Embed Size (px)
Citation preview
1
PowerPoint Slides English Spanish Translation
“Hereditary Breast and Ovarian Cancer Syndrome: Management of Ovarian Cancer Risk” Video Transcript
“Síndrome de cáncer hereditario de mama y ovario: Manejo del riesgo de cáncer de ovario” Transcripción del video
Professional Oncology Education Hereditary Breast and Ovarian Cancer Series Time: 36.01
Educación Oncológica Profesional Serie sobre cáncer hereditario de mama y ovario Duración: 36.01
Karen H.Lu, M.D. Professor Gynecologic Oncology Co-Medical Director, Clinical Cancer Genetics The University of Texas MD Anderson Cancer Center
Dra. Karen H. Lu Profesora Oncología Ginecológica Codirectora Médica, Genética Clínica del Cáncer MD Anderson Cancer Center de la Universidad de Texas
My name is Dr. Karen Lu and I am a Professor of Gynecologic Oncology at the University of Texas MD Anderson Cancer Center. I also serve as Co-Medical Director for Clinical Cancer Genetics. I’m going to be giving a talk on Hereditary Breast and Ovarian Cancer Syndrome: Management of Ovarian Cancer Risk.
Soy la Dra. Karen Lu, profesora de oncología ginecológica en el MD Anderson Cancer Center de la Universidad de Texas. También soy Codirectora Médica de Genética Clínica del Cáncer. Hoy hablaré del síndrome de cáncer hereditario de mama y ovario: Manejo del riesgo de cáncer de ovario.

2
The goals today are to discuss the management of patients’ ovarian cancer risk associated with BRCA mutations. We’ll also discuss with patients the risks, benefits, and limitations of ovarian cancer screening. Finally, we’ll gain knowledge about ovarian cancer prevention, including the use of oral contraceptives as a chemoprevention agent, and also the role of prophylactic bilateral salpingo-oophorectomy surgery in the prevention of ovarian cancer in women at high risk for the disease.
Nuestros objetivos son describir el manejo de los riesgos de cáncer de ovario asociados con mutaciones de genes BRCA, aprender cómo explicar a las pacientes los riesgos, beneficios y limitaciones de los exámenes de detección, y adquirir conocimientos sobre la prevención del cáncer de ovario, como anticonceptivos orales para quimioprevención, y la función de la salpingo-ooforectomía bilateral profiláctica en las mujeres con alto riesgo de adquirir la enfermedad.
Ovarian cancer is the number one cause of death amongst all gynecologic cancers. It is the second most common gynecologic cancer behind uterine cancer. In women at general population risk, the lifetime risk is 1.7 percent. Unfortunately, 70 percent of cases of ovarian cancer are detected in late stages when cure is less than 10 percent.
El cáncer de ovario es la primera causa de muerte entre los cánceres ginecológicos y es el segundo cáncer ginecológico después del uterino. En la población general, el riesgo de por vida es del 1.7%. El 70% de los casos se detectan en etapas tardías, cuando la cura es menor al 10%.

3
This slide highlights the difference in ovarian cancer risk between those individuals at general population risk and those women who have BRCA1 and BRCA2 mutations. In women at general population risk --- in women in the general population, ovarian cancer risk is about 1.7 percent. But as you can see here, individuals who have a BRCA1 mutation can have up to a 40 to 50 percent lifetime risk of ovarian cancer. For BRCA2 mutation carriers, their lifetime risk for ovarian cancer can be anywhere between 15 to 20 percent.
Aquí vemos la diferencia en el riesgo de cáncer de ovario entre la población general y las mujeres con mutaciones BRCA1 y 2. En la población general, el riesgo es del 1.7%, pero en las mujeres con mutación BRCA1, el riesgo de por vida puede ser de hasta un 40% o 50%. Para las portadoras de la mutación BRCA2, el riesgo de por vida de cáncer de ovario varía del 15% al 20%.
In the general U.S. population BRCA mutations occur in about one in 500 individuals. So we consider this not common nor is it rare. In certain populations there are founder mutations that result in a higher frequency of BRCA1 and BRCA2 mutations. For example, in the Ashkenazi Jewish population, BRCA1 and BRCA2 founder mutations occur in about one in 30 individuals.
En la población general de los Estados Unidos, estas mutaciones ocurren en 1 de cada 500 personas. No es común, pero tampoco infrecuente. En algunas poblaciones existen mutaciones fundadoras que aumentan la frecuencia de las mutaciones BRCA1 y BRCA2. Por ejemplo, en la población judía asquenazí, las mutaciones fundadoras ocurren en casi 1 de cada 30 individuos.

4
This is an example of a pedigree that demonstrates a family that has a substantial number of women that had both breast and ovarian cancer. As you can see, the circles in red represent women who were diagnosed with breast cancer. The grandmother was diagnosed with breast cancer at the age of 52, one daughter had breast cancer at the age of 49, and a granddaughter had breast cancer at the age of 37. The other daughter of the --- the woman with breast cancer had ovarian cancer at the age of 49. So if your patient was a woman who was age 24 who was unaffected with cancer, what would you tell her in terms of her risk for ovarian and breast cancer? Clearly, when you look at her family history she is at substantially increased risk.
Este es un ejemplo de un árbol genealógico que muestra a una familia con una gran proporción de mujeres que tuvieron cáncer de mama y ovario. Los círculos en rojo representan las mujeres diagnosticadas con cáncer de mama. La abuela fue diagnosticada con este cáncer a la edad de 52 años, una hija lo tuvo a los 49, y una nieta, a los 37 años. La otra hija de la mujer con cáncer de mama presentó cáncer de ovario a los 49 años. Si su paciente fuese una mujer de 24 años no afectada por cáncer, ¿qué le diría en términos de su riesgo de cáncer de ovario y mama? Es evidente que, según sus antecedentes familiares, tiene un riesgo sustancialmente mayor.
What I want to emphasize today is that genetic testing can really help us to determine in these unaffected individuals what their true risk for breast and ovarian cancer is. So if I go back to the prior slide, you can see that there is a substantial number of family members that have breast and ovarian cancer. So in the 19 --- early 1990s or before that time, we would have had to tell the unaffected young woman that she was at substantially increased risk for breast and ovarian cancer. However, since we’ve had clinical genetic testing for BRCA1 and BRCA2 available to us, it allows us to be much more precise with the unaffected daughters and granddaughters. Genetic testing can be extremely powerful. It allows us to say to that individual, “You have inherited the mutation that your mother and grandmother had and your risk for ovarian cancer may be as high as 40 percent.” And it also allows us
Lo que quiero destacar es que las pruebas genéticas pueden ayudarnos a determinar, en las personas no afectadas, cuál es su verdadero riesgo de cáncer de mama y ovario. En la diapositiva anterior vimos que hay una alta proporción de miembros de la familia con cáncer de mama u ovario. Hasta comienzos de la década de 1990, hubiéramos informado a la joven no afectada que tenía un riesgo sustancialmente mayor de estos cánceres; sin embargo, ahora disponemos de pruebas clínicas genéticas de BRCA1 y BRCA2, y podemos ser mucho más precisos en el caso de hijas y nietas no afectadas. Las pruebas genéticas suelen ser muy útiles y nos permiten afirmar “Usted ha heredado la mutación de su madre y su abuela, y su riesgo de cáncer de ovario puede ser de hasta un 40%”. También nos permiten decirle qué puede hacer para reducirlo.
5
to tell that daughter what can be done to reduce that risk. We’ll review today what the risk-producing strategies are that allow us to prevent cancer in these individuals that test positive. And I want to remind you that genetic testing is most informative when it’s performed on a cancer patient first. So we want the testing initially to be done on either the mother with breast cancer or the grandmother who had breast cancer. Once the specific mutation is found, then the daughter can be tested just for that specific mutation and she has a 50-50 chance of testing positive or testing negative. So again, if she tests negative, much of this information and much of the fear and anxiety around being at increased risk for cancer can be --- can be lessened.
Luego veremos las estrategias de reducción de riesgos para prevenir el cáncer en las personas con resultados positivos. Las pruebas genéticas son más informativas si se realizan primero en un paciente con cáncer. Por lo tanto, la prueba inicial debe hacerse en la madre o la abuela, que tienen cáncer de mama. Una vez localizada la mutación específica, la hija puede hacerse una prueba para detectarla, con la misma probabilidad de un resultado positivo o negativo. Si el resultado es negativo, la información permite mitigar gran parte del temor y ansiedad en torno a un mayor riesgo de cáncer.
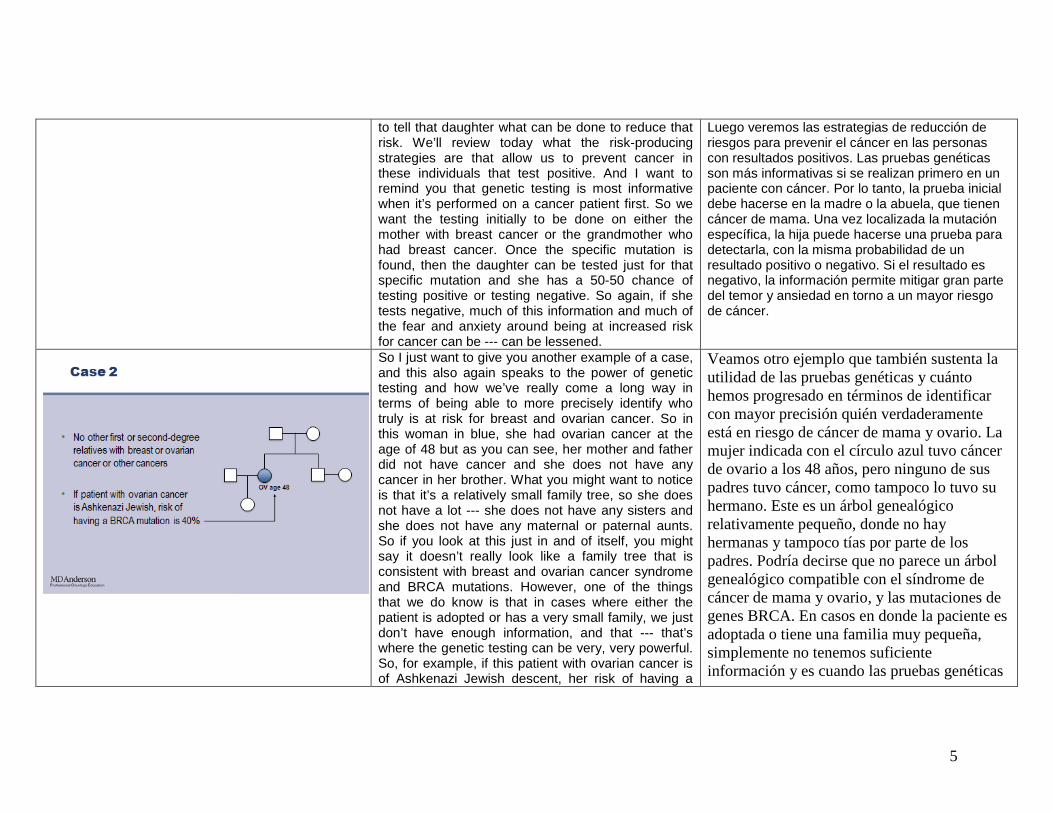
So I just want to give you another example of a case, and this also again speaks to the power of genetic testing and how we’ve really come a long way in terms of being able to more precisely identify who truly is at risk for breast and ovarian cancer. So in this woman in blue, she had ovarian cancer at the age of 48 but as you can see, her mother and father did not have cancer and she does not have any cancer in her brother. What you might want to notice is that it’s a relatively small family tree, so she does not have a lot --- she does not have any sisters and she does not have any maternal or paternal aunts. So if you look at this just in and of itself, you might say it doesn’t really look like a family tree that is consistent with breast and ovarian cancer syndrome and BRCA mutations. However, one of the things that we do know is that in cases where either the patient is adopted or has a very small family, we just don’t have enough information, and that --- that’s where the genetic testing can be very, very powerful. So, for example, if this patient with ovarian cancer is of Ashkenazi Jewish descent, her risk of having a
Veamos otro ejemplo que también sustenta la utilidad de las pruebas genéticas y cuánto hemos progresado en términos de identificar con mayor precisión quién verdaderamente está en riesgo de cáncer de mama y ovario. La mujer indicada con el círculo azul tuvo cáncer de ovario a los 48 años, pero ninguno de sus padres tuvo cáncer, como tampoco lo tuvo su hermano. Este es un árbol genealógico relativamente pequeño, donde no hay hermanas y tampoco tías por parte de los padres. Podría decirse que no parece un árbol genealógico compatible con el síndrome de cáncer de mama y ovario, y las mutaciones de genes BRCA. En casos en donde la paciente es adoptada o tiene una familia muy pequeña, simplemente no tenemos suficiente información y es cuando las pruebas genéticas

6
BRCA mutation, rather then being 10 percent, which is the --- the prevalence of BRCA mutations in ovarian cancer, it can be as high as 40 percent. So this is someone clearly that we would want to test for the BRCA mutation.
pueden ser muy útiles. Por ejemplo, si la paciente con cáncer de ovario es de ascendencia judía asquenazí, el riesgo de mutación de genes BRCA, en lugar de ser del 10%, que es la prevalencia de estas mutaciones, puede ser de hasta el 40%. Este es un caso en el que claramente deberíamos buscar la mutación BRCA.
And this is just a summary table that --- that discusses ethnicity in BRCA1 and BRCA2 mutations. So again, the prevalence in the general population is about one in 500 or about 0.2 percent. But again, in certain populations that have been isolated some time throughout their history and there are founder mutations that have been found in Icelandic populations, French Canadians, Ashkenazi Jewish, any --- any group that at some point has been isolated, they may have founder mutations. So there’s three founder mutations in the Ashkenazi Jewish population which is relevant to those of us who care for patients in the U.S. Two in BRCA1 and BRCA2, and the carrier frequency when you add up these three specific mutations is about 2 to 3 percent. So rather than 0.2 percent in the general population, it’s 2 to 3 percent.
En esta diapositiva se resume la etnicidad en las mutaciones de los genes BRCA1 y 2. La prevalencia en la población general es de aproximadamente 1 en 500, un 0.2%. En ciertas poblaciones que han permanecido aisladas a lo largo de su historia puede haber mutaciones fundadoras, como las que se han encontrado en poblaciones de Islandia, franco-canadienses, judíos asquenazí y otros grupos aislados. En la población judía asquenazí hay tres mutaciones fundadoras relevantes para el cuidado de pacientes en los Estados Unidos: dos en genes BRCA1 y una en genes BRCA2. La frecuencia total de portadoras es del 2% al 3%, en contraposición a la población general, que es inferior al 0.2%.
7
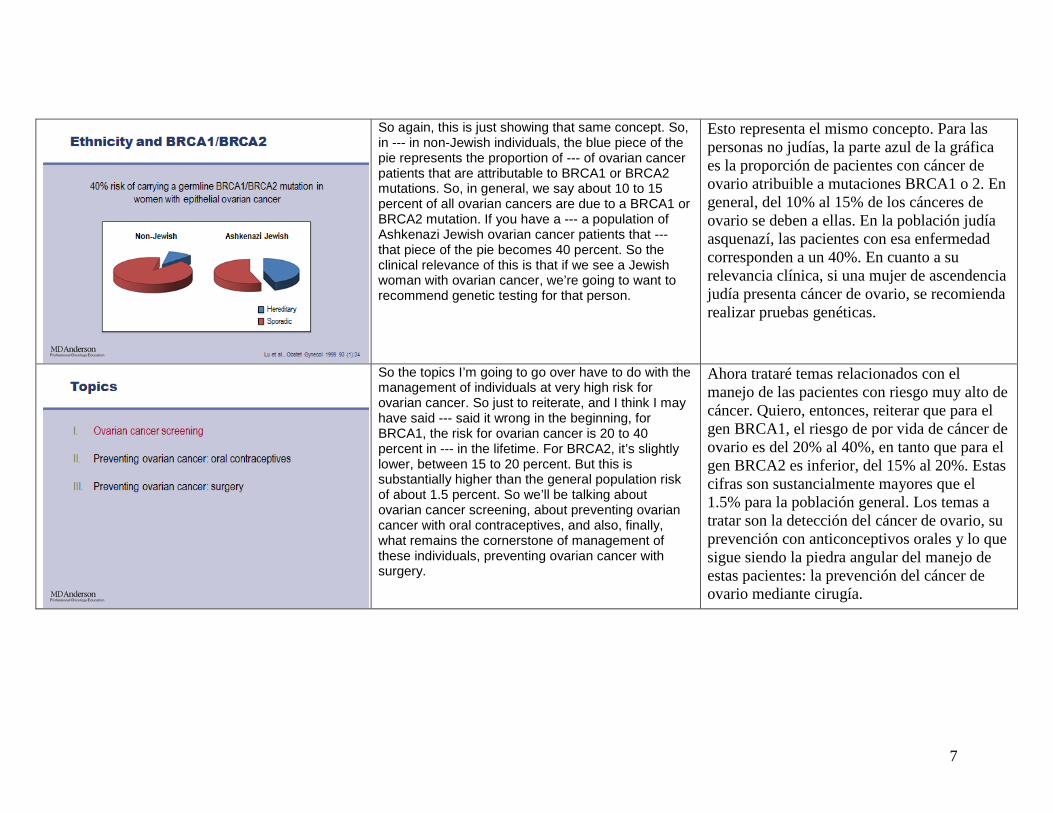
So again, this is just showing that same concept. So, in --- in non-Jewish individuals, the blue piece of the pie represents the proportion of --- of ovarian cancer patients that are attributable to BRCA1 or BRCA2 mutations. So, in general, we say about 10 to 15 percent of all ovarian cancers are due to a BRCA1 or BRCA2 mutation. If you have a --- a population of Ashkenazi Jewish ovarian cancer patients that --- that piece of the pie becomes 40 percent. So the clinical relevance of this is that if we see a Jewish woman with ovarian cancer, we’re going to want to recommend genetic testing for that person.
Esto representa el mismo concepto. Para las personas no judías, la parte azul de la gráfica es la proporción de pacientes con cáncer de ovario atribuible a mutaciones BRCA1 o 2. En general, del 10% al 15% de los cánceres de ovario se deben a ellas. En la población judía asquenazí, las pacientes con esa enfermedad corresponden a un 40%. En cuanto a su relevancia clínica, si una mujer de ascendencia judía presenta cáncer de ovario, se recomienda realizar pruebas genéticas.
So the topics I’m going to go over have to do with the management of individuals at very high risk for ovarian cancer. So just to reiterate, and I think I may have said --- said it wrong in the beginning, for BRCA1, the risk for ovarian cancer is 20 to 40 percent in --- in the lifetime. For BRCA2, it’s slightly lower, between 15 to 20 percent. But this is substantially higher than the general population risk of about 1.5 percent. So we’ll be talking about ovarian cancer screening, about preventing ovarian cancer with oral contraceptives, and also, finally, what remains the cornerstone of management of these individuals, preventing ovarian cancer with surgery.
Ahora trataré temas relacionados con el manejo de las pacientes con riesgo muy alto de cáncer. Quiero, entonces, reiterar que para el gen BRCA1, el riesgo de por vida de cáncer de ovario es del 20% al 40%, en tanto que para el gen BRCA2 es inferior, del 15% al 20%. Estas cifras son sustancialmente mayores que el 1.5% para la población general. Los temas a tratar son la detección del cáncer de ovario, su prevención con anticonceptivos orales y lo que sigue siendo la piedra angular del manejo de estas pacientes: la prevención del cáncer de ovario mediante cirugía.
8
So I’m going to start with this question: Ovarian cancer screening is effective, true or false? So the answer is false. There’ve never been any studies that have proven that ovarian cancer screening in women who are at very high risk for the disease can decrease mortality from that disease. So it’s very important for individuals who you see who have a BRCA1 or 2 mutation to not get falsely reassured that ovarian cancer screening is effective.
Comencemos con una pregunta: Los exámenes de detección del cáncer de ovario son eficaces. ¿Verdadero o falso? La respuesta es “falso”. Ningún estudio ha demostrado que los exámenes de detección de cáncer de ovario en las mujeres de alto riesgo reduzcan la mortalidad por esa enfermedad. Es muy importante que las pacientes con mutación BRCA1 o 2 no perciban erróneamente que los exámenes de detección son eficaces.
And, again, this is just, really we talk about a lifetime management stra --- strategy for these individuals and that includes three different arms – screening, chemoprevention, and preventive surgery.
Por eso nos referimos a una estrategia de manejo de por vida de estas pacientes, la cual incluye tres aspectos: detección, quimioprevención y cirugía preventiva.
9
So let’s jump right into screening. So the problem with really getting enough data to say whether it’s effective or not is that the vast majority of studies have been retrospective studies. So the inclusion criteria has been different, so some of the individuals have been high-risk just based on family history. Some of --- of the studies have been exclusively in individuals who have BRCA mutations. The screening protocols vary. So some studies have looked at annual screening with CA-125 and transvaginal ultrasound. Other screening --- other institutions have looked at doing these modalities every six months. And finally, in the reporting of the studies, oftentimes it’s un --- unclear whether they’re reporting incident cases, so cases that developed while the patient was getting screened. Or prevalent cases, which is at the very first time that they presented, they were diagnosed with cancer. So we don’t have really good data to help us, but the --- there’re general conclusions that can be made. The first general conclusion is that interval ovarian cancers can develop in individuals that are being screened, certainly that are being screened on a yearly basis. And so that’s why several years ago the recommendations really moved towards if you’re going to screen, to screen every six months. But even looking at every six months, sometimes interval cancers can develop. And those interval cancers may not be early stage; so that’s been disappointing. The second conclusion is that when you do screening protocols, oftentimes the cancers that you’re picking up are non-epithelial cancers or low malignant potential, not really the invasive ovarian cancers that are the ones that we worry about more. And finally, one of the general conclusions is that among the invasive cancers that are picked up, still less than half of them
Comencemos con la detección. El problema de no contar con datos suficientes para afirmar si es eficaz surge del hecho de que la gran mayoría de los estudios han sido retrospectivos. Los criterios de inclusión han diferido y algunas participantes se consideraron de alto riesgo por sus antecedentes familiares. En otros estudios solo participaron personas con mutaciones BRCA. Los protocolos de detección también varían. En algunos casos se consideraron exámenes anuales del antígeno CA-125 y ecografías transvaginales. En otros, estos exámenes se realizaron cada seis meses. Por último, al presentar los resultados, a veces no está claro si se están informando casos incidentes que ocurrieron mientras la paciente estaba bajo control, o casos prevalecientes, diagnosticados como cáncer cuando la paciente se presentó por primera vez. Entonces no tenemos datos realmente útiles, pero sí podemos extraer conclusiones. La primera es que el cáncer ovárico de intervalo puede desarrollarse en personas bajo control, aunque se hagan exámenes anuales. Por eso, desde hace varios años se recomienda que los exámenes de detección se hagan cada seis meses, aunque aun así pueden ocurrir cánceres de intervalo que tal vez no se detecten en una etapa incipiente. Esto ha sido decepcionante. La segunda conclusión es que al seguir protocolos de detección, los cánceres detectados son de tipo no epitelial o de bajo potencial maligno y no cánceres de ovario invasivos, que son los que más nos preocupan. Por último, otra conclusión general es que entre los cánceres invasivos que sí se detectan, casi la mitad están en una etapa tardía. Sería deseable que pudiésemos identificar muchos más cánceres en su etapa incipiente y, desde luego, los estudios retrospectivos no lo han logrado.

10
--- are lat --- are late stage. So you know, we want to move towards where --- where we’re identifying many, many more early stage cancers and certainly from the retrospective studies we’re not finding that.
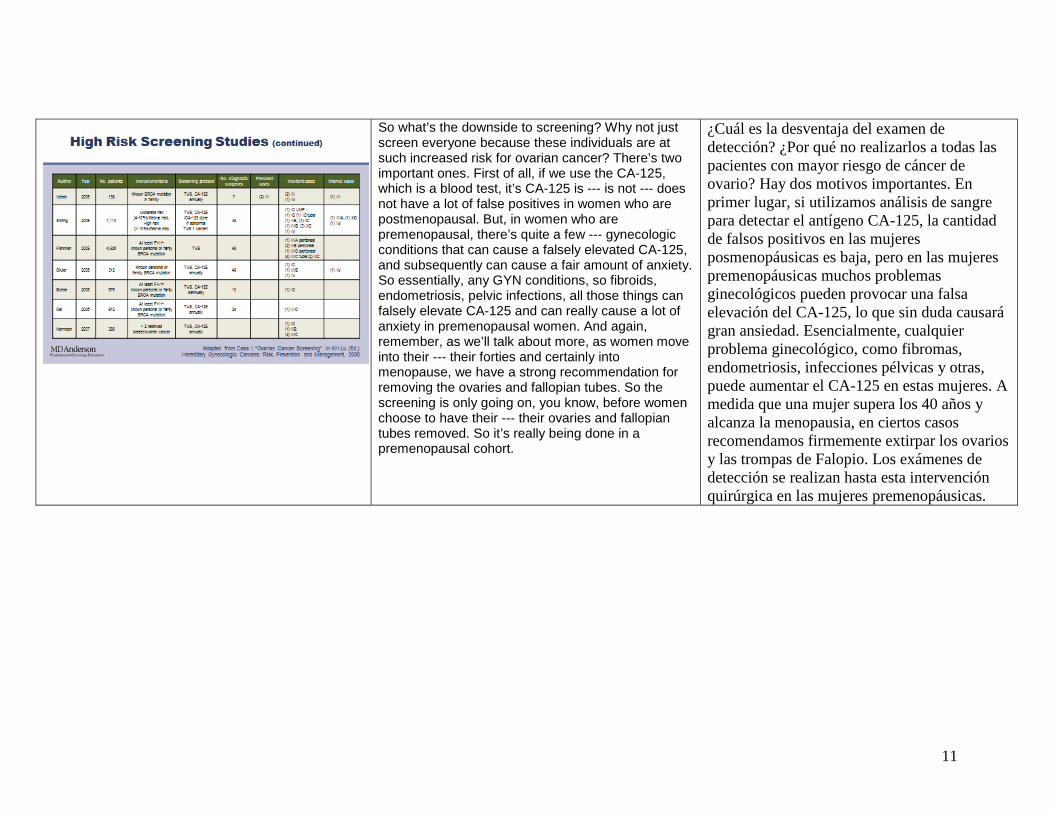
This is difficult to read but I just wanted to give you a sense that there have been quite a few studies that have looked at ovarian cancer screening in high-risk individuals and I just provide this to you so that if you’re interested, you can go back and look. This is a table of studies that include the year that it was published, the number of patients that were screened, the inclusion criteria, what the screening protocol was, whether it was annual or every six months, and how many prevalent cases, how many incident cases, and and then how many inter --- interval cases. And I think as you scroll through these, what you’ll see is that, you’ll see that what we’re looking for is, we’re looking for early stage incident cases. And when you scroll through the results here, you’ll see that in many cases, the incident cases are unfortunately Stage III or Stage IV.
Esta tabla no es fácil de interpretar. Solamente quiero mencionar que varios estudios han analizado la detección del cáncer de ovario en las mujeres de alto riesgo. Si esto es de su interés, puede referirse a la tabla en otro momento. Los datos son: autor, año de publicación, número de participantes, criterios de inclusión, protocolo utilizado, frecuencia de los exámenes, número de cirugías de diagnóstico, casos prevalecientes, casos incidentes y casos de intervalo. Entre estos datos, tal vez lo más relevante para nosotros sean los casos incidentes en etapa incipiente. Desafortunadamente, muchos de los casos incidentes fueron de estadio III o IV.
11
So what’s the downside to screening? Why not just screen everyone because these individuals are at such increased risk for ovarian cancer? There’s two important ones. First of all, if we use the CA-125, which is a blood test, it’s CA-125 is --- is not --- does not have a lot of false positives in women who are postmenopausal. But, in women who are premenopausal, there’s quite a few --- gynecologic conditions that can cause a falsely elevated CA-125, and subsequently can cause a fair amount of anxiety. So essentially, any GYN conditions, so fibroids, endometriosis, pelvic infections, all those things can falsely elevate CA-125 and can really cause a lot of anxiety in premenopausal women. And again, remember, as we’ll talk about more, as women move into their --- their forties and certainly into menopause, we have a strong recommendation for removing the ovaries and fallopian tubes. So the screening is only going on, you know, before women choose to have their --- their ovaries and fallopian tubes removed. So it’s really being done in a premenopausal cohort.
¿Cuál es la desventaja del examen de detección? ¿Por qué no realizarlos a todas las pacientes con mayor riesgo de cáncer de ovario? Hay dos motivos importantes. En primer lugar, si utilizamos análisis de sangre para detectar el antígeno CA-125, la cantidad de falsos positivos en las mujeres posmenopáusicas es baja, pero en las mujeres premenopáusicas muchos problemas ginecológicos pueden provocar una falsa elevación del CA-125, lo que sin duda causará gran ansiedad. Esencialmente, cualquier problema ginecológico, como fibromas, endometriosis, infecciones pélvicas y otras, puede aumentar el CA-125 en estas mujeres. A medida que una mujer supera los 40 años y alcanza la menopausia, en ciertos casos recomendamos firmemente extirpar los ovarios y las trompas de Falopio. Los exámenes de detección se realizan hasta esta intervención quirúrgica en las mujeres premenopáusicas.
12
The second downside is that for a transvaginal ultrasound, which is our other modality that we use, there really is quite a high false positive rate. So premenopausal women, they ovulate, cysts form which --- which is normal in the ovaries, and again, when we’re doing these transvaginal ultrasounds, we see that. And again, they can cause a fair number of follow up need to --- to look again with a transvaginal ultrasound after a few weeks just to reassure us that in fact, it’s not --- it’s a physiologic cyst and not a cancer.
La segunda desventaja es que, con la ecografía transvaginal, la otra modalidad utilizada, también hay un alto porcentaje de falsos positivos. Cuando una mujer premenopáusica ovula, se forman quistes en los ovarios, lo que es normal. Esto es detectado durante la ecografía y puede requerir un seguimiento de varias visitas para repetir la ecografía al cabo de unas semanas a fin de comprobar si se trata de un quiste fisiológico o un cáncer.
So what I really want to stress here is the importance of prospective studies. There is a growing cohort of women who have been identified in their twenties and early thirties as having a BRCA1 or BRCA2 mutation, very high risk for ovarian cancer. You know, we really owe it to them to do good prospective studies that have consistent inclusion criteria, consistent screening protocol, and --- so that we can tell them is this working or --- or not, and do we need to come up with newer strategies for ovarian cancer screening.
Lo que realmente quiero destacar es la importancia de los estudios prospectivos. Hay un creciente grupo de mujeres identificadas en sus 20 o 30 años con mutaciones BRCA1 o 2 y en muy alto riesgo de cáncer de ovario. Sería conveniente realizar buenos estudios prospectivos con criterios de inclusión uniformes y protocolos de detección coherentes para poder identificar qué métodos funcionan mejor e identificar nuevas estrategias para la detección del cáncer de ovario.

13
Just want to let you know that there’s currently two prospective ongoing trials, one being done in the United States with the Cancer Genetics Network and GOG-199. It’s evaluating CA-125 change over time using the ROCA, or Risk of Ovarian Cancer Algorithm. A second screening trial in a high-risk cohort is ongoing in the United Kingdom, also evaluating the same risk of ovarian cancer algorithm.
En este momento se están realizando dos ensayos clínicos: uno en los Estados Unidos a cargo de la Red de Genética del Cáncer, utilizando el protocolo GOG-199 que evalúa los cambios del CA-125 utilizando el algoritmo de riesgo de cáncer de ovario, o ROCA. El segundo ensayo de detección en grupos de alto riesgo se está llevando a cabo en el Reino Unido utilizando el mismo algoritmo.
And this is just the general idea, this pattern of women. This --- this --- these results are from postmenopausal women. But, the idea is the same, which is that each woman would establish their own baseline. So some would have a lower baseline, some have a higher baseline and as long as those values are all within the same general range, it’s unlikely to be cancer. But, once there’s a very sharp rise in the CA-125 that can be a sign that --- that cancer is --- is ongoing and the goal for these prospective studies is to determine when that happens and when an ultrasound and surgery is performed, does that result in us identifying more early stage cases. So we’ll have to wait for the results of those.
Esta gráfica brinda una idea general del patrón de resultados entre las mujeres posmenopáusicas. Se utilizó el concepto de que cada mujer definiría sus propios valores de referencia. Algunas partieron de un valor menor, otras de uno mayor, y en tanto esos valores permanezcan dentro del mismo rango, es poco probable que haya cáncer. Un gran aumento del CA-125 puede indicar el comienzo de un cáncer. La meta de estos estudios prospectivos es determinar cuándo sucede esto y establecer si una ecografía o una operación permiten identificar estos casos en etapas más precoces. Aún debemos esperar los resultados.

14
This is some very, very preliminary date --- data that was presented quite a few years ago. And in general, I think the important take home points is that these individuals are very, very compliant. They had compliance with really every three months, CA-125 testing and that was 80 --- 80 --- mid 80 --- 82 to 85 percent of women returned for those tests. We did not have --- have a high need to go on to ultrasounds. Only 10 percent of those --- those individuals that were screened had to go on for transvaginal ultrasound. I think that’s important. And ROCA did identify two incident cases and both of these were early stage. So we’ll have to wait a little bit longer for the results of this study.
Estos son datos muy preliminares que se publicaron hace unos años. Creo que, en general, lo más importante es que estas pacientes han seguido muy bien las pautas establecidas. Los estudios se realizaron cada tres meses para medir el CA-125, y del 82% al 85% de las pacientes regresaron para las pruebas. No hubo muchos casos que requiriesen ecografías. Solo el 10% de las pacientes examinadas debió hacerse una ecografía transvaginal. Esto es importante. El algoritmo ROCA identificó dos casos incidentes, ambos en etapa incipiente, pero aún debemos esperar para tener los resultados.
So let’s move on to preventing ovarian cancer through oral contraceptives.
Continuemos con la prevención del cáncer de ovario con anticonceptivos orales.

15
So the --- there has been a very, very large number of studies throughout a long period of time that have looked at the protection of ova --- of oral contraceptives in preventing ovarian cancer in the general population. And as this slide shows you that there’s a substantial decrease and consistent --- substantial and consistent decrease in risk of ovarian cancer if you take oral contraceptives.
Se han realizado numerosos estudios a lo largo de períodos prolongados para analizar la eficacia de los anticonceptivos orales a fin de prevenir el cáncer de ovario en la población general. Esta diapositiva muestra que hay una disminución sustancial y uniforme en el riesgo de cáncer de ovario si se toman anticonceptivos orales.
And when we perform studies specifically within individuals who have BRCA mutations, it is similar that there is a substantial decrease in risk if you take the oral contraceptive.
En los estudios específicos realizados en mujeres con mutaciones de genes BRCA también se observa una disminución sustancial en el riesgo al tomar anticonceptivos orales.

16
One of the things that is controversial and I think it is an important point for those of you who take care of these high-risk patients is that --- you can’t just be thinking about reducing their ovarian cancer risk because these individuals are at increased risk for both breast cancer and ovarian cancer. So you need to be thinking about, in whatever recommendation that you offer to these patients, you need to be thinking about both ovarian cancer risk as well as breast cancer risk. So one of the controversies is that, while oral contraceptives are associated with a decreased risk of ovarian cancer by 50 percent, so a very substantial decreased risk in ovarian cancer risk, they may be associated with a slight increase in breast cancer risk. So the data is not consistent. So there are some studies that show that there is no increase in risk in mutation carriers that take the current low-dose oral contraceptives. But there’re also been studies and these are all retrospective, that shows that there’s a slight increased risk of breast cancer in BRCA1 mutation carriers who use oral contraceptives. So I think that, in general, it’s --- it’s a --- it’s an area of controversy, I think, for individuals who --- who are using the oral contraceptive anyway for birth control, that you can tell them they will have a substantially decreased risk of ovarian cancer but that the data on breast cancer is --- is --- is currently unknown.
Una consideración que da lugar a discusión y que es importante para quienes atienden a pacientes de alto riesgo, es que no debemos pensar exclusivamente en reducir el riesgo de cáncer de ovario, porque estas pacientes también tienen un mayor riesgo de cáncer de mama. Cualquiera que sea la recomendación para estas pacientes, siempre debemos tener en cuenta el riesgo de cáncer de ovario y el riesgo de cáncer de mama. Si bien los anticonceptivos orales están asociados a una disminución del 50% en el riesgo de cáncer de ovario, lo cual es una cifra sustancial, también pueden estar asociados a un leve aumento en el riesgo de cáncer de mama. Los datos no son coherentes. Algunos estudios muestran que no hay un mayor riesgo en las portadoras de mutaciones que toman dosis bajas de anticonceptivos orales, mientras que otros estudios retrospectivos indican que existe un riesgo levemente mayor de cáncer de mama en las portadoras de mutaciones BRCA1 que toman anticonceptivos orales. Esta es, en general, un área de controversia. Si una paciente está tomando anticonceptivos orales para el control de la natalidad, se le debe informar que tiene un riesgo considerablemente menor de cáncer de ovario, pero que los datos sobre cáncer de mama aún se desconocen.
17
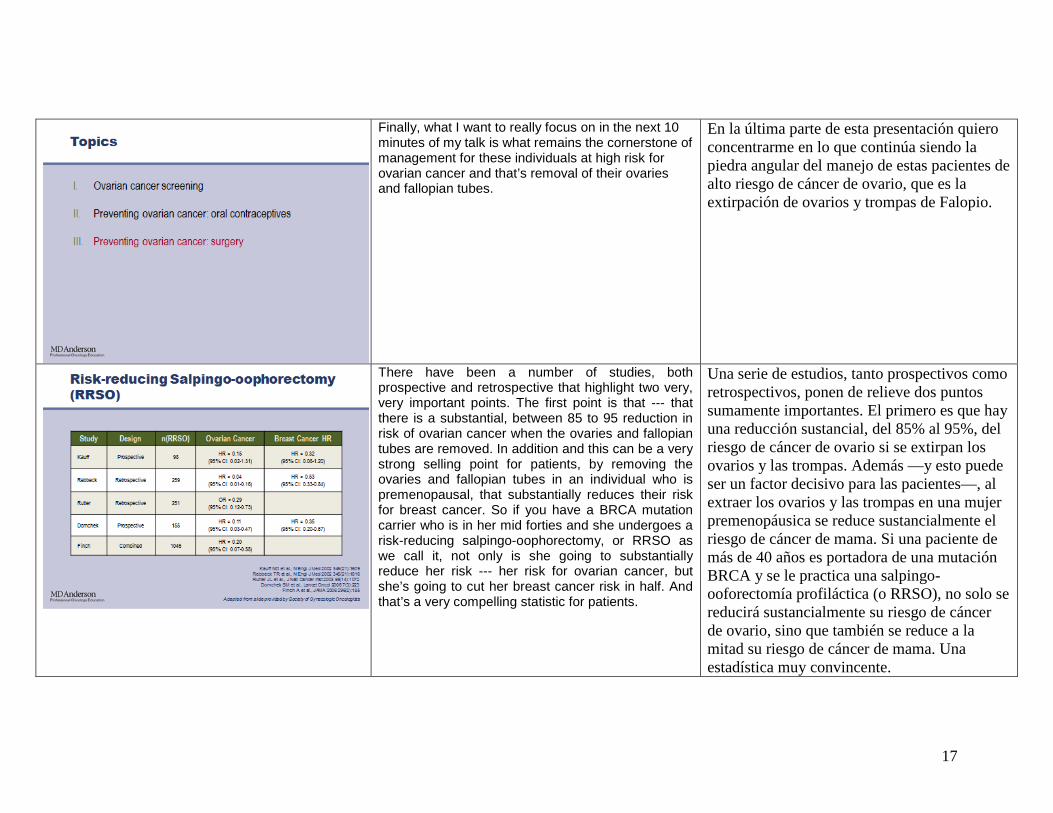
Finally, what I want to really focus on in the next 10 minutes of my talk is what remains the cornerstone of management for these individuals at high risk for ovarian cancer and that’s removal of their ovaries and fallopian tubes.
En la última parte de esta presentación quiero concentrarme en lo que continúa siendo la piedra angular del manejo de estas pacientes de alto riesgo de cáncer de ovario, que es la extirpación de ovarios y trompas de Falopio.
There have been a number of studies, both prospective and retrospective that highlight two very, very important points. The first point is that --- that there is a substantial, between 85 to 95 reduction in risk of ovarian cancer when the ovaries and fallopian tubes are removed. In addition and this can be a very strong selling point for patients, by removing the ovaries and fallopian tubes in an individual who is premenopausal, that substantially reduces their risk for breast cancer. So if you have a BRCA mutation carrier who is in her mid forties and she undergoes a risk-reducing salpingo-oophorectomy, or RRSO as we call it, not only is she going to substantially reduce her risk --- her risk for ovarian cancer, but she’s going to cut her breast cancer risk in half. And that’s a very compelling statistic for patients.
Una serie de estudios, tanto prospectivos como retrospectivos, ponen de relieve dos puntos sumamente importantes. El primero es que hay una reducción sustancial, del 85% al 95%, del riesgo de cáncer de ovario si se extirpan los ovarios y las trompas. Además —y esto puede ser un factor decisivo para las pacientes—, al extraer los ovarios y las trompas en una mujer premenopáusica se reduce sustancialmente el riesgo de cáncer de mama. Si una paciente de más de 40 años es portadora de una mutación BRCA y se le practica una salpingo-ooforectomía profiláctica (o RRSO), no solo se reducirá sustancialmente su riesgo de cáncer de ovario, sino que también se reduce a la mitad su riesgo de cáncer de mama. Una estadística muy convincente.
18
So what is our --- our protocol for risk-reducing salpingo-oophorectomy? Well, there’s a couple of things that I want to mention today. First of all, in the counseling session, to really let people that there are benefits not just for ovarian cancer but for breast cancer as well. We also want to do, when we do the consent form, we also want to --- to let them know that there’s always the possibility of actually having cancer found at the time of surgery. And so I will frequently consent them for definitive staging surgery if cancer is found, if gross cancer is found. The third point is that laparoscopic risk-reducing salpingo-oophorectomy is an excellent option rather than laparotomy. In a woman who is a candidate for laparoscopic surgery, you know, you get --- you are able to really see things clearly. You’re able to look at --- examine the upper abdomen as well as the pelvis. You’re able to do the full procedure and the recovery for patients is substantially improved. We like to let peop --- let surgeons know to biopsy any suspicious areas that they may see.
¿Cuál es el protocolo de una salpingo-ooforectomía profiláctica? Consiste en una serie de pasos que describiré a continuación. En primer lugar, en la sesión de asesoramiento, informar los beneficios en cuanto al cáncer de ovario y mama. Además, al entregarles el formulario de consentimiento debemos mencionar que existe la posibilidad de encontrar cáncer al momento de la cirugía. Con frecuencia, obtengo el consentimiento para cirugía de estadificación definitiva en caso de encontrar cáncer. Tercero, indicar que la salpingo-ooforectomía profiláctica por vía laparoscópica es una excelente alternativa a la laparotomía. Si una mujer es apta para la cirugía laparoscópica, el procedimiento permite evaluar claramente las condiciones. Es posible examinar el abdomen superior y la pelvis. Se puede realizar un procedimiento completo, la recuperación mejora sustancialmente y el cirujano puede hacer biopsias de cualquier área potencialmente cancerígena.
19
On key point that I’m going to show you --- I’m going to elaborate further on is, we want to do complete removal of both fallopian tubes and ovaries. So in the past the focus was really on the ovaries but I’m going to provide some --- some information ---that --- that shows that it may be the fallopian tubes that --- that --- where the cancer develops early on. And so, we want make sure to remove both the fallopian tubes and the ovaries. We want to make sure that we remove the entire ovary. So oftentimes we’ll want to remove some amount of margin from the ovary on the ovarian vessels. We want to remove all the fallopian tube that we can and we really want to --- if we’re going to perform a laparoscopic procedure, place the specimens in an endoscopic sac to avoid spillage. I like to do washings --- pelvic washings, abdominal washings. I do it as one together, just peritoneal cytology. There have been quite a few case reports of individuals with BRCA1 and BRCA2 mutations who undergo this procedure and turn out to have washings positive for cancer but no other cancer found in the specimen. And then again, in a few minutes, I’m going to talk about the importance, and this is a key point, pathologic microsectioning. So we take the entire ovary and the entire Fallopian tubes and we --- every 2 to 3 mm, we will section the sample and embed the entire sample and we often will find, not often, but about 5 to 8 percent of the time, we’ll find microscopic cancers that aren’t seen at the time of surgery but are seen at the time of pathology review.
Un aspecto importante que explicaré con más detalle es la extracción completa de ambas trompas y ambos ovarios. En el pasado, los médicos se centraban en los ovarios, pero algunos datos demuestran que el cáncer puede comenzar en las trompas de Falopio, por eso debemos asegurarnos de retirar tanto las trompas como los ovarios y de extirpar el ovario completo. Con frecuencia, en los vasos ováricos se retira el mismo margen que en el ovario. Deben retirarse las trompas en tu totalidad. Si se utiliza un procedimiento laparoscópico, las muestras deben colocarse en una bolsa endoscópica para evitar derrames. Usualmente hago lavados de la pelvis, lavados abdominales, en un mismo procedimiento de citología peritoneal. Se ha informado de casos con mutaciones BRCA1 y BRCA2 donde este procedimiento resulta en lavados positivos para cáncer, sin que se halle ningún cáncer en la muestra. Luego me referiré a un procedimiento clave, los microcortes transversales para análisis patológico. Retiramos todo el ovario y toda la trompa. Cada 2 a 3 mm, tomamos una muestra con corte transversal. En un 5% a un 8% de los casos se descubren cánceres microscópicos que no fueron detectados durante la cirugía, pero que se identifican en la revisión patológica.
20
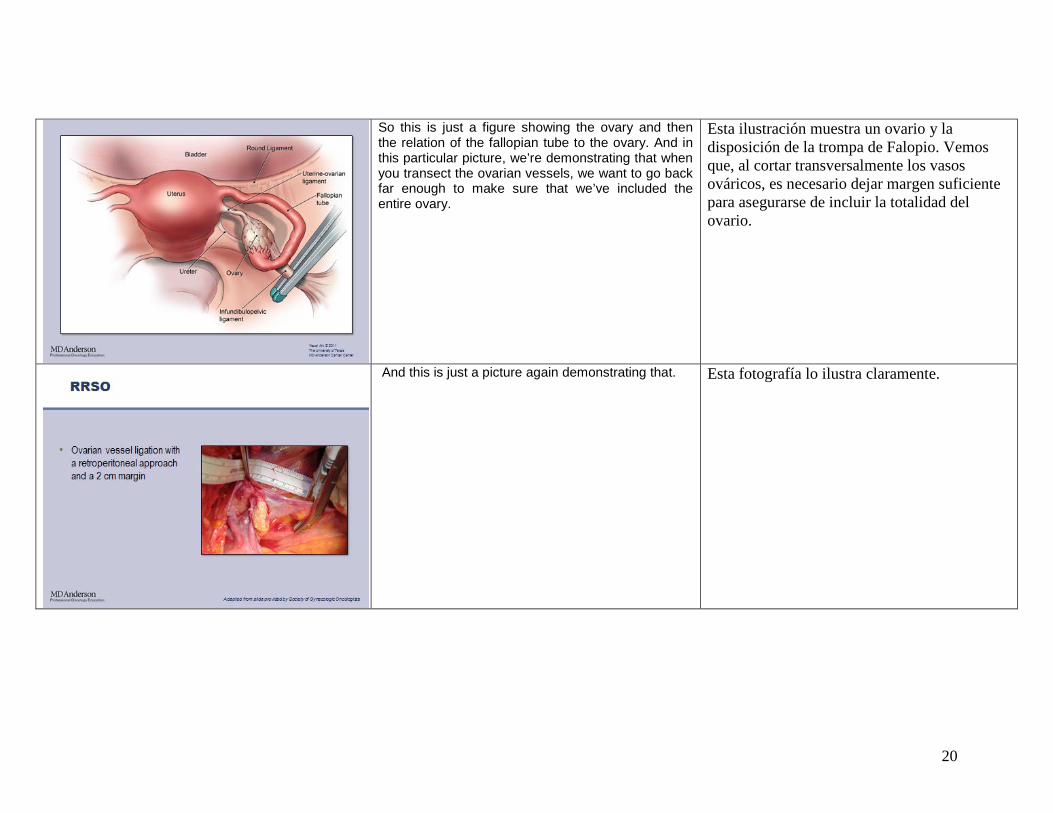
So this is just a figure showing the ovary and then the relation of the fallopian tube to the ovary. And in this particular picture, we’re demonstrating that when you transect the ovarian vessels, we want to go back far enough to make sure that we’ve included the entire ovary.
Esta ilustración muestra un ovario y la disposición de la trompa de Falopio. Vemos que, al cortar transversalmente los vasos ováricos, es necesario dejar margen suficiente para asegurarse de incluir la totalidad del ovario.
And this is just a picture again demonstrating that. Esta fotografía lo ilustra claramente.

21
We want to remove as much fallopian tube as possible. You know, I think that from a surgical standpoint, we --- we want to get right up to the cornua. It turns out that there have been literally thousands of risk-reducing salpingo-oophorectomy procedures performed in this very high risk population. And really we’ve had no case reports of individuals getting a fallopian tube cancer in the remaining residual part of the fallopian tube that inserts into the uterus. So I think, certainly, I take the message that it’s --- it’s likely that it’s the fimbrial portion of the fallopian tube that’s most at risk as well as the middle portion. So while you do want to be cautious to take as much fallopian tube as possible, we really haven’t seen any cancers that have developed in the residual portion.
Se debe retirar la trompa en su máxima medida posible. Desde el punto de vista quirúrgico, queremos llegar hasta el cuerno uterino. En esta población de muy alto riesgo hemos realizado miles de salpingo-ooforectomías profilácticas y no se han informado casos de cáncer de trompas de Falopio en la porción residual que se inserta en el útero. De esto deduzco que es probable que las partes que presentan el mayor riesgo sean la porción de las fimbrias de la trompa y su parte media. Tenemos la precaución de retirar las trompas en la mayor medida posible y no hemos visto ningún caso de cáncer que se haya desarrollado en la porción residual.
So here’s another question. Histologic processing of the ovaries and fallopian tubes in BRCA carriers is similar to women without a BRCA mutation undergoing bilateral salpingo-oophorectomy. True or False?
Veamos otra pregunta. El procesamiento histológico de los ovarios y las trompas en las portadoras de mutaciones BRCA es similar al de las no portadoras con salpingo-ooforectomía bilateral. ¿Verdadero o falso?

22
And the answer here is false and this is a very important point. For individuals who might be going to surgery, general population risk individuals who are going to surgery because they have symptomatic fibroids and they choose to have their ovaries removed as well, the pathology, the standard pathology review is to take a single representative section from the ovary --- from each ovary and each fallopian tube and then throw out the rest. And what we really have learned is that in these high-risk individuals, in individuals who are known to have BRCA1 and BRCA2 mutations, we need to look at the complete fallopian tube and the complete ovary and we do that by what’s called serial sectioning and embedding the entire specimen.
La respuesta es “falso” y esta es una cuestión muy importante. En las pacientes con el riesgo de la población general que se someten a cirugía debido a fibromas sintomáticos y optan por una extirpación de ovarios, la revisión patológica estándar solamente requiere tomar una única porción representativa de cada ovario y de cada trompa de Falopio. El resto se desecha. Sabemos ahora que en las pacientes de alto riesgo identificadas como portadoras de mutaciones en los genes BRCA1 y BRCA2 debemos analizar la totalidad de la trompa y todo el ovario. Esto se realiza mediante cortes transversales seriados, preservando la muestra completa.
And when we’ve looked for the prevalence of occult cancer in women with mutations, it’s about --- about a 4 to 8 percent, I usually quote about 5 to 8 percent risk of finding a microscopic cancer that’s not seen at the time of surgery, that’s not seen preoperatively, but really only found at the time of pathologic review. And this has been a very consistent story.
La prevalencia del cáncer oculto en las mujeres con estas mutaciones es del 4% al 8%, aunque el riesgo de detectar un cáncer microscópico no percibido ni antes ni durante la cirugía y que solo se descubre durante la revisión patológica es de un 5% a un 8%. Estas cifras han sido muy consistentes.
23
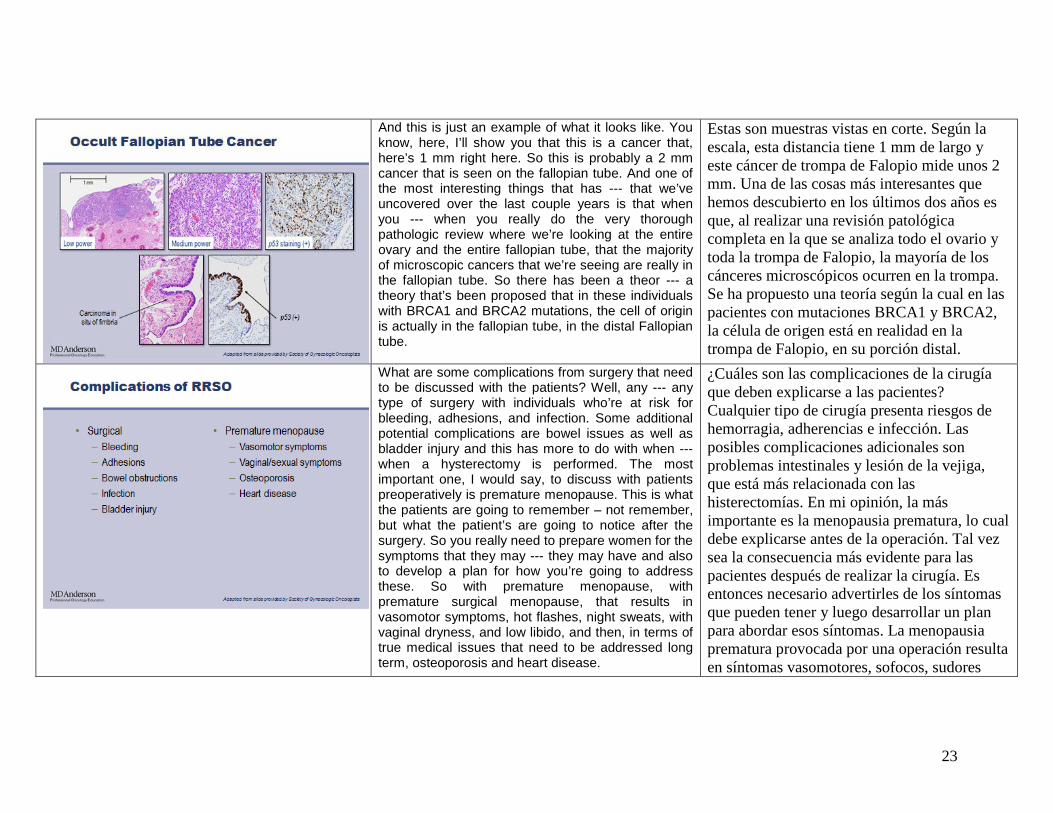
And this is just an example of what it looks like. You know, here, I’ll show you that this is a cancer that, here’s 1 mm right here. So this is probably a 2 mm cancer that is seen on the fallopian tube. And one of the most interesting things that has --- that we’ve uncovered over the last couple years is that when you --- when you really do the very thorough pathologic review where we’re looking at the entire ovary and the entire fallopian tube, that the majority of microscopic cancers that we’re seeing are really in the fallopian tube. So there has been a theor --- a theory that’s been proposed that in these individuals with BRCA1 and BRCA2 mutations, the cell of origin is actually in the fallopian tube, in the distal Fallopian tube.
Estas son muestras vistas en corte. Según la escala, esta distancia tiene 1 mm de largo y este cáncer de trompa de Falopio mide unos 2 mm. Una de las cosas más interesantes que hemos descubierto en los últimos dos años es que, al realizar una revisión patológica completa en la que se analiza todo el ovario y toda la trompa de Falopio, la mayoría de los cánceres microscópicos ocurren en la trompa. Se ha propuesto una teoría según la cual en las pacientes con mutaciones BRCA1 y BRCA2, la célula de origen está en realidad en la trompa de Falopio, en su porción distal.
What are some complications from surgery that need to be discussed with the patients? Well, any --- any type of surgery with individuals who’re at risk for bleeding, adhesions, and infection. Some additional potential complications are bowel issues as well as bladder injury and this has more to do with when --- when a hysterectomy is performed. The most important one, I would say, to discuss with patients preoperatively is premature menopause. This is what the patients are going to remember – not remember, but what the patient’s are going to notice after the surgery. So you really need to prepare women for the symptoms that they may --- they may have and also to develop a plan for how you’re going to address these. So with premature menopause, with premature surgical menopause, that results in vasomotor symptoms, hot flashes, night sweats, with vaginal dryness, and low libido, and then, in terms of true medical issues that need to be addressed long term, osteoporosis and heart disease.
¿Cuáles son las complicaciones de la cirugía que deben explicarse a las pacientes? Cualquier tipo de cirugía presenta riesgos de hemorragia, adherencias e infección. Las posibles complicaciones adicionales son problemas intestinales y lesión de la vejiga, que está más relacionada con las histerectomías. En mi opinión, la más importante es la menopausia prematura, lo cual debe explicarse antes de la operación. Tal vez sea la consecuencia más evidente para las pacientes después de realizar la cirugía. Es entonces necesario advertirles de los síntomas que pueden tener y luego desarrollar un plan para abordar esos síntomas. La menopausia prematura provocada por una operación resulta en síntomas vasomotores, sofocos, sudores
24
nocturnos, sequedad vaginal y disminución de la libido. Los problemas médicos que deberán ser tratados a largo plazo son la osteoporosis y la enfermedad cardíaca.
One of the questions that I frequently get –get asked is, does risk-reducing salpingo-oophorectomy need to include hysterectomy? And the bottom line answer from my standpoint is no, it does not. Really, removing the tubes and ovaries addressed the prevention of cancer aspect that we’re getting at. It --- I think that --- that there are certain circumstances where I think that it’s a reasonable thing to include, and I’m going to talk about those now. It simplifies hormonal management and this is where, you know, talking about quality of life and what the plan is for management of menopausal symptoms is important. So in premenopausal women who do not have breast cancer, you know, you need to be discussing hormone replacement for the management of menopausal symptoms. And if their uterus is retained then we’re going to recommend that the hormonal replacement is both with estrogen and progesterone to protect the uterus. If the uterus is removed we can use estrogen alone. There’s been some concern that the progesterone may have a negative effect on breast tissue, so I think that while there’s not an overwhelming amount of evidence, it certainly is something that needs to be discussed with the patient. Another reason to consider taking out the uterus is in individuals who have taken tamoxifen. There’s a two to threefold increased risk of uterine cancer with tamoxifen. So in an individual who has used tamoxifen, I think that this can be a reason to consider a hysterectomy. And then certainly, if someone has a history of abnormal PAP smears or has very symptomatic fibroids that
Una pregunta muy frecuente es si la salpingo-ooforectomía profiláctica debe incluir una histerectomía. Desde mi punto de vista, la respuesta es no. La extracción de trompas y ovarios resuelve la prevención del cáncer, que era el objetivo inicial. En ciertas circunstancias puede ser razonable incluirla y las describiré a continuación. La histerectomía simplifica el control hormonal, lo cual está relacionado con una buena calidad de vida y con un plan para controlar los síntomas de la menopausia. En las mujeres premenopáusicas que no presentan cáncer de mama debe considerase el reemplazo hormonal para tratar los síntomas menopáusicos. Si no se ha extirpado el útero, recomendamos un reemplazo hormonal con estrógeno y progesterona para protegerlo. Si se ha extirpado, solo utilizamos estrógeno. Se ha mencionado que la progesterona puede tener un efecto perjudicial sobre el tejido mamario. Aunque las evidencias no son abrumadoras, es algo que sin duda debe ser tratado con la paciente. En las pacientes que han tomado tamoxifeno debe considerarse la extirpación uterina. El tamoxifeno duplica o triplica el riesgo de cáncer uterino. En estos casos hay suficientes motivos para considerar una histerectomía. Por cierto, si hay antecedentes de exámenes de Papanicolaou anormales o hay fibromas sintomáticos, también debe considerarse una histerectomía. La desventaja es que aumenta los costos, el tiempo de hospitalización y el potencial de complicaciones. No se han informado

25
would be another reason to consider a hysterectomy. I think the downside is that it certainly increases cost, hospitalization --- potential hospitalization and potential complications. And again, as I said, there’s no reports of cancer in that cornual portion of the fallopian tube following risk-reducing salpingo-oophorectomy.
cánceres en la porción del cuerno uterino de las trompas luego de una salpingo-ooforectomía profiláctica.
This is an important point and something that’s actually changed in the last several years. If you really look at the risk of ovarian cancer by age 50, what you’ll notice is that in BRCA1 mutation carriers, it’s fairly substantial. So 11 to 21 percent risk of ovarian cancer by the age of 50. But, for BRCA2 mutation carriers, it’s really only a 2 to 3 percent risk. So what I will --- I will tailor the timing of the procedure based on whether someone has a BRCA1 or BRCA2 mutation. For BRCA1 mutation carriers, I really feel more comfortable having those ovaries out sometime by the age of 40. For BRCA2 mutations carriers, I’m okay waiting until sometime in the --- the mid forties. The reason that we don’t wait until after 50 to remove the --- to recommend removing the ovaries in BRCA2 mutation carriers is that, again, there is a substantial decrease in breast cancer risk if we remove the ovaries before menopause. And so that --- that is an advantage that you will lose if you wait until after menopause to remove the ovaries in BRCA2 mutation carriers.
El criterio del momento más oportuno para el procedimiento ha cambiado en los últimos años. El riesgo de cáncer de ovario a los 50 años para las portadoras de mutaciones BRCA1 es sustancial. El riesgo varía entre el 11% y el 21% a esta edad. Para las portadoras de la mutación BRCA2, es de apenas 2% a 3%. Por eso, solemos adaptar el momento en que realizamos el procedimiento al tipo de mutación. Para las portadoras de BRCA1, preferimos extirpar los ovarios antes de los 40 años, mientras que para las portadoras de BRCA2, usualmente esperamos hasta mediados de los 40. La razón para no esperar hasta después de los 50 años a fin de recomendar la extirpación de los ovarios en las portadoras de BRCA2 es la disminución sustancial en el riesgo de cáncer de mama si los extirpamos antes de la menopausia. Esta ventaja se pierde si se espera hasta la menopausia para extirpar los ovarios en las portadoras de BRCA2.

26
So what’s the role of hormonal replacement? I think it’s very important to speak with patients. It can certainly help with some of the side effects and I think what’s important is to differentiate hormone replacement in a 55 year old versus hormone replacement in a 39 year old. The data from the Women’s Health Initiative in 55 year olds does not really apply to our young mutation carriers.
¿Cuál es la función del reemplazo hormonal? Es muy importante hablar con las pacientes. Ciertamente, puede ayudar con algunos efectos secundarios y creo que es importante diferenciar entre el reemplazo hormonal a los 55 años y a los 39. Los datos de la Iniciativa de Salud de las Mujeres para las pacientes de 55 años no se aplican a las portadoras jóvenes.
So there’s been one study that’s been performed that’s been able to allow us to inform our patients that by taking hormone replacement, whether that’s estrogen alone or estrogen and progestin in women --- women who still have a uterus, it still substantially protects those individuals from breast cancer. And I think that’s an important message because, again, the benefit from removing the --- the --- the ovaries premenopausally is substantial. And even with short-term hormone replacement, --- the benefit overall to a mutation carrier for both breast and ovarian cancer holds true.
Uno de los estudios realizados nos ha permitido informar a nuestras pacientes que la terapia de reemplazo hormonal, ya sea con estrógeno solo o combinado con progestina en las mujeres con útero, las protege sustancialmente contra el cáncer de mama. Es un mensaje importante, pues la extirpación premenopáusica de los ovarios ofrece beneficios sustanciales. Incluso con el reemplazo hormonal a corto plazo hay un beneficio general para las portadoras en cuanto al cáncer de mama y ovario.

27
So this is just a summary slide talking about risk-reducing surgery that it’s really optimized when you counsel the patient beforehand that you perform the appropriate surgery and when you manage the menopausal consequences And absolutely very importantly, is that they undergo comprehensive pathologic evaluation.
Esta diapositiva es un resumen optimizado de la cirugía profiláctica que resulta útil al asesorar a las pacientes antes de realizar la cirugía apropiada y al manejar las consecuencias menopáusicas. Es muy importante realizar una evaluación patológica completa.
And this is just important to let you know that the Society of Gynecologic Oncologists do have a statement on prophylactic salpingo-oophorectomy as well as the American College of OB/GYN and these resources are available to physicians who will be managing these high-risk individuals.
Igualmente importante es informarles que la Sociedad de Oncólogos Ginecológicos ha emitido una declaración sobre la salpingo-ooforectomía profiláctica, al igual que el Colegio Americano de Ginecoobstetras. Estos recursos están disponibles para los médicos a cargo de pacientes de alto riesgo.
28
I want to end on what happens when you have a BRCA mutation negative woman? What is their risk for --- for ovarian cancer? So we’ll often find breast cancer patients who test negative. And if you look at their family history, they have a fair amount of breast cancer in their family, but not ovarian cancer. And in these individuals, there’s one study that shows us that if you test negative, you have breast cancer, and you don’t have any ovarian cancer in your family, that your risk may not be substantially increased for ovarian cancer. So that subsequently means you may not need to have that intense screening and prophylactic surgery.
Para finalizar, explicaré qué sucede cuando no hay mutación BCRA. ¿Cuál es el riesgo de cáncer de ovario? Solemos tener pacientes con cáncer de mama, pero resultados negativos. Al analizar los antecedentes familiares se comprueba una frecuencia notable de cáncer de mama, pero no de ovario. Un estudio de estas pacientes indica que si la prueba de mutación es negativa y la paciente tiene cáncer de mama, pero la familia no presenta cáncer de ovario, el riesgo de este tipo de cáncer no siempre es sustancialmente mayor. Esto significa que tal vez no necesite exámenes de detección frecuentes o cirugía profiláctica.
So in summary, I want to highlight four points. First, knowing the BRCA status helps to better define ovarian cancer risk. So is someone at 1 percent risk for ovarian cancer, or is someone at 40 percent ovarian cancer? Those are very different and our recommendations for management are --- are different, based on that risk. Second, prophylactic risk-reducing salpingo-oophorectomy decreases substantially the risk of ovarian cancer but also substantially reduces the risk of breast cancer when it’s performed premenopausally. The third key point is that special pathology review, it --- it needs to be arranged with your pathologist. So this is not something that they routinely do, so a phone call needs to be done to the pathologist to alert them. And finally, hormone replacement therapy can really help with postoperative symptoms and to make the quality of life of these individuals who are at increased risk for cancer not so bad. Thank you very much. I would really welcome any feedback on this
Para resumir, quiero destacar cuatro puntos. Primero, saber si hay mutación BRCA ayuda a definir el riesgo de cáncer de ovario. ¿Tiene un riesgo de cáncer de ovario del 1% o del 40%? Son cifras muy diferentes y nuestras recomendaciones de manejo varían según el riesgo. Segundo, la salpingo-ooforectomía profiláctica reduce sustancialmente el riesgo de cáncer de ovario, pero también el de cáncer de mama si se realiza antes de la menopausia. El tercer punto clave es que un patólogo debe realizar una revisión patológica. Este no es un procedimiento habitual, de modo que es necesario advertir al patólogo. Por último, la terapia de reemplazo hormonal puede aliviar los síntomas postoperatorios y mejorar la calidad de vida de las pacientes con mayor

29
talk and I appreciate your time. riesgo de cáncer. Muchas gracias. Agradeceremos cualquier comentario sobre esta presentación. Gracias por su tiempo.





























