Embed Size (px)
Citation preview
5302018
1
What Should We Look at When Evaluating Neonates
Building Our Capacity as Providers to Better Support Babies and
Families
Gerri A Duran MS OTL FAOTA
Occupational Therapist UNM Developmental Care Program
gduransaludunmedu
Pager 1-505-380-0776
Mobile (textcall 505-238-7223)
2018 NM FIT Annual Meeting 1
Agendabull wwwmenticom
bull 1000 Objectives
bull Overview of infant amp preterm infant development
bull NICU diagnoses that place a baby at risk for developmental delay
bull FIT 2017 PPT
bull 1015 DDSD Regulations
bull ldquoManrdquo does not
bull live by bread alone ndash and not by scores alonehellip
bull ldquoClinicalrdquo observations
bull Alberta Infant Motor Scales (AIMS)
bull Professional ldquoregulationsrdquo
bull High risk for CP
bull 1100 Brainstorming
bull 1115 Q amp A
2018 NM FIT Annual Meeting 2
Objectives
bull What and how should we look at
bull Why should we ask
bull Why is what we see important
bull How do we develop our own capacity
bull How do we support our colleagues as they develop their capacity
2018 NM FIT Annual Meeting 3
5302018
2
Basic Concepts For Todaybull Why we recommend following until they are 2
yo (especially when they are doing okay) bull At Risk Statebull Language and the ldquonext steprdquobull Issues that we see most frequently in SBC
follow-up and first visitsbull Head Shapebull Growth nutrition constipationbull Tummy Timebull Parent stress
2018 NM FIT Annual Meeting 4
Basic Concepts For Todaybull Prematurity
bull When is a baby preterm
bull How long do we correct for prematurity
bull What all gets ldquocorrected forrdquo
bull Everything but shots
2018 NM FIT Annual Meeting 5
Things that you should monitorbull Evaluation of Growth and Nutritionbull Vision and Hearing Screeningbull Ongoing Preventative Carebull Developmental Progressbull Close monitoring of common medical problems of the
preterm infantbull Out-patient specialty visits
bull Pulmonarybull Ophthalmologybull Cardiologybull Nephrologybull SBC
2018 NM FIT Annual Meeting 6
5302018
3
Development
Term
bull Cephalo-caudal (head-to-toe) motor control
bull Proximal to distal (inside-to-outside)
bull Resistancegravity
bull Energy
Preterm
bull Caudal-Cephalo
bull Still proximal-distal
bull Muscle mass
bull Resistancegravity
bull Energy (on O2)
2018 NM FIT Annual Meeting 7
Sensory Systems
bull Cutaneous 12-14 weeks
bull Vestibular 14-15 weeks functioning
bull Chemical- Olfactory (smell ) 24 Gustatory (taste)-17-18
bull Auditory (25 -29)
bull Visual
bull Critical periods of Development
bull Just because they are functioning doesnrsquot mean that they are supposed to be
2018 NM FIT Annual Meeting 8
FIT- frequentbull Meningitis bull Seizures bull BWbull GAbull Growth Restrictionsbull IVHbull Hydrocephalybull Club footbull Hypoglycemia bull HIE (neonatal
encephalopathy)
bull IUDEPDEbull Feeding
DisordersProblemsbull Cleftsbull Gastroschisisbull ROPbull Jaundicebull Trisomy 21bull Syndromesbull Environmentalbull Spina Bifida
2018 NM FIT Annual Meeting 9
5302018
4
NICU diagnoses that place a baby at risk for developmental delay
bull hellipAKA ldquoWhy does UNM NICU pick these babies up and transfer them to yourdquo
bull Cardiac conditions
bull ECMO
bull Cooling
bull ICO
2018 NM FIT Annual Meeting 10
Corrected Gestational Age (CGA)
bull Use until the infant reaches 24-36 months
bull Use for all developmental milestones including introduction of foods
bull The only schedule that should follow the preterm infantrsquos chronological age is their immunization schedule
bull AAP recommends correction until at least age 2 and most until age 3
2018 NM FIT Annual Meeting 11
Neurological Differences
bull When corrected to term the extremely preterm infantrsquos brain
bull Reduced gray matter volume
bull Increased cerebrospinal fluidbull Males have significantly lower white matter volumes
in specific areas
bull These findings persist to school age and are associated with learning challenges
Kesler SR et al J Peds 2008
2018 NM FIT Annual Meeting 12
5302018
5
We are growing brains in the NICU
2018 NM FIT Annual Meeting 13
PerinatalNeonatal Risk Factors
bull Risk Increased likelihood of disability
bull Risk ne disability
bull Many who have disability do not have risk
bull Some risk factors carry a higher risk of disability than others
bull More risk factors will lead to an additive effect
2018 NM FIT Annual Meeting 14
AAP Recommendation Screening
bull In the absence of risk or concernsbull 9 18 and 30 months
bull If surveillance identifies risk then additional screening is needed
bull Surveillance should be continued even if screening does not indicate a risk of delay
2018 NM FIT Annual Meeting 15
5302018
6
Long-term Outcome ndash this is where we come in
bull Complex interplaybull Biologic serves as the strongest predictor of long-
term function and development as the child recovers from perinatal and prenatal insults
bull Genetic and Environmental accounts for more of the variations seen in cognitive developmental
bull In most preterm children a positive environment can ameliorate many biologic risk factors
2018 NM FIT Annual Meeting 16
2 Year Re-hospitalizationOperationsle27 weeks
bull 12 Cerebral Palsy bull 6 mildbull 6 moderatesevere
bull 11 require special equipmentbull 86 bracesorthoticsbull 19 walker
Neonatal Research Network Data 2011
2018 NM FIT Annual Meeting 17
New Mexico Follow-Up Care- HM 14 (2018)
bull Currently we donrsquot have comprehensive care for high-risk neonates
bull UNMHrsquos NICU represents all regions of the State
bull 80 Medicaid
bull 2 No insurance
bull 50-60 from outside of Bernalillo County
bull More than 13 of births are to residents in rural and semi-rural areas
bull Preterm birth is more common in rural areas
bull 104 of children with special health care needs are without a usual source of care
2018 NM FIT Annual Meeting 18
5302018
7
United States Stats as of 2015
bull 4 million births per year
bull Gestational age
bull 96 are preterm (lt37 weeks gestation)
bull 7 late preterm (34-3667 weeks)
bull 26 (le34 weeks)
bull Weight
bull Low Birth Weight (lt2500g)
bull ~8 of annual births
bull ~90 (~288000) of these infants survive to discharge~ 13 will need specialty services
National Vital Statistics Report Vol 65 No 3 Preliminary Data
2018 NM FIT Annual Meeting 19
Plagiocephaly and Torticollis
bull NICU and Back to Sleep
bull Right-sided
bull AAP httpwwwaappublicationsorgnews20161027Plagiocephaly102016
bull Common condition
bull frac14 of US infants w some degree of positional plagiocephaly
bull The incidence has increased since AAP Back to Sleep campaign in 1994 (to prevent SIDS)
2018 NM FIT Annual Meeting 20
What to do about it
bull Ask your motor therapist
bull Ask your pediatrician
bull Do not wait to address itbull Positioningbull Routines
bull Active movements (you do not have to do passive stretch)
bull Best approach bull PREVENTION
2018 NM FIT Annual Meeting 21
5302018
8
Formulas
bull VLBW infants should remain on nutrient enriched post-discharge formulas (transitional) until at least 9 months CGA
bull Standard caloric of neosureenfacare 22kcaloz
bull Preterm infants need to consume at least as much formula per day as their term-born peers
bull If growth exceeds 2 birth percentile lines or if weightlength exceeds 90 20caloz term infant formula may be considered earlier
bull Kleinman RE American Academy of Pediatrics Committee on Nutrition 2004bull LewishttpswwwpreemietoolkitcompdfsE_PhysicalExaminationAssessmentRecommendations-for-
Postdischargepdf
2018 NM FIT Annual Meeting 22
Other Formulasbull No role for the use of low-iron formulas (constipation)
bull Soy protein-based formula not recommended for preterm infants weighing lt 1800 grams
bull Lacking in sufficient calcium phosphorous and protein
bull The presence of phytates (soy) decreases bioavailability of mineral absorption in the gut
Kleinman RE American Academy of Pediatrics Committee on Nutrition 2004
2018 NM FIT Annual Meeting 23
Standard Immunizations
bull Preterm infants should receive full immunizations based upon their chronological age consistent with the schedule and dose recommended for normal full-term infants
bull Synagis for some with chronic lung disease
AAP Committee on Infectious Diseases Red Book 2012
2018 NM FIT Annual Meeting 24
5302018
9
Put Your Microscope Lenses Onhellip
bull httpwwwpediatricsemoryedudivisionsneonatologydpcnicubehhtml
2018 NM FIT Annual Meeting 25
2018 NM FIT Annual Meeting 26
Synactive Theory
Infantrsquos communication is via hisher behavior
Behavior represents the hierarchical integration of his subsystems
Focuses on the unique way that each baby processes the environment at any given time
Subsystems are
interdependent
hierarchical
mature sequentially (Peters 2001)
2018 NM FIT Annual Meeting 27
5302018
10
Dynamic Systems
bull You cannot just look at each ldquopartrdquo of the baby You must look at how each of the pieces work together and affect the whole child and the family
2018 NM FIT Annual Meeting 28
NEW MEXICO DOH DDSD - FISCAL YEAR 2018
STATE GENERAL FUND
Services for Individuals with
Developmental Disabilities
and
FAMILY INFANT TODDLER PROGRAM
MEDICAID EPSDT
Services for infants and toddlers (birth to three)
with or at risk of Developmental Delays and their
families SERVICE DEFINITIONS AND STANDARDS
EFFECTIVE JULY 1 2017
2018 NM FIT Annual Meeting 29
COMPREHENSIVE MULTIDISCIPLINARY EVALUATION
bull The Comprehensive Multidisciplinary Evaluation (CME) is designed to inform the eligibility determination process through a timely non-discriminatory comprehensive and interdisciplinary approach The evaluation is designed to determine the developmental status of the child and to determine eligibility for early intervention services The evaluation shall include parentcaregiver report information from the routines based interview process and must cover the following developmental areas
bull Cognitive bull Physical motor (including vision and hearing) bull Communication bull Social or emotional bull Adaptive behavior
2018 NM FIT Annual Meeting 30
5302018
11
SCOPE OF SERVICE
bull ldquohelliphelliphellipEvaluation personnel should have an early childhood development background Evaluation personnel should also be trained in FIT evaluation and eligibility procedures and the tool(s) that they are administering Evaluation and assessment tools shall be used in accordance with the manual and established protocols To ensure accurate evaluation results evaluations must be conducted in an environment where the child typically spends hisher day
bull If the team decides to first conduct a developmental screening for a child referred and in accordance with NMAC 7308 10 E the Ages and Stages Questionnaire (ASQ) shall be utilized
bull A review and summary of the childrsquos records related to current health status and prior medical history (look at 2017 presentation)
2018 NM FIT Annual Meeting 31
Less than one-monthbull Given the unique characteristics of young infants and the challenges of
determining their developmental levels
bull For infants under one month of age (adjusted) the IDA will not be used Instead one of the approved tools below shall be used together with informed clinical opinion Informed clinical opinion (httpwwwnectacorg~pdfspubsnnotes10pdf) is used by early intervention professionals in the evaluation and assessment process to make a recommendation as to initial and continuing eligibility for services under Part C and as a basis for planning services to meet child and family needs
bull Informed clinical opinion makes use of qualitative and quantitative information to assist in forming a determination regarding difficult-to-measure aspects of current developmental status and the potential need for early intervention
2018 NM FIT Annual Meeting 32
Approved tools for infants under 1 month of age
bull AIMS (Alberta Infant Motor Scale)
bull TIMP (Test of Infant Motor Performance)
bull Infant Toddler Sensory Profile
bull Motor Skills Acquisition Checklist
bull Newborn Individualized Developmental Care and Assessment Program (NIDCAP) - for use with newborns in the newborn intensive care setting only
bull Newborn Behavior Assessment Scale (NBAS)
bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 33
5302018
12
For infants over one month of age (adjusted) and under four months of age including adjusted age the IDA shall be used in conjunction with one of the following approved tools listed below)
bull All 5 developmental domains shall be assessed and addressed in the CME report including parentcaregiver information AIMS (Alberta Infant Motor Scale
bull TIMP (Test of Infant Motor Performance) bull Infant Toddler Sensory Profile bull Peabody Developmental Motor Scale (PDMS-2) bull Motor Skills Acquisition Checklist bull REEL-3 bull The Rossetti Infant Toddler Language Scale bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 34
AIMS-Alberta Infant Motor ScalesMotor Assessment of the Developing Infant
bull 0 ndash 18 months or walking decreased accuracy at 3 months of
age decreased precision after 9 months of age
bull ldquoobservedrdquo or ldquonot observedrdquo Items in the observed range create a motor window
bull Subscale scores are calculated by giving credit for observed items within the motor window plus giving credit for all of the less mature items before the motor window
bull The AIMS total score calculated by summing the scores
bull Score converted to a percentile and compared with age-equivalent peers from the normative sample
bull BUY THE BOOK
2018 NM FIT Annual Meeting 35
Psychometrics of AIMSbull Normed on 2202 infants between the ages of 1 week to 18
months living in province of Alberta between 1990 and 1992
bull Interrater reliability using two therapists who assessed 221 typically developing r values from a Pearson Product 096 to 099
bull Test-retest reliability was assessed by administering the AIMS twice (7 days between assessments) to 233 infants r values from a Pearson Product Moment Correlation Coefficient ranged from 086 to 099 when the same assessor scored the AIMS on both assessment days
2018 NM FIT Annual Meeting 36
5302018
13
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull Recommended cut-off scores for atypical development are the 10th
percentile at 4 months of age and the 5th percentile at 8 months of age (Darrah Piper amp Watt 1998)
bull Even typically developing infants do not acquire gross motor skills at a stable rate and could have a score that places them below the ldquocut-offrdquo score (Darrah et al 1998)
bull It is important to complete serial assessments and not simply identify a child as being delayed based on a one time screening
2018 NM FIT Annual Meeting 37
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull AIMS is thought to be appropriate for children between 0 -18 months it has been shown to have a ceiling effect with low precision of measurement after ~ 9 months of age or when children are able to lower themselves from standing with control Liao amp Campbell 2004
bull AIMS is much better at identifying infants with motor disabilities at 6 9 and 12 months than at 3 months of age Kolobe amp Bulanda 2006
bull The AIMS misclassified a high percentage of 3 month old infants later diagnosed with cerebral palsy (CP) where as it did much better at identifying children later diagnosed with CP when using the 5th percentile as a cut-off at 6 9 and 12 months of age Kolobe amp Bulanda 2006
bull These studies results should encourage clinicians to use caution when interpreting AIMS scores for infants 3 months of age as well as infants who are 9 months of age or older
2018 NM FIT Annual Meeting 38
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoslip-throughrdquo
bull How do they ldquolookrdquobull Curled ndash ldquohe is so cuddlyrdquo
bull Sacral sitting
bull Hands closedbull Cortical thumb
bull Ankle Clonusbull A few beats vs prolonged
2018 NM FIT Annual Meeting 39
5302018
14
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoone with the surfacerdquo
bull ldquohe never stops movingrdquobull Pull-to-sit hellip And into standing
bull On toes (ask about walkers and saucers and Johnny jump-ups)
bull Does he bear weight
bull Head shape and its effects on prone and supine
2018 NM FIT Annual Meeting 40
AIMS ldquoBehaviorsrdquo (cont)
bull Locking kneesbull ldquoCollapsingrdquo
bull Pull-to-sit moves straight into standing
bull Asymmetries
2018 NM FIT Annual Meeting 41
Symmetry
bull Always look for symmetry (in all evaluations) ndashbull ldquoI think that he is going to be left-handedrdquo
bull Use your reasoning skills
bull Asymmetry because of gravity taking head to one side
bull 2 months before baby can maintain midlinebull Does baby visually scan to both sides
2018 NM FIT Annual Meeting 42
5302018
15
2018 NM FIT Annual Meeting 43
Think of Dynamic Systemshellip
bull ASQs are prime example (and IDA)
bull What are we really looking atbull Some examples of systems approach
2018 NM FIT Annual Meeting 44
2018 NM FIT Annual Meeting 45
5302018
16
2018 NM FIT Annual Meeting 46
2018 NM FIT Annual Meeting 47
2018 NM FIT Annual Meeting 48
5302018
17
When is a ldquosit uprdquo a bad thing Van Haastert et al
Dev Med Child Neurol 2012 Jun54(6)538-43
ldquoActive head lifting from supine in early infancy an indicator for non-optimal cognitive outcome in late infancyrdquo
bull AHLS is associated with a less favorable cognitive outcome in the second year of life in preterm and in term-born infants than in comparison infants
2018 NM FIT Annual Meeting 49
RBI
bull Describe your babyrsquos ________
bull Observe babies eatingbull Dribblingbull Noisybull Falls ldquoasleeprdquobull Pushes awaybull Arching
bull All babies refluxbull Meds donrsquot stop refluxbull Effects of PPIs and H2 inhibitors
2018 NM FIT Annual Meeting 50
Transdisciplinary and Coaching
bull Effective Transdisciplinary is dependent on recognizing our own strengths and limitations ndash self-reflection
bull TTA is critical
2018 NM FIT Annual Meeting 51
5302018
18
Can we predict
bull httppartnersforkidsorgwp-contentuploads20171115236_Neo_Cerebral-Palsy-Early-ID_Practice-Tool_Q4-RMpdf
bull We do NOT diagnose
2018 NM FIT Annual Meeting 52
FIT Technical Assistance Document-Evaluation and Assessment p24ICO
2018 NM FIT Annual Meeting 53
And this is where we need to build the capacityhellip
bull ldquoDue to the varying nature and purpose of the scores of each of the above approved tools the scores themselves will not lead to eligibility but rather they will provide additional information for the team to consider in reaching a determination of the childs developmental status and eligibility
determinationrdquo
2018 NM FIT Annual Meeting 54
5302018
19
Informed Clinical Opinionbull An evaluation of the childrsquos level of functioning in each of the
following developmental areas
bull Cognitive development
bull Physical development including vision and hearing
bull Communication development
bull Social or emotional development and
bull Adaptive development
bull A review of the pertinent records related to the childrsquos current health status and medical history and can include areas such as but not limited to feeding sleeping motor behavior state regulation communication visual tracking and auditory responses
bull All 5 developmental domains and pertinent information shall be addressed in the CME report as well as parent report and shall include a statement and approval signature indicating that Informed Clinical Opinion was used
2018 NM FIT Annual Meeting 55
ICO example
bull httpswwwyoutubecomwatchv=ztd2-O0z9rM
2018 NM FIT Annual Meeting 56
Risk for Cerebral Palsy Early Detection
and Early InterventionPoster Presentation at 2018 Annual FIT Meeting
NMOTA Conference
September 2018
Amazing Newborn Conference
November 8-9 2018
2018 NM FIT Annual Meeting 57
5302018
20
Risk Factors for Cerebral Palsy(McIntrye et al 2011)
bull Prior to conception
bull History of still births miscarriage premature birth family history of CP low SES
bull Early Pregnancy
bull Infection multiple births genetic predisposition male gender birth defects
bull During Pregnancy
bull Maternal disease preeclampsia infection placental abnormalities precursors to premature birth
2018 NM FIT Annual Meeting 58
Cerebral Palsy (Novak et al 2017)
bull Most Common Physical Disorder in Children
bull 2 in High Income Countries ldquoCP describes a group of developmental disorders of movement and posture causing activity restrictions or disability that are attributed to disturbances occurring in the fetal or infant brain The motor impairment may be accompanied by a seizure disorder or by impairment of sensation cognition communication and or behavior ldquo
bull Originates prenatally or early post-natally
2018 NM FIT Annual Meeting 59
Three Groups Classification
1 Premature Infants (30-40 of all cases)
2 Term infants who develop neonatal encephalopathy shortly after birth (15-20)
3 Term infants without risk factors (40-50)
2018 NM FIT Annual Meeting 60
5302018
21
86 of parents suspected their child
had Cerebral Palsy before a clinical
diagnosis was made
2018 NM FIT Annual Meeting 61
RISK for CP
Identification Intervention
2018 NM FIT Annual Meeting 62
How do we build capacity
bull REFLECTIONbull Individual
bull What do I NOT knowbull As a program director
bull What questions keep coming up
2018 NM FIT Annual Meeting 63
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65
5302018
2
Basic Concepts For Todaybull Why we recommend following until they are 2
yo (especially when they are doing okay) bull At Risk Statebull Language and the ldquonext steprdquobull Issues that we see most frequently in SBC
follow-up and first visitsbull Head Shapebull Growth nutrition constipationbull Tummy Timebull Parent stress
2018 NM FIT Annual Meeting 4
Basic Concepts For Todaybull Prematurity
bull When is a baby preterm
bull How long do we correct for prematurity
bull What all gets ldquocorrected forrdquo
bull Everything but shots
2018 NM FIT Annual Meeting 5
Things that you should monitorbull Evaluation of Growth and Nutritionbull Vision and Hearing Screeningbull Ongoing Preventative Carebull Developmental Progressbull Close monitoring of common medical problems of the
preterm infantbull Out-patient specialty visits
bull Pulmonarybull Ophthalmologybull Cardiologybull Nephrologybull SBC
2018 NM FIT Annual Meeting 6
5302018
3
Development
Term
bull Cephalo-caudal (head-to-toe) motor control
bull Proximal to distal (inside-to-outside)
bull Resistancegravity
bull Energy
Preterm
bull Caudal-Cephalo
bull Still proximal-distal
bull Muscle mass
bull Resistancegravity
bull Energy (on O2)
2018 NM FIT Annual Meeting 7
Sensory Systems
bull Cutaneous 12-14 weeks
bull Vestibular 14-15 weeks functioning
bull Chemical- Olfactory (smell ) 24 Gustatory (taste)-17-18
bull Auditory (25 -29)
bull Visual
bull Critical periods of Development
bull Just because they are functioning doesnrsquot mean that they are supposed to be
2018 NM FIT Annual Meeting 8
FIT- frequentbull Meningitis bull Seizures bull BWbull GAbull Growth Restrictionsbull IVHbull Hydrocephalybull Club footbull Hypoglycemia bull HIE (neonatal
encephalopathy)
bull IUDEPDEbull Feeding
DisordersProblemsbull Cleftsbull Gastroschisisbull ROPbull Jaundicebull Trisomy 21bull Syndromesbull Environmentalbull Spina Bifida
2018 NM FIT Annual Meeting 9
5302018
4
NICU diagnoses that place a baby at risk for developmental delay
bull hellipAKA ldquoWhy does UNM NICU pick these babies up and transfer them to yourdquo
bull Cardiac conditions
bull ECMO
bull Cooling
bull ICO
2018 NM FIT Annual Meeting 10
Corrected Gestational Age (CGA)
bull Use until the infant reaches 24-36 months
bull Use for all developmental milestones including introduction of foods
bull The only schedule that should follow the preterm infantrsquos chronological age is their immunization schedule
bull AAP recommends correction until at least age 2 and most until age 3
2018 NM FIT Annual Meeting 11
Neurological Differences
bull When corrected to term the extremely preterm infantrsquos brain
bull Reduced gray matter volume
bull Increased cerebrospinal fluidbull Males have significantly lower white matter volumes
in specific areas
bull These findings persist to school age and are associated with learning challenges
Kesler SR et al J Peds 2008
2018 NM FIT Annual Meeting 12
5302018
5
We are growing brains in the NICU
2018 NM FIT Annual Meeting 13
PerinatalNeonatal Risk Factors
bull Risk Increased likelihood of disability
bull Risk ne disability
bull Many who have disability do not have risk
bull Some risk factors carry a higher risk of disability than others
bull More risk factors will lead to an additive effect
2018 NM FIT Annual Meeting 14
AAP Recommendation Screening
bull In the absence of risk or concernsbull 9 18 and 30 months
bull If surveillance identifies risk then additional screening is needed
bull Surveillance should be continued even if screening does not indicate a risk of delay
2018 NM FIT Annual Meeting 15
5302018
6
Long-term Outcome ndash this is where we come in
bull Complex interplaybull Biologic serves as the strongest predictor of long-
term function and development as the child recovers from perinatal and prenatal insults
bull Genetic and Environmental accounts for more of the variations seen in cognitive developmental
bull In most preterm children a positive environment can ameliorate many biologic risk factors
2018 NM FIT Annual Meeting 16
2 Year Re-hospitalizationOperationsle27 weeks
bull 12 Cerebral Palsy bull 6 mildbull 6 moderatesevere
bull 11 require special equipmentbull 86 bracesorthoticsbull 19 walker
Neonatal Research Network Data 2011
2018 NM FIT Annual Meeting 17
New Mexico Follow-Up Care- HM 14 (2018)
bull Currently we donrsquot have comprehensive care for high-risk neonates
bull UNMHrsquos NICU represents all regions of the State
bull 80 Medicaid
bull 2 No insurance
bull 50-60 from outside of Bernalillo County
bull More than 13 of births are to residents in rural and semi-rural areas
bull Preterm birth is more common in rural areas
bull 104 of children with special health care needs are without a usual source of care
2018 NM FIT Annual Meeting 18
5302018
7
United States Stats as of 2015
bull 4 million births per year
bull Gestational age
bull 96 are preterm (lt37 weeks gestation)
bull 7 late preterm (34-3667 weeks)
bull 26 (le34 weeks)
bull Weight
bull Low Birth Weight (lt2500g)
bull ~8 of annual births
bull ~90 (~288000) of these infants survive to discharge~ 13 will need specialty services
National Vital Statistics Report Vol 65 No 3 Preliminary Data
2018 NM FIT Annual Meeting 19
Plagiocephaly and Torticollis
bull NICU and Back to Sleep
bull Right-sided
bull AAP httpwwwaappublicationsorgnews20161027Plagiocephaly102016
bull Common condition
bull frac14 of US infants w some degree of positional plagiocephaly
bull The incidence has increased since AAP Back to Sleep campaign in 1994 (to prevent SIDS)
2018 NM FIT Annual Meeting 20
What to do about it
bull Ask your motor therapist
bull Ask your pediatrician
bull Do not wait to address itbull Positioningbull Routines
bull Active movements (you do not have to do passive stretch)
bull Best approach bull PREVENTION
2018 NM FIT Annual Meeting 21
5302018
8
Formulas
bull VLBW infants should remain on nutrient enriched post-discharge formulas (transitional) until at least 9 months CGA
bull Standard caloric of neosureenfacare 22kcaloz
bull Preterm infants need to consume at least as much formula per day as their term-born peers
bull If growth exceeds 2 birth percentile lines or if weightlength exceeds 90 20caloz term infant formula may be considered earlier
bull Kleinman RE American Academy of Pediatrics Committee on Nutrition 2004bull LewishttpswwwpreemietoolkitcompdfsE_PhysicalExaminationAssessmentRecommendations-for-
Postdischargepdf
2018 NM FIT Annual Meeting 22
Other Formulasbull No role for the use of low-iron formulas (constipation)
bull Soy protein-based formula not recommended for preterm infants weighing lt 1800 grams
bull Lacking in sufficient calcium phosphorous and protein
bull The presence of phytates (soy) decreases bioavailability of mineral absorption in the gut
Kleinman RE American Academy of Pediatrics Committee on Nutrition 2004
2018 NM FIT Annual Meeting 23
Standard Immunizations
bull Preterm infants should receive full immunizations based upon their chronological age consistent with the schedule and dose recommended for normal full-term infants
bull Synagis for some with chronic lung disease
AAP Committee on Infectious Diseases Red Book 2012
2018 NM FIT Annual Meeting 24
5302018
9
Put Your Microscope Lenses Onhellip
bull httpwwwpediatricsemoryedudivisionsneonatologydpcnicubehhtml
2018 NM FIT Annual Meeting 25
2018 NM FIT Annual Meeting 26
Synactive Theory
Infantrsquos communication is via hisher behavior
Behavior represents the hierarchical integration of his subsystems
Focuses on the unique way that each baby processes the environment at any given time
Subsystems are
interdependent
hierarchical
mature sequentially (Peters 2001)
2018 NM FIT Annual Meeting 27
5302018
10
Dynamic Systems
bull You cannot just look at each ldquopartrdquo of the baby You must look at how each of the pieces work together and affect the whole child and the family
2018 NM FIT Annual Meeting 28
NEW MEXICO DOH DDSD - FISCAL YEAR 2018
STATE GENERAL FUND
Services for Individuals with
Developmental Disabilities
and
FAMILY INFANT TODDLER PROGRAM
MEDICAID EPSDT
Services for infants and toddlers (birth to three)
with or at risk of Developmental Delays and their
families SERVICE DEFINITIONS AND STANDARDS
EFFECTIVE JULY 1 2017
2018 NM FIT Annual Meeting 29
COMPREHENSIVE MULTIDISCIPLINARY EVALUATION
bull The Comprehensive Multidisciplinary Evaluation (CME) is designed to inform the eligibility determination process through a timely non-discriminatory comprehensive and interdisciplinary approach The evaluation is designed to determine the developmental status of the child and to determine eligibility for early intervention services The evaluation shall include parentcaregiver report information from the routines based interview process and must cover the following developmental areas
bull Cognitive bull Physical motor (including vision and hearing) bull Communication bull Social or emotional bull Adaptive behavior
2018 NM FIT Annual Meeting 30
5302018
11
SCOPE OF SERVICE
bull ldquohelliphelliphellipEvaluation personnel should have an early childhood development background Evaluation personnel should also be trained in FIT evaluation and eligibility procedures and the tool(s) that they are administering Evaluation and assessment tools shall be used in accordance with the manual and established protocols To ensure accurate evaluation results evaluations must be conducted in an environment where the child typically spends hisher day
bull If the team decides to first conduct a developmental screening for a child referred and in accordance with NMAC 7308 10 E the Ages and Stages Questionnaire (ASQ) shall be utilized
bull A review and summary of the childrsquos records related to current health status and prior medical history (look at 2017 presentation)
2018 NM FIT Annual Meeting 31
Less than one-monthbull Given the unique characteristics of young infants and the challenges of
determining their developmental levels
bull For infants under one month of age (adjusted) the IDA will not be used Instead one of the approved tools below shall be used together with informed clinical opinion Informed clinical opinion (httpwwwnectacorg~pdfspubsnnotes10pdf) is used by early intervention professionals in the evaluation and assessment process to make a recommendation as to initial and continuing eligibility for services under Part C and as a basis for planning services to meet child and family needs
bull Informed clinical opinion makes use of qualitative and quantitative information to assist in forming a determination regarding difficult-to-measure aspects of current developmental status and the potential need for early intervention
2018 NM FIT Annual Meeting 32
Approved tools for infants under 1 month of age
bull AIMS (Alberta Infant Motor Scale)
bull TIMP (Test of Infant Motor Performance)
bull Infant Toddler Sensory Profile
bull Motor Skills Acquisition Checklist
bull Newborn Individualized Developmental Care and Assessment Program (NIDCAP) - for use with newborns in the newborn intensive care setting only
bull Newborn Behavior Assessment Scale (NBAS)
bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 33
5302018
12
For infants over one month of age (adjusted) and under four months of age including adjusted age the IDA shall be used in conjunction with one of the following approved tools listed below)
bull All 5 developmental domains shall be assessed and addressed in the CME report including parentcaregiver information AIMS (Alberta Infant Motor Scale
bull TIMP (Test of Infant Motor Performance) bull Infant Toddler Sensory Profile bull Peabody Developmental Motor Scale (PDMS-2) bull Motor Skills Acquisition Checklist bull REEL-3 bull The Rossetti Infant Toddler Language Scale bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 34
AIMS-Alberta Infant Motor ScalesMotor Assessment of the Developing Infant
bull 0 ndash 18 months or walking decreased accuracy at 3 months of
age decreased precision after 9 months of age
bull ldquoobservedrdquo or ldquonot observedrdquo Items in the observed range create a motor window
bull Subscale scores are calculated by giving credit for observed items within the motor window plus giving credit for all of the less mature items before the motor window
bull The AIMS total score calculated by summing the scores
bull Score converted to a percentile and compared with age-equivalent peers from the normative sample
bull BUY THE BOOK
2018 NM FIT Annual Meeting 35
Psychometrics of AIMSbull Normed on 2202 infants between the ages of 1 week to 18
months living in province of Alberta between 1990 and 1992
bull Interrater reliability using two therapists who assessed 221 typically developing r values from a Pearson Product 096 to 099
bull Test-retest reliability was assessed by administering the AIMS twice (7 days between assessments) to 233 infants r values from a Pearson Product Moment Correlation Coefficient ranged from 086 to 099 when the same assessor scored the AIMS on both assessment days
2018 NM FIT Annual Meeting 36
5302018
13
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull Recommended cut-off scores for atypical development are the 10th
percentile at 4 months of age and the 5th percentile at 8 months of age (Darrah Piper amp Watt 1998)
bull Even typically developing infants do not acquire gross motor skills at a stable rate and could have a score that places them below the ldquocut-offrdquo score (Darrah et al 1998)
bull It is important to complete serial assessments and not simply identify a child as being delayed based on a one time screening
2018 NM FIT Annual Meeting 37
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull AIMS is thought to be appropriate for children between 0 -18 months it has been shown to have a ceiling effect with low precision of measurement after ~ 9 months of age or when children are able to lower themselves from standing with control Liao amp Campbell 2004
bull AIMS is much better at identifying infants with motor disabilities at 6 9 and 12 months than at 3 months of age Kolobe amp Bulanda 2006
bull The AIMS misclassified a high percentage of 3 month old infants later diagnosed with cerebral palsy (CP) where as it did much better at identifying children later diagnosed with CP when using the 5th percentile as a cut-off at 6 9 and 12 months of age Kolobe amp Bulanda 2006
bull These studies results should encourage clinicians to use caution when interpreting AIMS scores for infants 3 months of age as well as infants who are 9 months of age or older
2018 NM FIT Annual Meeting 38
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoslip-throughrdquo
bull How do they ldquolookrdquobull Curled ndash ldquohe is so cuddlyrdquo
bull Sacral sitting
bull Hands closedbull Cortical thumb
bull Ankle Clonusbull A few beats vs prolonged
2018 NM FIT Annual Meeting 39
5302018
14
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoone with the surfacerdquo
bull ldquohe never stops movingrdquobull Pull-to-sit hellip And into standing
bull On toes (ask about walkers and saucers and Johnny jump-ups)
bull Does he bear weight
bull Head shape and its effects on prone and supine
2018 NM FIT Annual Meeting 40
AIMS ldquoBehaviorsrdquo (cont)
bull Locking kneesbull ldquoCollapsingrdquo
bull Pull-to-sit moves straight into standing
bull Asymmetries
2018 NM FIT Annual Meeting 41
Symmetry
bull Always look for symmetry (in all evaluations) ndashbull ldquoI think that he is going to be left-handedrdquo
bull Use your reasoning skills
bull Asymmetry because of gravity taking head to one side
bull 2 months before baby can maintain midlinebull Does baby visually scan to both sides
2018 NM FIT Annual Meeting 42
5302018
15
2018 NM FIT Annual Meeting 43
Think of Dynamic Systemshellip
bull ASQs are prime example (and IDA)
bull What are we really looking atbull Some examples of systems approach
2018 NM FIT Annual Meeting 44
2018 NM FIT Annual Meeting 45
5302018
16
2018 NM FIT Annual Meeting 46
2018 NM FIT Annual Meeting 47
2018 NM FIT Annual Meeting 48
5302018
17
When is a ldquosit uprdquo a bad thing Van Haastert et al
Dev Med Child Neurol 2012 Jun54(6)538-43
ldquoActive head lifting from supine in early infancy an indicator for non-optimal cognitive outcome in late infancyrdquo
bull AHLS is associated with a less favorable cognitive outcome in the second year of life in preterm and in term-born infants than in comparison infants
2018 NM FIT Annual Meeting 49
RBI
bull Describe your babyrsquos ________
bull Observe babies eatingbull Dribblingbull Noisybull Falls ldquoasleeprdquobull Pushes awaybull Arching
bull All babies refluxbull Meds donrsquot stop refluxbull Effects of PPIs and H2 inhibitors
2018 NM FIT Annual Meeting 50
Transdisciplinary and Coaching
bull Effective Transdisciplinary is dependent on recognizing our own strengths and limitations ndash self-reflection
bull TTA is critical
2018 NM FIT Annual Meeting 51
5302018
18
Can we predict
bull httppartnersforkidsorgwp-contentuploads20171115236_Neo_Cerebral-Palsy-Early-ID_Practice-Tool_Q4-RMpdf
bull We do NOT diagnose
2018 NM FIT Annual Meeting 52
FIT Technical Assistance Document-Evaluation and Assessment p24ICO
2018 NM FIT Annual Meeting 53
And this is where we need to build the capacityhellip
bull ldquoDue to the varying nature and purpose of the scores of each of the above approved tools the scores themselves will not lead to eligibility but rather they will provide additional information for the team to consider in reaching a determination of the childs developmental status and eligibility
determinationrdquo
2018 NM FIT Annual Meeting 54
5302018
19
Informed Clinical Opinionbull An evaluation of the childrsquos level of functioning in each of the
following developmental areas
bull Cognitive development
bull Physical development including vision and hearing
bull Communication development
bull Social or emotional development and
bull Adaptive development
bull A review of the pertinent records related to the childrsquos current health status and medical history and can include areas such as but not limited to feeding sleeping motor behavior state regulation communication visual tracking and auditory responses
bull All 5 developmental domains and pertinent information shall be addressed in the CME report as well as parent report and shall include a statement and approval signature indicating that Informed Clinical Opinion was used
2018 NM FIT Annual Meeting 55
ICO example
bull httpswwwyoutubecomwatchv=ztd2-O0z9rM
2018 NM FIT Annual Meeting 56
Risk for Cerebral Palsy Early Detection
and Early InterventionPoster Presentation at 2018 Annual FIT Meeting
NMOTA Conference
September 2018
Amazing Newborn Conference
November 8-9 2018
2018 NM FIT Annual Meeting 57
5302018
20
Risk Factors for Cerebral Palsy(McIntrye et al 2011)
bull Prior to conception
bull History of still births miscarriage premature birth family history of CP low SES
bull Early Pregnancy
bull Infection multiple births genetic predisposition male gender birth defects
bull During Pregnancy
bull Maternal disease preeclampsia infection placental abnormalities precursors to premature birth
2018 NM FIT Annual Meeting 58
Cerebral Palsy (Novak et al 2017)
bull Most Common Physical Disorder in Children
bull 2 in High Income Countries ldquoCP describes a group of developmental disorders of movement and posture causing activity restrictions or disability that are attributed to disturbances occurring in the fetal or infant brain The motor impairment may be accompanied by a seizure disorder or by impairment of sensation cognition communication and or behavior ldquo
bull Originates prenatally or early post-natally
2018 NM FIT Annual Meeting 59
Three Groups Classification
1 Premature Infants (30-40 of all cases)
2 Term infants who develop neonatal encephalopathy shortly after birth (15-20)
3 Term infants without risk factors (40-50)
2018 NM FIT Annual Meeting 60
5302018
21
86 of parents suspected their child
had Cerebral Palsy before a clinical
diagnosis was made
2018 NM FIT Annual Meeting 61
RISK for CP
Identification Intervention
2018 NM FIT Annual Meeting 62
How do we build capacity
bull REFLECTIONbull Individual
bull What do I NOT knowbull As a program director
bull What questions keep coming up
2018 NM FIT Annual Meeting 63
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65
5302018
3
Development
Term
bull Cephalo-caudal (head-to-toe) motor control
bull Proximal to distal (inside-to-outside)
bull Resistancegravity
bull Energy
Preterm
bull Caudal-Cephalo
bull Still proximal-distal
bull Muscle mass
bull Resistancegravity
bull Energy (on O2)
2018 NM FIT Annual Meeting 7
Sensory Systems
bull Cutaneous 12-14 weeks
bull Vestibular 14-15 weeks functioning
bull Chemical- Olfactory (smell ) 24 Gustatory (taste)-17-18
bull Auditory (25 -29)
bull Visual
bull Critical periods of Development
bull Just because they are functioning doesnrsquot mean that they are supposed to be
2018 NM FIT Annual Meeting 8
FIT- frequentbull Meningitis bull Seizures bull BWbull GAbull Growth Restrictionsbull IVHbull Hydrocephalybull Club footbull Hypoglycemia bull HIE (neonatal
encephalopathy)
bull IUDEPDEbull Feeding
DisordersProblemsbull Cleftsbull Gastroschisisbull ROPbull Jaundicebull Trisomy 21bull Syndromesbull Environmentalbull Spina Bifida
2018 NM FIT Annual Meeting 9
5302018
4
NICU diagnoses that place a baby at risk for developmental delay
bull hellipAKA ldquoWhy does UNM NICU pick these babies up and transfer them to yourdquo
bull Cardiac conditions
bull ECMO
bull Cooling
bull ICO
2018 NM FIT Annual Meeting 10
Corrected Gestational Age (CGA)
bull Use until the infant reaches 24-36 months
bull Use for all developmental milestones including introduction of foods
bull The only schedule that should follow the preterm infantrsquos chronological age is their immunization schedule
bull AAP recommends correction until at least age 2 and most until age 3
2018 NM FIT Annual Meeting 11
Neurological Differences
bull When corrected to term the extremely preterm infantrsquos brain
bull Reduced gray matter volume
bull Increased cerebrospinal fluidbull Males have significantly lower white matter volumes
in specific areas
bull These findings persist to school age and are associated with learning challenges
Kesler SR et al J Peds 2008
2018 NM FIT Annual Meeting 12
5302018
5
We are growing brains in the NICU
2018 NM FIT Annual Meeting 13
PerinatalNeonatal Risk Factors
bull Risk Increased likelihood of disability
bull Risk ne disability
bull Many who have disability do not have risk
bull Some risk factors carry a higher risk of disability than others
bull More risk factors will lead to an additive effect
2018 NM FIT Annual Meeting 14
AAP Recommendation Screening
bull In the absence of risk or concernsbull 9 18 and 30 months
bull If surveillance identifies risk then additional screening is needed
bull Surveillance should be continued even if screening does not indicate a risk of delay
2018 NM FIT Annual Meeting 15
5302018
6
Long-term Outcome ndash this is where we come in
bull Complex interplaybull Biologic serves as the strongest predictor of long-
term function and development as the child recovers from perinatal and prenatal insults
bull Genetic and Environmental accounts for more of the variations seen in cognitive developmental
bull In most preterm children a positive environment can ameliorate many biologic risk factors
2018 NM FIT Annual Meeting 16
2 Year Re-hospitalizationOperationsle27 weeks
bull 12 Cerebral Palsy bull 6 mildbull 6 moderatesevere
bull 11 require special equipmentbull 86 bracesorthoticsbull 19 walker
Neonatal Research Network Data 2011
2018 NM FIT Annual Meeting 17
New Mexico Follow-Up Care- HM 14 (2018)
bull Currently we donrsquot have comprehensive care for high-risk neonates
bull UNMHrsquos NICU represents all regions of the State
bull 80 Medicaid
bull 2 No insurance
bull 50-60 from outside of Bernalillo County
bull More than 13 of births are to residents in rural and semi-rural areas
bull Preterm birth is more common in rural areas
bull 104 of children with special health care needs are without a usual source of care
2018 NM FIT Annual Meeting 18
5302018
7
United States Stats as of 2015
bull 4 million births per year
bull Gestational age
bull 96 are preterm (lt37 weeks gestation)
bull 7 late preterm (34-3667 weeks)
bull 26 (le34 weeks)
bull Weight
bull Low Birth Weight (lt2500g)
bull ~8 of annual births
bull ~90 (~288000) of these infants survive to discharge~ 13 will need specialty services
National Vital Statistics Report Vol 65 No 3 Preliminary Data
2018 NM FIT Annual Meeting 19
Plagiocephaly and Torticollis
bull NICU and Back to Sleep
bull Right-sided
bull AAP httpwwwaappublicationsorgnews20161027Plagiocephaly102016
bull Common condition
bull frac14 of US infants w some degree of positional plagiocephaly
bull The incidence has increased since AAP Back to Sleep campaign in 1994 (to prevent SIDS)
2018 NM FIT Annual Meeting 20
What to do about it
bull Ask your motor therapist
bull Ask your pediatrician
bull Do not wait to address itbull Positioningbull Routines
bull Active movements (you do not have to do passive stretch)
bull Best approach bull PREVENTION
2018 NM FIT Annual Meeting 21
5302018
8
Formulas
bull VLBW infants should remain on nutrient enriched post-discharge formulas (transitional) until at least 9 months CGA
bull Standard caloric of neosureenfacare 22kcaloz
bull Preterm infants need to consume at least as much formula per day as their term-born peers
bull If growth exceeds 2 birth percentile lines or if weightlength exceeds 90 20caloz term infant formula may be considered earlier
bull Kleinman RE American Academy of Pediatrics Committee on Nutrition 2004bull LewishttpswwwpreemietoolkitcompdfsE_PhysicalExaminationAssessmentRecommendations-for-
Postdischargepdf
2018 NM FIT Annual Meeting 22
Other Formulasbull No role for the use of low-iron formulas (constipation)
bull Soy protein-based formula not recommended for preterm infants weighing lt 1800 grams
bull Lacking in sufficient calcium phosphorous and protein
bull The presence of phytates (soy) decreases bioavailability of mineral absorption in the gut
Kleinman RE American Academy of Pediatrics Committee on Nutrition 2004
2018 NM FIT Annual Meeting 23
Standard Immunizations
bull Preterm infants should receive full immunizations based upon their chronological age consistent with the schedule and dose recommended for normal full-term infants
bull Synagis for some with chronic lung disease
AAP Committee on Infectious Diseases Red Book 2012
2018 NM FIT Annual Meeting 24
5302018
9
Put Your Microscope Lenses Onhellip
bull httpwwwpediatricsemoryedudivisionsneonatologydpcnicubehhtml
2018 NM FIT Annual Meeting 25
2018 NM FIT Annual Meeting 26
Synactive Theory
Infantrsquos communication is via hisher behavior
Behavior represents the hierarchical integration of his subsystems
Focuses on the unique way that each baby processes the environment at any given time
Subsystems are
interdependent
hierarchical
mature sequentially (Peters 2001)
2018 NM FIT Annual Meeting 27
5302018
10
Dynamic Systems
bull You cannot just look at each ldquopartrdquo of the baby You must look at how each of the pieces work together and affect the whole child and the family
2018 NM FIT Annual Meeting 28
NEW MEXICO DOH DDSD - FISCAL YEAR 2018
STATE GENERAL FUND
Services for Individuals with
Developmental Disabilities
and
FAMILY INFANT TODDLER PROGRAM
MEDICAID EPSDT
Services for infants and toddlers (birth to three)
with or at risk of Developmental Delays and their
families SERVICE DEFINITIONS AND STANDARDS
EFFECTIVE JULY 1 2017
2018 NM FIT Annual Meeting 29
COMPREHENSIVE MULTIDISCIPLINARY EVALUATION
bull The Comprehensive Multidisciplinary Evaluation (CME) is designed to inform the eligibility determination process through a timely non-discriminatory comprehensive and interdisciplinary approach The evaluation is designed to determine the developmental status of the child and to determine eligibility for early intervention services The evaluation shall include parentcaregiver report information from the routines based interview process and must cover the following developmental areas
bull Cognitive bull Physical motor (including vision and hearing) bull Communication bull Social or emotional bull Adaptive behavior
2018 NM FIT Annual Meeting 30
5302018
11
SCOPE OF SERVICE
bull ldquohelliphelliphellipEvaluation personnel should have an early childhood development background Evaluation personnel should also be trained in FIT evaluation and eligibility procedures and the tool(s) that they are administering Evaluation and assessment tools shall be used in accordance with the manual and established protocols To ensure accurate evaluation results evaluations must be conducted in an environment where the child typically spends hisher day
bull If the team decides to first conduct a developmental screening for a child referred and in accordance with NMAC 7308 10 E the Ages and Stages Questionnaire (ASQ) shall be utilized
bull A review and summary of the childrsquos records related to current health status and prior medical history (look at 2017 presentation)
2018 NM FIT Annual Meeting 31
Less than one-monthbull Given the unique characteristics of young infants and the challenges of
determining their developmental levels
bull For infants under one month of age (adjusted) the IDA will not be used Instead one of the approved tools below shall be used together with informed clinical opinion Informed clinical opinion (httpwwwnectacorg~pdfspubsnnotes10pdf) is used by early intervention professionals in the evaluation and assessment process to make a recommendation as to initial and continuing eligibility for services under Part C and as a basis for planning services to meet child and family needs
bull Informed clinical opinion makes use of qualitative and quantitative information to assist in forming a determination regarding difficult-to-measure aspects of current developmental status and the potential need for early intervention
2018 NM FIT Annual Meeting 32
Approved tools for infants under 1 month of age
bull AIMS (Alberta Infant Motor Scale)
bull TIMP (Test of Infant Motor Performance)
bull Infant Toddler Sensory Profile
bull Motor Skills Acquisition Checklist
bull Newborn Individualized Developmental Care and Assessment Program (NIDCAP) - for use with newborns in the newborn intensive care setting only
bull Newborn Behavior Assessment Scale (NBAS)
bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 33
5302018
12
For infants over one month of age (adjusted) and under four months of age including adjusted age the IDA shall be used in conjunction with one of the following approved tools listed below)
bull All 5 developmental domains shall be assessed and addressed in the CME report including parentcaregiver information AIMS (Alberta Infant Motor Scale
bull TIMP (Test of Infant Motor Performance) bull Infant Toddler Sensory Profile bull Peabody Developmental Motor Scale (PDMS-2) bull Motor Skills Acquisition Checklist bull REEL-3 bull The Rossetti Infant Toddler Language Scale bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 34
AIMS-Alberta Infant Motor ScalesMotor Assessment of the Developing Infant
bull 0 ndash 18 months or walking decreased accuracy at 3 months of
age decreased precision after 9 months of age
bull ldquoobservedrdquo or ldquonot observedrdquo Items in the observed range create a motor window
bull Subscale scores are calculated by giving credit for observed items within the motor window plus giving credit for all of the less mature items before the motor window
bull The AIMS total score calculated by summing the scores
bull Score converted to a percentile and compared with age-equivalent peers from the normative sample
bull BUY THE BOOK
2018 NM FIT Annual Meeting 35
Psychometrics of AIMSbull Normed on 2202 infants between the ages of 1 week to 18
months living in province of Alberta between 1990 and 1992
bull Interrater reliability using two therapists who assessed 221 typically developing r values from a Pearson Product 096 to 099
bull Test-retest reliability was assessed by administering the AIMS twice (7 days between assessments) to 233 infants r values from a Pearson Product Moment Correlation Coefficient ranged from 086 to 099 when the same assessor scored the AIMS on both assessment days
2018 NM FIT Annual Meeting 36
5302018
13
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull Recommended cut-off scores for atypical development are the 10th
percentile at 4 months of age and the 5th percentile at 8 months of age (Darrah Piper amp Watt 1998)
bull Even typically developing infants do not acquire gross motor skills at a stable rate and could have a score that places them below the ldquocut-offrdquo score (Darrah et al 1998)
bull It is important to complete serial assessments and not simply identify a child as being delayed based on a one time screening
2018 NM FIT Annual Meeting 37
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull AIMS is thought to be appropriate for children between 0 -18 months it has been shown to have a ceiling effect with low precision of measurement after ~ 9 months of age or when children are able to lower themselves from standing with control Liao amp Campbell 2004
bull AIMS is much better at identifying infants with motor disabilities at 6 9 and 12 months than at 3 months of age Kolobe amp Bulanda 2006
bull The AIMS misclassified a high percentage of 3 month old infants later diagnosed with cerebral palsy (CP) where as it did much better at identifying children later diagnosed with CP when using the 5th percentile as a cut-off at 6 9 and 12 months of age Kolobe amp Bulanda 2006
bull These studies results should encourage clinicians to use caution when interpreting AIMS scores for infants 3 months of age as well as infants who are 9 months of age or older
2018 NM FIT Annual Meeting 38
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoslip-throughrdquo
bull How do they ldquolookrdquobull Curled ndash ldquohe is so cuddlyrdquo
bull Sacral sitting
bull Hands closedbull Cortical thumb
bull Ankle Clonusbull A few beats vs prolonged
2018 NM FIT Annual Meeting 39
5302018
14
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoone with the surfacerdquo
bull ldquohe never stops movingrdquobull Pull-to-sit hellip And into standing
bull On toes (ask about walkers and saucers and Johnny jump-ups)
bull Does he bear weight
bull Head shape and its effects on prone and supine
2018 NM FIT Annual Meeting 40
AIMS ldquoBehaviorsrdquo (cont)
bull Locking kneesbull ldquoCollapsingrdquo
bull Pull-to-sit moves straight into standing
bull Asymmetries
2018 NM FIT Annual Meeting 41
Symmetry
bull Always look for symmetry (in all evaluations) ndashbull ldquoI think that he is going to be left-handedrdquo
bull Use your reasoning skills
bull Asymmetry because of gravity taking head to one side
bull 2 months before baby can maintain midlinebull Does baby visually scan to both sides
2018 NM FIT Annual Meeting 42
5302018
15
2018 NM FIT Annual Meeting 43
Think of Dynamic Systemshellip
bull ASQs are prime example (and IDA)
bull What are we really looking atbull Some examples of systems approach
2018 NM FIT Annual Meeting 44
2018 NM FIT Annual Meeting 45
5302018
16
2018 NM FIT Annual Meeting 46
2018 NM FIT Annual Meeting 47
2018 NM FIT Annual Meeting 48
5302018
17
When is a ldquosit uprdquo a bad thing Van Haastert et al
Dev Med Child Neurol 2012 Jun54(6)538-43
ldquoActive head lifting from supine in early infancy an indicator for non-optimal cognitive outcome in late infancyrdquo
bull AHLS is associated with a less favorable cognitive outcome in the second year of life in preterm and in term-born infants than in comparison infants
2018 NM FIT Annual Meeting 49
RBI
bull Describe your babyrsquos ________
bull Observe babies eatingbull Dribblingbull Noisybull Falls ldquoasleeprdquobull Pushes awaybull Arching
bull All babies refluxbull Meds donrsquot stop refluxbull Effects of PPIs and H2 inhibitors
2018 NM FIT Annual Meeting 50
Transdisciplinary and Coaching
bull Effective Transdisciplinary is dependent on recognizing our own strengths and limitations ndash self-reflection
bull TTA is critical
2018 NM FIT Annual Meeting 51
5302018
18
Can we predict
bull httppartnersforkidsorgwp-contentuploads20171115236_Neo_Cerebral-Palsy-Early-ID_Practice-Tool_Q4-RMpdf
bull We do NOT diagnose
2018 NM FIT Annual Meeting 52
FIT Technical Assistance Document-Evaluation and Assessment p24ICO
2018 NM FIT Annual Meeting 53
And this is where we need to build the capacityhellip
bull ldquoDue to the varying nature and purpose of the scores of each of the above approved tools the scores themselves will not lead to eligibility but rather they will provide additional information for the team to consider in reaching a determination of the childs developmental status and eligibility
determinationrdquo
2018 NM FIT Annual Meeting 54
5302018
19
Informed Clinical Opinionbull An evaluation of the childrsquos level of functioning in each of the
following developmental areas
bull Cognitive development
bull Physical development including vision and hearing
bull Communication development
bull Social or emotional development and
bull Adaptive development
bull A review of the pertinent records related to the childrsquos current health status and medical history and can include areas such as but not limited to feeding sleeping motor behavior state regulation communication visual tracking and auditory responses
bull All 5 developmental domains and pertinent information shall be addressed in the CME report as well as parent report and shall include a statement and approval signature indicating that Informed Clinical Opinion was used
2018 NM FIT Annual Meeting 55
ICO example
bull httpswwwyoutubecomwatchv=ztd2-O0z9rM
2018 NM FIT Annual Meeting 56
Risk for Cerebral Palsy Early Detection
and Early InterventionPoster Presentation at 2018 Annual FIT Meeting
NMOTA Conference
September 2018
Amazing Newborn Conference
November 8-9 2018
2018 NM FIT Annual Meeting 57
5302018
20
Risk Factors for Cerebral Palsy(McIntrye et al 2011)
bull Prior to conception
bull History of still births miscarriage premature birth family history of CP low SES
bull Early Pregnancy
bull Infection multiple births genetic predisposition male gender birth defects
bull During Pregnancy
bull Maternal disease preeclampsia infection placental abnormalities precursors to premature birth
2018 NM FIT Annual Meeting 58
Cerebral Palsy (Novak et al 2017)
bull Most Common Physical Disorder in Children
bull 2 in High Income Countries ldquoCP describes a group of developmental disorders of movement and posture causing activity restrictions or disability that are attributed to disturbances occurring in the fetal or infant brain The motor impairment may be accompanied by a seizure disorder or by impairment of sensation cognition communication and or behavior ldquo
bull Originates prenatally or early post-natally
2018 NM FIT Annual Meeting 59
Three Groups Classification
1 Premature Infants (30-40 of all cases)
2 Term infants who develop neonatal encephalopathy shortly after birth (15-20)
3 Term infants without risk factors (40-50)
2018 NM FIT Annual Meeting 60
5302018
21
86 of parents suspected their child
had Cerebral Palsy before a clinical
diagnosis was made
2018 NM FIT Annual Meeting 61
RISK for CP
Identification Intervention
2018 NM FIT Annual Meeting 62
How do we build capacity
bull REFLECTIONbull Individual
bull What do I NOT knowbull As a program director
bull What questions keep coming up
2018 NM FIT Annual Meeting 63
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65
5302018
4
NICU diagnoses that place a baby at risk for developmental delay
bull hellipAKA ldquoWhy does UNM NICU pick these babies up and transfer them to yourdquo
bull Cardiac conditions
bull ECMO
bull Cooling
bull ICO
2018 NM FIT Annual Meeting 10
Corrected Gestational Age (CGA)
bull Use until the infant reaches 24-36 months
bull Use for all developmental milestones including introduction of foods
bull The only schedule that should follow the preterm infantrsquos chronological age is their immunization schedule
bull AAP recommends correction until at least age 2 and most until age 3
2018 NM FIT Annual Meeting 11
Neurological Differences
bull When corrected to term the extremely preterm infantrsquos brain
bull Reduced gray matter volume
bull Increased cerebrospinal fluidbull Males have significantly lower white matter volumes
in specific areas
bull These findings persist to school age and are associated with learning challenges
Kesler SR et al J Peds 2008
2018 NM FIT Annual Meeting 12
5302018
5
We are growing brains in the NICU
2018 NM FIT Annual Meeting 13
PerinatalNeonatal Risk Factors
bull Risk Increased likelihood of disability
bull Risk ne disability
bull Many who have disability do not have risk
bull Some risk factors carry a higher risk of disability than others
bull More risk factors will lead to an additive effect
2018 NM FIT Annual Meeting 14
AAP Recommendation Screening
bull In the absence of risk or concernsbull 9 18 and 30 months
bull If surveillance identifies risk then additional screening is needed
bull Surveillance should be continued even if screening does not indicate a risk of delay
2018 NM FIT Annual Meeting 15
5302018
6
Long-term Outcome ndash this is where we come in
bull Complex interplaybull Biologic serves as the strongest predictor of long-
term function and development as the child recovers from perinatal and prenatal insults
bull Genetic and Environmental accounts for more of the variations seen in cognitive developmental
bull In most preterm children a positive environment can ameliorate many biologic risk factors
2018 NM FIT Annual Meeting 16
2 Year Re-hospitalizationOperationsle27 weeks
bull 12 Cerebral Palsy bull 6 mildbull 6 moderatesevere
bull 11 require special equipmentbull 86 bracesorthoticsbull 19 walker
Neonatal Research Network Data 2011
2018 NM FIT Annual Meeting 17
New Mexico Follow-Up Care- HM 14 (2018)
bull Currently we donrsquot have comprehensive care for high-risk neonates
bull UNMHrsquos NICU represents all regions of the State
bull 80 Medicaid
bull 2 No insurance
bull 50-60 from outside of Bernalillo County
bull More than 13 of births are to residents in rural and semi-rural areas
bull Preterm birth is more common in rural areas
bull 104 of children with special health care needs are without a usual source of care
2018 NM FIT Annual Meeting 18
5302018
7
United States Stats as of 2015
bull 4 million births per year
bull Gestational age
bull 96 are preterm (lt37 weeks gestation)
bull 7 late preterm (34-3667 weeks)
bull 26 (le34 weeks)
bull Weight
bull Low Birth Weight (lt2500g)
bull ~8 of annual births
bull ~90 (~288000) of these infants survive to discharge~ 13 will need specialty services
National Vital Statistics Report Vol 65 No 3 Preliminary Data
2018 NM FIT Annual Meeting 19
Plagiocephaly and Torticollis
bull NICU and Back to Sleep
bull Right-sided
bull AAP httpwwwaappublicationsorgnews20161027Plagiocephaly102016
bull Common condition
bull frac14 of US infants w some degree of positional plagiocephaly
bull The incidence has increased since AAP Back to Sleep campaign in 1994 (to prevent SIDS)
2018 NM FIT Annual Meeting 20
What to do about it
bull Ask your motor therapist
bull Ask your pediatrician
bull Do not wait to address itbull Positioningbull Routines
bull Active movements (you do not have to do passive stretch)
bull Best approach bull PREVENTION
2018 NM FIT Annual Meeting 21
5302018
8
Formulas
bull VLBW infants should remain on nutrient enriched post-discharge formulas (transitional) until at least 9 months CGA
bull Standard caloric of neosureenfacare 22kcaloz
bull Preterm infants need to consume at least as much formula per day as their term-born peers
bull If growth exceeds 2 birth percentile lines or if weightlength exceeds 90 20caloz term infant formula may be considered earlier
bull Kleinman RE American Academy of Pediatrics Committee on Nutrition 2004bull LewishttpswwwpreemietoolkitcompdfsE_PhysicalExaminationAssessmentRecommendations-for-
Postdischargepdf
2018 NM FIT Annual Meeting 22
Other Formulasbull No role for the use of low-iron formulas (constipation)
bull Soy protein-based formula not recommended for preterm infants weighing lt 1800 grams
bull Lacking in sufficient calcium phosphorous and protein
bull The presence of phytates (soy) decreases bioavailability of mineral absorption in the gut
Kleinman RE American Academy of Pediatrics Committee on Nutrition 2004
2018 NM FIT Annual Meeting 23
Standard Immunizations
bull Preterm infants should receive full immunizations based upon their chronological age consistent with the schedule and dose recommended for normal full-term infants
bull Synagis for some with chronic lung disease
AAP Committee on Infectious Diseases Red Book 2012
2018 NM FIT Annual Meeting 24
5302018
9
Put Your Microscope Lenses Onhellip
bull httpwwwpediatricsemoryedudivisionsneonatologydpcnicubehhtml
2018 NM FIT Annual Meeting 25
2018 NM FIT Annual Meeting 26
Synactive Theory
Infantrsquos communication is via hisher behavior
Behavior represents the hierarchical integration of his subsystems
Focuses on the unique way that each baby processes the environment at any given time
Subsystems are
interdependent
hierarchical
mature sequentially (Peters 2001)
2018 NM FIT Annual Meeting 27
5302018
10
Dynamic Systems
bull You cannot just look at each ldquopartrdquo of the baby You must look at how each of the pieces work together and affect the whole child and the family
2018 NM FIT Annual Meeting 28
NEW MEXICO DOH DDSD - FISCAL YEAR 2018
STATE GENERAL FUND
Services for Individuals with
Developmental Disabilities
and
FAMILY INFANT TODDLER PROGRAM
MEDICAID EPSDT
Services for infants and toddlers (birth to three)
with or at risk of Developmental Delays and their
families SERVICE DEFINITIONS AND STANDARDS
EFFECTIVE JULY 1 2017
2018 NM FIT Annual Meeting 29
COMPREHENSIVE MULTIDISCIPLINARY EVALUATION
bull The Comprehensive Multidisciplinary Evaluation (CME) is designed to inform the eligibility determination process through a timely non-discriminatory comprehensive and interdisciplinary approach The evaluation is designed to determine the developmental status of the child and to determine eligibility for early intervention services The evaluation shall include parentcaregiver report information from the routines based interview process and must cover the following developmental areas
bull Cognitive bull Physical motor (including vision and hearing) bull Communication bull Social or emotional bull Adaptive behavior
2018 NM FIT Annual Meeting 30
5302018
11
SCOPE OF SERVICE
bull ldquohelliphelliphellipEvaluation personnel should have an early childhood development background Evaluation personnel should also be trained in FIT evaluation and eligibility procedures and the tool(s) that they are administering Evaluation and assessment tools shall be used in accordance with the manual and established protocols To ensure accurate evaluation results evaluations must be conducted in an environment where the child typically spends hisher day
bull If the team decides to first conduct a developmental screening for a child referred and in accordance with NMAC 7308 10 E the Ages and Stages Questionnaire (ASQ) shall be utilized
bull A review and summary of the childrsquos records related to current health status and prior medical history (look at 2017 presentation)
2018 NM FIT Annual Meeting 31
Less than one-monthbull Given the unique characteristics of young infants and the challenges of
determining their developmental levels
bull For infants under one month of age (adjusted) the IDA will not be used Instead one of the approved tools below shall be used together with informed clinical opinion Informed clinical opinion (httpwwwnectacorg~pdfspubsnnotes10pdf) is used by early intervention professionals in the evaluation and assessment process to make a recommendation as to initial and continuing eligibility for services under Part C and as a basis for planning services to meet child and family needs
bull Informed clinical opinion makes use of qualitative and quantitative information to assist in forming a determination regarding difficult-to-measure aspects of current developmental status and the potential need for early intervention
2018 NM FIT Annual Meeting 32
Approved tools for infants under 1 month of age
bull AIMS (Alberta Infant Motor Scale)
bull TIMP (Test of Infant Motor Performance)
bull Infant Toddler Sensory Profile
bull Motor Skills Acquisition Checklist
bull Newborn Individualized Developmental Care and Assessment Program (NIDCAP) - for use with newborns in the newborn intensive care setting only
bull Newborn Behavior Assessment Scale (NBAS)
bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 33
5302018
12
For infants over one month of age (adjusted) and under four months of age including adjusted age the IDA shall be used in conjunction with one of the following approved tools listed below)
bull All 5 developmental domains shall be assessed and addressed in the CME report including parentcaregiver information AIMS (Alberta Infant Motor Scale
bull TIMP (Test of Infant Motor Performance) bull Infant Toddler Sensory Profile bull Peabody Developmental Motor Scale (PDMS-2) bull Motor Skills Acquisition Checklist bull REEL-3 bull The Rossetti Infant Toddler Language Scale bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 34
AIMS-Alberta Infant Motor ScalesMotor Assessment of the Developing Infant
bull 0 ndash 18 months or walking decreased accuracy at 3 months of
age decreased precision after 9 months of age
bull ldquoobservedrdquo or ldquonot observedrdquo Items in the observed range create a motor window
bull Subscale scores are calculated by giving credit for observed items within the motor window plus giving credit for all of the less mature items before the motor window
bull The AIMS total score calculated by summing the scores
bull Score converted to a percentile and compared with age-equivalent peers from the normative sample
bull BUY THE BOOK
2018 NM FIT Annual Meeting 35
Psychometrics of AIMSbull Normed on 2202 infants between the ages of 1 week to 18
months living in province of Alberta between 1990 and 1992
bull Interrater reliability using two therapists who assessed 221 typically developing r values from a Pearson Product 096 to 099
bull Test-retest reliability was assessed by administering the AIMS twice (7 days between assessments) to 233 infants r values from a Pearson Product Moment Correlation Coefficient ranged from 086 to 099 when the same assessor scored the AIMS on both assessment days
2018 NM FIT Annual Meeting 36
5302018
13
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull Recommended cut-off scores for atypical development are the 10th
percentile at 4 months of age and the 5th percentile at 8 months of age (Darrah Piper amp Watt 1998)
bull Even typically developing infants do not acquire gross motor skills at a stable rate and could have a score that places them below the ldquocut-offrdquo score (Darrah et al 1998)
bull It is important to complete serial assessments and not simply identify a child as being delayed based on a one time screening
2018 NM FIT Annual Meeting 37
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull AIMS is thought to be appropriate for children between 0 -18 months it has been shown to have a ceiling effect with low precision of measurement after ~ 9 months of age or when children are able to lower themselves from standing with control Liao amp Campbell 2004
bull AIMS is much better at identifying infants with motor disabilities at 6 9 and 12 months than at 3 months of age Kolobe amp Bulanda 2006
bull The AIMS misclassified a high percentage of 3 month old infants later diagnosed with cerebral palsy (CP) where as it did much better at identifying children later diagnosed with CP when using the 5th percentile as a cut-off at 6 9 and 12 months of age Kolobe amp Bulanda 2006
bull These studies results should encourage clinicians to use caution when interpreting AIMS scores for infants 3 months of age as well as infants who are 9 months of age or older
2018 NM FIT Annual Meeting 38
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoslip-throughrdquo
bull How do they ldquolookrdquobull Curled ndash ldquohe is so cuddlyrdquo
bull Sacral sitting
bull Hands closedbull Cortical thumb
bull Ankle Clonusbull A few beats vs prolonged
2018 NM FIT Annual Meeting 39
5302018
14
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoone with the surfacerdquo
bull ldquohe never stops movingrdquobull Pull-to-sit hellip And into standing
bull On toes (ask about walkers and saucers and Johnny jump-ups)
bull Does he bear weight
bull Head shape and its effects on prone and supine
2018 NM FIT Annual Meeting 40
AIMS ldquoBehaviorsrdquo (cont)
bull Locking kneesbull ldquoCollapsingrdquo
bull Pull-to-sit moves straight into standing
bull Asymmetries
2018 NM FIT Annual Meeting 41
Symmetry
bull Always look for symmetry (in all evaluations) ndashbull ldquoI think that he is going to be left-handedrdquo
bull Use your reasoning skills
bull Asymmetry because of gravity taking head to one side
bull 2 months before baby can maintain midlinebull Does baby visually scan to both sides
2018 NM FIT Annual Meeting 42
5302018
15
2018 NM FIT Annual Meeting 43
Think of Dynamic Systemshellip
bull ASQs are prime example (and IDA)
bull What are we really looking atbull Some examples of systems approach
2018 NM FIT Annual Meeting 44
2018 NM FIT Annual Meeting 45
5302018
16
2018 NM FIT Annual Meeting 46
2018 NM FIT Annual Meeting 47
2018 NM FIT Annual Meeting 48
5302018
17
When is a ldquosit uprdquo a bad thing Van Haastert et al
Dev Med Child Neurol 2012 Jun54(6)538-43
ldquoActive head lifting from supine in early infancy an indicator for non-optimal cognitive outcome in late infancyrdquo
bull AHLS is associated with a less favorable cognitive outcome in the second year of life in preterm and in term-born infants than in comparison infants
2018 NM FIT Annual Meeting 49
RBI
bull Describe your babyrsquos ________
bull Observe babies eatingbull Dribblingbull Noisybull Falls ldquoasleeprdquobull Pushes awaybull Arching
bull All babies refluxbull Meds donrsquot stop refluxbull Effects of PPIs and H2 inhibitors
2018 NM FIT Annual Meeting 50
Transdisciplinary and Coaching
bull Effective Transdisciplinary is dependent on recognizing our own strengths and limitations ndash self-reflection
bull TTA is critical
2018 NM FIT Annual Meeting 51
5302018
18
Can we predict
bull httppartnersforkidsorgwp-contentuploads20171115236_Neo_Cerebral-Palsy-Early-ID_Practice-Tool_Q4-RMpdf
bull We do NOT diagnose
2018 NM FIT Annual Meeting 52
FIT Technical Assistance Document-Evaluation and Assessment p24ICO
2018 NM FIT Annual Meeting 53
And this is where we need to build the capacityhellip
bull ldquoDue to the varying nature and purpose of the scores of each of the above approved tools the scores themselves will not lead to eligibility but rather they will provide additional information for the team to consider in reaching a determination of the childs developmental status and eligibility
determinationrdquo
2018 NM FIT Annual Meeting 54
5302018
19
Informed Clinical Opinionbull An evaluation of the childrsquos level of functioning in each of the
following developmental areas
bull Cognitive development
bull Physical development including vision and hearing
bull Communication development
bull Social or emotional development and
bull Adaptive development
bull A review of the pertinent records related to the childrsquos current health status and medical history and can include areas such as but not limited to feeding sleeping motor behavior state regulation communication visual tracking and auditory responses
bull All 5 developmental domains and pertinent information shall be addressed in the CME report as well as parent report and shall include a statement and approval signature indicating that Informed Clinical Opinion was used
2018 NM FIT Annual Meeting 55
ICO example
bull httpswwwyoutubecomwatchv=ztd2-O0z9rM
2018 NM FIT Annual Meeting 56
Risk for Cerebral Palsy Early Detection
and Early InterventionPoster Presentation at 2018 Annual FIT Meeting
NMOTA Conference
September 2018
Amazing Newborn Conference
November 8-9 2018
2018 NM FIT Annual Meeting 57
5302018
20
Risk Factors for Cerebral Palsy(McIntrye et al 2011)
bull Prior to conception
bull History of still births miscarriage premature birth family history of CP low SES
bull Early Pregnancy
bull Infection multiple births genetic predisposition male gender birth defects
bull During Pregnancy
bull Maternal disease preeclampsia infection placental abnormalities precursors to premature birth
2018 NM FIT Annual Meeting 58
Cerebral Palsy (Novak et al 2017)
bull Most Common Physical Disorder in Children
bull 2 in High Income Countries ldquoCP describes a group of developmental disorders of movement and posture causing activity restrictions or disability that are attributed to disturbances occurring in the fetal or infant brain The motor impairment may be accompanied by a seizure disorder or by impairment of sensation cognition communication and or behavior ldquo
bull Originates prenatally or early post-natally
2018 NM FIT Annual Meeting 59
Three Groups Classification
1 Premature Infants (30-40 of all cases)
2 Term infants who develop neonatal encephalopathy shortly after birth (15-20)
3 Term infants without risk factors (40-50)
2018 NM FIT Annual Meeting 60
5302018
21
86 of parents suspected their child
had Cerebral Palsy before a clinical
diagnosis was made
2018 NM FIT Annual Meeting 61
RISK for CP
Identification Intervention
2018 NM FIT Annual Meeting 62
How do we build capacity
bull REFLECTIONbull Individual
bull What do I NOT knowbull As a program director
bull What questions keep coming up
2018 NM FIT Annual Meeting 63
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65
5302018
5
We are growing brains in the NICU
2018 NM FIT Annual Meeting 13
PerinatalNeonatal Risk Factors
bull Risk Increased likelihood of disability
bull Risk ne disability
bull Many who have disability do not have risk
bull Some risk factors carry a higher risk of disability than others
bull More risk factors will lead to an additive effect
2018 NM FIT Annual Meeting 14
AAP Recommendation Screening
bull In the absence of risk or concernsbull 9 18 and 30 months
bull If surveillance identifies risk then additional screening is needed
bull Surveillance should be continued even if screening does not indicate a risk of delay
2018 NM FIT Annual Meeting 15
5302018
6
Long-term Outcome ndash this is where we come in
bull Complex interplaybull Biologic serves as the strongest predictor of long-
term function and development as the child recovers from perinatal and prenatal insults
bull Genetic and Environmental accounts for more of the variations seen in cognitive developmental
bull In most preterm children a positive environment can ameliorate many biologic risk factors
2018 NM FIT Annual Meeting 16
2 Year Re-hospitalizationOperationsle27 weeks
bull 12 Cerebral Palsy bull 6 mildbull 6 moderatesevere
bull 11 require special equipmentbull 86 bracesorthoticsbull 19 walker
Neonatal Research Network Data 2011
2018 NM FIT Annual Meeting 17
New Mexico Follow-Up Care- HM 14 (2018)
bull Currently we donrsquot have comprehensive care for high-risk neonates
bull UNMHrsquos NICU represents all regions of the State
bull 80 Medicaid
bull 2 No insurance
bull 50-60 from outside of Bernalillo County
bull More than 13 of births are to residents in rural and semi-rural areas
bull Preterm birth is more common in rural areas
bull 104 of children with special health care needs are without a usual source of care
2018 NM FIT Annual Meeting 18
5302018
7
United States Stats as of 2015
bull 4 million births per year
bull Gestational age
bull 96 are preterm (lt37 weeks gestation)
bull 7 late preterm (34-3667 weeks)
bull 26 (le34 weeks)
bull Weight
bull Low Birth Weight (lt2500g)
bull ~8 of annual births
bull ~90 (~288000) of these infants survive to discharge~ 13 will need specialty services
National Vital Statistics Report Vol 65 No 3 Preliminary Data
2018 NM FIT Annual Meeting 19
Plagiocephaly and Torticollis
bull NICU and Back to Sleep
bull Right-sided
bull AAP httpwwwaappublicationsorgnews20161027Plagiocephaly102016
bull Common condition
bull frac14 of US infants w some degree of positional plagiocephaly
bull The incidence has increased since AAP Back to Sleep campaign in 1994 (to prevent SIDS)
2018 NM FIT Annual Meeting 20
What to do about it
bull Ask your motor therapist
bull Ask your pediatrician
bull Do not wait to address itbull Positioningbull Routines
bull Active movements (you do not have to do passive stretch)
bull Best approach bull PREVENTION
2018 NM FIT Annual Meeting 21
5302018
8
Formulas
bull VLBW infants should remain on nutrient enriched post-discharge formulas (transitional) until at least 9 months CGA
bull Standard caloric of neosureenfacare 22kcaloz
bull Preterm infants need to consume at least as much formula per day as their term-born peers
bull If growth exceeds 2 birth percentile lines or if weightlength exceeds 90 20caloz term infant formula may be considered earlier
bull Kleinman RE American Academy of Pediatrics Committee on Nutrition 2004bull LewishttpswwwpreemietoolkitcompdfsE_PhysicalExaminationAssessmentRecommendations-for-
Postdischargepdf
2018 NM FIT Annual Meeting 22
Other Formulasbull No role for the use of low-iron formulas (constipation)
bull Soy protein-based formula not recommended for preterm infants weighing lt 1800 grams
bull Lacking in sufficient calcium phosphorous and protein
bull The presence of phytates (soy) decreases bioavailability of mineral absorption in the gut
Kleinman RE American Academy of Pediatrics Committee on Nutrition 2004
2018 NM FIT Annual Meeting 23
Standard Immunizations
bull Preterm infants should receive full immunizations based upon their chronological age consistent with the schedule and dose recommended for normal full-term infants
bull Synagis for some with chronic lung disease
AAP Committee on Infectious Diseases Red Book 2012
2018 NM FIT Annual Meeting 24
5302018
9
Put Your Microscope Lenses Onhellip
bull httpwwwpediatricsemoryedudivisionsneonatologydpcnicubehhtml
2018 NM FIT Annual Meeting 25
2018 NM FIT Annual Meeting 26
Synactive Theory
Infantrsquos communication is via hisher behavior
Behavior represents the hierarchical integration of his subsystems
Focuses on the unique way that each baby processes the environment at any given time
Subsystems are
interdependent
hierarchical
mature sequentially (Peters 2001)
2018 NM FIT Annual Meeting 27
5302018
10
Dynamic Systems
bull You cannot just look at each ldquopartrdquo of the baby You must look at how each of the pieces work together and affect the whole child and the family
2018 NM FIT Annual Meeting 28
NEW MEXICO DOH DDSD - FISCAL YEAR 2018
STATE GENERAL FUND
Services for Individuals with
Developmental Disabilities
and
FAMILY INFANT TODDLER PROGRAM
MEDICAID EPSDT
Services for infants and toddlers (birth to three)
with or at risk of Developmental Delays and their
families SERVICE DEFINITIONS AND STANDARDS
EFFECTIVE JULY 1 2017
2018 NM FIT Annual Meeting 29
COMPREHENSIVE MULTIDISCIPLINARY EVALUATION
bull The Comprehensive Multidisciplinary Evaluation (CME) is designed to inform the eligibility determination process through a timely non-discriminatory comprehensive and interdisciplinary approach The evaluation is designed to determine the developmental status of the child and to determine eligibility for early intervention services The evaluation shall include parentcaregiver report information from the routines based interview process and must cover the following developmental areas
bull Cognitive bull Physical motor (including vision and hearing) bull Communication bull Social or emotional bull Adaptive behavior
2018 NM FIT Annual Meeting 30
5302018
11
SCOPE OF SERVICE
bull ldquohelliphelliphellipEvaluation personnel should have an early childhood development background Evaluation personnel should also be trained in FIT evaluation and eligibility procedures and the tool(s) that they are administering Evaluation and assessment tools shall be used in accordance with the manual and established protocols To ensure accurate evaluation results evaluations must be conducted in an environment where the child typically spends hisher day
bull If the team decides to first conduct a developmental screening for a child referred and in accordance with NMAC 7308 10 E the Ages and Stages Questionnaire (ASQ) shall be utilized
bull A review and summary of the childrsquos records related to current health status and prior medical history (look at 2017 presentation)
2018 NM FIT Annual Meeting 31
Less than one-monthbull Given the unique characteristics of young infants and the challenges of
determining their developmental levels
bull For infants under one month of age (adjusted) the IDA will not be used Instead one of the approved tools below shall be used together with informed clinical opinion Informed clinical opinion (httpwwwnectacorg~pdfspubsnnotes10pdf) is used by early intervention professionals in the evaluation and assessment process to make a recommendation as to initial and continuing eligibility for services under Part C and as a basis for planning services to meet child and family needs
bull Informed clinical opinion makes use of qualitative and quantitative information to assist in forming a determination regarding difficult-to-measure aspects of current developmental status and the potential need for early intervention
2018 NM FIT Annual Meeting 32
Approved tools for infants under 1 month of age
bull AIMS (Alberta Infant Motor Scale)
bull TIMP (Test of Infant Motor Performance)
bull Infant Toddler Sensory Profile
bull Motor Skills Acquisition Checklist
bull Newborn Individualized Developmental Care and Assessment Program (NIDCAP) - for use with newborns in the newborn intensive care setting only
bull Newborn Behavior Assessment Scale (NBAS)
bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 33
5302018
12
For infants over one month of age (adjusted) and under four months of age including adjusted age the IDA shall be used in conjunction with one of the following approved tools listed below)
bull All 5 developmental domains shall be assessed and addressed in the CME report including parentcaregiver information AIMS (Alberta Infant Motor Scale
bull TIMP (Test of Infant Motor Performance) bull Infant Toddler Sensory Profile bull Peabody Developmental Motor Scale (PDMS-2) bull Motor Skills Acquisition Checklist bull REEL-3 bull The Rossetti Infant Toddler Language Scale bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 34
AIMS-Alberta Infant Motor ScalesMotor Assessment of the Developing Infant
bull 0 ndash 18 months or walking decreased accuracy at 3 months of
age decreased precision after 9 months of age
bull ldquoobservedrdquo or ldquonot observedrdquo Items in the observed range create a motor window
bull Subscale scores are calculated by giving credit for observed items within the motor window plus giving credit for all of the less mature items before the motor window
bull The AIMS total score calculated by summing the scores
bull Score converted to a percentile and compared with age-equivalent peers from the normative sample
bull BUY THE BOOK
2018 NM FIT Annual Meeting 35
Psychometrics of AIMSbull Normed on 2202 infants between the ages of 1 week to 18
months living in province of Alberta between 1990 and 1992
bull Interrater reliability using two therapists who assessed 221 typically developing r values from a Pearson Product 096 to 099
bull Test-retest reliability was assessed by administering the AIMS twice (7 days between assessments) to 233 infants r values from a Pearson Product Moment Correlation Coefficient ranged from 086 to 099 when the same assessor scored the AIMS on both assessment days
2018 NM FIT Annual Meeting 36
5302018
13
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull Recommended cut-off scores for atypical development are the 10th
percentile at 4 months of age and the 5th percentile at 8 months of age (Darrah Piper amp Watt 1998)
bull Even typically developing infants do not acquire gross motor skills at a stable rate and could have a score that places them below the ldquocut-offrdquo score (Darrah et al 1998)
bull It is important to complete serial assessments and not simply identify a child as being delayed based on a one time screening
2018 NM FIT Annual Meeting 37
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull AIMS is thought to be appropriate for children between 0 -18 months it has been shown to have a ceiling effect with low precision of measurement after ~ 9 months of age or when children are able to lower themselves from standing with control Liao amp Campbell 2004
bull AIMS is much better at identifying infants with motor disabilities at 6 9 and 12 months than at 3 months of age Kolobe amp Bulanda 2006
bull The AIMS misclassified a high percentage of 3 month old infants later diagnosed with cerebral palsy (CP) where as it did much better at identifying children later diagnosed with CP when using the 5th percentile as a cut-off at 6 9 and 12 months of age Kolobe amp Bulanda 2006
bull These studies results should encourage clinicians to use caution when interpreting AIMS scores for infants 3 months of age as well as infants who are 9 months of age or older
2018 NM FIT Annual Meeting 38
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoslip-throughrdquo
bull How do they ldquolookrdquobull Curled ndash ldquohe is so cuddlyrdquo
bull Sacral sitting
bull Hands closedbull Cortical thumb
bull Ankle Clonusbull A few beats vs prolonged
2018 NM FIT Annual Meeting 39
5302018
14
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoone with the surfacerdquo
bull ldquohe never stops movingrdquobull Pull-to-sit hellip And into standing
bull On toes (ask about walkers and saucers and Johnny jump-ups)
bull Does he bear weight
bull Head shape and its effects on prone and supine
2018 NM FIT Annual Meeting 40
AIMS ldquoBehaviorsrdquo (cont)
bull Locking kneesbull ldquoCollapsingrdquo
bull Pull-to-sit moves straight into standing
bull Asymmetries
2018 NM FIT Annual Meeting 41
Symmetry
bull Always look for symmetry (in all evaluations) ndashbull ldquoI think that he is going to be left-handedrdquo
bull Use your reasoning skills
bull Asymmetry because of gravity taking head to one side
bull 2 months before baby can maintain midlinebull Does baby visually scan to both sides
2018 NM FIT Annual Meeting 42
5302018
15
2018 NM FIT Annual Meeting 43
Think of Dynamic Systemshellip
bull ASQs are prime example (and IDA)
bull What are we really looking atbull Some examples of systems approach
2018 NM FIT Annual Meeting 44
2018 NM FIT Annual Meeting 45
5302018
16
2018 NM FIT Annual Meeting 46
2018 NM FIT Annual Meeting 47
2018 NM FIT Annual Meeting 48
5302018
17
When is a ldquosit uprdquo a bad thing Van Haastert et al
Dev Med Child Neurol 2012 Jun54(6)538-43
ldquoActive head lifting from supine in early infancy an indicator for non-optimal cognitive outcome in late infancyrdquo
bull AHLS is associated with a less favorable cognitive outcome in the second year of life in preterm and in term-born infants than in comparison infants
2018 NM FIT Annual Meeting 49
RBI
bull Describe your babyrsquos ________
bull Observe babies eatingbull Dribblingbull Noisybull Falls ldquoasleeprdquobull Pushes awaybull Arching
bull All babies refluxbull Meds donrsquot stop refluxbull Effects of PPIs and H2 inhibitors
2018 NM FIT Annual Meeting 50
Transdisciplinary and Coaching
bull Effective Transdisciplinary is dependent on recognizing our own strengths and limitations ndash self-reflection
bull TTA is critical
2018 NM FIT Annual Meeting 51
5302018
18
Can we predict
bull httppartnersforkidsorgwp-contentuploads20171115236_Neo_Cerebral-Palsy-Early-ID_Practice-Tool_Q4-RMpdf
bull We do NOT diagnose
2018 NM FIT Annual Meeting 52
FIT Technical Assistance Document-Evaluation and Assessment p24ICO
2018 NM FIT Annual Meeting 53
And this is where we need to build the capacityhellip
bull ldquoDue to the varying nature and purpose of the scores of each of the above approved tools the scores themselves will not lead to eligibility but rather they will provide additional information for the team to consider in reaching a determination of the childs developmental status and eligibility
determinationrdquo
2018 NM FIT Annual Meeting 54
5302018
19
Informed Clinical Opinionbull An evaluation of the childrsquos level of functioning in each of the
following developmental areas
bull Cognitive development
bull Physical development including vision and hearing
bull Communication development
bull Social or emotional development and
bull Adaptive development
bull A review of the pertinent records related to the childrsquos current health status and medical history and can include areas such as but not limited to feeding sleeping motor behavior state regulation communication visual tracking and auditory responses
bull All 5 developmental domains and pertinent information shall be addressed in the CME report as well as parent report and shall include a statement and approval signature indicating that Informed Clinical Opinion was used
2018 NM FIT Annual Meeting 55
ICO example
bull httpswwwyoutubecomwatchv=ztd2-O0z9rM
2018 NM FIT Annual Meeting 56
Risk for Cerebral Palsy Early Detection
and Early InterventionPoster Presentation at 2018 Annual FIT Meeting
NMOTA Conference
September 2018
Amazing Newborn Conference
November 8-9 2018
2018 NM FIT Annual Meeting 57
5302018
20
Risk Factors for Cerebral Palsy(McIntrye et al 2011)
bull Prior to conception
bull History of still births miscarriage premature birth family history of CP low SES
bull Early Pregnancy
bull Infection multiple births genetic predisposition male gender birth defects
bull During Pregnancy
bull Maternal disease preeclampsia infection placental abnormalities precursors to premature birth
2018 NM FIT Annual Meeting 58
Cerebral Palsy (Novak et al 2017)
bull Most Common Physical Disorder in Children
bull 2 in High Income Countries ldquoCP describes a group of developmental disorders of movement and posture causing activity restrictions or disability that are attributed to disturbances occurring in the fetal or infant brain The motor impairment may be accompanied by a seizure disorder or by impairment of sensation cognition communication and or behavior ldquo
bull Originates prenatally or early post-natally
2018 NM FIT Annual Meeting 59
Three Groups Classification
1 Premature Infants (30-40 of all cases)
2 Term infants who develop neonatal encephalopathy shortly after birth (15-20)
3 Term infants without risk factors (40-50)
2018 NM FIT Annual Meeting 60
5302018
21
86 of parents suspected their child
had Cerebral Palsy before a clinical
diagnosis was made
2018 NM FIT Annual Meeting 61
RISK for CP
Identification Intervention
2018 NM FIT Annual Meeting 62
How do we build capacity
bull REFLECTIONbull Individual
bull What do I NOT knowbull As a program director
bull What questions keep coming up
2018 NM FIT Annual Meeting 63
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65
5302018
6
Long-term Outcome ndash this is where we come in
bull Complex interplaybull Biologic serves as the strongest predictor of long-
term function and development as the child recovers from perinatal and prenatal insults
bull Genetic and Environmental accounts for more of the variations seen in cognitive developmental
bull In most preterm children a positive environment can ameliorate many biologic risk factors
2018 NM FIT Annual Meeting 16
2 Year Re-hospitalizationOperationsle27 weeks
bull 12 Cerebral Palsy bull 6 mildbull 6 moderatesevere
bull 11 require special equipmentbull 86 bracesorthoticsbull 19 walker
Neonatal Research Network Data 2011
2018 NM FIT Annual Meeting 17
New Mexico Follow-Up Care- HM 14 (2018)
bull Currently we donrsquot have comprehensive care for high-risk neonates
bull UNMHrsquos NICU represents all regions of the State
bull 80 Medicaid
bull 2 No insurance
bull 50-60 from outside of Bernalillo County
bull More than 13 of births are to residents in rural and semi-rural areas
bull Preterm birth is more common in rural areas
bull 104 of children with special health care needs are without a usual source of care
2018 NM FIT Annual Meeting 18
5302018
7
United States Stats as of 2015
bull 4 million births per year
bull Gestational age
bull 96 are preterm (lt37 weeks gestation)
bull 7 late preterm (34-3667 weeks)
bull 26 (le34 weeks)
bull Weight
bull Low Birth Weight (lt2500g)
bull ~8 of annual births
bull ~90 (~288000) of these infants survive to discharge~ 13 will need specialty services
National Vital Statistics Report Vol 65 No 3 Preliminary Data
2018 NM FIT Annual Meeting 19
Plagiocephaly and Torticollis
bull NICU and Back to Sleep
bull Right-sided
bull AAP httpwwwaappublicationsorgnews20161027Plagiocephaly102016
bull Common condition
bull frac14 of US infants w some degree of positional plagiocephaly
bull The incidence has increased since AAP Back to Sleep campaign in 1994 (to prevent SIDS)
2018 NM FIT Annual Meeting 20
What to do about it
bull Ask your motor therapist
bull Ask your pediatrician
bull Do not wait to address itbull Positioningbull Routines
bull Active movements (you do not have to do passive stretch)
bull Best approach bull PREVENTION
2018 NM FIT Annual Meeting 21
5302018
8
Formulas
bull VLBW infants should remain on nutrient enriched post-discharge formulas (transitional) until at least 9 months CGA
bull Standard caloric of neosureenfacare 22kcaloz
bull Preterm infants need to consume at least as much formula per day as their term-born peers
bull If growth exceeds 2 birth percentile lines or if weightlength exceeds 90 20caloz term infant formula may be considered earlier
bull Kleinman RE American Academy of Pediatrics Committee on Nutrition 2004bull LewishttpswwwpreemietoolkitcompdfsE_PhysicalExaminationAssessmentRecommendations-for-
Postdischargepdf
2018 NM FIT Annual Meeting 22
Other Formulasbull No role for the use of low-iron formulas (constipation)
bull Soy protein-based formula not recommended for preterm infants weighing lt 1800 grams
bull Lacking in sufficient calcium phosphorous and protein
bull The presence of phytates (soy) decreases bioavailability of mineral absorption in the gut
Kleinman RE American Academy of Pediatrics Committee on Nutrition 2004
2018 NM FIT Annual Meeting 23
Standard Immunizations
bull Preterm infants should receive full immunizations based upon their chronological age consistent with the schedule and dose recommended for normal full-term infants
bull Synagis for some with chronic lung disease
AAP Committee on Infectious Diseases Red Book 2012
2018 NM FIT Annual Meeting 24
5302018
9
Put Your Microscope Lenses Onhellip
bull httpwwwpediatricsemoryedudivisionsneonatologydpcnicubehhtml
2018 NM FIT Annual Meeting 25
2018 NM FIT Annual Meeting 26
Synactive Theory
Infantrsquos communication is via hisher behavior
Behavior represents the hierarchical integration of his subsystems
Focuses on the unique way that each baby processes the environment at any given time
Subsystems are
interdependent
hierarchical
mature sequentially (Peters 2001)
2018 NM FIT Annual Meeting 27
5302018
10
Dynamic Systems
bull You cannot just look at each ldquopartrdquo of the baby You must look at how each of the pieces work together and affect the whole child and the family
2018 NM FIT Annual Meeting 28
NEW MEXICO DOH DDSD - FISCAL YEAR 2018
STATE GENERAL FUND
Services for Individuals with
Developmental Disabilities
and
FAMILY INFANT TODDLER PROGRAM
MEDICAID EPSDT
Services for infants and toddlers (birth to three)
with or at risk of Developmental Delays and their
families SERVICE DEFINITIONS AND STANDARDS
EFFECTIVE JULY 1 2017
2018 NM FIT Annual Meeting 29
COMPREHENSIVE MULTIDISCIPLINARY EVALUATION
bull The Comprehensive Multidisciplinary Evaluation (CME) is designed to inform the eligibility determination process through a timely non-discriminatory comprehensive and interdisciplinary approach The evaluation is designed to determine the developmental status of the child and to determine eligibility for early intervention services The evaluation shall include parentcaregiver report information from the routines based interview process and must cover the following developmental areas
bull Cognitive bull Physical motor (including vision and hearing) bull Communication bull Social or emotional bull Adaptive behavior
2018 NM FIT Annual Meeting 30
5302018
11
SCOPE OF SERVICE
bull ldquohelliphelliphellipEvaluation personnel should have an early childhood development background Evaluation personnel should also be trained in FIT evaluation and eligibility procedures and the tool(s) that they are administering Evaluation and assessment tools shall be used in accordance with the manual and established protocols To ensure accurate evaluation results evaluations must be conducted in an environment where the child typically spends hisher day
bull If the team decides to first conduct a developmental screening for a child referred and in accordance with NMAC 7308 10 E the Ages and Stages Questionnaire (ASQ) shall be utilized
bull A review and summary of the childrsquos records related to current health status and prior medical history (look at 2017 presentation)
2018 NM FIT Annual Meeting 31
Less than one-monthbull Given the unique characteristics of young infants and the challenges of
determining their developmental levels
bull For infants under one month of age (adjusted) the IDA will not be used Instead one of the approved tools below shall be used together with informed clinical opinion Informed clinical opinion (httpwwwnectacorg~pdfspubsnnotes10pdf) is used by early intervention professionals in the evaluation and assessment process to make a recommendation as to initial and continuing eligibility for services under Part C and as a basis for planning services to meet child and family needs
bull Informed clinical opinion makes use of qualitative and quantitative information to assist in forming a determination regarding difficult-to-measure aspects of current developmental status and the potential need for early intervention
2018 NM FIT Annual Meeting 32
Approved tools for infants under 1 month of age
bull AIMS (Alberta Infant Motor Scale)
bull TIMP (Test of Infant Motor Performance)
bull Infant Toddler Sensory Profile
bull Motor Skills Acquisition Checklist
bull Newborn Individualized Developmental Care and Assessment Program (NIDCAP) - for use with newborns in the newborn intensive care setting only
bull Newborn Behavior Assessment Scale (NBAS)
bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 33
5302018
12
For infants over one month of age (adjusted) and under four months of age including adjusted age the IDA shall be used in conjunction with one of the following approved tools listed below)
bull All 5 developmental domains shall be assessed and addressed in the CME report including parentcaregiver information AIMS (Alberta Infant Motor Scale
bull TIMP (Test of Infant Motor Performance) bull Infant Toddler Sensory Profile bull Peabody Developmental Motor Scale (PDMS-2) bull Motor Skills Acquisition Checklist bull REEL-3 bull The Rossetti Infant Toddler Language Scale bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 34
AIMS-Alberta Infant Motor ScalesMotor Assessment of the Developing Infant
bull 0 ndash 18 months or walking decreased accuracy at 3 months of
age decreased precision after 9 months of age
bull ldquoobservedrdquo or ldquonot observedrdquo Items in the observed range create a motor window
bull Subscale scores are calculated by giving credit for observed items within the motor window plus giving credit for all of the less mature items before the motor window
bull The AIMS total score calculated by summing the scores
bull Score converted to a percentile and compared with age-equivalent peers from the normative sample
bull BUY THE BOOK
2018 NM FIT Annual Meeting 35
Psychometrics of AIMSbull Normed on 2202 infants between the ages of 1 week to 18
months living in province of Alberta between 1990 and 1992
bull Interrater reliability using two therapists who assessed 221 typically developing r values from a Pearson Product 096 to 099
bull Test-retest reliability was assessed by administering the AIMS twice (7 days between assessments) to 233 infants r values from a Pearson Product Moment Correlation Coefficient ranged from 086 to 099 when the same assessor scored the AIMS on both assessment days
2018 NM FIT Annual Meeting 36
5302018
13
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull Recommended cut-off scores for atypical development are the 10th
percentile at 4 months of age and the 5th percentile at 8 months of age (Darrah Piper amp Watt 1998)
bull Even typically developing infants do not acquire gross motor skills at a stable rate and could have a score that places them below the ldquocut-offrdquo score (Darrah et al 1998)
bull It is important to complete serial assessments and not simply identify a child as being delayed based on a one time screening
2018 NM FIT Annual Meeting 37
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull AIMS is thought to be appropriate for children between 0 -18 months it has been shown to have a ceiling effect with low precision of measurement after ~ 9 months of age or when children are able to lower themselves from standing with control Liao amp Campbell 2004
bull AIMS is much better at identifying infants with motor disabilities at 6 9 and 12 months than at 3 months of age Kolobe amp Bulanda 2006
bull The AIMS misclassified a high percentage of 3 month old infants later diagnosed with cerebral palsy (CP) where as it did much better at identifying children later diagnosed with CP when using the 5th percentile as a cut-off at 6 9 and 12 months of age Kolobe amp Bulanda 2006
bull These studies results should encourage clinicians to use caution when interpreting AIMS scores for infants 3 months of age as well as infants who are 9 months of age or older
2018 NM FIT Annual Meeting 38
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoslip-throughrdquo
bull How do they ldquolookrdquobull Curled ndash ldquohe is so cuddlyrdquo
bull Sacral sitting
bull Hands closedbull Cortical thumb
bull Ankle Clonusbull A few beats vs prolonged
2018 NM FIT Annual Meeting 39
5302018
14
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoone with the surfacerdquo
bull ldquohe never stops movingrdquobull Pull-to-sit hellip And into standing
bull On toes (ask about walkers and saucers and Johnny jump-ups)
bull Does he bear weight
bull Head shape and its effects on prone and supine
2018 NM FIT Annual Meeting 40
AIMS ldquoBehaviorsrdquo (cont)
bull Locking kneesbull ldquoCollapsingrdquo
bull Pull-to-sit moves straight into standing
bull Asymmetries
2018 NM FIT Annual Meeting 41
Symmetry
bull Always look for symmetry (in all evaluations) ndashbull ldquoI think that he is going to be left-handedrdquo
bull Use your reasoning skills
bull Asymmetry because of gravity taking head to one side
bull 2 months before baby can maintain midlinebull Does baby visually scan to both sides
2018 NM FIT Annual Meeting 42
5302018
15
2018 NM FIT Annual Meeting 43
Think of Dynamic Systemshellip
bull ASQs are prime example (and IDA)
bull What are we really looking atbull Some examples of systems approach
2018 NM FIT Annual Meeting 44
2018 NM FIT Annual Meeting 45
5302018
16
2018 NM FIT Annual Meeting 46
2018 NM FIT Annual Meeting 47
2018 NM FIT Annual Meeting 48
5302018
17
When is a ldquosit uprdquo a bad thing Van Haastert et al
Dev Med Child Neurol 2012 Jun54(6)538-43
ldquoActive head lifting from supine in early infancy an indicator for non-optimal cognitive outcome in late infancyrdquo
bull AHLS is associated with a less favorable cognitive outcome in the second year of life in preterm and in term-born infants than in comparison infants
2018 NM FIT Annual Meeting 49
RBI
bull Describe your babyrsquos ________
bull Observe babies eatingbull Dribblingbull Noisybull Falls ldquoasleeprdquobull Pushes awaybull Arching
bull All babies refluxbull Meds donrsquot stop refluxbull Effects of PPIs and H2 inhibitors
2018 NM FIT Annual Meeting 50
Transdisciplinary and Coaching
bull Effective Transdisciplinary is dependent on recognizing our own strengths and limitations ndash self-reflection
bull TTA is critical
2018 NM FIT Annual Meeting 51
5302018
18
Can we predict
bull httppartnersforkidsorgwp-contentuploads20171115236_Neo_Cerebral-Palsy-Early-ID_Practice-Tool_Q4-RMpdf
bull We do NOT diagnose
2018 NM FIT Annual Meeting 52
FIT Technical Assistance Document-Evaluation and Assessment p24ICO
2018 NM FIT Annual Meeting 53
And this is where we need to build the capacityhellip
bull ldquoDue to the varying nature and purpose of the scores of each of the above approved tools the scores themselves will not lead to eligibility but rather they will provide additional information for the team to consider in reaching a determination of the childs developmental status and eligibility
determinationrdquo
2018 NM FIT Annual Meeting 54
5302018
19
Informed Clinical Opinionbull An evaluation of the childrsquos level of functioning in each of the
following developmental areas
bull Cognitive development
bull Physical development including vision and hearing
bull Communication development
bull Social or emotional development and
bull Adaptive development
bull A review of the pertinent records related to the childrsquos current health status and medical history and can include areas such as but not limited to feeding sleeping motor behavior state regulation communication visual tracking and auditory responses
bull All 5 developmental domains and pertinent information shall be addressed in the CME report as well as parent report and shall include a statement and approval signature indicating that Informed Clinical Opinion was used
2018 NM FIT Annual Meeting 55
ICO example
bull httpswwwyoutubecomwatchv=ztd2-O0z9rM
2018 NM FIT Annual Meeting 56
Risk for Cerebral Palsy Early Detection
and Early InterventionPoster Presentation at 2018 Annual FIT Meeting
NMOTA Conference
September 2018
Amazing Newborn Conference
November 8-9 2018
2018 NM FIT Annual Meeting 57
5302018
20
Risk Factors for Cerebral Palsy(McIntrye et al 2011)
bull Prior to conception
bull History of still births miscarriage premature birth family history of CP low SES
bull Early Pregnancy
bull Infection multiple births genetic predisposition male gender birth defects
bull During Pregnancy
bull Maternal disease preeclampsia infection placental abnormalities precursors to premature birth
2018 NM FIT Annual Meeting 58
Cerebral Palsy (Novak et al 2017)
bull Most Common Physical Disorder in Children
bull 2 in High Income Countries ldquoCP describes a group of developmental disorders of movement and posture causing activity restrictions or disability that are attributed to disturbances occurring in the fetal or infant brain The motor impairment may be accompanied by a seizure disorder or by impairment of sensation cognition communication and or behavior ldquo
bull Originates prenatally or early post-natally
2018 NM FIT Annual Meeting 59
Three Groups Classification
1 Premature Infants (30-40 of all cases)
2 Term infants who develop neonatal encephalopathy shortly after birth (15-20)
3 Term infants without risk factors (40-50)
2018 NM FIT Annual Meeting 60
5302018
21
86 of parents suspected their child
had Cerebral Palsy before a clinical
diagnosis was made
2018 NM FIT Annual Meeting 61
RISK for CP
Identification Intervention
2018 NM FIT Annual Meeting 62
How do we build capacity
bull REFLECTIONbull Individual
bull What do I NOT knowbull As a program director
bull What questions keep coming up
2018 NM FIT Annual Meeting 63
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65
5302018
7
United States Stats as of 2015
bull 4 million births per year
bull Gestational age
bull 96 are preterm (lt37 weeks gestation)
bull 7 late preterm (34-3667 weeks)
bull 26 (le34 weeks)
bull Weight
bull Low Birth Weight (lt2500g)
bull ~8 of annual births
bull ~90 (~288000) of these infants survive to discharge~ 13 will need specialty services
National Vital Statistics Report Vol 65 No 3 Preliminary Data
2018 NM FIT Annual Meeting 19
Plagiocephaly and Torticollis
bull NICU and Back to Sleep
bull Right-sided
bull AAP httpwwwaappublicationsorgnews20161027Plagiocephaly102016
bull Common condition
bull frac14 of US infants w some degree of positional plagiocephaly
bull The incidence has increased since AAP Back to Sleep campaign in 1994 (to prevent SIDS)
2018 NM FIT Annual Meeting 20
What to do about it
bull Ask your motor therapist
bull Ask your pediatrician
bull Do not wait to address itbull Positioningbull Routines
bull Active movements (you do not have to do passive stretch)
bull Best approach bull PREVENTION
2018 NM FIT Annual Meeting 21
5302018
8
Formulas
bull VLBW infants should remain on nutrient enriched post-discharge formulas (transitional) until at least 9 months CGA
bull Standard caloric of neosureenfacare 22kcaloz
bull Preterm infants need to consume at least as much formula per day as their term-born peers
bull If growth exceeds 2 birth percentile lines or if weightlength exceeds 90 20caloz term infant formula may be considered earlier
bull Kleinman RE American Academy of Pediatrics Committee on Nutrition 2004bull LewishttpswwwpreemietoolkitcompdfsE_PhysicalExaminationAssessmentRecommendations-for-
Postdischargepdf
2018 NM FIT Annual Meeting 22
Other Formulasbull No role for the use of low-iron formulas (constipation)
bull Soy protein-based formula not recommended for preterm infants weighing lt 1800 grams
bull Lacking in sufficient calcium phosphorous and protein
bull The presence of phytates (soy) decreases bioavailability of mineral absorption in the gut
Kleinman RE American Academy of Pediatrics Committee on Nutrition 2004
2018 NM FIT Annual Meeting 23
Standard Immunizations
bull Preterm infants should receive full immunizations based upon their chronological age consistent with the schedule and dose recommended for normal full-term infants
bull Synagis for some with chronic lung disease
AAP Committee on Infectious Diseases Red Book 2012
2018 NM FIT Annual Meeting 24
5302018
9
Put Your Microscope Lenses Onhellip
bull httpwwwpediatricsemoryedudivisionsneonatologydpcnicubehhtml
2018 NM FIT Annual Meeting 25
2018 NM FIT Annual Meeting 26
Synactive Theory
Infantrsquos communication is via hisher behavior
Behavior represents the hierarchical integration of his subsystems
Focuses on the unique way that each baby processes the environment at any given time
Subsystems are
interdependent
hierarchical
mature sequentially (Peters 2001)
2018 NM FIT Annual Meeting 27
5302018
10
Dynamic Systems
bull You cannot just look at each ldquopartrdquo of the baby You must look at how each of the pieces work together and affect the whole child and the family
2018 NM FIT Annual Meeting 28
NEW MEXICO DOH DDSD - FISCAL YEAR 2018
STATE GENERAL FUND
Services for Individuals with
Developmental Disabilities
and
FAMILY INFANT TODDLER PROGRAM
MEDICAID EPSDT
Services for infants and toddlers (birth to three)
with or at risk of Developmental Delays and their
families SERVICE DEFINITIONS AND STANDARDS
EFFECTIVE JULY 1 2017
2018 NM FIT Annual Meeting 29
COMPREHENSIVE MULTIDISCIPLINARY EVALUATION
bull The Comprehensive Multidisciplinary Evaluation (CME) is designed to inform the eligibility determination process through a timely non-discriminatory comprehensive and interdisciplinary approach The evaluation is designed to determine the developmental status of the child and to determine eligibility for early intervention services The evaluation shall include parentcaregiver report information from the routines based interview process and must cover the following developmental areas
bull Cognitive bull Physical motor (including vision and hearing) bull Communication bull Social or emotional bull Adaptive behavior
2018 NM FIT Annual Meeting 30
5302018
11
SCOPE OF SERVICE
bull ldquohelliphelliphellipEvaluation personnel should have an early childhood development background Evaluation personnel should also be trained in FIT evaluation and eligibility procedures and the tool(s) that they are administering Evaluation and assessment tools shall be used in accordance with the manual and established protocols To ensure accurate evaluation results evaluations must be conducted in an environment where the child typically spends hisher day
bull If the team decides to first conduct a developmental screening for a child referred and in accordance with NMAC 7308 10 E the Ages and Stages Questionnaire (ASQ) shall be utilized
bull A review and summary of the childrsquos records related to current health status and prior medical history (look at 2017 presentation)
2018 NM FIT Annual Meeting 31
Less than one-monthbull Given the unique characteristics of young infants and the challenges of
determining their developmental levels
bull For infants under one month of age (adjusted) the IDA will not be used Instead one of the approved tools below shall be used together with informed clinical opinion Informed clinical opinion (httpwwwnectacorg~pdfspubsnnotes10pdf) is used by early intervention professionals in the evaluation and assessment process to make a recommendation as to initial and continuing eligibility for services under Part C and as a basis for planning services to meet child and family needs
bull Informed clinical opinion makes use of qualitative and quantitative information to assist in forming a determination regarding difficult-to-measure aspects of current developmental status and the potential need for early intervention
2018 NM FIT Annual Meeting 32
Approved tools for infants under 1 month of age
bull AIMS (Alberta Infant Motor Scale)
bull TIMP (Test of Infant Motor Performance)
bull Infant Toddler Sensory Profile
bull Motor Skills Acquisition Checklist
bull Newborn Individualized Developmental Care and Assessment Program (NIDCAP) - for use with newborns in the newborn intensive care setting only
bull Newborn Behavior Assessment Scale (NBAS)
bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 33
5302018
12
For infants over one month of age (adjusted) and under four months of age including adjusted age the IDA shall be used in conjunction with one of the following approved tools listed below)
bull All 5 developmental domains shall be assessed and addressed in the CME report including parentcaregiver information AIMS (Alberta Infant Motor Scale
bull TIMP (Test of Infant Motor Performance) bull Infant Toddler Sensory Profile bull Peabody Developmental Motor Scale (PDMS-2) bull Motor Skills Acquisition Checklist bull REEL-3 bull The Rossetti Infant Toddler Language Scale bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 34
AIMS-Alberta Infant Motor ScalesMotor Assessment of the Developing Infant
bull 0 ndash 18 months or walking decreased accuracy at 3 months of
age decreased precision after 9 months of age
bull ldquoobservedrdquo or ldquonot observedrdquo Items in the observed range create a motor window
bull Subscale scores are calculated by giving credit for observed items within the motor window plus giving credit for all of the less mature items before the motor window
bull The AIMS total score calculated by summing the scores
bull Score converted to a percentile and compared with age-equivalent peers from the normative sample
bull BUY THE BOOK
2018 NM FIT Annual Meeting 35
Psychometrics of AIMSbull Normed on 2202 infants between the ages of 1 week to 18
months living in province of Alberta between 1990 and 1992
bull Interrater reliability using two therapists who assessed 221 typically developing r values from a Pearson Product 096 to 099
bull Test-retest reliability was assessed by administering the AIMS twice (7 days between assessments) to 233 infants r values from a Pearson Product Moment Correlation Coefficient ranged from 086 to 099 when the same assessor scored the AIMS on both assessment days
2018 NM FIT Annual Meeting 36
5302018
13
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull Recommended cut-off scores for atypical development are the 10th
percentile at 4 months of age and the 5th percentile at 8 months of age (Darrah Piper amp Watt 1998)
bull Even typically developing infants do not acquire gross motor skills at a stable rate and could have a score that places them below the ldquocut-offrdquo score (Darrah et al 1998)
bull It is important to complete serial assessments and not simply identify a child as being delayed based on a one time screening
2018 NM FIT Annual Meeting 37
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull AIMS is thought to be appropriate for children between 0 -18 months it has been shown to have a ceiling effect with low precision of measurement after ~ 9 months of age or when children are able to lower themselves from standing with control Liao amp Campbell 2004
bull AIMS is much better at identifying infants with motor disabilities at 6 9 and 12 months than at 3 months of age Kolobe amp Bulanda 2006
bull The AIMS misclassified a high percentage of 3 month old infants later diagnosed with cerebral palsy (CP) where as it did much better at identifying children later diagnosed with CP when using the 5th percentile as a cut-off at 6 9 and 12 months of age Kolobe amp Bulanda 2006
bull These studies results should encourage clinicians to use caution when interpreting AIMS scores for infants 3 months of age as well as infants who are 9 months of age or older
2018 NM FIT Annual Meeting 38
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoslip-throughrdquo
bull How do they ldquolookrdquobull Curled ndash ldquohe is so cuddlyrdquo
bull Sacral sitting
bull Hands closedbull Cortical thumb
bull Ankle Clonusbull A few beats vs prolonged
2018 NM FIT Annual Meeting 39
5302018
14
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoone with the surfacerdquo
bull ldquohe never stops movingrdquobull Pull-to-sit hellip And into standing
bull On toes (ask about walkers and saucers and Johnny jump-ups)
bull Does he bear weight
bull Head shape and its effects on prone and supine
2018 NM FIT Annual Meeting 40
AIMS ldquoBehaviorsrdquo (cont)
bull Locking kneesbull ldquoCollapsingrdquo
bull Pull-to-sit moves straight into standing
bull Asymmetries
2018 NM FIT Annual Meeting 41
Symmetry
bull Always look for symmetry (in all evaluations) ndashbull ldquoI think that he is going to be left-handedrdquo
bull Use your reasoning skills
bull Asymmetry because of gravity taking head to one side
bull 2 months before baby can maintain midlinebull Does baby visually scan to both sides
2018 NM FIT Annual Meeting 42
5302018
15
2018 NM FIT Annual Meeting 43
Think of Dynamic Systemshellip
bull ASQs are prime example (and IDA)
bull What are we really looking atbull Some examples of systems approach
2018 NM FIT Annual Meeting 44
2018 NM FIT Annual Meeting 45
5302018
16
2018 NM FIT Annual Meeting 46
2018 NM FIT Annual Meeting 47
2018 NM FIT Annual Meeting 48
5302018
17
When is a ldquosit uprdquo a bad thing Van Haastert et al
Dev Med Child Neurol 2012 Jun54(6)538-43
ldquoActive head lifting from supine in early infancy an indicator for non-optimal cognitive outcome in late infancyrdquo
bull AHLS is associated with a less favorable cognitive outcome in the second year of life in preterm and in term-born infants than in comparison infants
2018 NM FIT Annual Meeting 49
RBI
bull Describe your babyrsquos ________
bull Observe babies eatingbull Dribblingbull Noisybull Falls ldquoasleeprdquobull Pushes awaybull Arching
bull All babies refluxbull Meds donrsquot stop refluxbull Effects of PPIs and H2 inhibitors
2018 NM FIT Annual Meeting 50
Transdisciplinary and Coaching
bull Effective Transdisciplinary is dependent on recognizing our own strengths and limitations ndash self-reflection
bull TTA is critical
2018 NM FIT Annual Meeting 51
5302018
18
Can we predict
bull httppartnersforkidsorgwp-contentuploads20171115236_Neo_Cerebral-Palsy-Early-ID_Practice-Tool_Q4-RMpdf
bull We do NOT diagnose
2018 NM FIT Annual Meeting 52
FIT Technical Assistance Document-Evaluation and Assessment p24ICO
2018 NM FIT Annual Meeting 53
And this is where we need to build the capacityhellip
bull ldquoDue to the varying nature and purpose of the scores of each of the above approved tools the scores themselves will not lead to eligibility but rather they will provide additional information for the team to consider in reaching a determination of the childs developmental status and eligibility
determinationrdquo
2018 NM FIT Annual Meeting 54
5302018
19
Informed Clinical Opinionbull An evaluation of the childrsquos level of functioning in each of the
following developmental areas
bull Cognitive development
bull Physical development including vision and hearing
bull Communication development
bull Social or emotional development and
bull Adaptive development
bull A review of the pertinent records related to the childrsquos current health status and medical history and can include areas such as but not limited to feeding sleeping motor behavior state regulation communication visual tracking and auditory responses
bull All 5 developmental domains and pertinent information shall be addressed in the CME report as well as parent report and shall include a statement and approval signature indicating that Informed Clinical Opinion was used
2018 NM FIT Annual Meeting 55
ICO example
bull httpswwwyoutubecomwatchv=ztd2-O0z9rM
2018 NM FIT Annual Meeting 56
Risk for Cerebral Palsy Early Detection
and Early InterventionPoster Presentation at 2018 Annual FIT Meeting
NMOTA Conference
September 2018
Amazing Newborn Conference
November 8-9 2018
2018 NM FIT Annual Meeting 57
5302018
20
Risk Factors for Cerebral Palsy(McIntrye et al 2011)
bull Prior to conception
bull History of still births miscarriage premature birth family history of CP low SES
bull Early Pregnancy
bull Infection multiple births genetic predisposition male gender birth defects
bull During Pregnancy
bull Maternal disease preeclampsia infection placental abnormalities precursors to premature birth
2018 NM FIT Annual Meeting 58
Cerebral Palsy (Novak et al 2017)
bull Most Common Physical Disorder in Children
bull 2 in High Income Countries ldquoCP describes a group of developmental disorders of movement and posture causing activity restrictions or disability that are attributed to disturbances occurring in the fetal or infant brain The motor impairment may be accompanied by a seizure disorder or by impairment of sensation cognition communication and or behavior ldquo
bull Originates prenatally or early post-natally
2018 NM FIT Annual Meeting 59
Three Groups Classification
1 Premature Infants (30-40 of all cases)
2 Term infants who develop neonatal encephalopathy shortly after birth (15-20)
3 Term infants without risk factors (40-50)
2018 NM FIT Annual Meeting 60
5302018
21
86 of parents suspected their child
had Cerebral Palsy before a clinical
diagnosis was made
2018 NM FIT Annual Meeting 61
RISK for CP
Identification Intervention
2018 NM FIT Annual Meeting 62
How do we build capacity
bull REFLECTIONbull Individual
bull What do I NOT knowbull As a program director
bull What questions keep coming up
2018 NM FIT Annual Meeting 63
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65

5302018
8
Formulas
bull VLBW infants should remain on nutrient enriched post-discharge formulas (transitional) until at least 9 months CGA
bull Standard caloric of neosureenfacare 22kcaloz
bull Preterm infants need to consume at least as much formula per day as their term-born peers
bull If growth exceeds 2 birth percentile lines or if weightlength exceeds 90 20caloz term infant formula may be considered earlier
bull Kleinman RE American Academy of Pediatrics Committee on Nutrition 2004bull LewishttpswwwpreemietoolkitcompdfsE_PhysicalExaminationAssessmentRecommendations-for-
Postdischargepdf
2018 NM FIT Annual Meeting 22
Other Formulasbull No role for the use of low-iron formulas (constipation)
bull Soy protein-based formula not recommended for preterm infants weighing lt 1800 grams
bull Lacking in sufficient calcium phosphorous and protein
bull The presence of phytates (soy) decreases bioavailability of mineral absorption in the gut
Kleinman RE American Academy of Pediatrics Committee on Nutrition 2004
2018 NM FIT Annual Meeting 23
Standard Immunizations
bull Preterm infants should receive full immunizations based upon their chronological age consistent with the schedule and dose recommended for normal full-term infants
bull Synagis for some with chronic lung disease
AAP Committee on Infectious Diseases Red Book 2012
2018 NM FIT Annual Meeting 24
5302018
9
Put Your Microscope Lenses Onhellip
bull httpwwwpediatricsemoryedudivisionsneonatologydpcnicubehhtml
2018 NM FIT Annual Meeting 25
2018 NM FIT Annual Meeting 26
Synactive Theory
Infantrsquos communication is via hisher behavior
Behavior represents the hierarchical integration of his subsystems
Focuses on the unique way that each baby processes the environment at any given time
Subsystems are
interdependent
hierarchical
mature sequentially (Peters 2001)
2018 NM FIT Annual Meeting 27
5302018
10
Dynamic Systems
bull You cannot just look at each ldquopartrdquo of the baby You must look at how each of the pieces work together and affect the whole child and the family
2018 NM FIT Annual Meeting 28
NEW MEXICO DOH DDSD - FISCAL YEAR 2018
STATE GENERAL FUND
Services for Individuals with
Developmental Disabilities
and
FAMILY INFANT TODDLER PROGRAM
MEDICAID EPSDT
Services for infants and toddlers (birth to three)
with or at risk of Developmental Delays and their
families SERVICE DEFINITIONS AND STANDARDS
EFFECTIVE JULY 1 2017
2018 NM FIT Annual Meeting 29
COMPREHENSIVE MULTIDISCIPLINARY EVALUATION
bull The Comprehensive Multidisciplinary Evaluation (CME) is designed to inform the eligibility determination process through a timely non-discriminatory comprehensive and interdisciplinary approach The evaluation is designed to determine the developmental status of the child and to determine eligibility for early intervention services The evaluation shall include parentcaregiver report information from the routines based interview process and must cover the following developmental areas
bull Cognitive bull Physical motor (including vision and hearing) bull Communication bull Social or emotional bull Adaptive behavior
2018 NM FIT Annual Meeting 30
5302018
11
SCOPE OF SERVICE
bull ldquohelliphelliphellipEvaluation personnel should have an early childhood development background Evaluation personnel should also be trained in FIT evaluation and eligibility procedures and the tool(s) that they are administering Evaluation and assessment tools shall be used in accordance with the manual and established protocols To ensure accurate evaluation results evaluations must be conducted in an environment where the child typically spends hisher day
bull If the team decides to first conduct a developmental screening for a child referred and in accordance with NMAC 7308 10 E the Ages and Stages Questionnaire (ASQ) shall be utilized
bull A review and summary of the childrsquos records related to current health status and prior medical history (look at 2017 presentation)
2018 NM FIT Annual Meeting 31
Less than one-monthbull Given the unique characteristics of young infants and the challenges of
determining their developmental levels
bull For infants under one month of age (adjusted) the IDA will not be used Instead one of the approved tools below shall be used together with informed clinical opinion Informed clinical opinion (httpwwwnectacorg~pdfspubsnnotes10pdf) is used by early intervention professionals in the evaluation and assessment process to make a recommendation as to initial and continuing eligibility for services under Part C and as a basis for planning services to meet child and family needs
bull Informed clinical opinion makes use of qualitative and quantitative information to assist in forming a determination regarding difficult-to-measure aspects of current developmental status and the potential need for early intervention
2018 NM FIT Annual Meeting 32
Approved tools for infants under 1 month of age
bull AIMS (Alberta Infant Motor Scale)
bull TIMP (Test of Infant Motor Performance)
bull Infant Toddler Sensory Profile
bull Motor Skills Acquisition Checklist
bull Newborn Individualized Developmental Care and Assessment Program (NIDCAP) - for use with newborns in the newborn intensive care setting only
bull Newborn Behavior Assessment Scale (NBAS)
bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 33
5302018
12
For infants over one month of age (adjusted) and under four months of age including adjusted age the IDA shall be used in conjunction with one of the following approved tools listed below)
bull All 5 developmental domains shall be assessed and addressed in the CME report including parentcaregiver information AIMS (Alberta Infant Motor Scale
bull TIMP (Test of Infant Motor Performance) bull Infant Toddler Sensory Profile bull Peabody Developmental Motor Scale (PDMS-2) bull Motor Skills Acquisition Checklist bull REEL-3 bull The Rossetti Infant Toddler Language Scale bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 34
AIMS-Alberta Infant Motor ScalesMotor Assessment of the Developing Infant
bull 0 ndash 18 months or walking decreased accuracy at 3 months of
age decreased precision after 9 months of age
bull ldquoobservedrdquo or ldquonot observedrdquo Items in the observed range create a motor window
bull Subscale scores are calculated by giving credit for observed items within the motor window plus giving credit for all of the less mature items before the motor window
bull The AIMS total score calculated by summing the scores
bull Score converted to a percentile and compared with age-equivalent peers from the normative sample
bull BUY THE BOOK
2018 NM FIT Annual Meeting 35
Psychometrics of AIMSbull Normed on 2202 infants between the ages of 1 week to 18
months living in province of Alberta between 1990 and 1992
bull Interrater reliability using two therapists who assessed 221 typically developing r values from a Pearson Product 096 to 099
bull Test-retest reliability was assessed by administering the AIMS twice (7 days between assessments) to 233 infants r values from a Pearson Product Moment Correlation Coefficient ranged from 086 to 099 when the same assessor scored the AIMS on both assessment days
2018 NM FIT Annual Meeting 36
5302018
13
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull Recommended cut-off scores for atypical development are the 10th
percentile at 4 months of age and the 5th percentile at 8 months of age (Darrah Piper amp Watt 1998)
bull Even typically developing infants do not acquire gross motor skills at a stable rate and could have a score that places them below the ldquocut-offrdquo score (Darrah et al 1998)
bull It is important to complete serial assessments and not simply identify a child as being delayed based on a one time screening
2018 NM FIT Annual Meeting 37
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull AIMS is thought to be appropriate for children between 0 -18 months it has been shown to have a ceiling effect with low precision of measurement after ~ 9 months of age or when children are able to lower themselves from standing with control Liao amp Campbell 2004
bull AIMS is much better at identifying infants with motor disabilities at 6 9 and 12 months than at 3 months of age Kolobe amp Bulanda 2006
bull The AIMS misclassified a high percentage of 3 month old infants later diagnosed with cerebral palsy (CP) where as it did much better at identifying children later diagnosed with CP when using the 5th percentile as a cut-off at 6 9 and 12 months of age Kolobe amp Bulanda 2006
bull These studies results should encourage clinicians to use caution when interpreting AIMS scores for infants 3 months of age as well as infants who are 9 months of age or older
2018 NM FIT Annual Meeting 38
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoslip-throughrdquo
bull How do they ldquolookrdquobull Curled ndash ldquohe is so cuddlyrdquo
bull Sacral sitting
bull Hands closedbull Cortical thumb
bull Ankle Clonusbull A few beats vs prolonged
2018 NM FIT Annual Meeting 39
5302018
14
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoone with the surfacerdquo
bull ldquohe never stops movingrdquobull Pull-to-sit hellip And into standing
bull On toes (ask about walkers and saucers and Johnny jump-ups)
bull Does he bear weight
bull Head shape and its effects on prone and supine
2018 NM FIT Annual Meeting 40
AIMS ldquoBehaviorsrdquo (cont)
bull Locking kneesbull ldquoCollapsingrdquo
bull Pull-to-sit moves straight into standing
bull Asymmetries
2018 NM FIT Annual Meeting 41
Symmetry
bull Always look for symmetry (in all evaluations) ndashbull ldquoI think that he is going to be left-handedrdquo
bull Use your reasoning skills
bull Asymmetry because of gravity taking head to one side
bull 2 months before baby can maintain midlinebull Does baby visually scan to both sides
2018 NM FIT Annual Meeting 42
5302018
15
2018 NM FIT Annual Meeting 43
Think of Dynamic Systemshellip
bull ASQs are prime example (and IDA)
bull What are we really looking atbull Some examples of systems approach
2018 NM FIT Annual Meeting 44
2018 NM FIT Annual Meeting 45
5302018
16
2018 NM FIT Annual Meeting 46
2018 NM FIT Annual Meeting 47
2018 NM FIT Annual Meeting 48
5302018
17
When is a ldquosit uprdquo a bad thing Van Haastert et al
Dev Med Child Neurol 2012 Jun54(6)538-43
ldquoActive head lifting from supine in early infancy an indicator for non-optimal cognitive outcome in late infancyrdquo
bull AHLS is associated with a less favorable cognitive outcome in the second year of life in preterm and in term-born infants than in comparison infants
2018 NM FIT Annual Meeting 49
RBI
bull Describe your babyrsquos ________
bull Observe babies eatingbull Dribblingbull Noisybull Falls ldquoasleeprdquobull Pushes awaybull Arching
bull All babies refluxbull Meds donrsquot stop refluxbull Effects of PPIs and H2 inhibitors
2018 NM FIT Annual Meeting 50
Transdisciplinary and Coaching
bull Effective Transdisciplinary is dependent on recognizing our own strengths and limitations ndash self-reflection
bull TTA is critical
2018 NM FIT Annual Meeting 51
5302018
18
Can we predict
bull httppartnersforkidsorgwp-contentuploads20171115236_Neo_Cerebral-Palsy-Early-ID_Practice-Tool_Q4-RMpdf
bull We do NOT diagnose
2018 NM FIT Annual Meeting 52
FIT Technical Assistance Document-Evaluation and Assessment p24ICO
2018 NM FIT Annual Meeting 53
And this is where we need to build the capacityhellip
bull ldquoDue to the varying nature and purpose of the scores of each of the above approved tools the scores themselves will not lead to eligibility but rather they will provide additional information for the team to consider in reaching a determination of the childs developmental status and eligibility
determinationrdquo
2018 NM FIT Annual Meeting 54
5302018
19
Informed Clinical Opinionbull An evaluation of the childrsquos level of functioning in each of the
following developmental areas
bull Cognitive development
bull Physical development including vision and hearing
bull Communication development
bull Social or emotional development and
bull Adaptive development
bull A review of the pertinent records related to the childrsquos current health status and medical history and can include areas such as but not limited to feeding sleeping motor behavior state regulation communication visual tracking and auditory responses
bull All 5 developmental domains and pertinent information shall be addressed in the CME report as well as parent report and shall include a statement and approval signature indicating that Informed Clinical Opinion was used
2018 NM FIT Annual Meeting 55
ICO example
bull httpswwwyoutubecomwatchv=ztd2-O0z9rM
2018 NM FIT Annual Meeting 56
Risk for Cerebral Palsy Early Detection
and Early InterventionPoster Presentation at 2018 Annual FIT Meeting
NMOTA Conference
September 2018
Amazing Newborn Conference
November 8-9 2018
2018 NM FIT Annual Meeting 57
5302018
20
Risk Factors for Cerebral Palsy(McIntrye et al 2011)
bull Prior to conception
bull History of still births miscarriage premature birth family history of CP low SES
bull Early Pregnancy
bull Infection multiple births genetic predisposition male gender birth defects
bull During Pregnancy
bull Maternal disease preeclampsia infection placental abnormalities precursors to premature birth
2018 NM FIT Annual Meeting 58
Cerebral Palsy (Novak et al 2017)
bull Most Common Physical Disorder in Children
bull 2 in High Income Countries ldquoCP describes a group of developmental disorders of movement and posture causing activity restrictions or disability that are attributed to disturbances occurring in the fetal or infant brain The motor impairment may be accompanied by a seizure disorder or by impairment of sensation cognition communication and or behavior ldquo
bull Originates prenatally or early post-natally
2018 NM FIT Annual Meeting 59
Three Groups Classification
1 Premature Infants (30-40 of all cases)
2 Term infants who develop neonatal encephalopathy shortly after birth (15-20)
3 Term infants without risk factors (40-50)
2018 NM FIT Annual Meeting 60
5302018
21
86 of parents suspected their child
had Cerebral Palsy before a clinical
diagnosis was made
2018 NM FIT Annual Meeting 61
RISK for CP
Identification Intervention
2018 NM FIT Annual Meeting 62
How do we build capacity
bull REFLECTIONbull Individual
bull What do I NOT knowbull As a program director
bull What questions keep coming up
2018 NM FIT Annual Meeting 63
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65
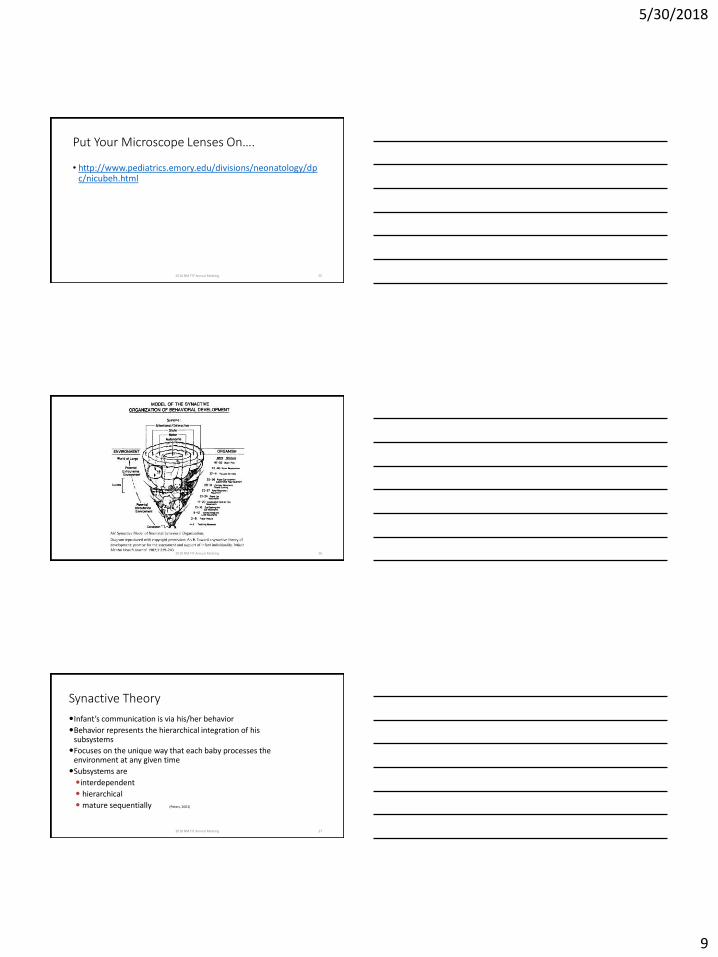
5302018
9
Put Your Microscope Lenses Onhellip
bull httpwwwpediatricsemoryedudivisionsneonatologydpcnicubehhtml
2018 NM FIT Annual Meeting 25
2018 NM FIT Annual Meeting 26
Synactive Theory
Infantrsquos communication is via hisher behavior
Behavior represents the hierarchical integration of his subsystems
Focuses on the unique way that each baby processes the environment at any given time
Subsystems are
interdependent
hierarchical
mature sequentially (Peters 2001)
2018 NM FIT Annual Meeting 27
5302018
10
Dynamic Systems
bull You cannot just look at each ldquopartrdquo of the baby You must look at how each of the pieces work together and affect the whole child and the family
2018 NM FIT Annual Meeting 28
NEW MEXICO DOH DDSD - FISCAL YEAR 2018
STATE GENERAL FUND
Services for Individuals with
Developmental Disabilities
and
FAMILY INFANT TODDLER PROGRAM
MEDICAID EPSDT
Services for infants and toddlers (birth to three)
with or at risk of Developmental Delays and their
families SERVICE DEFINITIONS AND STANDARDS
EFFECTIVE JULY 1 2017
2018 NM FIT Annual Meeting 29
COMPREHENSIVE MULTIDISCIPLINARY EVALUATION
bull The Comprehensive Multidisciplinary Evaluation (CME) is designed to inform the eligibility determination process through a timely non-discriminatory comprehensive and interdisciplinary approach The evaluation is designed to determine the developmental status of the child and to determine eligibility for early intervention services The evaluation shall include parentcaregiver report information from the routines based interview process and must cover the following developmental areas
bull Cognitive bull Physical motor (including vision and hearing) bull Communication bull Social or emotional bull Adaptive behavior
2018 NM FIT Annual Meeting 30
5302018
11
SCOPE OF SERVICE
bull ldquohelliphelliphellipEvaluation personnel should have an early childhood development background Evaluation personnel should also be trained in FIT evaluation and eligibility procedures and the tool(s) that they are administering Evaluation and assessment tools shall be used in accordance with the manual and established protocols To ensure accurate evaluation results evaluations must be conducted in an environment where the child typically spends hisher day
bull If the team decides to first conduct a developmental screening for a child referred and in accordance with NMAC 7308 10 E the Ages and Stages Questionnaire (ASQ) shall be utilized
bull A review and summary of the childrsquos records related to current health status and prior medical history (look at 2017 presentation)
2018 NM FIT Annual Meeting 31
Less than one-monthbull Given the unique characteristics of young infants and the challenges of
determining their developmental levels
bull For infants under one month of age (adjusted) the IDA will not be used Instead one of the approved tools below shall be used together with informed clinical opinion Informed clinical opinion (httpwwwnectacorg~pdfspubsnnotes10pdf) is used by early intervention professionals in the evaluation and assessment process to make a recommendation as to initial and continuing eligibility for services under Part C and as a basis for planning services to meet child and family needs
bull Informed clinical opinion makes use of qualitative and quantitative information to assist in forming a determination regarding difficult-to-measure aspects of current developmental status and the potential need for early intervention
2018 NM FIT Annual Meeting 32
Approved tools for infants under 1 month of age
bull AIMS (Alberta Infant Motor Scale)
bull TIMP (Test of Infant Motor Performance)
bull Infant Toddler Sensory Profile
bull Motor Skills Acquisition Checklist
bull Newborn Individualized Developmental Care and Assessment Program (NIDCAP) - for use with newborns in the newborn intensive care setting only
bull Newborn Behavior Assessment Scale (NBAS)
bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 33
5302018
12
For infants over one month of age (adjusted) and under four months of age including adjusted age the IDA shall be used in conjunction with one of the following approved tools listed below)
bull All 5 developmental domains shall be assessed and addressed in the CME report including parentcaregiver information AIMS (Alberta Infant Motor Scale
bull TIMP (Test of Infant Motor Performance) bull Infant Toddler Sensory Profile bull Peabody Developmental Motor Scale (PDMS-2) bull Motor Skills Acquisition Checklist bull REEL-3 bull The Rossetti Infant Toddler Language Scale bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 34
AIMS-Alberta Infant Motor ScalesMotor Assessment of the Developing Infant
bull 0 ndash 18 months or walking decreased accuracy at 3 months of
age decreased precision after 9 months of age
bull ldquoobservedrdquo or ldquonot observedrdquo Items in the observed range create a motor window
bull Subscale scores are calculated by giving credit for observed items within the motor window plus giving credit for all of the less mature items before the motor window
bull The AIMS total score calculated by summing the scores
bull Score converted to a percentile and compared with age-equivalent peers from the normative sample
bull BUY THE BOOK
2018 NM FIT Annual Meeting 35
Psychometrics of AIMSbull Normed on 2202 infants between the ages of 1 week to 18
months living in province of Alberta between 1990 and 1992
bull Interrater reliability using two therapists who assessed 221 typically developing r values from a Pearson Product 096 to 099
bull Test-retest reliability was assessed by administering the AIMS twice (7 days between assessments) to 233 infants r values from a Pearson Product Moment Correlation Coefficient ranged from 086 to 099 when the same assessor scored the AIMS on both assessment days
2018 NM FIT Annual Meeting 36
5302018
13
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull Recommended cut-off scores for atypical development are the 10th
percentile at 4 months of age and the 5th percentile at 8 months of age (Darrah Piper amp Watt 1998)
bull Even typically developing infants do not acquire gross motor skills at a stable rate and could have a score that places them below the ldquocut-offrdquo score (Darrah et al 1998)
bull It is important to complete serial assessments and not simply identify a child as being delayed based on a one time screening
2018 NM FIT Annual Meeting 37
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull AIMS is thought to be appropriate for children between 0 -18 months it has been shown to have a ceiling effect with low precision of measurement after ~ 9 months of age or when children are able to lower themselves from standing with control Liao amp Campbell 2004
bull AIMS is much better at identifying infants with motor disabilities at 6 9 and 12 months than at 3 months of age Kolobe amp Bulanda 2006
bull The AIMS misclassified a high percentage of 3 month old infants later diagnosed with cerebral palsy (CP) where as it did much better at identifying children later diagnosed with CP when using the 5th percentile as a cut-off at 6 9 and 12 months of age Kolobe amp Bulanda 2006
bull These studies results should encourage clinicians to use caution when interpreting AIMS scores for infants 3 months of age as well as infants who are 9 months of age or older
2018 NM FIT Annual Meeting 38
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoslip-throughrdquo
bull How do they ldquolookrdquobull Curled ndash ldquohe is so cuddlyrdquo
bull Sacral sitting
bull Hands closedbull Cortical thumb
bull Ankle Clonusbull A few beats vs prolonged
2018 NM FIT Annual Meeting 39
5302018
14
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoone with the surfacerdquo
bull ldquohe never stops movingrdquobull Pull-to-sit hellip And into standing
bull On toes (ask about walkers and saucers and Johnny jump-ups)
bull Does he bear weight
bull Head shape and its effects on prone and supine
2018 NM FIT Annual Meeting 40
AIMS ldquoBehaviorsrdquo (cont)
bull Locking kneesbull ldquoCollapsingrdquo
bull Pull-to-sit moves straight into standing
bull Asymmetries
2018 NM FIT Annual Meeting 41
Symmetry
bull Always look for symmetry (in all evaluations) ndashbull ldquoI think that he is going to be left-handedrdquo
bull Use your reasoning skills
bull Asymmetry because of gravity taking head to one side
bull 2 months before baby can maintain midlinebull Does baby visually scan to both sides
2018 NM FIT Annual Meeting 42
5302018
15
2018 NM FIT Annual Meeting 43
Think of Dynamic Systemshellip
bull ASQs are prime example (and IDA)
bull What are we really looking atbull Some examples of systems approach
2018 NM FIT Annual Meeting 44
2018 NM FIT Annual Meeting 45
5302018
16
2018 NM FIT Annual Meeting 46
2018 NM FIT Annual Meeting 47
2018 NM FIT Annual Meeting 48
5302018
17
When is a ldquosit uprdquo a bad thing Van Haastert et al
Dev Med Child Neurol 2012 Jun54(6)538-43
ldquoActive head lifting from supine in early infancy an indicator for non-optimal cognitive outcome in late infancyrdquo
bull AHLS is associated with a less favorable cognitive outcome in the second year of life in preterm and in term-born infants than in comparison infants
2018 NM FIT Annual Meeting 49
RBI
bull Describe your babyrsquos ________
bull Observe babies eatingbull Dribblingbull Noisybull Falls ldquoasleeprdquobull Pushes awaybull Arching
bull All babies refluxbull Meds donrsquot stop refluxbull Effects of PPIs and H2 inhibitors
2018 NM FIT Annual Meeting 50
Transdisciplinary and Coaching
bull Effective Transdisciplinary is dependent on recognizing our own strengths and limitations ndash self-reflection
bull TTA is critical
2018 NM FIT Annual Meeting 51
5302018
18
Can we predict
bull httppartnersforkidsorgwp-contentuploads20171115236_Neo_Cerebral-Palsy-Early-ID_Practice-Tool_Q4-RMpdf
bull We do NOT diagnose
2018 NM FIT Annual Meeting 52
FIT Technical Assistance Document-Evaluation and Assessment p24ICO
2018 NM FIT Annual Meeting 53
And this is where we need to build the capacityhellip
bull ldquoDue to the varying nature and purpose of the scores of each of the above approved tools the scores themselves will not lead to eligibility but rather they will provide additional information for the team to consider in reaching a determination of the childs developmental status and eligibility
determinationrdquo
2018 NM FIT Annual Meeting 54
5302018
19
Informed Clinical Opinionbull An evaluation of the childrsquos level of functioning in each of the
following developmental areas
bull Cognitive development
bull Physical development including vision and hearing
bull Communication development
bull Social or emotional development and
bull Adaptive development
bull A review of the pertinent records related to the childrsquos current health status and medical history and can include areas such as but not limited to feeding sleeping motor behavior state regulation communication visual tracking and auditory responses
bull All 5 developmental domains and pertinent information shall be addressed in the CME report as well as parent report and shall include a statement and approval signature indicating that Informed Clinical Opinion was used
2018 NM FIT Annual Meeting 55
ICO example
bull httpswwwyoutubecomwatchv=ztd2-O0z9rM
2018 NM FIT Annual Meeting 56
Risk for Cerebral Palsy Early Detection
and Early InterventionPoster Presentation at 2018 Annual FIT Meeting
NMOTA Conference
September 2018
Amazing Newborn Conference
November 8-9 2018
2018 NM FIT Annual Meeting 57
5302018
20
Risk Factors for Cerebral Palsy(McIntrye et al 2011)
bull Prior to conception
bull History of still births miscarriage premature birth family history of CP low SES
bull Early Pregnancy
bull Infection multiple births genetic predisposition male gender birth defects
bull During Pregnancy
bull Maternal disease preeclampsia infection placental abnormalities precursors to premature birth
2018 NM FIT Annual Meeting 58
Cerebral Palsy (Novak et al 2017)
bull Most Common Physical Disorder in Children
bull 2 in High Income Countries ldquoCP describes a group of developmental disorders of movement and posture causing activity restrictions or disability that are attributed to disturbances occurring in the fetal or infant brain The motor impairment may be accompanied by a seizure disorder or by impairment of sensation cognition communication and or behavior ldquo
bull Originates prenatally or early post-natally
2018 NM FIT Annual Meeting 59
Three Groups Classification
1 Premature Infants (30-40 of all cases)
2 Term infants who develop neonatal encephalopathy shortly after birth (15-20)
3 Term infants without risk factors (40-50)
2018 NM FIT Annual Meeting 60
5302018
21
86 of parents suspected their child
had Cerebral Palsy before a clinical
diagnosis was made
2018 NM FIT Annual Meeting 61
RISK for CP
Identification Intervention
2018 NM FIT Annual Meeting 62
How do we build capacity
bull REFLECTIONbull Individual
bull What do I NOT knowbull As a program director
bull What questions keep coming up
2018 NM FIT Annual Meeting 63
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65
5302018
10
Dynamic Systems
bull You cannot just look at each ldquopartrdquo of the baby You must look at how each of the pieces work together and affect the whole child and the family
2018 NM FIT Annual Meeting 28
NEW MEXICO DOH DDSD - FISCAL YEAR 2018
STATE GENERAL FUND
Services for Individuals with
Developmental Disabilities
and
FAMILY INFANT TODDLER PROGRAM
MEDICAID EPSDT
Services for infants and toddlers (birth to three)
with or at risk of Developmental Delays and their
families SERVICE DEFINITIONS AND STANDARDS
EFFECTIVE JULY 1 2017
2018 NM FIT Annual Meeting 29
COMPREHENSIVE MULTIDISCIPLINARY EVALUATION
bull The Comprehensive Multidisciplinary Evaluation (CME) is designed to inform the eligibility determination process through a timely non-discriminatory comprehensive and interdisciplinary approach The evaluation is designed to determine the developmental status of the child and to determine eligibility for early intervention services The evaluation shall include parentcaregiver report information from the routines based interview process and must cover the following developmental areas
bull Cognitive bull Physical motor (including vision and hearing) bull Communication bull Social or emotional bull Adaptive behavior
2018 NM FIT Annual Meeting 30
5302018
11
SCOPE OF SERVICE
bull ldquohelliphelliphellipEvaluation personnel should have an early childhood development background Evaluation personnel should also be trained in FIT evaluation and eligibility procedures and the tool(s) that they are administering Evaluation and assessment tools shall be used in accordance with the manual and established protocols To ensure accurate evaluation results evaluations must be conducted in an environment where the child typically spends hisher day
bull If the team decides to first conduct a developmental screening for a child referred and in accordance with NMAC 7308 10 E the Ages and Stages Questionnaire (ASQ) shall be utilized
bull A review and summary of the childrsquos records related to current health status and prior medical history (look at 2017 presentation)
2018 NM FIT Annual Meeting 31
Less than one-monthbull Given the unique characteristics of young infants and the challenges of
determining their developmental levels
bull For infants under one month of age (adjusted) the IDA will not be used Instead one of the approved tools below shall be used together with informed clinical opinion Informed clinical opinion (httpwwwnectacorg~pdfspubsnnotes10pdf) is used by early intervention professionals in the evaluation and assessment process to make a recommendation as to initial and continuing eligibility for services under Part C and as a basis for planning services to meet child and family needs
bull Informed clinical opinion makes use of qualitative and quantitative information to assist in forming a determination regarding difficult-to-measure aspects of current developmental status and the potential need for early intervention
2018 NM FIT Annual Meeting 32
Approved tools for infants under 1 month of age
bull AIMS (Alberta Infant Motor Scale)
bull TIMP (Test of Infant Motor Performance)
bull Infant Toddler Sensory Profile
bull Motor Skills Acquisition Checklist
bull Newborn Individualized Developmental Care and Assessment Program (NIDCAP) - for use with newborns in the newborn intensive care setting only
bull Newborn Behavior Assessment Scale (NBAS)
bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 33
5302018
12
For infants over one month of age (adjusted) and under four months of age including adjusted age the IDA shall be used in conjunction with one of the following approved tools listed below)
bull All 5 developmental domains shall be assessed and addressed in the CME report including parentcaregiver information AIMS (Alberta Infant Motor Scale
bull TIMP (Test of Infant Motor Performance) bull Infant Toddler Sensory Profile bull Peabody Developmental Motor Scale (PDMS-2) bull Motor Skills Acquisition Checklist bull REEL-3 bull The Rossetti Infant Toddler Language Scale bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 34
AIMS-Alberta Infant Motor ScalesMotor Assessment of the Developing Infant
bull 0 ndash 18 months or walking decreased accuracy at 3 months of
age decreased precision after 9 months of age
bull ldquoobservedrdquo or ldquonot observedrdquo Items in the observed range create a motor window
bull Subscale scores are calculated by giving credit for observed items within the motor window plus giving credit for all of the less mature items before the motor window
bull The AIMS total score calculated by summing the scores
bull Score converted to a percentile and compared with age-equivalent peers from the normative sample
bull BUY THE BOOK
2018 NM FIT Annual Meeting 35
Psychometrics of AIMSbull Normed on 2202 infants between the ages of 1 week to 18
months living in province of Alberta between 1990 and 1992
bull Interrater reliability using two therapists who assessed 221 typically developing r values from a Pearson Product 096 to 099
bull Test-retest reliability was assessed by administering the AIMS twice (7 days between assessments) to 233 infants r values from a Pearson Product Moment Correlation Coefficient ranged from 086 to 099 when the same assessor scored the AIMS on both assessment days
2018 NM FIT Annual Meeting 36
5302018
13
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull Recommended cut-off scores for atypical development are the 10th
percentile at 4 months of age and the 5th percentile at 8 months of age (Darrah Piper amp Watt 1998)
bull Even typically developing infants do not acquire gross motor skills at a stable rate and could have a score that places them below the ldquocut-offrdquo score (Darrah et al 1998)
bull It is important to complete serial assessments and not simply identify a child as being delayed based on a one time screening
2018 NM FIT Annual Meeting 37
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull AIMS is thought to be appropriate for children between 0 -18 months it has been shown to have a ceiling effect with low precision of measurement after ~ 9 months of age or when children are able to lower themselves from standing with control Liao amp Campbell 2004
bull AIMS is much better at identifying infants with motor disabilities at 6 9 and 12 months than at 3 months of age Kolobe amp Bulanda 2006
bull The AIMS misclassified a high percentage of 3 month old infants later diagnosed with cerebral palsy (CP) where as it did much better at identifying children later diagnosed with CP when using the 5th percentile as a cut-off at 6 9 and 12 months of age Kolobe amp Bulanda 2006
bull These studies results should encourage clinicians to use caution when interpreting AIMS scores for infants 3 months of age as well as infants who are 9 months of age or older
2018 NM FIT Annual Meeting 38
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoslip-throughrdquo
bull How do they ldquolookrdquobull Curled ndash ldquohe is so cuddlyrdquo
bull Sacral sitting
bull Hands closedbull Cortical thumb
bull Ankle Clonusbull A few beats vs prolonged
2018 NM FIT Annual Meeting 39
5302018
14
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoone with the surfacerdquo
bull ldquohe never stops movingrdquobull Pull-to-sit hellip And into standing
bull On toes (ask about walkers and saucers and Johnny jump-ups)
bull Does he bear weight
bull Head shape and its effects on prone and supine
2018 NM FIT Annual Meeting 40
AIMS ldquoBehaviorsrdquo (cont)
bull Locking kneesbull ldquoCollapsingrdquo
bull Pull-to-sit moves straight into standing
bull Asymmetries
2018 NM FIT Annual Meeting 41
Symmetry
bull Always look for symmetry (in all evaluations) ndashbull ldquoI think that he is going to be left-handedrdquo
bull Use your reasoning skills
bull Asymmetry because of gravity taking head to one side
bull 2 months before baby can maintain midlinebull Does baby visually scan to both sides
2018 NM FIT Annual Meeting 42
5302018
15
2018 NM FIT Annual Meeting 43
Think of Dynamic Systemshellip
bull ASQs are prime example (and IDA)
bull What are we really looking atbull Some examples of systems approach
2018 NM FIT Annual Meeting 44
2018 NM FIT Annual Meeting 45
5302018
16
2018 NM FIT Annual Meeting 46
2018 NM FIT Annual Meeting 47
2018 NM FIT Annual Meeting 48
5302018
17
When is a ldquosit uprdquo a bad thing Van Haastert et al
Dev Med Child Neurol 2012 Jun54(6)538-43
ldquoActive head lifting from supine in early infancy an indicator for non-optimal cognitive outcome in late infancyrdquo
bull AHLS is associated with a less favorable cognitive outcome in the second year of life in preterm and in term-born infants than in comparison infants
2018 NM FIT Annual Meeting 49
RBI
bull Describe your babyrsquos ________
bull Observe babies eatingbull Dribblingbull Noisybull Falls ldquoasleeprdquobull Pushes awaybull Arching
bull All babies refluxbull Meds donrsquot stop refluxbull Effects of PPIs and H2 inhibitors
2018 NM FIT Annual Meeting 50
Transdisciplinary and Coaching
bull Effective Transdisciplinary is dependent on recognizing our own strengths and limitations ndash self-reflection
bull TTA is critical
2018 NM FIT Annual Meeting 51
5302018
18
Can we predict
bull httppartnersforkidsorgwp-contentuploads20171115236_Neo_Cerebral-Palsy-Early-ID_Practice-Tool_Q4-RMpdf
bull We do NOT diagnose
2018 NM FIT Annual Meeting 52
FIT Technical Assistance Document-Evaluation and Assessment p24ICO
2018 NM FIT Annual Meeting 53
And this is where we need to build the capacityhellip
bull ldquoDue to the varying nature and purpose of the scores of each of the above approved tools the scores themselves will not lead to eligibility but rather they will provide additional information for the team to consider in reaching a determination of the childs developmental status and eligibility
determinationrdquo
2018 NM FIT Annual Meeting 54
5302018
19
Informed Clinical Opinionbull An evaluation of the childrsquos level of functioning in each of the
following developmental areas
bull Cognitive development
bull Physical development including vision and hearing
bull Communication development
bull Social or emotional development and
bull Adaptive development
bull A review of the pertinent records related to the childrsquos current health status and medical history and can include areas such as but not limited to feeding sleeping motor behavior state regulation communication visual tracking and auditory responses
bull All 5 developmental domains and pertinent information shall be addressed in the CME report as well as parent report and shall include a statement and approval signature indicating that Informed Clinical Opinion was used
2018 NM FIT Annual Meeting 55
ICO example
bull httpswwwyoutubecomwatchv=ztd2-O0z9rM
2018 NM FIT Annual Meeting 56
Risk for Cerebral Palsy Early Detection
and Early InterventionPoster Presentation at 2018 Annual FIT Meeting
NMOTA Conference
September 2018
Amazing Newborn Conference
November 8-9 2018
2018 NM FIT Annual Meeting 57
5302018
20
Risk Factors for Cerebral Palsy(McIntrye et al 2011)
bull Prior to conception
bull History of still births miscarriage premature birth family history of CP low SES
bull Early Pregnancy
bull Infection multiple births genetic predisposition male gender birth defects
bull During Pregnancy
bull Maternal disease preeclampsia infection placental abnormalities precursors to premature birth
2018 NM FIT Annual Meeting 58
Cerebral Palsy (Novak et al 2017)
bull Most Common Physical Disorder in Children
bull 2 in High Income Countries ldquoCP describes a group of developmental disorders of movement and posture causing activity restrictions or disability that are attributed to disturbances occurring in the fetal or infant brain The motor impairment may be accompanied by a seizure disorder or by impairment of sensation cognition communication and or behavior ldquo
bull Originates prenatally or early post-natally
2018 NM FIT Annual Meeting 59
Three Groups Classification
1 Premature Infants (30-40 of all cases)
2 Term infants who develop neonatal encephalopathy shortly after birth (15-20)
3 Term infants without risk factors (40-50)
2018 NM FIT Annual Meeting 60
5302018
21
86 of parents suspected their child
had Cerebral Palsy before a clinical
diagnosis was made
2018 NM FIT Annual Meeting 61
RISK for CP
Identification Intervention
2018 NM FIT Annual Meeting 62
How do we build capacity
bull REFLECTIONbull Individual
bull What do I NOT knowbull As a program director
bull What questions keep coming up
2018 NM FIT Annual Meeting 63
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65
5302018
11
SCOPE OF SERVICE
bull ldquohelliphelliphellipEvaluation personnel should have an early childhood development background Evaluation personnel should also be trained in FIT evaluation and eligibility procedures and the tool(s) that they are administering Evaluation and assessment tools shall be used in accordance with the manual and established protocols To ensure accurate evaluation results evaluations must be conducted in an environment where the child typically spends hisher day
bull If the team decides to first conduct a developmental screening for a child referred and in accordance with NMAC 7308 10 E the Ages and Stages Questionnaire (ASQ) shall be utilized
bull A review and summary of the childrsquos records related to current health status and prior medical history (look at 2017 presentation)
2018 NM FIT Annual Meeting 31
Less than one-monthbull Given the unique characteristics of young infants and the challenges of
determining their developmental levels
bull For infants under one month of age (adjusted) the IDA will not be used Instead one of the approved tools below shall be used together with informed clinical opinion Informed clinical opinion (httpwwwnectacorg~pdfspubsnnotes10pdf) is used by early intervention professionals in the evaluation and assessment process to make a recommendation as to initial and continuing eligibility for services under Part C and as a basis for planning services to meet child and family needs
bull Informed clinical opinion makes use of qualitative and quantitative information to assist in forming a determination regarding difficult-to-measure aspects of current developmental status and the potential need for early intervention
2018 NM FIT Annual Meeting 32
Approved tools for infants under 1 month of age
bull AIMS (Alberta Infant Motor Scale)
bull TIMP (Test of Infant Motor Performance)
bull Infant Toddler Sensory Profile
bull Motor Skills Acquisition Checklist
bull Newborn Individualized Developmental Care and Assessment Program (NIDCAP) - for use with newborns in the newborn intensive care setting only
bull Newborn Behavior Assessment Scale (NBAS)
bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 33
5302018
12
For infants over one month of age (adjusted) and under four months of age including adjusted age the IDA shall be used in conjunction with one of the following approved tools listed below)
bull All 5 developmental domains shall be assessed and addressed in the CME report including parentcaregiver information AIMS (Alberta Infant Motor Scale
bull TIMP (Test of Infant Motor Performance) bull Infant Toddler Sensory Profile bull Peabody Developmental Motor Scale (PDMS-2) bull Motor Skills Acquisition Checklist bull REEL-3 bull The Rossetti Infant Toddler Language Scale bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 34
AIMS-Alberta Infant Motor ScalesMotor Assessment of the Developing Infant
bull 0 ndash 18 months or walking decreased accuracy at 3 months of
age decreased precision after 9 months of age
bull ldquoobservedrdquo or ldquonot observedrdquo Items in the observed range create a motor window
bull Subscale scores are calculated by giving credit for observed items within the motor window plus giving credit for all of the less mature items before the motor window
bull The AIMS total score calculated by summing the scores
bull Score converted to a percentile and compared with age-equivalent peers from the normative sample
bull BUY THE BOOK
2018 NM FIT Annual Meeting 35
Psychometrics of AIMSbull Normed on 2202 infants between the ages of 1 week to 18
months living in province of Alberta between 1990 and 1992
bull Interrater reliability using two therapists who assessed 221 typically developing r values from a Pearson Product 096 to 099
bull Test-retest reliability was assessed by administering the AIMS twice (7 days between assessments) to 233 infants r values from a Pearson Product Moment Correlation Coefficient ranged from 086 to 099 when the same assessor scored the AIMS on both assessment days
2018 NM FIT Annual Meeting 36
5302018
13
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull Recommended cut-off scores for atypical development are the 10th
percentile at 4 months of age and the 5th percentile at 8 months of age (Darrah Piper amp Watt 1998)
bull Even typically developing infants do not acquire gross motor skills at a stable rate and could have a score that places them below the ldquocut-offrdquo score (Darrah et al 1998)
bull It is important to complete serial assessments and not simply identify a child as being delayed based on a one time screening
2018 NM FIT Annual Meeting 37
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull AIMS is thought to be appropriate for children between 0 -18 months it has been shown to have a ceiling effect with low precision of measurement after ~ 9 months of age or when children are able to lower themselves from standing with control Liao amp Campbell 2004
bull AIMS is much better at identifying infants with motor disabilities at 6 9 and 12 months than at 3 months of age Kolobe amp Bulanda 2006
bull The AIMS misclassified a high percentage of 3 month old infants later diagnosed with cerebral palsy (CP) where as it did much better at identifying children later diagnosed with CP when using the 5th percentile as a cut-off at 6 9 and 12 months of age Kolobe amp Bulanda 2006
bull These studies results should encourage clinicians to use caution when interpreting AIMS scores for infants 3 months of age as well as infants who are 9 months of age or older
2018 NM FIT Annual Meeting 38
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoslip-throughrdquo
bull How do they ldquolookrdquobull Curled ndash ldquohe is so cuddlyrdquo
bull Sacral sitting
bull Hands closedbull Cortical thumb
bull Ankle Clonusbull A few beats vs prolonged
2018 NM FIT Annual Meeting 39
5302018
14
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoone with the surfacerdquo
bull ldquohe never stops movingrdquobull Pull-to-sit hellip And into standing
bull On toes (ask about walkers and saucers and Johnny jump-ups)
bull Does he bear weight
bull Head shape and its effects on prone and supine
2018 NM FIT Annual Meeting 40
AIMS ldquoBehaviorsrdquo (cont)
bull Locking kneesbull ldquoCollapsingrdquo
bull Pull-to-sit moves straight into standing
bull Asymmetries
2018 NM FIT Annual Meeting 41
Symmetry
bull Always look for symmetry (in all evaluations) ndashbull ldquoI think that he is going to be left-handedrdquo
bull Use your reasoning skills
bull Asymmetry because of gravity taking head to one side
bull 2 months before baby can maintain midlinebull Does baby visually scan to both sides
2018 NM FIT Annual Meeting 42
5302018
15
2018 NM FIT Annual Meeting 43
Think of Dynamic Systemshellip
bull ASQs are prime example (and IDA)
bull What are we really looking atbull Some examples of systems approach
2018 NM FIT Annual Meeting 44
2018 NM FIT Annual Meeting 45
5302018
16
2018 NM FIT Annual Meeting 46
2018 NM FIT Annual Meeting 47
2018 NM FIT Annual Meeting 48
5302018
17
When is a ldquosit uprdquo a bad thing Van Haastert et al
Dev Med Child Neurol 2012 Jun54(6)538-43
ldquoActive head lifting from supine in early infancy an indicator for non-optimal cognitive outcome in late infancyrdquo
bull AHLS is associated with a less favorable cognitive outcome in the second year of life in preterm and in term-born infants than in comparison infants
2018 NM FIT Annual Meeting 49
RBI
bull Describe your babyrsquos ________
bull Observe babies eatingbull Dribblingbull Noisybull Falls ldquoasleeprdquobull Pushes awaybull Arching
bull All babies refluxbull Meds donrsquot stop refluxbull Effects of PPIs and H2 inhibitors
2018 NM FIT Annual Meeting 50
Transdisciplinary and Coaching
bull Effective Transdisciplinary is dependent on recognizing our own strengths and limitations ndash self-reflection
bull TTA is critical
2018 NM FIT Annual Meeting 51
5302018
18
Can we predict
bull httppartnersforkidsorgwp-contentuploads20171115236_Neo_Cerebral-Palsy-Early-ID_Practice-Tool_Q4-RMpdf
bull We do NOT diagnose
2018 NM FIT Annual Meeting 52
FIT Technical Assistance Document-Evaluation and Assessment p24ICO
2018 NM FIT Annual Meeting 53
And this is where we need to build the capacityhellip
bull ldquoDue to the varying nature and purpose of the scores of each of the above approved tools the scores themselves will not lead to eligibility but rather they will provide additional information for the team to consider in reaching a determination of the childs developmental status and eligibility
determinationrdquo
2018 NM FIT Annual Meeting 54
5302018
19
Informed Clinical Opinionbull An evaluation of the childrsquos level of functioning in each of the
following developmental areas
bull Cognitive development
bull Physical development including vision and hearing
bull Communication development
bull Social or emotional development and
bull Adaptive development
bull A review of the pertinent records related to the childrsquos current health status and medical history and can include areas such as but not limited to feeding sleeping motor behavior state regulation communication visual tracking and auditory responses
bull All 5 developmental domains and pertinent information shall be addressed in the CME report as well as parent report and shall include a statement and approval signature indicating that Informed Clinical Opinion was used
2018 NM FIT Annual Meeting 55
ICO example
bull httpswwwyoutubecomwatchv=ztd2-O0z9rM
2018 NM FIT Annual Meeting 56
Risk for Cerebral Palsy Early Detection
and Early InterventionPoster Presentation at 2018 Annual FIT Meeting
NMOTA Conference
September 2018
Amazing Newborn Conference
November 8-9 2018
2018 NM FIT Annual Meeting 57
5302018
20
Risk Factors for Cerebral Palsy(McIntrye et al 2011)
bull Prior to conception
bull History of still births miscarriage premature birth family history of CP low SES
bull Early Pregnancy
bull Infection multiple births genetic predisposition male gender birth defects
bull During Pregnancy
bull Maternal disease preeclampsia infection placental abnormalities precursors to premature birth
2018 NM FIT Annual Meeting 58
Cerebral Palsy (Novak et al 2017)
bull Most Common Physical Disorder in Children
bull 2 in High Income Countries ldquoCP describes a group of developmental disorders of movement and posture causing activity restrictions or disability that are attributed to disturbances occurring in the fetal or infant brain The motor impairment may be accompanied by a seizure disorder or by impairment of sensation cognition communication and or behavior ldquo
bull Originates prenatally or early post-natally
2018 NM FIT Annual Meeting 59
Three Groups Classification
1 Premature Infants (30-40 of all cases)
2 Term infants who develop neonatal encephalopathy shortly after birth (15-20)
3 Term infants without risk factors (40-50)
2018 NM FIT Annual Meeting 60
5302018
21
86 of parents suspected their child
had Cerebral Palsy before a clinical
diagnosis was made
2018 NM FIT Annual Meeting 61
RISK for CP
Identification Intervention
2018 NM FIT Annual Meeting 62
How do we build capacity
bull REFLECTIONbull Individual
bull What do I NOT knowbull As a program director
bull What questions keep coming up
2018 NM FIT Annual Meeting 63
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65
5302018
12
For infants over one month of age (adjusted) and under four months of age including adjusted age the IDA shall be used in conjunction with one of the following approved tools listed below)
bull All 5 developmental domains shall be assessed and addressed in the CME report including parentcaregiver information AIMS (Alberta Infant Motor Scale
bull TIMP (Test of Infant Motor Performance) bull Infant Toddler Sensory Profile bull Peabody Developmental Motor Scale (PDMS-2) bull Motor Skills Acquisition Checklist bull REEL-3 bull The Rossetti Infant Toddler Language Scale bull Other tools as approved by the FIT Program
2018 NM FIT Annual Meeting 34
AIMS-Alberta Infant Motor ScalesMotor Assessment of the Developing Infant
bull 0 ndash 18 months or walking decreased accuracy at 3 months of
age decreased precision after 9 months of age
bull ldquoobservedrdquo or ldquonot observedrdquo Items in the observed range create a motor window
bull Subscale scores are calculated by giving credit for observed items within the motor window plus giving credit for all of the less mature items before the motor window
bull The AIMS total score calculated by summing the scores
bull Score converted to a percentile and compared with age-equivalent peers from the normative sample
bull BUY THE BOOK
2018 NM FIT Annual Meeting 35
Psychometrics of AIMSbull Normed on 2202 infants between the ages of 1 week to 18
months living in province of Alberta between 1990 and 1992
bull Interrater reliability using two therapists who assessed 221 typically developing r values from a Pearson Product 096 to 099
bull Test-retest reliability was assessed by administering the AIMS twice (7 days between assessments) to 233 infants r values from a Pearson Product Moment Correlation Coefficient ranged from 086 to 099 when the same assessor scored the AIMS on both assessment days
2018 NM FIT Annual Meeting 36
5302018
13
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull Recommended cut-off scores for atypical development are the 10th
percentile at 4 months of age and the 5th percentile at 8 months of age (Darrah Piper amp Watt 1998)
bull Even typically developing infants do not acquire gross motor skills at a stable rate and could have a score that places them below the ldquocut-offrdquo score (Darrah et al 1998)
bull It is important to complete serial assessments and not simply identify a child as being delayed based on a one time screening
2018 NM FIT Annual Meeting 37
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull AIMS is thought to be appropriate for children between 0 -18 months it has been shown to have a ceiling effect with low precision of measurement after ~ 9 months of age or when children are able to lower themselves from standing with control Liao amp Campbell 2004
bull AIMS is much better at identifying infants with motor disabilities at 6 9 and 12 months than at 3 months of age Kolobe amp Bulanda 2006
bull The AIMS misclassified a high percentage of 3 month old infants later diagnosed with cerebral palsy (CP) where as it did much better at identifying children later diagnosed with CP when using the 5th percentile as a cut-off at 6 9 and 12 months of age Kolobe amp Bulanda 2006
bull These studies results should encourage clinicians to use caution when interpreting AIMS scores for infants 3 months of age as well as infants who are 9 months of age or older
2018 NM FIT Annual Meeting 38
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoslip-throughrdquo
bull How do they ldquolookrdquobull Curled ndash ldquohe is so cuddlyrdquo
bull Sacral sitting
bull Hands closedbull Cortical thumb
bull Ankle Clonusbull A few beats vs prolonged
2018 NM FIT Annual Meeting 39
5302018
14
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoone with the surfacerdquo
bull ldquohe never stops movingrdquobull Pull-to-sit hellip And into standing
bull On toes (ask about walkers and saucers and Johnny jump-ups)
bull Does he bear weight
bull Head shape and its effects on prone and supine
2018 NM FIT Annual Meeting 40
AIMS ldquoBehaviorsrdquo (cont)
bull Locking kneesbull ldquoCollapsingrdquo
bull Pull-to-sit moves straight into standing
bull Asymmetries
2018 NM FIT Annual Meeting 41
Symmetry
bull Always look for symmetry (in all evaluations) ndashbull ldquoI think that he is going to be left-handedrdquo
bull Use your reasoning skills
bull Asymmetry because of gravity taking head to one side
bull 2 months before baby can maintain midlinebull Does baby visually scan to both sides
2018 NM FIT Annual Meeting 42
5302018
15
2018 NM FIT Annual Meeting 43
Think of Dynamic Systemshellip
bull ASQs are prime example (and IDA)
bull What are we really looking atbull Some examples of systems approach
2018 NM FIT Annual Meeting 44
2018 NM FIT Annual Meeting 45
5302018
16
2018 NM FIT Annual Meeting 46
2018 NM FIT Annual Meeting 47
2018 NM FIT Annual Meeting 48
5302018
17
When is a ldquosit uprdquo a bad thing Van Haastert et al
Dev Med Child Neurol 2012 Jun54(6)538-43
ldquoActive head lifting from supine in early infancy an indicator for non-optimal cognitive outcome in late infancyrdquo
bull AHLS is associated with a less favorable cognitive outcome in the second year of life in preterm and in term-born infants than in comparison infants
2018 NM FIT Annual Meeting 49
RBI
bull Describe your babyrsquos ________
bull Observe babies eatingbull Dribblingbull Noisybull Falls ldquoasleeprdquobull Pushes awaybull Arching
bull All babies refluxbull Meds donrsquot stop refluxbull Effects of PPIs and H2 inhibitors
2018 NM FIT Annual Meeting 50
Transdisciplinary and Coaching
bull Effective Transdisciplinary is dependent on recognizing our own strengths and limitations ndash self-reflection
bull TTA is critical
2018 NM FIT Annual Meeting 51
5302018
18
Can we predict
bull httppartnersforkidsorgwp-contentuploads20171115236_Neo_Cerebral-Palsy-Early-ID_Practice-Tool_Q4-RMpdf
bull We do NOT diagnose
2018 NM FIT Annual Meeting 52
FIT Technical Assistance Document-Evaluation and Assessment p24ICO
2018 NM FIT Annual Meeting 53
And this is where we need to build the capacityhellip
bull ldquoDue to the varying nature and purpose of the scores of each of the above approved tools the scores themselves will not lead to eligibility but rather they will provide additional information for the team to consider in reaching a determination of the childs developmental status and eligibility
determinationrdquo
2018 NM FIT Annual Meeting 54
5302018
19
Informed Clinical Opinionbull An evaluation of the childrsquos level of functioning in each of the
following developmental areas
bull Cognitive development
bull Physical development including vision and hearing
bull Communication development
bull Social or emotional development and
bull Adaptive development
bull A review of the pertinent records related to the childrsquos current health status and medical history and can include areas such as but not limited to feeding sleeping motor behavior state regulation communication visual tracking and auditory responses
bull All 5 developmental domains and pertinent information shall be addressed in the CME report as well as parent report and shall include a statement and approval signature indicating that Informed Clinical Opinion was used
2018 NM FIT Annual Meeting 55
ICO example
bull httpswwwyoutubecomwatchv=ztd2-O0z9rM
2018 NM FIT Annual Meeting 56
Risk for Cerebral Palsy Early Detection
and Early InterventionPoster Presentation at 2018 Annual FIT Meeting
NMOTA Conference
September 2018
Amazing Newborn Conference
November 8-9 2018
2018 NM FIT Annual Meeting 57
5302018
20
Risk Factors for Cerebral Palsy(McIntrye et al 2011)
bull Prior to conception
bull History of still births miscarriage premature birth family history of CP low SES
bull Early Pregnancy
bull Infection multiple births genetic predisposition male gender birth defects
bull During Pregnancy
bull Maternal disease preeclampsia infection placental abnormalities precursors to premature birth
2018 NM FIT Annual Meeting 58
Cerebral Palsy (Novak et al 2017)
bull Most Common Physical Disorder in Children
bull 2 in High Income Countries ldquoCP describes a group of developmental disorders of movement and posture causing activity restrictions or disability that are attributed to disturbances occurring in the fetal or infant brain The motor impairment may be accompanied by a seizure disorder or by impairment of sensation cognition communication and or behavior ldquo
bull Originates prenatally or early post-natally
2018 NM FIT Annual Meeting 59
Three Groups Classification
1 Premature Infants (30-40 of all cases)
2 Term infants who develop neonatal encephalopathy shortly after birth (15-20)
3 Term infants without risk factors (40-50)
2018 NM FIT Annual Meeting 60
5302018
21
86 of parents suspected their child
had Cerebral Palsy before a clinical
diagnosis was made
2018 NM FIT Annual Meeting 61
RISK for CP
Identification Intervention
2018 NM FIT Annual Meeting 62
How do we build capacity
bull REFLECTIONbull Individual
bull What do I NOT knowbull As a program director
bull What questions keep coming up
2018 NM FIT Annual Meeting 63
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65
5302018
13
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull Recommended cut-off scores for atypical development are the 10th
percentile at 4 months of age and the 5th percentile at 8 months of age (Darrah Piper amp Watt 1998)
bull Even typically developing infants do not acquire gross motor skills at a stable rate and could have a score that places them below the ldquocut-offrdquo score (Darrah et al 1998)
bull It is important to complete serial assessments and not simply identify a child as being delayed based on a one time screening
2018 NM FIT Annual Meeting 37
Evidence Summary for Pediatric Rehabilitation Professionals Mayson 2007
bull AIMS is thought to be appropriate for children between 0 -18 months it has been shown to have a ceiling effect with low precision of measurement after ~ 9 months of age or when children are able to lower themselves from standing with control Liao amp Campbell 2004
bull AIMS is much better at identifying infants with motor disabilities at 6 9 and 12 months than at 3 months of age Kolobe amp Bulanda 2006
bull The AIMS misclassified a high percentage of 3 month old infants later diagnosed with cerebral palsy (CP) where as it did much better at identifying children later diagnosed with CP when using the 5th percentile as a cut-off at 6 9 and 12 months of age Kolobe amp Bulanda 2006
bull These studies results should encourage clinicians to use caution when interpreting AIMS scores for infants 3 months of age as well as infants who are 9 months of age or older
2018 NM FIT Annual Meeting 38
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoslip-throughrdquo
bull How do they ldquolookrdquobull Curled ndash ldquohe is so cuddlyrdquo
bull Sacral sitting
bull Hands closedbull Cortical thumb
bull Ankle Clonusbull A few beats vs prolonged
2018 NM FIT Annual Meeting 39
5302018
14
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoone with the surfacerdquo
bull ldquohe never stops movingrdquobull Pull-to-sit hellip And into standing
bull On toes (ask about walkers and saucers and Johnny jump-ups)
bull Does he bear weight
bull Head shape and its effects on prone and supine
2018 NM FIT Annual Meeting 40
AIMS ldquoBehaviorsrdquo (cont)
bull Locking kneesbull ldquoCollapsingrdquo
bull Pull-to-sit moves straight into standing
bull Asymmetries
2018 NM FIT Annual Meeting 41
Symmetry
bull Always look for symmetry (in all evaluations) ndashbull ldquoI think that he is going to be left-handedrdquo
bull Use your reasoning skills
bull Asymmetry because of gravity taking head to one side
bull 2 months before baby can maintain midlinebull Does baby visually scan to both sides
2018 NM FIT Annual Meeting 42
5302018
15
2018 NM FIT Annual Meeting 43
Think of Dynamic Systemshellip
bull ASQs are prime example (and IDA)
bull What are we really looking atbull Some examples of systems approach
2018 NM FIT Annual Meeting 44
2018 NM FIT Annual Meeting 45
5302018
16
2018 NM FIT Annual Meeting 46
2018 NM FIT Annual Meeting 47
2018 NM FIT Annual Meeting 48
5302018
17
When is a ldquosit uprdquo a bad thing Van Haastert et al
Dev Med Child Neurol 2012 Jun54(6)538-43
ldquoActive head lifting from supine in early infancy an indicator for non-optimal cognitive outcome in late infancyrdquo
bull AHLS is associated with a less favorable cognitive outcome in the second year of life in preterm and in term-born infants than in comparison infants
2018 NM FIT Annual Meeting 49
RBI
bull Describe your babyrsquos ________
bull Observe babies eatingbull Dribblingbull Noisybull Falls ldquoasleeprdquobull Pushes awaybull Arching
bull All babies refluxbull Meds donrsquot stop refluxbull Effects of PPIs and H2 inhibitors
2018 NM FIT Annual Meeting 50
Transdisciplinary and Coaching
bull Effective Transdisciplinary is dependent on recognizing our own strengths and limitations ndash self-reflection
bull TTA is critical
2018 NM FIT Annual Meeting 51
5302018
18
Can we predict
bull httppartnersforkidsorgwp-contentuploads20171115236_Neo_Cerebral-Palsy-Early-ID_Practice-Tool_Q4-RMpdf
bull We do NOT diagnose
2018 NM FIT Annual Meeting 52
FIT Technical Assistance Document-Evaluation and Assessment p24ICO
2018 NM FIT Annual Meeting 53
And this is where we need to build the capacityhellip
bull ldquoDue to the varying nature and purpose of the scores of each of the above approved tools the scores themselves will not lead to eligibility but rather they will provide additional information for the team to consider in reaching a determination of the childs developmental status and eligibility
determinationrdquo
2018 NM FIT Annual Meeting 54
5302018
19
Informed Clinical Opinionbull An evaluation of the childrsquos level of functioning in each of the
following developmental areas
bull Cognitive development
bull Physical development including vision and hearing
bull Communication development
bull Social or emotional development and
bull Adaptive development
bull A review of the pertinent records related to the childrsquos current health status and medical history and can include areas such as but not limited to feeding sleeping motor behavior state regulation communication visual tracking and auditory responses
bull All 5 developmental domains and pertinent information shall be addressed in the CME report as well as parent report and shall include a statement and approval signature indicating that Informed Clinical Opinion was used
2018 NM FIT Annual Meeting 55
ICO example
bull httpswwwyoutubecomwatchv=ztd2-O0z9rM
2018 NM FIT Annual Meeting 56
Risk for Cerebral Palsy Early Detection
and Early InterventionPoster Presentation at 2018 Annual FIT Meeting
NMOTA Conference
September 2018
Amazing Newborn Conference
November 8-9 2018
2018 NM FIT Annual Meeting 57
5302018
20
Risk Factors for Cerebral Palsy(McIntrye et al 2011)
bull Prior to conception
bull History of still births miscarriage premature birth family history of CP low SES
bull Early Pregnancy
bull Infection multiple births genetic predisposition male gender birth defects
bull During Pregnancy
bull Maternal disease preeclampsia infection placental abnormalities precursors to premature birth
2018 NM FIT Annual Meeting 58
Cerebral Palsy (Novak et al 2017)
bull Most Common Physical Disorder in Children
bull 2 in High Income Countries ldquoCP describes a group of developmental disorders of movement and posture causing activity restrictions or disability that are attributed to disturbances occurring in the fetal or infant brain The motor impairment may be accompanied by a seizure disorder or by impairment of sensation cognition communication and or behavior ldquo
bull Originates prenatally or early post-natally
2018 NM FIT Annual Meeting 59
Three Groups Classification
1 Premature Infants (30-40 of all cases)
2 Term infants who develop neonatal encephalopathy shortly after birth (15-20)
3 Term infants without risk factors (40-50)
2018 NM FIT Annual Meeting 60
5302018
21
86 of parents suspected their child
had Cerebral Palsy before a clinical
diagnosis was made
2018 NM FIT Annual Meeting 61
RISK for CP
Identification Intervention
2018 NM FIT Annual Meeting 62
How do we build capacity
bull REFLECTIONbull Individual
bull What do I NOT knowbull As a program director
bull What questions keep coming up
2018 NM FIT Annual Meeting 63
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65

5302018
14
AIMS ldquobehaviorsrdquobull Muscle stiffnesstone
bull ldquoone with the surfacerdquo
bull ldquohe never stops movingrdquobull Pull-to-sit hellip And into standing
bull On toes (ask about walkers and saucers and Johnny jump-ups)
bull Does he bear weight
bull Head shape and its effects on prone and supine
2018 NM FIT Annual Meeting 40
AIMS ldquoBehaviorsrdquo (cont)
bull Locking kneesbull ldquoCollapsingrdquo
bull Pull-to-sit moves straight into standing
bull Asymmetries
2018 NM FIT Annual Meeting 41
Symmetry
bull Always look for symmetry (in all evaluations) ndashbull ldquoI think that he is going to be left-handedrdquo
bull Use your reasoning skills
bull Asymmetry because of gravity taking head to one side
bull 2 months before baby can maintain midlinebull Does baby visually scan to both sides
2018 NM FIT Annual Meeting 42
5302018
15
2018 NM FIT Annual Meeting 43
Think of Dynamic Systemshellip
bull ASQs are prime example (and IDA)
bull What are we really looking atbull Some examples of systems approach
2018 NM FIT Annual Meeting 44
2018 NM FIT Annual Meeting 45
5302018
16
2018 NM FIT Annual Meeting 46
2018 NM FIT Annual Meeting 47
2018 NM FIT Annual Meeting 48
5302018
17
When is a ldquosit uprdquo a bad thing Van Haastert et al
Dev Med Child Neurol 2012 Jun54(6)538-43
ldquoActive head lifting from supine in early infancy an indicator for non-optimal cognitive outcome in late infancyrdquo
bull AHLS is associated with a less favorable cognitive outcome in the second year of life in preterm and in term-born infants than in comparison infants
2018 NM FIT Annual Meeting 49
RBI
bull Describe your babyrsquos ________
bull Observe babies eatingbull Dribblingbull Noisybull Falls ldquoasleeprdquobull Pushes awaybull Arching
bull All babies refluxbull Meds donrsquot stop refluxbull Effects of PPIs and H2 inhibitors
2018 NM FIT Annual Meeting 50
Transdisciplinary and Coaching
bull Effective Transdisciplinary is dependent on recognizing our own strengths and limitations ndash self-reflection
bull TTA is critical
2018 NM FIT Annual Meeting 51
5302018
18
Can we predict
bull httppartnersforkidsorgwp-contentuploads20171115236_Neo_Cerebral-Palsy-Early-ID_Practice-Tool_Q4-RMpdf
bull We do NOT diagnose
2018 NM FIT Annual Meeting 52
FIT Technical Assistance Document-Evaluation and Assessment p24ICO
2018 NM FIT Annual Meeting 53
And this is where we need to build the capacityhellip
bull ldquoDue to the varying nature and purpose of the scores of each of the above approved tools the scores themselves will not lead to eligibility but rather they will provide additional information for the team to consider in reaching a determination of the childs developmental status and eligibility
determinationrdquo
2018 NM FIT Annual Meeting 54
5302018
19
Informed Clinical Opinionbull An evaluation of the childrsquos level of functioning in each of the
following developmental areas
bull Cognitive development
bull Physical development including vision and hearing
bull Communication development
bull Social or emotional development and
bull Adaptive development
bull A review of the pertinent records related to the childrsquos current health status and medical history and can include areas such as but not limited to feeding sleeping motor behavior state regulation communication visual tracking and auditory responses
bull All 5 developmental domains and pertinent information shall be addressed in the CME report as well as parent report and shall include a statement and approval signature indicating that Informed Clinical Opinion was used
2018 NM FIT Annual Meeting 55
ICO example
bull httpswwwyoutubecomwatchv=ztd2-O0z9rM
2018 NM FIT Annual Meeting 56
Risk for Cerebral Palsy Early Detection
and Early InterventionPoster Presentation at 2018 Annual FIT Meeting
NMOTA Conference
September 2018
Amazing Newborn Conference
November 8-9 2018
2018 NM FIT Annual Meeting 57
5302018
20
Risk Factors for Cerebral Palsy(McIntrye et al 2011)
bull Prior to conception
bull History of still births miscarriage premature birth family history of CP low SES
bull Early Pregnancy
bull Infection multiple births genetic predisposition male gender birth defects
bull During Pregnancy
bull Maternal disease preeclampsia infection placental abnormalities precursors to premature birth
2018 NM FIT Annual Meeting 58
Cerebral Palsy (Novak et al 2017)
bull Most Common Physical Disorder in Children
bull 2 in High Income Countries ldquoCP describes a group of developmental disorders of movement and posture causing activity restrictions or disability that are attributed to disturbances occurring in the fetal or infant brain The motor impairment may be accompanied by a seizure disorder or by impairment of sensation cognition communication and or behavior ldquo
bull Originates prenatally or early post-natally
2018 NM FIT Annual Meeting 59
Three Groups Classification
1 Premature Infants (30-40 of all cases)
2 Term infants who develop neonatal encephalopathy shortly after birth (15-20)
3 Term infants without risk factors (40-50)
2018 NM FIT Annual Meeting 60
5302018
21
86 of parents suspected their child
had Cerebral Palsy before a clinical
diagnosis was made
2018 NM FIT Annual Meeting 61
RISK for CP
Identification Intervention
2018 NM FIT Annual Meeting 62
How do we build capacity
bull REFLECTIONbull Individual
bull What do I NOT knowbull As a program director
bull What questions keep coming up
2018 NM FIT Annual Meeting 63
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65
5302018
15
2018 NM FIT Annual Meeting 43
Think of Dynamic Systemshellip
bull ASQs are prime example (and IDA)
bull What are we really looking atbull Some examples of systems approach
2018 NM FIT Annual Meeting 44
2018 NM FIT Annual Meeting 45
5302018
16
2018 NM FIT Annual Meeting 46
2018 NM FIT Annual Meeting 47
2018 NM FIT Annual Meeting 48
5302018
17
When is a ldquosit uprdquo a bad thing Van Haastert et al
Dev Med Child Neurol 2012 Jun54(6)538-43
ldquoActive head lifting from supine in early infancy an indicator for non-optimal cognitive outcome in late infancyrdquo
bull AHLS is associated with a less favorable cognitive outcome in the second year of life in preterm and in term-born infants than in comparison infants
2018 NM FIT Annual Meeting 49
RBI
bull Describe your babyrsquos ________
bull Observe babies eatingbull Dribblingbull Noisybull Falls ldquoasleeprdquobull Pushes awaybull Arching
bull All babies refluxbull Meds donrsquot stop refluxbull Effects of PPIs and H2 inhibitors
2018 NM FIT Annual Meeting 50
Transdisciplinary and Coaching
bull Effective Transdisciplinary is dependent on recognizing our own strengths and limitations ndash self-reflection
bull TTA is critical
2018 NM FIT Annual Meeting 51
5302018
18
Can we predict
bull httppartnersforkidsorgwp-contentuploads20171115236_Neo_Cerebral-Palsy-Early-ID_Practice-Tool_Q4-RMpdf
bull We do NOT diagnose
2018 NM FIT Annual Meeting 52
FIT Technical Assistance Document-Evaluation and Assessment p24ICO
2018 NM FIT Annual Meeting 53
And this is where we need to build the capacityhellip
bull ldquoDue to the varying nature and purpose of the scores of each of the above approved tools the scores themselves will not lead to eligibility but rather they will provide additional information for the team to consider in reaching a determination of the childs developmental status and eligibility
determinationrdquo
2018 NM FIT Annual Meeting 54
5302018
19
Informed Clinical Opinionbull An evaluation of the childrsquos level of functioning in each of the
following developmental areas
bull Cognitive development
bull Physical development including vision and hearing
bull Communication development
bull Social or emotional development and
bull Adaptive development
bull A review of the pertinent records related to the childrsquos current health status and medical history and can include areas such as but not limited to feeding sleeping motor behavior state regulation communication visual tracking and auditory responses
bull All 5 developmental domains and pertinent information shall be addressed in the CME report as well as parent report and shall include a statement and approval signature indicating that Informed Clinical Opinion was used
2018 NM FIT Annual Meeting 55
ICO example
bull httpswwwyoutubecomwatchv=ztd2-O0z9rM
2018 NM FIT Annual Meeting 56
Risk for Cerebral Palsy Early Detection
and Early InterventionPoster Presentation at 2018 Annual FIT Meeting
NMOTA Conference
September 2018
Amazing Newborn Conference
November 8-9 2018
2018 NM FIT Annual Meeting 57
5302018
20
Risk Factors for Cerebral Palsy(McIntrye et al 2011)
bull Prior to conception
bull History of still births miscarriage premature birth family history of CP low SES
bull Early Pregnancy
bull Infection multiple births genetic predisposition male gender birth defects
bull During Pregnancy
bull Maternal disease preeclampsia infection placental abnormalities precursors to premature birth
2018 NM FIT Annual Meeting 58
Cerebral Palsy (Novak et al 2017)
bull Most Common Physical Disorder in Children
bull 2 in High Income Countries ldquoCP describes a group of developmental disorders of movement and posture causing activity restrictions or disability that are attributed to disturbances occurring in the fetal or infant brain The motor impairment may be accompanied by a seizure disorder or by impairment of sensation cognition communication and or behavior ldquo
bull Originates prenatally or early post-natally
2018 NM FIT Annual Meeting 59
Three Groups Classification
1 Premature Infants (30-40 of all cases)
2 Term infants who develop neonatal encephalopathy shortly after birth (15-20)
3 Term infants without risk factors (40-50)
2018 NM FIT Annual Meeting 60
5302018
21
86 of parents suspected their child
had Cerebral Palsy before a clinical
diagnosis was made
2018 NM FIT Annual Meeting 61
RISK for CP
Identification Intervention
2018 NM FIT Annual Meeting 62
How do we build capacity
bull REFLECTIONbull Individual
bull What do I NOT knowbull As a program director
bull What questions keep coming up
2018 NM FIT Annual Meeting 63
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65
5302018
16
2018 NM FIT Annual Meeting 46
2018 NM FIT Annual Meeting 47
2018 NM FIT Annual Meeting 48
5302018
17
When is a ldquosit uprdquo a bad thing Van Haastert et al
Dev Med Child Neurol 2012 Jun54(6)538-43
ldquoActive head lifting from supine in early infancy an indicator for non-optimal cognitive outcome in late infancyrdquo
bull AHLS is associated with a less favorable cognitive outcome in the second year of life in preterm and in term-born infants than in comparison infants
2018 NM FIT Annual Meeting 49
RBI
bull Describe your babyrsquos ________
bull Observe babies eatingbull Dribblingbull Noisybull Falls ldquoasleeprdquobull Pushes awaybull Arching
bull All babies refluxbull Meds donrsquot stop refluxbull Effects of PPIs and H2 inhibitors
2018 NM FIT Annual Meeting 50
Transdisciplinary and Coaching
bull Effective Transdisciplinary is dependent on recognizing our own strengths and limitations ndash self-reflection
bull TTA is critical
2018 NM FIT Annual Meeting 51
5302018
18
Can we predict
bull httppartnersforkidsorgwp-contentuploads20171115236_Neo_Cerebral-Palsy-Early-ID_Practice-Tool_Q4-RMpdf
bull We do NOT diagnose
2018 NM FIT Annual Meeting 52
FIT Technical Assistance Document-Evaluation and Assessment p24ICO
2018 NM FIT Annual Meeting 53
And this is where we need to build the capacityhellip
bull ldquoDue to the varying nature and purpose of the scores of each of the above approved tools the scores themselves will not lead to eligibility but rather they will provide additional information for the team to consider in reaching a determination of the childs developmental status and eligibility
determinationrdquo
2018 NM FIT Annual Meeting 54
5302018
19
Informed Clinical Opinionbull An evaluation of the childrsquos level of functioning in each of the
following developmental areas
bull Cognitive development
bull Physical development including vision and hearing
bull Communication development
bull Social or emotional development and
bull Adaptive development
bull A review of the pertinent records related to the childrsquos current health status and medical history and can include areas such as but not limited to feeding sleeping motor behavior state regulation communication visual tracking and auditory responses
bull All 5 developmental domains and pertinent information shall be addressed in the CME report as well as parent report and shall include a statement and approval signature indicating that Informed Clinical Opinion was used
2018 NM FIT Annual Meeting 55
ICO example
bull httpswwwyoutubecomwatchv=ztd2-O0z9rM
2018 NM FIT Annual Meeting 56
Risk for Cerebral Palsy Early Detection
and Early InterventionPoster Presentation at 2018 Annual FIT Meeting
NMOTA Conference
September 2018
Amazing Newborn Conference
November 8-9 2018
2018 NM FIT Annual Meeting 57
5302018
20
Risk Factors for Cerebral Palsy(McIntrye et al 2011)
bull Prior to conception
bull History of still births miscarriage premature birth family history of CP low SES
bull Early Pregnancy
bull Infection multiple births genetic predisposition male gender birth defects
bull During Pregnancy
bull Maternal disease preeclampsia infection placental abnormalities precursors to premature birth
2018 NM FIT Annual Meeting 58
Cerebral Palsy (Novak et al 2017)
bull Most Common Physical Disorder in Children
bull 2 in High Income Countries ldquoCP describes a group of developmental disorders of movement and posture causing activity restrictions or disability that are attributed to disturbances occurring in the fetal or infant brain The motor impairment may be accompanied by a seizure disorder or by impairment of sensation cognition communication and or behavior ldquo
bull Originates prenatally or early post-natally
2018 NM FIT Annual Meeting 59
Three Groups Classification
1 Premature Infants (30-40 of all cases)
2 Term infants who develop neonatal encephalopathy shortly after birth (15-20)
3 Term infants without risk factors (40-50)
2018 NM FIT Annual Meeting 60
5302018
21
86 of parents suspected their child
had Cerebral Palsy before a clinical
diagnosis was made
2018 NM FIT Annual Meeting 61
RISK for CP
Identification Intervention
2018 NM FIT Annual Meeting 62
How do we build capacity
bull REFLECTIONbull Individual
bull What do I NOT knowbull As a program director
bull What questions keep coming up
2018 NM FIT Annual Meeting 63
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65
5302018
17
When is a ldquosit uprdquo a bad thing Van Haastert et al
Dev Med Child Neurol 2012 Jun54(6)538-43
ldquoActive head lifting from supine in early infancy an indicator for non-optimal cognitive outcome in late infancyrdquo
bull AHLS is associated with a less favorable cognitive outcome in the second year of life in preterm and in term-born infants than in comparison infants
2018 NM FIT Annual Meeting 49
RBI
bull Describe your babyrsquos ________
bull Observe babies eatingbull Dribblingbull Noisybull Falls ldquoasleeprdquobull Pushes awaybull Arching
bull All babies refluxbull Meds donrsquot stop refluxbull Effects of PPIs and H2 inhibitors
2018 NM FIT Annual Meeting 50
Transdisciplinary and Coaching
bull Effective Transdisciplinary is dependent on recognizing our own strengths and limitations ndash self-reflection
bull TTA is critical
2018 NM FIT Annual Meeting 51
5302018
18
Can we predict
bull httppartnersforkidsorgwp-contentuploads20171115236_Neo_Cerebral-Palsy-Early-ID_Practice-Tool_Q4-RMpdf
bull We do NOT diagnose
2018 NM FIT Annual Meeting 52
FIT Technical Assistance Document-Evaluation and Assessment p24ICO
2018 NM FIT Annual Meeting 53
And this is where we need to build the capacityhellip
bull ldquoDue to the varying nature and purpose of the scores of each of the above approved tools the scores themselves will not lead to eligibility but rather they will provide additional information for the team to consider in reaching a determination of the childs developmental status and eligibility
determinationrdquo
2018 NM FIT Annual Meeting 54
5302018
19
Informed Clinical Opinionbull An evaluation of the childrsquos level of functioning in each of the
following developmental areas
bull Cognitive development
bull Physical development including vision and hearing
bull Communication development
bull Social or emotional development and
bull Adaptive development
bull A review of the pertinent records related to the childrsquos current health status and medical history and can include areas such as but not limited to feeding sleeping motor behavior state regulation communication visual tracking and auditory responses
bull All 5 developmental domains and pertinent information shall be addressed in the CME report as well as parent report and shall include a statement and approval signature indicating that Informed Clinical Opinion was used
2018 NM FIT Annual Meeting 55
ICO example
bull httpswwwyoutubecomwatchv=ztd2-O0z9rM
2018 NM FIT Annual Meeting 56
Risk for Cerebral Palsy Early Detection
and Early InterventionPoster Presentation at 2018 Annual FIT Meeting
NMOTA Conference
September 2018
Amazing Newborn Conference
November 8-9 2018
2018 NM FIT Annual Meeting 57
5302018
20
Risk Factors for Cerebral Palsy(McIntrye et al 2011)
bull Prior to conception
bull History of still births miscarriage premature birth family history of CP low SES
bull Early Pregnancy
bull Infection multiple births genetic predisposition male gender birth defects
bull During Pregnancy
bull Maternal disease preeclampsia infection placental abnormalities precursors to premature birth
2018 NM FIT Annual Meeting 58
Cerebral Palsy (Novak et al 2017)
bull Most Common Physical Disorder in Children
bull 2 in High Income Countries ldquoCP describes a group of developmental disorders of movement and posture causing activity restrictions or disability that are attributed to disturbances occurring in the fetal or infant brain The motor impairment may be accompanied by a seizure disorder or by impairment of sensation cognition communication and or behavior ldquo
bull Originates prenatally or early post-natally
2018 NM FIT Annual Meeting 59
Three Groups Classification
1 Premature Infants (30-40 of all cases)
2 Term infants who develop neonatal encephalopathy shortly after birth (15-20)
3 Term infants without risk factors (40-50)
2018 NM FIT Annual Meeting 60
5302018
21
86 of parents suspected their child
had Cerebral Palsy before a clinical
diagnosis was made
2018 NM FIT Annual Meeting 61
RISK for CP
Identification Intervention
2018 NM FIT Annual Meeting 62
How do we build capacity
bull REFLECTIONbull Individual
bull What do I NOT knowbull As a program director
bull What questions keep coming up
2018 NM FIT Annual Meeting 63
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65
5302018
18
Can we predict
bull httppartnersforkidsorgwp-contentuploads20171115236_Neo_Cerebral-Palsy-Early-ID_Practice-Tool_Q4-RMpdf
bull We do NOT diagnose
2018 NM FIT Annual Meeting 52
FIT Technical Assistance Document-Evaluation and Assessment p24ICO
2018 NM FIT Annual Meeting 53
And this is where we need to build the capacityhellip
bull ldquoDue to the varying nature and purpose of the scores of each of the above approved tools the scores themselves will not lead to eligibility but rather they will provide additional information for the team to consider in reaching a determination of the childs developmental status and eligibility
determinationrdquo
2018 NM FIT Annual Meeting 54
5302018
19
Informed Clinical Opinionbull An evaluation of the childrsquos level of functioning in each of the
following developmental areas
bull Cognitive development
bull Physical development including vision and hearing
bull Communication development
bull Social or emotional development and
bull Adaptive development
bull A review of the pertinent records related to the childrsquos current health status and medical history and can include areas such as but not limited to feeding sleeping motor behavior state regulation communication visual tracking and auditory responses
bull All 5 developmental domains and pertinent information shall be addressed in the CME report as well as parent report and shall include a statement and approval signature indicating that Informed Clinical Opinion was used
2018 NM FIT Annual Meeting 55
ICO example
bull httpswwwyoutubecomwatchv=ztd2-O0z9rM
2018 NM FIT Annual Meeting 56
Risk for Cerebral Palsy Early Detection
and Early InterventionPoster Presentation at 2018 Annual FIT Meeting
NMOTA Conference
September 2018
Amazing Newborn Conference
November 8-9 2018
2018 NM FIT Annual Meeting 57
5302018
20
Risk Factors for Cerebral Palsy(McIntrye et al 2011)
bull Prior to conception
bull History of still births miscarriage premature birth family history of CP low SES
bull Early Pregnancy
bull Infection multiple births genetic predisposition male gender birth defects
bull During Pregnancy
bull Maternal disease preeclampsia infection placental abnormalities precursors to premature birth
2018 NM FIT Annual Meeting 58
Cerebral Palsy (Novak et al 2017)
bull Most Common Physical Disorder in Children
bull 2 in High Income Countries ldquoCP describes a group of developmental disorders of movement and posture causing activity restrictions or disability that are attributed to disturbances occurring in the fetal or infant brain The motor impairment may be accompanied by a seizure disorder or by impairment of sensation cognition communication and or behavior ldquo
bull Originates prenatally or early post-natally
2018 NM FIT Annual Meeting 59
Three Groups Classification
1 Premature Infants (30-40 of all cases)
2 Term infants who develop neonatal encephalopathy shortly after birth (15-20)
3 Term infants without risk factors (40-50)
2018 NM FIT Annual Meeting 60
5302018
21
86 of parents suspected their child
had Cerebral Palsy before a clinical
diagnosis was made
2018 NM FIT Annual Meeting 61
RISK for CP
Identification Intervention
2018 NM FIT Annual Meeting 62
How do we build capacity
bull REFLECTIONbull Individual
bull What do I NOT knowbull As a program director
bull What questions keep coming up
2018 NM FIT Annual Meeting 63
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65
5302018
19
Informed Clinical Opinionbull An evaluation of the childrsquos level of functioning in each of the
following developmental areas
bull Cognitive development
bull Physical development including vision and hearing
bull Communication development
bull Social or emotional development and
bull Adaptive development
bull A review of the pertinent records related to the childrsquos current health status and medical history and can include areas such as but not limited to feeding sleeping motor behavior state regulation communication visual tracking and auditory responses
bull All 5 developmental domains and pertinent information shall be addressed in the CME report as well as parent report and shall include a statement and approval signature indicating that Informed Clinical Opinion was used
2018 NM FIT Annual Meeting 55
ICO example
bull httpswwwyoutubecomwatchv=ztd2-O0z9rM
2018 NM FIT Annual Meeting 56
Risk for Cerebral Palsy Early Detection
and Early InterventionPoster Presentation at 2018 Annual FIT Meeting
NMOTA Conference
September 2018
Amazing Newborn Conference
November 8-9 2018
2018 NM FIT Annual Meeting 57
5302018
20
Risk Factors for Cerebral Palsy(McIntrye et al 2011)
bull Prior to conception
bull History of still births miscarriage premature birth family history of CP low SES
bull Early Pregnancy
bull Infection multiple births genetic predisposition male gender birth defects
bull During Pregnancy
bull Maternal disease preeclampsia infection placental abnormalities precursors to premature birth
2018 NM FIT Annual Meeting 58
Cerebral Palsy (Novak et al 2017)
bull Most Common Physical Disorder in Children
bull 2 in High Income Countries ldquoCP describes a group of developmental disorders of movement and posture causing activity restrictions or disability that are attributed to disturbances occurring in the fetal or infant brain The motor impairment may be accompanied by a seizure disorder or by impairment of sensation cognition communication and or behavior ldquo
bull Originates prenatally or early post-natally
2018 NM FIT Annual Meeting 59
Three Groups Classification
1 Premature Infants (30-40 of all cases)
2 Term infants who develop neonatal encephalopathy shortly after birth (15-20)
3 Term infants without risk factors (40-50)
2018 NM FIT Annual Meeting 60
5302018
21
86 of parents suspected their child
had Cerebral Palsy before a clinical
diagnosis was made
2018 NM FIT Annual Meeting 61
RISK for CP
Identification Intervention
2018 NM FIT Annual Meeting 62
How do we build capacity
bull REFLECTIONbull Individual
bull What do I NOT knowbull As a program director
bull What questions keep coming up
2018 NM FIT Annual Meeting 63
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65
5302018
20
Risk Factors for Cerebral Palsy(McIntrye et al 2011)
bull Prior to conception
bull History of still births miscarriage premature birth family history of CP low SES
bull Early Pregnancy
bull Infection multiple births genetic predisposition male gender birth defects
bull During Pregnancy
bull Maternal disease preeclampsia infection placental abnormalities precursors to premature birth
2018 NM FIT Annual Meeting 58
Cerebral Palsy (Novak et al 2017)
bull Most Common Physical Disorder in Children
bull 2 in High Income Countries ldquoCP describes a group of developmental disorders of movement and posture causing activity restrictions or disability that are attributed to disturbances occurring in the fetal or infant brain The motor impairment may be accompanied by a seizure disorder or by impairment of sensation cognition communication and or behavior ldquo
bull Originates prenatally or early post-natally
2018 NM FIT Annual Meeting 59
Three Groups Classification
1 Premature Infants (30-40 of all cases)
2 Term infants who develop neonatal encephalopathy shortly after birth (15-20)
3 Term infants without risk factors (40-50)
2018 NM FIT Annual Meeting 60
5302018
21
86 of parents suspected their child
had Cerebral Palsy before a clinical
diagnosis was made
2018 NM FIT Annual Meeting 61
RISK for CP
Identification Intervention
2018 NM FIT Annual Meeting 62
How do we build capacity
bull REFLECTIONbull Individual
bull What do I NOT knowbull As a program director
bull What questions keep coming up
2018 NM FIT Annual Meeting 63
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65
5302018
21
86 of parents suspected their child
had Cerebral Palsy before a clinical
diagnosis was made
2018 NM FIT Annual Meeting 61
RISK for CP
Identification Intervention
2018 NM FIT Annual Meeting 62
How do we build capacity
bull REFLECTIONbull Individual
bull What do I NOT knowbull As a program director
bull What questions keep coming up
2018 NM FIT Annual Meeting 63
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65
5302018
22
How do we build capacity
Challenges
bull Accessibility for training
bull Cost of training
bull Developing Professionalism
Solutions
bull Options for face-to-face
bull Consolidate funding sources
bull Journal Clubsbull Professional
AssociationsCEUsbull NMOTAbull NMAPTAbull NMSHA
bull Early Childhood Learning Network
bull Networkingbull SBC visits with Families
2018 NM FIT Annual Meeting 64
AIMS youtube links
Baby is 18 -months but it is nice to practice and to compare their scoring with yours LOOK AND SCORE BEFORE you see what they scored look at the qualitative aspects
httpswwwyoutubecomwatchv=HM5KEMw-rmE
Infant There is no narration and no scoring What total scores to you get what qualitative observations can you makehttpswwwyoutubecomwatchv=Pxdh4Lp_Ml4
2018 NM FIT Annual Meeting 65









![Increasingimageresolutiononportabledisplays … · 2017. 9. 9. · increasingimageresolutiononportabledisplays5 Fig.7. DiagonalDirectSubpixel-basedDownsampling(DDSD)Pattern. In[15],FangandAuobservethattheimprovementof](https://img.pdfslide.net/doc/110x75/5fde9ea995b44a620b1acf69/increasingimageresolutiononportabledisplays-2017-9-9-increasingimageresolutiononportabledisplays5.jpg)



















