Embed Size (px)
Citation preview

230 | Healio.com/Pediatrics PEDIATRIC ANNALS 42:6 | JUNE 2013
Healthy BabyPractical advice for treating newborns and toddlers.
Infantile hemangiomas, which occur in about 4% to 5% of all children, create a difficult management dilemma in
routine pediatric practices and continue to stir debate and controversy.1 Practitioners are aware that all elevated hemangiomas and most flat hemangiomas typically grow throughout the first year of life, and that most elevated ones spontaneously involute over the next 5 to 10 years. The flat, less conspicuous hemangiomas often do not. Nonetheless, why should a clinician be concerned about these benign lesions?
I think it may become incumbent upon the pediatric community to alter their ap-proach to most hemangiomas. At birth, 65% of hemangioma precursors were pres-ent. A recent photographic report showed that the most rapid growth of hemangio-mas occurred between age 5.5 weeks and age 7.5 weeks.2 This age factor may be critical when deciding upon using a more prophylactic type of treatment, such as propanolol, because most children with hemangiomas are not referred to a derma-tologist until age 5 months.2 These authors have even suggested biweekly monitoring for any high-risk hemangiomas, such as
those listed in Sidebar 1 (see page 231), after the first month of age.2
Although the lesions are always benign and usually self-limited, some of them may be located in areas that become life-threat-ening or function-threatening, some may ulcerate and bleed, and some may lead to significant psychosocial distress or may cause permanent residual skin changes that are cosmetically undesirable.1,3 Important-ly, clinicians cannot reliably predict which hemangiomas in the first few months are going to create any of these problems. In addition, one must be very diligent about the further evaluation of children with pos-sible PHACE syndrome or multiple hem-angiomatosis, as additional expert consul-tation will be needed.1,4
CATEGORIZATION OF INFANTILE HEMANGIOMAS
Infantile hemangiomas are generally classified as focal, segmental, or indetermi-nate, and then subcategorized further into superficial, mixed, or deep. Tollefson et al2 scored hemangiomas based on intensity of color, degree of elevation, and distortion of
local landmarks. These parameters could be helpful for pediatricians too. I recom-mend that pediatricians read the entire electronic version of their article in August 2012 issue of Pediatrics for further edifi-cation as to whether and when to initiate therapy. I initially missed the true impact of this article because I rely more heavily on the paper version of the journal.
For the practitioner, it is the numerous smaller hemangiomas, the less conspicu-ous ones, or the more cosmetically subtle but noticeable hemangiomas that can cre-ate difficult psychosocial or emotional dilemmas for parents and practitioners when deciding upon whether to treat. Hindsight is always much better, and once again, as with other more cosmetic con-ditions such as plagiocephaly, early tim-ing of therapy may be much more critical than previously widely believed.5 It is also much more difficult to be prescient about the severity or complexity of these types of hemangiomas.
Although treatment timing and thera-peutic choices have been completely revo-lutionized in the past 4 years with the use
Treating Infantile Hemangiomatosis: A Case Study Stan L. Block, MD, FAAP; and Lindsay Blackmon, MD
Stan L. Block, MD, FAAP, is Professor of Clinical
Pediatrics, University of Louisville, and University
of Kentucky, Lexington, KY; President, Kentucky Pe-
diatric and Adult Research Inc.; and general pedia-
trician, Bardstown, KY. Lindsay Blackmon, MD, is a
pediatric resident at the University of Kentucky.
Address correspondence to Stan L. Block, MD,
FAAP, via email: [email protected].
Disclosure: Dr. Block has no relevant financial
relationships to disclose.
doi: 10.3928/00904481-20130522-05
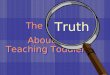
Figure 1. The photographs show the regression of the raised scalp focal hemangioma from age 4 months (A) at the initiation of treatment with propanolol (2 mg/kg/day); age 5 months (B); age 6.5 months (C); and age 9 months (D). The hemangioma sequentially becomes much less bright red, and totally flattened after 5 months of treatment.
A D
B
C
All i
mag
es c
ourte
sy o
f Lin
dsay
Bla
ckm
on, M
D.

PEDIATRIC ANNALS 42:6 | JUNE 2013 Healio.com/Pediatrics | 231
Healthy Baby
of propanolol,4 they still remain controver-sial. Before 2008, corticosteroids and laser therapy had been the mainstay of treatment for life-threatening, functioning-threaten-ing, complicated, or difficult lesions. How-ever, most other types of hemangiomas have been “treated” with benign neglect, knowing that most would eventually spon-taneously involute and dissipate by 6 to 10 years of age, leaving only minor or no re-sidual signs.
But is this last assumption true? Nearly 75% of nodular hemangiomas reportedly create discernible residual skin changes.6 The growth rate of hemangiomas is un-predictable and quite variable, and 12% are significantly complex.7 Adding to the clinicians’ consternation, no pharmaco-logic agents have been approved by the US Food and Drug Administration for the treat-ment of infant hemangiomas; no consen-sus guidelines from pediatric groups were available prior to 2013; and very few ran-domized control trials comparing the new-est therapy, propanolol, with placebo have been published.
USE OF PROPANOLOL IN OUTPATIENT SETTINGS
Overall, propanolol appears to be a very safe drug to use in infants. It certainly is much safer than long-term treatment with corticosteroids, vincristine, or methotrex-ate; and it is much more tolerable and in-expensive than laser therapies. In the past, most practitioners had used propanolol in at least a few infants who had supraventricular tachycardia. But for these patients, propa-nolol therapy has usually been initiated in an inpatient setting under cardiac monitor-ing. For routine infantile hemangiomas, we have begun to initiate propanolol treatment in healthy children without cardiac disease in outpatient settings.
Nearly 48 (56%) of the 85 articles evalu-ated by Drolet et al7 observed no compli-cations with propanolol use in any patient. Ensuing articles have subsequently report-ed occasional occurrences of hypotension, hypoglycemia, restless sleep, constipation,
and very rarely hypokalemia or adrenergic blockade (worsening asthma).4,7 Most of these adverse events were “infrequent and asymptomatic.”7 In contrast, Hermans et al8 recently reported somewhat higher rates for adverse effects (possible “background noise”) over an average of 10 months of therapy for hypotension (3.4%), noctur-nal restlessness (22.4%), cold extremities (36.2%), and wheezing (9.2%). This study had no control population, only 1 patient discontinued therapy, and the dose was re-duced in 8% of children.
In 3 prospective studies of propano-lol, the only clinically recognizable ad-verse events were cold extremities and prolonged capillary refill. The most wor-risome — albeit rare — serious concern with initiation of propanolol treatment, even with lower doses, is hypoglycemia and/or hypoglycemic seizures. But the few reported incidents were often associ-ated with “poor oral intake or concomitant infection.”7 It is important to remember that propanolol may mask some of the major symptoms of hypoglycemia, such as shakiness, anxiety, and hunger. Thus, parents should be advised that increased sweating is thought to be the most reliable and prominent symptom of hypoglycemia in infants before they develop more wor-risome symptoms such as lethargy, poor feeding, and seizures.
Other Precautions with Propanolol The recent use (within a few weeks) of
corticosteroids is believed to place these in-fants at potential increased risk for hypogly-cemia as well. Temporary discontinuation of propanolol may be prudent during any viral illness associated with reduced oral in-take, wheezing, or moderately severe cough (the only sign parents may have of a wheez-ing infant) (see Sidebar 2). Giving the dose of medication with or after meals may be advisable. Frequent feeding during the night for young infants or preterm infants is sug-gested as well.
Inpatient monitoring is advised for those who have PHACE syndrome; those with comorbid conditions of the cardiovascular, respiratory, or endocrine systems; those with visceral hemangiomas; and for those younger than 2 months or 48 weeks cor-rected gestational age.
Initiation of Propanolol TherapyOutpatient monitoring for pulse and
blood pressure is advised only at base-line, 1 and 2 hours after the first dose,
SIDEBAR 1.
Areas for High-Risk Hemangiomas
• Any facial hemangioma, particularly near
the eye, ear, mouth, or nasal region
• Facial hemangioma > 5 cm in diameter
(evaluate for PHACE syndrome: cerebro-
vascular, cardiac, coarctation of aorta,
ocular, and other anomalies)
• Lumbosacral or perineal hemangioma
• Airway ± “beard area” hemangioma
• Multifocal (≥ 5) hemangiomas (evaluate
particularly for hepatic hemangiomas or
other visceral ones)
Adapted from Tollefson et al2
SIDEBAR 2.
Propanolol Precautions • Three obvious physical signs
- Cardiogenic shock
- Heart failure
- Asthma (which is almost never diagnosed
younger than 12 months)
• Three physical signs that each clinical
examination should uncover:
- Hypotension (blood pressure)
- Bradycardia (heart rate)
- Arrhythmia (heart rate)
• Order an ECG when the screening history
reveals:
- Below-normal heart rate (< 70 BPM
younger than 1 month; < 80 BPM age 1 to
12 months)
- Family history of congenital heart condi-
tions or arrhythmias
- History of arrhythmia or connective tissue
disease in the child or family
BPM = beats per minute; ECG = electrocardiogram.
Adapted from Drolet et al7

232 | Healio.com/Pediatrics PEDIATRIC ANNALS 42:6 | JUNE 2013
Healthy Baby
or with any significant increase in dose (> 0.5 mg/kg/day).3,7 Routine electrocar-diogram or Holter monitoring is not in-dicated for otherwise healthy infants. My preference for dosing is 2 mg/kg/day di-vided in a twice-daily dose. This keeps all the calculations simple, easy to remem-ber, and easy to perform for practitioners (1 mg/kg per dose) and all the dosings much simpler for parents (adherence to twice daily dosing is far superior to three-times daily dosing). I suggest follow-up at 1 week and then monthly to evaluate the hemangiomas, for adverse events, and for monitoring of pulse and blood pressure.
Subsequently, how does one decide when and whether to “pull the trigger” and when to start therapy for many of these more benign, non-threatening lesions? When does the risk-to-benefit ratio become worthwhile? 4
What to Expect with Propanolol Therapy
The recent article by Hermans et al8 showed that nearly all of the 173 patients responded strikingly to propanolol therapy with a fading of abnormal color, immediate cessation of growth (a critical component of the early timing argument), softening, and rapid induction of regression. Medication was effective even though the mean age of
patients was older (4.8 months old) and all of the lesions were potentially threatening or complicated.
WHAT TO EXPECT WITH PROPANOLOL THERAPY: A PHOTOGRAPHIC CASE
Infantile hemangiomas are more com-monly observed in white, female, and pre-term infants, and those born to mothers with advanced maternal age (some apply here). The same white female infant is shown in each of the images.
The vigorous, pink, active, white female infant was born at 36 weeks gestation by spontaneous vaginal delivery with APGARS of 9/9 to a healthy 28-year old primigravida mother. The mother first noticed a small, dark, reddened, round discolored lesion on the thigh at 12 hours of age. Over the en-suing first month of age, several more red raised and flat hemangiomas had “popped up,” which were described as even bigger and redder. By age 2 months, she had about 10 hemangioma lesions present, and thus she was considered as having “infantile heman-giomatosis” (see Sidebar 1, page 231).
Indecision About Starting TreatmentSubsequently, she was seen in the local
hematology-oncology specialty clinic for infantile hemangiomatosis, where an ultra-
A B
C
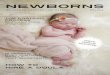
Figure 2. The photographs show the regression of the slightly raised focal leg hemangioma from age 4 months (A) at the initiation of treatment with propanolol (2 mg/kg/day); age 5 months (B); age 6.5 months (C); and age 9 months (D). The hemangioma sequentially faded to much less bright red, and eventually totally flattened with no more satellite metastasis after 2.5 months of treatment. The parents may want to consider further laser therapy for cosmetic reasons because these hemangiomas have a tendency not to dissipate further over time, unlike the hemangioma in Figure 1.
A
B
C
D
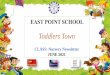
Figure 3. The photographs show the regression of the large, raised, solitary focal hemangioma and 4 brighter red hemangiomas from age 4 months (A) at the initiation of treatment with propanolol (2 mg/kg/day); age 5 months (B); age 6.5 months (C); and age 9 months (D). Each of the hemangiomas se-quentially faded to much less bright red, eventually totally flattened, and developed no more satellite metastases after 5 months of treatment. This dra-matic fading is a much more acceptable cosmetic result. Further laser therapy for cosmetic reasons for these proximal 3 particular focal hemangiomas will probably not be necessary as they are likely to totally disappear, and the well-faded focal ones on the sacral area are smaller, barely perceptible, and will remain covered by clothing.
D

PEDIATRIC ANNALS 42:6 | JUNE 2013 Healio.com/Pediatrics | 233
Healthy Baby
sound of the liver and spleen was performed. The results were normal. The mother was told that oral propanolol therapy could be considered as an option, but it was not rec-ommended for the patient at this point due to the lack of more serious or threatening lesions. By age 4 months, the mother no-ticed that the lesions on the head and back had continued to grow and proliferate (see Figures 1A and 3A). Furthermore the sur-face area of the flatter lesions on the hand and leg had continued to spread (see Figures 2A and 4A).
By age 4 months, the mother had be-come quite alarmed at the continued rapid proliferation of the hemangiomas. She had read about their potential for low-grade re-
sidual damage, such as permanent boggy dermis and telangiectasias, and the cosmet-ic and psychosocial issues the child would certainly encounter during the next decade of her life, even if many of the hemangio-mas did eventually disappear.
She had read even more details about the growing widespread use and the ben-efits of propanolol for hemangiomas. Thus, she elected to start therapy at age 4 months, particularly in light of several new barely perceptible lesions still cropping up on her child’s back.
Starting PropanololShe was advised to have the infant’s
blood pressure checked initially, at 1 and 2 hours after the first dose, or with any in-creased dose of medication. She was also instructed to wake the baby for a feeding at least once or twice during the night, and to particularly watch for any signs of hypogly-cemia.
She initiated propanolol therapy at 2 mg/kg/day divided in twice-daily doses. Drug adherence was good, as the family missed at most 1 to 2 doses monthly with the easier twice-daily dosing. With their hectic profes-sional work schedules, thrice-daily dosing would have doomed drug adherence. Pro-panolol was palatable and very inexpensive. The only adverse effects they observed with the infant were occasional cold hands and feet for less than a 1-hour interval.
Beneficial Effects of PropanololThe child received a total of 5 months
of propanolol therapy, with an increased dose every 2 months in order to maintain a total dose of 2 mg/kg/day. One can see in the sequential photographs of each group of lesions at baseline (age 4 months), age 5 months, age 6.5 months, and age 9 months that the raised lesions on the head (see Fig-ures 1B, C, D), the back (see Figures 3B, C, and D), and hand (see Figures 4B and C) had nearly flattened completely. Most of the hemangiomas except for those on the hand were much lighter, smaller, or al-most resolved over time. The hand merely appeared about half as dark red. During the
last 2 months of therapy, the parents noted no more additional benefits to therapy and elected to cease the propanolol at 9 months of age. No rebound growth of the heman-giomas was observed during the month post-therapy, which has been reported else-where.7
When asked if they would have done anything differently, the two parents re-sponded that they “wished they had started the propanolol at age 2 months” (and I now agree), which would have been the earliest possible time to avoid any need for moni-toring in the hospital. They stated that if cli-nicians or parents had any concerns about the cosmetic size or locations of the lesions, they would advise physicians to initiate therapy in the child. The article by Tollef-son et al2 may substantiate their concerns that the early unimpeded growth of super-ficial hemangiomas can lead to irreversible skin changes.
They are definitely considering future laser therapy of the flat hemangiomas of the hand and leg within the next few years.
REFERENCES 1. Lauren C, Garzon MC. Treatment of infantile
hemangiomas. Pediatr Ann. 2012;41(8):1-7. 2. Tollefson MM, Frieden IJ. Early growth of infan-
tile hemangiomas: what parents’ photographs tell us. Pediatrics. 2012;130(2):e314-320.
3. Metry DW. Management of infantile hem-angiomas. Available at: www.uptodate.com/contents/management-of-infantile-hemangiomas?source=search_result&search=hemangioma+children&selectedTitle=3~150. Ac-cessed May 15, 2013.
4. Chen TS, Eichenfield LF, Friedlander SF. Infan-tile hemangiomas: an update on pathogenesis and therapy. Pediatrics. 2013;131(1):99-108.
5. Block SL. ‘Skull-duggery’ and the manage-ment of positional plagiocephaly. Pediatr Ann. 2012;41(12):497-501.
6. Bauland CG, Lüning TH, Smit JM, Zeebregts CJ, Spauwen PH. Untreated hemangiomas: growth pattern and residual lesions. Plast Reconstr Surg. 2011;127(4):1643-1648.
7. Drolet BA, Frommelt PC, Chamlin SL, et al. Initiation and use of propranolol for infantile hemangioma: report of a consensus conference. Pediatrics. 2013;131(1):128-140.
8. Hermans DJ, Bauland CG, Zweegers J, van Bey-num IM, van der Vleuten CJ. Propranolol in a case series of 174 patients with complicated in-fantile haemangioma: indications, safety and fu-ture directions. Br J Dermatol. 2013;168(4):837-843.
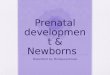
Figure 4. The 3 photographs show the regression of the minimally raised segmental hand hemangioma from age 4 months (A) at the initiation of treatment with propanolol (2 mg/kg/day); age 6.5 months (B); and age 9 months (C). The hemangioma sequential-ly faded to much less bright red and became totally flattened with no more satellite metastases after 2.5 months of treatment. This fading is a marginally ac-ceptable cosmetic result. The parents will likely con-sider further laser therapy for cosmetic reasons as the location of this segmental hemangioma is more conspicuous and will be unlikely to dissipate further over time, unlike the hemangioma in Figure 1.
A B
C

Reproduced with permission of the copyright owner. Further reproduction prohibited withoutpermission.