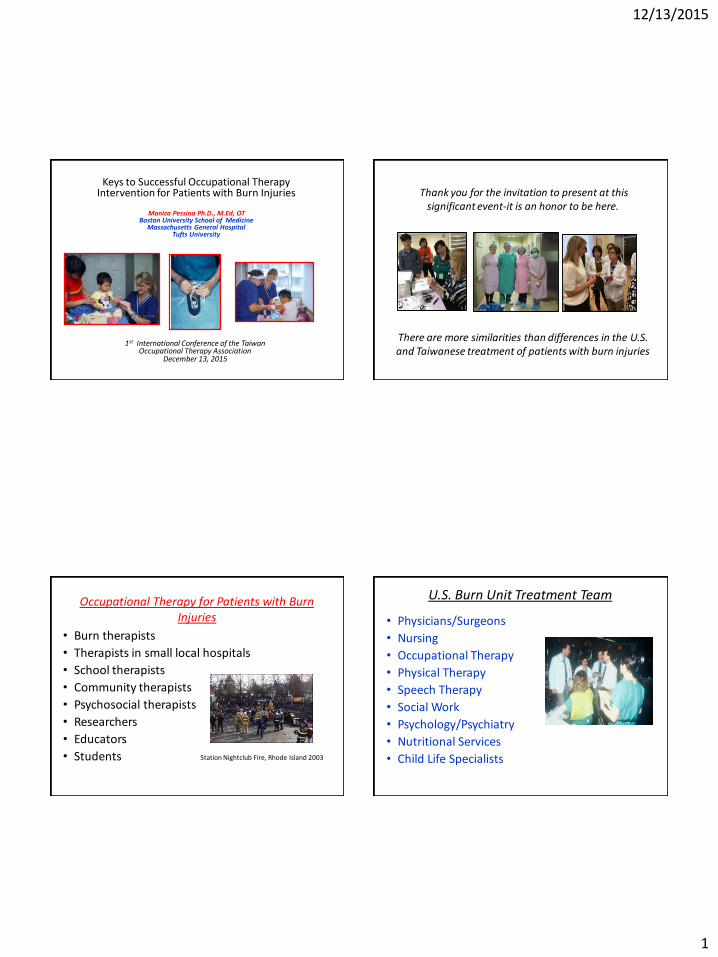
Keys to Successful Occupational Therapy Intervention for Patients with Burn Injuries
Monica Pessina Ph.D., M.Ed, OT
Boston University School of Medicine Massachusetts General Hospital
Tufts University
1st International Conference of the Taiwan
Occupational Therapy Association December 13, 2015
Thank you for the invitation to present at this significant event-it is an honor to be here.
There are more similarities than differences in the U.S. and Taiwanese treatment of patients with burn injuries
Occupational Therapy for Patients with Burn Injuries
• Burn therapists
• Therapists in small local hospitals
• School therapists
• Community therapists
• Psychosocial therapists
• Researchers
• Educators
• Students
Station Nightclub Fire, Rhode Island 2003
U.S. Burn Unit Treatment Team
• Physicians/Surgeons
• Nursing
• Occupational Therapy
• Physical Therapy
• Speech Therapy
• Social Work
• Psychology/Psychiatry
• Nutritional Services
• Child Life Specialists
12/13/2015
2
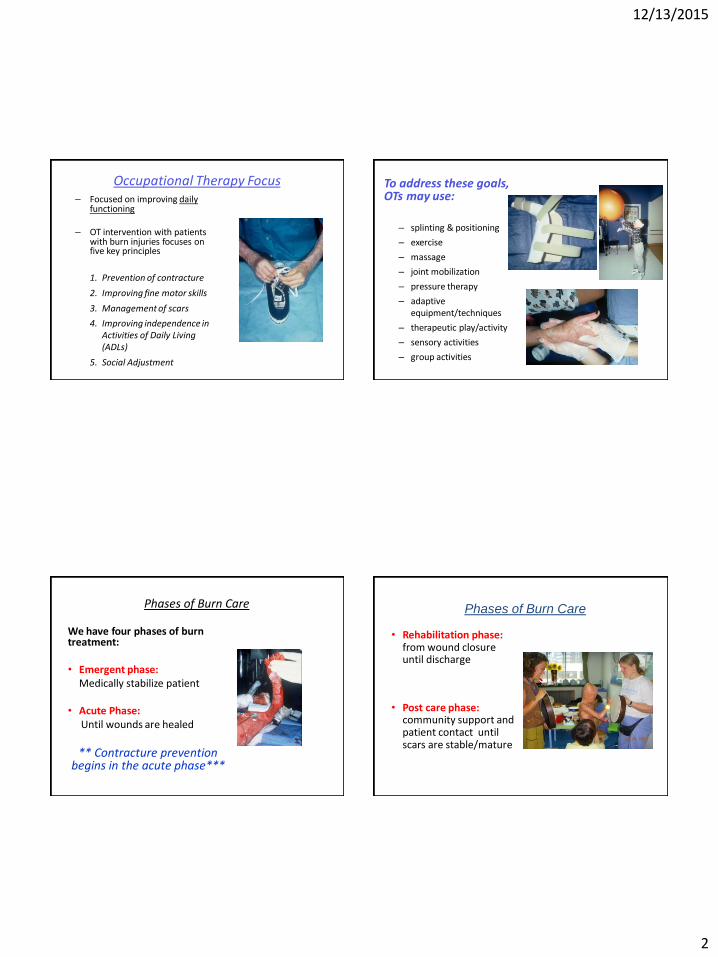
Occupational Therapy Focus – Focused on improving daily
functioning
– OT intervention with patients with burn injuries focuses on five key principles
1. Prevention of contracture
2. Improving fine motor skills
3. Management of scars
4. Improving independence in Activities of Daily Living (ADLs)
5. Social Adjustment
To address these goals, OTs may use:
– splinting & positioning
– exercise
– massage
– joint mobilization
– pressure therapy
– adaptive equipment/techniques
– therapeutic play/activity
– sensory activities
– group activities
Phases of Burn Care
We have four phases of burn treatment: • Emergent phase: Medically stabilize patient • Acute Phase: Until wounds are healed
** Contracture prevention begins in the acute phase***
• Rehabilitation phase: from wound closure until discharge
• Post care phase: community support and patient contact until scars are stable/mature
Phases of Burn Care
12/13/2015
3
Occupational Therapy Focus – Focused on improving daily
functioning
– OT intervention with patients with burn injuries focuses on five key principles
1. Prevention of contracture
2. Improving fine motor skills
3. Management of scars
4. Improving independence in Activities of Daily Living (ADLs)
5. Social Adjustment
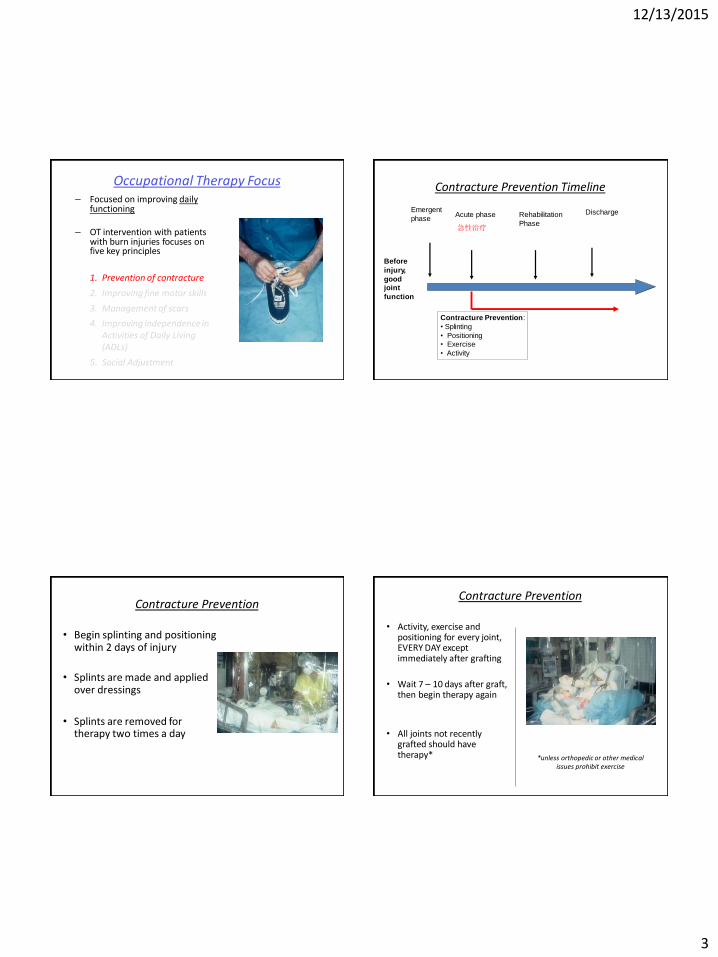
Contracture Prevention Timeline
Before
injury,
good
joint
function
Emergent
phase Acute phase Rehabilitation
Phase
Discharge
Contracture Prevention:
• Splinting
• Positioning
• Exercise
• Activity
急性治疗
Contracture Prevention
• Begin splinting and positioning within 2 days of injury
• Splints are made and applied over dressings
• Splints are removed for therapy two times a day
Contracture Prevention
• Activity, exercise and positioning for every joint, EVERY DAY except immediately after grafting
• Wait 7 – 10 days after graft, then begin therapy again
• All joints not recently grafted should have therapy*
*unless orthopedic or other medical issues prohibit exercise
12/13/2015
4
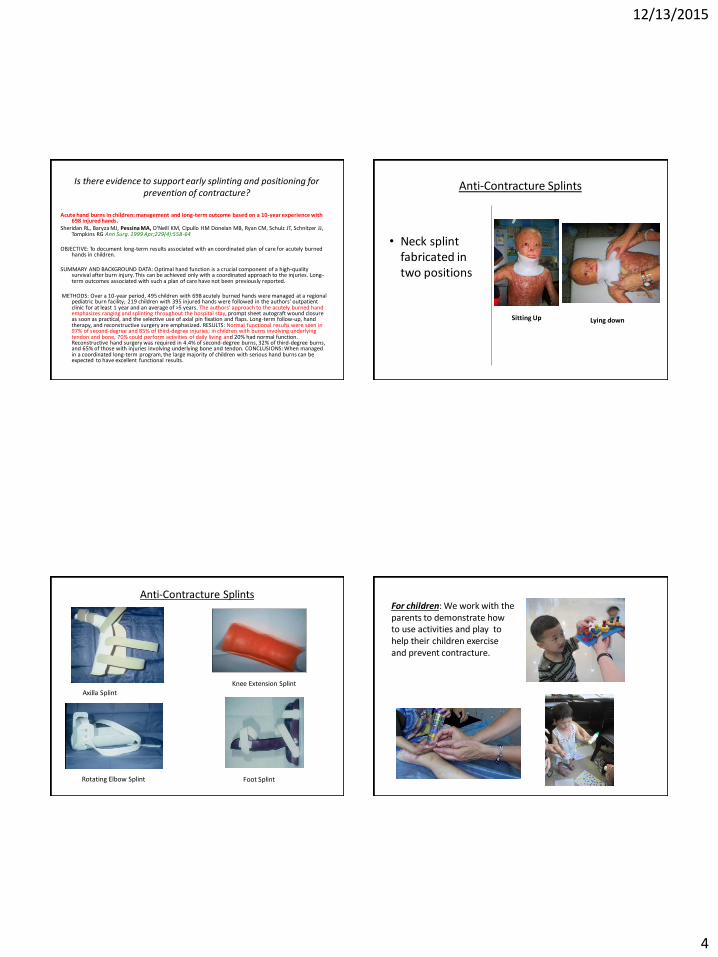
Is there evidence to support early splinting and positioning for prevention of contracture?
. Acute hand burns in children: management and long-term outcome based on a 10-year experience with
698 injured hands. Sheridan RL, Baryza MJ, Pessina MA, O'Neill KM, Cipullo HM Donelan MB, Ryan CM, Schulz JT, Schnitzer JJ,
Tompkins RG Ann Surg. 1999 Apr;229(4):558-64 OBJECTIVE: To document long-term results associated with an coordinated plan of care for acutely burned
hands in children. SUMMARY AND BACKGROUND DATA: Optimal hand function is a crucial component of a high-quality
survival after burn injury. This can be achieved only with a coordinated approach to the injuries. Long-term outcomes associated with such a plan of care have not been previously reported.
METHODS: Over a 10-year period, 495 children with 698 acutely burned hands were managed at a regional
pediatric burn facility; 219 children with 395 injured hands were followed in the authors' outpatient clinic for at least 1 year and an average of >5 years. The authors' approach to the acutely burned hand emphasizes ranging and splinting throughout the hospital stay, prompt sheet autograft wound closure as soon as practical, and the selective use of axial pin fixation and flaps. Long-term follow-up, hand therapy, and reconstructive surgery are emphasized. RESULTS: Normal functional results were seen in 97% of second-degree and 85% of third-degree injuries; in children with burns involving underlying tendon and bone, 70% could perform activities of daily living and 20% had normal function. Reconstructive hand surgery was required in 4.4% of second-degree burns, 32% of third-degree burns, and 65% of those with injuries involving underlying bone and tendon. CONCLUSIONS: When managed in a coordinated long-term program, the large majority of children with serious hand burns can be expected to have excellent functional results.
• Neck splint fabricated in two positions
Sitting Up
Lying down
Anti-Contracture Splints
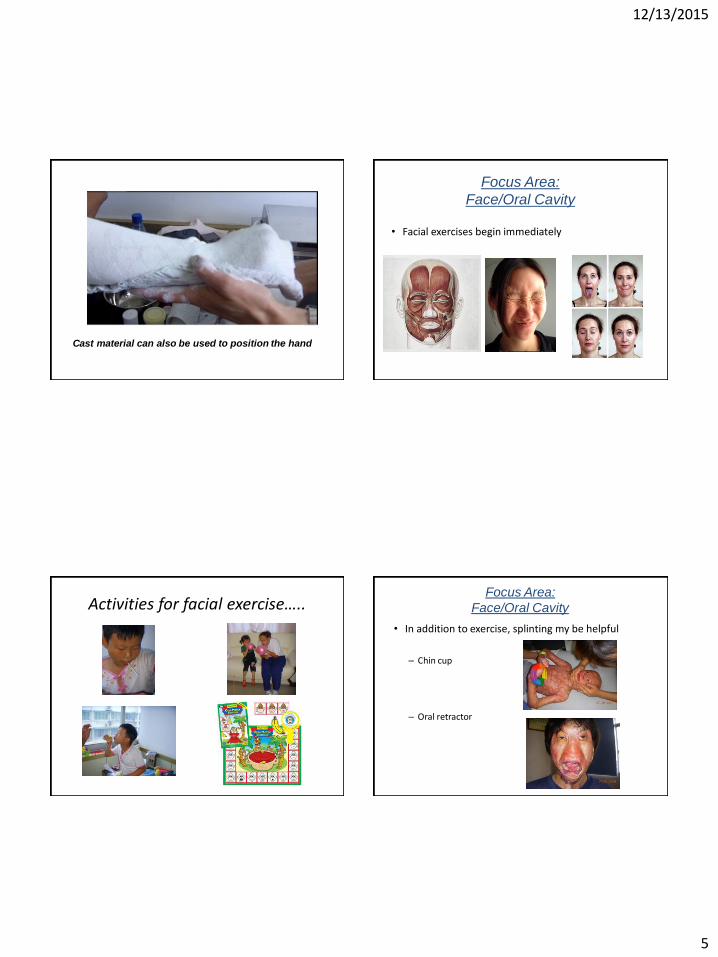
Anti-Contracture Splints
Axilla Splint
Rotating Elbow Splint
Knee Extension Splint
Foot Splint
For children: We work with the parents to demonstrate how to use activities and play to help their children exercise and prevent contracture.
12/13/2015
5
Cast material can also be used to position the hand
• Facial exercises begin immediately
Focus Area:
Face/Oral Cavity
Activities for facial exercise…..
• In addition to exercise, splinting my be helpful
– Chin cup
– Oral retractor
Focus Area:
Face/Oral Cavity
12/13/2015
6
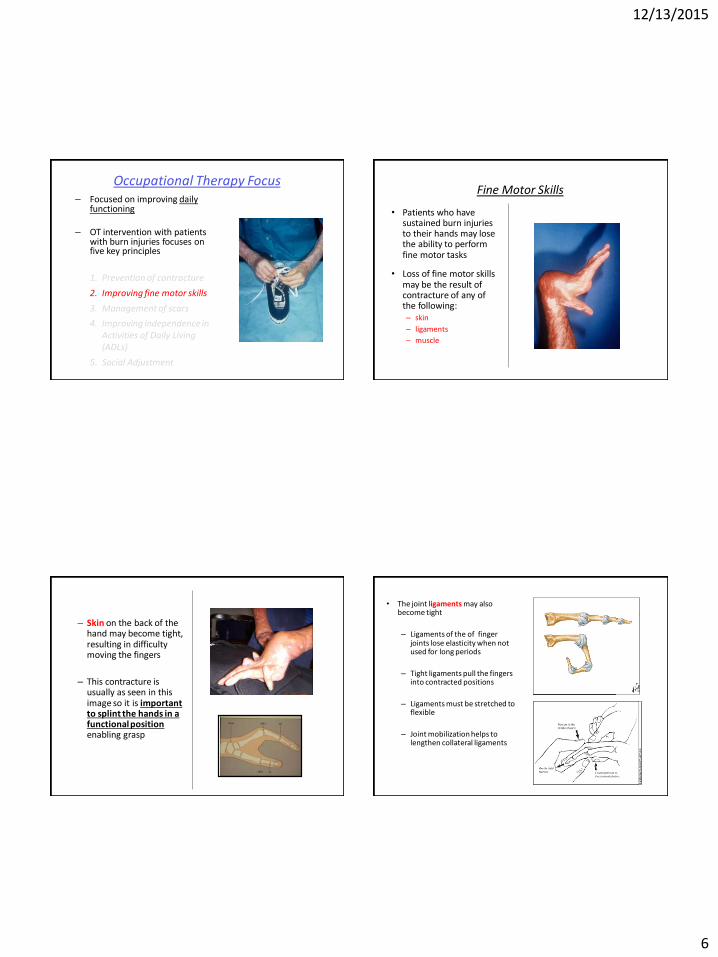
Occupational Therapy Focus – Focused on improving daily
functioning
– OT intervention with patients with burn injuries focuses on five key principles
1. Prevention of contracture
2. Improving fine motor skills
3. Management of scars
4. Improving independence in Activities of Daily Living (ADLs)
5. Social Adjustment
Fine Motor Skills
• Patients who have sustained burn injuries to their hands may lose the ability to perform fine motor tasks
• Loss of fine motor skills may be the result of contracture of any of the following: – skin
– ligaments
– muscle
– Skin on the back of the hand may become tight, resulting in difficulty moving the fingers
– This contracture is usually as seen in this image so it is important to splint the hands in a functional position enabling grasp
• The joint ligaments may also become tight
– Ligaments of the of finger joints lose elasticity when not used for long periods
– Tight ligaments pull the fingers into contracted positions
– Ligaments must be stretched to flexible
– Joint mobilization helps to lengthen collateral ligaments
12/13/2015
7
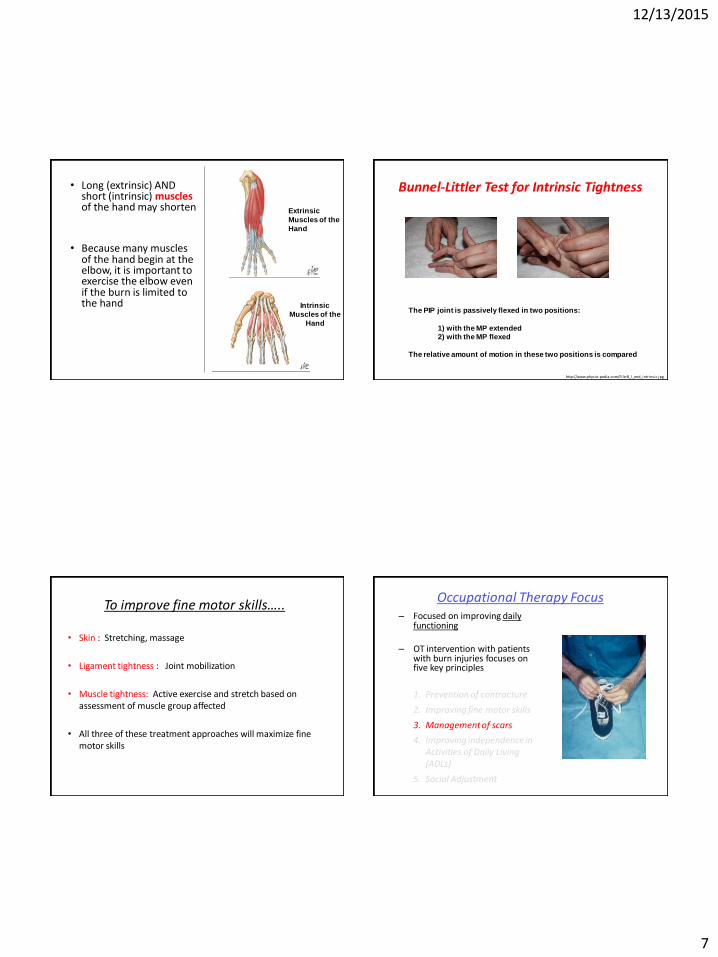
• Long (extrinsic) AND short (intrinsic) muscles of the hand may shorten
• Because many muscles of the hand begin at the elbow, it is important to exercise the elbow even if the burn is limited to the hand
Extrinsic
Muscles of the
Hand
Intrinsic
Muscles of the
Hand
Bunnel-Littler Test for Intrinsic Tightness
The PIP joint is passively flexed in two positions:
1) with the MP extended
2) with the MP flexed
The relative amount of motion in these two positions is compared
http://www.physio-pedia.com/File:B_l_end_intrinsic.jpg
To improve fine motor skills…..
• Skin : Stretching, massage
• Ligament tightness : Joint mobilization
• Muscle tightness: Active exercise and stretch based on assessment of muscle group affected
• All three of these treatment approaches will maximize fine motor skills
Occupational Therapy Focus – Focused on improving daily
functioning
– OT intervention with patients with burn injuries focuses on five key principles
1. Prevention of contracture
2. Improving fine motor skills
3. Management of scars
4. Improving independence in Activities of Daily Living (ADLs)
5. Social Adjustment
12/13/2015
8
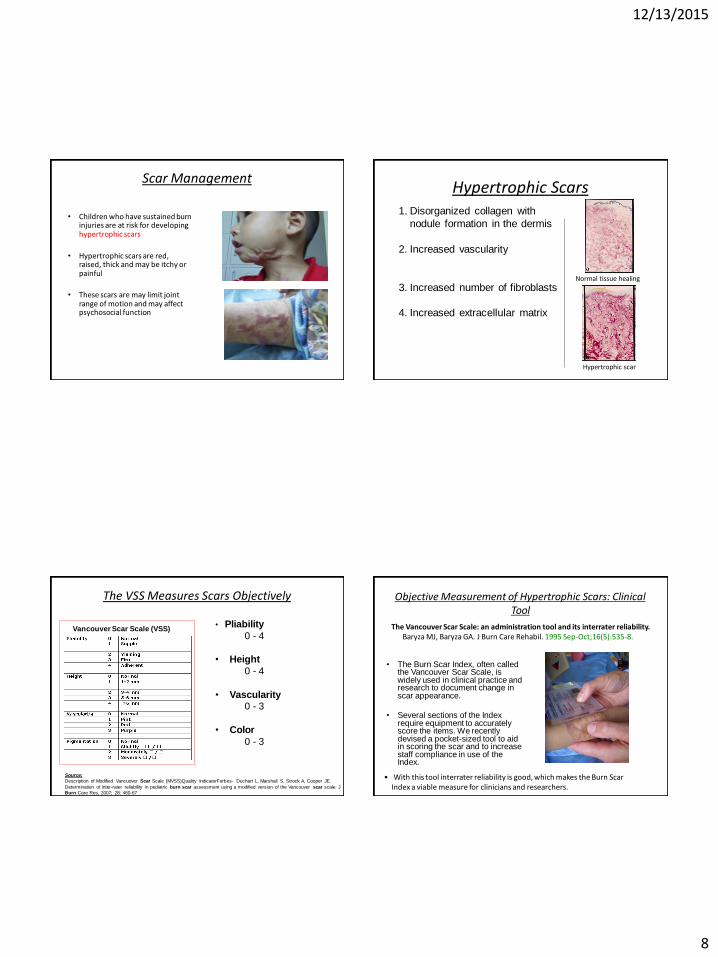
Scar Management
• Children who have sustained burn injuries are at risk for developing hypertrophic scars
• Hypertrophic scars are red, raised, thick and may be itchy or painful
• These scars are may limit joint range of motion and may affect psychosocial function
Hypertrophic Scars 1. Disorganized collagen with
nodule formation in the dermis
2. Increased vascularity
3. Increased number of fibroblasts
4. Increased extracellular matrix
Hypertrophic scar
Normal tissue healing
The VSS Measures Scars Objectively
Vancouver Scar Scale (VSS)
Source:
Description of Modified Vancuover Scar Scale (MVSS)Quality IndicatorForbes- Duchart L, Marshall S, Strock A, Cooper JE.
Determination of inter-rater reliability in pediatric burn scar assessment using a modified version of the Vancouver scar scale. J
Burn Care Res, 2007; 28: 460-67
• Pliability
0 - 4
• Height
0 - 4
• Vascularity 0 - 3
• Color
0 - 3
Objective Measurement of Hypertrophic Scars: Clinical Tool
The Vancouver Scar Scale: an administration tool and its interrater reliability. Baryza MJ, Baryza GA. J Burn Care Rehabil. 1995 Sep-Oct;16(5):535-8.
• The Burn Scar Index, often called the Vancouver Scar Scale, is widely used in clinical practice and research to document change in scar appearance.
• Several sections of the Index
require equipment to accurately score the items. We recently devised a pocket-sized tool to aid in scoring the scar and to increase staff compliance in use of the Index.
• With this tool interrater reliability is good, which makes the Burn Scar Index a viable measure for clinicians and researchers.
12/13/2015
9
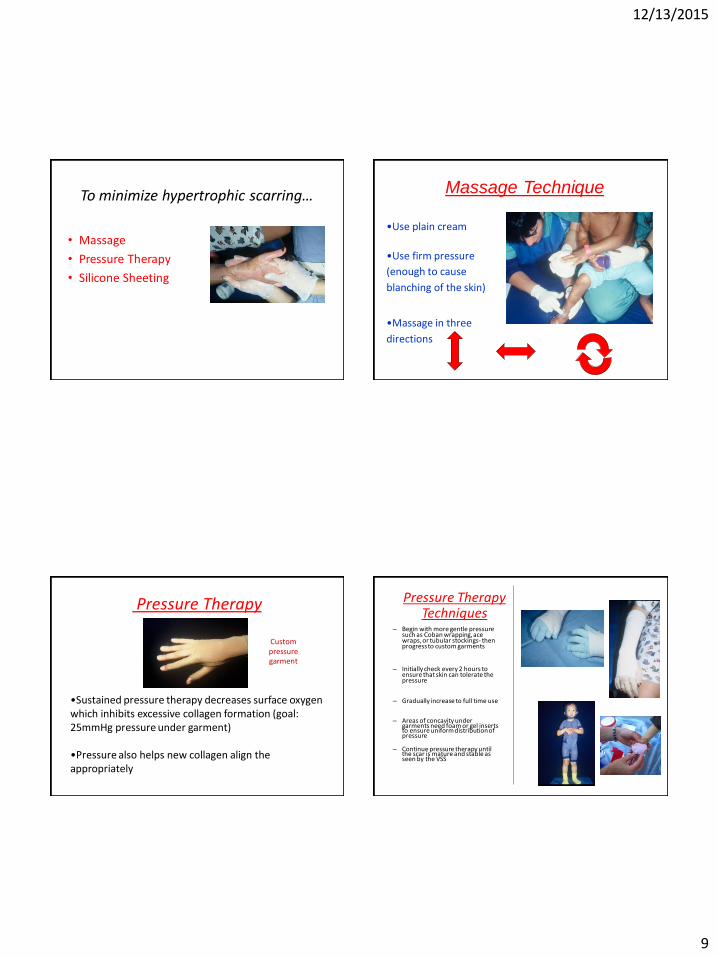
To minimize hypertrophic scarring…
• Massage
• Pressure Therapy
• Silicone Sheeting
•Use plain cream
•Use firm pressure
(enough to cause
blanching of the skin)
•Massage in three
directions
Massage Technique
Pressure Therapy
•Sustained pressure therapy decreases surface oxygen which inhibits excessive collagen formation (goal: 25mmHg pressure under garment)
•Pressure also helps new collagen align the appropriately
Custom pressure garment
– Begin with more gentle pressure such as Coban wrapping, ace wraps, or tubular stockings- then progress to custom garments
– Initially check every 2 hours to ensure that skin can tolerate the pressure
– Gradually increase to full time use
– Areas of concavity under
garments need foam or gel inserts to ensure uniform distribution of pressure
– Continue pressure therapy until the scar is mature and stable as seen by the VSS
Pressure Therapy Techniques
12/13/2015
10
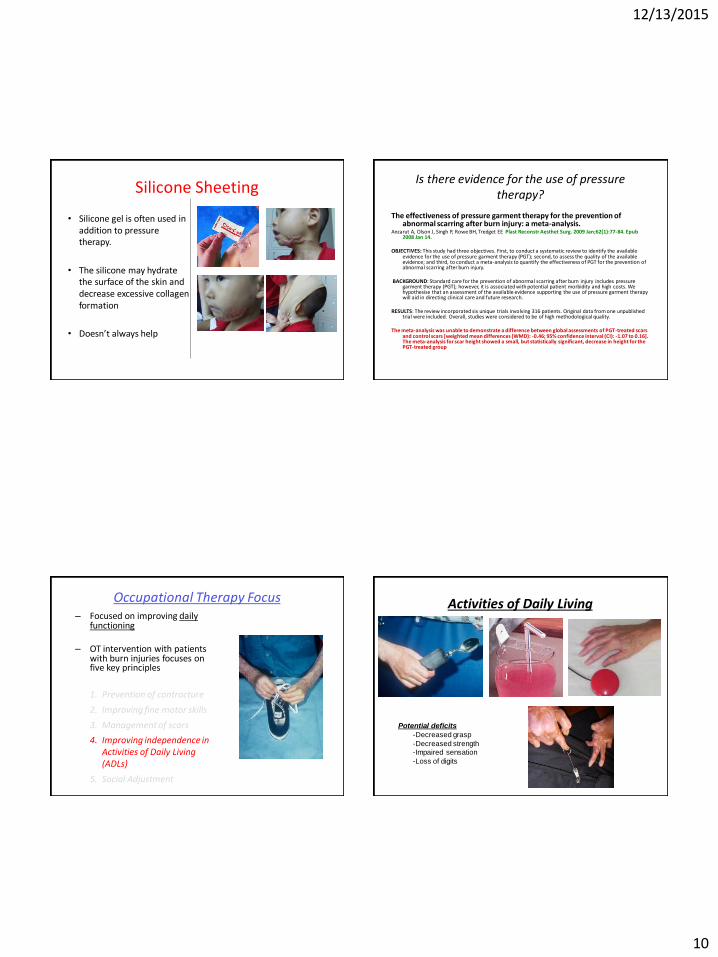
Silicone Sheeting
• Silicone gel is often used in addition to pressure therapy.
• The silicone may hydrate the surface of the skin and decrease excessive collagen formation
• Doesn’t always help
Is there evidence for the use of pressure therapy?
The effectiveness of pressure garment therapy for the prevention of abnormal scarring after burn injury: a meta-analysis.
Anzarut A, Olson J, Singh P, Rowe BH, Tredget EE Plast Reconstr Aesthet Surg. 2009 Jan;62(1):77-84. Epub 2008 Jan 14.
OBJECTIVES: This study had three objectives. First, to conduct a systematic review to identify the available
evidence for the use of pressure garment therapy (PGT); second, to assess the quality of the available evidence; and third, to conduct a meta-analysis to quantify the effectiveness of PGT for the prevention of abnormal scarring after burn injury.
BACKGROUND: Standard care for the prevention of abnormal scarring after burn injury includes pressure
garment therapy (PGT); however, it is associated with potential patient morbidity and high costs. We hypothesise that an assessment of the available evidence supporting the use of pressure garment therapy will aid in directing clinical care and future research.
RESULTS: The review incorporated six unique trials involving 316 patients. Original data from one unpublished
trial were included. Overall, studies were considered to be of high methodological quality. The meta-analysis was unable to demonstrate a difference between global assessments of PGT-treated scars
and control scars [weighted mean differences (WMD): -0.46; 95% confidence interval (CI): -1.07 to 0.16]. The meta-analysis for scar height showed a small, but statistically significant, decrease in height for the PGT-treated group
Occupational Therapy Focus – Focused on improving daily
functioning
– OT intervention with patients with burn injuries focuses on five key principles
1. Prevention of contracture
2. Improving fine motor skills
3. Management of scars
4. Improving independence in Activities of Daily Living (ADLs)
5. Social Adjustment
Activities of Daily Living
Potential deficits
-Decreased grasp
-Decreased strength
-Impaired sensation
-Loss of digits
12/13/2015
11
Occupational Therapy Focus – Focused on improving daily
functioning
– OT intervention with patients with burn injuries focuses on five key principles
1. Prevention of contracture
2. Improving fine motor skills
3. Management of scars
4. Improving independence in Activities of Daily Living (ADLs)
5. Social Adjustment
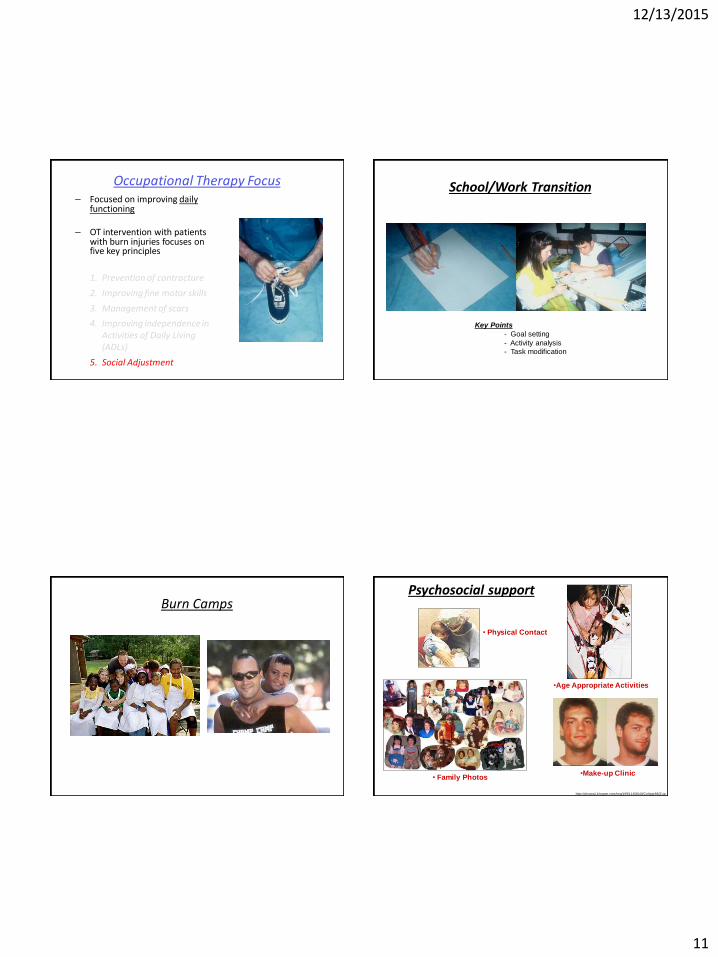
School/Work Transition
Key Points
- Goal setting
- Activity analysis
- Task modification
Burn Camps Psychosocial support
http://photos1.blogger.com/img/199/1160/640/Collage88(2).jp
• Physical Contact
• Family Photos
•Age Appropriate Activities
•Make-up Clinic

12/13/2015
12
Occupational Therapy Focus – Focused on improving daily
functioning
– OT intervention with patients with burn injuries focuses on five key principles
1. Prevention of contracture
2. Improving fine motor skills
3. Management of scars
4. Improving independence in Activities of Daily Living (ADLs)
5. Social Adjustment
謝謝 !
Email: [email protected]


![Woundedness and Transformation: Encountering Christ as the ...myocn.net/wp-content/uploads/2019/04/Woundedness-and-Transfor… · by His bruise [wounds] we are healed.” (Isaiah](https://img.pdfslide.net/doc/110x75/5f6abd9770f4670e05626bb2/woundedness-and-transformation-encountering-christ-as-the-myocnnetwp-contentuploads201904woundedness-and-transfor.jpg)