Embed Size (px)
Citation preview
E. Magnus Ohman, MD, FRCPI, FACCE. Magnus Ohman, MD, FRCPI, FACCProgram ChairmanProgram ChairmanProfessor of MedicineProfessor of Medicine
Director, Program for Advanced Coronary DiseaseDirector, Program for Advanced Coronary DiseaseDivision of CardiologyDivision of Cardiology
Duke University Medical CenterDuke University Medical CenterDurham, North CarolinaDurham, North Carolina
Critical Challenges in Critical Challenges in Cardiovascular MedicineCardiovascular Medicine
Translating Landmark Trials and AHA/ACC Guidelines Translating Landmark Trials and AHA/ACC Guidelines into the Front Lines of Cardiovascular Care for Acute, into the Front Lines of Cardiovascular Care for Acute,
Ischemic Heart DiseaseIschemic Heart Disease
Getting in the ACS (Up)Stream of ThingsGetting in the ACS (Up)Stream of Things
CME-accredited symposium jointly sponsored by the University of Massachusetts Medical School and CMEducation Resources, LLC
Commercial Support: Sponsored by an independent educational grant from The Medicines Company
Mission statement: Improve patient care through evidence-based education, expert analysis, and case study-based management
Processes: Strives for fair balance, clinical relevance, on-label indications for agents discussed, and emerging evidence and information from recent studies
COI: Full faculty disclosures provided in syllabus and at the beginning of the program
Welcome and Program OverviewWelcome and Program Overview
Program Educational ObjectivesProgram Educational Objectives
As a result of this educational activity, physicians will:As a result of this educational activity, physicians will:
► Learn to identify signs, symptoms, and prognostic features of acute Learn to identify signs, symptoms, and prognostic features of acute coronary syndrome (ACS) and related ischemic conditions, and their coronary syndrome (ACS) and related ischemic conditions, and their implications for invasive vascular management.implications for invasive vascular management.
► Learn how recently issued 2007 AHA/ACC Guidelines for UA/Non ST-Learn how recently issued 2007 AHA/ACC Guidelines for UA/Non ST-Elevation Myocardial Infarction are best applied to appropriately risk-Elevation Myocardial Infarction are best applied to appropriately risk-stratified patients with UA and NSTEMI.stratified patients with UA and NSTEMI.
► Learn to assess and implement optimal pharmacologic interventions, Learn to assess and implement optimal pharmacologic interventions, especially antithrombotic therapy, in the upstream setting, for patients especially antithrombotic therapy, in the upstream setting, for patients presenting with manifestations of UA, NSTEMI and related conditions.presenting with manifestations of UA, NSTEMI and related conditions.
► Learn to understand the implications of recent clinical data, trials, and Learn to understand the implications of recent clinical data, trials, and recommendations on switching antithrombotic therapy in patients who recommendations on switching antithrombotic therapy in patients who present with acute ischemic coronary syndromes, with an emphasis on present with acute ischemic coronary syndromes, with an emphasis on determining when switching from one agent to another is appropriate, determining when switching from one agent to another is appropriate, safe, and feasible; and, when switching among antithrombotic agents safe, and feasible; and, when switching among antithrombotic agents may be problematic.may be problematic.
Program Educational ObjectivesProgram Educational Objectives
As a result of this educational activity, physicians will:As a result of this educational activity, physicians will:
► Learn to characterize, identify, and evaluate the safety, efficacy, and Learn to characterize, identify, and evaluate the safety, efficacy, and side effects of myriad therapeutic options used for acute ischemic side effects of myriad therapeutic options used for acute ischemic coronary syndromes including: Aspirin, antiplatelet agents, direct coronary syndromes including: Aspirin, antiplatelet agents, direct thrombin inhibitors, UFH, LMWHs, and factor Xa inhibitors. thrombin inhibitors, UFH, LMWHs, and factor Xa inhibitors.
► Learn to understand the specific advantages and potential Learn to understand the specific advantages and potential disadvantages of pharmacologic agents currently used to reduce disadvantages of pharmacologic agents currently used to reduce ischemic and bleeding end points in the setting of cardiovascular ischemic and bleeding end points in the setting of cardiovascular emergencies.emergencies.
► Learn to identify the ideal properties of antithrombotic agents used in Learn to identify the ideal properties of antithrombotic agents used in conjunction with stent insertion.conjunction with stent insertion.
► Learn to discuss and assess the impact that new trials and Year 2007 Learn to discuss and assess the impact that new trials and Year 2007 AHA/ACC Guidelines are likely to have on future invasive management AHA/ACC Guidelines are likely to have on future invasive management of patients with UA and NSTEMI.of patients with UA and NSTEMI.
► Learn to apply national guidelines and expert, consensus-based Learn to apply national guidelines and expert, consensus-based recommendations in order to optimize invasive vascular management recommendations in order to optimize invasive vascular management of patients with acute, ischemic heart disease.of patients with acute, ischemic heart disease.
Program FacultyProgram Faculty
Program ChairmanProgram ChairmanE. Magnus Ohman, MD, E. Magnus Ohman, MD, FRCPI, FACCFRCPI, FACCProfessor of MedicineProfessor of MedicineDirector, Program for Advanced Coronary Director, Program for Advanced Coronary DiseaseDiseaseDivision of CardiologyDivision of CardiologyDuke University Medical CenterDuke University Medical CenterDurham, North CarolinaDurham, North Carolina
Distinguished FacultyDistinguished FacultyC. Michael Gibson, MS, MDC. Michael Gibson, MS, MDDirector, TIMI Core Laboratories and Data Director, TIMI Core Laboratories and Data Coordinating CenterCoordinating CenterAssociate Professor Associate Professor Harvard Medical SchoolHarvard Medical SchoolBoston, MassachusettsBoston, Massachusetts
A. Michael Lincoff, MDA. Michael Lincoff, MDVice Chairman for ResearchVice Chairman for ResearchDepartment of Cardiovascular MedicineDepartment of Cardiovascular MedicineDirector, Cleveland Clinic CardiovascularDirector, Cleveland Clinic CardiovascularCoordinating CenterCoordinating CenterProfessor of MedicineProfessor of MedicineCleveland Clinic Lerner College of Medicine of Cleveland Clinic Lerner College of Medicine of Case Western Reserve UniversityCase Western Reserve UniversityThe Cleveland Clinic FoundationThe Cleveland Clinic FoundationCleveland, Ohio Cleveland, Ohio
Charles V. Pollack Jr, MA, MD, Charles V. Pollack Jr, MA, MD, FACEP, FAAEMFACEP, FAAEMChairman, Department of Emergency MedicineChairman, Department of Emergency MedicinePennsylvania HospitalPennsylvania HospitalProfessor of Emergency MedicineProfessor of Emergency MedicineUniversity of Pennsylvania School of MedicineUniversity of Pennsylvania School of MedicinePhiladelphia, Pennsylvania Philadelphia, Pennsylvania
Faculty COI DisclosuresFaculty COI Disclosures
E. Magnus Ohman, MD, FRCPI, FACCE. Magnus Ohman, MD, FRCPI, FACCResearch Grants: Berlex, sanofi-aventis, Schering-Plough Corporation, Bristol Meyer Squibb, and Millennium. Stockholder: Medtronic. Consultant: Response Biomedical, Liposcience, and Inovise Medical
C. Michael Gibson, MS, MDC. Michael Gibson, MS, MDPresent Research/Grant Funding:Present Research/Grant Funding: CardioKinetix, Eli Lilly, KAI Pharmaceuticals, CardioKinetix, Eli Lilly, KAI Pharmaceuticals, Nuvelo, Schering Plough Corporation, Sanofi-Aventis, St. Jude Medical, Baxter, Nuvelo, Schering Plough Corporation, Sanofi-Aventis, St. Jude Medical, Baxter, Novartis, FoldRx, INO Therapeutics, LLCNovartis, FoldRx, INO Therapeutics, LLCSpeakers Bureau:Speakers Bureau: Genentech, Inc., GlaxoSmithKline, Schering Plough Corporation, Genentech, Inc., GlaxoSmithKline, Schering Plough Corporation, The Medicines CompanyThe Medicines CompanyConsultant:Consultant: Angel Medical Systems, The Medicines Company. HeartScape Angel Medical Systems, The Medicines Company. HeartScape Technologies, Inc., Ascenta Therapeutics, Inc., Archemix Corp., PDL Technologies, Inc., Ascenta Therapeutics, Inc., Archemix Corp., PDL Pharmaceuticals, Atrium Medical Corporation, TIMI3 Systems, Biogen IDECPharmaceuticals, Atrium Medical Corporation, TIMI3 Systems, Biogen IDEC
Charles V. Pollack Jr, MA, MD, FACEP, FAAEMCharles V. Pollack Jr, MA, MD, FACEP, FAAEMGrant/Research Support: GlaxoSmithKlineConsultant: The Medicines Co., Schering-Plough, Sanofi-Aventis, BMS, GenentechSpeaker’s Bureau: Schering-Plough, Sanofi-Aventis, BMS, Genentech
► AbraxisAbraxis► Alexion PharmaAlexion Pharma► AstraZenecaAstraZeneca► AtherogenicsAtherogenics► AventisAventis► Biosense WebsterBiosense Webster► BiositeBiosite► Boehringer IngelheimBoehringer Ingelheim► Boston ScientificBoston Scientific► Bristol-Myers Squibb (BMS)Bristol-Myers Squibb (BMS)► CardionetCardionet► CentocorCentocor► Converge Medical Inc.Converge Medical Inc.► CordisCordis► Dr. Reddy’s LaboratoryDr. Reddy’s Laboratory► NovartisNovartis► Novo NordiskNovo Nordisk► Orphan TherapeuticsOrphan Therapeutics► P&G PharmaP&G Pharma► PfizerPfizer► RocheRoche► SankyoSankyo► Sanofi-AventisSanofi-Aventis► Schering-PloughSchering-Plough► SciosScios► St. Jude MedicalSt. Jude Medical► TakedaTakeda► VasoGenixVasoGenix► ViacorViacor
► Edwards Lifesciences Edwards Lifesciences ► EsperionEsperion► GE MedicalGE Medical► GenentechGenentech► GilfordGilford► GSKGSK► GuidantGuidant► J&JJ&J► Kensey-NashKensey-Nash► LillyLilly► Medicines CompanyMedicines Company► MedtronicMedtronic► MerckMerck► MytogenMytogen► NovartisNovartis► Novo NordiskNovo Nordisk► Orphan TherapeuticsOrphan Therapeutics► P&G PharmaP&G Pharma► PfizerPfizer► RocheRoche► SankyoSankyo► Sanofi-AventisSanofi-Aventis► Schering-PloughSchering-Plough► SciosScios► St. Jude MedicalSt. Jude Medical► TakedaTakeda► VasoGenixVasoGenix► ViacorViacor
► NovartisNovartis► Novo NordiskNovo Nordisk► Orphan TherapeuticsOrphan Therapeutics► P&G PharmaP&G Pharma► PfizerPfizer► RocheRoche► SankyoSankyo► Sanofi-AventisSanofi-Aventis► Schering-PloughSchering-Plough► SciosScios► St. Jude MedicalSt. Jude Medical► TakedaTakeda► VasoGenixVasoGenix► ViacorViacor
A. Michael Lincoff, MD Relationships with Industry Research Sponsors A. Michael Lincoff, MD Relationships with Industry Research Sponsors C5ResearchC5Research
Faculty COI DisclosuresFaculty COI Disclosures
Critical Challenges in Acute Ischemic Heart Disease — Overview
Where Metal Meets Thrombus, Drugs, and Vascular Endothelium: A State of the “Union” Synthesis
E. Magnus Ohman MD, FRCPI, FACC Program Chairman
Professor of Medicine | Director, Program for Advanced Coronary Disease | Professor of Medicine | Director, Program for Advanced Coronary Disease | Division of Cardiology | Duke University Medical Center | Division of Cardiology | Duke University Medical Center |
Durham, North CarolinaDurham, North Carolina
Getting in the ACS (Up)Stream of ThingsGetting in the ACS (Up)Stream of Things
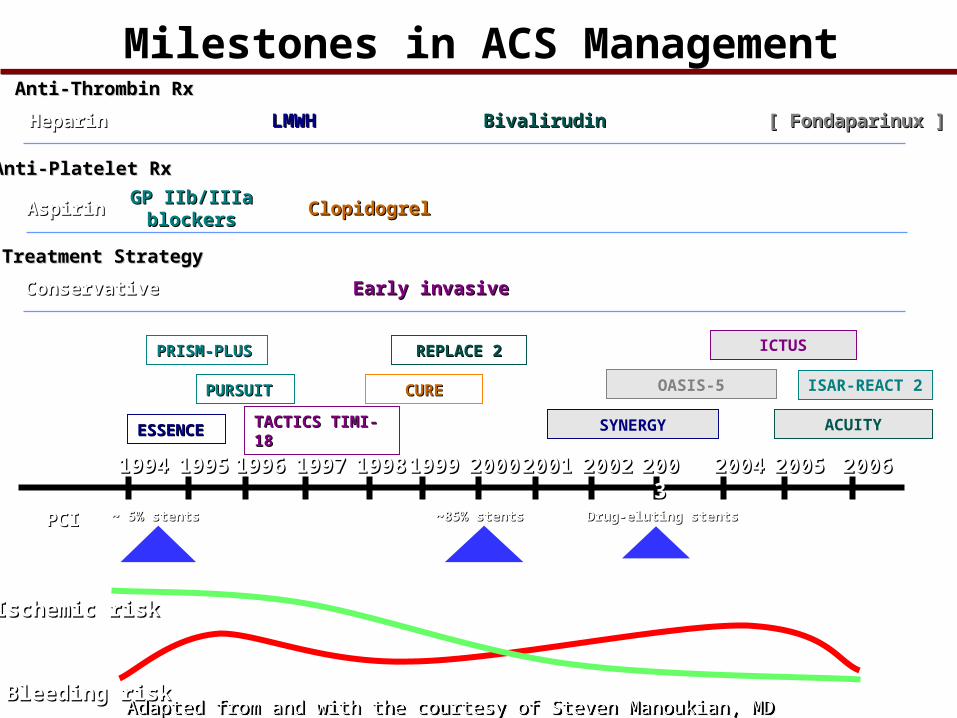
SYNERGY
LMWHLMWH
ESSENCEESSENCE
19941994 19951995 19961996 19971997 19981998 19991999 20002000 20022002 20032003 20042004 20052005 2006200620012001
CURECURE
ClopidogrelClopidogrel
Bleeding riskBleeding risk
Ischemic riskIschemic risk
GP IIb/IIIa GP IIb/IIIa blockersblockers
PRISM-PLUSPRISM-PLUS
PURSUITPURSUIT
ACUITYTACTICS TIMI-18TACTICS TIMI-18
Early invasiveEarly invasive
PCIPCI ~ 5% stents~ 5% stents ~85% stents~85% stents Drug-eluting stentsDrug-eluting stents
ISAR-REACT 2
Milestones in ACS Management
OASIS-5
[ Fondaparinux ][ Fondaparinux ]Anti-Thrombin RxAnti-Thrombin Rx
Anti-Platelet RxAnti-Platelet Rx
Treatment StrategyTreatment Strategy
HeparinHeparin
AspirinAspirin
ConservativeConservative
ICTUS
BivalirudinBivalirudin
REPLACE 2REPLACE 2
Adapted from and with the courtesy of Steven Manoukian, MDAdapted from and with the courtesy of Steven Manoukian, MD
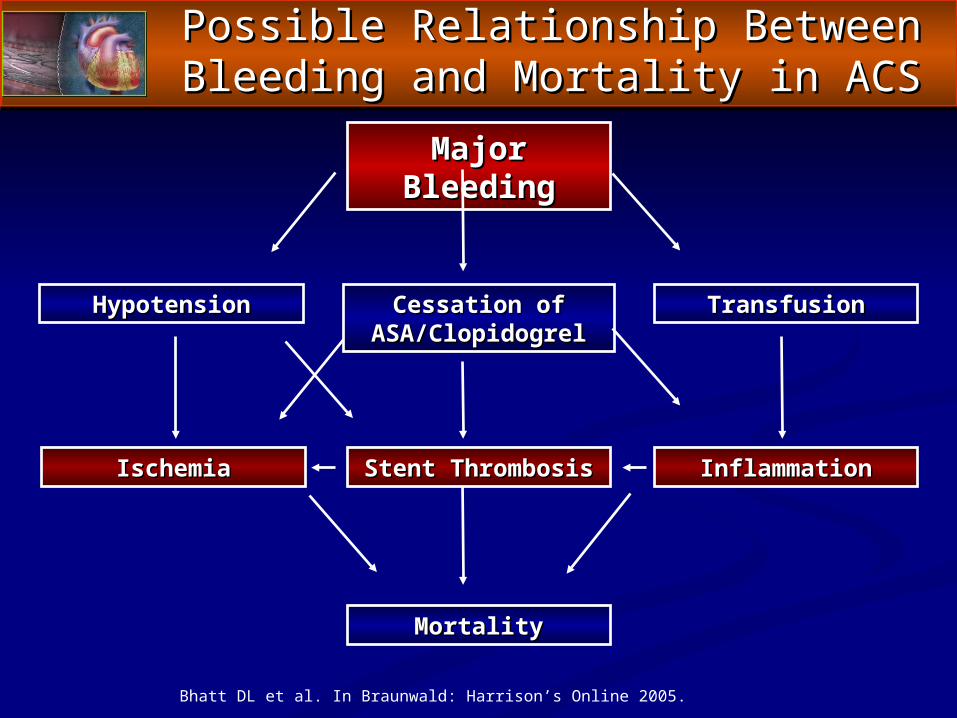
MortalityMortality
Major BleedingMajor Bleeding
TransfusionTransfusionHypotensionHypotension Cessation of Cessation of ASA/ClopidogrelASA/Clopidogrel
IschemiaIschemia Stent ThrombosisStent Thrombosis InflammationInflammation
Bhatt DL et al. In Braunwald: Harrison’s Online 2005.
Possible Relationship BetweenPossible Relationship BetweenBleeding and Mortality in ACSBleeding and Mortality in ACS
Issues We Will Address TonightIssues We Will Address Tonight
• • GUIDELINESGUIDELINES — Do we need them? If so, why? In what — Do we need them? If so, why? In what situations? And how do we adapt to new evidence presented situations? And how do we adapt to new evidence presented after guidelines are released?after guidelines are released?
• • UPSTREAM THERAPY—UPSTREAM THERAPY—How do we identify optimal How do we identify optimal strategies?strategies?
• • COLLABORATIONCOLLABORATION—How do we facilitate collaboration —How do we facilitate collaboration among ED physicians and CV specialists?among ED physicians and CV specialists?
• • CASE STUDIES—CASE STUDIES—Translating science and evidence to Translating science and evidence to practice practice
Getting in the ACS (Up)Stream of ThingsGetting in the ACS (Up)Stream of Things
THE BIG PICTURE: EARLY INVASIVE VS. THE BIG PICTURE: EARLY INVASIVE VS. INITIAL CONSERVATIVE THERAPYINITIAL CONSERVATIVE THERAPY
““An early invasive strategy (i.e., diagnostic angiography with intent to perform An early invasive strategy (i.e., diagnostic angiography with intent to perform revascularization) is indicated in initially stabilized UA/NSTEMI patients revascularization) is indicated in initially stabilized UA/NSTEMI patients (without serious comorbidities or contraindications to such procedures) (without serious comorbidities or contraindications to such procedures) who who have an elevated risk for clinical eventshave an elevated risk for clinical events.”.”
““In initially stabilized patients, an In initially stabilized patients, an initially conservative (i.e., a selectively initially conservative (i.e., a selectively invasive) strategy may be consideredinvasive) strategy may be considered as a treatment strategy for UA/NSTEMI as a treatment strategy for UA/NSTEMI patients (without serious comorbidities or contraindications to such patients (without serious comorbidities or contraindications to such procedures) who have an elevated risk for clinical events, procedures) who have an elevated risk for clinical events, including those who including those who are troponin positiveare troponin positive.”.”
““The decision to implement an initial conservative (vs. initial invasive) strategy The decision to implement an initial conservative (vs. initial invasive) strategy in these patients may be made by in these patients may be made by considering physician and patient considering physician and patient preferencepreference.” .”
UA/NSTEMI Strategy OverviewUA/NSTEMI Strategy Overview
ACC/AHA 2007 Guidelines for the Management of UA/NSTEMI. August 6, 2007, ACC/AHA 2007 Guidelines for the Management of UA/NSTEMI. August 6, 2007, Circulation.Circulation.
BIG PICTURE: ANTIPLATELET AGENTSBIG PICTURE: ANTIPLATELET AGENTS
““Support for thienopyridine use (primarily with clopidogrel) Support for thienopyridine use (primarily with clopidogrel) continues to grow, including higher loading-dose options, continues to grow, including higher loading-dose options, earlier (upstream) administrationearlier (upstream) administration, and longer administration , and longer administration (especially after drug-eluting stent placement).” (especially after drug-eluting stent placement).”
““The question of how best to integrate thienopyridine use with The question of how best to integrate thienopyridine use with parenteral glycoprotein (GP) IIb/IIIa antagonists to provide parenteral glycoprotein (GP) IIb/IIIa antagonists to provide optimal antiplatelet therapy early in the course of UA/NSTEMI optimal antiplatelet therapy early in the course of UA/NSTEMI therapy, including cardiac catheterization, therapy, including cardiac catheterization, is an evolving areais an evolving area.”.”
UA/NSTEMI Strategy OverviewUA/NSTEMI Strategy Overview
ACC/AHA 2007 Guidelines for the Management of UA/NSTEMI. August 6, 2007, Circulation.
BIG PICTURE: ANTICOAGULANTSBIG PICTURE: ANTICOAGULANTS
““Two new anticoagulants, Two new anticoagulants, fondaparinux and bivalirudinfondaparinux and bivalirudin, , have undergone have undergone favorable testing in clinical trialsfavorable testing in clinical trials and and are recommendedare recommended as alternatives to unfractionated as alternatives to unfractionated heparin (UFH) and low-molecular-weight heparins heparin (UFH) and low-molecular-weight heparins (LMWHs) for specific or more general applications.”(LMWHs) for specific or more general applications.”
ACC/AHA 2007 Guidelines for the Management of UA/NSTEMI. August 6, 2007, Circulation.
UA/NSTEMI Strategy OverviewUA/NSTEMI Strategy Overview
PIVOTAL TRIALSPIVOTAL TRIALSSnapshot of Trial Results that Supported Addition Snapshot of Trial Results that Supported Addition
of Bivalirudin and Fondaparinux to Year 2007 of Bivalirudin and Fondaparinux to Year 2007 AHA/ACC UA/NSTEMI GuidelinesAHA/ACC UA/NSTEMI Guidelines
ACC/AHA 2007 Guidelines for the Management of UA/NSTEMI. August 6, 2007, Circulation.
UA/NSTEMI Pivotal TrialsUA/NSTEMI Pivotal Trials
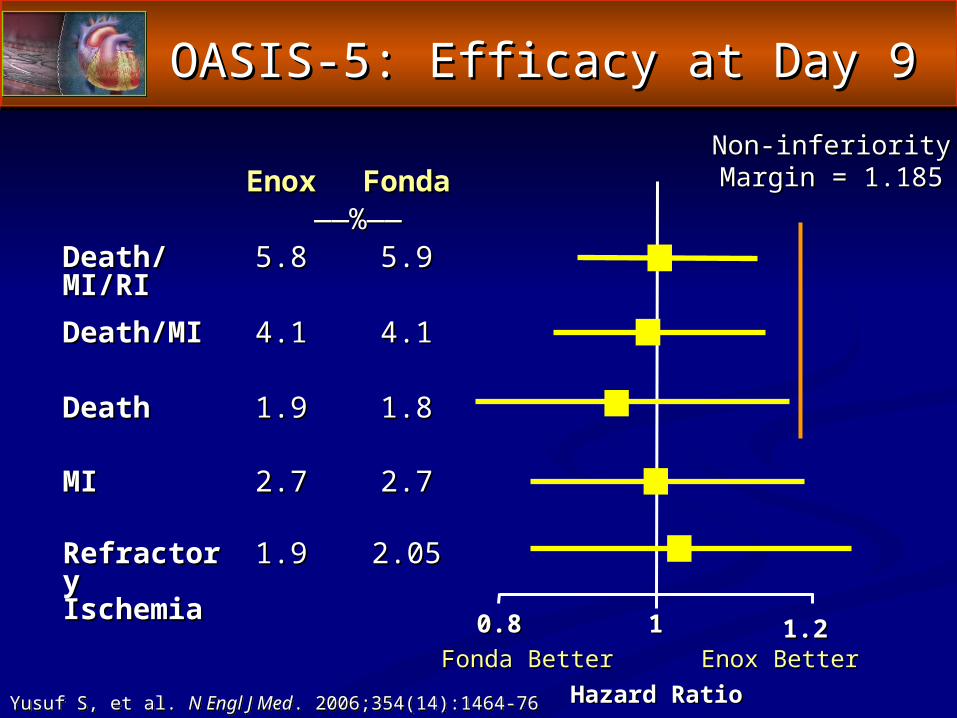
OASIS-5: Efficacy at Day 9OASIS-5: Efficacy at Day 9
EnoxEnox FondaFonda————%——%——
Death/MI/RIDeath/MI/RI 5.85.8 5.95.9
Death/MIDeath/MI 4.14.1 4.14.1
DeathDeath 1.91.9 1.81.8
MIMI 2.72.7 2.72.7
Refractory Refractory IschemiaIschemia
1.91.9 2.052.05
0.80.8 11 1.21.2
Non-inferiorityNon-inferiorityMargin = 1.185Margin = 1.185
Hazard RatioHazard RatioFonda BetterFonda Better Enox BetterEnox Better
Yusuf S, et al. N Engl J Med. 2006;354(14):1464-76
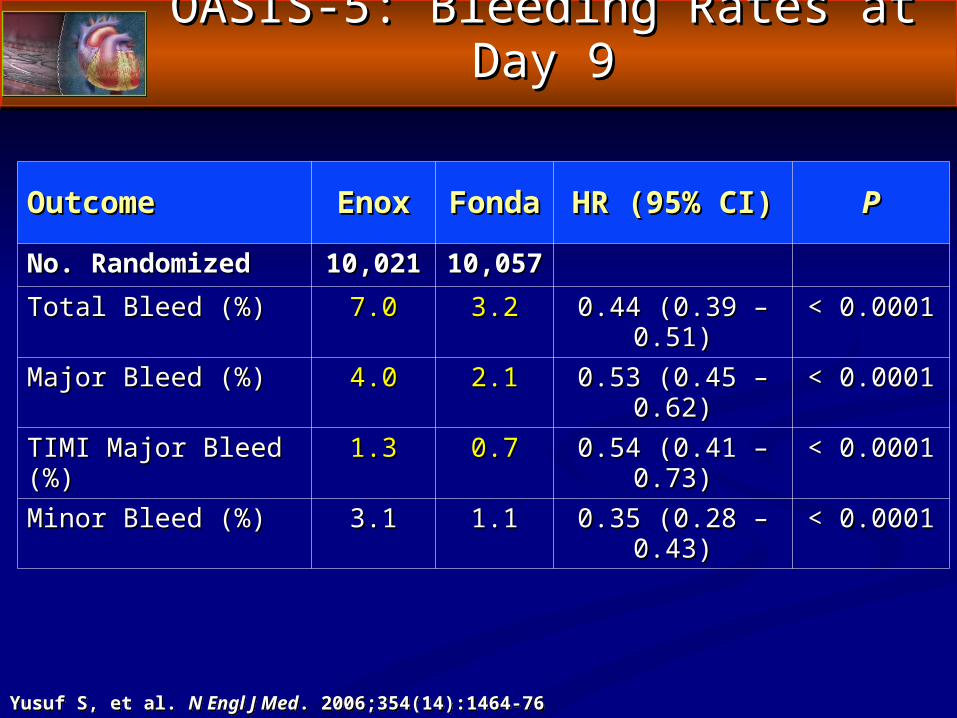
OASIS-5: Bleeding Rates at Day 9OASIS-5: Bleeding Rates at Day 9
OutcomeOutcome EnoxEnox FondaFonda HR (95% CI)HR (95% CI) PP
No. RandomizedNo. Randomized 10,02110,021 10,05710,057Total Bleed (%)Total Bleed (%) 7.07.0 3.23.2 0.44 (0.39 – 0.51)0.44 (0.39 – 0.51) < 0.0001< 0.0001
Major Bleed (%)Major Bleed (%) 4.04.0 2.12.1 0.53 (0.45 – 0.62)0.53 (0.45 – 0.62) < 0.0001< 0.0001
TIMI Major Bleed (%)TIMI Major Bleed (%) 1.31.3 0.70.7 0.54 (0.41 – 0.73)0.54 (0.41 – 0.73) < 0.0001< 0.0001
Minor Bleed (%)Minor Bleed (%) 3.13.1 1.11.1 0.35 (0.28 – 0.43)0.35 (0.28 – 0.43) < 0.0001< 0.0001
Yusuf S, et al. N Engl J Med. 2006;354(14):1464-76
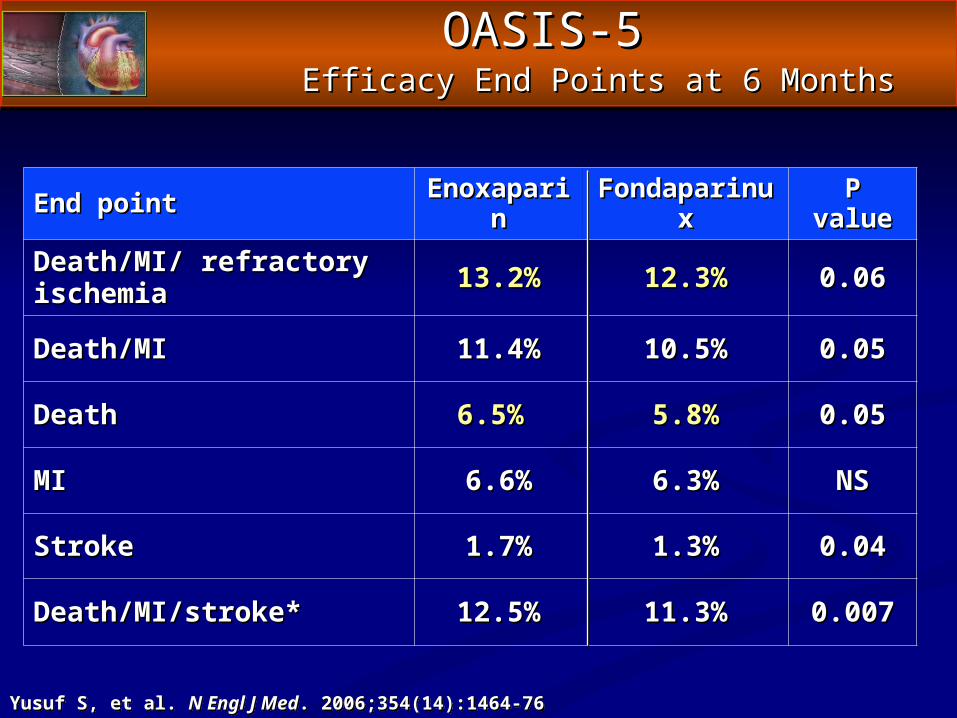
OASIS-5OASIS-5 Efficacy End Points at 6 MonthsEfficacy End Points at 6 Months
End point End point EnoxaparinEnoxaparin FondaparinuxFondaparinux P valueP value
Death/MI/ refractory Death/MI/ refractory ischemia ischemia 13.2%13.2% 12.3%12.3% 0.060.06
Death/MI Death/MI 11.4%11.4% 10.5%10.5% 0.050.05
Death Death 6.5% 6.5% 5.8%5.8% 0.050.05
MI MI 6.6%6.6% 6.3%6.3% NSNS
Stroke Stroke 1.7%1.7% 1.3%1.3% 0.040.04
Death/MI/stroke*Death/MI/stroke* 12.5%12.5% 11.3%11.3% 0.0070.007
Yusuf S, et al. N Engl J Med. 2006;354(14):1464-76
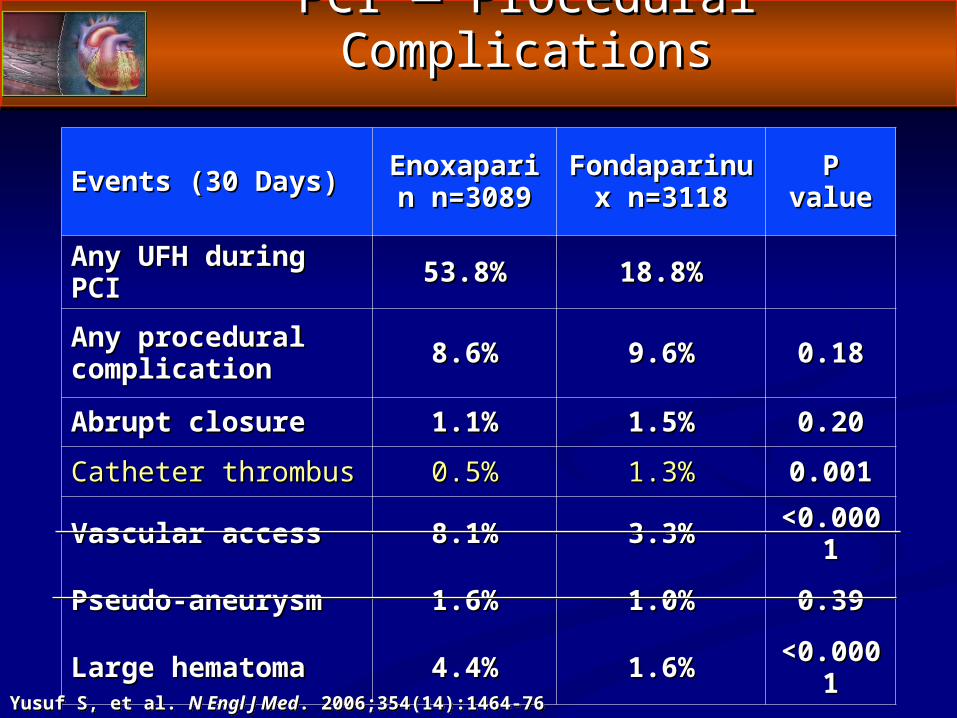
PCI — Procedural ComplicationsPCI — Procedural Complications
Events (30 Days)Events (30 Days) Enoxaparin Enoxaparin n=3089n=3089
Fondaparinux Fondaparinux n=3118n=3118 P valueP value
Any UFH during PCI Any UFH during PCI 53.8%53.8% 18.8%18.8%
Any procedural Any procedural complication complication 8.6%8.6% 9.6%9.6% 0.180.18
Abrupt closureAbrupt closure 1.1%1.1% 1.5%1.5% 0.200.20
Catheter thrombus Catheter thrombus 0.5%0.5% 1.3%1.3% 0.0010.001
Vascular access Vascular access 8.1%8.1% 3.3%3.3% <0.0001<0.0001
Pseudo-aneurysmPseudo-aneurysm 1.6%1.6% 1.0%1.0% 0.390.39
Large hematomaLarge hematoma 4.4%4.4% 1.6%1.6% <0.0001<0.0001
Yusuf S, et al. N Engl J Med. 2006;354(14):1464-76
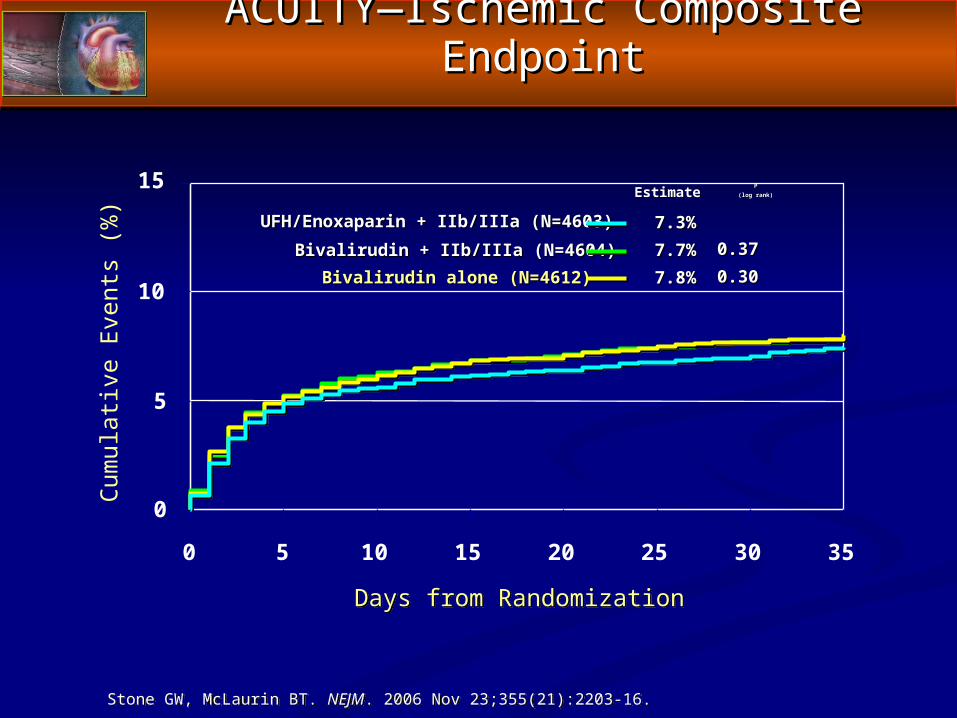
ACUITY—Ischemic Composite EndpointACUITY—Ischemic Composite Endpoint
0
5
10
15
0 5 10 15 20 25 30 35
Cum
ulat
ive
Eve
nts
(%)
Days from Randomization
EstimateEstimate PP(log rank)(log rank)
7.3%7.3%UFH/Enoxaparin + IIb/IIIa (N=4603)UFH/Enoxaparin + IIb/IIIa (N=4603)Bivalirudin + IIb/IIIa (N=4604)Bivalirudin + IIb/IIIa (N=4604) 0.370.377.7%7.7%
Bivalirudin alone (N=4612)Bivalirudin alone (N=4612) 0.300.307.8%7.8%
Stone GW, McLaurin BT. NEJM. 2006 Nov 23;355(21):2203-16.
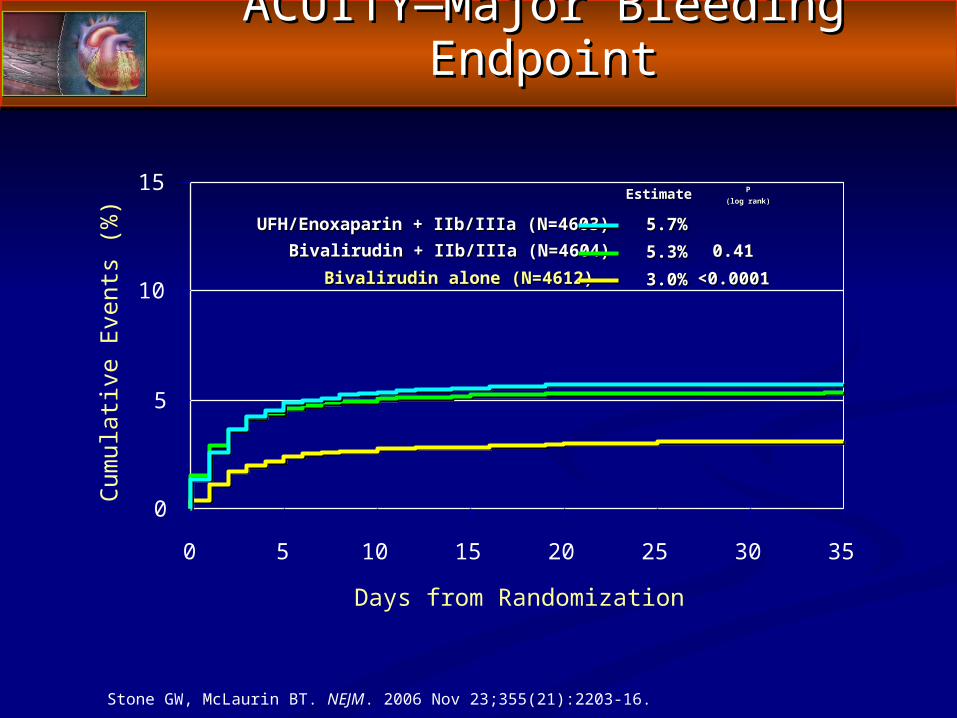
ACUITY—Major Bleeding EndpointACUITY—Major Bleeding Endpoint
0
5
10
15
0 5 10 15 20 25 30 35
Cum
ulat
ive
Eve
nts
(%)
Days from Randomization
EstimateEstimate PP(log rank)(log rank)
5.7%5.7%UFH/Enoxaparin + IIb/IIIa (N=4603)UFH/Enoxaparin + IIb/IIIa (N=4603)Bivalirudin + IIb/IIIa (N=4604)Bivalirudin + IIb/IIIa (N=4604) 0.410.415.3%5.3%
Bivalirudin alone (N=4612Bivalirudin alone (N=4612)) <0.0001<0.00013.0%3.0%
Stone GW, McLaurin BT. NEJM. 2006 Nov 23;355(21):2203-16.
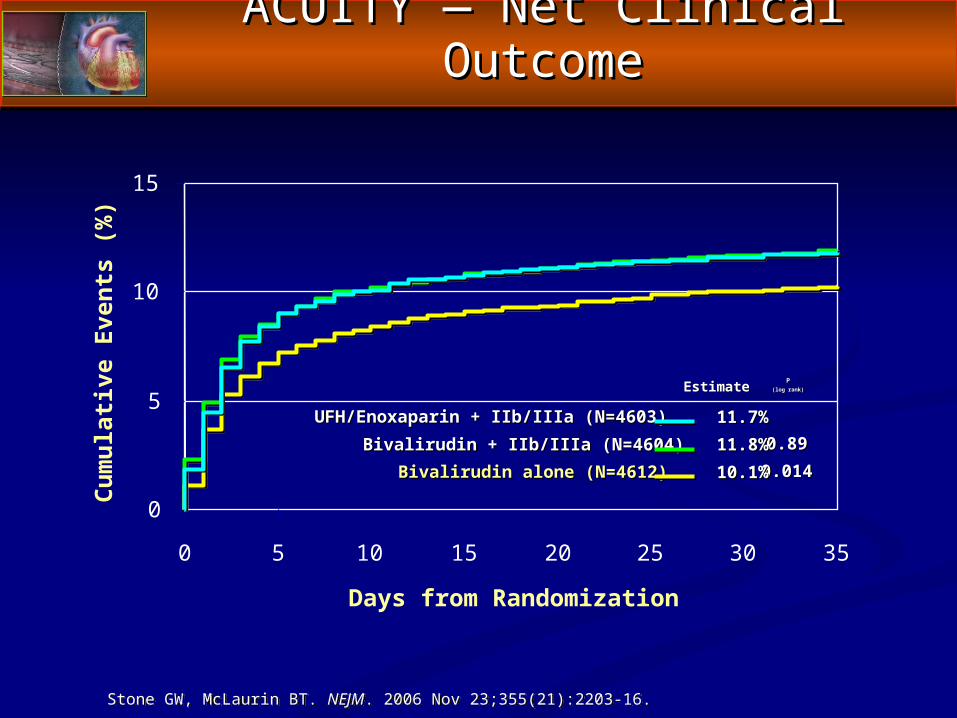
ACUITY — Net Clinical OutcomeACUITY — Net Clinical Outcome
0
5
10
15
0 5 10 15 20 25 30 35
Cum
ulat
ive
Even
ts (%
)
Days from Randomization
EstimateEstimate PP(log rank)(log rank)
11.7%11.7%UFH/Enoxaparin + IIb/IIIa (N=4603)UFH/Enoxaparin + IIb/IIIa (N=4603)Bivalirudin + IIb/IIIa (N=4604)Bivalirudin + IIb/IIIa (N=4604) 0.890.8911.8%11.8%
Bivalirudin alone (N=4612)Bivalirudin alone (N=4612) 0.0140.01410.1%10.1%
Stone GW, McLaurin BT. NEJM. 2006 Nov 23;355(21):2203-16.
0 30 60 90 120 150 180 210 240 270 300 330 360 3900
4
5
Mor
talit
y (%
)
Days from Randomization
2
1
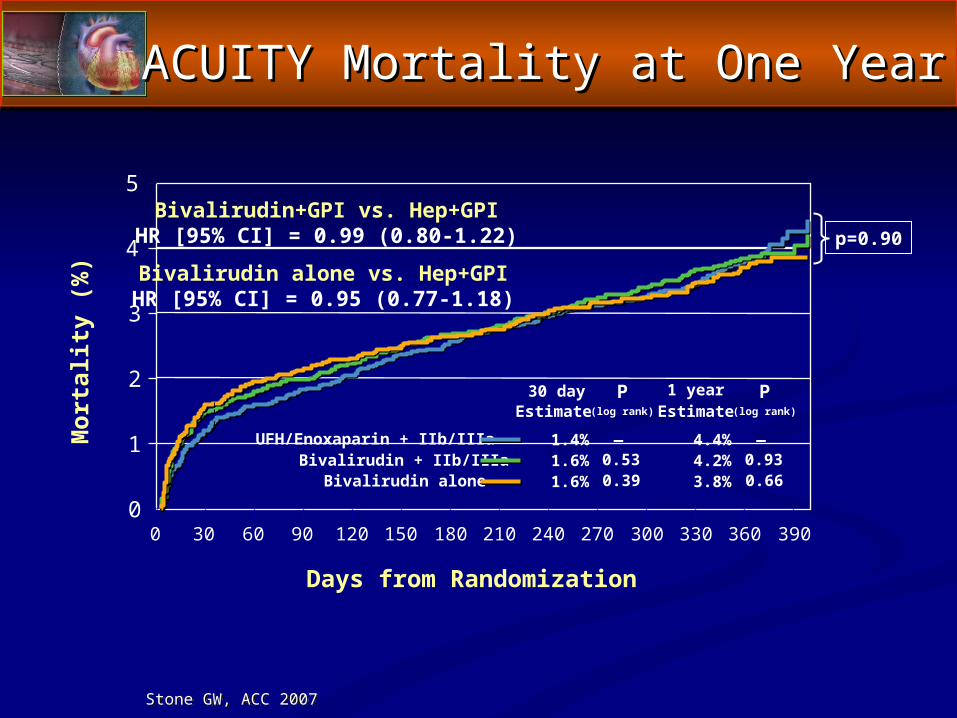
ACUITY Mortality at One YearACUITY Mortality at One Year
UFH/Enoxaparin + IIb/IIIaBivalirudin + IIb/IIIa
Bivalirudin alone
EstimateP
(log rank)
1.4%0.531.6%0.391.6%
—
EstimateP
(log rank)
4.4%0.934.2%0.663.8%
1 year
—
p=0.90Bivalirudin+GPI vs. Hep+GPIHR [95% CI] = 0.99 (0.80-1.22)
30 day
3
Bivalirudin alone vs. Hep+GPIHR [95% CI] = 0.95 (0.77-1.18)
Stone GW, ACC 2007
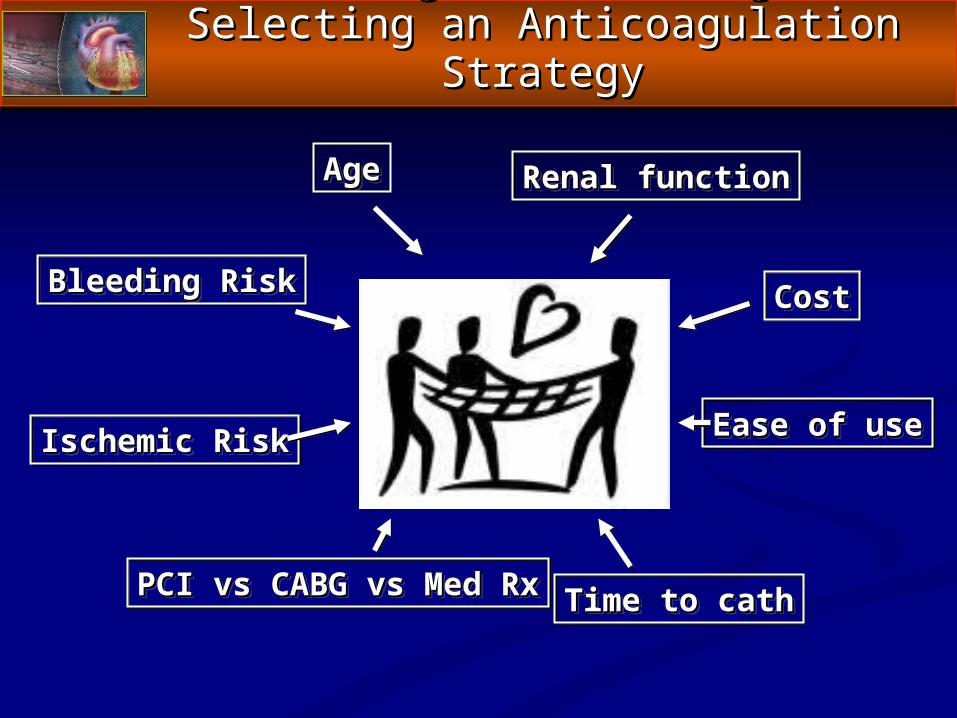
Addressing the Challenge of Addressing the Challenge of Selecting an Anticoagulation StrategySelecting an Anticoagulation Strategy
Bleeding RiskBleeding Risk
Ischemic RiskIschemic Risk
Renal functionRenal functionAgeAge
Time to cathTime to cath
CostCost
Ease of useEase of use
PCI vs CABG vs Med RxPCI vs CABG vs Med Rx
Sea and Stream Changes in ACSSea and Stream Changes in ACS► The 2007 Guidelines have created a “Sea Change” in The 2007 Guidelines have created a “Sea Change” in
the care of patients with UA/NSTEMIthe care of patients with UA/NSTEMI
New “Streams” of care, with new anticoagulants, New “Streams” of care, with new anticoagulants, are in playare in play
Clopidogrel use has been liberalizedClopidogrel use has been liberalized
Bleeding end points play a more important role in Bleeding end points play a more important role in drug selectiondrug selection
Dogmatism is out, customization is inDogmatism is out, customization is in
Collaboration is emphasizedCollaboration is emphasized
C. Michael Gibson, M.S., M.D., FACCC. Michael Gibson, M.S., M.D., FACCDirector, TIMI Core Laboratories and Data Coordinating CenterDirector, TIMI Core Laboratories and Data Coordinating Center
Associate Professor, Harvard Medical SchoolAssociate Professor, Harvard Medical SchoolBoston, MassachusettsBoston, Massachusetts
Getting in the Stream(s) of Antithrombotic Getting in the Stream(s) of Antithrombotic Therapy for ACS: Therapy for ACS:
What Do The Trials Tell Us?What Do The Trials Tell Us?
To Switch or Not to Switch —To Switch or Not to Switch —If, When, How, To What?If, When, How, To What?
Getting in the ACS Stream of ThingsGetting in the ACS Stream of Things
Overview of PresentationOverview of Presentation
► Mechanistic rational for switchingMechanistic rational for switching► Why is there a concern about switching Why is there a concern about switching
antithrombins in patients with ACS (lessons from antithrombins in patients with ACS (lessons from SYNERGY) SYNERGY)
► Why should switching to bivalirudin for PCI be Why should switching to bivalirudin for PCI be reasonable?reasonable?
► Clinical evidence in support of switchingClinical evidence in support of switching SWITCHSWITCH REPLACE 2REPLACE 2 ACUITYACUITY
Background — Issues and ConcernsBackground — Issues and Concerns
► ACS patientsACS patients 87% of patients receive either UFH, enoxaparin, or fondaparinux 87% of patients receive either UFH, enoxaparin, or fondaparinux
within 24 hours after admissionwithin 24 hours after admission11
72% of patients in SYNERGY and 50 % of patients in OASIS- 572% of patients in SYNERGY and 50 % of patients in OASIS- 5
received prior antithrombinreceived prior antithrombin2,32,3
► Published studies and perceptionsPublished studies and perceptions Patients in SYNERGY who crossed over between UFH and Patients in SYNERGY who crossed over between UFH and
enoxaparin had an increase in bleeding complicationsenoxaparin had an increase in bleeding complications22
• This activity occurred at various times through the study period: At This activity occurred at various times through the study period: At times in response to clinical or clinician perceptiontimes in response to clinical or clinician perception
Consistent therapy is betterConsistent therapy is better44
1 CRUSADE( 1Q-2006 results); 2 SYNERGY results; JAMA 2004; 3 OASIS -5; Yusuf et al,NEJM 2006; 4 Cohen et al, JACC 2006.
Bivalirudin: A Guidelines-Supported Bivalirudin: A Guidelines-Supported Alternative to UFH/LMWH in ACSAlternative to UFH/LMWH in ACS
► Advantages of the direct thrombin inhibitor Advantages of the direct thrombin inhibitor bivalirudinbivalirudin No requirement for antithrombin IIINo requirement for antithrombin III Effective on clot-bound thrombinEffective on clot-bound thrombin Inhibits thrombin-mediated platelet activationInhibits thrombin-mediated platelet activation No interactions with PF- 4No interactions with PF- 4 Plasma half-life 25 minutesPlasma half-life 25 minutes No requirement for anticoagulant monitoringNo requirement for anticoagulant monitoring
► Clinical results with bivalirudin in PCIClinical results with bivalirudin in PCI Similar protection from ischemic events as UFH + GP IIb/IIIa Similar protection from ischemic events as UFH + GP IIb/IIIa
inhibitors, with markedly reduced bleedinginhibitors, with markedly reduced bleeding11
► Not previously tested in contemporary ACS patientsNot previously tested in contemporary ACS patients
REPLACE 2. Lincoff AM et al. JAMA 2003;289:853-863.
Switching Antithrombins: SYNERGYSwitching Antithrombins: SYNERGY
► The The SYNERGYSYNERGY trial suggested a switch in trial suggested a switch in anthithrombins (from heparin to LMWH) can lead anthithrombins (from heparin to LMWH) can lead to increase in bleeding. to increase in bleeding.
► What outcomes are observed when switching What outcomes are observed when switching from from heparin, LMWH, or fondaparinux to bivalirudin in heparin, LMWH, or fondaparinux to bivalirudin in PCI?PCI?
► Is it better to switch or to stay on consistent Is it better to switch or to stay on consistent therapy?therapy?
Switching from Enoxaparin to Bivalirudin in Patients Switching from Enoxaparin to Bivalirudin in Patients with Acute Coronary Syndromes Without ST-with Acute Coronary Syndromes Without ST-segment Elevation Undergoing Percutaneous segment Elevation Undergoing Percutaneous
Coronary Intervention (PCI)Coronary Intervention (PCI)
Ron Waksman, MD, FACC, FSCAIRon Waksman, MD, FACC, FSCAIAssociate Director Division of CardiologyAssociate Director Division of Cardiology
Washington Hospital CenterWashington Hospital CenterWashington, DCWashington, DC
The study was sponsored in part by The Medicines Company
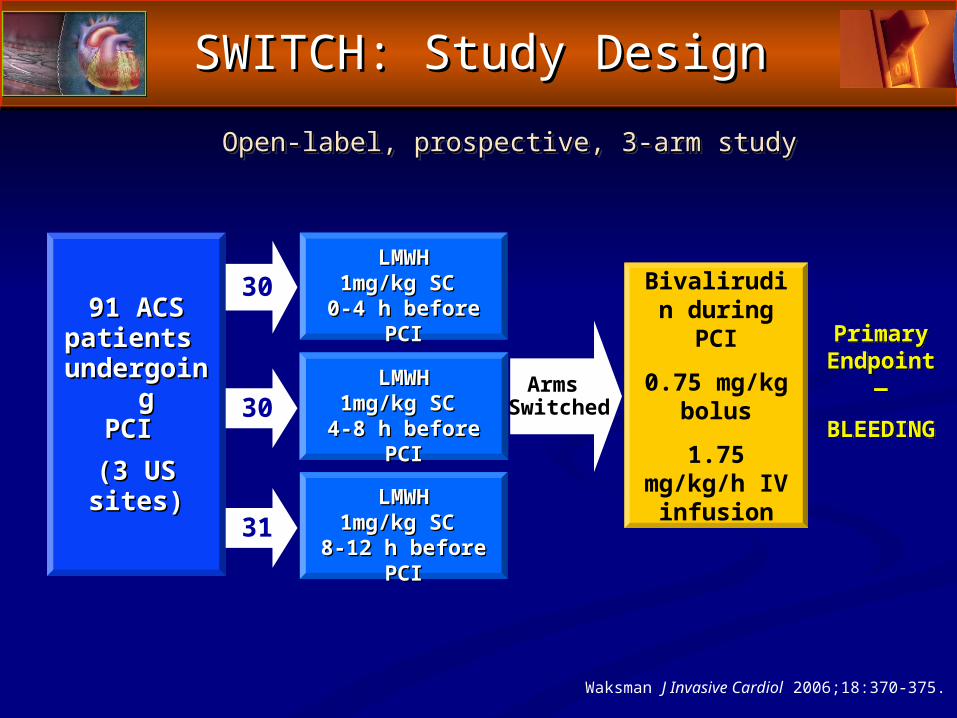
The SWITCH StudyThe SWITCH Study
31
30
30Primary
Endpoint —
BLEEDING
91 ACS91 ACSpatients patients
undergoing undergoing PCI PCI
(3 US(3 USsites)sites)
Open-label, prospective, 3-arm studyOpen-label, prospective, 3-arm study
LMWHLMWH1mg/kg SC 1mg/kg SC
0-4 h before PCI0-4 h before PCI
LMWHLMWH1mg/kg SC 1mg/kg SC
4-8 h before PCI4-8 h before PCI
LMWHLMWH1mg/kg SC 1mg/kg SC
8-12 h before8-12 h before PCI PCI
Bivalirudin during PCI
0.75 mg/kg bolus
1.75 mg/kg/h IV infusion
Arms Switched
SWITCH: Study DesignSWITCH: Study Design
Waksman J Invasive Cardiol 2006;18:370-375.
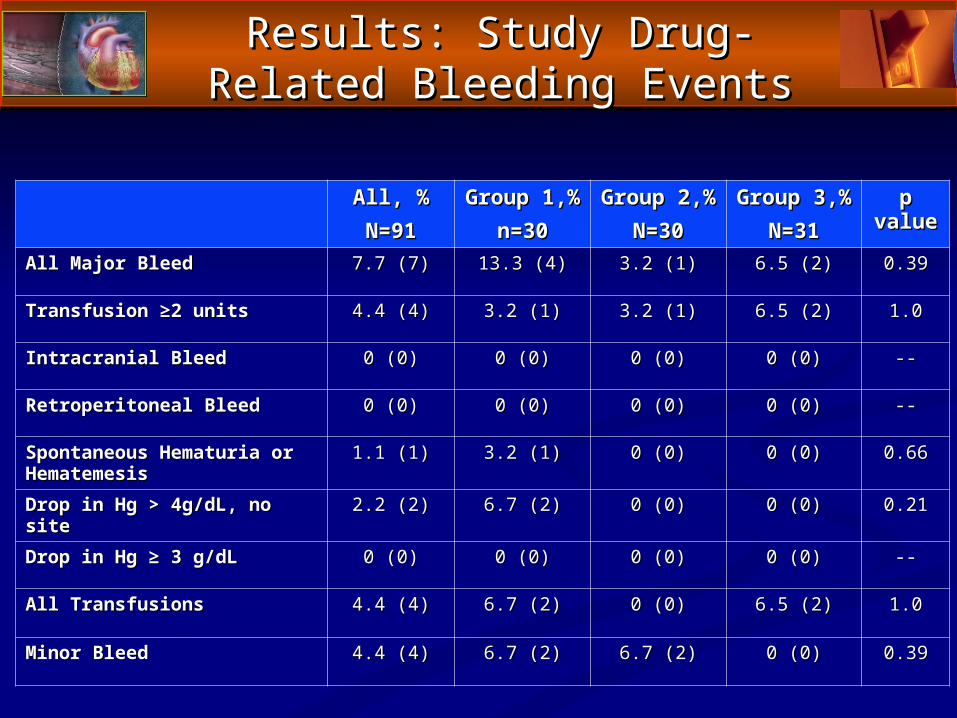
Results: Study Drug-Related Results: Study Drug-Related Bleeding EventsBleeding Events
All, %All, %N=91N=91
Group 1,%Group 1,%n=30n=30
Group 2,%Group 2,%N=30N=30
Group 3,%Group 3,%N=31N=31
p p valuevalue
All Major BleedAll Major Bleed 7.7 (7)7.7 (7) 13.3 (4) 13.3 (4) 3.2 (1)3.2 (1) 6.5 (2)6.5 (2) 0.390.39
Transfusion ≥2 units Transfusion ≥2 units 4.4 (4)4.4 (4) 3.2 (1)3.2 (1) 3.2 (1)3.2 (1) 6.5 (2)6.5 (2) 1.01.0
Intracranial BleedIntracranial Bleed 0 (0)0 (0) 0 (0)0 (0) 0 (0)0 (0) 0 (0)0 (0) ----
Retroperitoneal BleedRetroperitoneal Bleed 0 (0)0 (0) 0 (0)0 (0) 0 (0)0 (0) 0 (0)0 (0) ----
Spontaneous Hematuria or Spontaneous Hematuria or HematemesisHematemesis
1.1 (1)1.1 (1) 3.2 (1)3.2 (1) 0 (0)0 (0) 0 (0)0 (0) 0.660.66
Drop in Hg > 4g/dL, no siteDrop in Hg > 4g/dL, no site 2.2 (2)2.2 (2) 6.7 (2)6.7 (2) 0 (0)0 (0) 0 (0)0 (0) 0.210.21
Drop in Hg ≥ 3 g/dLDrop in Hg ≥ 3 g/dL 0 (0)0 (0) 0 (0)0 (0) 0 (0)0 (0) 0 (0)0 (0) ----
All TransfusionsAll Transfusions 4.4 (4)4.4 (4) 6.7 (2)6.7 (2) 0 (0)0 (0) 6.5 (2)6.5 (2) 1.01.0
Minor BleedMinor Bleed 4.4 (4)4.4 (4) 6.7 (2)6.7 (2) 6.7 (2)6.7 (2) 0 (0)0 (0) 0.390.39
SWITCH: ConclusionsSWITCH: Conclusions
► Switching from LMWH to bivalirudin during Switching from LMWH to bivalirudin during PCI for patients with ACS was safe PCI for patients with ACS was safe
► Switching was not associated with major Switching was not associated with major bleeding complications regardless of when bleeding complications regardless of when LMWH was administeredLMWH was administered
► The use of bivalirudin as the sole antithrombin The use of bivalirudin as the sole antithrombin agent during PCI can be extended for patients agent during PCI can be extended for patients who were pretreated with enoxaparin 8 hours who were pretreated with enoxaparin 8 hours post the last dose of LMWHpost the last dose of LMWH
Association of Pre-Randomization Anticoagulant Association of Pre-Randomization Anticoagulant Switching with Bleeding in the Setting of Percutaneous Switching with Bleeding in the Setting of Percutaneous
Coronary Intervention: A REPLACE-2 AnalysisCoronary Intervention: A REPLACE-2 Analysis
The goal of this analysis was to evaluate whether a The goal of this analysis was to evaluate whether a hazard existed when either UFH or LMWH were hazard existed when either UFH or LMWH were
administered prior to study medication in the administered prior to study medication in the REPLACE-2 trialREPLACE-2 trial
C. Michael Gibson, Yuli Ten, Sabina A. Murphy, Lauren N. Ciaglo, Matthew C. Southard, A. Michael Lincoff, and Ron Waksman
Gibson CM, Am J Cardiol. 2007 Jun 15;99(12):1687-90.
REPLACE-2 Trial: Impact of REPLACE-2 Trial: Impact of Antithrombin SwitchingAntithrombin Switching
Pre-Randomization Anticoagulant Pre-Randomization Anticoagulant Switching and BleedingSwitching and Bleeding
The present study compared bleeding The present study compared bleeding among patients treated either with among patients treated either with
preceding antithrombin therapy or no preceding antithrombin therapy or no preceding antithrombin therapy in the preceding antithrombin therapy in the
prior 48 hours.prior 48 hours.
Gibson CM, Am J Cardiol. 2007 Jun 15;99(12):1687-90.
The method of switching or transition involved The method of switching or transition involved administration of bivalirudin as follows:administration of bivalirudin as follows:
>8 hours after last low molecular weight heparin >8 hours after last low molecular weight heparin (LMWH) dose (LMWH) dose
OROR> 6 hours after unfractionated heparin, unless in the case > 6 hours after unfractionated heparin, unless in the case of UFH therapy the activated partial thromboplastin time of UFH therapy the activated partial thromboplastin time was ≤ 50 seconds or the activated clotting time was ≤ was ≤ 50 seconds or the activated clotting time was ≤ 175 seconds175 seconds
Pre-Randomization Anticoagulant Pre-Randomization Anticoagulant Switching and BleedingSwitching and Bleeding
Gibson CM, Am J Cardiol. 2007 Jun 15;99(12):1687-90.
VariableVariableNaive→ Naive→
BIV*BIV*(n=2,345)(n=2,345)
UFH→UFH→BIVBIV
(n=287)(n=287)
LMWH→LMWH→BIVBIV
(n=258)(n=258)
Naive→Naive→GP IIbIIIaGP IIbIIIa
/UFH/UFH(n=2,325)(n=2,325)
UFH→UFH→GPGPIIbIIIa/IIbIIIa/UFHUFH
(n=349)(n=349)
LMWH→LMWH→GP GP IIbIIIa/UIIbIIIa/U
FHFH(n=313)(n=313)
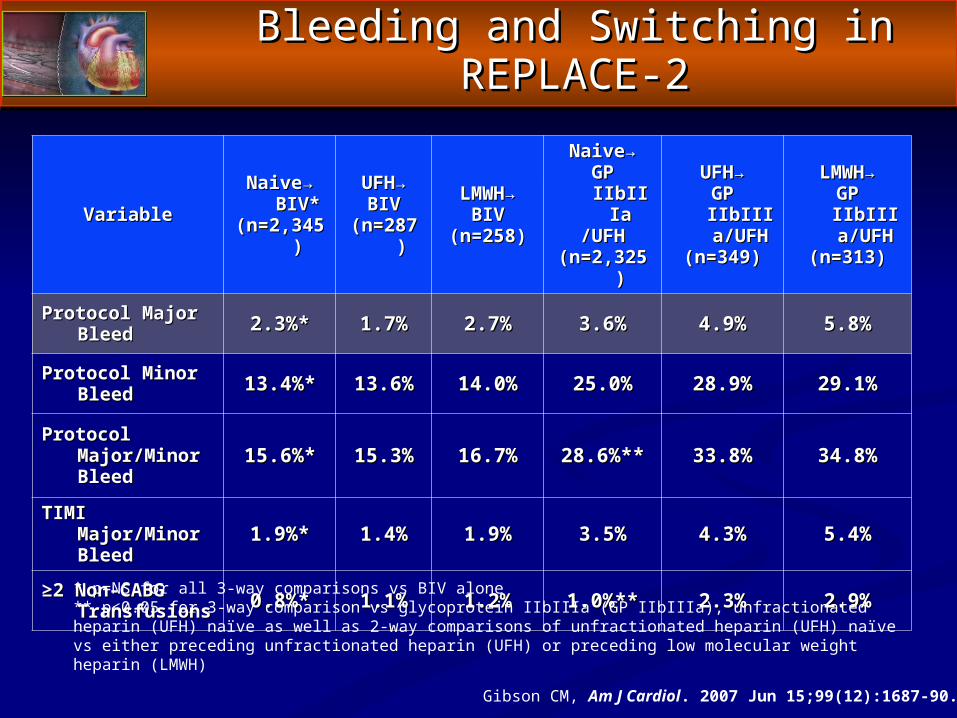
Protocol Major Protocol Major BleedBleed 2.3%*2.3%* 1.7%1.7% 2.7%2.7% 3.6%3.6% 4.9%4.9% 5.8%5.8%
Protocol Minor Protocol Minor BleedBleed 13.4%*13.4%* 13.6%13.6% 14.0%14.0% 25.0%25.0% 28.9%28.9% 29.1%29.1%
Protocol Protocol Major/Minor Major/Minor BleedBleed
15.6%*15.6%* 15.3%15.3% 16.7%16.7% 28.6%**28.6%** 33.8%33.8% 34.8%34.8%
TIMI Major/Minor TIMI Major/Minor BleedBleed 1.9%*1.9%* 1.4%1.4% 1.9%1.9% 3.5%3.5% 4.3%4.3% 5.4%5.4%
≥≥2 Non-CABG 2 Non-CABG TransfusionsTransfusions 0.8%*0.8%* 1.1%1.1% 1.2%1.2% 1.0%**1.0%** 2.3%2.3% 2.9%2.9%
Bleeding and Switching in REPLACE-2Bleeding and Switching in REPLACE-2
* p=NS for all 3-way comparisons vs BIV alone** p<0.05 for 3-way comparison vs glycoprotein IIbIIIa (GP IIbIIIa), unfractionated heparin (UFH) naïve as well as 2-way comparisons of unfractionated heparin (UFH) naïve vs either preceding unfractionated heparin (UFH) or preceding low molecular weight heparin (LMWH)
Gibson CM, Am J Cardiol. 2007 Jun 15;99(12):1687-90.
0.0
0.5
1.0
0 6 12 18 24 30 36 42 48
Frac
tion
of P
atie
nts
with
hou
rs <
X ax
is
Time to PCI (hours)
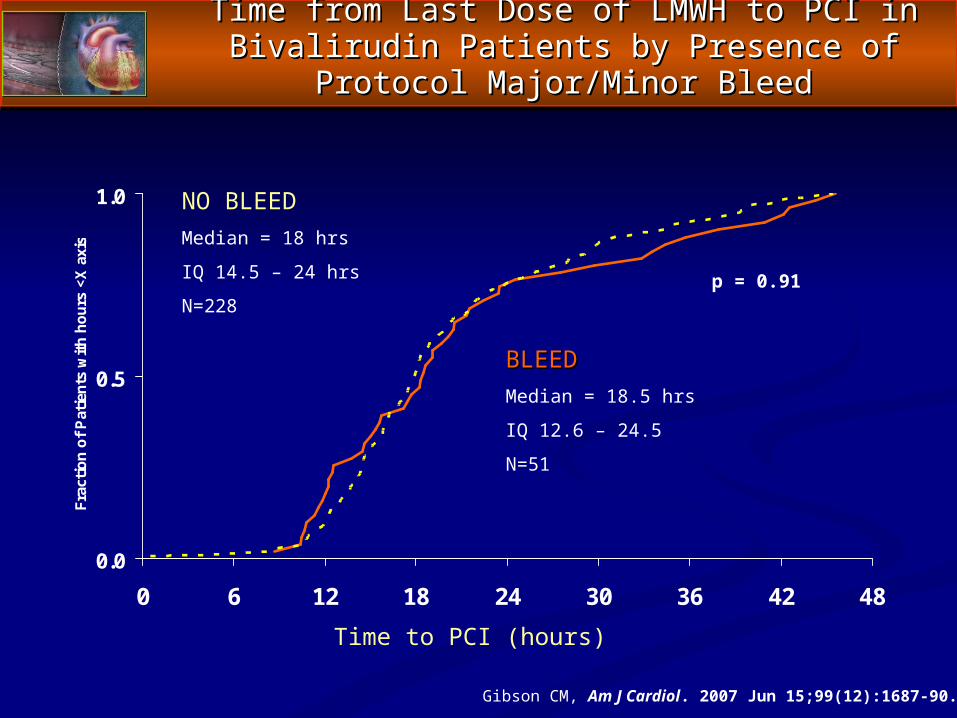
NO BLEEDMedian = 18 hrs
IQ 14.5 – 24 hrs
N=228
Time from Last Dose of LMWH to PCI in Bivalirudin Time from Last Dose of LMWH to PCI in Bivalirudin Patients by Presence of Protocol Major/Minor BleedPatients by Presence of Protocol Major/Minor Bleed
BLEEDBLEEDMedian = 18.5 hrs
IQ 12.6 – 24.5
N=51
p = 0.91
Gibson CM, Am J Cardiol. 2007 Jun 15;99(12):1687-90.
SwitchingSwitching and One Year Mortality and One Year Mortality
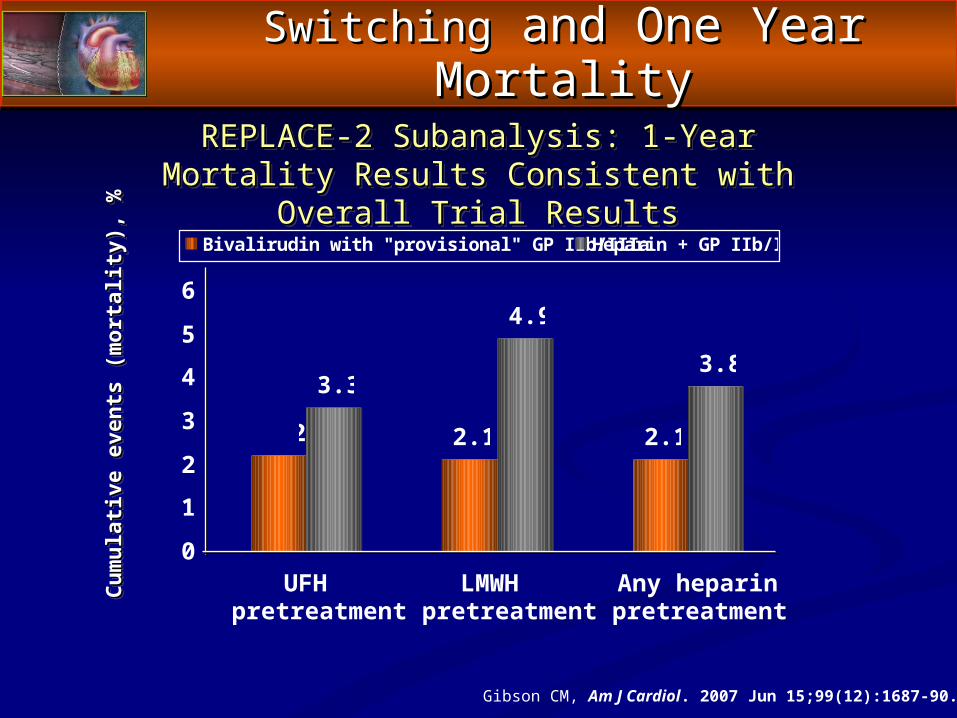
2.2 2.1 2.1
3.3
4.9
3.8
0
1
2
3
4
5
6
UFHpretreatment
LMWHpretreatment
Any heparinpretreatment
Bivalirudin with "provisional" GP IIb/IIIa Heparin + GP IIb/IIIa
Cum
ulat
ive
even
ts (m
orta
lity)
, %C
umul
ativ
e ev
ents
(mor
talit
y), %
REPLACE-2 Subanalysis: 1-Year Mortality Results REPLACE-2 Subanalysis: 1-Year Mortality Results Consistent with Overall Trial ResultsConsistent with Overall Trial Results
Gibson CM, Am J Cardiol. 2007 Jun 15;99(12):1687-90.
Pre-Randomization Anticoagulant Pre-Randomization Anticoagulant Switching and BleedingSwitching and Bleeding
► When switching to bivalirudin was undertaken in When switching to bivalirudin was undertaken in this fashion, preceding therapy with either LMWH this fashion, preceding therapy with either LMWH or UFH was or UFH was notnot associated with an excess of associated with an excess of bleeding or transfusions compared with bivalirudin bleeding or transfusions compared with bivalirudin therapy alone in the cardiac catheterization therapy alone in the cardiac catheterization laboratory.laboratory.
Gibson CM, Am J Cardiol. 2007 Jun 15;99(12):1687-90.
How to Switch — Science to PracticeHow to Switch — Science to Practice
From UFH to Bivalirudin —
• Discontinue UFH for 30 minutes before starting bivalirudin for PCI
From LMWH to Bivalirudin —
• Discontinue LMWH for 8 hours before starting bivalirudin for PCI
Gibson CM, Am J Cardiol. 2007 Jun 15;99(12):1687-90.
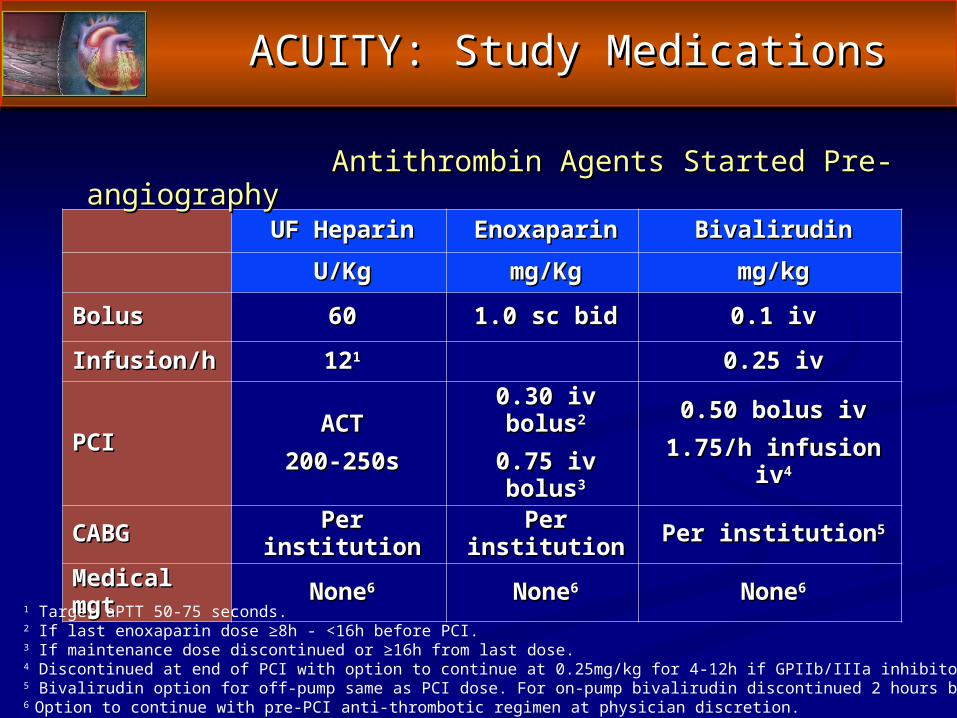
UF HeparinUF Heparin EnoxaparinEnoxaparin BivalirudinBivalirudin
U/KgU/Kg mg/Kgmg/Kg mg/kgmg/kg
BolusBolus 6060 1.0 sc bid1.0 sc bid 0.1 iv0.1 iv
Infusion/hInfusion/h 121211 0.25 iv0.25 iv
PCIPCIACTACT
200-250s200-250s0.30 iv bolus0.30 iv bolus22
0.75 iv bolus0.75 iv bolus33
0.50 bolus iv0.50 bolus iv1.75/h infusion iv1.75/h infusion iv44
CABGCABG Per institutionPer institution Per institutionPer institution Per institutionPer institution55
Medical mgtMedical mgt NoneNone66 NoneNone66 NoneNone66
ACUITY: Study MedicationsACUITY: Study Medications
Antithrombin Agents Started Pre-angiographyAntithrombin Agents Started Pre-angiography
1 Target aPTT 50-75 seconds.2 If last enoxaparin dose ≥8h - <16h before PCI.3 If maintenance dose discontinued or ≥16h from last dose.4 Discontinued at end of PCI with option to continue at 0.25mg/kg for 4-12h if GPIIb/IIIa inhibitor not used.5 Bivalirudin option for off-pump same as PCI dose. For on-pump bivalirudin discontinued 2 hours before.6 Option to continue with pre-PCI anti-thrombotic regimen at physician discretion.
Switching Hypothesis and QuestionSwitching Hypothesis and Question
► Hypothesis:Hypothesis: Bivalirudin improves bleeding outcomes while Bivalirudin improves bleeding outcomes while
preserving ischemic protection for ACS patients preserving ischemic protection for ACS patients even if the patients are switched from either UFH even if the patients are switched from either UFH or enoxaparin to bivalirudin (monotherapy) at the or enoxaparin to bivalirudin (monotherapy) at the time of presentation.time of presentation.
► Question:Question: Is it better to Is it better to switch to bivalirudin or remain on switch to bivalirudin or remain on consistent therapyconsistent therapy with the antithrombin with the antithrombin originally started?originally started?
ACUITY: “Switching” AnalysisACUITY: “Switching” Analysis
► Study MethodsStudy Methods Patients on prior antithrombin therapyPatients on prior antithrombin therapy
• Consistent:Consistent: No switchingNo switching from pre-randomization from pre-randomization antithrombin agent to randomized therapy: antithrombin agent to randomized therapy:
– Enoxaparin Enoxaparin →→Enoxaparin or UFH Enoxaparin or UFH →→ UFH UFH• Switch:Switch: Single switchSingle switch to bivalirudin determined by to bivalirudin determined by
randomization code randomization code – from Enoxaparin from Enoxaparin →→ Bivalirudin or UFH Bivalirudin or UFH → → BivalirudinBivalirudin
Event rates at 30-daysEvent rates at 30-days• Net clinical outcome Net clinical outcome • Ischemic compositeIschemic composite• Major bleedingMajor bleeding
ACUITY Primary Endpoints at 30 DaysACUITY Primary Endpoints at 30 Days
► Net Clinical EndpointNet Clinical Endpoint Composite ischemic and non-CABG major bleeding Composite ischemic and non-CABG major bleeding
endpointsendpoints
► Ischemic EndpointIschemic Endpoint Death, MI, or unplanned revascularizationDeath, MI, or unplanned revascularization
► Non-CABG Major Bleeding EndpointNon-CABG Major Bleeding Endpoint Intracranial, intraocular, or retroperitoneal bleedingIntracranial, intraocular, or retroperitoneal bleeding Access site bleed requiring intervention/surgeryAccess site bleed requiring intervention/surgery Hematoma ≥5 cmHematoma ≥5 cm Hgb Hgb ≥3g/dL with an overt source or ≥3g/dL with an overt source or ≥4g/dL w/o overt ≥4g/dL w/o overt
sourcesource Blood transfusionBlood transfusion
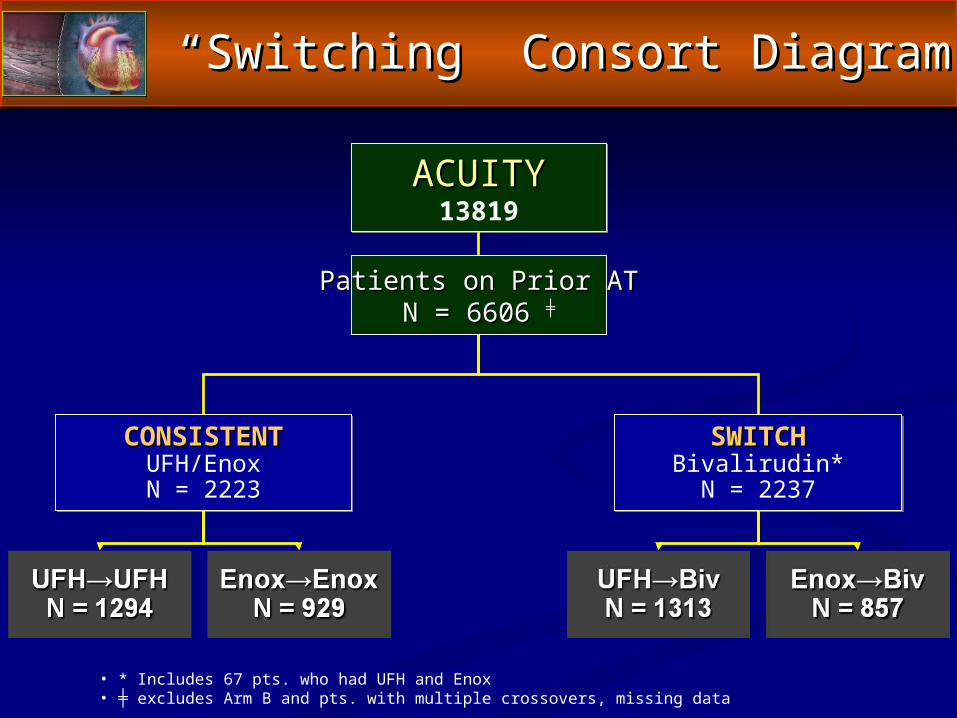
““Switching” Consort DiagramSwitching” Consort Diagram
ACUITYACUITY13819
CONSISTENTCONSISTENTUFH/EnoxN = 2223
SWITCHSWITCHBivalirudin*N = 2237
Patients on Prior ATPatients on Prior ATN = 6606 N = 6606 ╪╪
• * Includes 67 pts. who had UFH and Enox • ╪ excludes Arm B and pts. with multiple crossovers, missing data
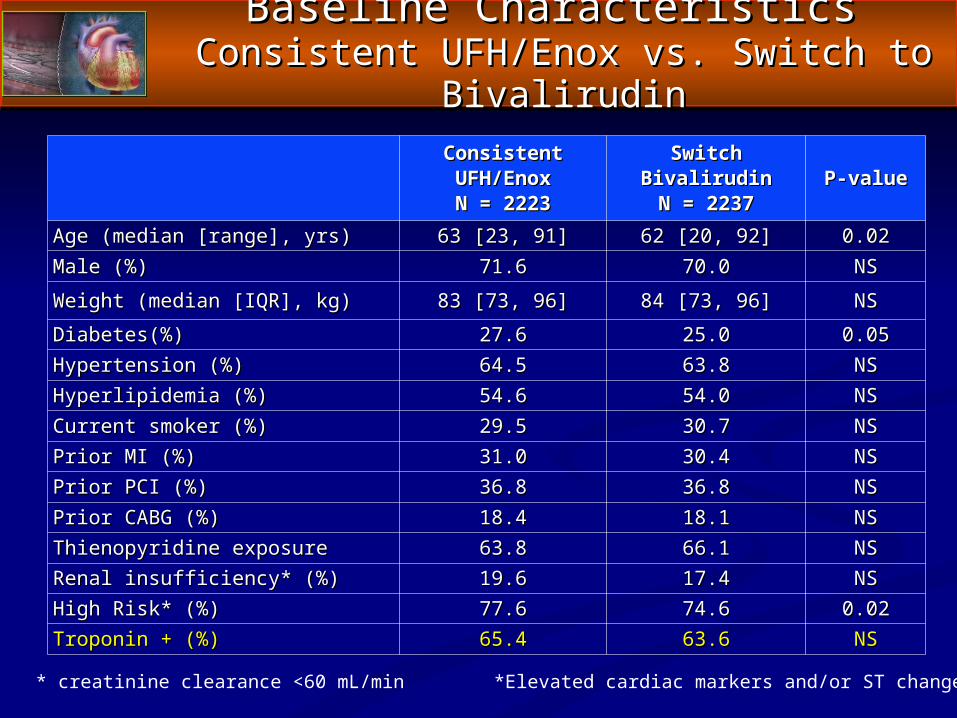
Baseline Characteristics Baseline Characteristics Consistent UFH/Enox vs. Switch to BivalirudinConsistent UFH/Enox vs. Switch to Bivalirudin
ConsistentConsistentUFH/EnoxUFH/EnoxN = 2223N = 2223
SwitchSwitchBivalirudinBivalirudinN = 2237N = 2237
P-valueP-value
Age (median [range], yrs)Age (median [range], yrs) 63 [23, 91]63 [23, 91] 62 [20, 92]62 [20, 92] 0.020.02Male (%)Male (%) 71.671.6 70.070.0 NSNS
Weight (median [IQR], kg)Weight (median [IQR], kg) 83 [73, 96]83 [73, 96] 84 [73, 96]84 [73, 96] NSNS
Diabetes(%)Diabetes(%) 27.627.6 25.025.0 0.050.05Hypertension (%)Hypertension (%) 64.564.5 63.863.8 NSNSHyperlipidemia (%)Hyperlipidemia (%) 54.654.6 54.054.0 NSNSCurrent smoker (%)Current smoker (%) 29.529.5 30.730.7 NSNSPrior MI (%)Prior MI (%) 31.031.0 30.430.4 NSNSPrior PCI (%)Prior PCI (%) 36.836.8 36.836.8 NSNSPrior CABG (%)Prior CABG (%) 18.418.4 18.118.1 NSNSThienopyridine exposureThienopyridine exposure 63.863.8 66.166.1 NSNSRenal insufficiency* (%)Renal insufficiency* (%) 19.619.6 17.417.4 NSNSHigh Risk* (%)High Risk* (%) 77.677.6 74.674.6 0.020.02Troponin + (%)Troponin + (%) 65.465.4 63.663.6 NSNS
* creatinine clearance <60 mL/min *Elevated cardiac markers and/or ST changes
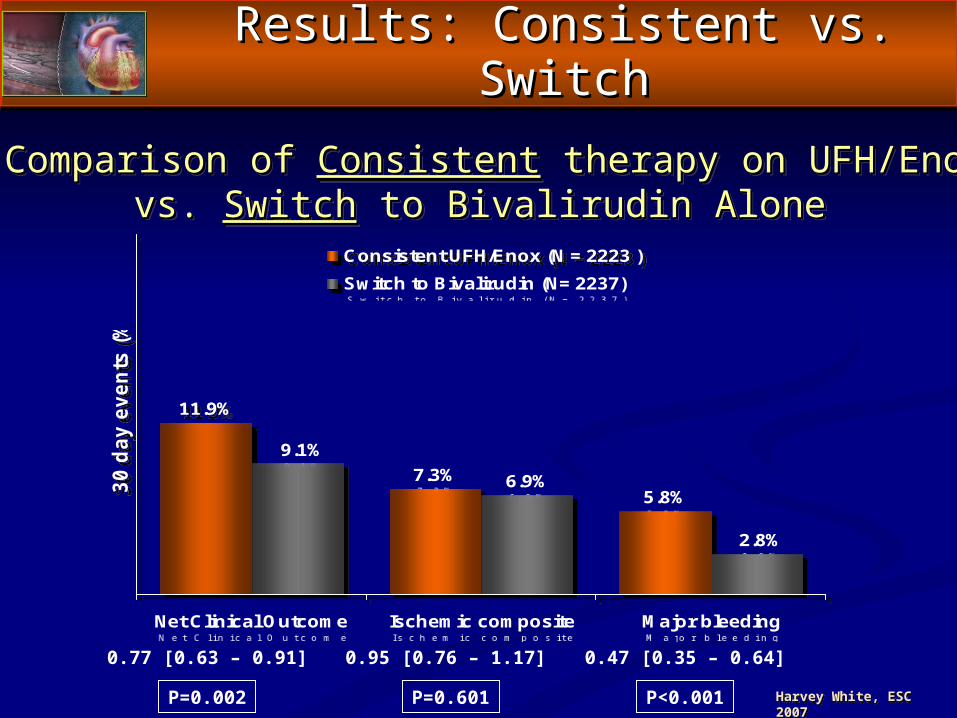
Results: Consistent vs. SwitchResults: Consistent vs. Switch
11.9%
7.3%5.8%
6.9%
9.1%
2.8%
Net Clinical Outcome Ischemic composite Major bleeding
30 d
ay e
vent
s (%
)
Consistent UFH/Enox (N = 2223 ) Switch to Bivalirudin (N= 2237)
Comparison of Comparison of ConsistentConsistent therapy on UFH/Enox therapy on UFH/Enoxvs. vs. SwitchSwitch to Bivalirudin Alone to Bivalirudin Alone
P=0.002
0.77 [0.63 – 0.91]
P=0.601
0.95 [0.76 – 1.17]
P<0.001
0.47 [0.35 – 0.64]
Harvey White, ESC 2007
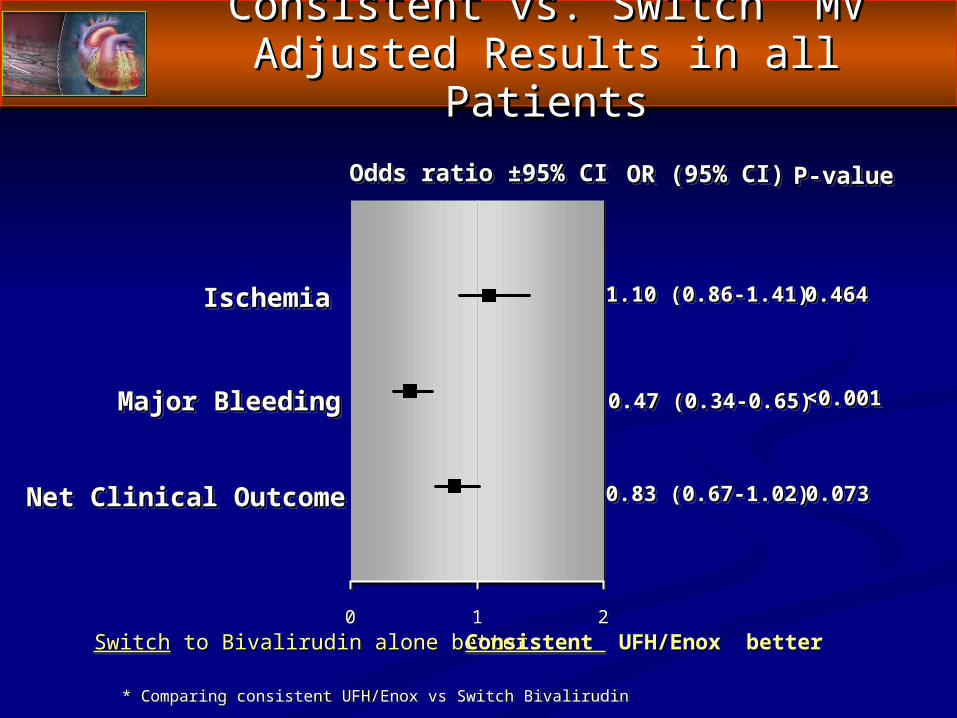
0 1 2
0.83 (0.67-1.02)0.83 (0.67-1.02)
OR (95% CI)OR (95% CI)Odds ratio ±95% CIOdds ratio ±95% CI
SwitchSwitch to Bivalirudin alone better to Bivalirudin alone better Consistent Consistent UFH/Enox better UFH/Enox better
Major BleedingMajor Bleeding
IschemiaIschemia
Net Clinical OutcomeNet Clinical Outcome
1.10 (0.86-1.41)1.10 (0.86-1.41)
0.47 (0.34-0.65)0.47 (0.34-0.65)
P-valueP-value
0.0730.073
0.4640.464
<0.001<0.001
* Comparing consistent UFH/Enox vs Switch Bivalirudin
Consistent vs. Switch MV Adjusted Consistent vs. Switch MV Adjusted Results in all PatientsResults in all Patients
0 1 2
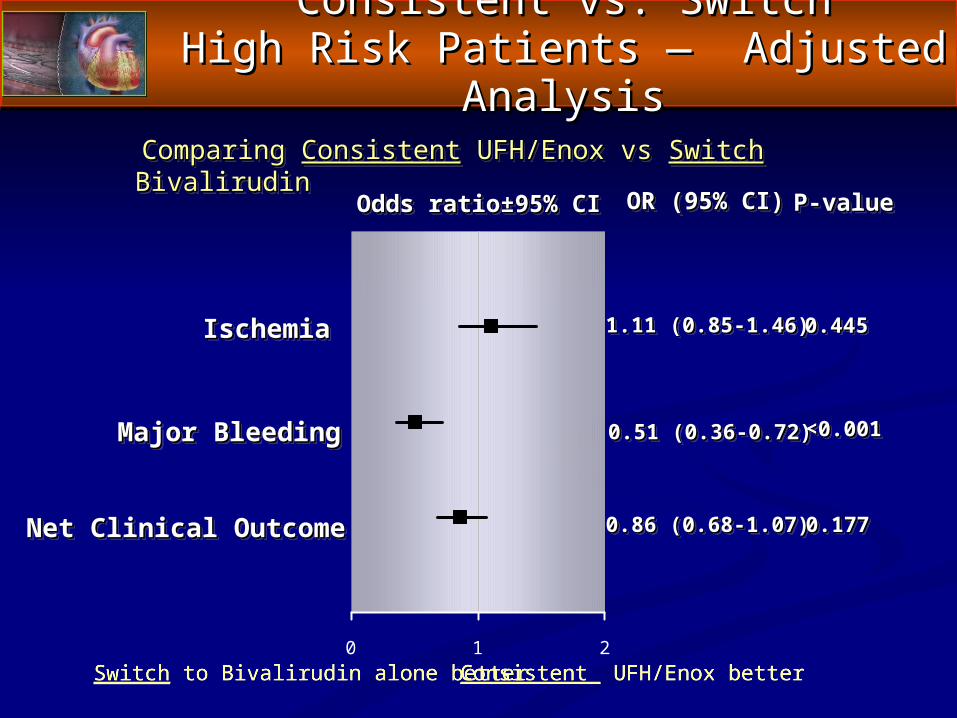
0.86 (0.68-1.07)0.86 (0.68-1.07)
OR (95% CI)OR (95% CI)Odds ratio±95% CIOdds ratio±95% CI
Switch to Bivalirudin alone better Consistent UFH/Enox better
Major BleedingMajor Bleeding
IschemiaIschemia
Net Clinical OutcomeNet Clinical Outcome
1.11 (0.85-1.46)1.11 (0.85-1.46)
0.51 (0.36-0.72)0.51 (0.36-0.72)
P-valueP-value
0.1770.177
0.4450.445
<0.001<0.001
Consistent vs. SwitchConsistent vs. SwitchHigh Risk Patients — Adjusted AnalysisHigh Risk Patients — Adjusted Analysis
Comparing Comparing ConsistentConsistent UFH/Enox vs UFH/Enox vs Switch Switch BivalirudinBivalirudin
Consistent vs. SwitchConsistent vs. Switch
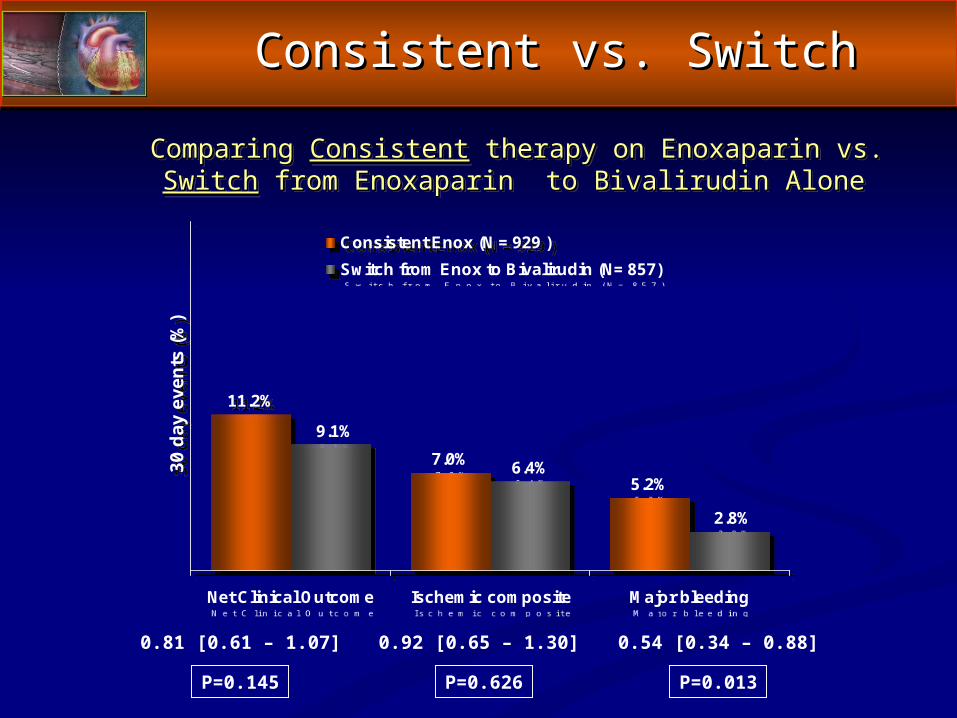
11.2%
7.0%5.2%
6.4%
9.1%
2.8%
Net Clinical Outcome Ischemic composite Major bleeding
30 d
ay e
vent
s (%
)
Consistent Enox (N = 929 ) Switch from Enox to Bivalirudin (N= 857)
Comparing Comparing ConsistentConsistent therapy on Enoxaparin vs. therapy on Enoxaparin vs. SwitchSwitch from from Enoxaparin to Bivalirudin AloneEnoxaparin to Bivalirudin Alone
P=0.145
0.81 [0.61 – 1.07]
P=0.626
0.92 [0.65 – 1.30]
P=0.013
0.54 [0.34 – 0.88]
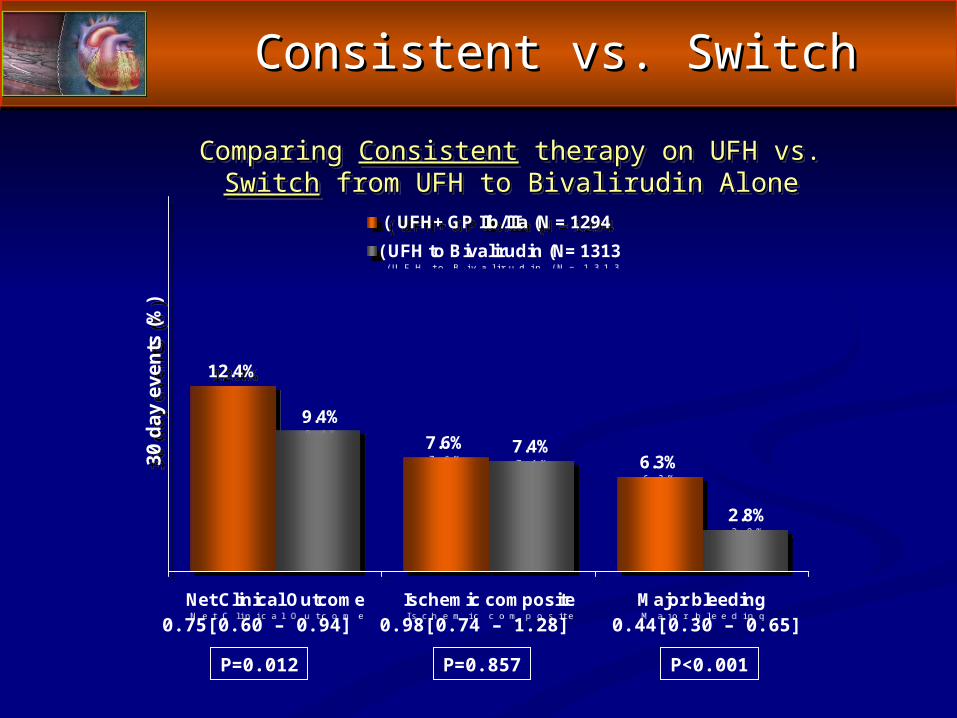
12.4%
7.6%6.3%
7.4%9.4%
2.8%
Net Clinical Outcome Ischemic composite Major bleeding
30 d
ay e
vent
s (%
)
( UFH+ GP IIb/IIIa (N = 1294(UFH to Bivalirudin (N= 1313
Comparing Comparing ConsistentConsistent therapy on UFH vs. therapy on UFH vs. SwitchSwitch from UFH to Bivalirudin Alone from UFH to Bivalirudin Alone
P=0.012
0.75[0.60 – 0.94]
P=0.857
0.98[0.74 – 1.28]
P<0.001
0.44[0.30 – 0.65]
Consistent vs. SwitchConsistent vs. Switch
ConclusionsConclusions
► Switching to bivalirudin is safeSwitching to bivalirudin is safe Switching from any heparin (either enoxaparin Switching from any heparin (either enoxaparin
or UFH) to bivalirudin monotherapy is not or UFH) to bivalirudin monotherapy is not associated with an increased risk for ischemic associated with an increased risk for ischemic events.events.
► FurthermoreFurthermore Switching to bivalirudin provides patients the Switching to bivalirudin provides patients the
50% bleeding advantage of bivalirudin 50% bleeding advantage of bivalirudin compared with consistent therapy on UFH or compared with consistent therapy on UFH or enoxaparin.enoxaparin.
NSTE Acute Coronary SyndromesNSTE Acute Coronary SyndromesThe Year 2007 ACC/AHA GuidelinesThe Year 2007 ACC/AHA Guidelines
and Upstream Therapy — and Upstream Therapy — How Do We Collaborate Across Best Evidence?How Do We Collaborate Across Best Evidence?
Charles V. Pollack, Jr., M.A., M.D., FACEP, FAHACharles V. Pollack, Jr., M.A., M.D., FACEP, FAHAProfessor and ChairmanProfessor and Chairman
Emergency Medicine, Pennsylvania HospitalEmergency Medicine, Pennsylvania HospitalUniversity of Pennsylvania Health SystemUniversity of Pennsylvania Health System
PhiladelphiaPhiladelphia
Getting in the ACS (Up)Stream of Things
► Anderson JL, Adams CD, Antman EM, et al. 2007 Anderson JL, Adams CD, Antman EM, et al. 2007 guidelines for the management of patients with unstable guidelines for the management of patients with unstable angina/non-ST-segment-elevation myocardial infarction: a angina/non-ST-segment-elevation myocardial infarction: a report of the American College of Cardiology/American report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Heart Association Task Force on Practice Guidelines. J Am J Am Coll CardiolColl Cardiol 2007;50:e1-e157, and 2007;50:e1-e157, and CirculationCirculation 2007;116:e148-e304, and at www.acc.org and at 2007;116:e148-e304, and at www.acc.org and at www.americanheart.org. www.americanheart.org.
► Pollack CV, Braunwald E: 2007 Update to the ACC/AHA Pollack CV, Braunwald E: 2007 Update to the ACC/AHA guidelines for the management of patients with unstable guidelines for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction: angina and non-ST-segment elevation myocardial infarction: Implications for emergency department practice. Implications for emergency department practice. Ann Ann Emerg MedEmerg Med 2007, in press. 2007, in press.
NSTE ACS: Optimal Therapy, 8/6/07NSTE ACS: Optimal Therapy, 8/6/07
The Role of the Emergency Physician in the The Role of the Emergency Physician in the Management of Chest PainManagement of Chest Pain
► StabilizationStabilization When requiredWhen required
► RecognitionRecognition ““Atypical is the new typical”Atypical is the new typical”
► Prompt STEMI managementPrompt STEMI management ~ 15% of our ACS population—new data to follow~ 15% of our ACS population—new data to follow
► Risk Stratification of the restRisk Stratification of the rest > 50% don’t have ACS> 50% don’t have ACS Of those who do, fewer than 30% are high Of those who do, fewer than 30% are high
(ischemic) risk in the ED(ischemic) risk in the ED
The Role of the Emergency Physician in the The Role of the Emergency Physician in the Management of Chest PainManagement of Chest Pain
► Communication with CardiologyCommunication with Cardiology Often hospital medicine, PCP, and noninterventionalists as part Often hospital medicine, PCP, and noninterventionalists as part
of process-of-care in ACSof process-of-care in ACS
► Confluent Therapeutic Choices — Considerations Include:Confluent Therapeutic Choices — Considerations Include: Ischemic riskIschemic risk Bleeding riskBleeding risk Choice of upstream therapyChoice of upstream therapy Reversibility of upstream therapy—re CABG and bleedingReversibility of upstream therapy—re CABG and bleeding Likely duration of upstream therapyLikely duration of upstream therapy
► Transition of careTransition of care If patient going to cath, time frame increasingly compressedIf patient going to cath, time frame increasingly compressed If to tele/CCU, emergency physician has If to tele/CCU, emergency physician has moremore impact impact
Patients with Chest Pain Syndrome Must Be Risk-Stratified in ED
► Three levels of risk stratification are pertinent to the Three levels of risk stratification are pertinent to the ED:ED:LowLow, , intermediate, or intermediate, or highhigh risk that ischemic symptoms risk that ischemic symptoms
are a result of CADare a result of CAD
LowLow, intermediate, intermediate, or , or high riskhigh risk of short-term death or of short-term death or nonfatal MI from ACSnonfatal MI from ACS
Dynamic, ongoing risk-oriented evaluation of low- or Dynamic, ongoing risk-oriented evaluation of low- or intermediate-risk patients for “conversion” to high-risk intermediate-risk patients for “conversion” to high-risk
status status that is linked to intensity of treatmentthat is linked to intensity of treatment
Risk StratificationRisk Stratification
““Dynamic Risk Stratification” ToolsDynamic Risk Stratification” Tools
► History and PhysicalHistory and Physical► Standard EKG and Non-standard EKG leadsStandard EKG and Non-standard EKG leads
15-lead ECGs should perhaps be “standard” in all 15-lead ECGs should perhaps be “standard” in all but very-low-risk patientsbut very-low-risk patients
► MarkersMarkers CPK-MB, Troponins I and T, MyoglobinCPK-MB, Troponins I and T, Myoglobin Markers of inflammation and ischemiaMarkers of inflammation and ischemia BNPBNP
► Non-Invasive ImagingNon-Invasive Imaging EchocardiogramEchocardiogram Stress testingStress testing Technetium-99m-sestamibi Technetium-99m-sestamibi CT coronary angiographyCT coronary angiography
► Predictive Indices/SchemesPredictive Indices/Schemes TIMI, GRACE, PURSUITTIMI, GRACE, PURSUIT
CRUSADE: A National CRUSADE: A National Quality Improvement InitiativeQuality Improvement Initiative
CCan an RRapid Risk Stratification of apid Risk Stratification of UUnstable Angina Patients nstable Angina Patients
SSuppress uppress ADADverse Outcomes with verse Outcomes with EEarly Implementation arly Implementation
of the ACC/AHA Guidelinesof the ACC/AHA Guidelines
2002-20072002-2007
The CRUSADE ExperienceThe CRUSADE Experience
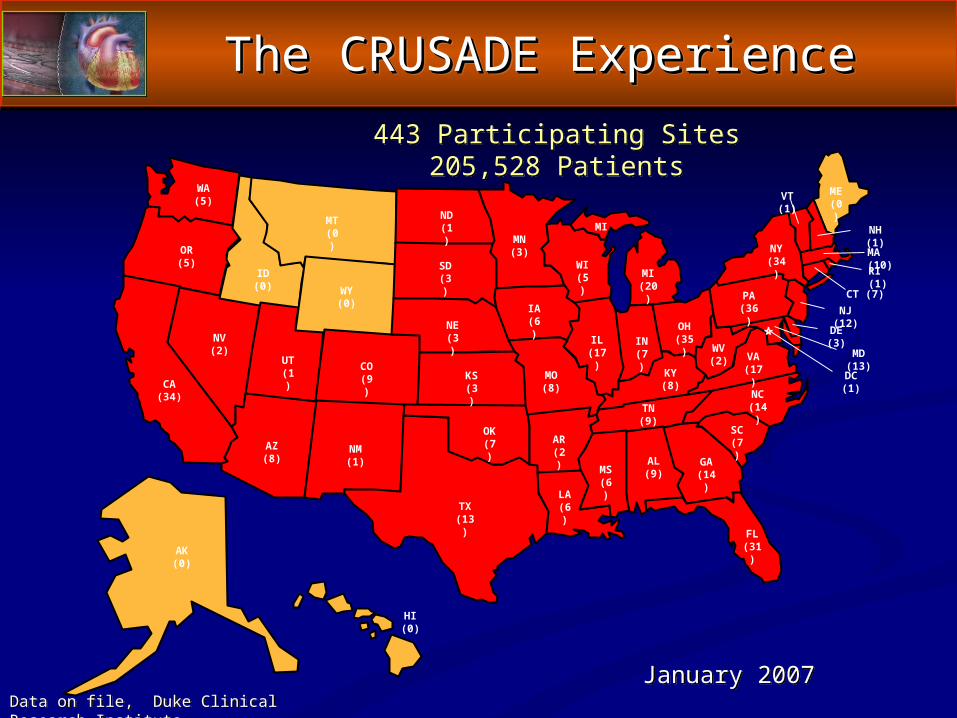
January 2007
443 Participating Sites205,528 Patients
AK(0)
WA(5)
OR(5)
CA(34)
ID(0)
NV(2)
MT(0)
WY(0)
CO(9)
NM(1)
ND(1)
SD(3)
NE (3)
KS(3)
OK(7)
TX(13)
MN(3)
IA(6)
MO(8)
AR(2)
LA(6)
WI(5) MI
(20)
MI
UT(1)
AZ(8)
HI (0)
IL(17)
IN(7)
KY(8)
TN (9)
MS(6)
AL(9)
GA(14)
FL(31)
SC(7)
NC(14)
VA(17)
OH(35)
WV(2)
PA(36)
NY(34)
MD (13)
ME(0)
VT (1)
NH (1)
NJ (12)
MA (10)
CT (7)
DE (3)
RI (1)
DC (1)
The CRUSADE ExperienceThe CRUSADE Experience
Data on file, Duke Clinical Research Institute.
Quality and OutcomesQuality and Outcomes
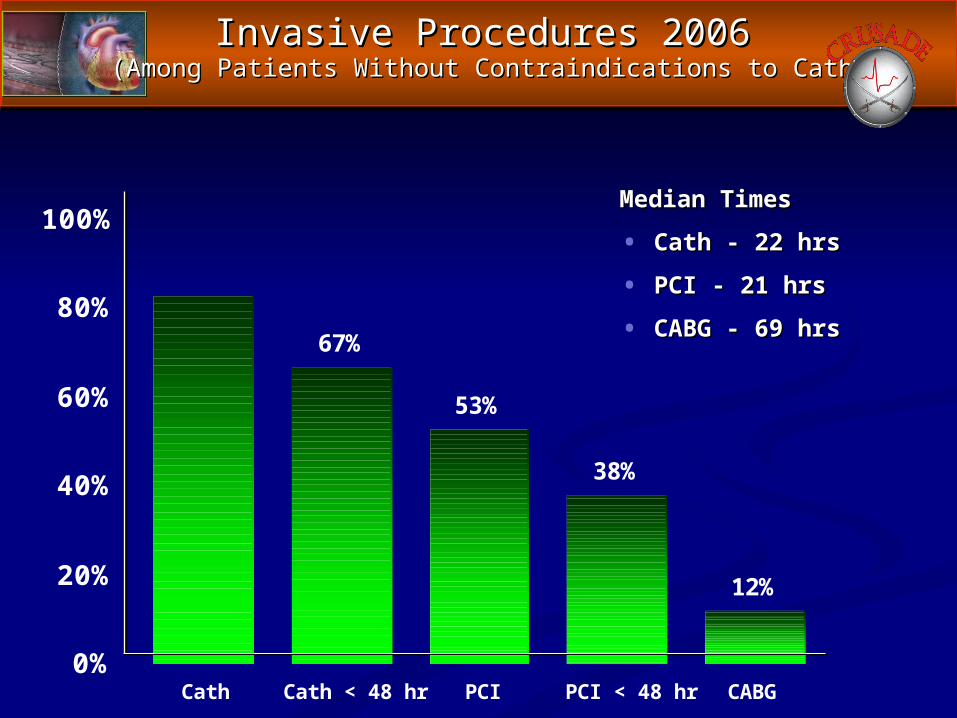
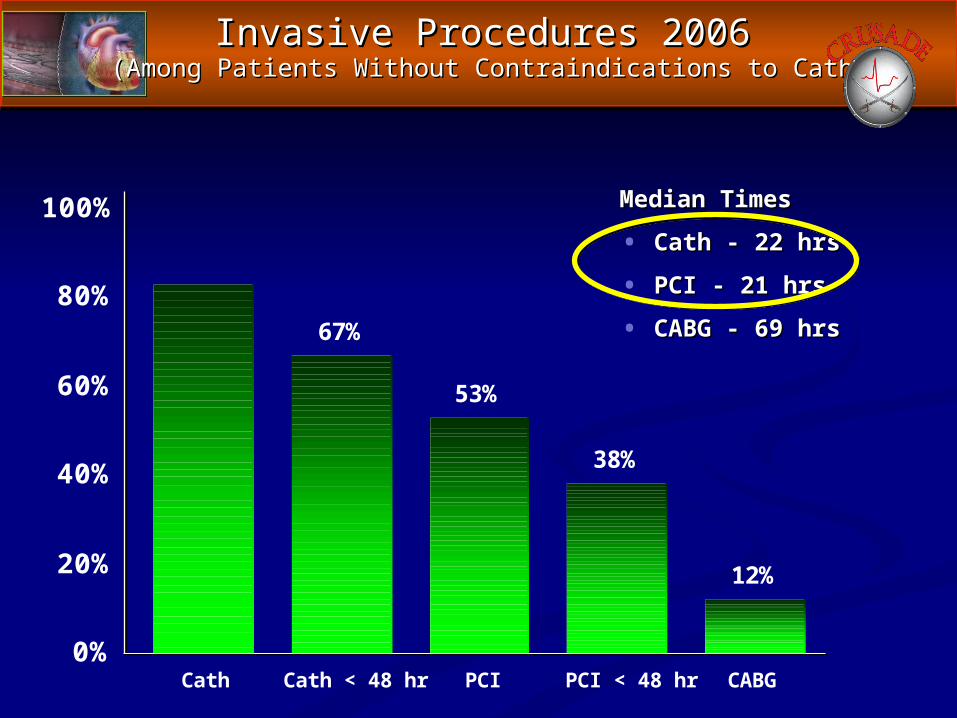
Invasive Procedures 2006Invasive Procedures 2006(Among Patients Without Contraindications to Cath(Among Patients Without Contraindications to Cath
Median TimesMedian Times
• Cath - 22 hrsCath - 22 hrs
• PCI - 21 hrsPCI - 21 hrs
• CABG - 69 hrsCABG - 69 hrs
83%
67%
53%
38%
12%
0%
20%
40%
60%
80%
100%
Cath Cath < 48 hr PCI PCI < 48 hr CABG
Management Strategies: 2007Management Strategies: 2007Early Invasive versus Selectively InvasiveEarly Invasive versus Selectively Invasive
► Early Invasive:Early Invasive: Diagnostic angiography with intent Diagnostic angiography with intent to perform revascularizationto perform revascularization Cath anticipated within 4-24 hoursCath anticipated within 4-24 hours Follows a foundation of risk-directed medical Follows a foundation of risk-directed medical
therapytherapy► Selectively InvasiveSelectively Invasive (or (or Early ConservativeEarly Conservative):):
Invasive evaluation only if optimal medical Invasive evaluation only if optimal medical management failsmanagement fails
► Note: From the ED perspective, both strategies Note: From the ED perspective, both strategies involve risk-directed, evidence-based medical involve risk-directed, evidence-based medical therapytherapy
What Is “Risk-Directed” What Is “Risk-Directed” Medical Management?Medical Management?
► ASAASA► Antithrombin therapyAntithrombin therapy
I-A: Enoxaparin or UFHI-A: Enoxaparin or UFH I-B: Bivalirudin or I-B: Bivalirudin or
fondaparinuxfondaparinux
► Antiplatelet therapyAntiplatelet therapy Oral anti-activation therapyOral anti-activation therapy Parenteral anti-aggregation Parenteral anti-aggregation
therapytherapy As number of therapies increases, bleeding risk generally increases
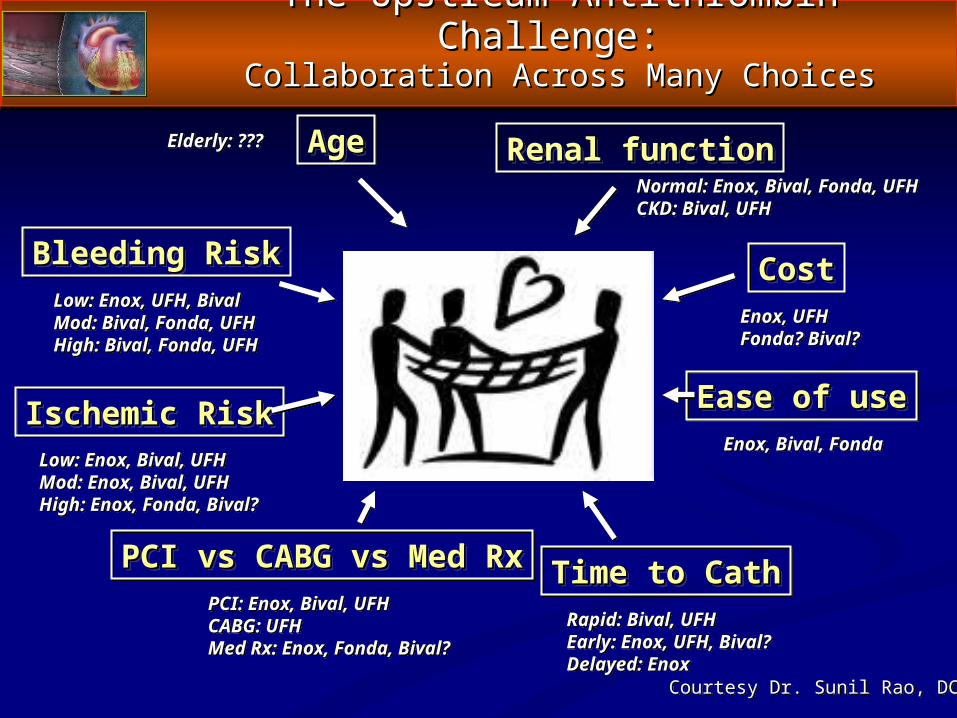
The Upstream Antithrombin Challenge: The Upstream Antithrombin Challenge: Collaboration Across Many ChoicesCollaboration Across Many Choices
Bleeding RiskBleeding Risk
Ischemic RiskIschemic Risk
Renal functionRenal functionAgeAge
Time to CathTime to Cath
CostCost
Ease of useEase of use
PCI vs CABG vs Med RxPCI vs CABG vs Med Rx
Low: Enox, Bival, UFHMod: Enox, Bival, UFHHigh: Enox, Fonda, Bival?
Low: Enox, UFH, BivalMod: Bival, Fonda, UFHHigh: Bival, Fonda, UFH
Elderly: ???
Normal: Enox, Bival, Fonda, UFHCKD: Bival, UFH
Enox, UFHFonda? Bival?
Enox, Bival, Fonda
Rapid: Bival, UFHEarly: Enox, UFH, Bival?Delayed: Enox
PCI: Enox, Bival, UFHCABG: UFHMed Rx: Enox, Fonda, Bival?
Courtesy Dr. Sunil Rao, DCRI
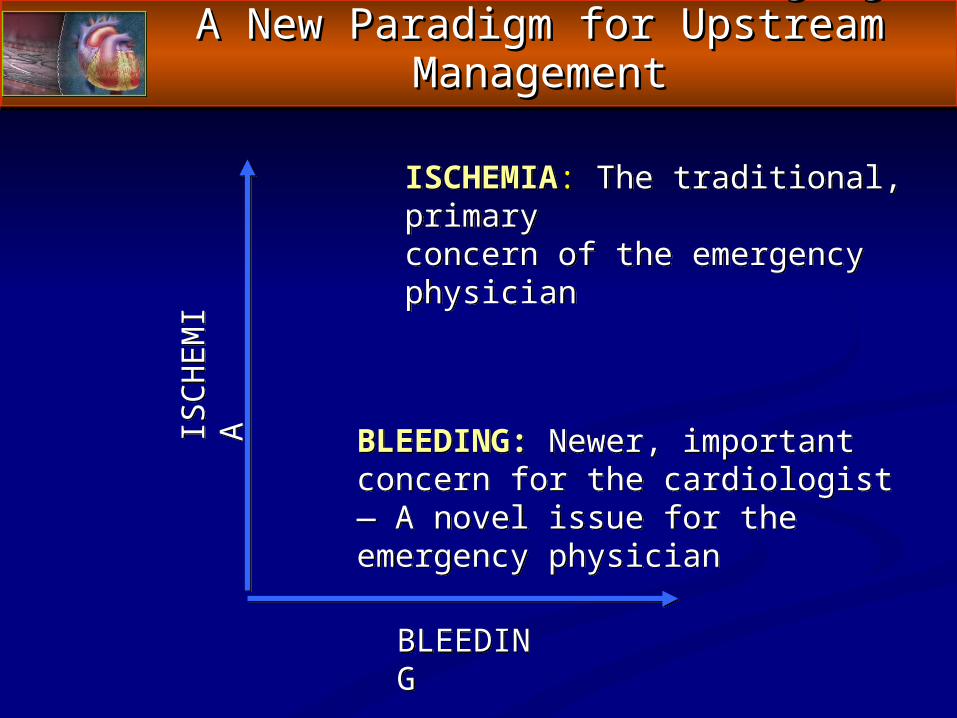
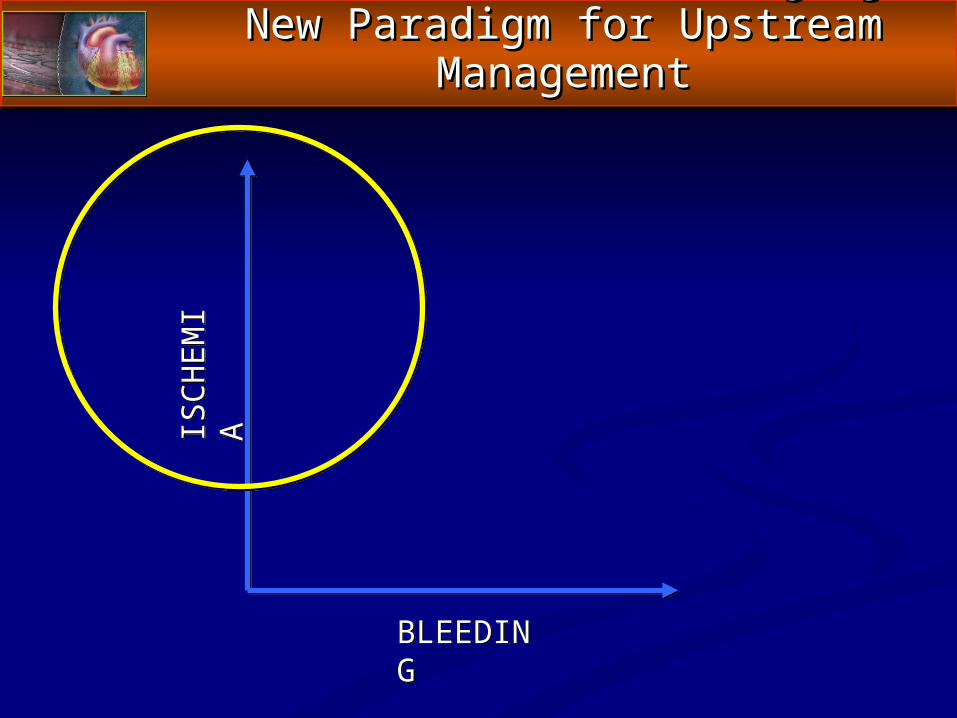
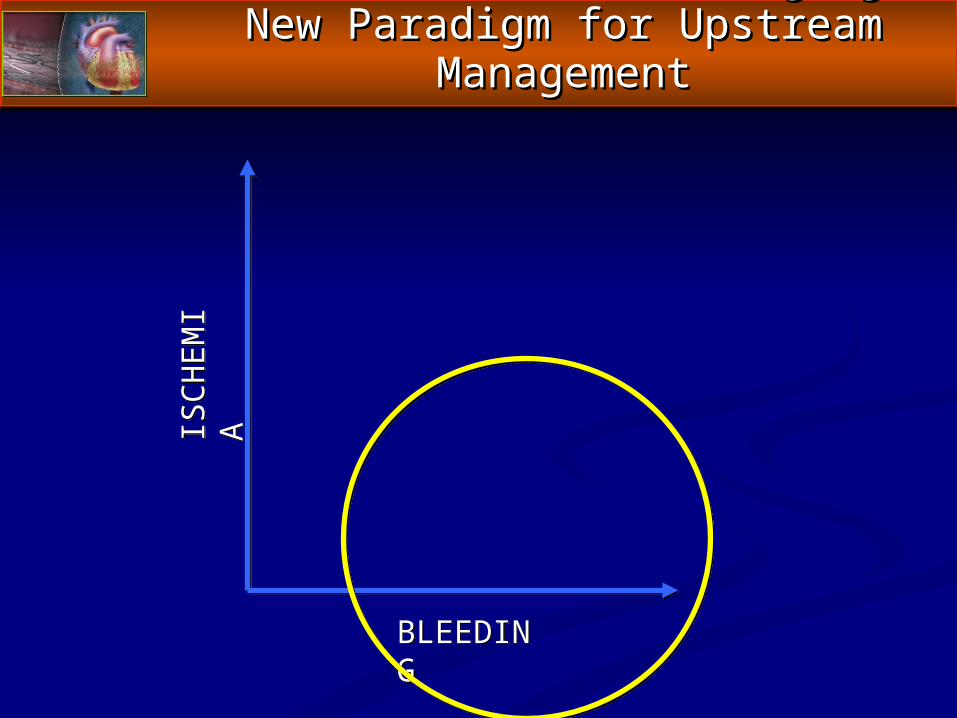
Recent ACS Trials — Forging A New Recent ACS Trials — Forging A New Paradigm for Upstream ManagementParadigm for Upstream Management
ISC
HE
MI
A
BLEEDING
ISCHEMIA: The traditional, primary concern of the emergency physician
BLEEDING: Newer, important concern for the cardiologist — A novel issue for the emergency physician
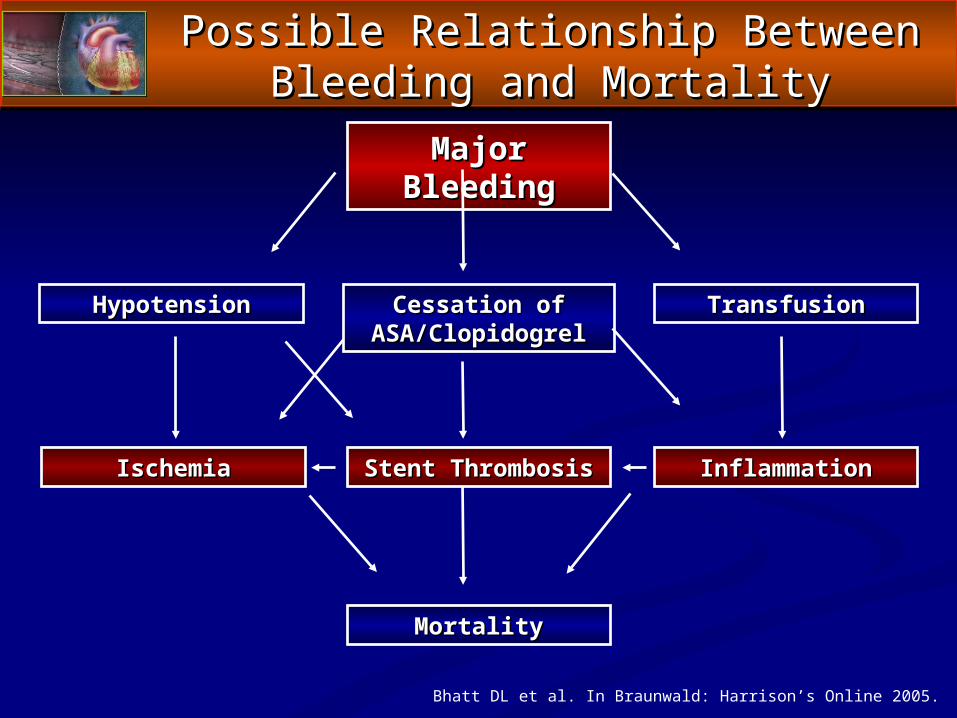
MortalityMortality
Major BleedingMajor Bleeding
TransfusionTransfusionHypotensionHypotension Cessation of Cessation of ASA/ClopidogrelASA/Clopidogrel
IschemiaIschemia Stent ThrombosisStent Thrombosis InflammationInflammation
Bhatt DL et al. In Braunwald: Harrison’s Online 2005.
Possible Relationship BetweenPossible Relationship BetweenBleeding and MortalityBleeding and Mortality
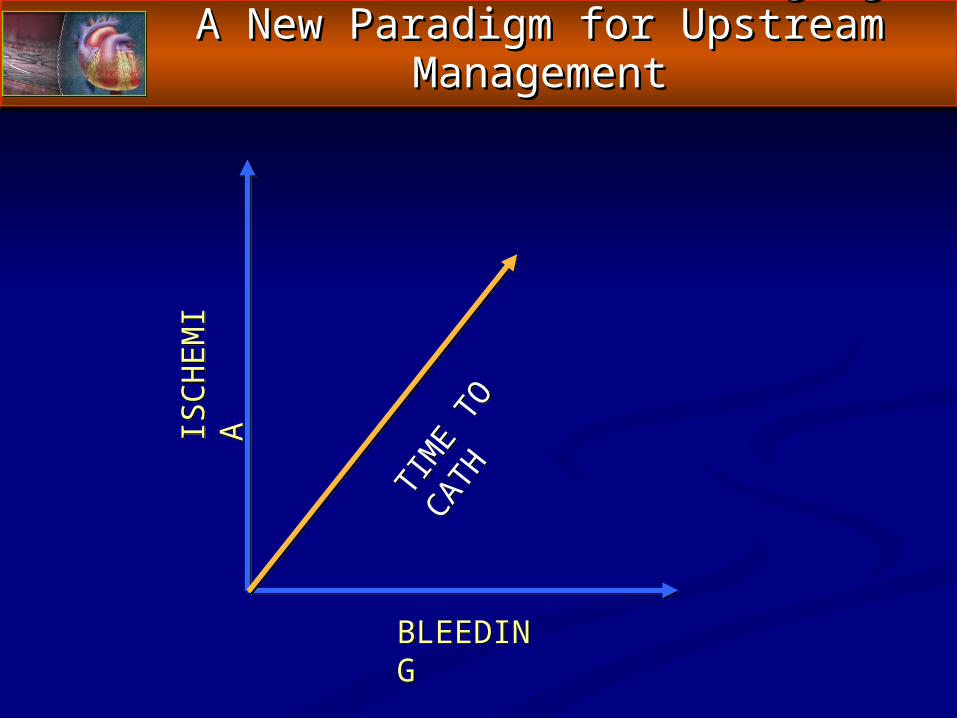
Recent ACS Trials — Forging A New Recent ACS Trials — Forging A New Paradigm for Upstream ManagementParadigm for Upstream Management
ISC
HE
MI
A
BLEEDING
TIM
E TO
CATH
Invasive Procedures 2006Invasive Procedures 2006(Among Patients Without Contraindications to Cath(Among Patients Without Contraindications to Cath
Median TimesMedian Times
• Cath - 22 hrsCath - 22 hrs
• PCI - 21 hrsPCI - 21 hrs
• CABG - 69 hrsCABG - 69 hrs
83%
67%
53%
38%
12%
0%
20%
40%
60%
80%
100%
Cath Cath < 48 hr PCI PCI < 48 hr CABG
Management Strategies: 2007Management Strategies: 2007Early Invasive versus Selectively InvasiveEarly Invasive versus Selectively Invasive
► Early Invasive:Early Invasive: Diagnostic angiography with intent Diagnostic angiography with intent to perform revascularizationto perform revascularization Cath anticipated within 4-24 hoursCath anticipated within 4-24 hours Follows a foundation of risk-directed medical Follows a foundation of risk-directed medical
therapytherapy► Selectively InvasiveSelectively Invasive (or (or Early ConservativeEarly Conservative):):
Invasive evaluation only if optimal medical Invasive evaluation only if optimal medical management failsmanagement fails
► Note: From the ED perspective, both strategies Note: From the ED perspective, both strategies involve risk-directed, evidence-based medical involve risk-directed, evidence-based medical therapytherapy
Case Studies in Upstream ManagementCase Studies in Upstream ManagementHow Many Ways Can We Cut the Cake?How Many Ways Can We Cut the Cake?
► Consider Case Scenario 1:Consider Case Scenario 1: 5555 year-old man with chest pain syndrome for year-old man with chest pain syndrome for 4 4
hourshours Smoker, diabetic, normal renal functionSmoker, diabetic, normal renal function Troponin not elevatedTroponin not elevated; nonspecific ST-T; nonspecific ST-T wave wave
changeschanges Unless he deteriorates, not likely to go to cath before Unless he deteriorates, not likely to go to cath before
tomorrowtomorrow► Optimal Upstream Therapy in Emergency DepartmentOptimal Upstream Therapy in Emergency Department::
Enoxaparin or UFHEnoxaparin or UFH Strongly consider clopidogrelStrongly consider clopidogrel GPI if troponin GPI if troponin ↑ overnight↑ overnight
Case Studies in Upstream ManagementCase Studies in Upstream ManagementHow Many Ways Can We Cut the Cake?How Many Ways Can We Cut the Cake?
► Consider Case Scenario 2Consider Case Scenario 2:: 55 year-old man with chest pain syndrome for 4 55 year-old man with chest pain syndrome for 4
hourshours Smoker, diabetic, normal renal functionSmoker, diabetic, normal renal function Troponin not elevated; Non-specific ST-T wave Troponin not elevated; Non-specific ST-T wave
changeschanges Going to cath later todayGoing to cath later today
► Optimal Upstream Therapy in Emergency DepartmentOptimal Upstream Therapy in Emergency Department:: Bivalirudin or UFHBivalirudin or UFH Stronger support for clopidogrelStronger support for clopidogrel
Case Studies in Upstream ManagementCase Studies in Upstream ManagementHow Many Ways Can We Cut the Cake?How Many Ways Can We Cut the Cake?
► Consider Case Scenario 3:Consider Case Scenario 3:► 8080 year-old year-old womanwoman with chest pain syndrome for 4 with chest pain syndrome for 4
hourshours Smoker, diabetic, Smoker, diabetic, Cr Cl 40 ml/minCr Cl 40 ml/min Troponin elevated; ST-T Wave changesTroponin elevated; ST-T Wave changes Going to cath later todayGoing to cath later today
► Optimal Upstream Therapy in Emergency Department:Optimal Upstream Therapy in Emergency Department: Bivalirudin Bivalirudin Consider clopidogrel, but CABG risk may be higher Consider clopidogrel, but CABG risk may be higher
herehere
Case Studies in Upstream ManagementCase Studies in Upstream ManagementHow Many Ways Can We Cut the Cake?How Many Ways Can We Cut the Cake?
► Consider Case Scenario 4:Consider Case Scenario 4: 80 year-old woman with chest pain syndrome for 4 80 year-old woman with chest pain syndrome for 4
hourshours Smoker, diabetic, Cr Cl 40 ml/minSmoker, diabetic, Cr Cl 40 ml/min Troponin elevated, NSSTTTroponin elevated, NSSTTΔΔss No catheterization lab in hospital; transfer time No catheterization lab in hospital; transfer time
uncertainuncertain► Optimal Upstream Therapy:Optimal Upstream Therapy:
Enoxaparin or fondaparinuxEnoxaparin or fondaparinux Strongly consider clopidogrelStrongly consider clopidogrel Consider renal-adjusted small-molecule GPIConsider renal-adjusted small-molecule GPI
Recent ACS Trials — Forging A New Recent ACS Trials — Forging A New Paradigm for Upstream ManagementParadigm for Upstream Management
ISC
HE
MI
A
BLEEDING
Optimal Upstream ManagementOptimal Upstream ManagementIschemic Risk AssessmentIschemic Risk Assessment
► Basis for Assessment:Basis for Assessment: ““Pain story”Pain story” Background ASCVD riskBackground ASCVD risk ECGECG Troponin in pertinent time frameTroponin in pertinent time frame Predictive scorePredictive score
► Options:Options: UFH and enoxaparin establishedUFH and enoxaparin established Bivalirudin and fondaparinux: New options that are Bivalirudin and fondaparinux: New options that are
non-inferiornon-inferior Antiplatelet therapy increasingly more important as Antiplatelet therapy increasingly more important as
ischemic risk increasesischemic risk increases
Recent ACS Trials — Forging A New Recent ACS Trials — Forging A New Paradigm for Upstream ManagementParadigm for Upstream Management
ISC
HE
MI
A
BLEEDING
Optimal Upstream ManagementOptimal Upstream ManagementBleeding Risk AssessmentBleeding Risk Assessment
► Basis for AssessmentBasis for Assessment:: Female > maleFemale > male Old > youngOld > young CKD > normal renal functionCKD > normal renal function Anemic > normal H/HAnemic > normal H/H Diabetic > nondiabeticDiabetic > nondiabetic
► Options:Options: Bivalirudin and fondaparinux associated with less Bivalirudin and fondaparinux associated with less
bleeding than UFH and enoxaparinbleeding than UFH and enoxaparin Clopidogrel not reversibleClopidogrel not reversible GPIs increase bleeding risk but with renal-adjusted GPIs increase bleeding risk but with renal-adjusted
doses seem to have reasonable safety margindoses seem to have reasonable safety margin
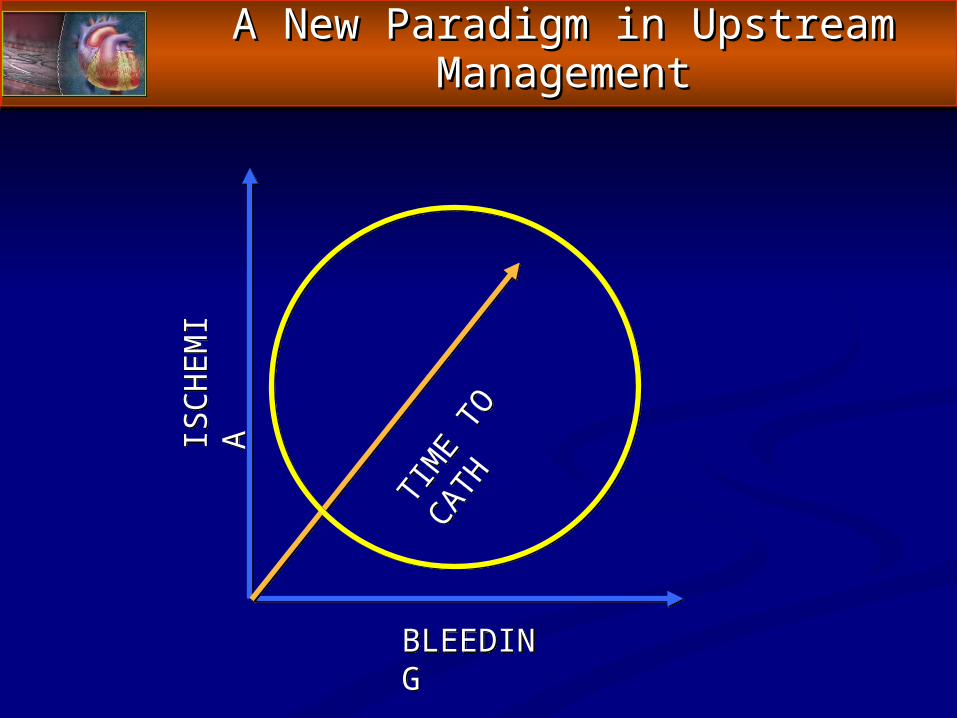
A New Paradigm in Upstream A New Paradigm in Upstream ManagementManagement
ISC
HE
MI
A
BLEEDING
TIM
E TO
CATH
Optimal Upstream ManagementOptimal Upstream ManagementTime to CatheterizationTime to Catheterization
► Basis for Assessment:Basis for Assessment: Time to catheterization is frequently an unknown variable in the ED Time to catheterization is frequently an unknown variable in the ED
for UA/NSTEMI patients: May have impact on initial antithrombin for UA/NSTEMI patients: May have impact on initial antithrombin selectionselection
Improved collaboration among CV specialists and ED physicians—Improved collaboration among CV specialists and ED physicians—and perhaps, development of EDICT for ACS therapeutic teams—and perhaps, development of EDICT for ACS therapeutic teams—would lead to more consistent management of ACS and would lead to more consistent management of ACS and predictability of time to catheterization predictability of time to catheterization
► Options:Options: With shorter times to catheterization, increasing support for With shorter times to catheterization, increasing support for
bivalirudinbivalirudin With longer times to catheterization or medical management, With longer times to catheterization or medical management,
increasing support for enoxaparin and UFH increasing support for enoxaparin and UFH Role of fondaparinux in patients going to cath may be problematic Role of fondaparinux in patients going to cath may be problematic
and not adequately testedand not adequately tested Note Dr. Gibson’s “switch” data re: bivalirudinNote Dr. Gibson’s “switch” data re: bivalirudin
► Chest Pain or ACS CommitteeChest Pain or ACS Committee
► Meets quarterly or PRNMeets quarterly or PRN PRN means afterPRN means after . . . . . .
• Pertinent, “practice-changing” new study Pertinent, “practice-changing” new study publishedpublished
• ACC / AHA / TCT meetingsACC / AHA / TCT meetings• M & M or sentinel eventM & M or sentinel event• New guidelines publishedNew guidelines published
Optimal Management of NSTE ACS: Optimal Management of NSTE ACS: ED to Cardiology — A Functional ModelED to Cardiology — A Functional Model
► Chest Pain or ACS Committee comprised of:Chest Pain or ACS Committee comprised of: Emergency physiciansEmergency physicians Interventional cardiologistsInterventional cardiologists Medical cardiologistsMedical cardiologists HospitalistsHospitalists CT surgeonsCT surgeons ED nursingED nursing Cath lab nursingCath lab nursing CCU nursingCCU nursing LabLab ImagingImaging
Optimal Management of NSTE ACS Optimal Management of NSTE ACS ED to Cardiology — A Functional ModelED to Cardiology — A Functional Model
► Chest Pain or ACS Committee discusses:Chest Pain or ACS Committee discusses: Protocols and standing ordersProtocols and standing orders Practice variations versus evidencePractice variations versus evidence Time to catheterization predictabilityTime to catheterization predictability Reduction of medical errors in ACS careReduction of medical errors in ACS care DTB timesDTB times QI issues (CRUSADE / NRMI / ACTION)QI issues (CRUSADE / NRMI / ACTION) Transfers in, transfers outTransfers in, transfers out New data: How should it impact our protocols?New data: How should it impact our protocols?
Optimal Management of NSTE ACSOptimal Management of NSTE ACS ED to Cardiology — A Functional Model ED to Cardiology — A Functional Model
► ED physicians should be using optimal, evidence-ED physicians should be using optimal, evidence-based, guideline-consistent medical therapy for NSTE based, guideline-consistent medical therapy for NSTE ACSACS
► ED physicians must work with their colleagues in ED physicians must work with their colleagues in cardiology to develop pathways and approaches cardiology to develop pathways and approaches (EDICT for ACS) for proper use of antithrombotic and (EDICT for ACS) for proper use of antithrombotic and antiplatelet therapy at all levelsantiplatelet therapy at all levels
► ED physicians should facilitate early invasive ED physicians should facilitate early invasive management of ACS whenever feasible and management of ACS whenever feasible and appropriateappropriate
► ED physicians should address issues related to ED physicians should address issues related to bleeding risk as well as ischemic risk. bleeding risk as well as ischemic risk.
► A seamless transition of care is most likely to result in A seamless transition of care is most likely to result in good outcomes.good outcomes.
Optimal Management of NSTE ACS Optimal Management of NSTE ACS ED to Cardiology — Summary and Game PlanED to Cardiology — Summary and Game Plan
UPSTREAM ACS CAREUPSTREAM ACS CARECollaborations, Models, and ProtocolsCollaborations, Models, and Protocols
The Mandate to Cooperate The Mandate to Cooperate and Collaborateand Collaborate
EDEDEmergencyEmergencyDepartmentDepartment
ICICInterventionalInterventional
CardiologyCardiology+
TTTherapeuticTherapeutic
TeamsTeams+ ACSfor
UPSTREAM ACS CAREUPSTREAM ACS CARECollaborations, Models, and ProtocolsCollaborations, Models, and Protocols
The Mandate to Cooperate The Mandate to Cooperate and Collaborateand Collaborate
EDEDEmergencyEmergencyDepartmentDepartment
ICICInterventionalInterventional
CardiologyCardiology+
TTTherapeuticTherapeutic
TeamsTeams+ ACSfor
Same m
odel
appli
es to
STEMI care
: It’s
not
just a
disc
ussio
n of D
2B tim
e
A Prospective, Randomized Comparison of A Prospective, Randomized Comparison of Bivalirudin vs. Heparin Plus Glycoprotein Bivalirudin vs. Heparin Plus Glycoprotein
IIb/IIIa Inhibitors During Primary Angioplasty in IIb/IIIa Inhibitors During Primary Angioplasty in Acute Myocardial InfarctionAcute Myocardial Infarction
– – 30 Day Results –30 Day Results –
Gregg W. Stone MDGregg W. Stone MDFor the HORIZONS AMI InvestigatorsFor the HORIZONS AMI Investigators
TCT 2007TCT 2007
HORIZONS AMIHORIZONS AMI
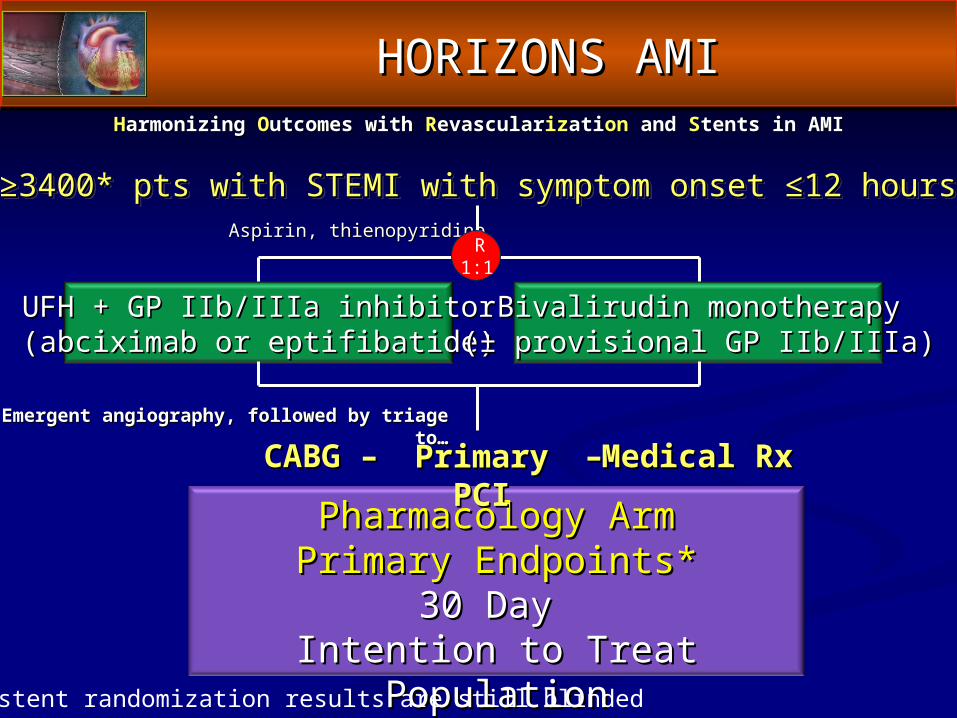
HHarmonizing armonizing OOutcomes with utcomes with RRevascularevascularizizatiationon and and SStents in AMItents in AMI
≥≥3400* pts with STEMI with symptom onset ≤12 hours3400* pts with STEMI with symptom onset ≤12 hours
UFH + GP IIb/IIIa inhibitorUFH + GP IIb/IIIa inhibitor(abciximab or eptifibatide)(abciximab or eptifibatide)
Bivalirudin monotherapyBivalirudin monotherapy(± provisional GP IIb/IIIa)(± provisional GP IIb/IIIa)
Aspirin, thienopyridineAspirin, thienopyridine R 1:1
Pharmacology ArmPharmacology ArmPrimary Endpoints*Primary Endpoints*
30 Day 30 Day Intention to Treat PopulationIntention to Treat Population
* All stent randomization results are still blinded
HORIZONS AMIHORIZONS AMI
Emergent angiography, followed by triage to…Emergent angiography, followed by triage to…
Primary PCIPrimary PCICABGCABG –– Medical RxMedical Rx––
Inclusion CriteriaInclusion Criteria
► STEMI >20 mins and <12 hours in durationSTEMI >20 mins and <12 hours in duration ST-segment elevation of ST-segment elevation of 1 mm in 1 mm in 2 contiguous leads; 2 contiguous leads;
oror Presumably new left bundle branch block; orPresumably new left bundle branch block; or True posterior MI with ST depression of True posterior MI with ST depression of 1 mm in 1 mm in 2 2
contiguous anterior leadscontiguous anterior leads Patients with cardiogenic shock, left main disease, etc., Patients with cardiogenic shock, left main disease, etc.,
were not excludedwere not excluded
► Age ≥18 yearsAge ≥18 years► Written, informed consentWritten, informed consent
Principal Exclusion CriteriaPrincipal Exclusion Criteria► Contraindication to any of the study medicationsContraindication to any of the study medications► Prior administration of thrombolytic therapy, bivalirudin, GP Prior administration of thrombolytic therapy, bivalirudin, GP
IIb/IIIa inhibitors, LMWH or fondaparinux for the present IIb/IIIa inhibitors, LMWH or fondaparinux for the present admission admission (prior UFH allowed)(prior UFH allowed)
► Current use of coumadinCurrent use of coumadin► History of bleeding diathesis or known coagulopathy (including History of bleeding diathesis or known coagulopathy (including
HIT), or will refuse blood transfusionsHIT), or will refuse blood transfusions► History of intracerebral mass, aneurysm, AVM, or hemorrhagic History of intracerebral mass, aneurysm, AVM, or hemorrhagic
stroke; stroke or TIA within 6 months or any permanent stroke; stroke or TIA within 6 months or any permanent neurologic deficit; GI or GU bleed within 2 months, or major neurologic deficit; GI or GU bleed within 2 months, or major surgery within 6 weeks; recent or known platelet count surgery within 6 weeks; recent or known platelet count <100,000 cells/mm<100,000 cells/mm33 or hgb <10 g/dL or hgb <10 g/dL
► Planned elective surgical procedure that would necessitate Planned elective surgical procedure that would necessitate interruption of thienopyridines during the first 6 months post interruption of thienopyridines during the first 6 months post enrollment enrollment
Study Medications (i)Study Medications (i)► Unfractionated heparinUnfractionated heparin
60 U/kg IV*; subsequent boluses titrated by nomogram to 60 U/kg IV*; subsequent boluses titrated by nomogram to ACT 200-250 secs; terminated at procedure end unless ACT 200-250 secs; terminated at procedure end unless prolonged antithrombin neededprolonged antithrombin needed
► BivalirudinBivalirudin Bolus 0.75 mg/kg IV**, infusion 1.75 mg/kg/h, not titrated to Bolus 0.75 mg/kg IV**, infusion 1.75 mg/kg/h, not titrated to
ACT; terminated at procedure end unless prolonged ACT; terminated at procedure end unless prolonged antithrombin needed (0.25 mg/kg/hr infusion)antithrombin needed (0.25 mg/kg/hr infusion)
► Glycoprotein IIb/IIIa inhibitorsGlycoprotein IIb/IIIa inhibitors Routine use in UFH arm; recommended only for giant Routine use in UFH arm; recommended only for giant
thrombus or refractory no reflow in bivalirudin armthrombus or refractory no reflow in bivalirudin arm Abciximab or double bolus eptifibatide as per investigator Abciximab or double bolus eptifibatide as per investigator
discretion – dosing per FDA label, renal adjusted; continued discretion – dosing per FDA label, renal adjusted; continued for 12for 12 (abcx) or 12-18 (abcx) or 12-18 (eptif) (eptif)
* If pre randomization UFH administered, ACT is checked first* If pre randomization UFH administered, ACT is checked first** If pre randomization UFH administered, started 30’ after last bolus** If pre randomization UFH administered, started 30’ after last bolus
Study Medications (ii)Study Medications (ii)► AspirinAspirin
324 mg chewed non enteric coated or 500 mg IV in the ER, followed 324 mg chewed non enteric coated or 500 mg IV in the ER, followed by 300-325 mg/day in-hospital and 75-81 mg/day as out patient by 300-325 mg/day in-hospital and 75-81 mg/day as out patient indefinitelyindefinitely
► ThienopyridinesThienopyridines Clopidogrel 300 mg or 600 mg loading dose (per investigator Clopidogrel 300 mg or 600 mg loading dose (per investigator
discretion) in the ER followed by 75 mg PO QD for at least 6 months discretion) in the ER followed by 75 mg PO QD for at least 6 months (1 year or longer recommended(1 year or longer recommended))• Ticlopidine load + daily dose permissible if clopiodgrel is unavailable or Ticlopidine load + daily dose permissible if clopiodgrel is unavailable or
patient is allergicpatient is allergic
► OtherOther Beta blockers: IV pre procedure followed by PO QD in the absence Beta blockers: IV pre procedure followed by PO QD in the absence
of contraindications; ACE inhibitors for HTN, CHF or LVEF <40%; of contraindications; ACE inhibitors for HTN, CHF or LVEF <40%; Statin if LDL >100 mg/dlStatin if LDL >100 mg/dl
2 Primary Endpoints (at 30 Days)2 Primary Endpoints (at 30 Days)
1) Net Adverse Clinical Events1) Net Adverse Clinical Events
2) Major Bleeding (non CABG)2) Major Bleeding (non CABG)• Intracranial bleeding• intraocular bleeding
• Retroperitoneal bleeding• Access site bleed requiring
intervention/surgery• Hematoma ≥5 cm
• Hgb ≥3g/dL with an overt source• Hgb ≥4g/dL w/o overt source
• Reoperation for bleeding• Blood product transfusion
and
2 Primary Endpoints (at 30 Days)2 Primary Endpoints (at 30 Days)
1) Net Adverse Clinical Events1) Net Adverse Clinical Events
2) Major Bleeding (non CABG)2) Major Bleeding (non CABG)==
oror
• All cause deathAll cause death• ReinfarctionReinfarction
• Ischemic TVRIschemic TVR• StrokeStroke
Major adverseMajor adversecardiovascular eventscardiovascular events
(major secondary endpoint)(major secondary endpoint)
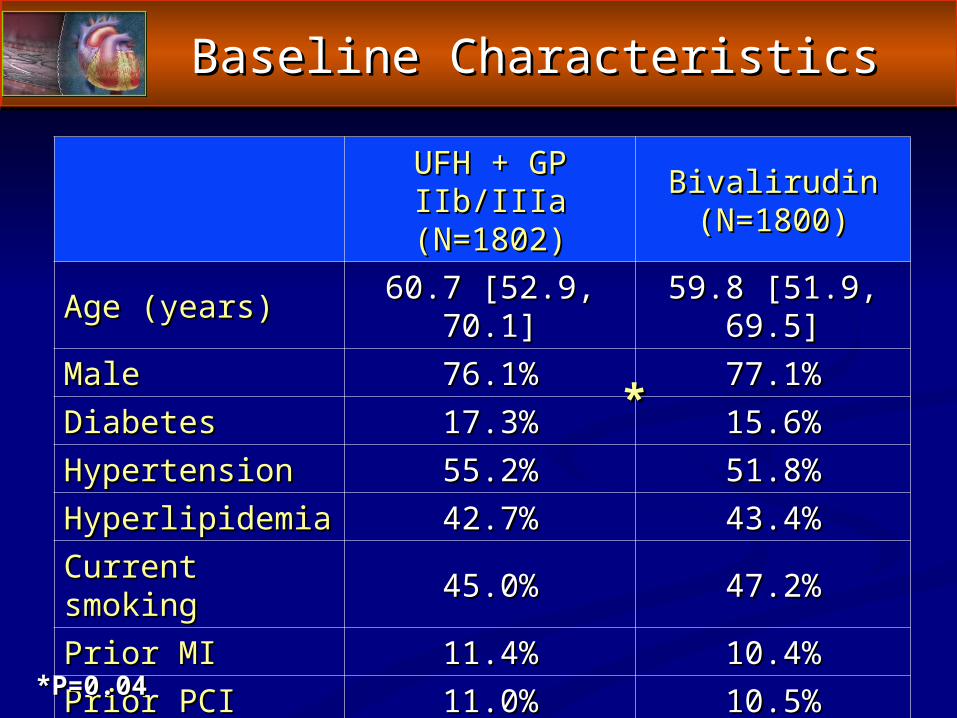
Baseline CharacteristicsBaseline Characteristics
UFH + GP IIb/IIIaUFH + GP IIb/IIIa(N=1802)(N=1802)
BivalirudinBivalirudin(N=1800)(N=1800)
Age (years)Age (years) 60.7 [52.9, 70.1]60.7 [52.9, 70.1] 59.8 [51.9, 69.5]59.8 [51.9, 69.5]MaleMale 76.1%76.1% 77.1%77.1%DiabetesDiabetes 17.3%17.3% 15.6%15.6%HypertensionHypertension 55.2%55.2% 51.8%51.8%HyperlipidemiaHyperlipidemia 42.7%42.7% 43.4%43.4%Current smokingCurrent smoking 45.0%45.0% 47.2%47.2%Prior MIPrior MI 11.4%11.4% 10.4%10.4%Prior PCIPrior PCI 11.0%11.0% 10.5%10.5%Prior CABGPrior CABG 2.6%2.6% 3.3%3.3%
*P=0.04*P=0.04
**
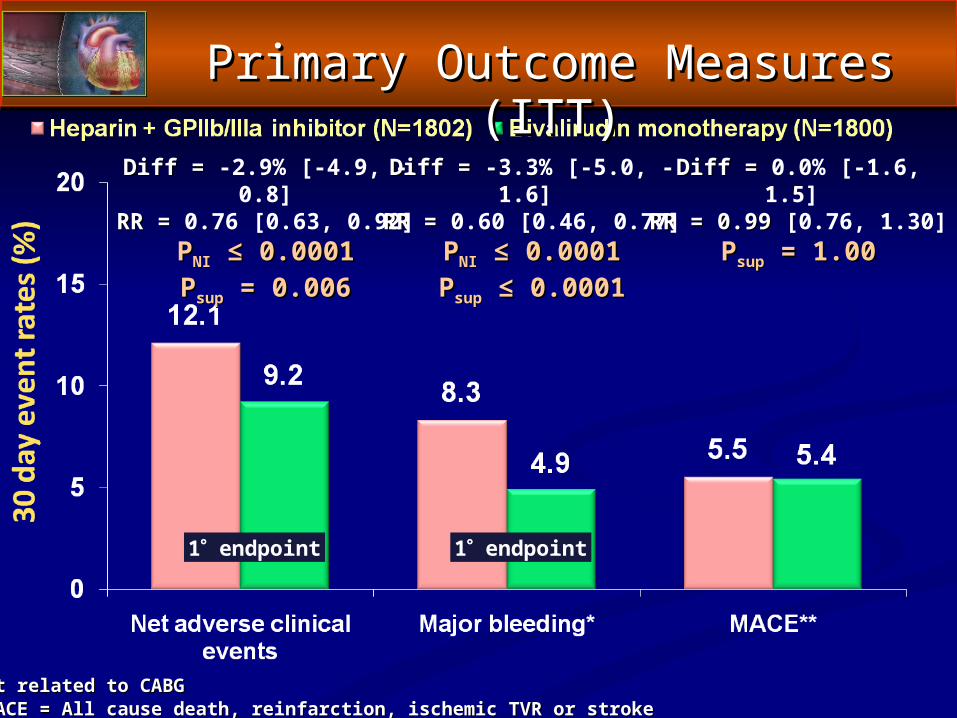
Diff = Diff = 0.0% [-1.6, 1.5] RR = 0.99RR = 0.99 [0.76, 1.30]
PPsupsup = 1.00 = 1.00
Primary Outcome Measures (ITT)Primary Outcome Measures (ITT)
Diff = Diff = -3.3% [-5.0, -1.6] RR = RR = 0.60 [0.46, 0.77]
PPNINI ≤ 0.0001 ≤ 0.0001PPsupsup ≤ 0.0001 ≤ 0.0001
Diff = Diff = -2.9% [-4.9, -0.8]RR = RR = 0.76 [0.63, 0.92]
PPNINI ≤ 0.0001 ≤ 0.0001PPsupsup = 0.006 = 0.006
1 endpoint 1 endpoint
*Not related to CABG*Not related to CABG**MACE = All cause death, reinfarction, ischemic TVR or stroke**MACE = All cause death, reinfarction, ischemic TVR or stroke
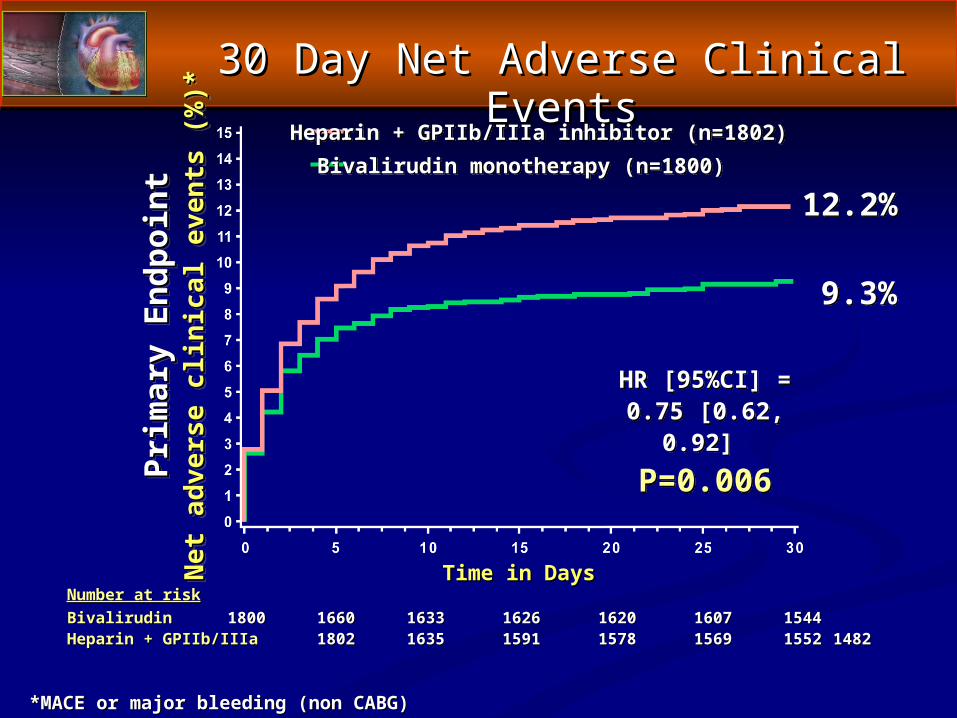
30 Day Net Adverse Clinical Events30 Day Net Adverse Clinical Events
*MACE or major bleeding (non CABG)*MACE or major bleeding (non CABG)
Number at riskNumber at riskBivalirudinBivalirudin 18001800 16601660 16331633 16261626 16201620 16071607 15441544Heparin + GPIIb/IIIaHeparin + GPIIb/IIIa 18021802 16351635 15911591 15781578 15691569 15521552 14821482
Prim
ary
Endp
oint
Prim
ary
Endp
oint
Net
adv
erse
clin
ical
eve
nts
(%)*
Net
adv
erse
clin
ical
eve
nts
(%)*
Time in DaysTime in Days
12.2%
9.3%
HR [95%CI] =0.75 [0.62, 0.92]
P=0.006
Heparin + GPIIb/IIIa inhibitor (n=1802)Bivalirudin monotherapy (n=1800)
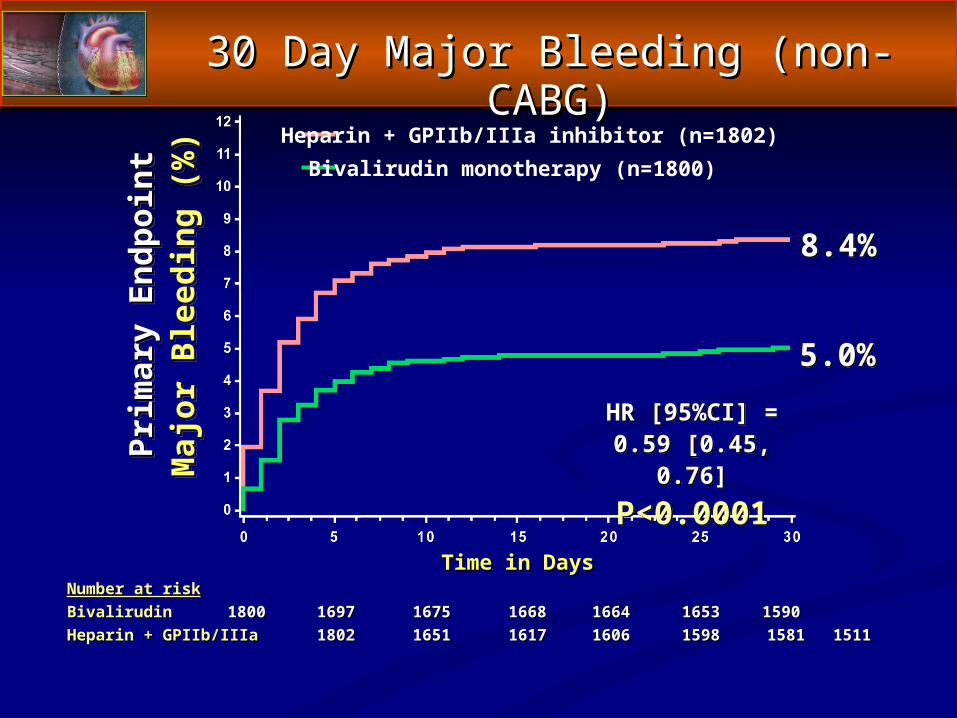
Number at riskNumber at riskBivalirudinBivalirudin 18001800 16971697 16751675 16681668 16641664 16531653 15901590 Heparin + GPIIb/IIIaHeparin + GPIIb/IIIa 18021802 16511651 16171617 16061606 15981598 15811581 15111511
Prim
ary
Endp
oint
Prim
ary
Endp
oint
Maj
or B
leed
ing
(%)
Maj
or B
leed
ing
(%)
Time in DaysTime in Days
8.4%
5.0%HR [95%CI] =
0.59 [0.45, 0.76]P<0.0001
Heparin + GPIIb/IIIa inhibitor (n=1802)Bivalirudin monotherapy (n=1800)
30 Day Major Bleeding (non-CABG)30 Day Major Bleeding (non-CABG)
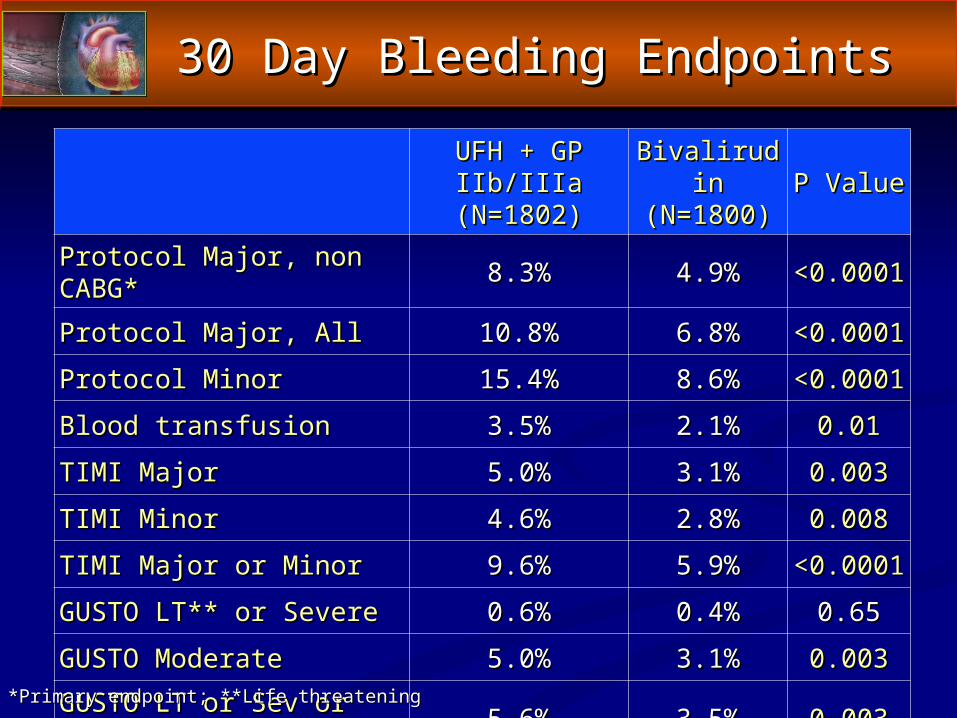
30 Day Bleeding Endpoints30 Day Bleeding Endpoints
UFH + GP IIb/IIIaUFH + GP IIb/IIIa(N=1802)(N=1802)
BivalirudinBivalirudin(N=1800)(N=1800) P ValueP Value
Protocol Major, non CABG*Protocol Major, non CABG* 8.3%8.3% 4.9%4.9% <0.0001<0.0001
Protocol Major, AllProtocol Major, All 10.8%10.8% 6.8%6.8% <0.0001<0.0001
Protocol MinorProtocol Minor 15.4%15.4% 8.6%8.6% <0.0001<0.0001
Blood transfusionBlood transfusion 3.5%3.5% 2.1%2.1% 0.010.01
TIMI MajorTIMI Major 5.0%5.0% 3.1%3.1% 0.0030.003
TIMI MinorTIMI Minor 4.6%4.6% 2.8%2.8% 0.0080.008
TIMI Major or MinorTIMI Major or Minor 9.6%9.6% 5.9%5.9% <0.0001<0.0001
GUSTO LT** or SevereGUSTO LT** or Severe 0.6%0.6% 0.4%0.4% 0.650.65
GUSTO ModerateGUSTO Moderate 5.0%5.0% 3.1%3.1% 0.0030.003
GUSTO LT or Sev or ModGUSTO LT or Sev or Mod 5.6%5.6% 3.5%3.5% 0.0030.003*Primary endpoint; **Life threatening*Primary endpoint; **Life threatening
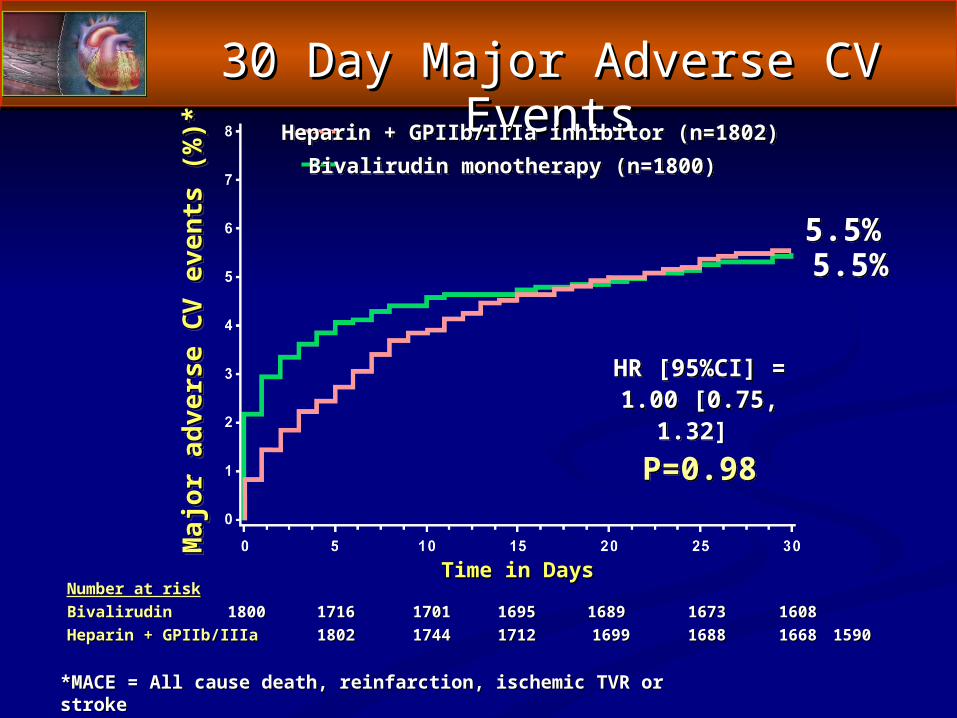
30 Day Major Adverse CV Events30 Day Major Adverse CV Events
Number at riskNumber at riskBivalirudinBivalirudin 18001800 17161716 17011701 1695 1695 1689 1689 16731673 1608 1608 Heparin + GPIIb/IIIaHeparin + GPIIb/IIIa 18021802 17441744 1712 1712 16991699 16881688 1668 1668 15901590
Maj
or a
dver
se C
V ev
ents
(%)*
Maj
or a
dver
se C
V ev
ents
(%)*
Time in DaysTime in Days
5.5%5.5%
HR [95%CI] =1.00 [0.75, 1.32]
P=0.98
Heparin + GPIIb/IIIa inhibitor (n=1802)Bivalirudin monotherapy (n=1800)
*MACE = All cause death, reinfarction, ischemic TVR or stroke*MACE = All cause death, reinfarction, ischemic TVR or stroke
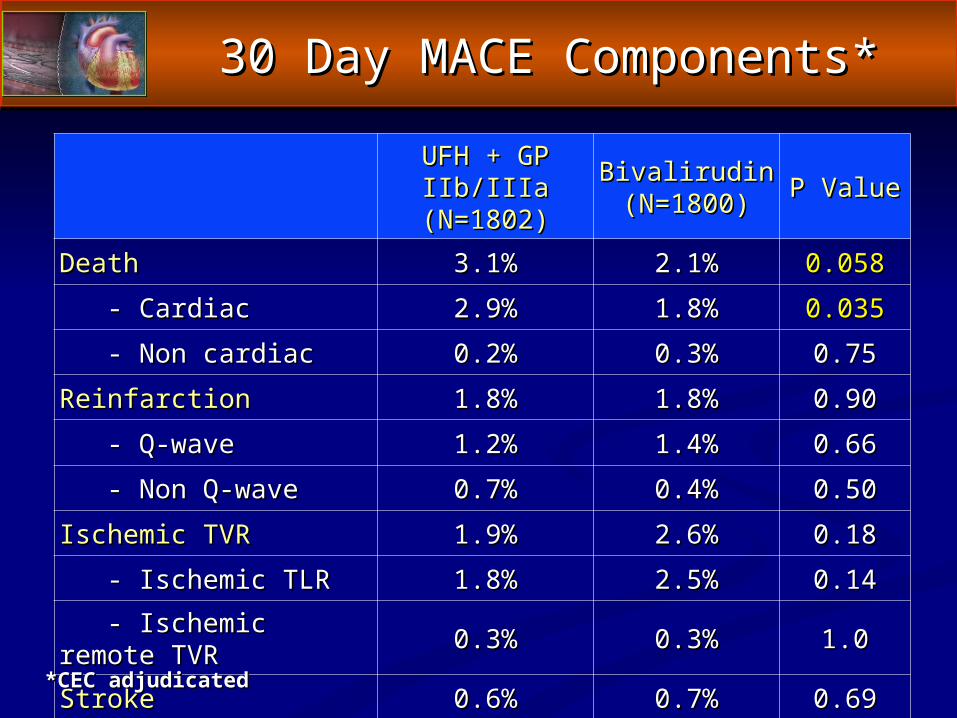
30 Day MACE Components*30 Day MACE Components*
UFH + GP IIb/IIIaUFH + GP IIb/IIIa(N=1802)(N=1802)
BivalirudinBivalirudin(N=1800)(N=1800) P ValueP Value
DeathDeath 3.1%3.1% 2.1%2.1% 0.0580.058
- Cardiac- Cardiac 2.9%2.9% 1.8%1.8% 0.0350.035
- Non cardiac- Non cardiac 0.2%0.2% 0.3%0.3% 0.750.75
ReinfarctionReinfarction 1.8%1.8% 1.8%1.8% 0.900.90
- Q-wave- Q-wave 1.2%1.2% 1.4%1.4% 0.660.66
- Non Q-wave- Non Q-wave 0.7%0.7% 0.4%0.4% 0.500.50
Ischemic TVRIschemic TVR 1.9%1.9% 2.6%2.6% 0.180.18
- Ischemic TLR- Ischemic TLR 1.8%1.8% 2.5%2.5% 0.140.14
- Ischemic remote TVR- Ischemic remote TVR 0.3%0.3% 0.3%0.3% 1.01.0
StrokeStroke 0.6%0.6% 0.7%0.7% 0.690.69*CEC adjudicated*CEC adjudicated
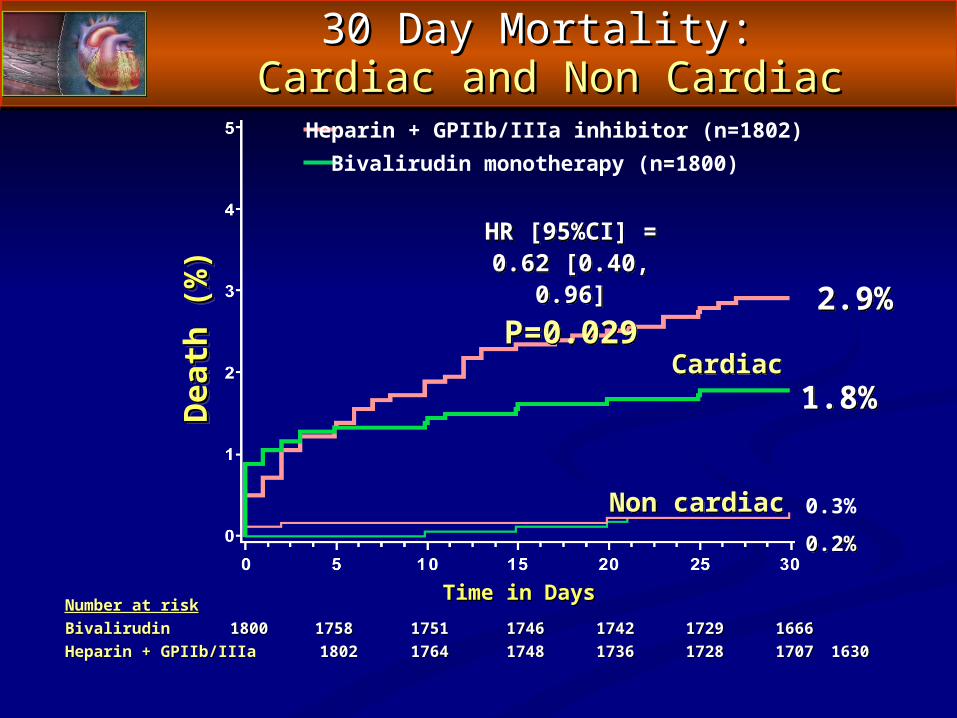
30 Day Mortality: 30 Day Mortality: Cardiac and Non CardiacCardiac and Non Cardiac
Number at riskNumber at riskBivalirudinBivalirudin 1800 1800 17581758 17511751 17461746 17421742 17291729 16661666Heparin + GPIIb/IIIaHeparin + GPIIb/IIIa 1802 1802 17641764 17481748 17361736 17281728 17071707 16301630
Dea
th (%
)D
eath
(%)
Time in DaysTime in Days
2.9%
1.8%
Heparin + GPIIb/IIIa inhibitor (n=1802)Bivalirudin monotherapy (n=1800)
0.3%
0.2%
Cardiac
Non cardiac
HR [95%CI] =0.62 [0.40, 0.96]
P=0.029
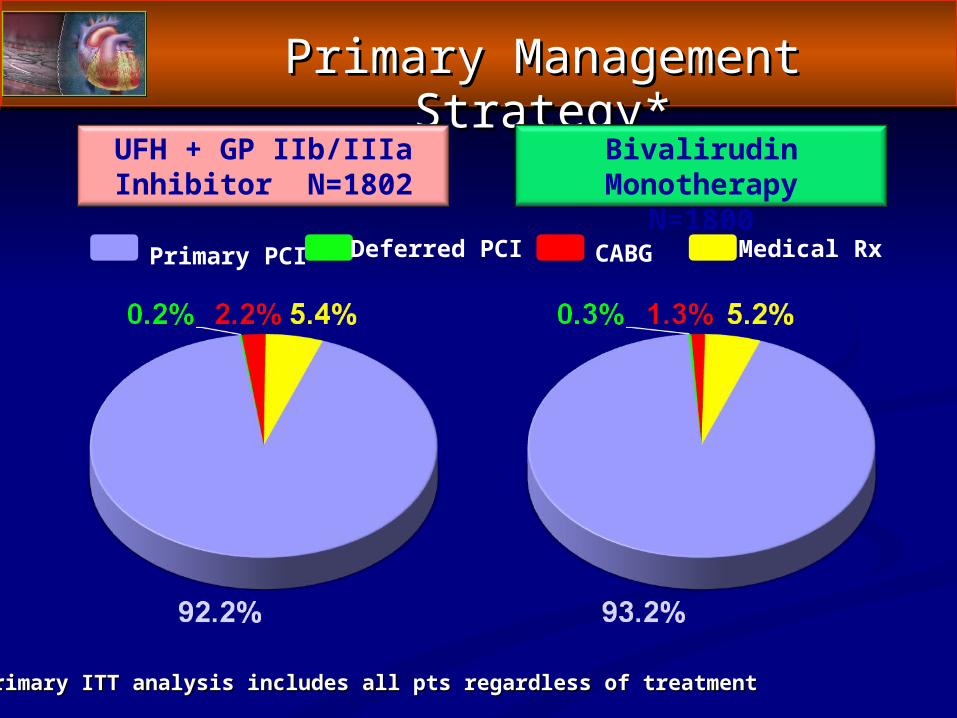
Primary Management Strategy*Primary Management Strategy*
UFH + GP IIb/IIIa Inhibitor N=1802
Bivalirudin MonotherapyN=1800
Primary PCI Deferred PCI CABG Medical Rx
*Primary ITT analysis includes all pts regardless of treatment*Primary ITT analysis includes all pts regardless of treatment
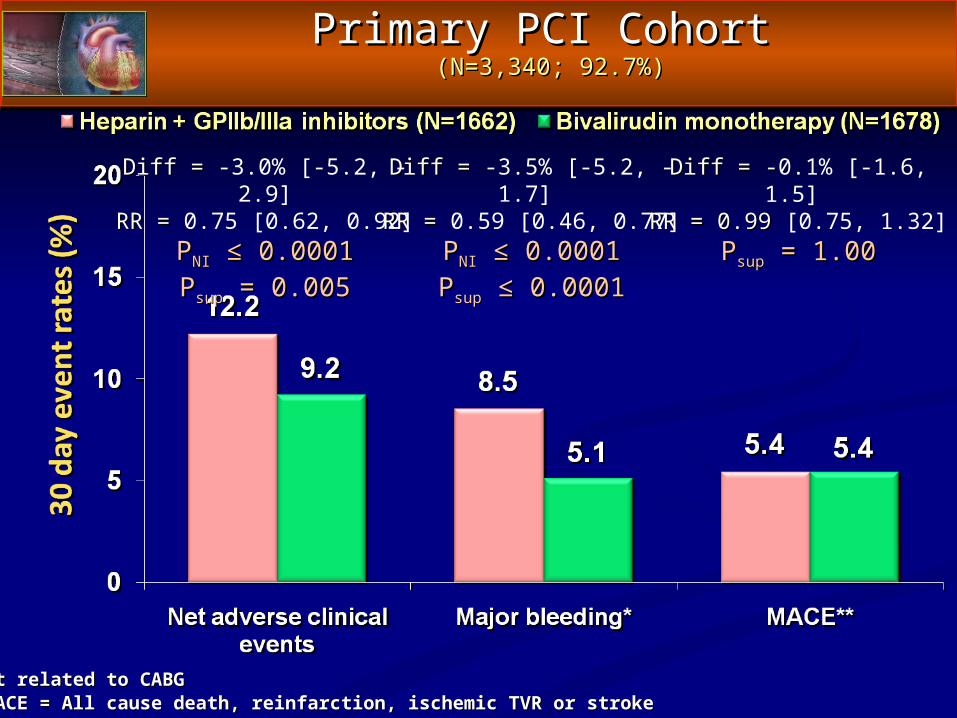
Primary PCI CohortPrimary PCI Cohort (N=3,340; 92.7%)(N=3,340; 92.7%)
Diff = -Diff = -0.1% [-1.6, 1.5] RR = 0.99RR = 0.99 [0.75, 1.32]
PPsupsup = 1.00 = 1.00
Diff = Diff = -3.5% [-5.2, -1.7] RR = RR = 0.59 [0.46, 0.77]
PPNINI ≤ 0.0001 ≤ 0.0001PPsupsup ≤ 0.0001 ≤ 0.0001
Diff = Diff = -3.0% [-5.2, -2.9]RR = RR = 0.75 [0.62, 0.92]
PPNINI ≤ 0.0001 ≤ 0.0001PPsupsup = 0.005 = 0.005
*Not related to CABG*Not related to CABG**MACE = All cause death, reinfarction, ischemic TVR or stroke**MACE = All cause death, reinfarction, ischemic TVR or stroke
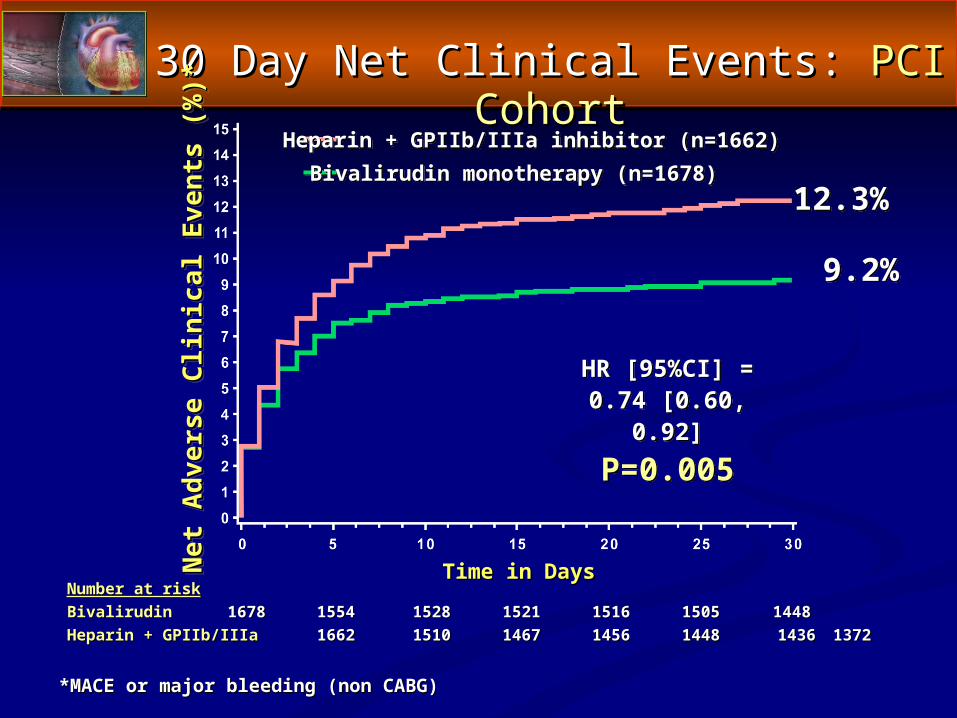
30 Day Net Clinical Events: 30 Day Net Clinical Events: PCI CohortPCI Cohort
*MACE or major bleeding (non CABG)*MACE or major bleeding (non CABG)
Number at riskNumber at riskBivalirudinBivalirudin 16781678 15541554 15281528 15211521 15161516 15051505 1448 1448 Heparin + GPIIb/IIIaHeparin + GPIIb/IIIa 16621662 15101510 14671467 14561456 14481448 14361436 13721372
Net
Adv
erse
Clin
ical
Eve
nts
(%)*
Net
Adv
erse
Clin
ical
Eve
nts
(%)*
Time in DaysTime in Days
12.3%
9.2%
HR [95%CI] =0.74 [0.60, 0.92]
P=0.005
Heparin + GPIIb/IIIa inhibitor (n=1662)Bivalirudin monotherapy (n=1678)
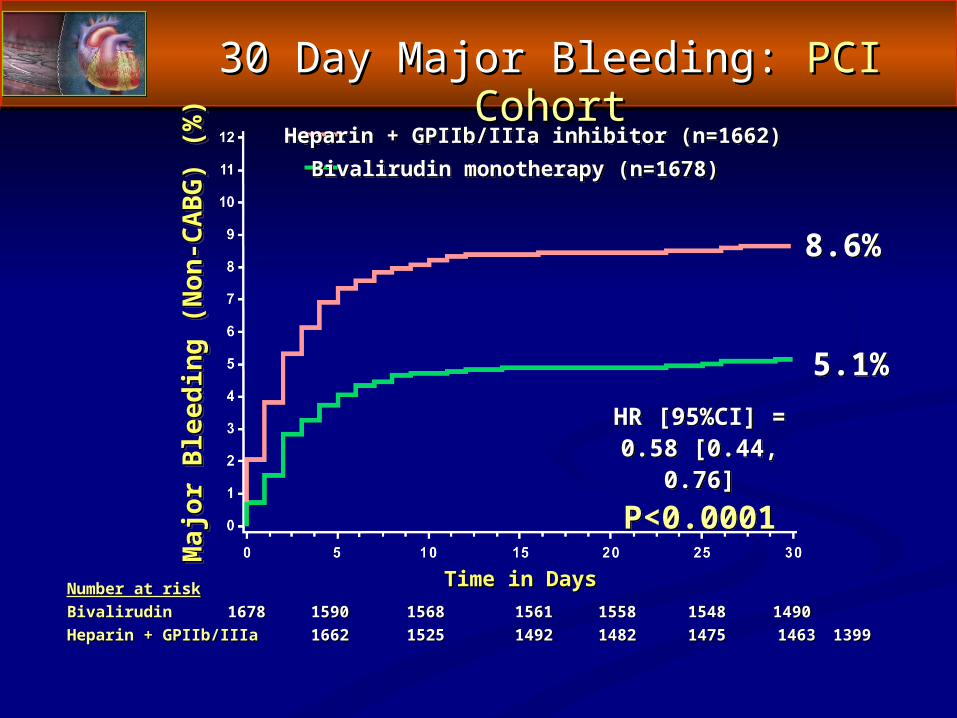
30 Day Major Bleeding: 30 Day Major Bleeding: PCI CohortPCI Cohort
Number at riskNumber at riskBivalirudinBivalirudin 16781678 15901590 15681568 15611561 15581558 15481548 1490 1490 Heparin + GPIIb/IIIaHeparin + GPIIb/IIIa 16621662 15251525 14921492 14821482 14751475 14631463 13991399
Maj
or B
leed
ing
(Non
-CA
BG
) (%
)M
ajor
Ble
edin
g (N
on-C
AB
G) (
%)
Time in DaysTime in Days
8.6%
5.1%HR [95%CI] =
0.58 [0.44, 0.76]P<0.0001
Heparin + GPIIb/IIIa inhibitor (n=1662)Bivalirudin monotherapy (n=1678)
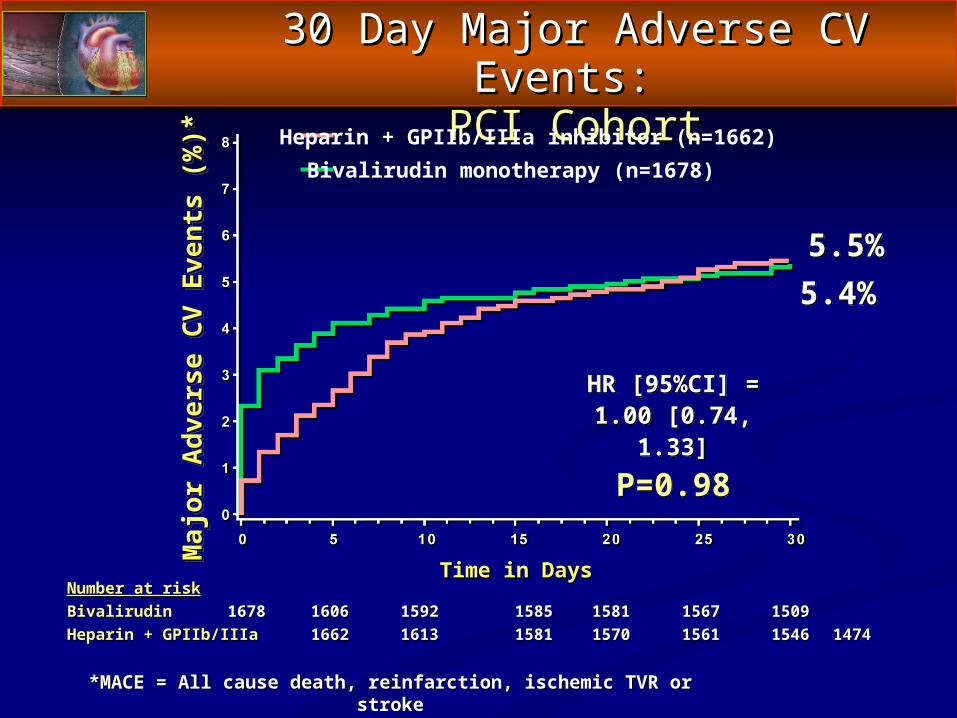
30 Day Major Adverse CV Events:30 Day Major Adverse CV Events: PCI CohortPCI Cohort
*MACE = All cause death, reinfarction, ischemic TVR or stroke*MACE = All cause death, reinfarction, ischemic TVR or stroke
Number at riskNumber at riskBivalirudinBivalirudin 16781678 16061606 15921592 15851585 15811581 15671567 15091509Heparin + GPIIb/IIIaHeparin + GPIIb/IIIa 16621662 16131613 15811581 15701570 15611561 15461546 14741474
Maj
or A
dver
se C
V Ev
ents
(%)*
Maj
or A
dver
se C
V Ev
ents
(%)*
Time in DaysTime in Days
5.5%5.4%
Heparin + GPIIb/IIIa inhibitor (n=1662)Bivalirudin monotherapy (n=1678)
HR [95%CI] =1.00 [0.74, 1.33]
P=0.98
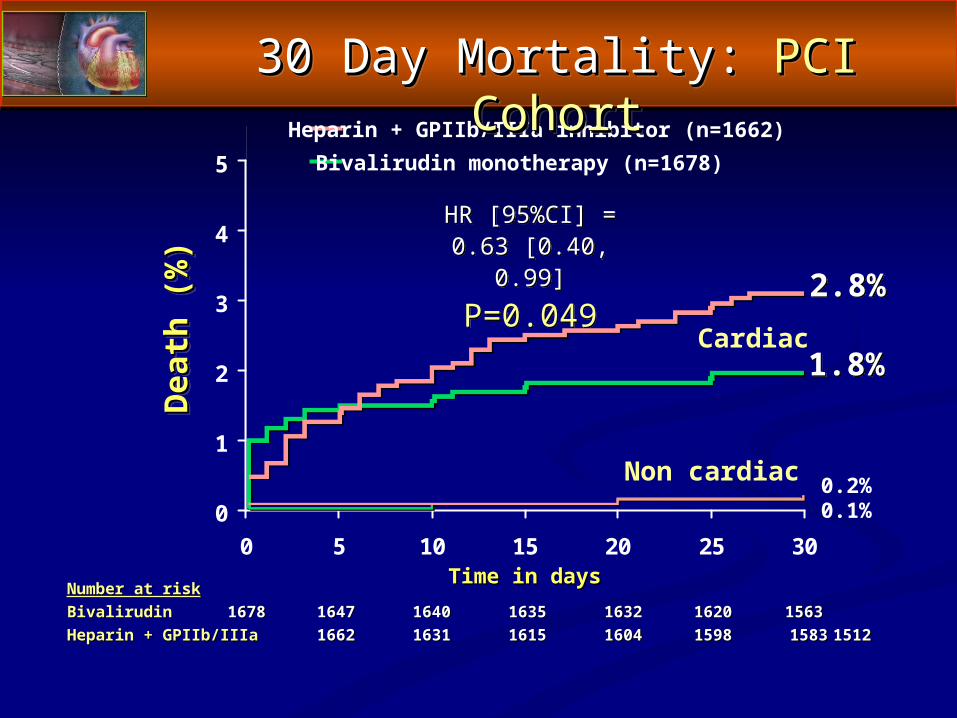
Number at riskNumber at riskBivalirudin Bivalirudin 16781678 16471647 16401640 16351635 16321632 16201620 1563 1563 Heparin + GPIIb/IIIa Heparin + GPIIb/IIIa 16621662 16311631 16151615 16041604 15981598 15831583 1512 1512
Dea
th (%
)D
eath
(%)
Time in daysTime in days
1.8%
Heparin + GPIIb/IIIa inhibitor (n=1662)Bivalirudin monotherapy (n=1678)
0.2%0.1%
Cardiac
Non cardiac
30 Day Mortality: 30 Day Mortality: PCI CohortPCI Cohort
0
1
2
3
4
5
0 5 10 15 20 25 30
2.8%
HR [95%CI] =0.63 [0.40, 0.99]
P=0.049
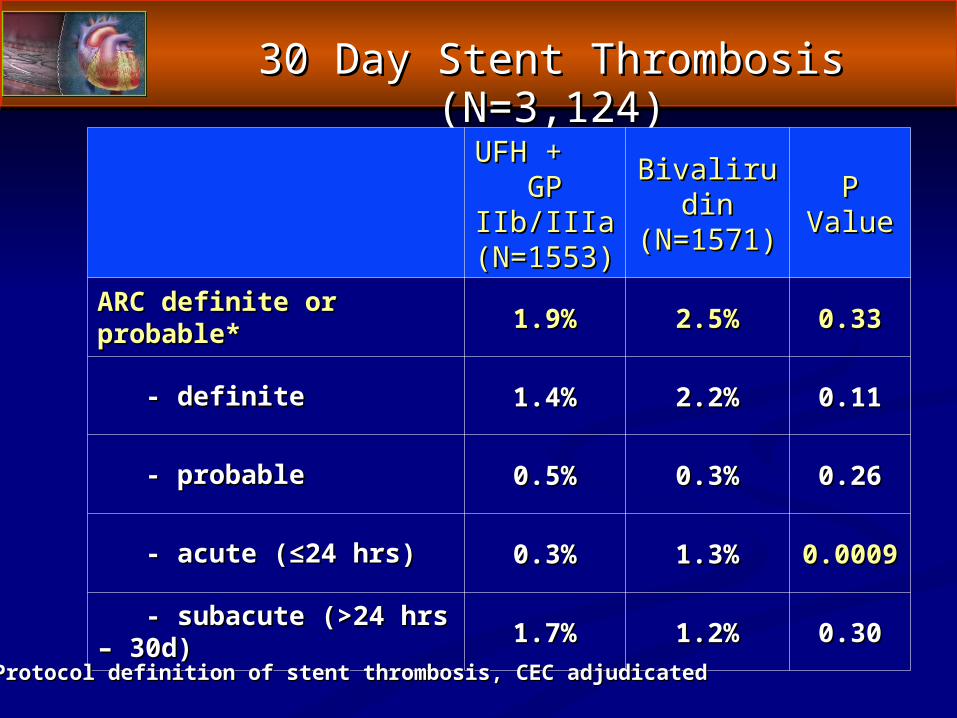
30 Day Stent Thrombosis (N=3,124)30 Day Stent Thrombosis (N=3,124)
UFH + UFH + GP IIb/IIIaGP IIb/IIIa(N=1553)(N=1553)
BivalirudinBivalirudin(N=1571)(N=1571)
PPValueValue
ARC definite or probable*ARC definite or probable* 1.9%1.9% 2.5%2.5% 0.330.33
- definite- definite 1.4%1.4% 2.2%2.2% 0.110.11
- probable- probable 0.5%0.5% 0.3%0.3% 0.260.26
- acute (≤24 hrs)- acute (≤24 hrs) 0.3%0.3% 1.3%1.3% 0.00090.0009
- subacute (>24 hrs – 30d)- subacute (>24 hrs – 30d) 1.7%1.7% 1.2%1.2% 0.300.30
*Protocol definition of stent thrombosis, CEC adjudicated*Protocol definition of stent thrombosis, CEC adjudicated
ConclusionsConclusions
► In this large scale, prospective, randomized trial of pts In this large scale, prospective, randomized trial of pts with STEMI undergoing a primary PCI management with STEMI undergoing a primary PCI management strategy, compared to UFH plus the routine use of GP strategy, compared to UFH plus the routine use of GP IIb/IIIa inhibitors, bivalirudin monotherapy with GP IIb/IIIa inhibitors, bivalirudin monotherapy with GP IIb/IIIa inhibitors reserved for suboptimal PCI IIb/IIIa inhibitors reserved for suboptimal PCI outcomes resulted in:outcomes resulted in:
A significant 24% reduction in the 30 day primary A significant 24% reduction in the 30 day primary endpoint of net adverse clinical eventsendpoint of net adverse clinical events
A significant 40% reduction in the 30 day primary A significant 40% reduction in the 30 day primary endpoint of major bleedingendpoint of major bleeding
► Risk Stratification is an essential function of the ED Risk Stratification is an essential function of the ED evaluation.evaluation.
► ““Treatment stratification” must be coupled to risk Treatment stratification” must be coupled to risk stratification.stratification.
► Risk stratification must be considered for bleeding as Risk stratification must be considered for bleeding as well as ischemia.well as ischemia.
► Time issues also direct therapeutic choices, but Time issues also direct therapeutic choices, but management of these issues must be multidisciplinary.management of these issues must be multidisciplinary.
► We now have evidence across the ACS spectrum that We now have evidence across the ACS spectrum that bivalirudin is associated with superior bleeding bivalirudin is associated with superior bleeding outcomes.outcomes.
► A seamless transition of care is most likely to result in A seamless transition of care is most likely to result in good outcomes.good outcomes.
Optimal Management of ACS Optimal Management of ACS ED to Cardiology — Summary and Game PlanED to Cardiology — Summary and Game Plan
Chairman and Distinguished FacultyChairman and Distinguished Faculty
Where Metal Meets Thrombus and Where Metal Meets Thrombus and Vascular EndotheliumVascular Endothelium
A Case Study Analysis of Upstream InterventionsA Case Study Analysis of Upstream Interventions
Getting in the ACS Stream of ThingsGetting in the ACS Stream of Things
ACS Case Presentation #1ACS Case Presentation #1
► 77 year old female presents to ED with 2 weeks of 77 year old female presents to ED with 2 weeks of progressive angina, one episode lasting 90 minutesprogressive angina, one episode lasting 90 minutes History of Type 2 DM, HTN, cigarette smokingHistory of Type 2 DM, HTN, cigarette smoking Weight 65 kgWeight 65 kg
► ECG non-specific, POS TnI 0.79 (ULN 0.5), nl CKMB, ECG non-specific, POS TnI 0.79 (ULN 0.5), nl CKMB, CrCL 40 ml/min, Hgb 9.7 g/dlCrCL 40 ml/min, Hgb 9.7 g/dl
► Given ASA, 300 mg clopidogrel, 5 mg IV metoprolol, IV Given ASA, 300 mg clopidogrel, 5 mg IV metoprolol, IV NTGNTG
► Continued chest painContinued chest pain Anticoagulation options in the ED?Anticoagulation options in the ED? Risk stratification strategy?Risk stratification strategy? Which upstream strategy makes most sense?Which upstream strategy makes most sense? Collaboration with cardiology colleagues?Collaboration with cardiology colleagues?
► Decision made to pursue rapid invasive risk Decision made to pursue rapid invasive risk stratificationstratification High-risk featuresHigh-risk features
• Elevated troponinElevated troponin• Ongoing chest pain despiteOngoing chest pain despite
medical therapymedical therapy
► AntithrombinAntithrombin therapy choicestherapy choices Risk for bleedingRisk for bleeding
• Age, Female sex, renalAge, Female sex, renalinsufficiency, anemiainsufficiency, anemia
Bivalirudin bolus and drip initiatedBivalirudin bolus and drip initiated
► AngiographyAngiography
ACS Case Presentation #1ACS Case Presentation #1
► A 76 year-old white male with h/o stent to LAD 1 year A 76 year-old white male with h/o stent to LAD 1 year agoago
► Presents with multiple episodes of recurrent chest pain Presents with multiple episodes of recurrent chest pain including rest pain over 2 daysincluding rest pain over 2 days
► Pain similar to time of PCI in pastPain similar to time of PCI in past► Symptoms relieved in ED with sl NTGSymptoms relieved in ED with sl NTG► PMH: IDDM, HTN, CHOL elevationPMH: IDDM, HTN, CHOL elevation► PE: benign (weight 84 kg).PE: benign (weight 84 kg).► Labs: Labs: Hgb 10.7Hgb 10.7, , Cr 1.9,Cr 1.9, CK 173/2, Tr <0.03. CK 173/2, Tr <0.03.► ECG (next slide)ECG (next slide)
ACS Case Presentation #2ACS Case Presentation #2
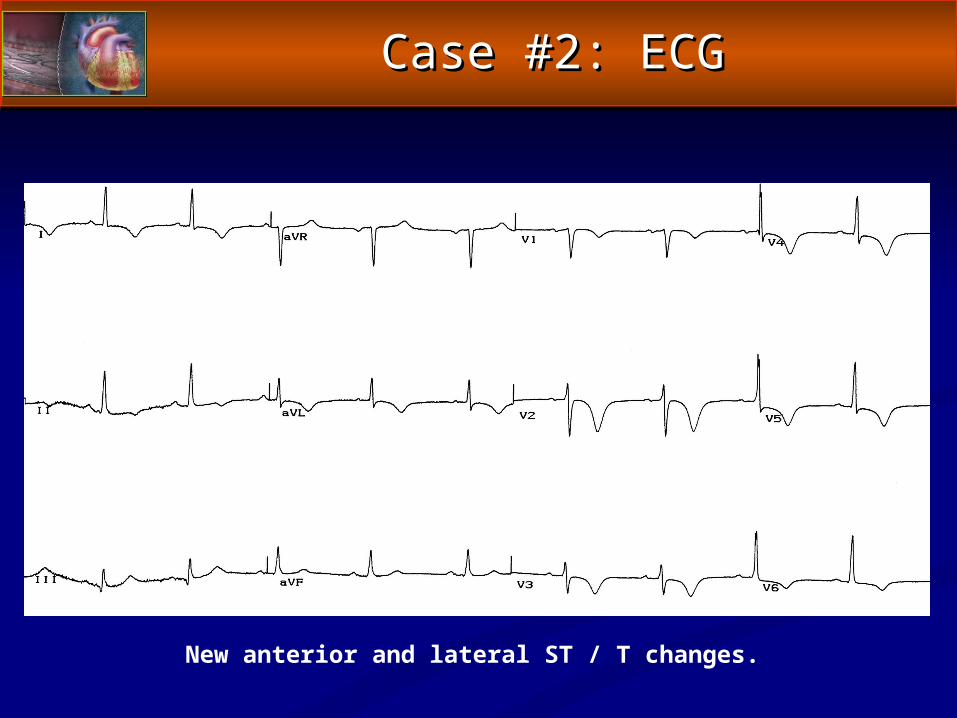
New anterior and lateral ST / T changes.
Case #2: ECGCase #2: ECG
Based on your clinical assessment, this patient’s risk of Based on your clinical assessment, this patient’s risk of short-term (30-Day) ischemic events is:short-term (30-Day) ischemic events is:
A.A. LowLow
B.B. ModerateModerate
C.C. HighHigh
D.D. Very highVery high
ACS Case Presentation #2ACS Case Presentation #2
Which of this patient’s baseline factors do you consider most Which of this patient’s baseline factors do you consider most important for determining this patient’s ischemic risk?important for determining this patient’s ischemic risk?
A.A. Advanced age Advanced age
B.B. Anginal pattern Anginal pattern
C.C. ECG findings ECG findings
D.D. Biomarkers Biomarkers
*
ACS Case Presentation #2ACS Case Presentation #2
Based on your clinical assessment, this patient’s risk of incurring Based on your clinical assessment, this patient’s risk of incurring a short-term (30-Day) hemorrhagic event related to PCI is:a short-term (30-Day) hemorrhagic event related to PCI is:
A.A. LowLow
B.B. ModerateModerate
C.C. HighHigh
D.D. Very highVery high
ACS Case Presentation #2ACS Case Presentation #2
Which of this patient’s baseline factors do you consider most Which of this patient’s baseline factors do you consider most important for determining hemorrhagic risk?important for determining hemorrhagic risk?
A.A. Advanced age Advanced age
B.B. Hypertension Hypertension
C.C. Impaired creatinine clearance Impaired creatinine clearance
D.D. Anemia Anemia
*
ACS Case Presentation #2ACS Case Presentation #2
In ACS patients, do you alter your choice of anticoagulant/ In ACS patients, do you alter your choice of anticoagulant/ antithrombotic therapy based upon an assessment of the antithrombotic therapy based upon an assessment of the
individual patient’s risk of hemorrhagic complications?individual patient’s risk of hemorrhagic complications?
A.A. Yes Yes
B.B. No No
*
ACS Case Presentation #2ACS Case Presentation #2
Among those of you who Among those of you who wouldwould alter or customize alter or customize antithrombotic therapy based on an ACS patient’s risk for antithrombotic therapy based on an ACS patient’s risk for hemorrhage in the setting of PCI, which of the following hemorrhage in the setting of PCI, which of the following
baseline characteristics would you consider most important baseline characteristics would you consider most important in supporting the use of a “hemorrhage-minimizing” in supporting the use of a “hemorrhage-minimizing”
anithrombotic regimen:anithrombotic regimen:
A.A. Elderly and femaleElderly and female
B.B. Renal insufficiency and positive biomarkersRenal insufficiency and positive biomarkers
C.C. Anemia and high risk ischemic featuresAnemia and high risk ischemic features
*
ACS Case Presentation #2ACS Case Presentation #2
What would you likely use for anticoagulation in this patient, What would you likely use for anticoagulation in this patient, prior to catheterization, if you anticipated catheterization prior to catheterization, if you anticipated catheterization
would occur in would occur in 4 hours or less?4 hours or less?
A.A. Unfractionated heparin alone Unfractionated heparin alone
B.B. Enoxaparin alone Enoxaparin alone
C.C. Bivalirudin alone Bivalirudin alone
D.D. A heparin with a GP IIb/IIIa inhibitor A heparin with a GP IIb/IIIa inhibitor
E.E. FondaparinuxFondaparinux
*
ACS Case Presentation #2ACS Case Presentation #2
What would your choice of upstream anticoagulation therapy What would your choice of upstream anticoagulation therapy be, if you anticipated cardiac catheterization be, if you anticipated cardiac catheterization the same day the same day
(within 12 hours)?(within 12 hours)?
A.A. Unfractionated heparin alone Unfractionated heparin alone
B.B. Enoxaparin alone Enoxaparin alone
C.C. Bivalirudin alone Bivalirudin alone
D.D. A heparin with a GP IIb/IIIa inhibitor A heparin with a GP IIb/IIIa inhibitor
E.E. FondaparinuxFondaparinux
*
ACS Case Presentation #2ACS Case Presentation #2
What would your choice of upstream anticoagulation therapy What would your choice of upstream anticoagulation therapy be, if you anticipated cardiac catheterization be, if you anticipated cardiac catheterization the next day the next day
(within 24 hours)?(within 24 hours)?
A.A. Unfractionated heparin alone Unfractionated heparin alone
B.B. Enoxaparin alone Enoxaparin alone
C.C. Bivalirudin alone Bivalirudin alone
D.D. A heparin with a GP IIb/IIIa inhibitor A heparin with a GP IIb/IIIa inhibitor
E.E. FondaparinuxFondaparinux
*
ACS Case Presentation #2ACS Case Presentation #2
At this point, your anticoagulation regimen for PCI in this At this point, your anticoagulation regimen for PCI in this patient would be?patient would be?
A.A. Additional heparin Additional heparin
B.B. Switch to enoxaparin Switch to enoxaparin
C.C. Switch to bivalirudin Switch to bivalirudin
D.D. Additional heparin plus GP IIb/IIIa inhibitor Additional heparin plus GP IIb/IIIa inhibitor
*
ACS Case Presentation #2ACS Case Presentation #2