Embed Size (px)
Citation preview

Filariasis
Can be classified depending on their
habitat in human tissues
1- Lymphatic filariasis.
2- body cavity filariasis.
3- Connective tissue filariasis.
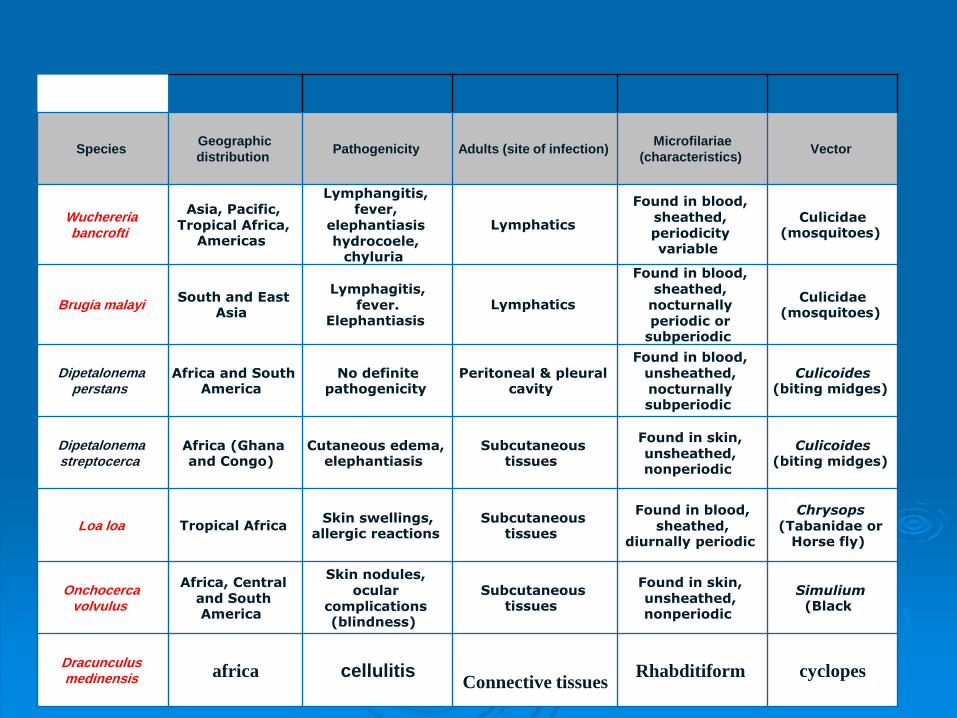
Species Geographic
distribution Pathogenicity Adults (site of infection)
Microfilariae
(characteristics) Vector
Wuchereriabancrofti
Asia, Pacific, Tropical Africa,
Americas
Lymphangitis, fever,
elephantiasis hydrocoele,
chyluria
Lymphatics
Found in blood, sheathed, periodicity variable
Culicidae (mosquitoes)
Brugia malayiSouth and East
Asia
Lymphagitis, fever.
Elephantiasis Lymphatics
Found in blood, sheathed,
nocturnally periodic or
subperiodic
Culicidae (mosquitoes)
Dipetalonema perstans
Africa and South America
No definite pathogenicity
Peritoneal & pleural cavity
Found in blood, unsheathed, nocturnally subperiodic
Culicoides (biting midges)
Dipetalonema streptocerca
Africa (Ghana and Congo)
Cutaneous edema, elephantiasis
Subcutaneous tissues
Found in skin, unsheathed, nonperiodic
Culicoides (biting midges)
Loa loa Tropical Africa Skin swellings,
allergic reactions Subcutaneous
tissues
Found in blood, sheathed,
diurnally periodic
Chrysops(Tabanidae or
Horse fly)
Onchocercavolvulus
Africa, Central and South America
Skin nodules, ocular
complications (blindness)
Subcutaneous tissues
Found in skin, unsheathed, nonperiodic
Simulium(Black
Dracunculusmedinensis africa cellulitis
Connective tissuesRhabditiform cyclopes

What is Lymphatic Filariasis?
Parasitic disease where microfilaria enter the blood stream through mosquito bites

Parasites
White, slender roundworms
Three types: Wuchereriabancrofti, Brugia malayi, Brugia timori
Live for 5-7 years, produce millions of microfilaria
Creamy filarform 2-50cm female twice male
Microfilria 200 micrhabditiform and filariform
EPIDEMIOLOGY
W. bancrofti occurs in the following regions: sub-Saharan Africa, Southeast Asia, the Indian subcontinent, many of the Pacific islands, and focal areas in Latin America.
B. malayi occurs mainly in China, India, Malaysia, the Philippines, Indonesia, and various Pacific islands.
B. timori is limited to the Timor Island of Indonesia.

EPIDEMIOLOGY
It is estimated that more than 120 million people worldwide are infected with one of these three microfilariae.
More than 90 percent of these infections are due to W. bancrofti, and the remainder are mostly due to B. malayi.
Estimates suggest that more than 40 million infected individuals are seriously incapacitated and disfigured by the disease.

Infected Regions

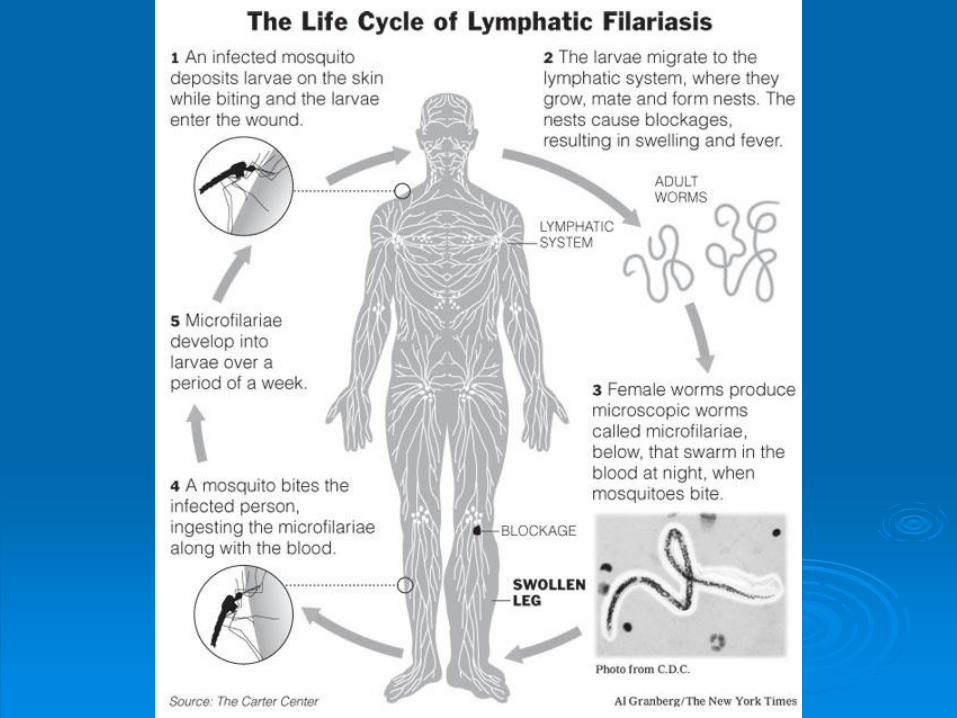
LIFE CYCLE
W. bancrofti, B. malayi, and B. timori are all acquired via the bite of mosquitoes.
When mosquitoes bite humans, they deposit third-stage infective larvae into the skin.
These larvae travel through the dermis and enter local lymphatic vessels. Over a period of approximately nine months, these larvae undergo a series of molts and develop into mature adult worms, which range from 2 to 5cm in length.
These adults reside in the lymphatics, generally several centimeters from lymph nodes. They survive for approximately five years (occasionally up to 12 to 15 years), during which time male and females worms mate and produce microfilariae.
Female parasites can release more than 10,000 microfilariae per day into the bloodstream. These microfilariae are also known as embryonic or first-stage larvae, and measure approximately 200 to 300 µm by 10 µm.

LIFE CYCLE
Mosquitoes, which bite infected individuals, can take up these circulating microfilariae. Within the mosquito, these embryonic larvae develop into second then third stage larvae over a period of 10 to 14 days. The mosquito is then ready to bite and infect a new human host, thereby completing the life cycle.
The interval between acquisition of infective larvae from a mosquito bite and detection of microfilariae in the blood is known as the prepatent period. This interval is usually approximately 12 months in duration.

Process of Infection

Symptoms

CLINICAL FEATURES
Most people infected with Brugian or Bancroftianfilariasis in endemic areas are asymptomatic, since the development of symptoms relates to the cumulative acquisition of increasing numbers of worms.
The clinical course of lymphatic filariasis includes three distinct phases:
asymptomatic microfilaremia,
acute episodes of adenolymphangitis (ADL),
chronic lymphedema disease (irreversible lymphedema), which is often superimposed upon repeated episodes of ADL.

Acute adenolymphangitis
Acute adenolymphangitis (ADL) characteristically presents with the sudden onset of fever and painful lymphadenopathy.
ADL is thought to occur because of immune-mediated responses to dying adult worms. It can manifest in a variety of locations, but the inguinal nodes and lower limbs are commonly involved.
The inflammation tends to resolve spontaneously after four to seven days, but recurrences are frequent.
In addition, secondary bacterial infections can occur related to the breakdown of skin barriers in edematous or elephantatic skin or overlying intensely inflamed lymph nodes.

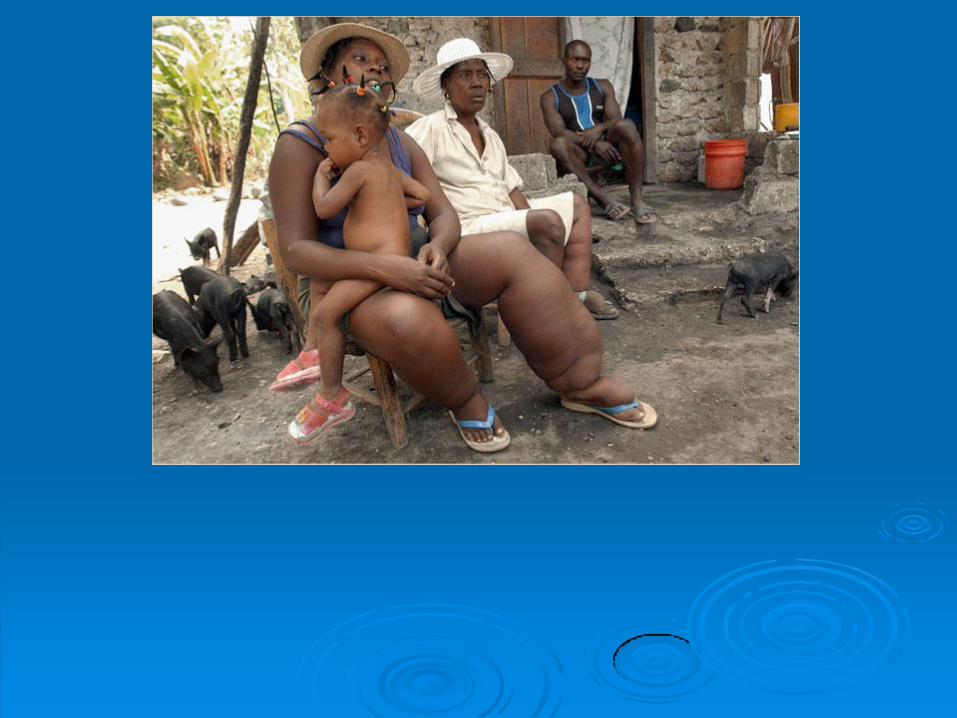
Chronic Lymphedema
Lymphedema, or swelling of a limb related to chronic inflammation of the lymphatic vessels, is a common late sequela of filarial infection.
When the lymph vessels in the inguinal region are involved, swelling of the lower limb(s) ensues.
When axillary lymph nodes are involved, swelling of the upper limb(s) results.
Involvement of the breast can also occur in women.
Pitting edema is present early, but with more chronic inflammation, brawny edema and hardening of the tissues develops, eventually resulting in hyperpigmentation and hyperkeratosis.
When lymphedema is severe, it is often referred to as elephantiasis.

Worms within Lymph Vessel

Filarial fever
Another clinical syndrome is known as filarial fever. This is characterized by acute, self-limiting episodes of fever, often in the absence of any obvious lymphangitis or lymphadenopathy.
Because of the lack of associated features, this syndrome is frequently confused with other causes of fever in the tropics, such as malaria.

Tropical pulmonary eosinophilia
Tropical pulmonary
eosinophilia is characterized
by nocturnal wheezing.
It is caused by an immune
hyperresponsiveness to
microfilariae trapped in the
lungs and is typically seen
in young males.

Chronic Lymphedema

DIAGNOSIS
Nonspecific test abnormalities – Eosinophilia up to 3000/microL
Blood examination for detection of microfilariae should be performed in all individuals in whom the diagnosis of filariasis is suspected. Bancroftian and Brugian filariasistend to show nocturnal periodicity. Blood should be drawn between 10 p.m. and 2 a.m. because the greatest number of microfilariae can be found in blood during this peak biting time of the mosquito vectors. The pattern of periodicity can be reversed by changing the patient's sleep-wake cycle.
Antibody tests — Serologic tests for filarial antibodies which detect elevated levels of IgG and IgE are available


TREATMENT
Diethylcarbamazine — DEC with or without corticosteroieds.
Ivermectin — Studies have established that ivermectingiven as a single dose in Bancroftian filariasis reduces microfilaremia by approximately 90 percent even one year after treatment
Albendazole — has also been used in filarial infections. Prolonged courses of high dose albendazole have a significant macrofilaricidal effect and result in a gradual decrease in microfilarial levels.
Doxycycline — Initial studies suggested that doxycycline, which has good activity against filaria spp, leads to sterility of adult worms